
Prognostic Value of Circulating Cell-Free DNA Concentration and Neutrophil-to-Lymphocyte Ratio in Patients with Pancreatic Ductal Adenocarcinoma: A Prospective Cohort Study

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
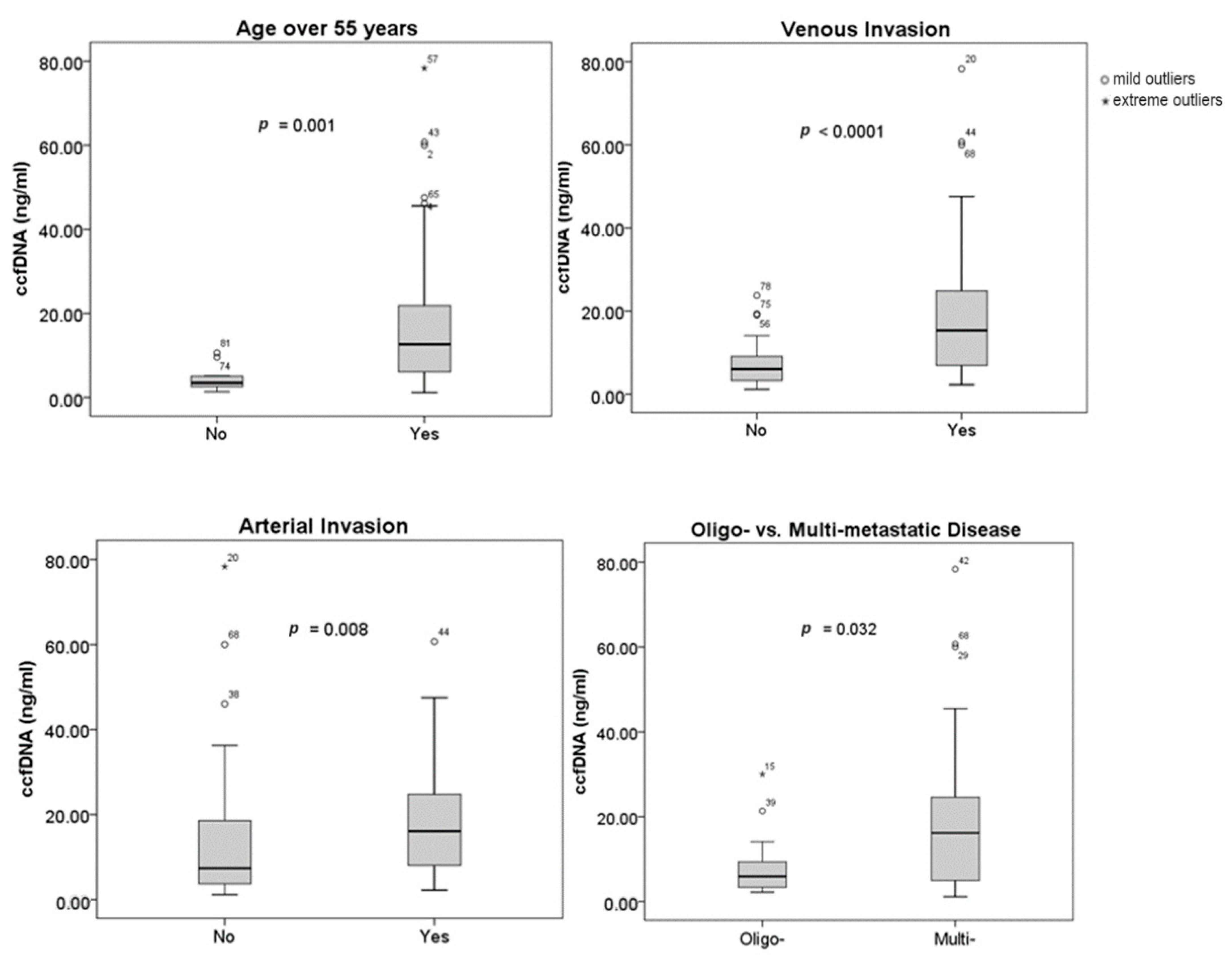
2.2. Measurement of ccfDNA Concentration and Correlations with Clinical and Tumor Characteristics
2.3. Survival Analysis
2.4. Higher ccfDNA Concentration and NLR Are Associated with Poorer Survival in PDAC Patients
2.5. The Combination of ccfDNA Concentration and NLR Values Significantly Improves Prognostic Accuracy of PDAC Patients
3. Materials and Methods
3.1. Study Design
3.2. Blood Sample Collection and ccfDNA Isolation from Plasma
3.3. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic Cancer; Elsevier: Amsterdam, The Netherlands, 2008; Volume 395, Available online: www.thelancet.com (accessed on 26 July 2023).
