

Urinary Angiotensinogen Displays Sexual Dimorphism in Non-Diabetic Humans and Mice with Overweight

 , , , , and
, , , , and
Abstract

1. Introduction
2. Results
2.1. Results in Humans
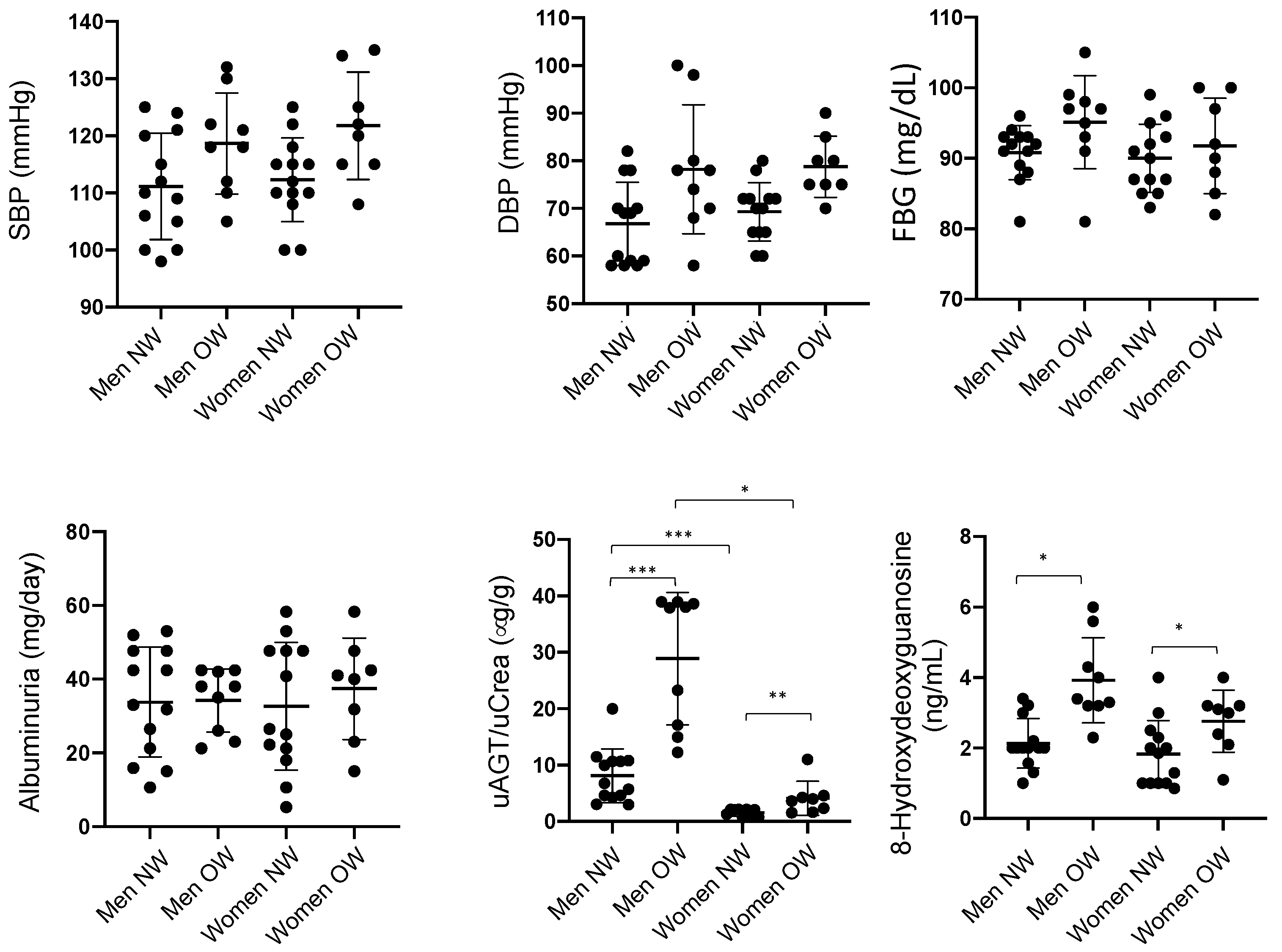
2.1.1. Clinical Characteristics and Urinary AGT Levels in Normal and Overweight Subjects
2.1.2. Urinary AGT Levels in Normal and Overweight Subjects and Possible Predictors of High Levels of uAGT
2.1.3. Reactive Oxygen Species in Urine
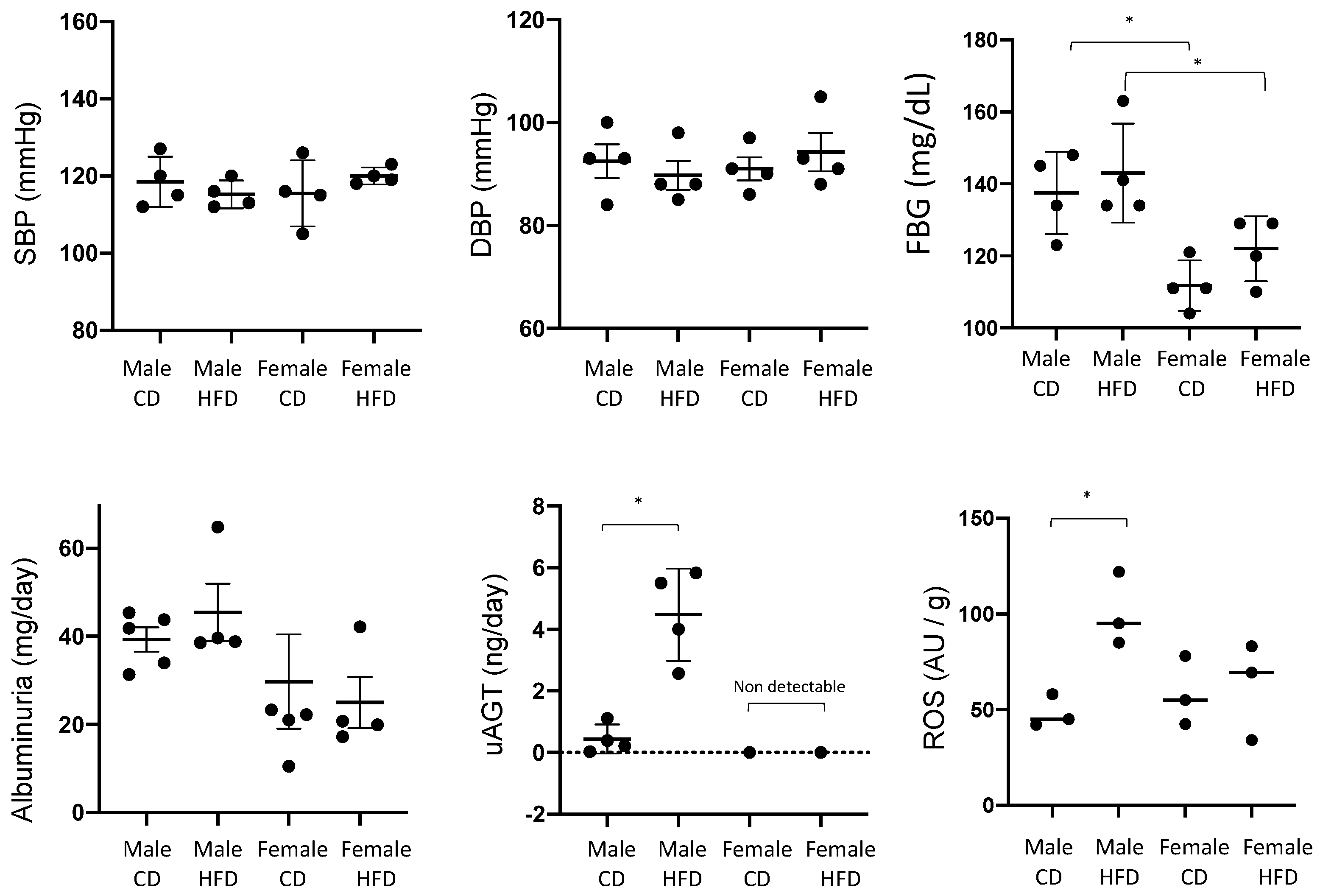
2.2. Results in Mice
Physiological Characteristics and Urinary Angiotensinogen in Females and Males in Mice with Control and High Fat Diet
3. Discussion
4. Materials and Methods
4.1. Studies in Humans
4.2. Studies in Mice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kurian, M.J.; Rentzepis, P.J.; Carracher, A.M.; Close, K.L. American Heart Association Scientific Sessions 2018. J. Diabetes 2019, 11, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.J.; Toma, I.; Sipos, A.; Meer, E.J.; Vargas, S.L.; Peti-Peterdi, J. The collecting duct is the major source of prorenin in diabetes. Hypertension 2008, 51, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Rohrwasser, A.; Morgan, T.; Dillon, H.F.; Zhao, L.; Callaway, C.W.; Hillas, E.; Zhang, S.H.; Cheng, T.; Inagami, T.; Ward, K.; et al. Elements of a paracrine tubular renin-angiotensin system along the entire nephron. Hypertension 1999, 34, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Mamenko, M.; Zaika, O.; Doris, P.A.; Pochynyuk, O. Salt-Dependent Inhibition of Epithelial Na+ Channel-Mediated Sodium Reabsorption in the Aldosterone-Sensitive Distal Nephron by Bradykinin. Hypertension 2012, 60, 1234–1241. [Google Scholar] [CrossRef]
- Ritz, E.; Bakris, G.; World Kidney Day Organising, C. World Kidney Day: Hypertension and chronic kidney disease. Lancet 2009, 373, 1157–1158. [Google Scholar] [CrossRef]
- Nagai, Y.; Yao, L.; Kobori, H.; Miyata, K.; Ozawa, Y.; Miyatake, A.; Yukimura, T.; Shokoji, T.; Kimura, S.; Kiyomoto, H.; et al. Temporary angiotensin II blockade at the prediabetic stage attenuates the development of renal injury in type 2 diabetic rats. J. Am. Soc. Nephrol. 2005, 16, 703–711. [Google Scholar] [CrossRef]
- Parving, H.H.; Hommel, E.; Jensen, B.R.; Hansen, H.P. Long-term beneficial effect of ACE inhibition on diabetic nephropathy in normotensive type 1 diabetic patients. Kidney Int. 2001, 60, 228–234. [Google Scholar] [CrossRef]
