
Biopolymer Drug Delivery Systems for Oromucosal Application: Recent Trends in Pharmaceutical R&D



Abstract
1. Introduction
2. Biological Barriers in the Oral Cavity
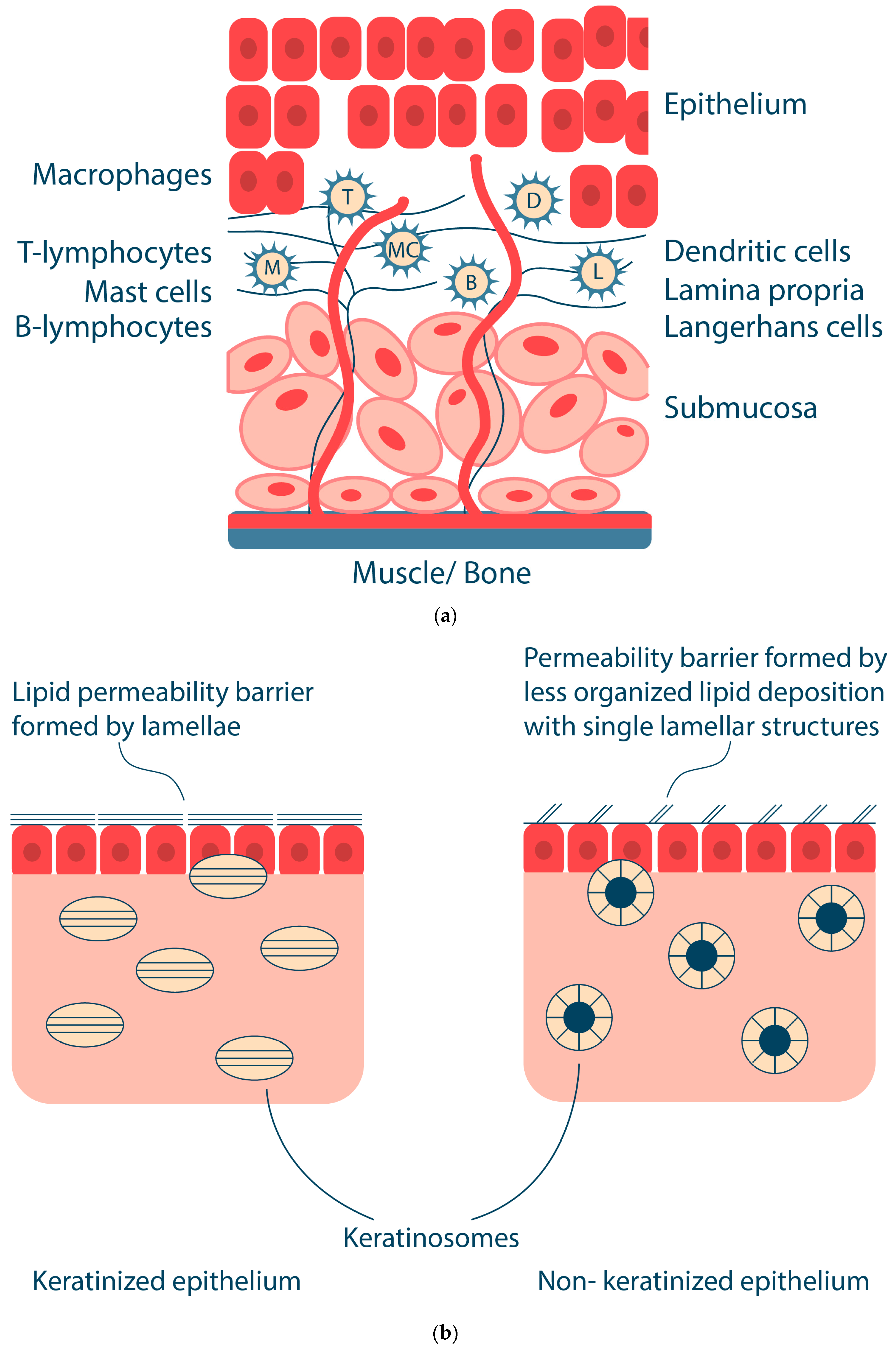
2.1. Structure and Functions of the Oral Mucosa
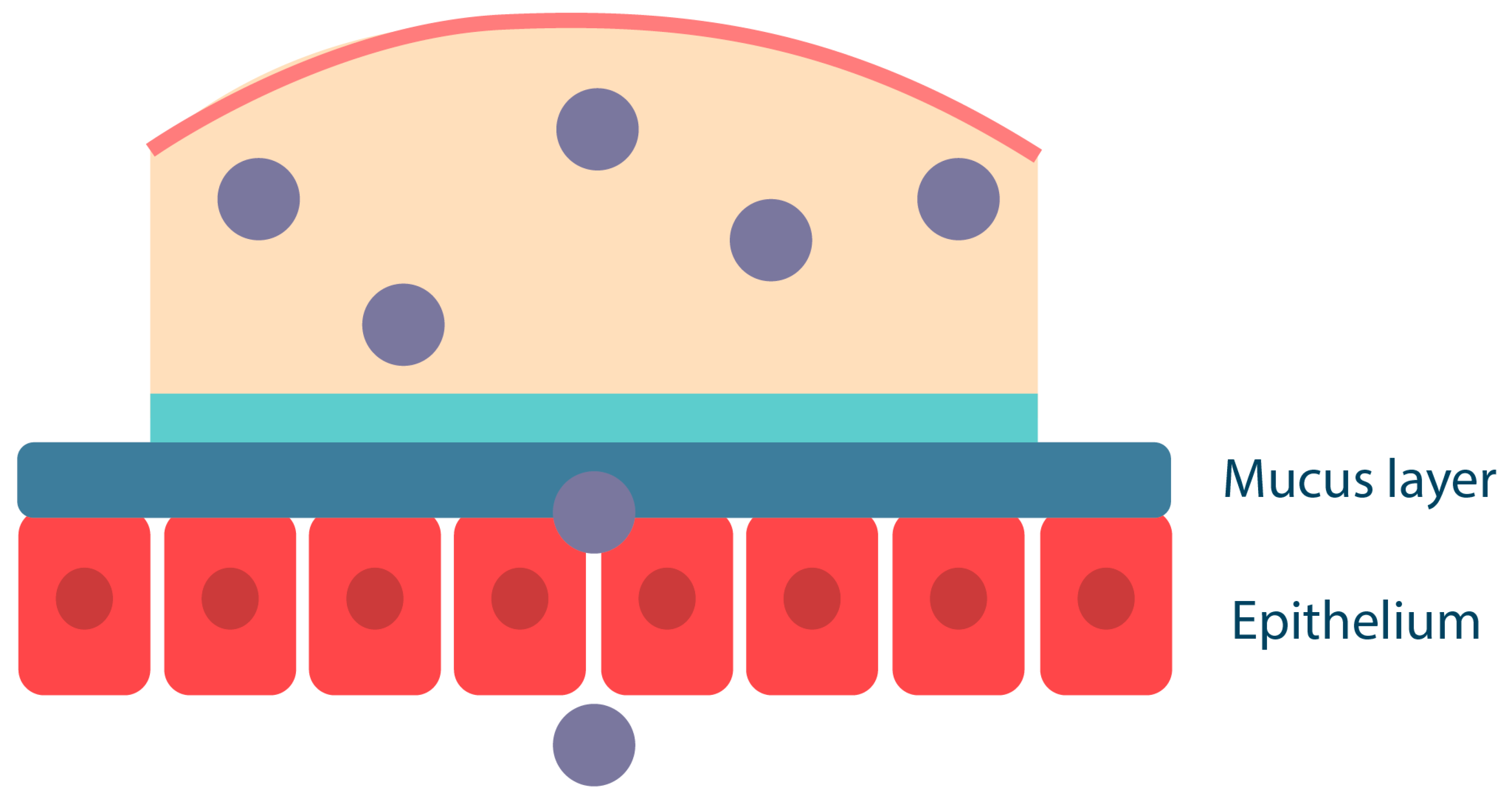
2.2. Mucus and Mucins: Structure and Function
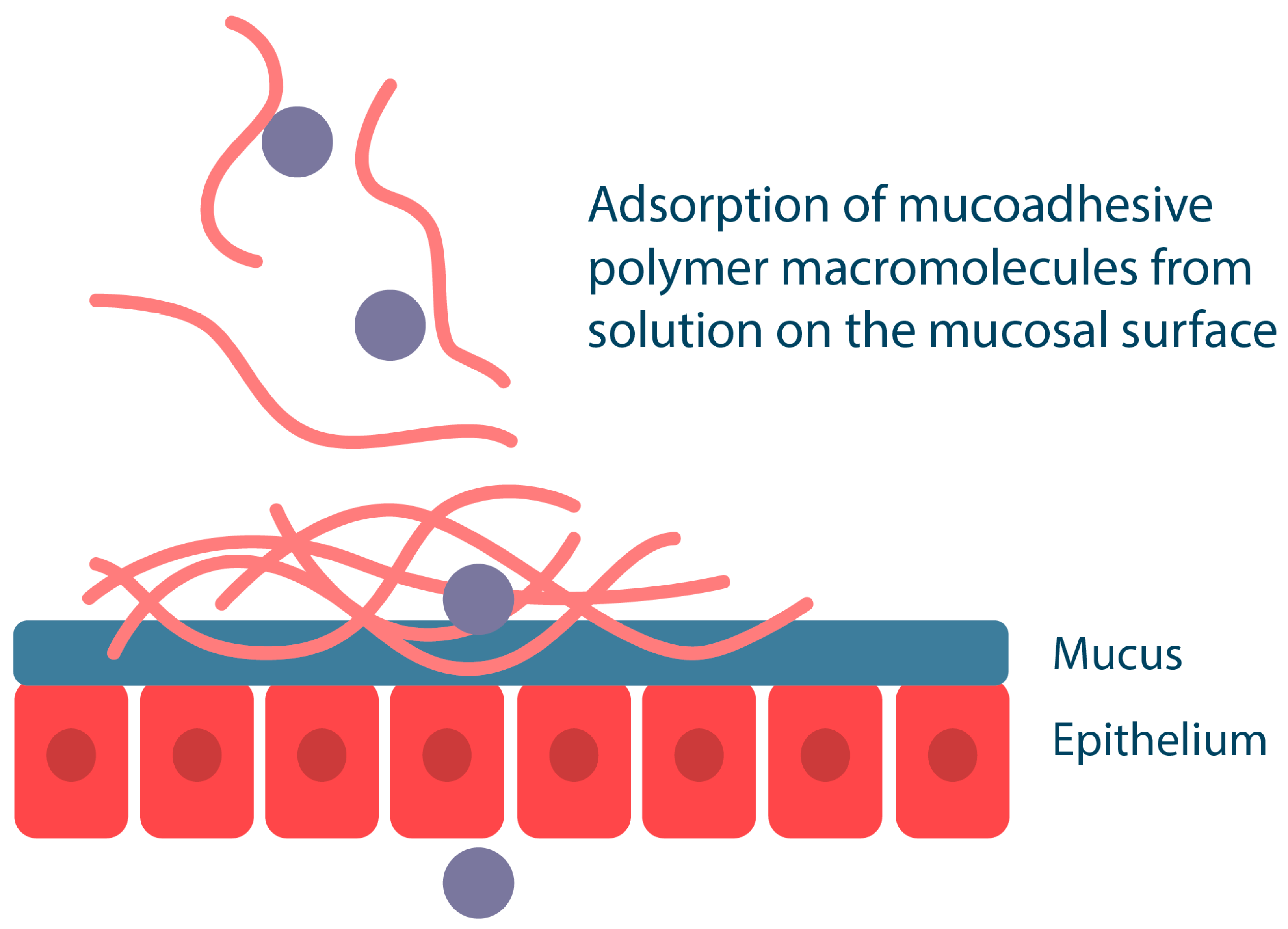
2.3. Mucoadhesion and Mucoadhesive Properties of Various Dosage Forms
- (i)
- Adsorption theory is based on the formation of chemical bonds of covalent and non-covalent nature (hydrogen bonds, electrostatic and hydrophobic interactions, and van der Waals forces) between the polymer and mucin;
- (ii)
- Diffusion theory focuses on the entanglement of polymer chains with mucin macromolecules, resulting in the formation of a strong polymer network. Important characteristics of polymers that affect their diffusion properties are the flexibility of the polymer chain, the similarity of chemical structures and diffusion coefficients, and the contact time of the polymer with the mucosa;
- (iii)
- The electron theory is based on the different electronic properties of polymers and mucins, which leads to electron transfer between the two surfaces; as a result, a doubly charged layer is formed at the mucus/polymer interface, allowing attraction and diffusion of the polymer with the mucin;
- (iv)
- Fracture theory considers the strength of the adhesive bond between the polymer and the mucins as a function of the force required to detach the polymer layer from the mucosal surface;
- (v)
- Mechanical theory is based on the process of adhesion of the polymer to the rough surface of the mucosa. The rough surface provides a larger contact area between the polymer and the mucosa and also provides increased viscoelastic and plastic energy dissipation during bond disruption, which is an important factor in mucoadhesion;
- (vi)
- Wetting theory refers to the ability of the polymer to spread spontaneously over the mucosal surface; this ability is a necessary property for the occurrence of mucoadhesion.
