
The GDF15 3′ UTR Polymorphism rs1054564 Is Associated with Diabetes and Subclinical Atherosclerosis
 , ,
, ,  , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Results
2.1. Genotype and Allele Frequencies of GDF15 SNPs in Both Healthy Volunteers and Patients with Lipid Alterations and Related Disorders
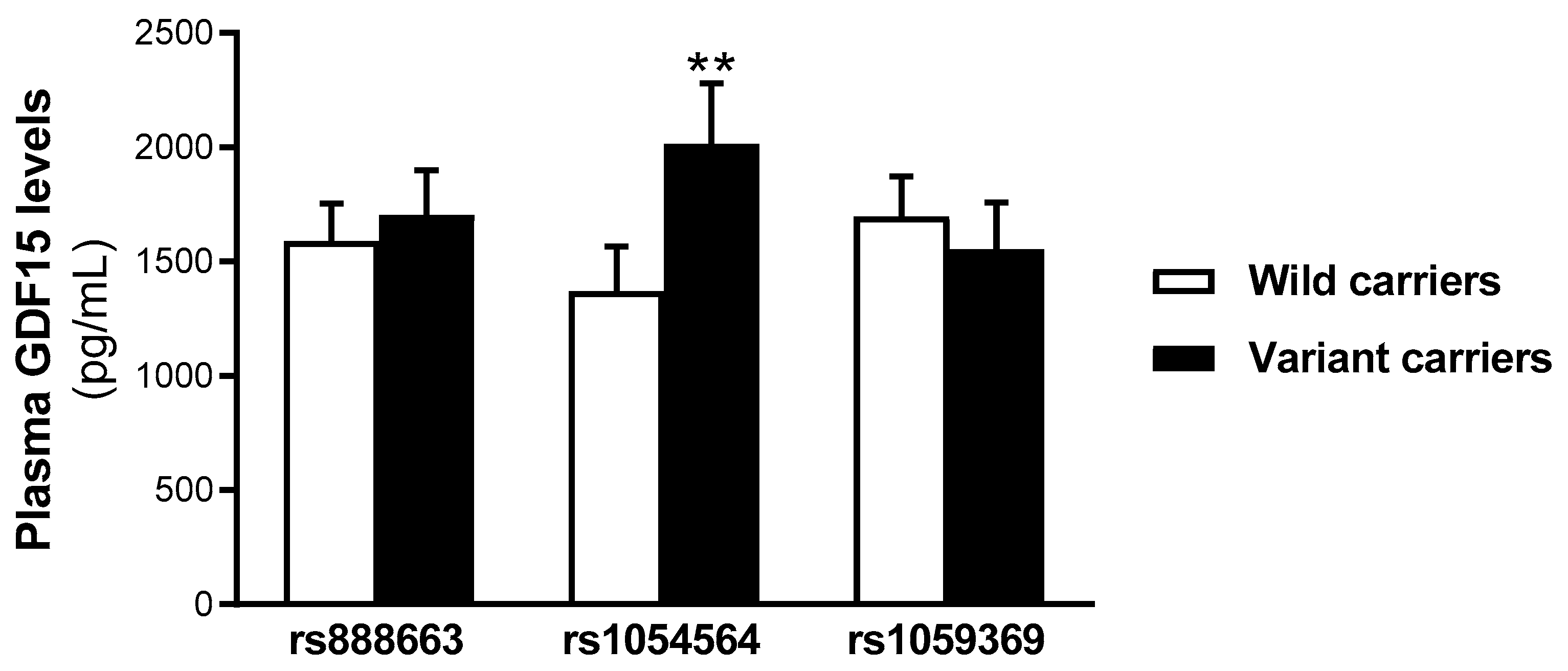
2.2. Serum GDF15 Levels Are Increased in rs1054564 Variant Carriers
2.3. Characteristics of Study Populations According to rs1054564 Genotype
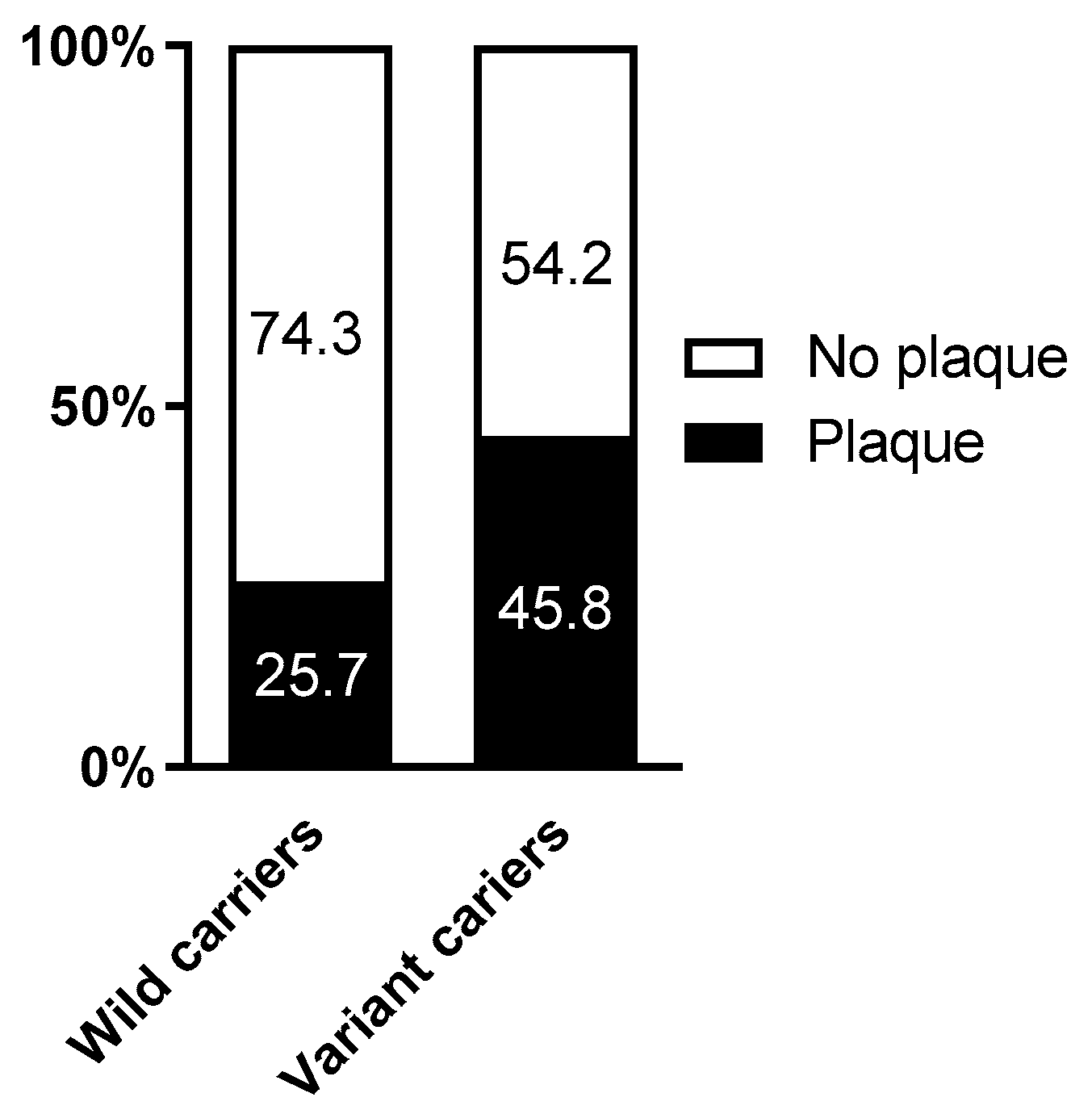
2.4. Association of the rs1054564 Variants with the Carotid Plaque Burden
3. Discussion
4. Materials and Methods
4.1. Study Subjects
4.2. Clinical and Standard Biochemical Determinations
4.3. SNP Selection and Genotyping
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bootcov, M.R.; Bauskin, A.R.; Valenzuela, S.M.; Moore, A.G.; Bansal, M.; He, X.Y.; Zhang, H.P.; Donnellan, M.; Mahler, S.; Pryor, K.; et al. MIC-1, a novel macrophage inhibitory cytokine, is a divergent member of the TGF-beta superfamily. Proc. Natl. Acad. Sci. USA 1997, 94, 11514–11519. [Google Scholar] [CrossRef]
- Breit, S.N.; Johnen, H.; Cook, A.D.; Tsai, V.W.; Mohammad, M.G.; Kuffner, T.; Zhang, H.P.; Marquis, C.P.; Jiang, L.; Lockwood, G.; et al. The TGF-beta superfamily cytokine, MIC-1/GDF15: A pleotrophic cytokine with roles in inflammation, cancer and metabolism. Growth Factors 2011, 29, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Tsai, V.W.; Lin, S.; Brown, D.A.; Salis, A.; Breit, S.N. Anorexia-cachexia and obesity treatment may be two sides of the same coin: Role of the TGF-b superfamily cytokine MIC-1/GDF15. Int. J. Obes. 2016, 40, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Assadi, A.; Zahabi, A.; Hart, R.A. GDF15, an update of the physiological and pathological roles it plays: A review. Pflug. Arch. Eur. J. Physiol. 2020, 472, 1535–1546. [Google Scholar] [CrossRef] [PubMed]