- Kobori, H.; Nishiyama, A.; Abe, Y.; Navar, L.G. Enhancement of intrarenal angiotensinogen in Dahl salt-sensitive rats on high salt diet. Hypertension 2003, 41, 592–597. [Google Scholar] [CrossRef]
- Kobori, H.; Nishiyama, A.; Harrison-Bernard, L.M.; Navar, L.G. Urinary angiotensinogen as an indicator of intrarenal angiotensin status in hypertension. Hypertension 2003, 41, 42–49. [Google Scholar] [CrossRef]
- Nishiyama, A.; Konishi, Y.; Ohashi, N.; Morikawa, T.; Urushihara, M.; Maeda, I.; Hamada, M.; Kishida, M.; Hitomi, H.; Shirahashi, N.; et al. Urinary angiotensinogen reflects the activity of intrarenal renin-angiotensin system in patients with IgA nephropathy. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.—Eur. Ren. Assoc. 2011, 26, 170–177. [Google Scholar] [CrossRef]
- Mizushige, T.; Kobori, H.; Nishijima, Y.; Yano, Y.; Sakata, K.; Hayakawa, M.; Nishiyama, A. Urinary Angiotensinogen Could Be a Prognostic Marker of Renoprotective Effects of Alogliptin in Patients with Type 2 Diabetes. J. Diabetes Res. 2015, 2015, 517472. [Google Scholar] [CrossRef] [PubMed]
- Rivera, P.; Miranda, C.; Roldan, N.; Guerrero, A.; Olave, J.; Cardenas, P.; Nguyen, Q.M.; Kassan, M.; Gonzalez, A.A. Augmented transcripts of kidney injury markers and renin angiotensin system in urine samples of overweight young adults. Sci. Rep. 2020, 10, 21154. [Google Scholar] [CrossRef] [PubMed]
- Coca, A.; Messerli, F.H.; Benetos, A.; Zhou, Q.; Champion, A.; Cooper-DeHoff, R.M.; Pepine, C.J. Predicting stroke risk in hypertensive patients with coronary artery disease: A report from the INVEST. Stroke 2008, 39, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Selvaraju, V.; Ayine, P.; Fadamiro, M.; Babu, J.R.; Brown, M.; Geetha, T. Urinary Biomarkers of Inflammation and Oxidative Stress Are Elevated in Obese Children and Correlate with a Marker of Endothelial Dysfunction. Oxid Med. Cell Longev. 2019, 2019, 9604740. [Google Scholar] [CrossRef] [PubMed]
- Iwano, M.; Neilson, E.G. Mechanisms of tubulointerstitial fibrosis. Curr. Opin. Nephrol. Hypertens 2004, 13, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Miao, X.J.; Bi, T.T.; Tang, J.M.; Lv, R.; Gui, D.K.; Yang, X.F. Regulatory mechanism of TGF-beta1/SGK1 pathway in tubulointerstitial fibrosis of diabetic nephropathy. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 10482–10488. [Google Scholar] [CrossRef]