2.4. Overview of Mucoadhesion Assays
- (1)
- Tensile strength (mechanical method), which is based on measuring the detachment force of the test material from the mucosal surface. This method uses an instrument such as a texture analyzer and can be used to study solid and semi-solid formulations. A variation of this method is the shear test, which measures the force required to detach mucoadhesive samples layer by layer (this test is specific to mucoadhesive patches [50]);
- (2)
- The method of dynamic and electrophoretic light scattering is based on the measurement of hydrodynamic diameters and ζ-potentials of mucin particles before and after interaction with liquid mucoadhesive systems [68]. For example, the study [69] has shown that the determination of the ζ-potential of chitosan nanoparticles in the presence of mucin is a fast and convenient technique to study the mucoadhesive properties of chitosan nanoparticles cross-linked with tripolyphosphate. The interaction of NH3+ groups of chitosan with ionized COO− groups of sialic acid of mucin resulted in a significant increase in the hydrodynamic size of the obtained particles and a decrease in their ζ-potential;
- (3)
- Spectrophotometric methods, namely colorimetric and turbidimetric methods. The colorimetric method is based on the determination of the amount of mucin adsorbed on the surface of mucoadhesive biopolymer particles. The biopolymer system is incubated with mucin solution and separated. The non-adsorbed mucin is then treated with periodic acid to oxidize the hydroxyl groups to aldehyde groups and quantified using Schiff’s reagent [70]. This method is convenient and reproducible, correlates well with in vivo conditions, and has been widely used to determine the mucoadhesion properties of chitosan-based biopolymer delivery systems [69]. The turbidimetric titration method can also be used to study the mucoadhesive properties of polymers. In turbidimetric titration, polymers with high affinity to mucin easily form aggregates, which changes the turbidity of the system. The method can also be used to estimate the degree of polymer-mucin complexation [71];
- (4)
- Rheological method. The interaction of polymer gel with mucins can be evaluated by increasing the viscosity of the system through rheological synergism due to the rearrangement of macromolecules [51]. This behavior is characteristic of anionic macromolecules that possess both many hydrogen-bonding functional groups and a branched structure (e.g., carrageenans) [72]. However, polycationic molecules (e.g., chitosan) that form particles upon interaction with mucins are then characterized by a decrease in the viscosity of the system [69].
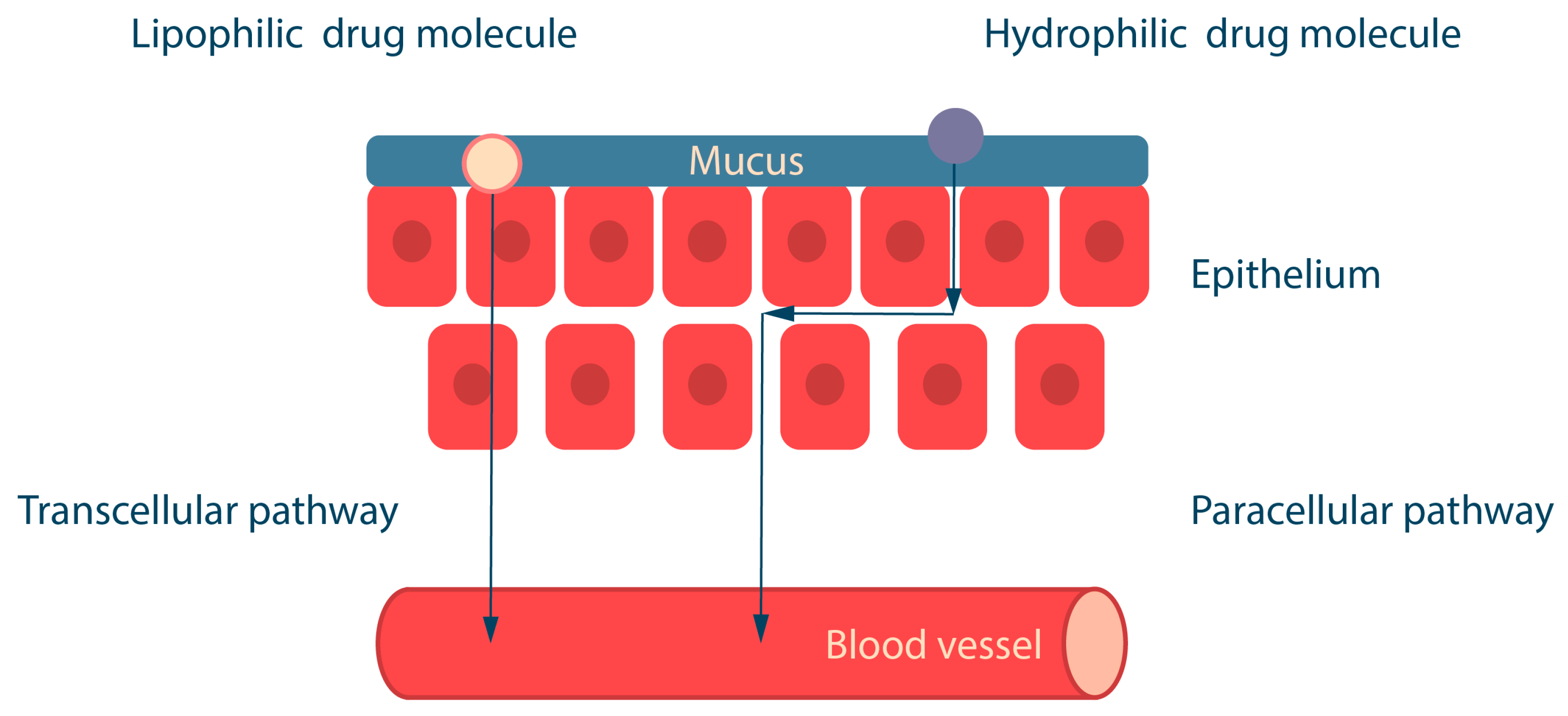
3. Drug Absorption in the Oral Cavity: Transcellular and Paracellular Transport
4. Mucoadhesive Biopolymers
- (1)
- The molecular weight of the polymer should generally be in the range of 10 to 4000 kDa, which allows polymers to hydrate easily, releasing active groups for interaction with mucin and, at the same time, forming strong gels; polymers with a lower MW pass easily into a dissolved state, while those with a higher MW are poorly hydrated; the length of the polymer chain should be optimal on the one hand to promote interpenetration of macromolecules and on the other hand not to hinder diffusion;
- (2)
- Molecular conformation: the helical conformation of some biopolymers, such as dextrans, protects the chemical groups responsible for mucoadhesion, in contrast to linear biopolymers, whose conformation provides accessibility for chemical interactions with mucin;
- (3)
- The flexibility of the polymer chains allows interpenetration and adhesion of the polymer molecules with the mucins; the optimal degree of cross-linking of the polymers has a positive effect on gel formation and mucoadhesion and thus provides a controlled release of the drug;
- (4)
- The mucoadhesive properties of polymers containing ionizable groups are affected by pH, e.g., for high mucoadhesion of polymers with a large number of carboxylate groups, the groups must be in non-ionized form (i.e., at pH below pKa). pH also affects positively charged polymers, e.g., the protonated amino groups of chitosan form ionic bonds with mucins, enhancing mucoadhesion. pH can also alter the conformation of macromolecules.