- McGrath, R.T.; Glastras, S.J.; Scott, E.S.; Hocking, S.L.; Fulcher, G.R. Outcomes for Women with Gestational Diabetes Treated with Metformin: A Retrospective, Case-Control Study. J. Clin. Med. 2018, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.A.; Breit, S.N.; Buring, J.; Fairlie, W.D.; Bauskin, A.R.; Liu, T.; Ridker, P.M. Concentration in plasma of macrophage inhibitory cytokine-1 and risk of cardiovascular events in women: A nested case-control study. Lancet 2002, 359, 2159–2163. [Google Scholar] [CrossRef]
- De Rosa, S.; Arcidiacono, B.; Chiefari, E.; Brunetti, A.; Indolfi, C.; Foti, D.P. Type 2 Diabetes Mellitus and Cardiovascular Disease: Genetic and Epigenetic Links. Front. Endocrinol. 2018, 9, 2. [Google Scholar] [CrossRef]
- Piccirillo, F.; Mastroberardino, S.; Nusca, A.; Frau, L.; Guarino, L.; Napoli, N.; Ussia, G.P.; Grigioni, F. Novel Antidiabetic Agents and Their Effects on Lipid Profile: A Single Shot for Several Cardiovascular Targets. Int. J. Mol. Sci. 2023, 24, 10164. [Google Scholar] [CrossRef]
- Stern, M.P. Diabetes and cardiovascular disease. The “common soil” hypothesis. Diabetes 1995, 44, 369–374. [Google Scholar] [CrossRef]
- Fernandes Silva, L.; Vangipurapu, J.; Laakso, M. The “Common Soil Hypothesis” Revisited-Risk Factors for Type 2 Diabetes and Cardiovascular Disease. Metabolites 2021, 11, 691. [Google Scholar] [CrossRef]
- Ferrannini, G.; Manca, M.L.; Magnoni, M.; Andreotti, F.; Andreini, D.; Latini, R.; Maseri, A.; Maggioni, A.P.; Ostroff, R.M.; Williams, S.A.; et al. Coronary Artery Disease and Type 2 Diabetes: A Proteomic Study. Diabetes Care 2020, 43, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Kempf, T.; Guba-Quint, A.; Torgerson, J.; Magnone, M.C.; Haefliger, C.; Bobadilla, M.; Wollert, K.C. Growth differentiation factor 15 predicts future insulin resistance and impaired glucose control in obese nondiabetic individuals: Results from the XENDOS trial. Eur. J. Endocrinol. 2012, 167, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Frimodt-Moller, M.; von Scholten, B.J.; Reinhard, H.; Jacobsen, P.K.; Hansen, T.W.; Persson, F.I.; Parving, H.H.; Rossing, P. Growth differentiation factor-15 and fibroblast growth factor-23 are associated with mortality in type 2 diabetes—An observational follow-up study. PLoS ONE 2018, 13, e0196634. [Google Scholar] [CrossRef] [PubMed]