- Garrido-Laguna, I.; Hidalgo, M. Pancreatic Cancer: From State-of-the-Art Treatments to Promising Novel Therapies. Nat. Rev. Clin. Oncol. 2015, 12, 319–334. [Google Scholar] [CrossRef]
- Christenson, E.S.; Jaffee, E.; Azad, N.S. Current and Emerging Therapies for Patients with Advanced Pancreatic Ductal Adenocarcinoma: A Bright Future. Lancet Oncol. 2020, 21, e135–e145. [Google Scholar] [CrossRef]
- Pereira, S.P.; Oldfield, L.; Ney, A.; Hart, P.A.; Keane, M.G.; Pandol, S.J.; Li, D.; Greenhalf, W.; Jeon, C.Y.; Koay, E.J.; et al. Early Detection of Pancreatic Cancer. Lancet Gastroenterol. Hepatol. 2020, 5, 698–710. [Google Scholar] [CrossRef]
- Ligorio, M.; Sil, S.; Malagon-lopez, J.; Nieman, L.T.; Pilato, M.D.i.; Ebright, R.Y.; Karabacak, M.N.; Anupriya, S.; Liu, A.; Jordan, N.V.; et al. Stromal Microenvironment Shapes the Intratumoral Architecture of Pancreatic Cancer. Cell 2020, 178, 160–175. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, J.R.; Puig, C.A.; Shubert, C.R.; Groeschl, R.T.; Habermann, E.B.; Kendrick, M.L.; Nagorney, D.M.; Smoot, R.L.; Farnell, M.B.; Truty, M.J. Carbohydrate Antigen 19-9 Elevation in Anatomically Resectable, Early Stage Pancreatic Cancer Is Independently Associated with Decreased Overall Survival and an Indication for Neoadjuvant Therapy: A National Cancer Database Study. J. Am. Coll. Surg. 2016, 223, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Perusina Lanfranca, M.; Zhang, Y.; Girgis, A.; Kasselman, S.; Lazarus, J.; Kryczek, I.; Delrosario, L.; Rhim, A.; Koneva, L.; Sartor, M.; et al. Interleukin 22 Signaling Regulates Acinar Cell Plasticity to Promote Pancreatic Tumor Development in Mice. Gastroenterology 2020, 158, 1417–1432.e11. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Xue, J. Inflammation and Development of Pancreatic Ductal Adenocarcinoma. Chin. Clin. Oncol. 2019, 8, 1–10. [Google Scholar] [CrossRef]
- Iwai, N.; Okuda, T.; Sakagami, J.; Harada, T.; Ohara, T.; Taniguchi, M.; Sakai, H.; Oka, K.; Hara, T.; Tsuji, T.; et al. Neutrophil to Lymphocyte Ratio Predicts Prognosis in Unresectable Pancreatic Cancer. Sci. Rep. 2020, 10, 18758. [Google Scholar] [CrossRef]
- Oh, D.; Pyo, J.S.; Son, B.K. Prognostic Roles of Inflammatory Markers in Pancreatic Cancer: Comparison between the Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio. Gastroenterol. Res. Pract. 2018, 2018, 9745601. [Google Scholar] [CrossRef]
- Crowley, E.; Di Nicolantonio, F.; Loupakis, F.; Bardelli, A. Liquid Biopsy: Monitoring Cancer-Genetics in the Blood. Nat. Rev. Clin. Oncol. 2013, 10, 472–484. [Google Scholar] [CrossRef]