4.1. Cationic Biopolymers
4.2. Anionic Biopolymers
4.3. Non-Ionic Biopolymers
4.4. Polyampholyte Biopolymers
4.5. Thiolated Biopolymers (Thiomers)
4.6. Catechol-Based Adhesive Biopolymers as Products of Mussel-Inspired Chemistry
5. Dosage Forms for Oromucosal Application
5.1. Oromucosal Patches
5.2. Buccal Tablets
5.3. Oromucosal Gels
6. Nanotechnology-Based Systems to Improve Buccal Drug Delivery
7. Conclusions and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Halwani, A.A. Development of pharmaceutical nanomedicines: From the bench to the market. Pharmaceutics 2022, 14, 106. [Google Scholar] [CrossRef]
- Sahu, T.; Ratre, Y.K.; Chauhan, S.; Bhaskar, L.; Nair, M.P.; Verma, H.K. Nanotechnology based drug delivery system: Current strategies and emerging therapeutic potential for medical science. J. Drug Deliv. Sci. Technol. 2021, 63, 102487. [Google Scholar] [CrossRef]
- Singh, A.P.; Biswas, A.; Shukla, A.; Maiti, P. Targeted therapy in chronic diseases using nanomaterial-based drug delivery vehicles. Signal Transduct. Target. Ther. 2019, 4, 33. [Google Scholar] [CrossRef]
- Babadi, D.; Dadashzadeh, S.; Osouli, M.; Abbasian, Z.; Daryabari, M.S.; Sadrai, S.; Haeri, A. Biopharmaceutical and pharmacokinetic aspects of nanocarrier-mediated oral delivery of poorly soluble drugs. J. Drug Deliv. Sci. Technol. 2021, 62, 102324. [Google Scholar] [CrossRef]
- Mitragotri, S.; Burke, P.A.; Langer, R. Overcoming the challenges in administering biopharmaceuticals: Formulation and delivery strategies. Nat. Rev. Drug Discov. 2014, 13, 655–672. [Google Scholar] [CrossRef]
- Shirvan, A.R.; Bashari, A.; Hemmatinejad, N. New insight into the fabrication of smart mucoadhesive buccal patches as a novel controlled-drug delivery system. Eur. Polym. J. 2019, 119, 541–550. [Google Scholar] [CrossRef]
- Jain, S.K.; Sahu, A.; Keservani, R.K. Oral Drug Delivery System. In Advances in Novel Formulations for Drug Delivery; Keservani, R.K., Kesharwani, R.K., Sharma, A.K., Eds.; Wiley VCH Verlag: Weinheim, Germany, 2023; pp. 383–400. [Google Scholar] [CrossRef]
- Goyal, A.K.; Singh, R.; Chauhan, G.; Rath, G. Non-invasive systemic drug delivery through mucosal routes. Artif. Cells Nanomed. Biotechnol. 2018, 46, 539–551. [Google Scholar] [CrossRef]
- Dubashynskaya, N.V.; Skorik, Y.A. Patches as polymeric systems for improved delivery of topical corticosteroids: Advances and future perspectives. Int. J. Mol. Sci. 2022, 23, 12980. [Google Scholar] [CrossRef]
- Colley, H.; Said, Z.; Santocildes-Romero, M.; Baker, S.; D’Apice, K.; Hansen, J.; Madsen, L.S.; Thornhill, M.; Hatton, P.; Murdoch, C. Pre-clinical evaluation of novel mucoadhesive bilayer patches for local delivery of clobetasol-17-propionate to the oral mucosa. Biomaterials 2018, 178, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Nair, V.V.; Cabrera, P.; Ramírez-Lecaros, C.; Jara, M.O.; Brayden, D.J.; Morales, J.O. Buccal delivery of small molecules and biologics: Of mucoadhesive polymers, films, and nanoparticles–an update. Int. J. Pharm. 2023, 636, 122789. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Strandman, S.; Zhu, J.X.; Barralet, J.; Cerruti, M. Genipin-crosslinked catechol-chitosan mucoadhesive hydrogels for buccal drug delivery. Biomaterials 2015, 37, 395–404. [Google Scholar] [CrossRef]
- Anand, R.; Kumar, A. Significant biopolymers and their applications in buccal mediated drug delivery. J. Biomater. Sci. Polym. Ed. 2021, 32, 1203–1218. [Google Scholar] [CrossRef]
- Mura, P.; Maestrelli, F.; Cirri, M.; Mennini, N. Multiple roles of chitosan in mucosal drug delivery: An updated review. Mar. Drugs 2022, 20, 335. [Google Scholar] [CrossRef]
- Kumar, A.; Naik, P.K.; Pradhan, D.; Ghosh, G.; Rath, G. Mucoadhesive formulations: Innovations, merits, drawbacks, and future outlook. Pharm. Dev. Technol. 2020, 25, 797–814. [Google Scholar] [CrossRef]
- Macedo, A.S.; Castro, P.M.; Roque, L.; Thomé, N.G.; Reis, C.P.; Pintado, M.E.; Fonte, P. Novel and revisited approaches in nanoparticle systems for buccal drug delivery. J. Control. Release 2020, 320, 125–141. [Google Scholar] [CrossRef]
- Kragelund, C.; Hansen, C.; Torpet, L.; Nauntofte, B.; Brøsen, K.; Pedersen, A.; Buchwald, C.; Therkildsen, M.; Reibel, J. Expression of two drug-metabolizing cytochrome p450-enzymes in human salivary glands. Oral Dis. 2008, 14, 533–540. [Google Scholar] [CrossRef]
- Cruchley, A.T.; Bergmeier, L.A. Structure and Functions of the Oral Mucosa. In Oral Mucosa in Health and Disease: A Concise Handbook; Bergmeier, L.A., Ed.; Springer: Cham, Switzerland, 2018; pp. 1–18. [Google Scholar]
- Şenel, S. An overview of physical, microbiological and immune barriers of oral mucosa. Int. J. Mol. Sci. 2021, 22, 7821. [Google Scholar] [CrossRef]
- Vielmuth, F. Anatomy of the Oral Mucosa. In Diseases of the Oral Mucosa; Schmidt, E., Ed.; Springer: Cham, Switzerland, 2021; pp. 5–19. [Google Scholar] [CrossRef]
- Groeger, S.; Meyle, J. Oral mucosal epithelial cells. Front. Immunol. 2019, 10, 208. [Google Scholar] [CrossRef]
- Wan, H.; Gadmor, H.; Brown, L. Cell-Cell Interactions in the Oral Mucosa: Tight Junctions and Gap Junctions. In Oral Mucosa in Health and Disease: A Concise Handbook; Bergmeier, L.A., Ed.; Springer: Cham, Switzerland, 2018; pp. 19–30. [Google Scholar] [CrossRef]
- Tsukita, S.; Furuse, M.; Itoh, M. Multifunctional strands in tight junctions. Nat. Rev. Mol. Cell Biol. 2001, 2, 285–293. [Google Scholar] [CrossRef]
- Dejana, E. Endothelial cell–cell junctions: Happy together. Nat. Rev. Mol. Cell Biol. 2004, 5, 261–270. [Google Scholar] [CrossRef]
- Squier, C.A.; Kremer, M.J. Biology of oral mucosa and esophagus. JNCI Monogr. 2001, 2001, 7–15. [Google Scholar] [CrossRef]
- Roy, R.R.; Shimada, K.; Murakami, S.; Hasegawa, H. Contribution of transglutaminases and their substrate proteins to the formation of cornified cell envelope in oral mucosal epithelium. Eur. J. Oral Sci. 2021, 129, e12760. [Google Scholar] [CrossRef]
- Nakamura, T.; Endo, K.-I.; Kinoshita, S. Identification of human oral keratinocyte stem/progenitor cells by neurotrophin receptor p75 and the role of neurotrophin/p75 signaling. Stem Cells 2007, 25, 628–638. [Google Scholar] [CrossRef]
- Évora, A.S.; Adams, M.J.; Johnson, S.A.; Zhang, Z. Corneocytes: Relationship between structural and biomechanical properties. Ski. Pharmacol. Physiol. 2021, 34, 146–161. [Google Scholar] [CrossRef]
- Guo, Y.-G.; Singh, A.P. Emerging strategies for enhancing buccal and sublingual administration of nutraceuticals and pharamaceuticals. J. Drug Deliv. Sci. Technol. 2019, 52, 440–451. [Google Scholar] [CrossRef]
- Kraan, H.; Vrieling, H.; Czerkinsky, C.; Jiskoot, W.; Kersten, G.; Amorij, J.-P. Buccal and sublingual vaccine delivery. J. Control. Release 2014, 190, 580–592. [Google Scholar] [CrossRef]
- Wertz, P.W. Roles of lipids in the permeability barriers of skin and oral mucosa. Int. J. Mol. Sci. 2021, 22, 5229. [Google Scholar] [CrossRef]
- Trincado, V.; Gala, R.P.; Morales, J.O. Buccal and sublingual vaccines: A review on oral mucosal immunization and delivery systems. Vaccines 2021, 9, 1177. [Google Scholar] [CrossRef]
- Pinto, S.; Pintado, M.E.; Sarmento, B. In Vivo, Ex Vivo and In Vitro assessment of buccal permeation of drugs from delivery systems. Expert Opin. Drug Deliv. 2020, 17, 33–48. [Google Scholar] [CrossRef]
- Squier, C.; Rooney, L. The permeability of keratinized and nonkeratinized oral epithelium to lanthanum in vivo. J. Ultrastruct. Res. 1976, 54, 286–295. [Google Scholar] [CrossRef]
- Squier, C. Membrane coating granules in nonkeratinizing oral epithelium. J. Ultrastruct. Res. 1977, 60, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Wertz, P.; Squier, C. Cellular and molecular basis of barrier function in oral epithelium. Crit. Rev. Ther. Drug Carr. Syst. 1991, 8, 237–269. [Google Scholar]
- Squier, C.; Cox, P.; Wertz, P.; Downing, D. The lipid composition of porcine epidermis and oral epithelium. Arch. Oral Biol. 1986, 31, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Squier, C.; Cox, P.; Hall, B. Enhanced penetration of nitrosonornicotine across oral mucosa in the presence of ethanol. J. Oral Pathol. Med. 1986, 15, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Gibbins, H.L.; Proctor, G.B.; Yakubov, G.E.; Wilson, S.; Carpenter, G.H. Siga binding to mucosal surfaces is mediated by mucin-mucin interactions. PLoS ONE 2015, 10, e0119677. [Google Scholar] [CrossRef] [PubMed]
- Taherali, F.; Varum, F.; Basit, A.W. A slippery slope: On the origin, role and physiology of mucus. Adv. Drug Deliv. Rev. 2018, 124, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Bansil, R.; Turner, B.S. The biology of mucus: Composition, synthesis and organization. Adv. Drug Deliv. Rev. 2018, 124, 3–15. [Google Scholar] [CrossRef]
- Bansil, R.; Turner, B.S. Mucin structure, aggregation, physiological functions and biomedical applications. Curr. Opin. Colloid Interface Sci. 2006, 11, 164–170. [Google Scholar] [CrossRef]
- Murgia, X.; Loretz, B.; Hartwig, O.; Hittinger, M.; Lehr, C.-M. The role of mucus on drug transport and its potential to affect therapeutic outcomes. Adv. Drug Deliv. Rev. 2018, 124, 82–97. [Google Scholar] [CrossRef]
- Boegh, M.; Nielsen, H.M. Mucus as a barrier to drug delivery–understanding and mimicking the barrier properties. Basic Clin. Pharmacol. Toxicol. 2015, 116, 179–186. [Google Scholar] [CrossRef]
- Leal, J.; Smyth, H.D.; Ghosh, D. Physicochemical properties of mucus and their impact on transmucosal drug delivery. Int. J. Pharm. 2017, 532, 555–572. [Google Scholar] [CrossRef]
