

Interleukin-1β/Interleukin (IL)-1-Receptor-Antagonist (IL1-RA) Axis in Invasive Bladder Cancer—An Exploratory Analysis of Clinical and Tumor Biological Significance


 ,
,  ,
,  and
and
Abstract
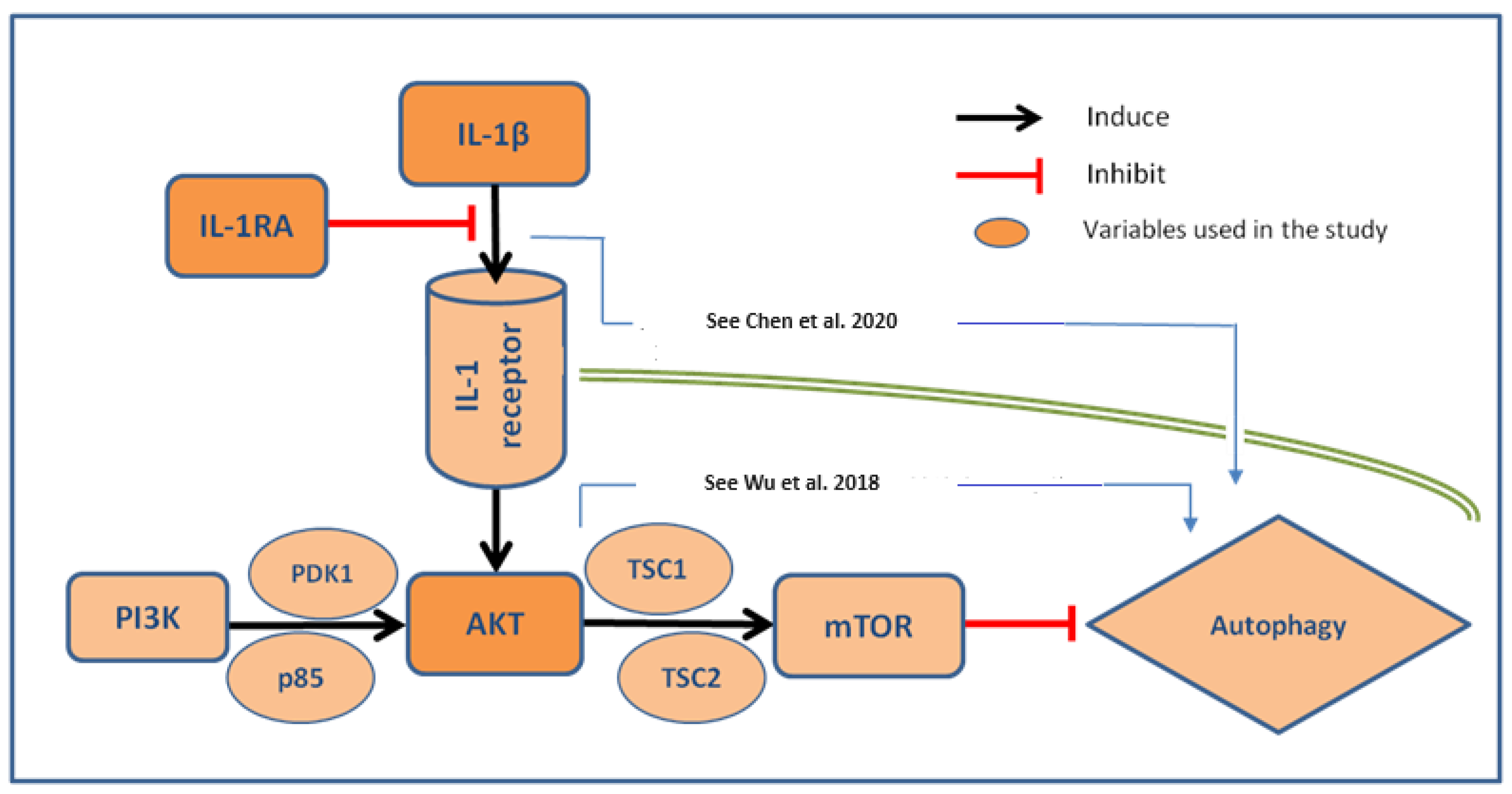
1. Introduction
2. Results
2.1. Patients’ Characteristics
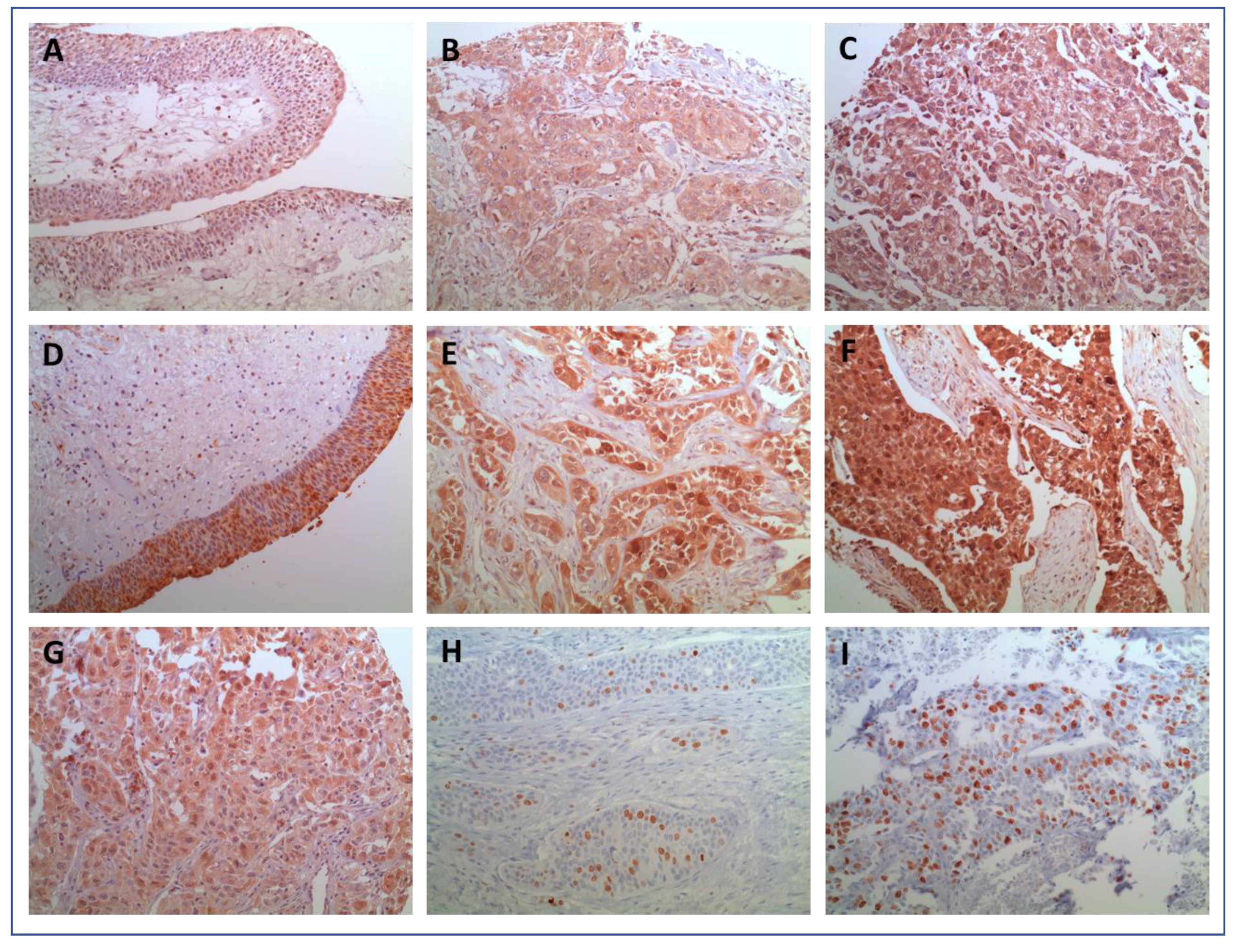
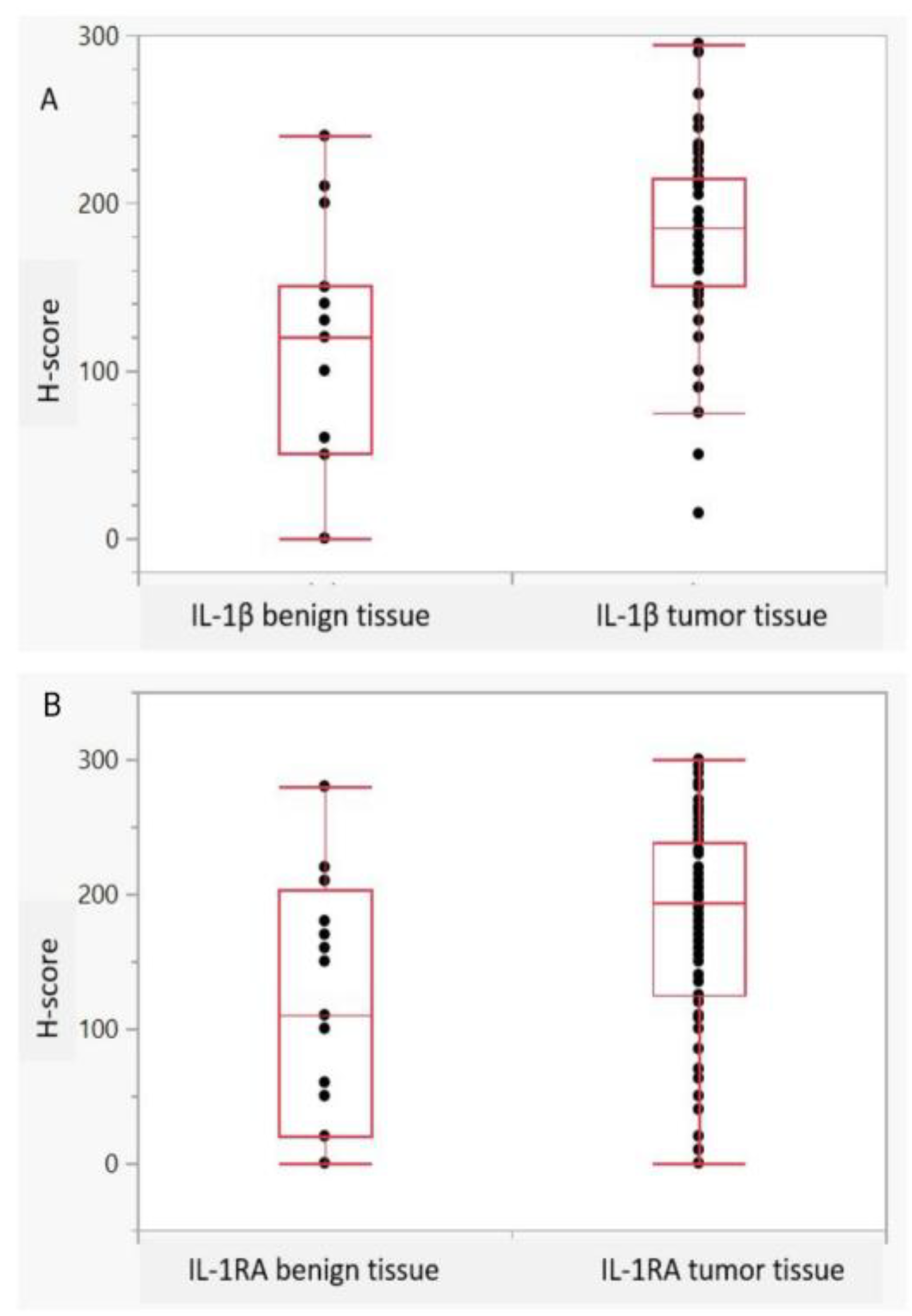
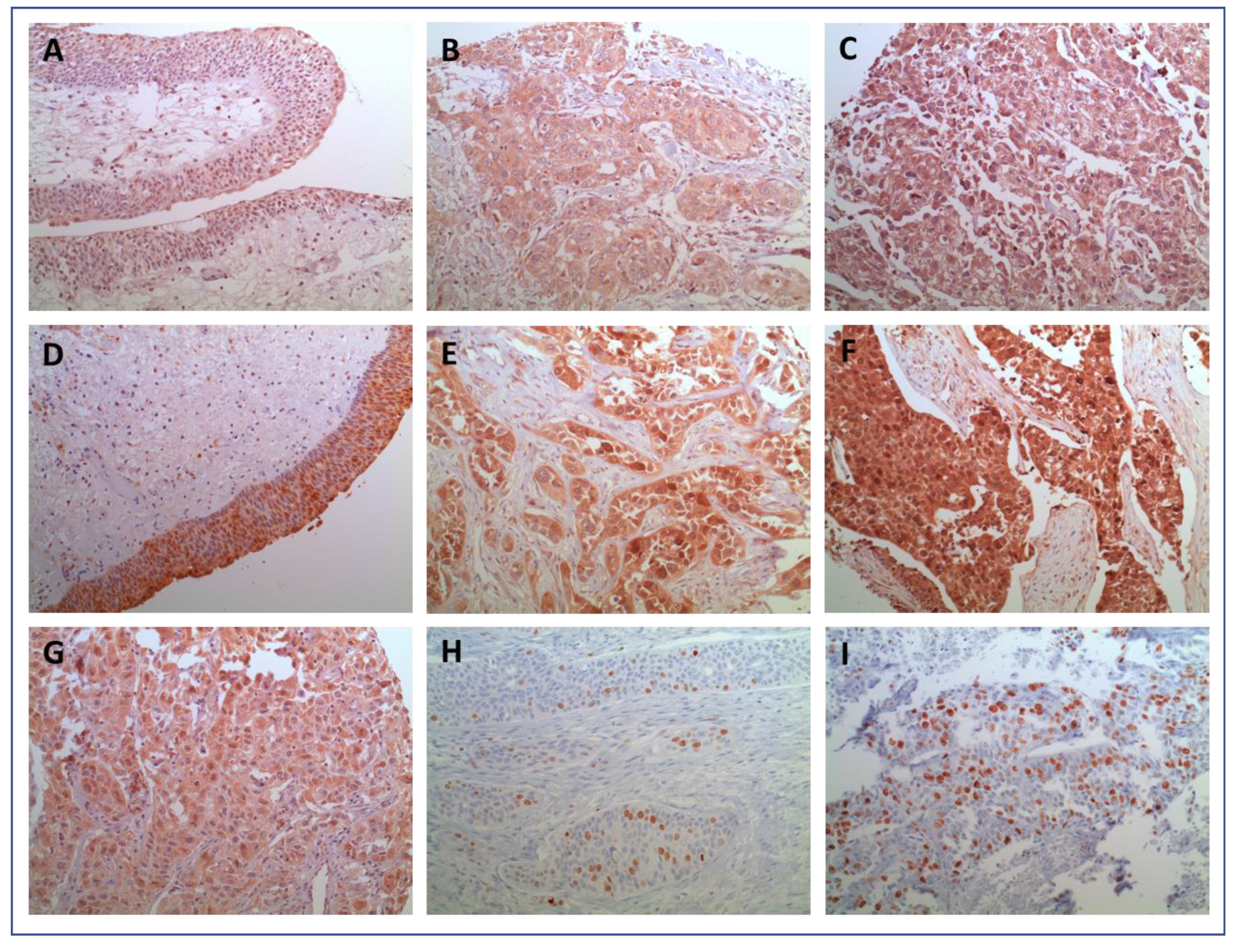
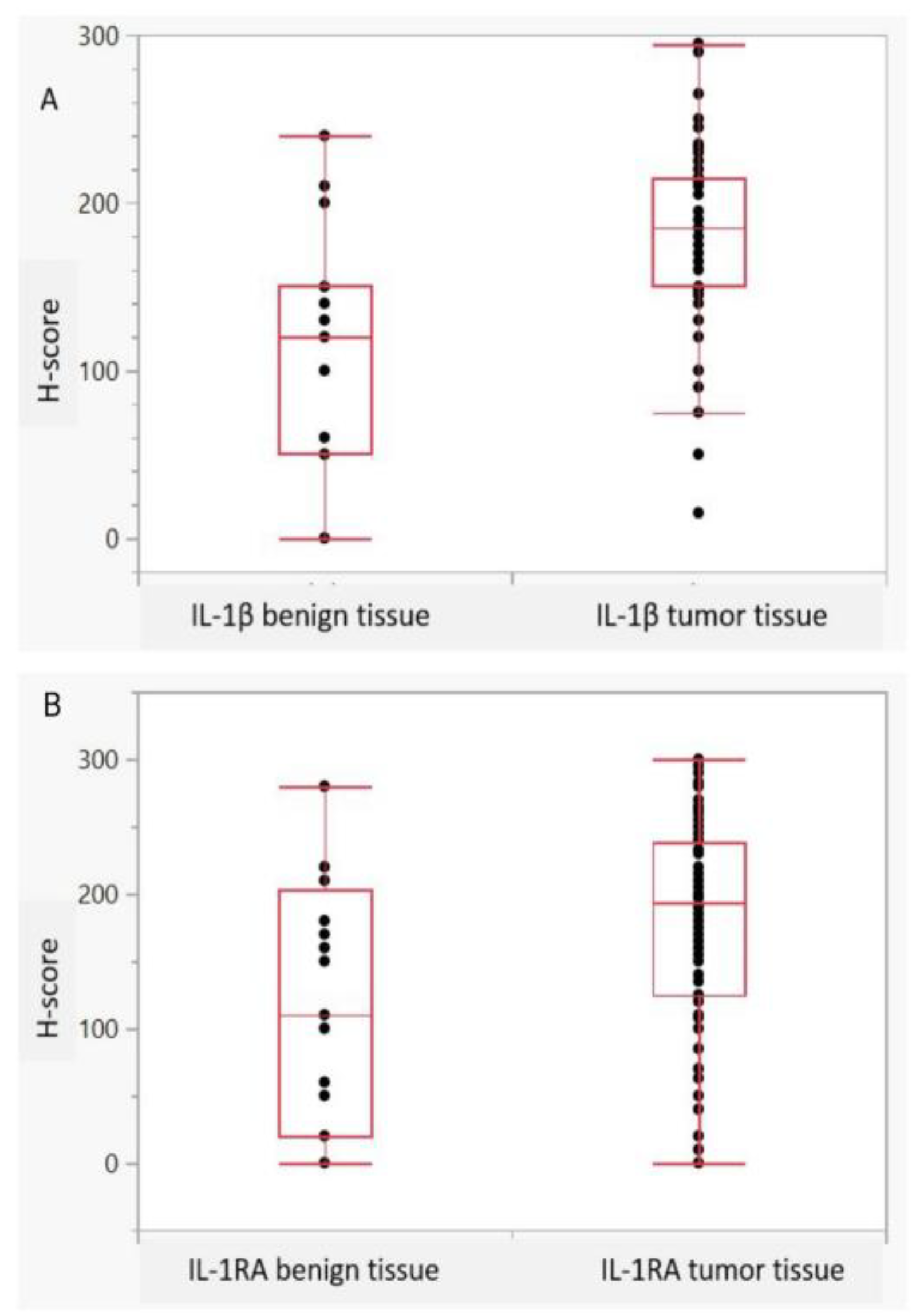
2.2. Expression Characteristics of IL-1β and IL1RA
2.3. Correlation of IL-1 Axis with Histopathologic Parameters
2.4. Combined Scores and Clinical Data
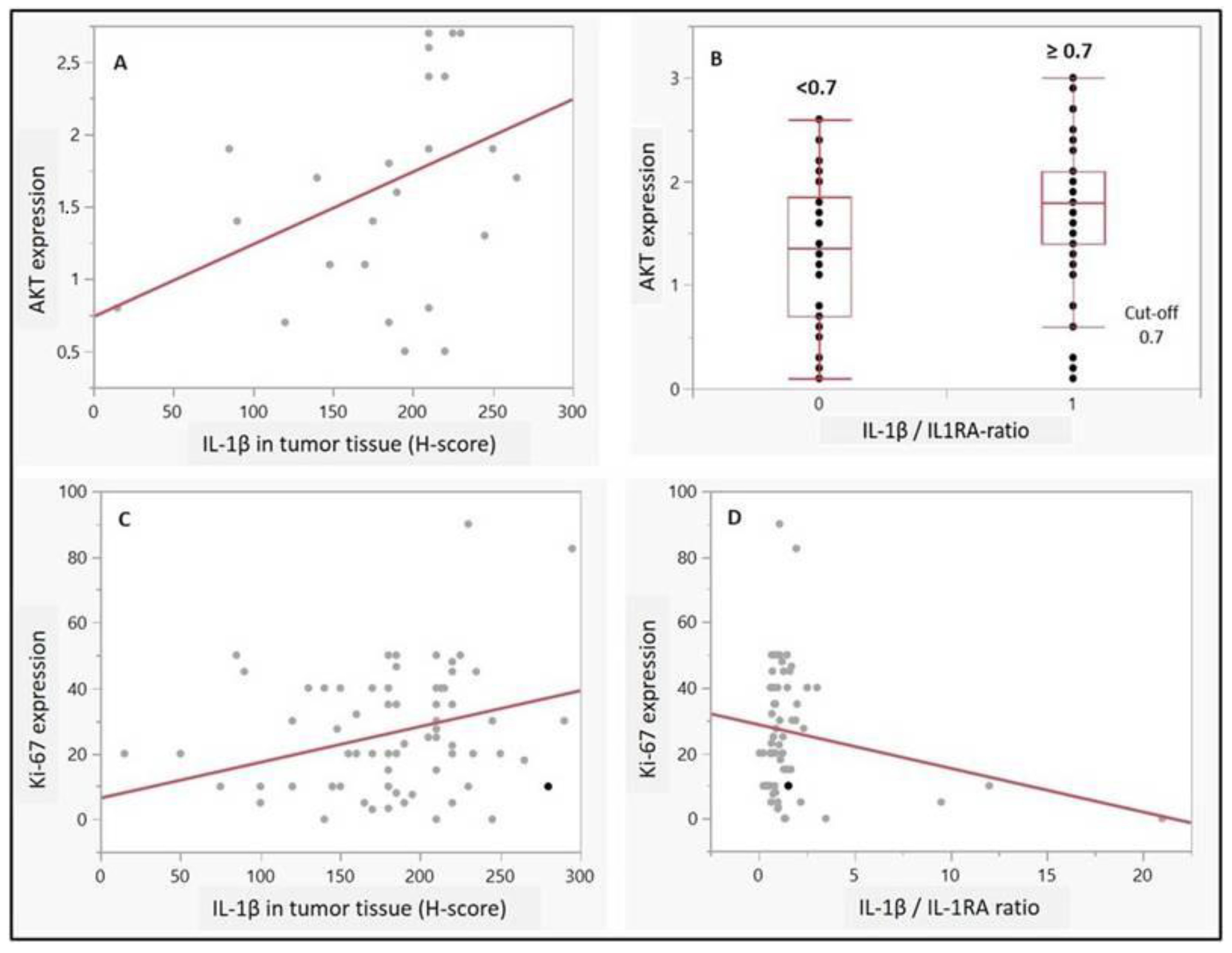
2.5. Correlation of IL-1 Axis with Ki-67 and AKT Expression
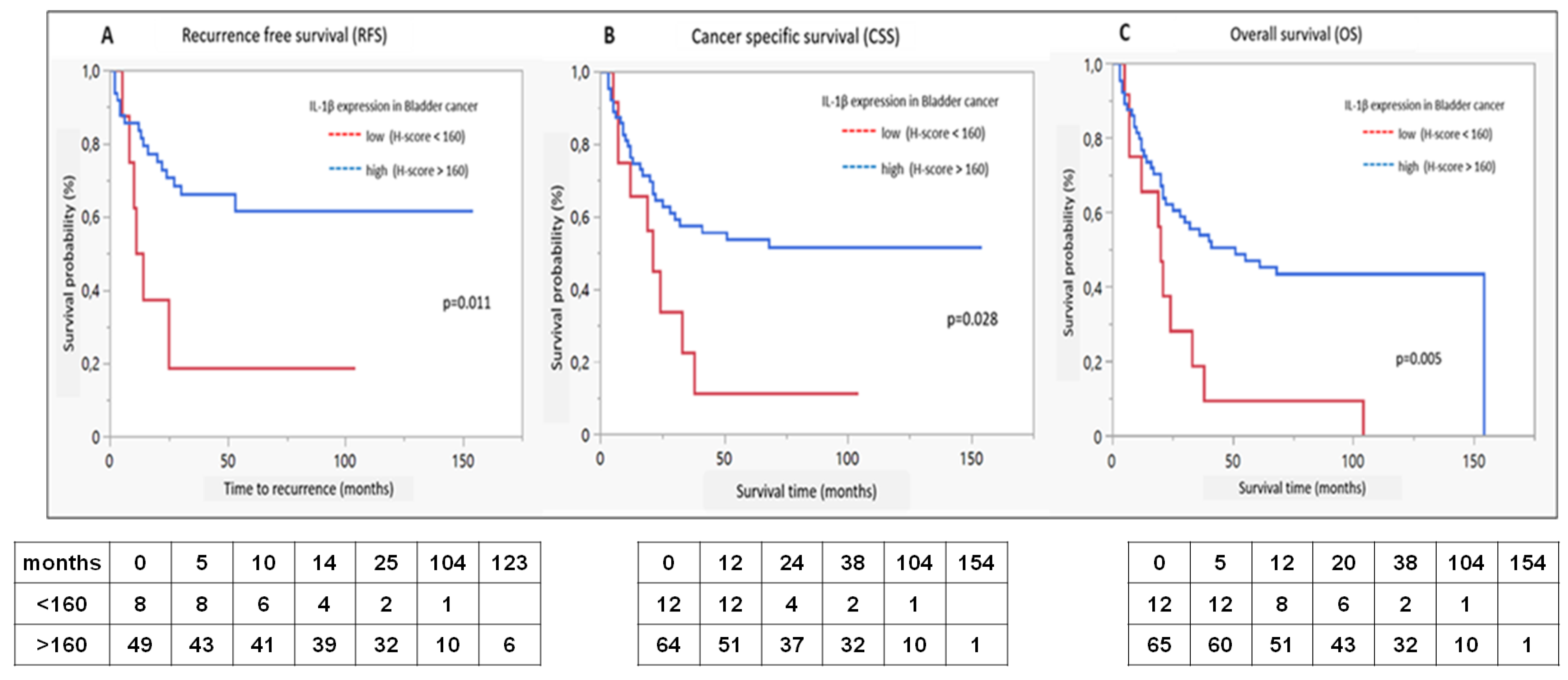
2.6. Survival Analysis
2.7. Uni- and Multivariate Cox Proportional Hazard Analysis
3. Discussion
4. Materials and Methods
4.1. Patient Cohorts
4.2. Tissue Microarray (TMA) and Immunohistochemical (IHC) Staining
4.3. Immunohistochemical Protocol
4.4. Patient Follow-up
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, J.Z.; Zhu, W.; Han, J.; Yang, X.; Zhou, R.; Lu, H.C.; Yu, H.; Yuan, W.B.; Li, P.C.; Tao, J.; et al. The role of the HIF-1α/ALYREF/PKM2 axis in glycolysis and tumorigenesis of bladder cancer. Cancer Commun. 2021, 41, 560–575. [Google Scholar] [CrossRef]
- Huang, W.; Zhang, C.; Li, Y.; Zha, H.; Zhou, X.; Fu, B.; Guo, J.; Wang, G. IGF2BP3 facilitates cell proliferation and tumorigenesis via modulation of JAK/STAT signalling pathway in human bladder cancer. J. Cell. Mol. Med. 2020, 24, 13949–13960. [Google Scholar] [CrossRef]
- Rausch, S.; Hennenlotter, J.; Teepe, K.; Kuehs, U.; Aufderklamm, S.; Bier, S.; Mischinger, J.; Gakis, G.; Stenzl, A.; Schwentner, C.; et al. Muscle-invasive bladder cancer is characterized by overexpression of thymidine kinase 1. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 426.e21–426.e29. [Google Scholar] [CrossRef]