- Chen, E.; Cario, C.L.; Leong, L.; Lopez, K.; Márquez, C.P.; Chu, C.; Li, P.S.; Oropeza, E.; Tenggara, I.; Cowan, J.; et al. Cell-Free DNA Concentration and Fragment Size as a Biomarker for Prostate Cancer. Sci. Rep. 2021, 11, 5040. [Google Scholar] [CrossRef]
- de Miranda, F.S.; Barauna, V.G.; Dos Santos, L.; Costa, G.; Vassallo, P.F.; Campos, L.C.G. Properties and Application of Cell-Free DNA as a Clinical Biomarker. Int. J. Mol. Sci. 2021, 22, 9110. [Google Scholar] [CrossRef]
- Takai, E.; Totoki, Y.; Nakamura, H.; Morizane, C.; Nara, S.; Hama, N.; Suzuki, M.; Furukawa, E.; Kato, M.; Hayashi, H.; et al. Clinical Utility of Circulating Tumor DNA for Molecular Assessment in Pancreatic Cancer. Sci. Rep. 2015, 5, 18425. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, Y.; Cheng, Y.; Zhang, D.; Zhu, S.; Ma, X. Prognostic Value of Circulating Cell-Free DNA in Patients with Pancreatic Cancer: A Systemic Review and Meta-Analysis. Gene 2018, 679, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.G.; Malapelle, U.; André, F.; Paz-Ares, L.; Schuler, M.; Thomas, D.M.; Vainer, G.; Yoshino, T.; Rolfo, C. Practical Considerations for the Use of Circulating Tumor DNA in the Treatment of Patients with Cancer: A Narrative Review. JAMA Oncol. 2022, 8, 1830–1839. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.; Onieva, J.L.; Garrido-Barros, M.; Cobo-Dols, M.; Martínez-Gálvez, B.; García-Pelícano, A.I.; Dubbelman, J.; Benítez, J.C.; Martín, J.Z.; Cantero, A.; et al. Fluorometric Quantification of Total Cell-Free DNA as a Prognostic Biomarker in Non-Small-Cell Lung Cancer Patients Treated with Immune Checkpoint Blockade. Cancers 2023, 15, 3357. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Hothorn, T.; Lausen, B. On the Exact Distribution of Maximally Selected Rank Statistics. Comput. Stat. Data Anal. 2003, 43, 121–137. [Google Scholar] [CrossRef]
- Lausen, B.; Schumacher, M. Maximally Selected Rank Statistics. Biometrics 1992, 48, 73. [Google Scholar] [CrossRef]
- Toledano-Fonseca, M.; Teresa Cano, M.; Inga, E.; Gómez-España, A.; Guil-Luna, S.; García-Ortiz, M.V.; Mena-Osuna, R.; De La Haba-Rodriguez, J.R.; Rodríguez-Ariza, A.; Aranda, E. The Combination of Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio with Liquid Biopsy Biomarkers Improves Prognosis Prediction in Metastatic Pancreatic Cancer. Cancers 2021, 13, 1210. [Google Scholar] [CrossRef]
- De Oliveira, I.B.D.; Hirata, R.D.C. Circulating Cell-Free DNA as a Biomarker in the Diagnosis and Prognosis of Colorectal Cancer. Braz. J. Pharm. Sci. 2018, 54, 1–14. [Google Scholar] [CrossRef]
- Dao, J.; Conway, P.J.; Subramani, B.; Meyyappan, D.; Russell, S.; Mahadevan, D. Using CfDNA and CtDNA as Oncologic Markers: A Path to Clinical Validation. Int. J. Mol. Sci. 2023, 24, 13219. [Google Scholar] [CrossRef] [PubMed]