- Perez-Vilar, J.; Hill, R.L. The structure and assembly of secreted mucins* 210. J. Biol. Chem. 1999, 274, 31751–31754. [Google Scholar] [CrossRef]
- Bell, S.L.; Xu, G.; Forstner, J.F. Role of the cystine-knot motif at the c-terminus of rat mucin protein muc2 in dimer formation and secretion. Biochem. J. 2001, 357, 203–209. [Google Scholar] [CrossRef]
- Curnutt, A.; Smith, K.; Darrow, E.; Walters, K.B. Chemical and microstructural characterization of ph and [ca2+] dependent sol-gel transitions in mucin biopolymer. Sci. Rep. 2020, 10, 8760. [Google Scholar] [CrossRef]
- Filatova, L.; Emelianov, G.; Balabushevich, N.; Klyachko, N. Supramolecular assemblies of mucin and lysozyme: Formation and physicochemical characterization. Process Biochem. 2022, 113, 97–106. [Google Scholar] [CrossRef]
- Khutoryanskiy, V.V. Advances in mucoadhesion and mucoadhesive polymers. Macromol. Biosci. 2011, 11, 748–764. [Google Scholar] [CrossRef]
- Mansuri, S.; Kesharwani, P.; Jain, K.; Tekade, R.K.; Jain, N. Mucoadhesion: A promising approach in drug delivery system. React. Funct. Polym. 2016, 100, 151–172. [Google Scholar] [CrossRef]
- Yaqoob, M.; Jalil, A.; Bernkop-Schnürch, A. Mucoadhesive Polymers: Gateway to Innovative Drug Delivery. In Modeling and Control of Drug Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2021; pp. 351–383. [Google Scholar]
- Smart, J.D. Theories of Mucoadhesion. In Mucoadhesive Materials and Drug Delivery Systems; Khutoryanskiy, V.V., Ed.; Wiley VCH Verlag: Weinheim, Germany, 2014; pp. 159–174. [Google Scholar] [CrossRef]
- Anil, A.; Sudheer, P. Mucoadhesive polymers: A review. J. Pharm. Res. 2018, 17, 47–55. [Google Scholar]
- Bayer, I.S. Recent advances in mucoadhesive interface materials, mucoadhesion characterization, and technologies. Adv. Mater. Interfaces 2022, 9, 2200211. [Google Scholar] [CrossRef]
- Salamat-Miller, N.; Chittchang, M.; Johnston, T.P. The use of mucoadhesive polymers in buccal drug delivery. Adv. Drug Deliv. Rev. 2005, 57, 1666–1691. [Google Scholar] [CrossRef]
- Smart, J.D. The basics and underlying mechanisms of mucoadhesion. Adv. Drug Deliv. Rev. 2005, 57, 1556–1568. [Google Scholar] [CrossRef]
- Brannigan, R.P.; Khutoryanskiy, V.V. Progress and current trends in the synthesis of novel polymers with enhanced mucoadhesive properties. Macromol. Biosci. 2019, 19, 1900194. [Google Scholar] [CrossRef]
- Peppas, N.A.; Sahlin, J.J. Hydrogels as mucoadhesive and bioadhesive materials: A review. Biomaterials 1996, 17, 1553–1561. [Google Scholar] [CrossRef]
- Khare, A.R.; Peppas, N.A.; Massimo, G.; Colombo, P. Measurement of the swelling force in ionic polymeric networks i. Effect of ph and ionic content. J. Control. Release 1992, 22, 239–244. [Google Scholar] [CrossRef]
- Lehr, C.-M.; Bouwstra, J.A.; Boddé, H.E.; Junginger, H.E. A surface energy analysis of mucoadhesion: Contact angle measurements on polycarbophil and pig intestinal mucosa in physiologically relevant fluids. Pharm. Res. 1992, 9, 70–75. [Google Scholar] [CrossRef]
- Batchelor, H.; Banning, D.; Dettmar, P.; Hampson, F.; Jolliffe, I.; Craig, D. An in vitro mucosal model for prediction of the bioadhesion of alginate solutions to the oesophagus. Int. J. Pharm. 2002, 238, 123–132. [Google Scholar] [CrossRef]
- Dubashynskaya, N.V.; Bokatyi, A.N.; Skorik, Y.A. Dexamethasone conjugates: Synthetic approaches and medical prospects. Biomedicines 2021, 9, 341. [Google Scholar] [CrossRef]
- Patel, D.; Smith, A.; Grist, N.; Barnett, P.; Smart, J. An In Vitro mucosal model predictive of bioadhesive agents in the oral cavity. J. Control. Release 1999, 61, 175–183. [Google Scholar] [CrossRef]
- Kockisch, S.; Rees, G.D.; Young, S.A.; Tsibouklis, J.; Smart, J.D. A direct-staining method to evaluate the mucoadhesion of polymers from aqueous dispersion. J. Control. Release 2001, 77, 1–6. [Google Scholar] [CrossRef]
- Bassi da Silva, J.; Ferreira, S.B.d.S.; de Freitas, O.; Bruschi, M.L. A critical review about methodologies for the analysis of mucoadhesive properties of drug delivery systems. Drug Dev. Ind. Pharm. 2017, 43, 1053–1070. [Google Scholar] [CrossRef]
- Djekic, L.; Martinovic, M. In Vitro, Ex Vivo and In Vivo Methods for Characterization of Bioadhesiveness of Drug Delivery Systems. In Bioadhesives in Drug Delivery; Mittal, K.L., Bakshi, I.S., Narang, J.K., Eds.; Wiley VCH Verlag: Weinheim, Germany, 2020; pp. 57–98. [Google Scholar] [CrossRef]
- Griffiths, P.C.; Cattoz, B.; Ibrahim, M.S.; Anuonye, J.C. Probing the interaction of nanoparticles with mucin for drug delivery applications using dynamic light scattering. Eur. J. Pharm. Biopharm. 2015, 97, 218–222. [Google Scholar] [CrossRef]
- Hejjaji, E.M.; Smith, A.M.; Morris, G.A. Evaluation of the mucoadhesive properties of chitosan nanoparticles prepared using different chitosan to tripolyphosphate (cs: Tpp) ratios. Int. J. Biol. Macromol. 2018, 120, 1610–1617. [Google Scholar] [CrossRef]
- Yamabayashi, S. Periodic acid—Schiff—Alcian blue: A method for the differential staining of glycoproteins. Histochem. J. 1987, 19, 565–571. [Google Scholar] [CrossRef]
- Kim, K.; Kim, K.; Ryu, J.H.; Lee, H. Chitosan-catechol: A polymer with long-lasting mucoadhesive properties. Biomaterials 2015, 52, 161–170. [Google Scholar] [CrossRef]
- Madsen, F.; Eberth, K.; Smart, J.D. A rheological examination of the mucoadhesive/mucus interaction: The effect of mucoadhesive type and concentration. J. Control. Release 1998, 50, 167–178. [Google Scholar] [CrossRef]
- Patel, D.; Smith, J.R.; Smith, A.W.; Grist, N.; Barnett, P.; Smart, J.D. An atomic force microscopy investigation of bioadhesive polymer adsorption onto human buccal cells. Int. J. Pharm. 2000, 200, 271–277. [Google Scholar] [CrossRef]
- Sajomsang, W.; Nuchuchua, O.; Gonil, P.; Saesoo, S.; Sramala, I.; Soottitantawat, A.; Puttipipatkhachorn, S.; Ruktanonchai, U.R. Water-soluble β-cyclodextrin grafted with chitosan and its inclusion complex as a mucoadhesive eugenol carrier. Carbohydr. Polym. 2012, 89, 623–631. [Google Scholar] [CrossRef]
- Amézqueta, S.; Subirats, X.; Fuguet, E.; Rosés, M.; Ràfols, C. Octanol-Water Partition Constant. In Handbooks in Separation Science, Liquid-Phase Extraction; Poole, C.F., Ed.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 183–208. [Google Scholar] [CrossRef]
- Wanasathop, A.; Patel, P.B.; Choi, H.A.; Li, S.K. Permeability of buccal mucosa. Pharmaceutics 2021, 13, 1814. [Google Scholar] [CrossRef]
- He, S.; Mu, H. Microenvironmental pH modification in buccal/sublingual dosage forms for systemic drug delivery. Pharmaceutics 2023, 15, 637. [Google Scholar] [CrossRef]
- Madhav, N.S.; Shakya, A.K.; Shakya, P.; Singh, K. Orotransmucosal drug delivery systems: A review. J. Control. Release 2009, 140, 2–11. [Google Scholar] [CrossRef]
- Padhye, T.; Maravajjala, K.S.; Swetha, K.L.; Sharma, S.; Roy, A. A comprehensive review of the strategies to improve oral drug absorption with special emphasis on the cellular and molecular mechanisms. J. Drug Deliv. Sci. Technol. 2021, 61, 102178. [Google Scholar] [CrossRef]
- Sattar, M.; Sayed, O.M.; Lane, M.E. Oral transmucosal drug delivery–current status and future prospects. Int. J. Pharm. 2014, 471, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Morsi, N.M.; Abdelbary, G.A.; Elshafeey, A.H.; Ahmed, M.A. Engineering of a novel optimized platform for sublingual delivery with novel characterization tools: In vitro evaluation and in vivo pharmacokinetics study in human. Drug Deliv. 2017, 24, 918–931. [Google Scholar] [CrossRef] [PubMed]
- Pushpamalar, J.; Veeramachineni, A.K.; Owh, C.; Loh, X.J. Biodegradable polysaccharides for controlled drug delivery. ChemPlusChem 2016, 81, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.K.; Xu, Y.; Worsley, A.; Wong, I.C. Oral transmucosal drug delivery for pediatric use. Adv. Drug Deliv. Rev. 2014, 73, 50–62. [Google Scholar] [CrossRef]
- Williams, A.C.; Barry, B.W. Penetration enhancers. Adv. Drug Deliv. Rev. 2012, 64, 128–137. [Google Scholar] [CrossRef]
- He, F.; Liu, W.; Zheng, S.; Zhou, L.; Ye, B.; Qi, Z. Ion transport through dimethyl sulfoxide (DMSO) induced transient water pores in cell membranes. Mol. Membr. Biol. 2012, 29, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Lundborg, M.; Wennberg, C.L.; Narangifard, A.; Lindahl, E.; Norlén, L. Predicting drug permeability through skin using molecular dynamics simulation. J. Control. Release 2018, 283, 269–279. [Google Scholar] [CrossRef]
- Sohi, H.; Ahuja, A.; Ahmad, F.J.; Khar, R.K. Critical evaluation of permeation enhancers for oral mucosal drug delivery. Drug Dev. Ind. Pharm. 2010, 36, 254–282. [Google Scholar] [CrossRef]
- Lee, V.H. Protease inhibitors and penetration enhancers as approaches to modify peptide absorption. J. Control. Release 1990, 13, 213–223. [Google Scholar] [CrossRef]
- Renukuntla, J.; Vadlapudi, A.D.; Patel, A.; Boddu, S.H.; Mitra, A.K. Approaches for enhancing oral bioavailability of peptides and proteins. Int. J. Pharm. 2013, 447, 75–93. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Bahumik, A. Protein and peptide drug delivery: A fundamental novel approach and future perspective. World J. Pharm. Pharm. Sci. 2016, 5, 763–776. [Google Scholar]
- Caon, T.; Jin, L.; Simões, C.M.; Norton, R.S.; Nicolazzo, J.A. Enhancing the buccal mucosal delivery of peptide and protein therapeutics. Pharm. Res. 2015, 32, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Fantini, A.; Giulio, L.; Delledonne, A.; Pescina, S.; Sissa, C.; Nicoli, S.; Santi, P.; Padula, C. Buccal permeation of polysaccharide high molecular weight compounds: Effect of chemical permeation enhancers. Pharmaceutics 2022, 15, 129. [Google Scholar] [CrossRef] [PubMed]