- Daniels, L.B.; Clopton, P.; Laughlin, G.A.; Maisel, A.S.; Barrett-Connor, E. Growth-differentiation factor-15 is a robust, independent predictor of 11-year mortality risk in community-dwelling older adults: The Rancho Bernardo Study. Circulation 2011, 123, 2101–2110. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Wallentin, L.; Kempf, T.; Tapken, H.; Quint, A.; Lindahl, B.; Olofsson, S.; Venge, P.; Larsson, A.; Hulthe, J.; et al. Growth-differentiation factor-15 is an independent marker of cardiovascular dysfunction and disease in the elderly: Results from the Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) Study. Eur. Heart J. 2009, 30, 2346–2353. [Google Scholar] [CrossRef]
- Rohatgi, A.; Patel, P.; Das, S.R.; Ayers, C.R.; Khera, A.; Martinez-Rumayor, A.; Berry, J.D.; McGuire, D.K.; de Lemos, J.A. Association of growth differentiation factor-15 with coronary atherosclerosis and mortality in a young, multiethnic population: Observations from the Dallas Heart Study. Clin. Chem. 2012, 58, 172–182. [Google Scholar] [CrossRef]
- Wiklund, F.E.; Bennet, A.M.; Magnusson, P.K.; Eriksson, U.K.; Lindmark, F.; Wu, L.; Yaghoutyfam, N.; Marquis, C.P.; Stattin, P.; Pedersen, N.L.; et al. Macrophage inhibitory cytokine-1 (MIC-1/GDF15): A new marker of all-cause mortality. Aging Cell 2010, 9, 1057–1064. [Google Scholar] [CrossRef]
- Ho, J.E.; Mahajan, A.; Chen, M.H.; Larson, M.G.; McCabe, E.L.; Ghorbani, A.; Cheng, S.; Johnson, A.D.; Lindgren, C.M.; Kempf, T.; et al. Clinical and genetic correlates of growth differentiation factor 15 in the community. Clin. Chem. 2012, 58, 1582–1591. [Google Scholar] [CrossRef]
- Teng, M.S.; Hsu, L.A.; Juan, S.H.; Lin, W.C.; Lee, M.C.; Su, C.W.; Wu, S.; Ko, Y.L. A GDF15 3′ UTR variant, rs1054564, results in allele-specific translational repression of GDF15 by hsa-miR-1233-3p. PLoS ONE 2017, 12, e0183187. [Google Scholar] [CrossRef]