- Reverte, V.; Gogulamudi, V.R.; Rosales, C.B.; Musial, D.C.; Gonsalez, S.R.; Parra-Vitela, A.J.; Galeas-Pena, M.; Sure, V.N.; Visniauskas, B.; Lindsey, S.H.; et al. Urinary angiotensinogen increases in the absence of overt renal injury in high fat diet-induced type 2 diabetic mice. J. Diabetes Complicat. 2020, 34, 107448. [Google Scholar] [CrossRef]
- Chen, Q.; Su, Y.; Ju, Y.; Ma, K.; Li, W.; Li, W. Astragalosides IV protected the renal tubular epithelial cells from free fatty acids-induced injury by reducing oxidative stress and apoptosis. Biomed. Pharmacother. 2018, 108, 679–686. [Google Scholar] [CrossRef]
- Han, Y.; Xu, X.; Tang, C.; Gao, P.; Chen, X.; Xiong, X.; Yang, M.; Yang, S.; Zhu, X.; Yuan, S.; et al. Reactive oxygen species promote tubular injury in diabetic nephropathy: The role of the mitochondrial ros-txnip-nlrp3 biological axis. Redox Biol. 2018, 16, 32–46. [Google Scholar] [CrossRef]
- Visniauskas, B.; Arita, D.Y.; Rosales, C.B.; Feroz, M.A.; Luffman, C.; Accavitti, M.J.; Dawkins, G.; Hong, J.; Curnow, A.C.; Thethi, T.K.; et al. Sex differences in soluble prorenin receptor in patients with type 2 diabetes. Biol. Sex Differ. 2021, 12, 33. [Google Scholar] [CrossRef]
- Ichihara, A.; Suzuki, F.; Nakagawa, T.; Kaneshiro, Y.; Takemitsu, T.; Sakoda, M.; Nabi, A.H.M.N.; Nishiyama, A.; Sugaya, T.; Hayashi, M.; et al. Prorenin receptor blockade inhibits development of glomerulosclerosis in diabetic angiotensin II type 1a receptor-deficient mice. J. Am. Soc. Nephrol. 2006, 17, 1950–1961. [Google Scholar] [CrossRef]
- Kaneshiro, Y.; Ichihara, A.; Takemitsu, T.; Sakoda, M.; Suzuki, F.; Nakagawa, T.; Hayashi, M.; Inagami, T. Increased expression of cyclooxygenase-2 in the renal cortex of human prorenin receptor gene-transgenic rats. Kidney Int. 2006, 70, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, N.; Murata, I.; Takemura, G.; Okada, H.; Kanamori, H.; Matsumoto-Miyazaki, J.; Yoshida, G.; Izumi, K.; Kashi, H.; Niimi, K.; et al. Expression of prorenin receptor in renal biopsies from patients with IgA nephropathy. Int. J. Clin. Exp. Pathol. 2014, 7, 7485–7496. [Google Scholar] [PubMed]
- Visniauskas, B.; Reverte, V.; Abshire, C.M.; Ogola, B.O.; Rosales, C.B.; Galeas-Pena, M.; Sure, V.N.; Sakamuri, S.; Harris, N.R.; Kilanowski-Doroh, I.; et al. High-plasma soluble prorenin receptor is associated with vascular damage in male, but not female, mice fed a high-fat diet. Am. J. Physiology. Heart Circ. Physiol. 2023, 324, H762–H775. [Google Scholar] [CrossRef] [PubMed]