- Rai, V.; Tan, H.S.; Michniak-Kohn, B. Effect of surfactants and pH on naltrexone (NTX) permeation across buccal mucosa. Int. J. Pharm. 2011, 411, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Padula, C.; Pescina, S.; Nicoli, S.; Santi, P. New insights on the mechanism of fatty acids as buccal permeation enhancers. Pharmaceutics 2018, 10, 201. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Islam, T.; Nurunnabi, M. Mucoadhesive carriers for oral drug delivery. J. Control. Release 2022, 351, 504–559. [Google Scholar] [CrossRef] [PubMed]
- Rambharose, S.; Ojewole, E.; Mackraj, I.; Govender, T. Comparative buccal permeability enhancement of didanosine and tenofovir by potential multifunctional polymeric excipients and their effects on porcine buccal histology. Pharm. Dev. Technol. 2014, 19, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Park, J.H.; Robinson, J.R. Bioadhesive-based dosage forms: The next generation. J. Pharm. Sci. 2000, 89, 850–866. [Google Scholar] [CrossRef] [PubMed]
- Duceac, I.A.; Coseri, S. Biopolymers and their derivatives: Key components of advanced biomedical technologies. Biotechnol. Adv. 2022, 61, 108056. [Google Scholar] [CrossRef]
- Jabeen, N.; Atif, M. Polysaccharides based biopolymers for biomedical applications: A review. Polym. Adv. Technol. 2024, 35, e6203. [Google Scholar] [CrossRef]
- Raghav, N.; Vashisth, C.; Mor, N.; Arya, P.; Sharma, M.R.; Kaur, R.; Bhatti, S.P.; Kennedy, J.F. Recent advances in cellulose, pectin, carrageenan and alginate-based oral drug delivery systems. Int. J. Biol. Macromol. 2023, 244, 125357. [Google Scholar] [CrossRef]
- Szekalska, M.; Wróblewska, M.; Trofimiuk, M.; Basa, A.; Winnicka, K. Alginate oligosaccharides affect mechanical properties and antifungal activity of alginate buccal films with posaconazole. Mar. Drugs 2019, 17, 692. [Google Scholar] [CrossRef]
- Abo-shady, A.Z.; Elkammar, H.; Elwazzan, V.S.; Nasr, M. Formulation and clinical evaluation of mucoadhesive buccal films containing hyaluronic acid for treatment of aphthous ulcer. J. Drug Deliv. Sci. Technol. 2020, 55, 101442. [Google Scholar] [CrossRef]
- Haggag, Y.A.; Abd Elrahman, A.A.; Ulber, R.; Zayed, A. Fucoidan in pharmaceutical formulations: A comprehensive review for smart drug delivery systems. Mar. Drugs 2023, 21, 112. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xue, C.; Mao, X. Chitosan: Structural modification, biological activity and application. Int. J. Biol. Macromol. 2020, 164, 4532–4546. [Google Scholar] [CrossRef]
- Ardean, C.; Davidescu, C.M.; Nemeş, N.S.; Negrea, A.; Ciopec, M.; Duteanu, N.; Negrea, P.; Duda-Seiman, D.; Muntean, D. Antimicrobial activities of chitosan derivatives. Pharmaceutics 2021, 13, 1639. [Google Scholar] [CrossRef] [PubMed]
- Ways, T.M.M.; Lau, W.M.; Khutoryanskiy, V.V. Chitosan and its derivatives for application in mucoadhesive drug delivery systems. Polymers 2018, 10, 267. [Google Scholar] [CrossRef] [PubMed]
- Hasnain, M.S.; Nayak, A.K. Chitosan as Mucoadhesive Polymer in Drug Delivery. In Chitosan in Drug Delivery; Elsevier: Amsterdam, The Netherlands, 2022; pp. 225–246. [Google Scholar]
- Kumar, A.; Sahu, R.K.; Chameettachal, S.; Pati, F.; Kumar, A. Fabrication and analysis of chitosan oligosaccharide based mucoadhesive patch for oromucosal drug delivery. Drug Dev. Ind. Pharm. 2022, 48, 602–610. [Google Scholar] [CrossRef]
- Cazorla-Luna, R.; Martín-Illana, A.; Notario-Pérez, F.; Ruiz-Caro, R.; Veiga, M.-D. Naturally occurring polyelectrolytes and their use for the development of complex-based mucoadhesive drug delivery systems: An overview. Polymers 2021, 13, 2241. [Google Scholar] [CrossRef]
- Manna, S.; Seth, A.; Gupta, P.; Nandi, G.; Dutta, R.; Jana, S.; Jana, S. Chitosan derivatives as carriers for drug delivery and biomedical applications. ACS Biomater. Sci. Eng. 2023, 9, 2181–2202. [Google Scholar] [CrossRef] [PubMed]
- Freitas, E.D.; Moura, C.F., Jr.; Kerwald, J.; Beppu, M.M. An overview of current knowledge on the properties, synthesis and applications of quaternary chitosan derivatives. Polymers 2020, 12, 2878. [Google Scholar] [CrossRef]
- Piras, A.M.; Esin, S.; Benedetti, A.; Maisetta, G.; Fabiano, A.; Zambito, Y.; Batoni, G. Antibacterial, antibiofilm, and antiadhesive properties of different quaternized chitosan derivatives. Int. J. Mol. Sci. 2019, 20, 6297. [Google Scholar] [CrossRef]
- Dubashynskaya, N.V.; Bokatyi, A.N.; Trulioff, A.S.; Rubinstein, A.A.; Kudryavtsev, I.V.; Skorik, Y.A. Development and bioactivity of zinc sulfate cross-linked polysaccharide delivery system of dexamethasone phosphate. Pharmaceutics 2023, 15, 2396. [Google Scholar] [CrossRef]
- Netsomboon, K.; Jalil, A.; Laffleur, F.; Hupfauf, A.; Gust, R.; Bernkop-Schnürch, A. Thiolated chitosans: Are cys-cys ligands key to the next generation? Carbohydr. Polym. 2020, 242, 116395. [Google Scholar] [CrossRef] [PubMed]
- Tekade, M.; Maheshwari, N.; Youngren-Ortiz, S.R.; Pandey, V.; Chourasiya, Y.; Soni, V.; Deb, P.K.; Sharma, M.C. Thiolated-Chitosan: A Novel Mucoadhesive Polymer for Better-Targeted Drug Delivery. In Biomaterials and Bionanotechnology; Elsevier: Amsterdam, The Netherlands, 2019; pp. 459–493. [Google Scholar]
- Sosnik, A.; das Neves, J.; Sarmento, B. Mucoadhesive polymers in the design of nano-drug delivery systems for administration by non-parenteral routes: A review. Prog. Polym. Sci. 2014, 39, 2030–2075. [Google Scholar] [CrossRef]
- Carmen Chifiriuc, M.; Mihai Grumezescu, A.; Grumezescu, V.; Bezirtzoglou, E.; Lazar, V.; Bolocan, A. Biomedical applications of natural polymers for drug delivery. Curr. Org. Chem. 2014, 18, 152–164. [Google Scholar] [CrossRef]
- Yermak, I.M.; Davydova, V.N.; Volod’ko, A.V. Mucoadhesive marine polysaccharides. Mar. Drugs 2022, 20, 522. [Google Scholar] [CrossRef]
- Pamlényi, K.; Kristó, K.; Jójárt-Laczkovich, O.; Regdon, G., Jr. Formulation and optimization of sodium alginate polymer film as a buccal mucoadhesive drug delivery system containing cetirizine dihydrochloride. Pharmaceutics 2021, 13, 619. [Google Scholar] [CrossRef]
- Prezotti, F.G.; Siedle, I.; Boni, F.I.; Chorilli, M.; Müller, I.; Cury, B.S.F. Mucoadhesive films based on gellan gum/pectin blends as potential platform for buccal drug delivery. Pharm. Dev. Technol. 2020, 25, 159–167. [Google Scholar] [CrossRef]
- Pacheco-Quito, E.-M.; Ruiz-Caro, R.; Veiga, M.-D. Carrageenan: Drug delivery systems and other biomedical applications. Mar. Drugs 2020, 18, 583. [Google Scholar] [CrossRef] [PubMed]
- Yermak, I.M.; Davydova, V.N.; Kravchenko, A.O.; Chistyulin, D.A.; Pimenova, E.A.; Glazunov, V.P. Mucoadhesive properties of sulphated polysaccharides carrageenans from red seaweed families gigartinaceae and tichocarpaceae. Int. J. Biol. Macromol. 2020, 142, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Solanki, P.; Ansari, D.; Sultana, Y. Nanostructured Carrageenan as Drug Carrier. In Nanoengineering of Biomaterials; Jana, S., Jana, S., Eds.; Wiley VCH Verlag: Weinheim, Germany, 2022; pp. 523–542. [Google Scholar] [CrossRef]
- Fauzi, M.A.R.D.; Pudjiastuti, P.; Wibowo, A.C.; Hendradi, E. Preparation, properties and potential of carrageenan-based hard capsules for replacing gelatine: A review. Polymers 2021, 13, 2666. [Google Scholar] [CrossRef] [PubMed]
- Kianfar, F.; Antonijevic, M.; Chowdhry, B.; Boateng, J.S. Lyophilized wafers comprising carrageenan and pluronic acid for buccal drug delivery using model soluble and insoluble drugs. Colloids Surf. B Biointerfaces 2013, 103, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Elbanna, S.A.; Ebada, H.M.; Abdallah, O.Y.; Essawy, M.M.; Abdelhamid, H.M.; Barakat, H.S. Novel tetrahydrocurcumin integrated mucoadhesive nanocomposite κ-carrageenan/xanthan gum sponges: A strategy for effective local treatment of oral cancerous and precancerous lesions. Drug Deliv. 2023, 30, 2254530. [Google Scholar] [CrossRef] [PubMed]
- Dubashynskaya, N.V.; Gasilova, E.R.; Skorik, Y.A. Nano-sized fucoidan interpolyelectrolyte complexes: Recent advances in design and prospects for biomedical applications. Int. J. Mol. Sci. 2023, 24, 2615. [Google Scholar] [CrossRef] [PubMed]
- Man, E.; Hoskins, C. Towards advanced wound regeneration. Eur. J. Pharm. Sci. 2020, 149, 105360. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Hao, Y.; Wang, D.; Huang, H.; Guo, F.; Sun, Z.; Shen, P.; Sui, K.; Yuan, C.; Zhou, Q. Preparation of triamcinolone acetonide-loaded chitosan/fucoidan hydrogel and its potential application as an oral mucosa patch. Carbohydr. Polym. 2021, 272, 118493. [Google Scholar] [CrossRef] [PubMed]
- Dou, X.; Li, G.; Wang, S.; Shao, D.; Wang, D.; Deng, X.; Zhu, Y.; Gao, P.; Liu, J.; Deng, N. Probiotic-loaded calcium alginate/fucoidan hydrogels for promoting oral ulcer healing. Int. J. Biol. Macromol. 2023, 244, 125273. [Google Scholar] [CrossRef]
- Meher, J.G.; Tarai, M.; Yadav, N.P.; Patnaik, A.; Mishra, P.; Yadav, K.S. Development and characterization of cellulose–polymethacrylate mucoadhesive film for buccal delivery of carvedilol. Carbohydr. Polym. 2013, 96, 172–180. [Google Scholar] [CrossRef]
- Surendranath, M.; Rekha, M.; Parameswaran, R. Recent advances in functionally modified polymers for mucoadhesive drug delivery. J. Mater. Chem. B 2022, 10, 5913–5924. [Google Scholar] [CrossRef] [PubMed]
