
The Impact of the Mediterranean Diet and Lifestyle Intervention on Lipoprotein Subclass Profiles among Metabolic Syndrome Patients: Findings of a Randomized Controlled Trial

 , , , ,
, , , ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Results
2.1. Effect of MedDiet and er-MedDiet+PA Based Intervention on Anthropometric Characteristics and Lipid Profile
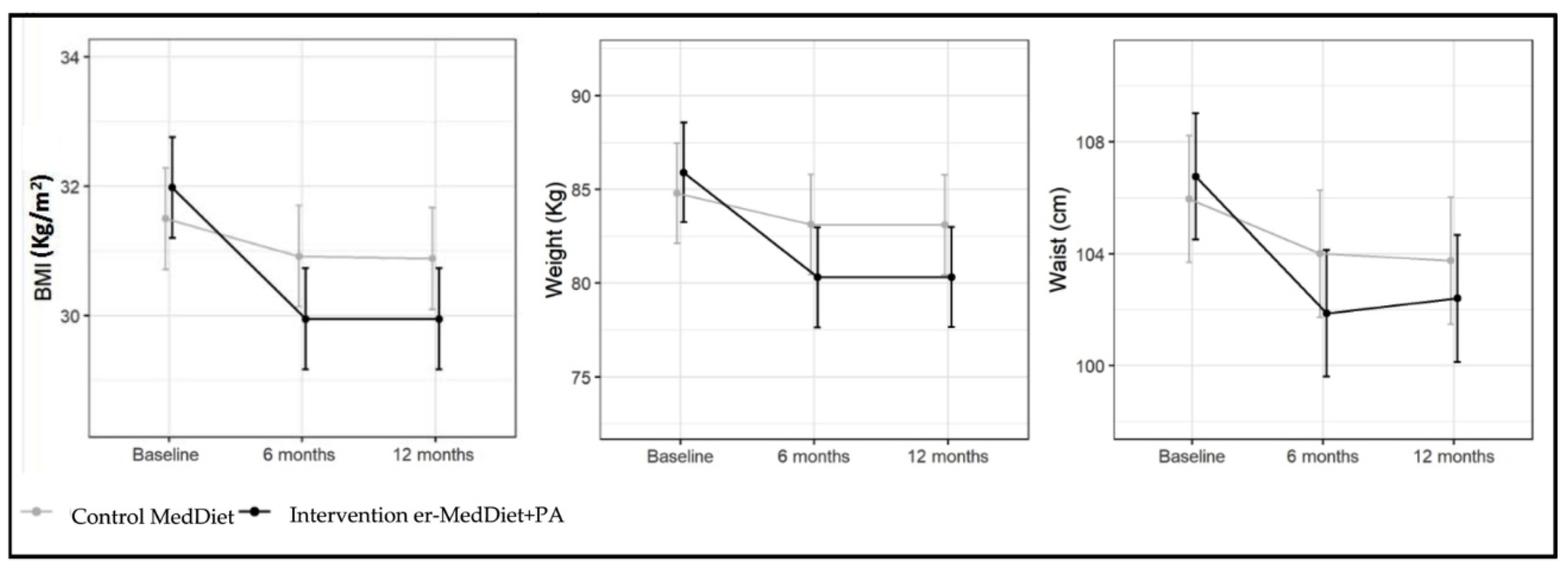
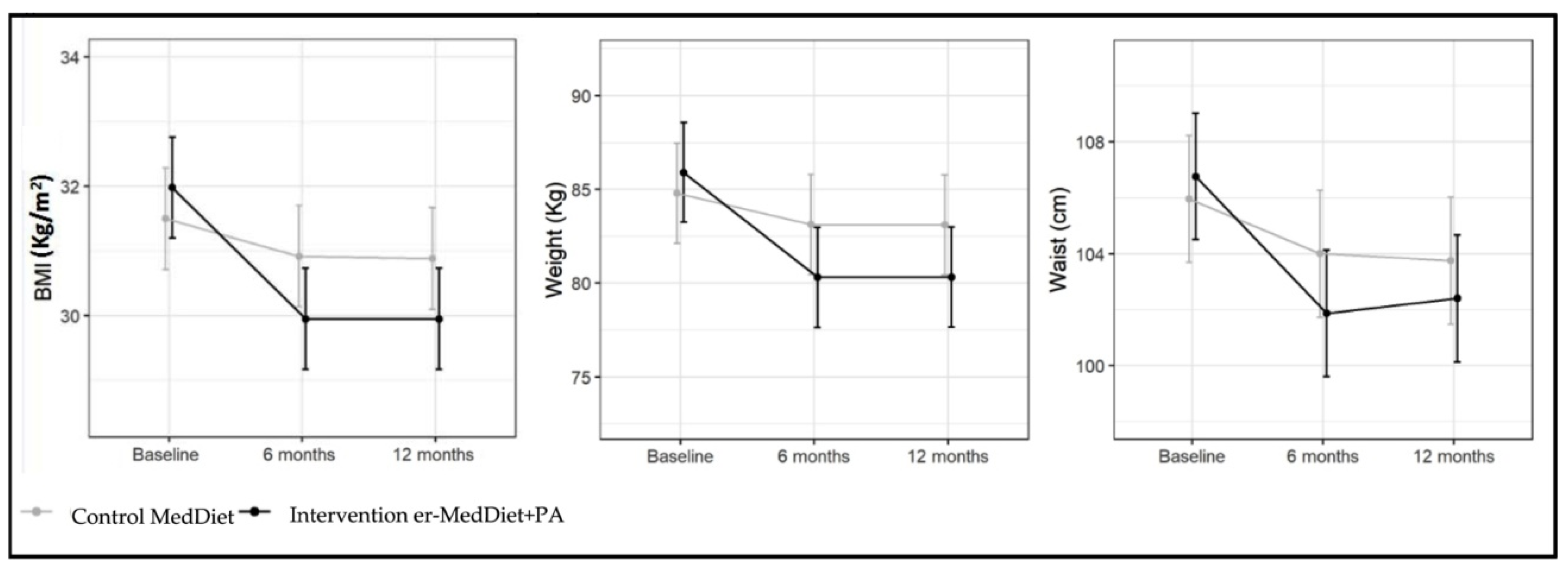
2.1.1. Anthropometric Variables
2.1.2. Lipid Profile
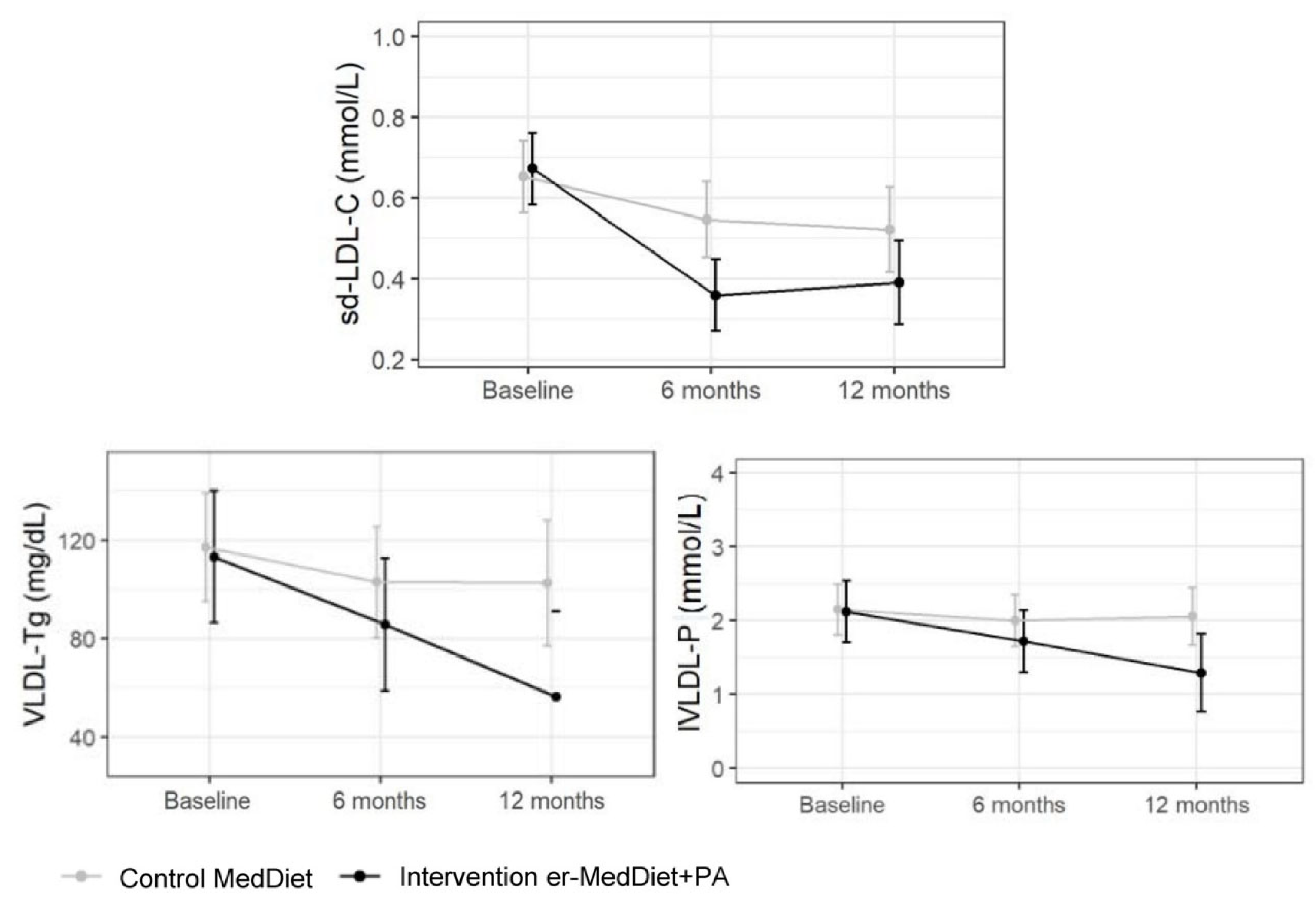
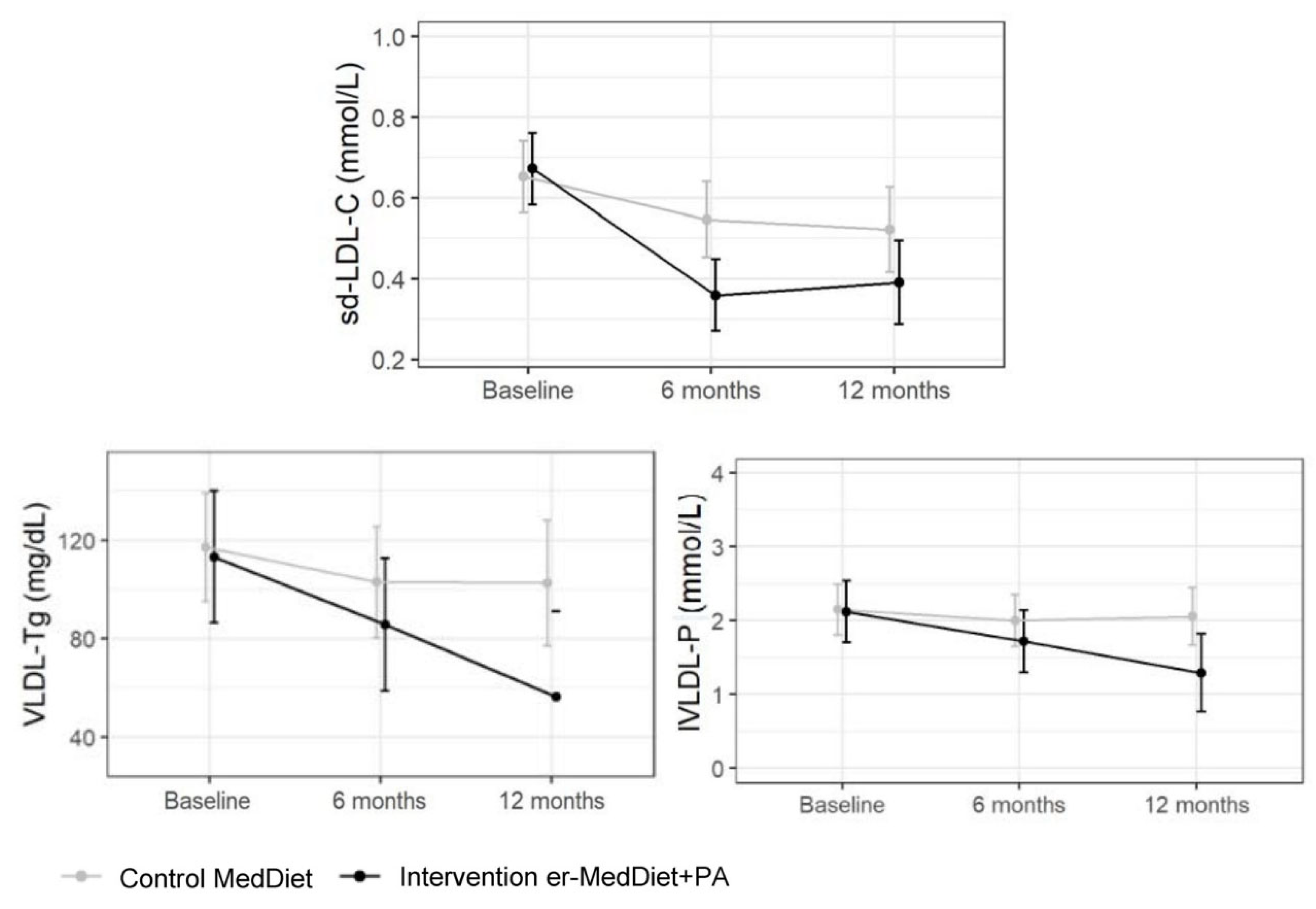
2.1.3. Advanced Lipoprotein Tests
3. Discussion
3.1. Anthropometric Variables
3.2. Conventional Lipid Profile
3.3. Advanced Lipid Profile
4. Materials and Methods
4.1. Study Design
4.2. Study Subjects
4.3. Methods
4.3.1. Conventional Lipid Profile
4.3.2. Advanced Lipoprotein Precipitation Assays
4.3.3. Advanced Lipoprotein Profile by NMR Spectroscopy
4.3.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.-P.; Fullerton, H.J.; et al. Heart disease and stroke statistics—2016 update: A report from the American Heart Association. Circulation 2015, 133, e38–e360. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Nichols, M.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe—Epidemiological update 2015. Eur. Heart J. 2015, 36, 2696–2705. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; et al. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [PubMed]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Theroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W.; et al. Ezetimibe added to statin therapy after acute coronary syndromes. N. Engl. J. Med. 2015, 372, 2387–2397. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, M.; Yokote, K.; Arai, H.; Iida, M.; Ishigaki, Y.; Ishibashi, S.; Umemoto, S.; Egusa, G.; Ohmura, H.; Okamura, T.; et al. Japan Atherosclerosis Society (JAS) Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2017. J. Atheroscler. Thromb 2018, 25, 846–984. [Google Scholar] [CrossRef]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [PubMed]
- Agarwal, S.; Jacobs, D.R., Jr.; Vaidya, D.; Sibley, C.T.; Jorgensen, N.W.; Rotter, J.I.; Chen, Y.D.; Liu, Y.; Andrews, J.S.; Kritchevsky, S.; et al. Metabolic Syndrome Derived from Principal Component Analysis and Incident Cardiovascular Events: The Multi Ethnic Study of Atherosclerosis (MESA) and Health, Aging, and Body Composition (Health ABC). Cardiol. Res. Pract. 2012, 2012, 919425. [Google Scholar] [CrossRef]
- Narayan, K.M.V.; Patel, S.A.; Cunningham, S.A.; Curran, J. Ominous reversal of health gains in the United States: Time to rethink research priorities? Ann. Intern. Med. 2019, 170, 330–331. [Google Scholar] [CrossRef]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef]
- Sanllorente, A.; Soria-Florido, M.T.; Castañer, O.; Lassale, C.; Salas-Salvadó, J.; Martínez-González, M.Á.; Subirana, I.; Ros, E.; Corella, D.; Estruch, R.; et al. A lifestyle intervention with an energy-restricted Mediterranean diet and physical activity enhances HDL function: A substudy of the PREDIMED-Plus randomized controlled trial. Am. J. Clin. Nutr. 2021, 114, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, K.; Tango, T. Effects of lifestyle modification on metabolic syndrome: A systematic review and meta-analysis. BMC Med. 2012, 10, 138. [Google Scholar] [CrossRef] [PubMed]