- Sartori-Valinotti, J.C.; Iliescu, R.; Yanes, L.L.; Dorsett-Martin, W.; Reckelhoff, J.F. Sex differences in the pressor response to angiotensin II when the endogenous renin-angiotensin system is blocked. Hypertension 2008, 51, 1170–1176. [Google Scholar] [CrossRef]
- Hall, J.E.; Henegar, J.R.; Dwyer, T.M.; Liu, J.; Da Silva, A.A.; Kuo, J.J.; Tallam, L. Is obesity a major cause of chronic kidney disease? Adv. Ren. Replace Ther. 2004, 11, 41–54. [Google Scholar] [CrossRef]
- Sato, E.; Mori, T.; Satoh, M.; Fujiwara, M.; Nakamichi, Y.; Oba, I.; Ogawa, S.; Kinouchi, Y.; Sato, H.; Ito, S.; et al. Urinary angiotensinogen excretion is associated with blood pressure in obese young adults. Clin. Exp. Hypertens 2016, 38, 203–208. [Google Scholar] [CrossRef]
- Kobori, H.; Urushihara, M.; Xu, J.H.; Berenson, G.S.; Navar, L.G. Urinary angiotensinogen is correlated with blood pressure in men (Bogalusa Heart Study). J. Hypertens 2010, 28, 1422–1428. [Google Scholar] [CrossRef]
- Bourgeois, C.T.; Satou, R.; Prieto, M.C. HDAC9 is an epigenetic repressor of kidney angiotensinogen establishing a sex difference. Biol. Sex Differ. 2017, 8, 18. [Google Scholar] [CrossRef]
- Fischer, M.; Baessler, A.; Schunkert, H. Renin angiotensin system and gender differences in the cardiovascular system. Cardiovasc. Res. 2002, 53, 672–677. [Google Scholar] [CrossRef]
- Rands, V.F.; Seth, D.M.; Kobori, H.; Prieto, M.C. Sexual dimorphism in urinary angiotensinogen excretion during chronic angiotensin II-salt hypertension. Gend Med. 2012, 9, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Roksnoer, L.C.; Verdonk, K.; van den Meiracker, A.H.; Hoorn, E.J.; Zietse, R.; Danser, A.H. Urinary markers of intrarenal renin-angiotensin system activity in vivo. Curr. Hypertens Rep. 2013, 15, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Salih, M.; Bovee, D.M.; Roksnoer, L.C.W.; Casteleijn, N.F.; Bakker, S.J.L.; Gansevoort, R.T.; Zietse, R.; Danser, A.H.J.; Hoorn, E.J. Urinary renin-angiotensin markers in polycystic kidney disease. Am. J. Physiol. Ren. Physiol. 2017, 313, F874–F881. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Gonzalez, A.A.; McCormack, M.; Seth, D.M.; Kobori, H.; Navar, L.G.; Prieto, M.C. Increased renin excretion is associated with augmented urinary angiotensin II levels in chronic angiotensin II-infused hypertensive rats. Am. J. Physiol.-Ren. 2011, 301, F1195–F1201. [Google Scholar] [CrossRef] [PubMed]