- Jiang, J.; Thalamuthu, A.; Ho, J.E.; Mahajan, A.; Ek, W.E.; Brown, D.A.; Breit, S.N.; Wang, T.J.; Gyllensten, U.; Chen, M.H.; et al. A Meta-Analysis of Genome-Wide Association Studies of Growth Differentiation Factor-15 Concentration in Blood. Front. Genet. 2018, 9, 97. [Google Scholar] [CrossRef]
- Hsu, L.A.; Wu, S.; Juang, J.J.; Chiang, F.T.; Teng, M.S.; Lin, J.F.; Huang, H.L.; Ko, Y.L. Growth Differentiation Factor 15 May Predict Mortality of Peripheral and Coronary Artery Diseases and Correlate with Their Risk Factors. Mediat. Inflamm. 2017, 2017, 9398401. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.A.; Lindmark, F.; Stattin, P.; Balter, K.; Adami, H.O.; Zheng, S.L.; Xu, J.; Isaacs, W.B.; Gronberg, H.; Breit, S.N.; et al. Macrophage inhibitory cytokine 1: A new prognostic marker in prostate cancer. Clin. Cancer Res. 2009, 15, 6658–6664. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Qin, L.; Liang, Y.; Xu, M.; Zhang, J.; Mo, X.; Tang, X.; Lu, Y.; Wang, X.; Cao, J.; et al. Correlations between growth differentiation factor 15 (GDF-15) serum levels and gene polymorphism with type 2 diabetes mellitus. Heliyon 2024, 10, e33044. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Vedia, J.; Llop, D.; Rodriguez-Calvo, R.; Plana, N.; Amigo, N.; Rosales, R.; Esteban, Y.; Masana, L.; Ibarretxe, D.; Girona, J. Lipidomics of triglyceride-rich lipoproteins derived from hyperlipidemic patients on inflammation. Eur. J. Clin. Investig. 2024, 54, e14132. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Calvo, R.; Moreno-Vedia, J.; Girona, J.; Ibarretxe, D.; Martinez-Micaelo, N.; Merino, J.; Plana, N.; Masana, L. Relationship Between Fatty Acid Binding Protein 4 and Liver Fat in Individuals at Increased Cardiometabolic Risk. Front. Physiol. 2021, 12, 781789. [Google Scholar] [CrossRef]
- Girona, J.; Rodriguez-Borjabad, C.; Ibarretxe, D.; Vallve, J.C.; Ferre, R.; Heras, M.; Rodriguez-Calvo, R.; Guaita-Esteruelas, S.; Martinez-Micaelo, N.; Plana, N.; et al. The Circulating GRP78/BiP Is a Marker of Metabolic Diseases and Atherosclerosis: Bringing Endoplasmic Reticulum Stress into the Clinical Scenario. J. Clin. Med. 2019, 8, 1793. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006–2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [PubMed]