- Jahangiry, L.; Shojaeizadeh, D.; Montazeri, A.; Najafi, M.; Mohammad, K.; Farhangi, M.A. Modifiable lifestyle risk factors and metabolic syndrome: Opportunities for a web based preventive program. J. Res. Health Sci. 2014, 14, 303–307. [Google Scholar] [PubMed]
- Hsiao, P.Y.; Mitchell, D.C.; Coffman, D.L.; Craig Wood, G.; Hartman, T.J.; Still, C.; Jensen, G.L. Dietary patterns and relationship to obesity-related health outcomes and mortality in adults 75 years of age or greater. J. Nutr. Health Aging 2013, 17, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.Á.; Gea, A.; Ruiz-Canela, M. The Mediterranean diet and cardiovascular health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Castillejo, S.; Valls, R.M.; Castañer, O.; Rubió, L.; Catalán, Ú.; Pedret, A.; Macià, A.; Sampson, M.L.; Covas, M.I.; Fitó, M.; et al. Polyphenol rich olive oils improve lipoprotein particle atherogenic ratios and subclasses profile: A randomized, crossover, controlled trial. Mol. Nutr. Food Res. 2016, 60, 1544–1554. [Google Scholar] [CrossRef]
- Hernáez, Á.; Remaley, A.T.; Farràs, M.; Fernández-Castillejo, S.; Subirana, I.; Schröder, H.; Fernández-Mampel, M.; Muñoz-Aguayo, D.; Sampson, M.; Solà, R.; et al. Olive Oil Polyphenols Decrease LDL Concentrations and LDL Atherogenicity in Men in a Randomized Controlled Trial. J. Nutr. 2015, 145, 1692–1697. [Google Scholar] [CrossRef]
- Ma, S.; Xia, M.; Gao, X. Biomarker Discovery in Atherosclerotic Diseases Using Quantitative Nuclear Magnetic Reso-nance Metabolomics. Front. Cardiovasc. Med. 2021, 8, 681444. [Google Scholar] [CrossRef]
- Stahel, P.; Xiao, C.; Hegele, R.A.; Lewis, G.F. The Atherogenic Dyslipidemia Complex and Novel Approaches to Cardiovascular Disease Prevention in Diabetes. Can. J. Cardiol. 2018, 34, 595–604. [Google Scholar] [CrossRef]
- Marston, N.A.; Giugliano, R.P.; Melloni, G.E.M.; Park, J.G.; Morrill, V.; Blazing, M.A. Association of Apolipoprotein B-Containing Lipoproteins and Risk of Myocardial Infarction in Individuals with and without Atherosclerosis: Distinguishing between Particle Concentration, Type, and Content. JAMA Cardiol. 2022, 7, 250–256. [Google Scholar] [CrossRef]
- Wu, J.; Shi, Y.H.; Niu, D.M.; Li, H.Q.; Zhang, C.N.; Wang, J.J. Association among retinol-binding protein 4, small dense LDL cholesterol and oxidized LDL levels in dyslipidemia subjects. Clin. Biochem. 2012, 45, 619–622. [Google Scholar] [CrossRef] [PubMed]
- Mallol, R.; Rodriguez, M.A.; Brezmes, J.; Masana, L.; Correig, X. Human serum/plasma lipoprotein analysis by NMR: Application to the study of diabetic dyslipidemia. Prog. Nucl. Magn. Reason. Spectrosc. 2013, 70, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Damasceno, N.R.; Sala-Vila, A.; Cofán, M.; Pérez-Heras, A.M.; Fitó, M.; Ruiz-Gutiérrez, V.; Martínez-González, M.