- Kobori, H.; Kamiyama, M.; Harrison-Bernard, L.M.; Navar, L.G. Cardinal role of the intrarenal renin-angiotensin system in the pathogenesis of diabetic nephropathy. J. Investig. Med. 2013, 61, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Yokota, H.; Mori, F.; Kai, K.; Nagaoka, T.; Izumi, N.; Takahashi, A.; Hikichi, T.; Yoshida, A.; Suzuki, F.; Ishida, Y. Serum prorenin levels and diabetic retinopathy in type 2 diabetes: New method to measure serum level of prorenin using antibody activating direct kinetic assay. Br. J. Ophthalmol. 2005, 89, 871–873. [Google Scholar] [CrossRef] [PubMed]
- Yokota, H.; Nagaoka, T.; Tani, T.; Takahashi, A.; Sato, E.; Kato, Y.; Yoshida, A. Higher levels of prorenin predict development of diabetic retinopathy in patients with type 2 diabetes. J. Renin-Angiotensin-Aldosterone Syst. JRAAS 2011, 12, 290–294. [Google Scholar] [CrossRef]
- Cuevas, C.; Gonzalez, A.; Inestrosa, N.; Vio, C.; Prieto, M. The activation of the(Pro)renin receptor (PRR) stimulates fibrotic factors expression independent of b-catenin signaling pathway in collecting duct cells. Faseb J. 2015, 29. [Google Scholar] [CrossRef]
- Gonzalez, A.A.; Zamora, L.; Reyes-Martinez, C.; Salinas-Parra, N.; Roldan, N.; Cuevas, C.A.; Figueroa, S.; Gonzalez-Vergara, A.; Prieto, M.C. (Pro)renin receptor activation increases profibrotic markers and fibroblast-like phenotype through MAPK-dependent ROS formation in mouse renal collecting duct cells. Clin. Exp. Pharmacol. Physiol. 2017, 44, 1134–1144. [Google Scholar] [CrossRef]
- Gilbert, R.E.; Akdeniz, A.; Weitz, S.; Usinger, W.R.; Molineaux, C.; Jones, S.E.; Langham, R.G.; Jerums, G. Urinary connective tissue growth factor excretion in patients with type 1 diabetes and nephropathy. Diabetes Care 2003, 26, 2632–2636. [Google Scholar] [CrossRef]
- Terami, T.; Wada, J.; Inoue, K.; Nakatsuka, A.; Ogawa, D.; Teshigawara, S.; Murakami, K.; Katayama, A.; Eguchi, J.; Makino, H. Urinary angiotensinogen is a marker for tubular injuries in patients with type 2 diabetes. Int. J. Nephrol. Renov. Dis. 2013, 6, 233–240. [Google Scholar] [CrossRef]