- Xia, H.; Green, D.R.; Zou, W. Autophagy in tumour immunity and therapy. Nat. Rev. Cancer 2021, 21, 281–297. [Google Scholar] [CrossRef]
- Vetterlein, M.W.; Roschinski, J.; Gild, P.; Marks, P.; Soave, A.; Doh, O.; Isbarn, H.; Höppner, W.; Wagner, W.; Shariat, S.F.; et al. Impact of the Ki-67 labeling index and p53 expression status on disease-free survival in pT1 urothelial carcinoma of the bladder. Transl. Androl. Urol. 2017, 6, 1018–1026. [Google Scholar] [CrossRef]
- Liu, G.H.; Zhong, Q.; Ye, Y.L.; Wang, H.B.; Hu, L.J.; Qin, Z.K.; Zeng, M.S.; Zeng, B.H. Expression of beclin 1 in bladder cancer and its clinical significance. Int. J. Biol. Markers 2013, 28, 56–62. [Google Scholar] [CrossRef]
- Kim, H.; Lee, S.J.; Lee, I.K.; Min, S.C.; Sung, H.H.; Jeong, B.C.; Lee, J.; Park, S.H. Synergistic Effects of Combination Therapy with AKT and mTOR Inhibitors on Bladder Cancer Cells. Int. J. Mol. Sci. 2020, 21, 2825. [Google Scholar] [CrossRef]
- Matsumoto, H.; Munemori, M.; Shimizu, K.; Fujii, N.; Kobayashi, K.; Inoue, R.; Yamamoto, Y.; Nagao, K.; Matsuyama, H. Risk stratification using Bmi-1 and Snail expression is a useful prognostic tool for patients with upper tract urothelial carcinoma. nt. J. Urol. 2016, 23, 1030–1037. [Google Scholar]
- Wang, F.; Liu, J.; Chen, X.; Zheng, X.; Qu, N.; Zhang, B.; Xia, C. IL-1β receptor antagonist (IL-1Ra) combined with autophagy inducer (TAT-Beclin1) is an effective alternative for attenuating extracellular matrix degradation in rat and human osteoarthritis chondrocytes. Arthritis Res. Ther. 2019, 21, 171. [Google Scholar] [CrossRef]
- De Luca, A.; Smeekens, S.; Casagrande, A.; Iannitti, R.; Conway, K.L.; Gresnigt, M.S.; Begun, J.; Plantinga, T.S.; Joosten, L.A.; van der Meer, J.W.; et al. IL-1 receptor blockade restores autophagy and reduces inflammation in chronic granulomatous disease in mice and in humans. Proc. Natl. Acad. Sci. USA 2014, 111, 3526–3531. [Google Scholar] [CrossRef]