Á.; Corella, D.; Arós, F.; Estruch, R.; et al. Mediterranean diet supplemented with nuts reduces waist circumference and shifts lipoprotein subfractions to a less atherogenic pattern in subjects at high cardiovascular risk. Atherosclerosis 2013, 230, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cidón, B.; Padró-Miquel, A.; Alía-Ramos, P.; Castro-Castro, M.J.; Fanlo-Maresma, M.; Dot-Bach, D.; Valero-Politi, J.; Pintó-Sala, X.; Candás-Estébanez, B. Reference values assessment in a Mediterranean population for small dense low-density lipoprotein concentration isolated by an optimized precipitation method. Vasc. Health Risk Manag. 2017, 13, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Chiva-Blanch, G.; Fiol, M.; Gómez-Gracia, E.; Arós, F.; Lapetra, J.; et al. Effect of a high-fat Mediterranean diet on bodyweight and waist circumference: A prespecified secondary outcomes analysis of the PREDIMED randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, e6–e17. [Google Scholar] [CrossRef]
- Mallol, R.; Amigó, N.; Rodríguez, M.A.; Heras, M.; Vinaixa, M.; Plana, N.; Rock, E.; Ribalta, J.; Yanes, O.; Masana, L.; et al. Liposcale: A novel advanced lipoprotein test based on 2D diffusion-ordered 1H NMR spectroscopy. J. Lipid Res. 2015, 56, 737–746. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bulló, M.; Fitó, M.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; López-Miranda, J.; et al. Cohort Profile: Design and methods of the PREDIMED-Plus randomized trial. Int. J. Epidemiol. 2019, 48, 387–388. [Google Scholar] [CrossRef]
- Garber, A.J.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.T.; Bush, M.A.; Dagogo-Jack, S.; Davidson, M.B.; Einhorn, D.; Garvey, W.T.; et al. American association of clinical endocrinologists’ comprehensive diabetes management algorithm 2013 consensus statement. Endocr. Pract. 2013, 19 (Suppl. S1), 1–48. [Google Scholar] [CrossRef]
- Ansell, B.J.; Fonarow, G.C.; Fogelman, A.M. High-density lipoprotein: Is it always atheroprotective? Curr. Atheroscler. Rep. 2006, 8, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Masana, L.; Cabré, A.; Heras, M.; Amigó, N.; Correig, X.; Martínez-Hervás, S.; Real, J.T.; Ascaso, J.F.; Quesada, H.; Julve, J.; et al. Remarkable quantitative and qualitative differences in HDL after niacin or fenofibrate therapy in type 2 diabetic patients. Atherosclerosis 2015, 238, 213–939. [Google Scholar] [CrossRef] [PubMed]
- Bendall, C.L.; Mayr, H.L.; Opie, R.S. Central obesity and the Mediterranean diet: A systematic review of intervention trials. Crit. Rev. Food Sci. Nutr. 2019, 58, 3070–3084. [Google Scholar] [CrossRef] [PubMed]
- Chooi, Y.C.; Ding, C.; Chan, Z.; Lo, J.; Choo, J.; Ding, B.T.K.; Leow, M.K.; Magkos, F. Lipoprotein Subclass Profile after Progressive Energy Deficits Induced by Calorie Restriction or Exercise. Nutrients 2018, 10, 1814. [Google Scholar] [CrossRef]
- Richard, C.; Couture, P.; Ooi, E.M.; Tremblay, A.J.; Desroches, S.; Charest, A.; Lichtenstein, A.H.; Lamarche, B. Effect of mediterranean diet with and without weight loss on apolipoprotein B100 metabolism in men with metabolic syndrome. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.L.; Comperatore, M.; Barona, J.; Calle, M.C.; Andersen, C.; McIntosh, M.; Najm, W.; Lerman, R.H.; Fernandez, M.L. A mediterranean-style, low-glycemic-load diet decreases atherogenic lipoproteins and reduces lipoprotein (a) and oxidized low-density lipoprotein in women with metabolic syndrome. Metabolism 2012, 61, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Goulet, J.; Lamarche, B.; Charest, A.; Nadeau, G.; Lapointe, A.; Desroches, S.; Lemieux, S. Effect of a nutritional intervention promoting the mediterranean food pattern on electrophoretic characteristics of low-density lipoprotein particles in healthy women from the quebec city metropolitan area. Br. J. Nutr. 2004, 92, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Girona, J.; Amigó, N.; Ibarretxe, D.; Plana, N.; Rodríguez-Borjabad, C.; Heras, M.; Ferré, R.; Gil, M.; Correig, X.; Masana, H.D.L. Triglycerides: A New Marker of Metabolic and Cardiovascular Risk. Int. J. Mol. Sci. 2019, 20, 3151. [Google Scholar] [CrossRef]
- Duparc, T.; Ruidavets, J.B.; Genoux, A.; Ingueneau, C.; Najib, S.; Ferrières, J.; Perret, B.; Martinez, L.O. Serum level of HDL particles are independently associated with long-term prognosis in patients with coronary artery disease: The GENES study. Sci. Rep. 2020, 10, 8138. [Google Scholar] [CrossRef]
- Ebbeling, C.B.; Knapp, A.; Johnson, A.; Wong, J.M.W.; Greco, K.F.; Ma, C.; Mora, S.; Ludwig, D.S. Effects of a low-carbohydrate diet on insulin-resistant dyslipoproteinemia—A randomized controlled feeding trial. Am. J. Clin. Nutr. 2022, 115, 154–162. [Google Scholar] [CrossRef]
- Gjuladin-Hellon, T.; Davies, I.G.; Penson, P.; Amiri Baghbadorani, R. Effects of carbohydrate-restricted diets on low-density lipoprotein cholesterol levels in overweight and obese adults: A systematic review and meta-analysis. Nutr. Rev. 2019, 77, 161–180. [Google Scholar] [CrossRef] [PubMed]
- Falkenhain, K.; Roach, L.A.; McCreary, S.; McArthur, E.; Weiss, E.J.; Francois, M.E.; Little, J.P. Effect of carbohydrate-restricted dietary interventions on LDL particle size and number in adults in the context of weight loss or weight maintenance: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2021, 114, 1455–1466. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.L.; Park, Y.; Lee, J.; Lerman, R.H.; Fernandez, M.L. A Mediterranean-style, low-glycemic-load diet reduces the expression of 3-hydroxy-3-methylglutaryl-coenzymeA reductase in mononuclear cells and plasma insulin in women with metabolic syndrome. Nutr. Res. 2011, 31, 659–664. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, B.J. Effect of low-carbohydrate diets on cardiometabolic risk, insulin resistance, and metabolic syndrome. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 301–307. [Google Scholar] [CrossRef]
- Diamond, D.M.; O’Neill, B.J.; Volek, J.S. Low carbohydrate diet: Are concerns with saturated fat, lipids, and cardiovascular disease risk justified? Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Holmes, M.V.; Millwood, I.Y.; Kartsonaki, C.; Hill, M.R.; Bennett, D.A.; Boxall, R.; Guo, Y.; Xu, X.; Bian, Z.; Hu, R.; et al. Lipids, Lipoproteins, and Metabolites and Risk of Myocardial Infarction and Stroke. J. Am. Coll. Cardiol. 2018, 71, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Hyde, P.N.; Sapper, T.N.; Crabtree, C.D.; LaFountain, R.A.; Bowling, M.L.; Buga, A.; Fell, B.; McSwiney, F.T.; Dickerson, R.M.; Miller, V.J.; et al. Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI Insight 2019, 4, e128308. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.; Chen, S.; Durstine, J.L. The effects of exercise training on the traditional lipid profile and beyond. Curr. Sports Med. Rep. 2014, 13, 253–259. [Google Scholar] [CrossRef]