- Kali, G.; Özkahraman, B.; Laffleur, F.; Knoll, P.; Wibel, R.; Zoller, K.; Bernkop-Schnurch, A. Thiolated cellulose: A dual-acting mucoadhesive and permeation-enhancing polymer. Biomacromolecules 2023, 24, 4880–4889. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.A.V.T.; Cesar, A.L.A.; Garcia, C.F.; Faraco, A.A.G. Starch Applied for Pharmaceutical Use. In Starch Industries: Processes and Innovative Products in Food and Non-Food Uses; Elsevier: Amsterdam, The Netherlands, 2024; pp. 349–376. [Google Scholar]
- Elgaied-Lamouchi, D.; Descamps, N.; Lefevre, P.; Rambur, I.; Pierquin, J.-Y.; Siepmann, F.; Siepmann, J.; Muschert, S. Starch-based controlled release matrix tablets: Impact of the type of starch. J. Drug Deliv. Sci. Technol. 2021, 61, 102152. [Google Scholar] [CrossRef]
- Song, Y.; Wang, Y.; Thakur, R.; Meidan, V.M.; Michniak, B. Mucosal drug delivery: Membranes, methodologies, and applications. Crit. Rev. Ther. Drug Carr. Syst. 2004, 21, 195–256. [Google Scholar] [CrossRef] [PubMed]
- Mulhbacher, J.; Ispas-Szabo, P.; Ouellet, M.; Alex, S.; Mateescu, M.A. Mucoadhesive properties of cross-linked high amylose starch derivatives. Int. J. Biol. Macromol. 2006, 40, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Jelkmann, M.; Leichner, C.; Menzel, C.; Kreb, V.; Bernkop-Schnürch, A. Cationic starch derivatives as mucoadhesive and soluble excipients in drug delivery. Int. J. Pharm. 2019, 570, 118664. [Google Scholar] [CrossRef]
- Kudaibergenov, S.E.; Nuraje, N. Intra-and interpolyelectrolyte complexes of polyampholytes. Polymers 2018, 10, 1146. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Filippov, S.K.; Williams, A.C.; Khutoryanskiy, V.V. On the mucoadhesive properties of synthetic and natural polyampholytes. J. Colloid Interface Sci. 2024, 659, 849–858. [Google Scholar] [CrossRef]
- Yang, X.; Robinson, J. Bioadhesion in Mucosal Drug Delivery; Academic Press: San Diego, CA, USA, 1998; pp. 135–192. [Google Scholar]
- Wang, J.; Tauchi, Y.; Deguchi, Y.; Morimoto, K.; Tabata, Y.; Ikada, Y. Positively charged gelatin microspheres as gastric mucoadhesive drug delivery system for eradication of h. Pylori. Drug Deliv. 2000, 7, 237–243. [Google Scholar]
- Wang, J.; Tabata, Y.; Bi, D.; Morimoto, K. Evaluation of gastric mucoadhesive properties of aminated gelatin microspheres. J. Control. Release 2001, 73, 223–231. [Google Scholar] [CrossRef]
- Puri, V.; Sharma, A.; Kumar, P.; Singh, I. Thiolation of biopolymers for developing drug delivery systems with enhanced mechanical and mucoadhesive properties: A review. Polymers 2020, 12, 1803. [Google Scholar] [CrossRef]
- Mfoafo, K.; Mittal, R.; Eshraghi, A.; Omidi, Y.; Omidian, H. Thiolated polymers: An overview of mucoadhesive properties and their potential in drug delivery via mucosal tissues. J. Drug Deliv. Sci. Technol. 2023, 85, 104596. [Google Scholar] [CrossRef]
- Kali, G.; Fürst, A.; Efiana, N.A.; Dizdarević, A.; Bernkop-Schnürch, A. Intraoral drug delivery: Highly thiolated κ-carrageenan as mucoadhesive excipient. Pharmaceutics 2023, 15, 1993. [Google Scholar] [CrossRef] [PubMed]
- Rahbarian, M.; Mortazavian, E.; Dorkoosh, F.A.; Tehrani, M.R. Preparation, evaluation and optimization of nanoparticles composed of thiolated triethyl chitosan: A potential approach for buccal delivery of insulin. J. Drug Deliv. Sci. Technol. 2018, 44, 254–263. [Google Scholar] [CrossRef]
- S Boateng, J.; C Mitchell, J.; Pawar, H.; Ayensu, I. Functional characterisation and permeation studies of lyophilised thiolated chitosan xerogels for buccal delivery of insulin. Protein Pept. Lett. 2014, 21, 1163–1175. [Google Scholar] [CrossRef] [PubMed]
- Mortazavian, E.; Dorkoosh, F.A.; Rafiee-Tehrani, M. Design, characterization and ex vivo evaluation of chitosan film integrating of insulin nanoparticles composed of thiolated chitosan derivative for buccal delivery of insulin. Drug Dev. Ind. Pharm. 2014, 40, 691–698. [Google Scholar] [CrossRef]
- Özbaş, Z.; Özkahraman, B.; Akgüner, Z.P.; Bal-Öztürk, A. Evaluation of modified pectin/alginate buccal patches with enhanced mucoadhesive properties for drug release systems: In-vitro and ex-vivo study. J. Drug Deliv. Sci. Technol. 2022, 67, 102991. [Google Scholar] [CrossRef]
- Özkahraman, B.; Özbaş, Z.; Yaşayan, G.; Akgüner, Z.P.; Yarımcan, F.; Alarçin, E.; Bal-Öztürk, A. Development of mucoadhesive modified kappa-carrageenan/pectin patches for controlled delivery of drug in the buccal cavity. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Pei, X.; Duan, L.; Zhu, Z.; Liu, Y.; Chen, J.; Chen, T.; Ji, P.; Wan, Q.; Wang, J. A mussel-inspired film for adhesion to wet buccal tissue and efficient buccal drug delivery. Nat. Commun. 2021, 12, 1689. [Google Scholar] [CrossRef]
- Pathak, K. Marine bioadhesives: Opportunities and challenges. Ther. Deliv. 2019, 10, 749–751. [Google Scholar] [CrossRef]
- Xu, J.; Soliman, G.M.; Barralet, J.; Cerruti, M. Mollusk glue inspired mucoadhesives for biomedical applications. Langmuir 2012, 28, 14010–14017. [Google Scholar] [CrossRef]
- Liu, F.; Liu, X.; Chen, F.; Fu, Q. Mussel-inspired chemistry: A promising strategy for natural polysaccharides in biomedical applications. Prog. Polym. Sci. 2021, 123, 101472. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, R.; Sun, Z.; Zhu, X.; Zhao, Q.; Zhang, T.; Cholewinski, A.; Yang, F.K.; Zhao, B.; Pinnaratip, R. Catechol-functionalized hydrogels: Biomimetic design, adhesion mechanism, and biomedical applications. Chem. Soc. Rev. 2020, 49, 433–464. [Google Scholar] [CrossRef]
- Petrone, L.; Kumar, A.; Sutanto, C.N.; Patil, N.J.; Kannan, S.; Palaniappan, A.; Amini, S.; Zappone, B.; Verma, C.; Miserez, A. Mussel adhesion is dictated by time-regulated secretion and molecular conformation of mussel adhesive proteins. Nat. Commun. 2015, 6, 8737. [Google Scholar] [CrossRef]
- Farsad, N.; Sone, E.D. Zebra mussel adhesion: Structure of the byssal adhesive apparatus in the freshwater mussel, dreissena polymorpha. J. Struct. Biol. 2012, 177, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.P.; Messersmith, P.B.; Israelachvili, J.N.; Waite, J.H. Mussel-inspired adhesives and coatings. Annu. Rev. Mater. Res. 2011, 41, 99–132. [Google Scholar] [CrossRef]
- Mancebo Aracil, J.; Nador, F.G.; Busque, F.; Ruiz Molina, D. The chemistry behind catechol-based adhesion. Angew. Chem. Int. Ed. 2019, 58, 696–714. [Google Scholar]
- Mian, S.A.; Khan, Y.; Ahmad, U.; Khan, M.A.; Rahman, G.; Ali, S. Investigating the adsorption mechanism of glycine in comparison with catechol on cristobalite surface using density functional theory for bio-adhesive materials. RSC Adv. 2016, 6, 114313–114319. [Google Scholar] [CrossRef]
- Ma, Y.; Cao, J.; Li, S.; Wang, L.; Meng, Y.; Chen, Y. Nature-inspired wet drug delivery platforms. Small Methods 2024, 2301726. [Google Scholar] [CrossRef]
- Lee, H.; Lee, B.P.; Messersmith, P.B. A reversible wet/dry adhesive inspired by mussels and geckos. Nature 2007, 448, 338–341. [Google Scholar] [CrossRef]
- Xu, Z. Mechanics of metal-catecholate complexes: The roles of coordination state and metal types. Sci. Rep. 2013, 3, 2914. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Yan, J.; Liu, C.; Zhang, J.; Wang, H.; Gao, X.; Yan, H.; Niu, B.; Li, W. Preparation and characterization of catechol-grafted chitosan/gelatin/modified chitosan-agnp blend films. Carbohydr. Polym. 2020, 247, 116643. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wen, J.; Qin, M.; Cao, Y.; Ma, H.; Wang, W. Single-molecule mechanics of catechol-iron coordination bonds. ACS Biomater. Sci. Eng. 2017, 3, 979–989. [Google Scholar] [CrossRef]
- Zhou, H.R.; Huang, J.; Chen, M.; Li, Y.; Yuan, M.; Yang, H. Effect of metal ions with reducing properties on hydrogels containing catechol groups. Colloids Surf. A Physicochem. Eng. Asp. 2021, 631, 127657. [Google Scholar] [CrossRef]
- Lee, H.; Dellatore, S.M.; Miller, W.M.; Messersmith, P.B. Mussel-inspired surface chemistry for multifunctional coatings. science 2007, 318, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Gwak, M.A.; Hong, B.M.; Seok, J.M.; Park, S.A.; Park, W.H. Effect of tannic acid on the mechanical and adhesive properties of catechol-modified hyaluronic acid hydrogels. Int. J. Biol. Macromol. 2021, 191, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.; Kim, K.; Shim, W.; Yang, J.W.; Lee, H. Tannic acid as a degradable mucoadhesive compound. ACS Biomater. Sci. Eng. 2016, 2, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Chung, H.J.; Yeo, S.; Ahn, C.-H.; Lee, H.; Messersmith, P.B.; Park, T.G. Thermo-sensitive, injectable, and tissue adhesive sol–gel transition hyaluronic acid/pluronic composite hydrogels prepared from bio-inspired catechol-thiol reaction. Soft Matter 2010, 6, 977–983. [Google Scholar] [CrossRef]
- Bastos, F.; Pinto, A.C.; Nunes, A.; Simoes, S. Oromucosal products–market landscape and innovative technologies: A review. J. Control. Release 2022, 348, 305–320. [Google Scholar] [CrossRef]
- Desai, D.D.; Manikkath, J.; Lad, H.; Kulkarni, M.; Manikkath, A.; Radhakrishnan, R. Nanotechnology-based mucoadhesive and mucus-penetrating drug-delivery systems for transbuccal drug delivery. Nanomedicine 2023, 18, 1495–1514. [Google Scholar] [CrossRef]
- Chen, G.; Bunt, C.; Wen, J. Mucoadhesive polymers-based film as a carrier system for sublingual delivery of glutathione. J. Pharm. Pharmacol. 2015, 67, 26–34. [Google Scholar] [CrossRef]
- Bruschi, M.L.; de Souza Ferreira, S.B.; da Silva, J.B. Mucoadhesive and Mucus-Penetrating Polymers for Drug Delivery. In Nanotechnology for Oral Drug Delivery; Elsevier: Amsterdam, The Netherlands, 2020; pp. 77–141. [Google Scholar]