- Crişan, T.O.; Plantinga, T.S.; van de Veerdonk, F.L.; Farcaş, M.F.; Stoffels, M.; Kullberg, B.-J.; van der Meer, J.W.M.; Joosten, L.A.; Netea, M.G. Inflammasome-independent modulation of cytokine response by autophagy in human cells. PLoS ONE 2011, 6, e18666. [Google Scholar] [CrossRef]
- Semilia, M.; Hennenlotter, J.; Pavone, C.; Bischoff, T.; Kühs, U.; Gakis, G.; Bedke, J.; Stenzl, A.; Schwentner, C.; Todenhöfer, T. Expression patterns and prognostic role of transketolase-like 1 in muscle-invasive bladder cancer. World J. Urol. 2015, 33, 1403–1409. [Google Scholar] [CrossRef]
- Wilson, F.; Joseph, N.; Choudhury, A. Biomarkers in muscle invasive bladder cancer. Adv. Clin. Chem. 2022, 107, 265–297. [Google Scholar] [PubMed]
- Audenet, F.; Attalla, K.; Sfakianos, J.P. The evolution of bladder cancer genomics: What have we learned and how can we use it? Urol. Oncol. 2018, 36, 313–320. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, Z.; Deng, B.; Wu, D.; Quan, Y.; Min, Z. Interleukin 1β/1RA axis in colorectal cancer regulates tumor invasion, proliferation and apoptosis via autophagy. Oncol. Rep. 2020, 43, 908–918. [Google Scholar] [CrossRef]
- Rébé, C.; Ghiringhelli, F. Interleukin-1β and Cancer. Cancers 2020, 12, 1791. [Google Scholar] [CrossRef]
- Schneider, L.; Liu, J.; Zhang, C.; Azoitei, A.; Meessen, S.; Zheng, X.; Cremer, C.; Gorzelanny, C.; Kempe-Gonzales, S.; Brunner, C.; et al. The Role of Interleukin-1-Receptor-Antagonist in Bladder Cancer Cell Migration and Invasion. Int. J. Mol. Sci. 2021, 22, 5875. [Google Scholar] [CrossRef]
- Waugh, J.; Perry, C.M. Anakinra: A review of its use in the management of rheumatoid arthritis. BioDrugs 2005, 19, 189–202. [Google Scholar] [CrossRef]