- Moreno-Vedia, J.; Rosales, R.; Ozcariz, E.; Llop, D.; Lahuerta, M.; Benavent, M.; Rodriguez-Calvo, R.; Plana, N.; Pedragosa, A.; Masana, L.; et al. Triglyceride-Rich Lipoproteins and Glycoprotein A and B Assessed by 1H-NMR in Metabolic-Associated Fatty Liver Disease. Front. Endocrinol. 2021, 12, 775677. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| SNPs | Healthy Volunteers | Patients | p-Value |
|---|---|---|---|
| rs888663 | |||
| TT | 41 (73.2%) | 69 (71.9%) | 0.859 |
| TG | 12 (21.4%) | 19 (18.8%) | |
| GG | 3 (5.4%) | 8 (8.3%) | |
| rs1054564 | |||
| GG | 44 (78.6%) | 60 (61.9%) | 0.033 |
| GC | 11 (19.6%) | 36 (37.1%) | |
| CC | 1 (1.8%) | 1 (1.0%) | |
| rs1059369 | |||
| TT | 29 (51.8%) | 59 (64.1%) | 0.138 |
| TA | 24 (42.9%) | 31 (33.7%) | |
| AA | 3 (5.4%) | 2 (2.2%) |
| Wild-Type Carriers (N = 104) | Variant Carriers (N = 49) | p-Value | |
|---|---|---|---|
| Clinical data | |||
| Age (years) | 55.2 ± 1.2 | 57.0 ± 1.5 | 0.374 |
| Gender (F) | 52.9% | 51% | 0.829 |
| Hypertension | 32.7% | 42.9% | 0.221 |
| Diabetes | 38.5% | 63.3% | 0.004 |
| Obesity | 32.7% | 42.9% | 0.221 |
| Metabolic syndrome | 53.8% | 67.3% | 0.114 |
| Liver steatosis | 43.7% | 54.2% | 0.230 |
| Anthropometric and analytical data | |||
| Systolic BP (mmHg) | 130.3 ± 2.0 | 130.8 ± 2.8 | 0.887 |
| Diastolic BP (mmHg) | 78.0 (70.0–83.0) | 78.3 (72.5–80.8) | 0.863 |
| Weight (Kg) | 78.0 ± 1.5 | 80.1 ± 2.3 | 0.429 |
| Waist circumference (cm) | 96.8 ± 1.4 | 99.1 ± 2.2 | 0.354 |
| BMI (Kg/m2) | 28.6 ± 0.5 | 29.8 ± 0.8 | 0.175 |
| Glucose (mg/dL) | 102.2 (85.8–133.0) | 119.0 (91.0–153.0) | 0.040 |
| Triglycerides (mmol/L) | 1.4 (0.8–2.5) | 1.6 (0.9–3.1) | 0.390 |
| Total cholesterol (mmol/L) | 5.8 ± 0.1 | 6.1 ± 0.2 | 0.237 |
| LDL (mmol/L) | 3.5 ± 0.1 | 3.7 ± 0.2 | 0.358 |
| HDL (mmol/L) | 1.3 ± 0.0 | 1.3 ± 0.0 | 0.880 |
| AST (U/L) | 22.0 (20.0–26.0) | 22.0 (20.0–30.0) | 0.518 |
| ALT (U/L) | 16.0 (12.0–23.0) | 19.0 (13.0–24.5) | 0.310 |
| GGT (U/L) | 19.5 (14.0–30.8) | 21.0 (14.0–38.5) | 0.442 |