- Crouse, S.F.; O’Brien, B.C.; Grandjean, P.W.; Lowe, R.C.; Rohack, J.J.; Green, J.S. Effects of training and a single session of exercise on lipids and apolipoproteins in hypercholesterolemic men. J. Appl. Physiol. 1997, 83, 2019–2028. [Google Scholar] [CrossRef]
- Straniero, S.; Rosqvist, F.; Edholm, D.; Ahlström, H.; Kullberg, J.; Sundbom, M.; Risérus, U.; Rudling, M. Acute caloric restriction counteracts hepatic bile acid and cholesterol deficiency in morbid obesity. J. Intern. Med. 2017, 281, 507–517. [Google Scholar] [CrossRef]
- Zomer, E.; Gurusamy, K.; Leach, R.; Trimmer, C.; Lobstein, T.; Morris, S.; James, W.P.; Finer, N. Interventions that cause weight loss and the impact on cardiovascular risk factors: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Díaz-López, A.; Ruiz-Canela, M.; Basora, J.; Fitó, M.; Corella, D.; Serra-Majem, L.; Wärnberg, J.; Romaguera, D.; Estruch, R.; et al. Effect of a Lifestyle Intervention Program With Energy-Restricted Mediterranean Diet and Exercise on Weight Loss and Cardiovascular Risk Factors: One-Year Results of the PREDIMED-Plus Trial. Diabetes Care 2019, 42, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Cárdenas-Fuentes, G.; Martínez-González, M.A.; Corella, D.; Vioque, J.; Romaguera, D.; Alfredo Martínez, J.; Tinahones, F.J.; Miranda, J.L.; Estruch, R.; et al. Effectiveness of the physical activity intervention program in the PREDIMED-Plus study: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 110. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Activity and Older Adults. 2021. Available online: https://www.who.int/ncds/prevention/physical-activity/factsheet_olderadults/en (accessed on 9 June 2023).
- Fernandez-Lazaro, C.I.; Toledo, E.; Buil-Cosiales, P.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Martínez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; Vioque, J.; et al. Factors associated with successful dietary changes in an energy-reduced Mediterranean diet intervention: A longitudinal analysis in the PREDIMED-Plus trial. Eur. J. Nutr. 2022, 61, 1457–1475. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Molina, L.; Sarmiento, M.; Peñafiel, J.; Donaire, D.; Garcia-Aymerich, J.; Gomez, M.; Ble, M.; Ruiz, S.; Frances, A.; Schröder, H.; et al. Validation of the Regicor Short Physical Activity Questionnaire for the Adult Population. PLoS ONE 2017, 12, e0168148. [Google Scholar] [CrossRef]
- Abell, L.L.; Levy, B.B.; Brodie, B.B.; Kendall, F.E. A simplified method for the estimation of total cholesterol in serum and demonstration of its specificity. J. Biol. Chem. 1952, 195, 357–366. [Google Scholar] [CrossRef]
- Recommendations for Improving Cholesterol Measurement: A Report from the Laboratory Standardization Panel of the National Cholesterol Education Program; NIH Publication No. 90-2964; U.S. Department of Health and Human Services, Public Health Service, National Institute of Health: Bethesda, MD, USA, 1990.