- Sawaguchi, M.; Araki, S.I.; Kobori, H.; Urushihara, M.; Haneda, M.; Koya, D.; Kashiwagi, A.; Uzu, T.; Maegawa, H. Association between urinary angiotensinogen levels and renal and cardiovascular prognoses in patients with type 2 diabetes mellitus. J. Diabetes Investig. 2012, 3, 318–324. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Non-smoking | Smokers |
| No acute or chronic infection | Acute or chronic infection |
| No treatment with ARBs, ACE inhibitors (preceding 4 weeks) | Treatment with anti-hypertensive drugs (preceding 4 weeks) |
| No diabetic treatment (preceding 4 weeks) | Diabetic treatment (preceding 4 weeks) |
| Variables | Odds Ratio | 95% CI | P |
|---|---|---|---|
| Gender (Male?) | 1.056 | 0.8967–1.271 | 0.4887 |
| FBG ≥ 100 mg/dL | 0.893 | 0.1281–1.948 | 0.1697 |
| SBP ≥ 120 mmHg | 1.008 | 0.8393–1.194 | 0.3329 |
| DBP ≥ 80 mmHg | 1.056 | 0.8831–1.2614 | 0.7410 |
| Albuminuria ≥ 30 mg/g | 2.324 | 1.107–11.83 | 0.0448 * |
| Overweight (BMI ≥ 25) | 3.933 | 0.2712–0.7226 | <0.0001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez, A.A.; Visniauskas, B.; Reverte, V.; Sure, V.N.; Vallotton, Z.; Torres, B.S.; Acosta, M.A.; Zemedkun, M.; Katakam, P.V.; Prieto, M.C. Urinary Angiotensinogen Displays Sexual Dimorphism in Non-Diabetic Humans and Mice with Overweight. Int. J. Mol. Sci. 2024, 25, 635. https://doi.org/10.3390/ijms25010635
Gonzalez AA, Visniauskas B, Reverte V, Sure VN, Vallotton Z, Torres BS, Acosta MA, Zemedkun M, Katakam PV, Prieto MC. Urinary Angiotensinogen Displays Sexual Dimorphism in Non-Diabetic Humans and Mice with Overweight. International Journal of Molecular Sciences. 2024; 25(1):635. https://doi.org/10.3390/ijms25010635
Chicago/Turabian StyleGonzalez, Alexis A., Bruna Visniauskas, Virginia Reverte, Ventaka N. Sure, Zoe Vallotton, Bryan S. Torres, Marco A. Acosta, Mahlet Zemedkun, Prasad V. Katakam, and Minolfa C. Prieto. 2024. "Urinary Angiotensinogen Displays Sexual Dimorphism in Non-Diabetic Humans and Mice with Overweight" International Journal of Molecular Sciences 25, no. 1: 635. https://doi.org/10.3390/ijms25010635
APA StyleGonzalez, A. A., Visniauskas, B., Reverte, V., Sure, V. N., Vallotton, Z., Torres, B. S., Acosta, M. A., Zemedkun, M., Katakam, P. V., & Prieto, M. C. (2024). Urinary Angiotensinogen Displays Sexual Dimorphism in Non-Diabetic Humans and Mice with Overweight. International Journal of Molecular Sciences, 25(1), 635. https://doi.org/10.3390/ijms25010635