| HsCRP (mg/L) | 1.9 ± 0.1 | 2.1 ± 0.2 | 0.397 |
| Glyc-A (µmol/L) | 835.8 ± 28.9 | 908.2 ± 48.5 | 0.179 |
| Glyc-B (µmol/L) | 348.3 ± 7.4 | 361.8 ± 13.7 | 0.346 |
| FIB-4 | 1.6 ± 0.0 | 1.6 ± 0.1 | 0.728 |
| FLI (%) | 43.1 (17.3–83.7) | 68.9 (24.7–92.7) | 0.136 |
| OR (95% CI) | p | |
|---|---|---|
| Crude | 2.75 (1.37–5.56) | 0.005 |
| Model 1 | 3.13 (1.36–7.19) | 0.007 |
| Model 2 | 4.22 (1.57–11.34) | 0.007 |
| OR (95% CI) | p | |
|---|---|---|
| Crude | 2.44 (1.19–5.03) | 0.015 |
| Model 1 | 2.44 (1.11–5.37) | 0.026 |
| Model 2 | 2.41 (1.08–5.37) | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guardiola, M.; Girona, J.; Barroso, E.; García-Altares, M.; Ibarretxe, D.; Plana, N.; Ribalta, J.; Correig, X.; Vázquez-Carrera, M.; Masana, L.; et al. The GDF15 3′ UTR Polymorphism rs1054564 Is Associated with Diabetes and Subclinical Atherosclerosis. Int. J. Mol. Sci. 2024, 25, 11985. https://doi.org/10.3390/ijms252211985
Guardiola M, Girona J, Barroso E, García-Altares M, Ibarretxe D, Plana N, Ribalta J, Correig X, Vázquez-Carrera M, Masana L, et al. The GDF15 3′ UTR Polymorphism rs1054564 Is Associated with Diabetes and Subclinical Atherosclerosis. International Journal of Molecular Sciences. 2024; 25(22):11985. https://doi.org/10.3390/ijms252211985
Chicago/Turabian StyleGuardiola, Montse, Josefa Girona, Emma Barroso, María García-Altares, Daiana Ibarretxe, Núria Plana, Josep Ribalta, Xavier Correig, Manuel Vázquez-Carrera, Lluís Masana, and et al. 2024. "The GDF15 3′ UTR Polymorphism rs1054564 Is Associated with Diabetes and Subclinical Atherosclerosis" International Journal of Molecular Sciences 25, no. 22: 11985. https://doi.org/10.3390/ijms252211985
APA StyleGuardiola, M., Girona, J., Barroso, E., García-Altares, M., Ibarretxe, D., Plana, N., Ribalta, J., Correig, X., Vázquez-Carrera, M., Masana, L., & Rodríguez-Calvo, R. (2024). The GDF15 3′ UTR Polymorphism rs1054564 Is Associated with Diabetes and Subclinical Atherosclerosis. International Journal of Molecular Sciences, 25(22), 11985. https://doi.org/10.3390/ijms252211985