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Fernández-Cidón, B.; Candás-Estébanez, B.; Ribalta, J.; Rock, E.; Guardiola-Guionnet, M.; Amigó, N.; Padró-Miquel, A.; Alía-Ramos, P.; Pintó-Sala, X. Precipitated sdLDL: An easy method to estimate LDL particle size. J. Clin. Lab. Anal. 2020, 34, e23282. [Google Scholar] [CrossRef] [PubMed]
- Dalenberg, D.A.; Schryver, P.G.; Klee, G.G. Analytical performance specifications: Relating laboratory performance to quality required for intended clinical use. Clin. Lab. Med. 2013, 33, 55–73. [Google Scholar] [CrossRef]
- Puig-Jové, C.; Castelblanco, E.; Falguera, M.; Hernández, M.; Soldevila, B.; Julián, M.T.; Teis, A.; Julve, J.; Barranco-Altirriba, M.; Franch-Nadal, J.; et al. Advanced lipoprotein profile in individuals with normal and impaired glucose metabolism. Rev. Esp. Cardiol. (Engl. Ed.) 2022, 75, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Control Group n = 95 | Intervention Group n = 107 | p-Value | |
|---|---|---|---|
| Age (years) | 64.2 (63.3, 65.2) | 64.8 (63.9, 65.6) | 0.427 |
| Men (%) | 49 (51.6%) | 54 (50.5%) | 0.875 |
| Smoker (%) | 0.774 | ||
| Current smoker | 12 (12.6%) | 15 (14.0%) | |
| Former smoker | 42 (44.2%) | 42 (39.3%) | |
| Never smoker | 41 (43.2%) | 50 (46.7%) | |
| Education (%) | 0.619 | ||
| Elementary (5–8 years) | 48 (50.5%) | 61 (57%) | |
| Secondary (9–12 years) | 26 (27.4%) | 27 (25.2%) | |
| Post-secondary (>12 years) | 21 (22.1%) | 19 (17.8%) | |
| Hypertension (%) | 79 (83.2%) | 92 (86%) | 0.578 |
| Diabetes (%) | 29 (30.5%) | 37 (34.6%) | 0.540 |
| Dyslipidemia (%) | 76 (80%) | 82 (76.6%) | 0.563 |
| Lipid-lowering treatment (%) | 55 (57.9%) | 63 (58.9%) | 0.887 |
| Weight (kg) | 85.4 (82.8, 87.9) | 85.3 (82.9, 87.8) | 0.997 |
| Body mass index (kg/m2) | 31.9 (31.4, 32.5) | 32.0 (31.5, 32.6) | 0.754 |
| Waist circumference (cm) | 107 (105.1, 108.8) | 107 (105.3, 109) | 0.925 |
| Hip (cm) | 107 (105.6, 108.6) | 108 (106.2, 109.4) | 0.555 |
| Waist-to-hip ratio | 1.00 (0.98, 1.02) | 1.00 (0.98,1.01) | 0.629 |
| LDL-cholesterol (mmol/L) | 3.04 (2.84, 3.23) | 3.00 (2.83, 3.16) | 0.765 |
| LDL-cholesterol ≤ 3.37 mmol/L (%) | 57 (66.3%) | 71 (68.3%) | 0.771 |
| HDL-cholesterol (mmol/L) | 1.24 (1.16, 1.31) | 1.25 (1.18, 1.31) | 0.802 |
| HDL-cholesterol ≥ 1.04 mmol/L (%) | 62 (65.3%) | 75 (70.1%) | 0.463 |
| Triglycerides (mmol/L) * | 1.73 (1.56, 1.92) | 1.57 (1.43, 1.71) | 0.152 |
| Triglycerides ≤ 1.70 mmol/L (%) | 48 (50.5%) | 60 (56.1%) | 0.430 |
| Non-HDL-cholesterol (mmol/L) | 3.81 (3.62, 4.0) | 3.49 (3.25, 3.73) | 0.045 |
| Non-HDL-cholesterol ≤ 4.14 mmol/L (%) | 63 (66.3%) | 70 (68.6%) | 0.729 |
| Energy and Nutrients | Visit | Control Group n = 95 | Intervention Group n = 107 | p-Value |
|---|---|---|---|---|
| Energy–Kcal/day | Baseline | 2352 (2213, 2490) | 2343 (2221, 2464) | 0.923 |
| 6m.change | −215 (−338, −91) | −252 (−356, −148) | 0.650 | |
| 12m.change | −250 (−378, −122) | −252 (−356, −148) | 0.982 | |
| Protein—% Energy | Baseline | 17.9 (17.1, 18.6) | 17.6 (17.0, 18.3) | 0.622 |
| 6m.change | +0.7 (+0.03, +1.3) | +2.9 (+2.2, +3.5) | <0.001 | |
| 12m.change | +1.0 (+0.4, +1.7) | +2.7 (+2.0, +3.4) | 0.001 | |
| Protein—g/kg of body weight | Baseline | 1.21 (1.15, 1.27) | 1.19 (1.14, 1.25) | 0.682 |
| 6m.change | −0.016 (−0.068, +0.036) | +0.17 (+0.116, +0.222) | <0.001 | |
| 12m.change | −0.02 (−0.083, +0.053) | +0.15 (+0.095, +0.204) | <0.001 | |
| Carbohydrate—% Energy | Baseline | 37.7 (36.2, 39.2) | 39.1 (37.8, 40.4) | 0.165 |
| 6m.change | −4.2 (−5.7, −2.7) | −6.6 (−7.9, −5.2) | 0.021 | |
| 12m.change | −3.8 (−5.2, −2.3) | −7.0 (−8.4, −5.7) | 0.001 | |
| Total fat—% Energy | Baseline | 42.1 (40.8, 43.5) | 40.4 (39.2, 41.6) | 0.058 |