- Lust, J.A.; Lacy, M.Q.; Zeldenrust, S.R.; Dispenzieri, A.; Gertz, M.A.; Witzig, T.E.; Kumar, S.; Hayman, S.R.; Rusell, S.R.; Buadi, F.K.; et al. Induction of a chronic disease state in patients with smoldering or indolent multiple myeloma by targeting interleukin 1{beta}-induced interleukin 6 production and the myeloma proliferative component. Mayo Clin. Proc. 2009, 84, 114–122. [Google Scholar] [CrossRef]
- Minoli, M.; Kiener, M.; Thalmann, G.N.; Kruithof-de Julio, M.; Seiler, R. Evolution of Urothelial Bladder Cancer in the Context of Molecular Classifications. Int. J. Mol. Sci. 2020, 21, 5670. [Google Scholar] [CrossRef]
- Yao, S.J.; Ma, H.S.; Liu, G.M.; Gao, Y.; Wang, W. Increased IL-1α expression is correlated with bladder cancer malignant progression. Arch. Med. Sci. 2020, 19, 160–170. [Google Scholar] [PubMed]
- Iula, L.; Keitelman, I.A.; Sabbione, F.; Fuentes, F.; Guzman, M.; Galletti, J.G.; Gerber, P.P.; Ostrowski, M.; Geffner, J.R.; Jancic, C.C.; et al. Autophagy Mediates Interleukin-1β Secretion in Human Neutrophils. Front. Immunol. 2018, 9, 269. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Zhu, Y.; Xu, X.; Zhu, Y.; Song, Y.; Pang, L.; Chen, Z. The anti-tumor effects of dual PI3K/mTOR inhibitor BEZ235 and histone deacetylase inhibitor Trichostatin A on inducing autophagy in esophageal squamous cell carcinoma. J. Cancer. 2018, 9, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Bertz, S.; Otto, W.; Denzinger, S.; Wieland, W.F.; Burger, M.; Stöhr, R.; Link, S.; Hofstädter, F.; Hartmann, A. Combination of CK20 and Ki-67 immunostaining analysis predicts recurrence, progression, and cancer-specific survival in pT1 urothelial bladder cancer. Eur. Urol. 2014, 65, 218–226. [Google Scholar] [CrossRef]