- Haan, D.; Bergamaschi, A.; Guler, G.D.; Friedl, V.; Ning, Y.; Reggiardo, R.; Kesling, M.; Collins, M.; Gibb, B.; Pitea, A.; et al. Validation of a Pancreatic Cancer Detection Test in New-Onset Diabetes Using Cell-Free DNA 5-Hydroxymethylation Signatures. medRxiv 2021. [Google Scholar] [CrossRef]
- Lennon, A.M.; Buchanan, A.H.; Kinde, I.; Warren, A.; Honushefsky, A.; Cohain, A.T.; Ledbetter, D.H.; Sanfilippo, F.; Sheridan, K.; Rosica, D.; et al. Feasibility of Blood Testing Combined with PET-CT to Screen for Cancer and Guide Intervention. Science 2020, 369, eabb9601. [Google Scholar] [CrossRef] [PubMed]
- Kananen, L.; Hurme, M.; Jylhä, M.; Härkänen, T.; Koskinen, S.; Stenholm, S.; Kähönen, M.; Lehtimäki, T.; Ukkola, O.; Jylhävä, J. Circulating Cell-Free DNA Level Predicts All-Cause Mortality Independent of Other Predictors in the Health 2000 Survey. Sci. Rep. 2020, 10, 13809. [Google Scholar] [CrossRef] [PubMed]
- Jylhävä, J.; Nevalainen, T.; Marttila, S.; Jylhä, M.; Hervonen, A.; Hurme, M. Characterization of the Role of Distinct Plasma Cell-Free DNA Species in Age-Associated Inflammation and Frailty. Aging Cell 2013, 12, 388–397. [Google Scholar] [CrossRef]
- Xu, X.; Yu, Y.; Shen, M.; Liu, M.; Wu, S.; Liang, L.; Huang, F.; Zhang, C.; Guo, W.; Liu, T. Role of Circulating Free DNA in Evaluating Clinical Tumor Burden and Predicting Survival in Chinese Metastatic Colorectal Cancer Patients. BMC Cancer 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Wang, D.; Hu, X.; Long, G.; Xiao, L.; Wang, Z.-M.; Zhou, L.-D. The Clinical Value of Total Plasma Cell-Free DNA in Hepatitis B Virus-Related Hepatocellular Carcinoma. Ann. Transl. Med. 2019, 7, 650. [Google Scholar] [CrossRef]
- Kirchweger, P.; Kupferthaler, A.; Burghofer, J.; Webersinke, G.; Jukic, E.; Schwendinger, S.; Weitzendorfer, M.; Petzer, A.; Függer, R.; Rumpold, H.; et al. Circulating Tumor DNA Correlates with Tumor Burden and Predicts Outcome in Pancreatic Cancer Irrespective of Tumor Stage. Eur. J. Surg. Oncol. 2022, 48, 1046–1053. [Google Scholar] [CrossRef]
- Mettler, E.; Fottner, C.; Bakhshandeh, N.; Trenkler, A.; Kuchen, R.; Weber, M.M. Quantitative Analysis of Plasma Cell-Free DNA and Its DNA Integrity and Hypomethylation Status as Biomarkers for Tumor Burden and Disease Progression in Patients with Metastatic Neuroendocrine Neoplasias. Cancers 2022, 14, 1025. [Google Scholar] [CrossRef]
- Huang, C.J.; Huang, W.Y.; Chen, C.Y.; Chao, Y.J.; Chiang, N.J.; Shan, Y.S. Cancer-Cell-Derived Cell-Free DNA Can Predict Distant Metastasis Earlier in Pancreatic Cancer: A Prospective Cohort Study. Ther. Adv. Med. Oncol. 2022, 14, 17588359221106558. [Google Scholar] [CrossRef]