| 6m.change | +3.6 (+2.1, +5.1) | +4.2 (+2.9, +5.5) | 0.522 | |
| 12m.change | +2.5 (+1.1, +3.9) | +4.7 (+3.3, +6.2) | 0.028 | |
| SFA—% Energy | Baseline | 10.9 (10.4, 11.3) | 10.2 (9.8, 10.6) | 0.035 |
| 6m.change | −0.7 (−1.2, −0.2) | −1.2 (−1.6, −0.8) | 0.120 | |
| 12m.change | −1.3 (−1.8, −0.8) | −0.7 (−1.1,−0.3) | 0.070 | |
| MUFA—% Energy | Baseline | 21.8 (20.8, 22.8) | 20.6 (19.8, 21.4) | 0.057 |
| 6m.change | +4.0 (+2.8,+5.1) | +5.8 (4.9, +6.8) | 0.012 | |
| 12m.change | +3.3 (+2.2, +4.4) | +5.9 (+4.8, +6.9) | 0.001 | |
| PUFA—% Energy | Baseline | 7.2 (6.8, 7.6) | 7.1 (6.7, 7.4) | 0.638 |
| 6m.change | +1.1 (+0.7, +1.5) | +1.4 (+1.0, +1.9) | 0.204 | |
| 12m.change | +1.2 (0.7, +1.6) | +1.6 (+1.2, +2.0) | 0.170 | |
| Fiber–g/day | Baseline | 25.2 (23.7, 26.6) | 24.5 (23.0, 26.1) | 0.551 |
| 6m.change | +2.7 (1.0, +4.5) | +5.7 (+3.8, +7.5) | 0.026 | |
| 12m.change | +2.8 (+1.0, +4.3) | +4.9 (+3.2, +6.6) | 0.067 | |
| Cholesterol–mg/day | Baseline | 399 (375, 424) | 396 (373, 419) | 0.852 |
| 6m.change | −25.6 (−49.0, −2.2) | −29.1 (−51.2,−6.9) | 0.833 | |
| 12m.change | −27.8 (−52.5, −3.1) | −13.2 (−38.0, +11.6) | 0.413 | |
| Alcohol intake–g/day | Baseline | 8.1 (5.9, 10.3) | 10.1 (7.6, 12.6) | 0.243 |
| 6m.change | −0.9 (−2.4, +0.5) | −2.2 (−3.9, −0.6) | 0.251 | |
| 12m.change | +0.03 (−1.5, +1.6) | −1.9 (+3.8, −0.1) | 0.115 | |
| Physical activity–MET min/week | Baseline | 2336 (1957, 2715) | 2614 (2240, 2987) | 0.303 |
| 6m.change | +404 (45, 763) | +1263 (847, 1681) | 0.002 | |
| 12m.change | +569 (8, 1129) | +1242 (743, 1741) | 0.076 |
| Time Effect (Control Effect *) | Interaction Group and Time (Intervention vs. Control Effect **) | |||||||
|---|---|---|---|---|---|---|---|---|
| 6 Months | 12 Months | 6 Months | 12 Months | |||||
| Coefficient [95% CI] | p-Value | Coefficient [95% CI] | p-Value | Coefficient [95% CI] | p-Value | Coefficient [95% CI] | p-Value | |
| Body mass index (kg/m2) | −0.58 [−0.84; −0.32] | <0.01 | −0.62 [−0.88; −0.35] | <0.01 | −1.45 [−1.82; −1.09] | <0.01 | −1.42 [−1.78; −1.05] | <0.01 |
| Waist circumference (cm) | −1.95 [−2.99; −0.91] | <0.01 | −2.21 [−3.26; −1.15] | <0.01 | −2.94 [−4.4; −1.48] | <0.01 | −2.16 [−3.64; −0.68] | <0.01 |
| Cholesterol | ||||||||
| LDL (mmol/L) | −0.1 [−0.26; 0.06] | 0.212 | −0.26 [−0.42; −0.1] | <0.01 | 0.04 [−0.18; 0.26] | 0.727 | 0.2 3[0.01; 0.45] | 0.044 |
| sd-LDL (mmol/L) | −0.11 [−0.23; 0.02] | 0.091 | −0.13 [−0.26; 0] | 0.049 | −0.21 [−0.38; −0.04] | 0.016 | −0.15 [−0.33; 0.03] | 0.108 |
| HDL (mmol/L) | 0.04 [0; 0.09] | 0.047 | 0.02 [−0.03; 0.06] | 0.446 | 0.04 [−0.02; 0.1] | 0.233 | 0.1 [0.04; 0.17] | <0.01 |
| Non-HDL (mmol/L) | −0.1 [−0.33; 0.13] | 0.385 | −0.37 [−0.62; −0.11] | <0.01 | 0.08 [−0.25; 0.4] | 0.65 | 0.54 [0.17; 0.91] | <0.01 |
| IDL (mg/dL) | −2.28 [−4.66; 0.09] | 0.06 | −2.72 [−5.43; −0.01] | 0.049 | −0.78 [−4.29; 2.72] | 0.661 | −1.97 [−6.43; 2.49] | 0.386 |
| VLDL (mg/dL) | −4.98 [−10.55; 0.6] | 0.08 | −4.11 [−10.51; 2.29] | 0.208 | −3.32 [−11.58; 4.94] | 0.431 | −10.38 [−21.02; 0.26] | 0.056 |
| VLDL+IDL (mg/dL) | −7.26 [−14.73; 0.21] | 0.057 | −6.87 [−15.44; 1.69] | 0.116 | −4.17 [−15.23; 6.89] | 0.46 | −12.19 [−26.38; 1.99] | 0.092 |
| Triglycerides | ||||||||
| LOG(TG (mmol/L)) | −0.16 [−0.25; −0.08] | <0.01 | −0.06 [−0.15; 0.03] | 0.176 | −0.06 [−0.18; 0.07] | 0.385 | −0.15 [−0.28; −0.02] | 0.021 |
| LDL (mg/dL) | −1.87 [−4.64; 0.9] | 0.186 | −2.45 [−5.6; 0.7] | 0.127 | −1.58 [−5.66; 2.51] | 0.449 | −2.7 [−7.86; 2.45] | 0.304 |
| HDL (mg/dL) | −4.19 [−8.2; −0.19] | 0.04 | −0.96 [−5.46; 3.54] | 0.676 | −1.48 [−7.32; 4.36] | 0.62 | −6.56 [−13.87; 0.74] | 0.078 |
| IDL (mg/dL) | −1.75 [−3.67; 0.17] | 0.075 | −1.8 [−3.99; 0.4] | 0.108 | −0.66 [−3.5; 2.17] | 0.647 | −2.23 [−5.84; 1.38] | 0.226 |