- Spirito, L.; Maturi, R.; Credendino, S.C.; Manfredi, C.; Arcaniolo, D.; De Martino, M.; Esposito, F.; Napolitano, L.; Di Bello, F.; Fusco, A.; et al. Differential Expression of LncRNA in Bladder Cancer Development. Diagnostics 2023, 13, 1745. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part B: Prostate and Bladder Tumours. Eur Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef] [PubMed]
- John, A.; Günes, C.; Bolenz, C.; Vidal-Y-Sy, S.; Bauer, A.T.; Schneider, S.W.; Gorzelanny, C. Bladder cancer-derived interleukin-1 converts the vascular endothelium into a pro-inflammatory and pro-coagulatory surface. BMC Cancer 2020, 2, 1178. [Google Scholar] [CrossRef]
- Andersen, N.L.; Brügmann, A.; Lelkaitis, G.; Nielsen, S.; Lippert, M.F.; Vyberg, M. Virtual Double Staining: A Digital Approach to Immunohistochemical Quantification of Estrogen Receptor Protein in Breast Carcinoma Specimens. Appl. Immunohistochem. Mol. Morphol. 2018, 26, 620–626. [Google Scholar] [CrossRef]
- Le Page, C.; Koumakpayi, I.H.; Alam-Fahmy, M.; Mes-Masson, A.-M.; Saad, F. Expression and localisation of Akt-1, Akt-2 and Akt-3 correlate with clinical outcome of prostate cancer patients. Br. J. Cancer 2006, 94, 1906–1912. [Google Scholar] [CrossRef]
- Aman, N.A.; Doukoure, B.; Koffi, K.D.; Koui, B.S.; Traore, Z.C.; Kouyate, M.; Toure, I.; Effi, A.B. Immunohistochemical Evaluation of Ki-67 and Comparison with Clinicopathologic Factors in Breast Carcinomas. Asian Pac. J. Cancer Prev. 2019, 20, 73–79. [Google Scholar] [CrossRef]
- Liu, Y.; Tang, Y.; Wie, Y.W. What is the difference between overall survival, recurrence-free survival and time-to-recurrence? Br. J. Surg. 2020, 107, e634. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Group I (n = 102) | Group II (n = 92) | p | ||
|---|---|---|---|---|---|
| N | % | n | % | ||
| Gender | 0.56 | ||||
| -Female | 24 | 23.53 | 25 | 27.18 | |
| -Male | 78 | 76.47 | 67 | 72.82 | |
