1. Introduction
Tuberculosis (TB), caused by
Mycobacterium tuberculosis, is a major global health concern, predominantly spread via respiratory transmission, and responsible for infecting approximately one-quarter of the world’s population [
1]. Despite this high infection rate, only an estimated 5–10% of infected individuals develop TB in their lifetime [
2]. TB predominantly affects adults, with a higher incidence in males, and can target multiple organs, most commonly the lungs. Without effective treatment, TB has a high mortality rate: approximately 50% [
3]. The burden of TB is geographically skewed, with the majority of cases and deaths concentrated in specific regions of Asia and Africa. Influenced by factors such as undernourishment, diabetes, HIV infection, alcohol use disorders, and smoking, TB was the leading cause of death from a single infectious agent, surpassing HIV/AIDS, until the advent of COVID-19 [
4,
5].
In 2021, there was a notable increase in the global incidence of tuberculosis (TB), with 10.6 million cases reported—a 4.5% rise from 2020, ending a long-term trend of decline. This surge was most pronounced in Southeast Asia (45%), Africa (23%), and the Western Pacific (18%), with adult men being the most affected group, comprising 57% of the cases. The COVID-19 pandemic complicated incidence estimations, necessitating reliance on dynamic models due to disrupted national disease surveillance [
3].
Simultaneously, TB mortality also rose significantly, reversing the declining trend observed since 2005. Approximately 1.6 million deaths were recorded in 2021, up from 1.5 million in 2020, with the majority among HIV-negative individuals. This increase undid progress towards the End TB Strategy’s goal of reducing TB deaths by 35% from 2015 to 2020, with only a 5.9% reduction achieved by 2021. This higher mortality can be attributed to pandemic-related disruptions in TB services, particularly in case detection and treatment, which have a rapid and severe impact on mortality rates [
3].
The recent global health crisis, initiated by the highly pathogenic human coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has led to the most severe pandemic of the last century, resulting in coronavirus disease 2019 (COVID-19) [
6]. Characterized by significant mortality and morbidity, the outbreak began in December 2019 with unusual viral pneumonia cases in Wuhan, Hubei Province, China, and it quickly spread globally [
7]. As of mid-2023, the WHO has shifted its approach, recognizing COVID-19 as an established health issue and advising on transitioning to its long-term management [
8]. This pandemic has significantly disrupted healthcare services worldwide, impacting access to essential TB services and leading to pronounced drops in TB case notifications [
9,
10]. The end of 2022 marked the beginning of a recovery in essential health services, as per WHO reports. However, economic recovery, especially in emerging economies and disadvantaged groups, is anticipated to take longer [
11,
12].
In 2020, Romania reported the highest incidence of TB within the European Union/European Economic Area (EU/EEA), accounting for 23.2% of the 33,148 TB cases reported across 29 EU/EEA countries. This stark contrast underscores Romania’s unique challenge with TB, marking it as the European country with the highest TB incidence rate during that period [
13]. Additionally, Romania has recorded a total of 3,501,193 confirmed COVID-19 cases, with 68,590 deaths [
14].
Serum magnesium maintains normal cellular function and metabolism, and it is crucial for various enzymatic reactions, ion channel regulation, and energy production. The interaction between SARS-CoV-2 and ACE-2 receptors, found in pneumocytes and endothelial cells, is facilitated by the virus’s S-spike protein. This interaction alters ACE-2 pathways, leading to acute damage in the lungs, heart, and endothelial cells [
15].
A serum magnesium deficiency might contribute to the pathophysiology of SARS-CoV-2 infection. During the progression of COVID-19, a lack of serum magnesium can increase the risk of initiating a severe inflammatory response known as a “cytokine storm”, harm the vascular endothelium, and trigger a coagulation cascade that could result in disseminated intravascular coagulation. Magnesium, an essential mineral, plays a pivotal role in the optimal functioning of various immune cells, including T cells, B cells, and macrophages. These cells are integral to the body’s defense mechanisms and crucial for cytokine production. Serum magnesium deficiency can disrupt cellular functions, potentially leading to an exaggerated inflammatory response. This is particularly relevant in inflammatory diseases like COVID-19, where cytokine production is a critical factor.