- Demers, M.; Wagner, D.D. Neutrophil Extracellular Traps: A New Link to Cancer-Associated Thrombosis and Potential Implications for Tumor Progression. Oncoimmunology 2013, 2, 12–14. [Google Scholar] [CrossRef]
- Cedervall, J.; Zhang, Y.; Olsson, A.K. Tumor-Induced NETosis as a Risk Factor for Metastasis and Organ Failure. Cancer Res. 2016, 76, 4311–4315. [Google Scholar] [CrossRef]
- Cicchillitti, L.; Corrado, G.; de Angeli, M.; Mancini, E.; Baiocco, E.; Patrizi, L.; Zampa, A.; Merola, R.; Martayan, A.; Conti, L.; et al. Circulating Cell-Free DNA Content as Blood Based Biomarker in Endometrial Cancer. Oncotarget 2017, 8, 115230–115243. [Google Scholar] [CrossRef]
- Coffelt, S.B.; Wellenstein, M.D.; de Visser, K.E. Neutrophils in Cancer: Neutral No More. Nat. Rev. Cancer 2016, 16, 431–446. [Google Scholar] [CrossRef]
- Luo, G.; Guo, M.; Liu, Z.; Xiao, Z.; Jin, K.; Long, J.; Liu, L.; Liu, C.; Xu, J.; Ni, Q.; et al. Blood Neutrophil–Lymphocyte Ratio Predicts Survival in Patients with Advanced Pancreatic Cancer Treated with Chemotherapy. Ann. Surg. Oncol. 2015, 22, 670–676. [Google Scholar] [CrossRef]
- Kadokura, M.; Ishida, Y.; Tatsumi, A.; Takahashi, E.; Shindo, H.; Amemiya, F.; Takano, S.; Fukasawa, M.; Sato, T.; Enomoto, N. Performance Status and Neutrophil-Lymphocyte Ratio Are Important Prognostic Factors in Elderly Patients with Unresectable Pancreatic Cancer. J. Gastrointest. Oncol. 2016, 7, 982–988. [Google Scholar] [CrossRef]
- Mowbray, N.G.; Griffith, D.; Hammoda, M.; Shingler, G.; Kambal, A.; Al-Sarireh, B. A Meta-Analysis of the Utility of the Neutrophil-to-Lymphocyte Ratio in Predicting Survival after Pancreatic Cancer Resection; HPB. Elsevier B.V.: Amsterdam, The Netherlands, 2018; pp. 379–384. [Google Scholar] [CrossRef]
- Lapin, M.; Oltedal, S.; Tjensvoll, K.; Buhl, T.; Smaaland, R.; Garresori, H.; Javle, M.; Glenjen, N.I.; Abelseth, B.K.; Gilje, B.; et al. Fragment Size and Level of Cell-Free DNA Provide Prognostic Information in Patients with Advanced Pancreatic Cancer. J. Transl. Med. 2018, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- An, X.; Ding, P.R.; Li, Y.H.; Wang, F.H.; Shi, Y.X.; Wang, Z.Q.; He, Y.J.; Xu, R.H.; Jiang, W.Q. Elevated Neutrophil to Lymphocyte Ratio Predicts Survival in Advanced Pancreatic Cancer. Biomarkers 2010, 15, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Stotz, M.; Gerger, A.; Eisner, F.; Szkandera, J.; Loibner, H.; LRess, A.; Kornprat, P.; AZoughbi, W.; Seggewies, F.S.; Lackner, C.; et al. Increased Neutrophil-Lymphocyte Ratio Is a Poor Prognostic Factor in Patients with Primary Operable and Inoperable Pancreatic Cancer. Br. J. Cancer 2013, 109, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Varzaru, B.; Iacob, R.A.; Croitoru, A.E.; Iacob, S.M.; Radu, C.E.; Dumitrescu, S.M.; Gheorghe, C. Real-Life Results of Palliative Chemotherapy in Metastatic Pancreatic Ductal Adenocarcinoma. Cancers 2023, 15, 3500. [Google Scholar] [CrossRef]