| VLDL (mg/dL) | −14.14 [−35.32; 7.04] | 0.191 | −14.5 [−38.78; 9.79] | 0.242 | −13.36 [−44.71; 17.99] | 0.404 | −42.33 [−82.56; −2.1] | 0.039 |
| Particle number | ||||||||
| LDL (nmol/L) | 30 [−110.2; 170.21] | 0.675 | −111.06 [−269.85; 47.72] | 0.17 | −86.05 [−292.51; 120.41] | 0.414 | −41 [−299.64; 217.64] | 0.756 |
| lLDL (µmol/L) | 17.31 [0.99; 33.63] | 0.038 | 6.06 [−12.53; 24.66] | 0.523 | −3.26 [−27.35; 20.82] | 0.791 | −0.24 [−30.77; 30.29] | 0.988 |
| sLDL (nmol/L) | 14.63 [−76.17; 105.43] | 0.752 | −87.05 [−189.62; 15.53] | 0.096 | −72.6 [−206.2; 61] | 0.287 | −40.29 [−206.9; 126.2] | 0.635 |
| HDL (µmol/L) | −2.67 [−5.3; −0.05] | 0.046 | −0.17 [−3.15; 2.8] | 0.909 | 2.45 [−1.41; 6.31] | 0.214 | −0.81 [−5.66; 4.04] | 0.744 |
| lHDL (µmol/L) | −0.02 [−0.04; 0.01] | 0.191 | −0.01 [−0.04; 0.02] | 0.489 | 0.02 [−0.02; 0.06] | 0.3 | −0.01 [−0.06; 0.03] | 0.539 |
| sHDL (µmol/L) | −1.7 [−3.81; 0.41] | 0.115 | 0.12 [−2.28; 2.53] | 0.92 | 1.06 [−2.05; 4.18] | 0.503 | −0.98 [−4.91; 2.96] | 0.627 |
| VLDL (nmol/L) | −12.06 [−26.75; 2.62] | 0.107 | −11.78 [−28.65; 5.09] | 0.171 | −3.18 [−25.27; 18.91] | 0.778 | −20.8 [−49.42; 7.82] | 0.154 |
| lVLDL (nmol/L) | −0.15 [−0.45; 0.16] | 0.336 | −0.1 [−0.45; 0.25] | 0.588 | −0.25 [−0.7; 0.2] | 0.276 | −0.73 [−1.32; −0.15] | 0.014 |
| sVLDL (nmol/L) | −10.87 [−25.99; 4.26] | 0.159 | −10.99 [−28.32; 6.34] | 0.214 | 2.11 [−20.27; 24.49] | 0.853 | −10.02 [−38.7; 18.65] | 0.493 |
| Particle size | ||||||||
| VLDL (nm) | 0.05 [−0.11; 0.2] | 0.567 | 0.1 [−0.07; 0.28] | 0.241 | 0.05 [−0.18; 0.28] | 0.653 | 0.23 [−0.05; 0.51] | 0.115 |
| LDL (nm) | 0.07 [−0.1; 0.24] | 0.424 | 0.15 [−0.04; 0.34] | 0.128 | 0.11 [−0.14;0.36] | 0.376 | 0.05 [−0.26; 0.37] | 0.74 |
| HDL (nm) | 0 [−0.03; 0.03] | 0.904 | −0.01 [−0.05; 0.02] | 0.401 | 0 [−0.04; 0.04] | 0.966 | 0.03 [−0.02; 0.08] | 0.252 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Candás-Estébanez, B.; Fernández-Cidón, B.; Corbella, E.; Tebé, C.; Fanlo-Maresma, M.; Esteve-Luque, V.; Salas-Salvadó, J.; Fitó, M.; Riera-Mestre, A.; Ros, E.; et al. The Impact of the Mediterranean Diet and Lifestyle Intervention on Lipoprotein Subclass Profiles among Metabolic Syndrome Patients: Findings of a Randomized Controlled Trial. Int. J. Mol. Sci. 2024, 25, 1338. https://doi.org/10.3390/ijms25021338
Candás-Estébanez B, Fernández-Cidón B, Corbella E, Tebé C, Fanlo-Maresma M, Esteve-Luque V, Salas-Salvadó J, Fitó M, Riera-Mestre A, Ros E, et al. The Impact of the Mediterranean Diet and Lifestyle Intervention on Lipoprotein Subclass Profiles among Metabolic Syndrome Patients: Findings of a Randomized Controlled Trial. International Journal of Molecular Sciences. 2024; 25(2):1338. https://doi.org/10.3390/ijms25021338
Chicago/Turabian StyleCandás-Estébanez, Beatriz, Bárbara Fernández-Cidón, Emili Corbella, Cristian Tebé, Marta Fanlo-Maresma, Virginia Esteve-Luque, Jordi Salas-Salvadó, Montserrat Fitó, Antoni Riera-Mestre, Emilio Ros, and et al. 2024. "The Impact of the Mediterranean Diet and Lifestyle Intervention on Lipoprotein Subclass Profiles among Metabolic Syndrome Patients: Findings of a Randomized Controlled Trial" International Journal of Molecular Sciences 25, no. 2: 1338. https://doi.org/10.3390/ijms25021338
APA StyleCandás-Estébanez, B., Fernández-Cidón, B., Corbella, E., Tebé, C., Fanlo-Maresma, M., Esteve-Luque, V., Salas-Salvadó, J., Fitó, M., Riera-Mestre, A., Ros, E., & Pintó, X. (2024). The Impact of the Mediterranean Diet and Lifestyle Intervention on Lipoprotein Subclass Profiles among Metabolic Syndrome Patients: Findings of a Randomized Controlled Trial. International Journal of Molecular Sciences, 25(2), 1338. https://doi.org/10.3390/ijms25021338