Increased levels of pro-inflammatory cytokines, such as TNF-α, IL-6, and IL-1β, are linked to serum magnesium deficiency. These cytokines are central to developing a cytokine storm, a severe inflammatory response that can occur in diseases like COVID-19 and lead to dangerous complications [
16]. Ashique et al. [
16] highlighted serum magnesium’s role in mitigating oxidative stress, closely related to inflammation. In conditions like COVID-19, oxidative stress can intensify the inflammatory response, leading to severe complications. Serum magnesium’s ability to reduce oxidative stress is crucial in modulating inflammation and preventing exacerbated responses, such as cytokine storms. Additionally, serum magnesium functions as a natural antagonist to serum calcium. It affects the activity of NMDA receptors involved in inflammation. A deficiency in serum magnesium may increase serum calcium influx, further stimulating the release of inflammatory cytokines and exacerbating the inflammatory response. Given its critical role in immune function and inflammation regulation, serum magnesium supplementation is suggested as a potential therapeutic approach for reducing the severity of inflammatory diseases, including COVID-19. Maintaining adequate serum magnesium levels controls immune responses and prevents excessive inflammation.
Furthermore, serum magnesium may play a role in the onset of long COVID-19 syndrome, potentially exacerbating symptoms or existing health conditions [
17]. A study indicated that 70% of acutely ill patients exhibited reduced serum calcium levels (−0.25 to −0.2 mmol/L), linked with a poorer prognosis [
17]. Earlier research on COVID-19 patients revealed that severe or critical cases often involve electrolyte disturbances, including serum calcium level imbalances [
18].
In recent medical research, the assessment of serum calcium levels has emerged as a crucial factor in understanding and managing various infectious diseases, including tuberculosis (TB) and COVID-19. Serum calcium, a vital electrolyte in the body, plays a significant role in numerous physiological processes, including cell signaling, muscle function, and vascular contraction. Its levels in the blood can reflect changes in bodily function and disease states.
Our decision to assess serum calcium levels stems from their potential as diagnostic and prognostic biomarkers in infectious diseases. In TB, for example, a study by Chandra TJ [
19] on 100 participants highlighted a correlation between serum calcium levels and disease severity, as indicated by smear grading. Although the statistical significance was not strong, the trend observed suggests an inverse relationship between serum calcium levels and TB severity [
19].
Similarly, in the context of the ongoing COVID-19 pandemic, understanding the multifaceted pathophysiology of the virus is crucial. A 2023 study involving 127 COVID-19 patients revealed that lower serum calcium levels are common in these patients, regardless of disease severity. Particularly in severe or critical cases, most exhibited low serum calcium levels. This trend, alongside correlations with severe organ injuries and elevated levels of pro-inflammatory cytokines like IL-6, underscores the importance of serum calcium in the pathophysiological mechanisms of COVID-19 [
20].
This study aims to thoroughly investigate the relationship between electrolyte imbalances, specifically serum calcium and serum magnesium levels, and the severity of COVID-19 and TB. We intend to analyze whether these electrolyte disturbances correlate with the severity of these diseases. Additionally, our study will explore the potential impact of such imbalances on the pulmonary function parameters, including forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), maximum expiratory flow at 50% of FVC (MEF 50), and the FEV1/FVC ratio, in patients diagnosed with COVID-19 and TB. This research aims to provide deeper insights into the pathophysiology of these infections and contribute to developing more effective clinical management strategies for patients suffering from these diseases.
3. Discussion
To the best of our knowledge, this study is among the first to concurrently evaluate the implications of COVID-19 and tuberculosis, offering unique insights into their comparative pathophysiology.