- Toledano-Fonseca, M.; Cano, M.T.; Inga, E.; Rodríguez-Alonso, R.; Gómez-España, M.A.; Guil-Luna, S.; Mena-Osuna, R.; De la Haba-Rodríguez, J.R.; Rodríguez-Ariza, A.; Aranda, E. Circulating cell-free dna-based liquid biopsy markers for the non-invasive prognosis and monitoring of metastatic pancreatic cancer. Cancers 2020, 12, 1754. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 82) |
|---|---|
| Median age | 67 (62–70) |
| Age ≥ 55 years, n (%) | 73 (89.02) |
| Sex, male, n (%) | 45 (54.88) |
| ECOG-PS, n (%) | |
| 0/1 | 76 (92.7) |
| 2/3 | 6 (7.3) |
| CA 19-9, n (%) | |
| <39 U/mL | 24 (29.27) |
| ≥39 U/mL | 55 (67.07) |
| Missing data | 3 (3.66) |
| Median tumor size (mm) | 40 (32.75–50) |
| Primary tumor location, n (%) | |
| Head/uncinate process | 51 (62.2) |
| Body/tail | 31 (37.8) |
| Vascular involvement, n (%) | |
| Venous invasion | 56 (68.29) |
| Arterial invasion | 36 (43.9) |
| Tumor stage *, n (%) | |
| IA | 1 (1.2) |
| IB | 8 (9.8) |
| IIA | 2 (2.4) |
| IIB | 8 (9.8) |
| III | 21 (25.6) |
| IV | 42 (51.2) |
| Metastatic status, n (%) | |
| No metastases | 35 (42.7) |
| Oligo-metastatic | 17 (20.7) |
| Multi-metastatic | 30 (36.6) |
| ccfDNA concentration (ng/mL) | 10.3 (5.1–21.46) |
| NLR | 3.22 (2.34–4.42) |
| Prognostic Factor | p | HR (95% CI) |
|---|---|---|
| Age (years) | 0.446 | 0.99 (0.96–1.02) |
| Age > 55 years | 0.084 | 1.88 (0.92–3.85) |
| Sex: Male vs. Female | 0.242 | 0.76 (0.48–1.20) |
| Diabetes | 0.415 | 0.82 (0.51–1.32) |
| Baseline ECOG-PS (0/1 vs. 2) | 0.057 | 2.28 (0.98–5.34) |
| Tumor size | 0.004 | 1.02 (1.01–1.04) |
| Tumor location: | ||
| Head vs. Body | 0.623 | 0.88 (0.53–1.46) |
| Head vs. Tail | 0.19 | 1.66 (0.78–3.53) |
| Metastatic status: | ||
| M0 vs. Oligo-metastatic | 0.018 | 2.09 (1.13–3.84) |
| M0 vs. Multi-metastatic | 0.001 | 2.53 (1.49–4.29) |
| Tumor stage: | ||
| Stage I/II vs. Stage III | 0.717 | 1.13 (0.59–2.16) |
| Stage I/II vs. Stage IV | 0.013 | 2.08 (1.16–3.73) |
| CA 19-9 ≥ 39 UI/mL vs. <39 UI/mL | 0.377 | 0.79 (0.49–1.31) |
| NLR ≥ 3.31 vs. NLR < 3.31 | 0.017 | 0.58 (0.37–0.91) |
| ccfDNA concentration (continuous) | 0.104 | 1.01 (0.99–1.03) |
| ccfDNA levels ≥ 25.79 ng/mL vs. <25.79 ng/mL | 0.015 | 0.46 (0.25–0.86) |
| Combination of ccfDNA levels with NLR | ||
| NN vs. PN | 0.048 | 1.62 (1.01–2.62) |
| NN vs. PP | 0.002 | 3.21 (1.51–6.83) |
| Prognostic Factor | p | HR (95% CI) |
|---|---|---|
| Age > 55 years | 0.27 | 1.56 (0.71–3.45) |
| Baseline ECOG-PS (0/1 vs. 2) | 0.748 | 0.85 (0.32–2.29) |
| Tumor size | 0.049 | 1.02 (1.00–1.03) |
| Metastatic status: | ||