- Kutscher, A.H.; Zegarelli, E.V.; Beube, F.E.; Chilton, N.W.; Berman, C.; Mercadante, J.L.; Stern, I.B.; Roland, N. A new vehicle (orabase) for the application of drugs to the oral mucous membranes. Oral Surg. Oral Med. Oral Pathol. 1959, 12, 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Rathore, A.; Sharma, S.; Sadhu, V.; Reddy, K.R.; Kulkarni, R.V. Recent Progress in Mucoadhesive Polymers for Buccal Drug Delivery Applications. In Nanomaterials in Diagnostic Tools and Devices; Kanchi, S., Sharma, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 213–240. [Google Scholar] [CrossRef]
- Preis, M.; Woertz, C.; Kleinebudde, P.; Breitkreutz, J. Oromucosal film preparations: Classification and characterization methods. Expert Opin. Drug Deliv. 2013, 10, 1303–1317. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, N.; Aslam, S. Recent advancements and patents on buccal drug delivery systems: A comprehensive review. Recent Pat. Nanotechnol. 2022, 16, 308–325. [Google Scholar] [CrossRef]
- Lindert, S.; Breitkreutz, J. Oromucosal multilayer films for tailor-made, controlled drug delivery. Expert Opin. Drug Deliv. 2017, 14, 1265–1279. [Google Scholar] [CrossRef]
- Paderni, C.; Compilato, D.; Giannola, L.I.; Campisi, G. Oral local drug delivery and new perspectives in oral drug formulation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, e25–e34. [Google Scholar] [CrossRef]
- Owji, N.; Mandakhbayar, N.; Gregory, D.A.; Marcello, E.; Kim, H.-W.; Roy, I.; Knowles, J.C. Mussel inspired chemistry and bacteria derived polymers for oral mucosal adhesion and drug delivery. Front. Bioeng. Biotechnol. 2021, 9, 663764. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Moghadam, R.; Mehryab, F.; Torshabi, M.; Haeri, A. Applications of novel and nanostructured drug delivery systems for the treatment of oral cavity diseases. Clin. Ther. 2021, 43, e377–e402. [Google Scholar] [CrossRef]
- Kesharwani, P.; Tekade, R.K.; Jain, N.K. Generation dependent cancer targeting potential of poly (propyleneimine) dendrimer. Biomaterials 2014, 35, 5539–5548. [Google Scholar] [CrossRef]
- Tonglairoum, P.; Ngawhirunpat, T.; Rojanarata, T.; Panomsuk, S.; Kaomongkolgit, R.; Opanasopit, P. Fabrication of mucoadhesive chitosan coated polyvinylpyrrolidone/cyclodextrin/clotrimazole sandwich patches for oral candidiasis. Carbohydr. Polym. 2015, 132, 173–179. [Google Scholar] [CrossRef]
- Dodero, A.; Alloisio, M.; Castellano, M.; Vicini, S. Multilayer alginate–polycaprolactone electrospun membranes as skin wound patches with drug delivery abilities. ACS Appl. Mater. Interfaces 2020, 12, 31162–31171. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, P.; Jahanban-Esfahlan, A.; Ahmadi, A.; Tabibiazar, M.; Mohammadifar, M. Development of ethyl cellulose-based formulations: A perspective on the novel technical methods. Food Rev. Int. 2022, 38, 685–732. [Google Scholar] [CrossRef]
- Singh, J.; Tan, N.C.; Mahadevaswamy, U.R.; Chanchareonsook, N.; Steele, T.W.; Lim, S. Bacterial cellulose adhesive composites for oral cavity applications. Carbohydr. Polym. 2021, 274, 118403. [Google Scholar] [CrossRef]
- Heggset, E.B.; Strand, B.L.; Sundby, K.W.; Simon, S.; Chinga-Carrasco, G.; Syverud, K. Viscoelastic properties of nanocellulose based inks for 3d printing and mechanical properties of cnf/alginate biocomposite gels. Cellulose 2019, 26, 581–595. [Google Scholar] [CrossRef]
- Siqueira, G.; Kokkinis, D.; Libanori, R.; Hausmann, M.K.; Gladman, A.S.; Neels, A.; Tingaut, P.; Zimmermann, T.; Lewis, J.A.; Studart, A.R. Cellulose nanocrystal inks for 3d printing of textured cellular architectures. Adv. Funct. Mater. 2017, 27, 1604619. [Google Scholar] [CrossRef]
- Bom, S.; Santos, C.; Barros, R.; Martins, A.M.; Paradiso, P.; Cláudio, R.; Pinto, P.C.; Ribeiro, H.M.; Marto, J. Effects of starch incorporation on the physicochemical properties and release kinetics of alginate-based 3d hydrogel patches for topical delivery. Pharmaceutics 2020, 12, 719. [Google Scholar] [CrossRef] [PubMed]
- Olmos-Juste, R.; Alonso-Lerma, B.; Pérez-Jiménez, R.; Gabilondo, N.; Eceiza, A. 3d printed alginate-cellulose nanofibers based patches for local curcumin administration. Carbohydr. Polym. 2021, 264, 118026. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.; Trenfield, S.J.; Basit, A.W. Solid Oral Dosage Forms. In Remington; Elsevier: Amsterdam, The Netherlands, 2021; pp. 333–358. [Google Scholar]
- Zhang, H.; Zhang, J.; Streisand, J.B. Oral mucosal drug delivery: Clinical pharmacokinetics and therapeutic applications. Clin. Pharmacokinet. 2002, 41, 661–680. [Google Scholar] [CrossRef] [PubMed]
- Pratap-Singh, A.; Guo, Y.; Baldelli, A.; Singh, A. Concept for a unidirectional release mucoadhesive buccal tablet for oral delivery of antidiabetic peptide drugs such as insulin, glucagon-like peptide 1 (glp-1), and their analogs. Pharmaceutics 2023, 15, 2265. [Google Scholar] [CrossRef]
- Mašková, E.; Kubová, K.; Raimi-Abraham, B.T.; Vllasaliu, D.; Vohlídalová, E.; Turánek, J.; Mašek, J. Hypromellose–a traditional pharmaceutical excipient with modern applications in oral and oromucosal drug delivery. J. Control. Release 2020, 324, 695–727. [Google Scholar] [CrossRef]
- Sudhakar, Y.; Kuotsu, K.; Bandyopadhyay, A. Buccal bioadhesive drug delivery—A promising option for orally less efficient drugs. J. Control. Release 2006, 114, 15–40. [Google Scholar] [CrossRef] [PubMed]
- Al-Taie, A.; Al-Shohani, A.D.; Albasry, Z.; Altaee, A. Current topical trends and novel therapeutic approaches and delivery systems for oral mucositis management. J. Pharm. Bioallied Sci. 2020, 12, 94. [Google Scholar] [CrossRef] [PubMed]
- Buchsel, P.C.; Murphy, P.J. Polyvinylpyrrolidone–sodium hyaluronate gel (gelclair®): A bioadherent oral gel for the treatment of oral mucositis and other painful oral lesions. Expert Opin. Drug Metab. Toxicol. 2008, 4, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- Pignatello, R.; Basile, L.; Puglisi, G. Chitosan glutamate hydrogels with local anesthetic activity for buccal application. Drug Deliv. 2009, 16, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Boynueğri, D.; Özcan, G.; Şenel, S.; Uç, D.; Uraz, A.; Öğüş, E.; Çakılcı, B.; Karaduman, B. Clinical and radiographic evaluations of chitosan gel in periodontal intraosseous defects: A pilot study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 90, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Samiraninezhad, N.; Asadi, K.; Rezazadeh, H.; Gholami, A. Using chitosan, hyaluronic acid, alginate, and gelatin-based smart biological hydrogels for drug delivery in oral mucosal lesions: A review. Int. J. Biol. Macromol. 2023, 252, 126573. [Google Scholar] [CrossRef] [PubMed]
- Modi, J.; Joshi, G.; Sawant, K. Chitosan based mucoadhesive nanoparticles of ketoconazole for bioavailability enhancement: Formulation, optimization, In Vitro and Ex Vivo evaluation. Drug Dev. Ind. Pharm. 2013, 39, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Özdoğan, A.I.; Akca, G.; Şenel, S. Development and in vitro evaluation of chitosan based system for local delivery of atorvastatin for treatment of periodontitis. Eur. J. Pharm. Sci. 2018, 124, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Hosny, K.M.; Aldawsari, H.M.; Bahmdan, R.H.; Sindi, A.M.; Kurakula, M.; Alrobaian, M.M.; Aldryhim, A.Y.; Alkhalidi, H.M.; Bahmdan, H.H.; Khallaf, R.A. Preparation, optimization, and evaluation of hyaluronic acid-based hydrogel loaded with miconazole self-nanoemulsion for the treatment of oral thrush. AAPS PharmSciTech 2019, 20, 297. [Google Scholar] [CrossRef]
- Kraisit, P.; Limmatvapirat, S.; Luangtana-Anan, M.; Sriamornsak, P. Buccal administration of mucoadhesive blend films saturated with propranolol loaded nanoparticles. Asian J. Pharm. Sci. 2018, 13, 34–43. [Google Scholar] [CrossRef]
- Anwunobi, A.; Emeje, M. Recent applications of natural polymers in nanodrug delivery. J. Nanomedic. Nanotechnol. S 2011, 4, 1–6. [Google Scholar] [CrossRef]
- Spleis, H.; Sandmeier, M.; Claus, V.; Bernkop-Schnürch, A. Surface design of nanocarriers: Key to more efficient oral drug delivery systems. Adv. Colloid Interface Sci. 2023, 313, 102848. [Google Scholar] [CrossRef] [PubMed]
- Pangua, C.; Reboredo, C.; Campión, R.; Gracia, J.M.; Martínez-López, A.L.; Irache, J.M. Mucus-Penetrating Nanocarriers. In Theory and Applications of Nonparenteral Nanomedicines; Elsevier: Amsterdam, The Netherlands, 2021; pp. 137–152. [Google Scholar]
- Wang, Y.; Pi, C.; Feng, X.; Hou, Y.; Zhao, L.; Wei, Y. The influence of nanoparticle properties on oral bioavailability of drugs. Int. J. Nanomed. 2020, 15, 6295–6310. [Google Scholar] [CrossRef] [PubMed]
- Pattani, A.; McKay, P.F.; Garland, M.J.; Curran, R.M.; Migalska, K.; Cassidy, C.M.; Malcolm, R.K.; Shattock, R.J.; McCarthy, H.O.; Donnelly, R.F. Microneedle mediated intradermal delivery of adjuvanted recombinant HIV-1 CN54gp140 effectively primes mucosal boost inoculations. J. Control. Release 2012, 162, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Pearton, M.; Kang, S.-M.; Song, J.-M.; Kim, Y.-C.; Quan, F.-S.; Anstey, A.; Ivory, M.; Prausnitz, M.R.; Compans, R.W.; Birchall, J.C. Influenza virus-like particles coated onto microneedles can elicit stimulatory effects on langerhans cells in human skin. Vaccine 2010, 28, 6104–6113. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.O.; Brayden, D.J. Buccal delivery of small molecules and biologics: Of mucoadhesive polymers, films, and nanoparticles. Curr. Opin. Pharmacol. 2017, 36, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Baudner, B.C.; O’Hagan, D.T. Bioadhesive delivery systems for mucosal vaccine delivery. J. Drug Target. 2010, 18, 752–770. [Google Scholar] [CrossRef] [PubMed]