| Age | Median 69 | Range (59–74) | Median 65 | Range (55–72) | 0.19 |
| Pathological stage | 0.55 | ||||
| -T1 | 0 | 0.00 | 9 | 9.78 | |
| -T2 | 31 | 30.39 | 21 | 22.82 | |
| -T3 | 47 | 46.08 | 42 | 45.66 | |
| -T4 | 24 | 23.53 | 18 | 19.57 | |
| -Only CIS | 0 | 0.00 | 2 | 2.17 | |
| Lymph node status | 0.50 | ||||
| -N0 | 58 | 56.86 | 57 | 61.95 | |
| -N+ | 44 | 43.14 | 35 | 38.05 | |
| Distant metastasis | 0.59 | ||||
| -M0 | 89 | 87.23 | 82 | 89.13 | |
| -M1 | 9 | 8.83 | 10 | 10.87 | |
| -Mx | 4 | 3.93 | 0 | 0.00 | |
| Pathological grade | 0.94 | ||||
| -G1 | 0 | 0.00 | 1 | 1.08 | |
| -G2 | 24 | 23.53 | 20 | 21.74 | |
| -G3 | 78 | 76.47 | 71 | 77.18 | |
| Resection margin status | 0.74 | ||||
| -R0 | 84 | 82.35 | 74 | 80.43 | |
| -R1 | 15 | 14.70 | 14 | 15.22 | |
| -R2 | 3 | 2.95 | 2 | 2.18 | |
| -Rx | 0 | 0.00 | 2 | 2.17 | |
| Carcinoma in situ (CIS) | 0.57 | ||||
| -No | 68 | 66.66 | 61 | 66.31 | |
| -Yes | 29 | 28.44 | 31 | 33.69 | |
| -CISx | 5 | 4.90 | 0 | 0.00 | |
| Histopathology Variables | IL-1β Expression (H-Score) | IL-1RA Expression (H-Score) | IL1-β/IL-1RA Ratio (Cut-Off 0.7) |
|---|---|---|---|
| Tumor grade | Medians | ||
| G2 | 188 | 250 *** | 0.7 |
| G3 | 193 * | 185 | 1.1 *** |
| Tumor stadium pT | |||
| T2 | 205 | 178 | 1.0 |
| T3 | 190 | 200 | 1.0 |
| T4 | 190 | 200 | 0.9 |
| Lymphatic invasion | |||
| No | 180 | 194 | 1.0 |
| yes | 210 * | 200 | 1.0 |
| Vascular invasion | |||
| no | 183 | 190 | 1.0 |
| yes | 210 * | 203 | 1.0 |
| Nodal invasion | |||
| N0 | 185 | 194 | 1.0 |
| N1 | 185 | 200 | 0.9 |
| N2 | 210 | 205 | 1.1 |
| N3 | 198 | 175 | 1.0 |
| Metastatic disease | |||
| M0 | 185 | 194 | 1.0 |
| M1 | 210 | 200 | 1.0 |
| Variable | Ki-67+ and IL-1β+ | Ki-67+ (15%) or IL-1β+ | Ki-67+ and IL1RA+ | Ki-67+ (15%) or IL-1RA+ |
|---|---|---|---|---|
| Pathological stage >T2 vs. T2 | 0.61 | 0.67 | 0.81 | 0.06 |