| M0 vs. Oligo-metastatic | 0.026 | 3.78 (1.17–12.19) |
| M0 vs. Multi-metastatic | 0.018 | 5.37 (1.33–21.62) |
| Tumor stage: | ||
| Stage I/II vs. Stage III | 0.6 | 0.83 (0.41–1.69) |
| Stage I/II vs. Stage IV | 0.136 | 0.35 (0.09–1.39) |
| NLR ≥ 3.31 vs. NLR < 3.31 | 0.192 | 0.71 (0.43–1.19) |
| ccfDNA levels ≥ 25.79 ng/mL vs. <25.79 ng/mL | 0.041 | 0.45 (0.21–0.97) |
| Prognostic Factor | p | HR (95% CI) |
|---|---|---|
| Age > 55 years | 0.364 | 1.44 (0.66–3.17) |
| Baseline ECOG-PS (0/1 vs. 2) | 0.894 | 0.93 (0.34–2.56) |
| Tumor size | 0.057 | 1.02 (1.00–1.03) |
| Metastatic status: | ||
| M0 vs. Oligo-metastatic | 0.026 | 3.78 (1.17–12.21) |
| M0 vs. Multi-metastatic | 0.015 | 5.73 (1.40–23.37) |
| Tumor stage: | ||
| Stage I/II vs. Stage III | 0.561 | 0.81 (0.39–1.65) |
| Stage I/II vs. Stage IV | 0.104 | 0.32 (0.08–1.26) |
| Combination of ccfDNA with NLR | ||
| NN vs. PN | 0.092 | 1.56 (0.93–2.63) |
| NN vs. PP | 0.030 | 2.81 (1.11–7.15) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varzaru, B.; Iacob, R.A.; Bunduc, S.; Manea, I.; Sorop, A.; Spiridon, A.; Chelaru, R.; Croitoru, A.; Topala, M.; Becheanu, G.; et al. Prognostic Value of Circulating Cell-Free DNA Concentration and Neutrophil-to-Lymphocyte Ratio in Patients with Pancreatic Ductal Adenocarcinoma: A Prospective Cohort Study. Int. J. Mol. Sci. 2024, 25, 2854. https://doi.org/10.3390/ijms25052854
Varzaru B, Iacob RA, Bunduc S, Manea I, Sorop A, Spiridon A, Chelaru R, Croitoru A, Topala M, Becheanu G, et al. Prognostic Value of Circulating Cell-Free DNA Concentration and Neutrophil-to-Lymphocyte Ratio in Patients with Pancreatic Ductal Adenocarcinoma: A Prospective Cohort Study. International Journal of Molecular Sciences. 2024; 25(5):2854. https://doi.org/10.3390/ijms25052854
Chicago/Turabian StyleVarzaru, Bianca, Razvan Andrei Iacob, Stefania Bunduc, Ioana Manea, Andrei Sorop, Andreea Spiridon, Raluca Chelaru, Adina Croitoru, Mihaela Topala, Gabriel Becheanu, and et al. 2024. "Prognostic Value of Circulating Cell-Free DNA Concentration and Neutrophil-to-Lymphocyte Ratio in Patients with Pancreatic Ductal Adenocarcinoma: A Prospective Cohort Study" International Journal of Molecular Sciences 25, no. 5: 2854. https://doi.org/10.3390/ijms25052854
APA StyleVarzaru, B., Iacob, R. A., Bunduc, S., Manea, I., Sorop, A., Spiridon, A., Chelaru, R., Croitoru, A., Topala, M., Becheanu, G., Dumbrava, M., Dima, S., Popescu, I., & Gheorghe, C. (2024). Prognostic Value of Circulating Cell-Free DNA Concentration and Neutrophil-to-Lymphocyte Ratio in Patients with Pancreatic Ductal Adenocarcinoma: A Prospective Cohort Study. International Journal of Molecular Sciences, 25(5), 2854. https://doi.org/10.3390/ijms25052854