- Feitosa, R.C.; Geraldes, D.C.; Beraldo-de-Araújo, V.L.; Costa, J.S.R.; Oliveira-Nascimento, L. Pharmacokinetic aspects of nanoparticle-in-matrix drug delivery systems for oral/buccal delivery. Front. Pharmacol. 2019, 10, 1057. [Google Scholar] [CrossRef]
- Choi, S.G.; Lee, S.-E.; Kang, B.-S.; Ng, C.L.; Davaa, E.; Park, J.-S. Thermosensitive and mucoadhesive sol-gel composites of paclitaxel/dimethyl-β-cyclodextrin for buccal delivery. PLoS ONE 2014, 9, e109090. [Google Scholar] [CrossRef]
- Zeng, N.; Dumortier, G.; Maury, M.; Mignet, N.; Boudy, V. Influence of additives on a thermosensitive hydrogel for buccal delivery of salbutamol: Relation between micellization, gelation, mechanic and release properties. Int. J. Pharm. 2014, 467, 70–83. [Google Scholar] [CrossRef]
- Mankotia, P.; Choudhary, S.; Sharma, K.; Kumar, V.; Bhatia, J.K.; Parmar, A.; Sharma, S.; Sharma, V. Neem gum based pH responsive hydrogel matrix: A new pharmaceutical excipient for the sustained release of anticancer drug. Int. J. Biol. Macromol. 2020, 142, 742–755. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.O.; McConville, J.T. Manufacture and characterization of mucoadhesive buccal films. Eur. J. Pharm. Biopharm. 2011, 77, 187–199. [Google Scholar] [CrossRef]
- Nii, T.; Ishii, F. Encapsulation efficiency of water-soluble and insoluble drugs in liposomes prepared by the microencapsulation vesicle method. Int. J. Pharm. 2005, 298, 198–205. [Google Scholar] [CrossRef]
- Zewail, M.B.; Asaad, G.F.; Swellam, S.M.; Abd-Allah, S.M.; Hosny, S.K.; Sallah, S.K.; Eissa, J.E.; Mohamed, S.S.; El-Dakroury, W.A. Design, characterization and in vivo performance of solid lipid nanoparticles (slns)-loaded mucoadhesive buccal tablets for efficient delivery of lornoxicam in experimental inflammation. Int. J. Pharm. 2022, 624, 122006. [Google Scholar] [CrossRef]
- Nazem, Z.; Firoozian, F.; Khodabandelou, S.; Mohammadi, M.; Mahboobian, M.M. Systematic optimization of solid lipid nanoparticles of silybin for improved oral drug delivery by box-behnken design: In vitro and in vivo evaluations. J. Pharm. Innov. 2023, 18, 472–484. [Google Scholar] [CrossRef]
- Madkhali, O.A. Perspectives and prospective on solid lipid nanoparticles as drug delivery systems. Molecules 2022, 27, 1543. [Google Scholar] [CrossRef]
- Beloqui, A.; del Pozo-Rodríguez, A.; Isla, A.; Rodríguez-Gascón, A.; Solinís, M.Á. Nanostructured lipid carriers as oral delivery systems for poorly soluble drugs. J. Drug Deliv. Sci. Technol. 2017, 42, 144–154. [Google Scholar] [CrossRef]
- Le, N.D.; Tran, P.H.; Lee, B.-J.; Tran, T.T. Solid lipid particle-based tablets for buccal delivery: The role of solid lipid particles in drug release. J. Drug Deliv. Sci. Technol. 2019, 52, 96–102. [Google Scholar] [CrossRef]
- Hazzah, H.A.; Farid, R.M.; Nasra, M.M.; El-Massik, M.A.; Abdallah, O.Y. Lyophilized sponges loaded with curcumin solid lipid nanoparticles for buccal delivery: Development and characterization. Int. J. Pharm. 2015, 492, 248–257. [Google Scholar] [CrossRef]
- Joshi, S.; Hussain, M.T.; Roces, C.B.; Anderluzzi, G.; Kastner, E.; Salmaso, S.; Kirby, D.J.; Perrie, Y. Microfluidics based manufacture of liposomes simultaneously entrapping hydrophilic and lipophilic drugs. Int. J. Pharm. 2016, 514, 160–168. [Google Scholar] [CrossRef]
- Abd El Azim, H.; Nafee, N.; Ramadan, A.; Khalafallah, N. Liposomal buccal mucoadhesive film for improved delivery and permeation of water-soluble vitamins. Int. J. Pharm. 2015, 488, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Pistone, S.; Goycoolea, F.M.; Young, A.; Smistad, G.; Hiorth, M. Formulation of polysaccharide-based nanoparticles for local administration into the oral cavity. Eur. J. Pharm. Sci. 2017, 96, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.J.; Calpena, A.C.; Fernandez, F.; Mallandrich, M.; Gálvez, P.; Clares, B. Development of alginate microspheres as nystatin carriers for oral mucosa drug delivery. Carbohydr. Polym. 2015, 117, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Maghrebi, S.; Prestidge, C.A.; Joyce, P. An update on polymer-lipid hybrid systems for improving oral drug delivery. Expert Opin. Drug Deliv. 2019, 16, 507–524. [Google Scholar] [CrossRef] [PubMed]
- Sivadasan, D.; Sultan, M.H.; Madkhali, O.; Almoshari, Y.; Thangavel, N. Polymeric lipid hybrid nanoparticles (PLNs) as emerging drug delivery platform—A comprehensive review of their properties, preparation methods, and therapeutic applications. Pharmaceutics 2021, 13, 1291. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.; Latha, M.; Thomas, K.K. Synthesis and in vitro evaluation of alginate-cellulose nanocrystal hybrid nanoparticles for the controlled oral delivery of rifampicin. J. Drug Deliv. Sci. Technol. 2018, 46, 392–399. [Google Scholar] [CrossRef]
- Liu, K.-H.; Liu, T.-Y.; Chen, S.-Y.; Liu, D.-M. Effect of clay content on electrostimulus deformation and volume recovery behavior of a clay–chitosan hybrid composite. Acta Biomater. 2007, 3, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Pongjanyakul, T.; Khunawattanakul, W.; Strachan, C.J.; Gordon, K.C.; Puttipipatkhachorn, S.; Rades, T. Characterization of chitosan–magnesium aluminum silicate nanocomposite films for buccal delivery of nicotine. Int. J. Biol. Macromol. 2013, 55, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Mallakpour, S. Ultrasonic-assisted fabrication of starch/mwcnt-glucose nanocomposites for drug delivery. Ultrason. Sonochemistry 2018, 40, 402–409. [Google Scholar] [CrossRef]
- Mallakpour, S.; Soltanian, S. Surface functionalization of carbon nanotubes: Fabrication and applications. RSC Adv. 2016, 6, 109916–109935. [Google Scholar] [CrossRef]
- Yeo, W.W.Y.; Maran, S.; Kong, A.S.-Y.; Cheng, W.-H.; Lim, S.-H.E.; Loh, J.-Y.; Lai, K.-S. A metal-containing np approach to treat methicillin-resistant staphylococcus aureus (mrsa): Prospects and challenges. Materials 2022, 15, 5802. [Google Scholar] [CrossRef] [PubMed]
- Iudin, D.; Vasilieva, M.; Knyazeva, E.; Korzhikov-Vlakh, V.; Demyanova, E.; Lavrentieva, A.; Skorik, Y.; Korzhikova-Vlakh, E. Hybrid nanoparticles and composite hydrogel systems for delivery of peptide antibiotics. Int. J. Mol. Sci. 2022, 23, 2771. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, G.A.; Ali, A.E.-H.; Raafat, A.I.; Badawy, N.A.; Elshahawy, M.F. Development of (acrylic acid/polyethylene glycol)-zinc oxide mucoadhesive nanocomposites for buccal administration of propranolol HCL. Radiat. Phys. Chem. 2018, 147, 18–26. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biopolymers | Mucoadhesive Properties |
|---|---|
| Cationic (such as chitosan and its cationic derivatives) | Chitosan is characterized by high mucoadhesion due to the formation of ionic bonds with mucins. Cationic quaternized derivatives of chitosan are characterized by improved mucoadhesion compared to chitosan and also form more stable polyelectrolyte complexes with various polyanions. Chitosan and its derivatives improve the intercellular permeability of drugs by opening up tight junctions. |
| Anionic (such as alginic acid, hyaluronic acid, pectin, CMC, carrageenans, fucoidans) | Anionic polymers have high mucoadhesive properties due to the formation of strong hydrogen bonds with mucins. Moreover, the presence of carboxyl or sulfate functional groups with different pKa allows us to vary the properties of drug delivery systems based on them, especially the stability of the complexes and the rate of drug release. |
| Non-ionic (such as starch, cellulose, HPMC, methylcellulose) | In general, the mucoadhesive properties of nonionic biopolymers should be improved by grafting fragments that enhance mucoadhesion. |
| Polyampholites (such as collagen, gelatin) | The mucoadhesive properties of polyampholytes can be controlled by changing the pH. |
| Thiolated biopolymers | Thiolated polymers have higher mucoadhesive properties due to the formation of a disulfide bridge with mucin molecules. |
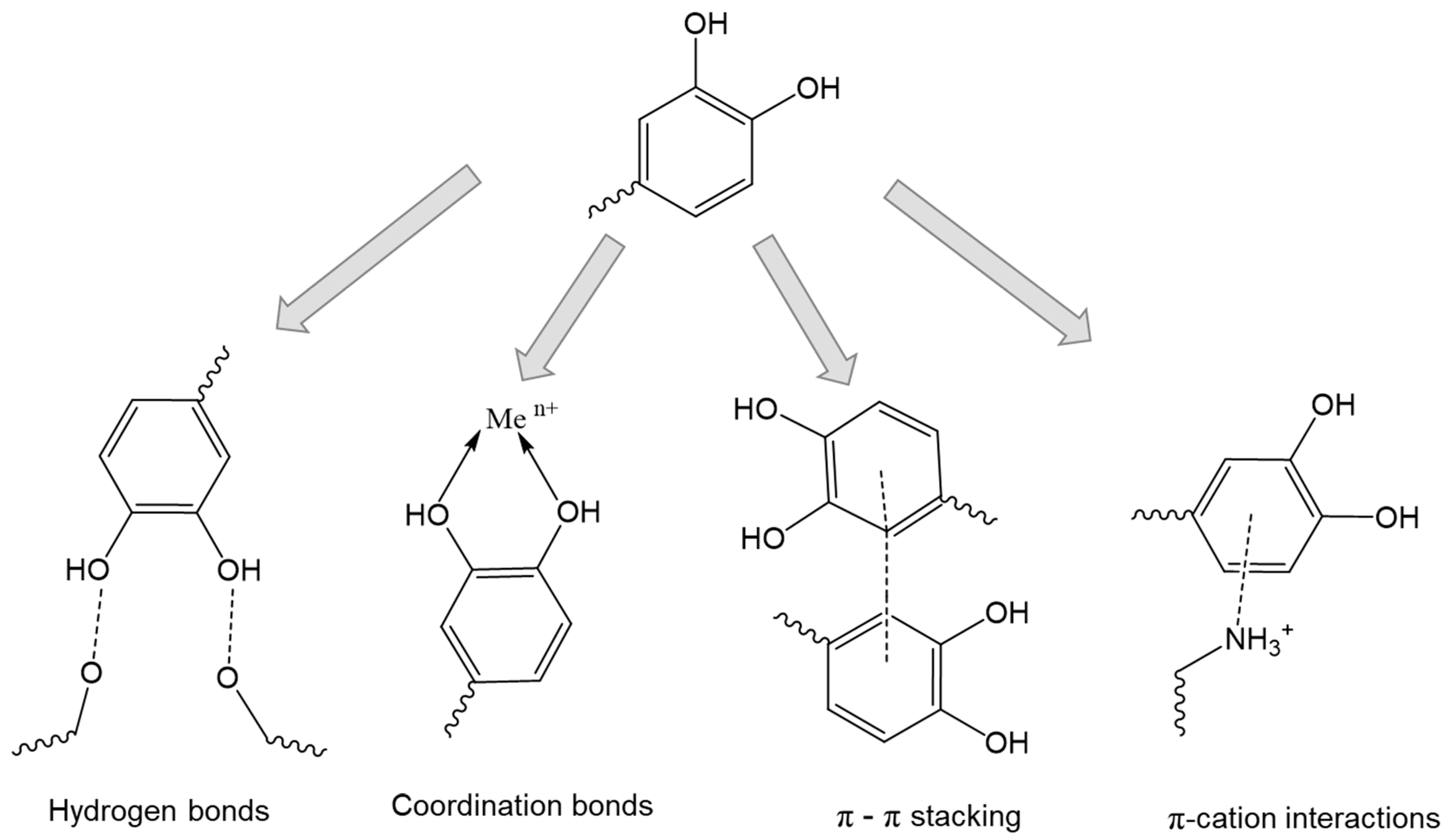
| Catechol-based biopolymers | Catechol moieties provide extremely strong adhesion, even in wet environments, as well as broad possibilities for conjugation with bioactive molecules. Catechol moieties can be formed by additional coordination bonds, π-π stacking, and π-cation interactions. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubashynskaya, N.V.; Petrova, V.A.; Skorik, Y.A. Biopolymer Drug Delivery Systems for Oromucosal Application: Recent Trends in Pharmaceutical R&D. Int. J. Mol. Sci. 2024, 25, 5359. https://doi.org/10.3390/ijms25105359
Dubashynskaya NV, Petrova VA, Skorik YA. Biopolymer Drug Delivery Systems for Oromucosal Application: Recent Trends in Pharmaceutical R&D. International Journal of Molecular Sciences. 2024; 25(10):5359. https://doi.org/10.3390/ijms25105359
Chicago/Turabian StyleDubashynskaya, Natallia V., Valentina A. Petrova, and Yury A. Skorik. 2024. "Biopolymer Drug Delivery Systems for Oromucosal Application: Recent Trends in Pharmaceutical R&D" International Journal of Molecular Sciences 25, no. 10: 5359. https://doi.org/10.3390/ijms25105359
APA StyleDubashynskaya, N. V., Petrova, V. A., & Skorik, Y. A. (2024). Biopolymer Drug Delivery Systems for Oromucosal Application: Recent Trends in Pharmaceutical R&D. International Journal of Molecular Sciences, 25(10), 5359. https://doi.org/10.3390/ijms25105359