| Nodal status N+ vs. N0 | 0.97 | 0.25 | 0.39 | 0.54 |
| Metastasis status M+ vs. M0 | 0.28 | 0.40 | 0.46 | 0.56 |
| Grade ≥G3 vs. <G3 | 1.00 | 0.02 | 0.52 | 0.57 |
| Lymphatic invasion L+ vs. L0 | 0.93 | 0.51 | 0.30 | 0.70 |
| Vascular invasion V+ vs. V0 | 0.02 | 0.92 | 0.33 | 0.90 |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Recurrence (RFS) | p | HR | 95% CI | p | HR | 95% CI |
| Pathological stage >T2 vs. T2 | 0.0099 | 3.25 | 1.33–7.95 | 0.1339 | 2.14 | 0.79–5.80 |
| Nodal status N+ vs. N0 | 0.0879 | 1.88 | 0.91–3.88 | - | ||
| Metastasis status M+ vs. M0 | - | - | ||||
| Grade ≥G3 vs. <G3 | 0.0531 | 1.30 | 0.60–2.83 | - | ||
| IL-1β Low vs. high tumor expression (cut-off 160) | 0.0172 | 3.16 | 1.23–8.16 | 0.0265 | 2.97 | 1.14–7.77 |
| Age, year | 0.2397 | 1.02 | 0.99–1.06 | - | ||
| Variable | Univariate analysis | Multivariate analysis | ||||
| CSS | p | HR | 95% CI | p | HR | 95% CI |
| Pathological stage >T2 vs. T2 | 0.0107 | 2.53 | 1.24–5.17 | 0.3407 | 1.51 | 0.65–3.49 |
| Nodal status N+ vs. N0 | 0.0309 | 1.96 | 1.06–3.62 | 0.3170 | 1.48 | 0.69–3.17 |
| Metastasis status M+ vs. M0 | 0.0015 | 3.56 | 1.63–7.79 | 0.0504 | 2.58 | 1.00–6.65 |
| Grade ≥G3 vs. <G3 | 0.0069 | 3.62 | 1.42–9.22 | 0.1247 | 2.38 | 0.79–7.18 |
| IL-1β Low vs. high tumor expression (cut-off 160) | 0.0343 | 2.27 | 1.06–4.84 | 0.0460 | 2.35 | 1.02–5.42 |
| Age, year | 0.0047 | 1.05 | 1.01–1.08 | 0.3421 | 1.02 | 0.98–1.06 |
| Variable | Univariate analysis | Multivariate analysis | ||||
| OS | p | HR | 95% CI | p | HR | 95% CI |
| Pathological stage >T2 vs. T2 | 0.0020 | 2.79 | 1.45–5.33 | 0.1240 | 1.85 | 0.85–4.03 |
| Nodal status N+ vs. N0 | 0.0258 | 1.85 | 1.08–3.17 | 0.1909 | 1.60 | 0.79–3.24 |
| Metastasis status M+ vs. M0 | 0.0036 | 3.13 | 1.45–6.73 | 0.1148 | 2.12 | 0.83–5.37 |
| Grade ≥G3 vs. < G3 | 0.0173 | 2.31 | 1.16–4.60 | 0.1611 | 1.94 | 0.77–4.88 |
| IL-1β Low vs. high tumor expression (cut-off 160) | 0.0082 | 2.54 | 1.27–5.06 | 0.0249 | 2.40 | 1.12–5.18 |
| Age, year | 0.0031 | 1.05 | 1.02–1.08 | 0.1274 | 1.03 | 0.99–1.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vukovic, M.; Chamlati, J.M.; Hennenlotter, J.; Todenhöfer, T.; Lütfrenk, T.; Jersinovic, S.; Tsaur, I.; Stenzl, A.; Rausch, S. Interleukin-1β/Interleukin (IL)-1-Receptor-Antagonist (IL1-RA) Axis in Invasive Bladder Cancer—An Exploratory Analysis of Clinical and Tumor Biological Significance. Int. J. Mol. Sci. 2024, 25, 2447. https://doi.org/10.3390/ijms25042447
Vukovic M, Chamlati JM, Hennenlotter J, Todenhöfer T, Lütfrenk T, Jersinovic S, Tsaur I, Stenzl A, Rausch S. Interleukin-1β/Interleukin (IL)-1-Receptor-Antagonist (IL1-RA) Axis in Invasive Bladder Cancer—An Exploratory Analysis of Clinical and Tumor Biological Significance. International Journal of Molecular Sciences. 2024; 25(4):2447. https://doi.org/10.3390/ijms25042447
Chicago/Turabian StyleVukovic, Marko, Jorge M. Chamlati, Jörg Hennenlotter, Tilman Todenhöfer, Thomas Lütfrenk, Sebastian Jersinovic, Igor Tsaur, Arnulf Stenzl, and Steffen Rausch. 2024. "Interleukin-1β/Interleukin (IL)-1-Receptor-Antagonist (IL1-RA) Axis in Invasive Bladder Cancer—An Exploratory Analysis of Clinical and Tumor Biological Significance" International Journal of Molecular Sciences 25, no. 4: 2447. https://doi.org/10.3390/ijms25042447
APA StyleVukovic, M., Chamlati, J. M., Hennenlotter, J., Todenhöfer, T., Lütfrenk, T., Jersinovic, S., Tsaur, I., Stenzl, A., & Rausch, S. (2024). Interleukin-1β/Interleukin (IL)-1-Receptor-Antagonist (IL1-RA) Axis in Invasive Bladder Cancer—An Exploratory Analysis of Clinical and Tumor Biological Significance. International Journal of Molecular Sciences, 25(4), 2447. https://doi.org/10.3390/ijms25042447