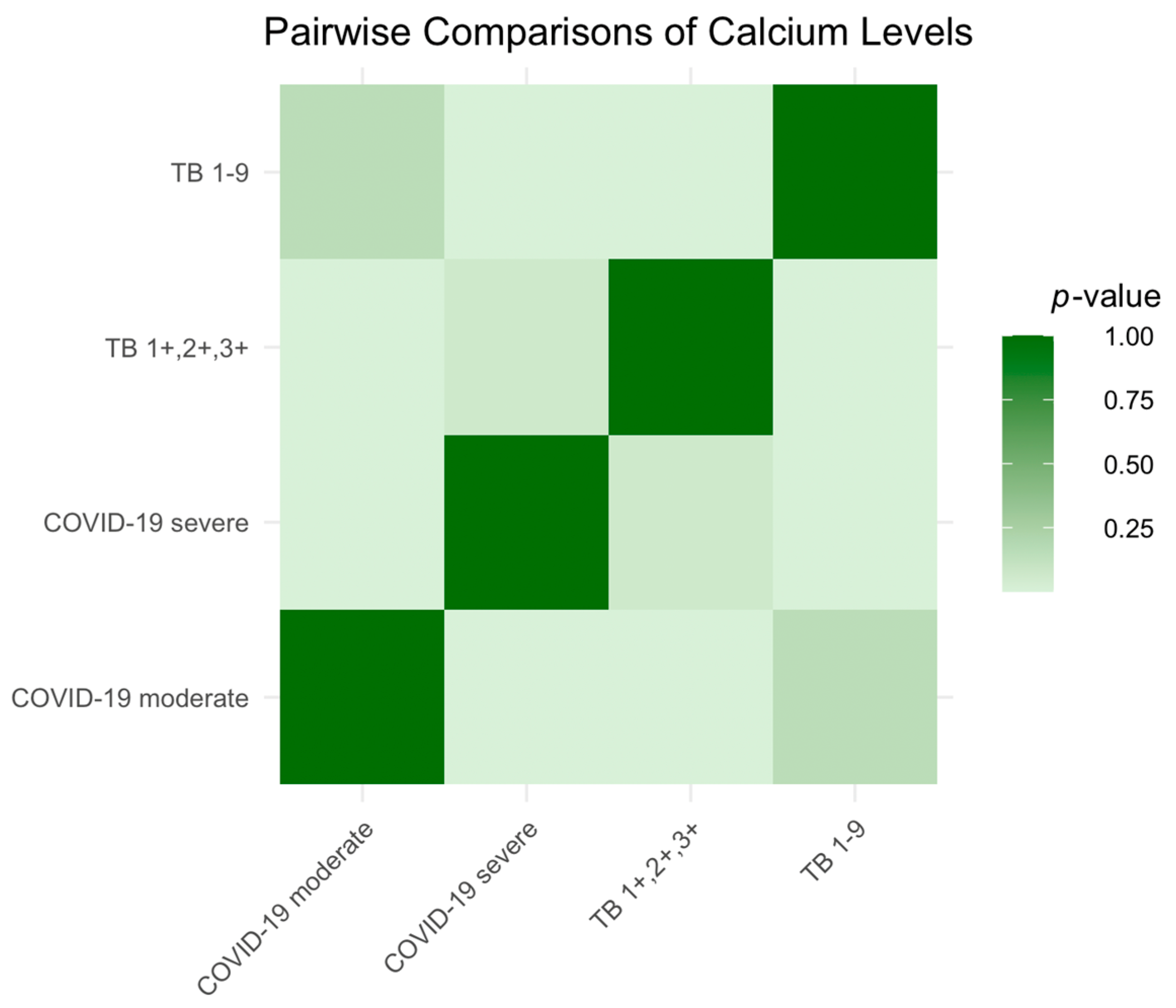
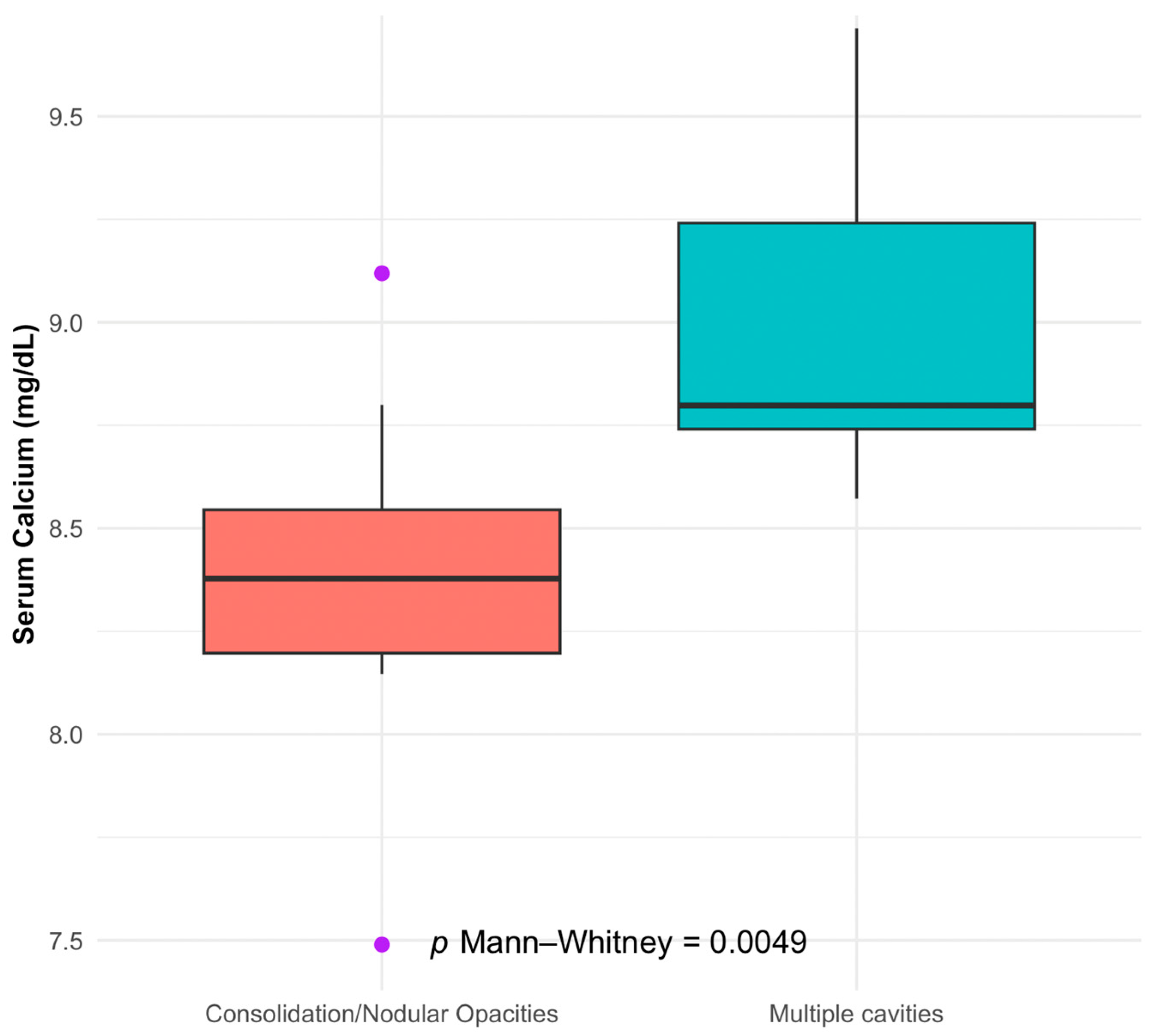
We identified several significant associations in our investigation of the correlations between electrolyte imbalances and disease severity in tuberculosis (TB) and COVID-19 patients. Our study found that patients with TB presenting with multiple cavities, indicative of more severe disease, had notably lower serum calcium levels. This relationship was statistically significant and suggests that serum calcium levels may be inversely correlated with the severity of TB’s radiological findings.
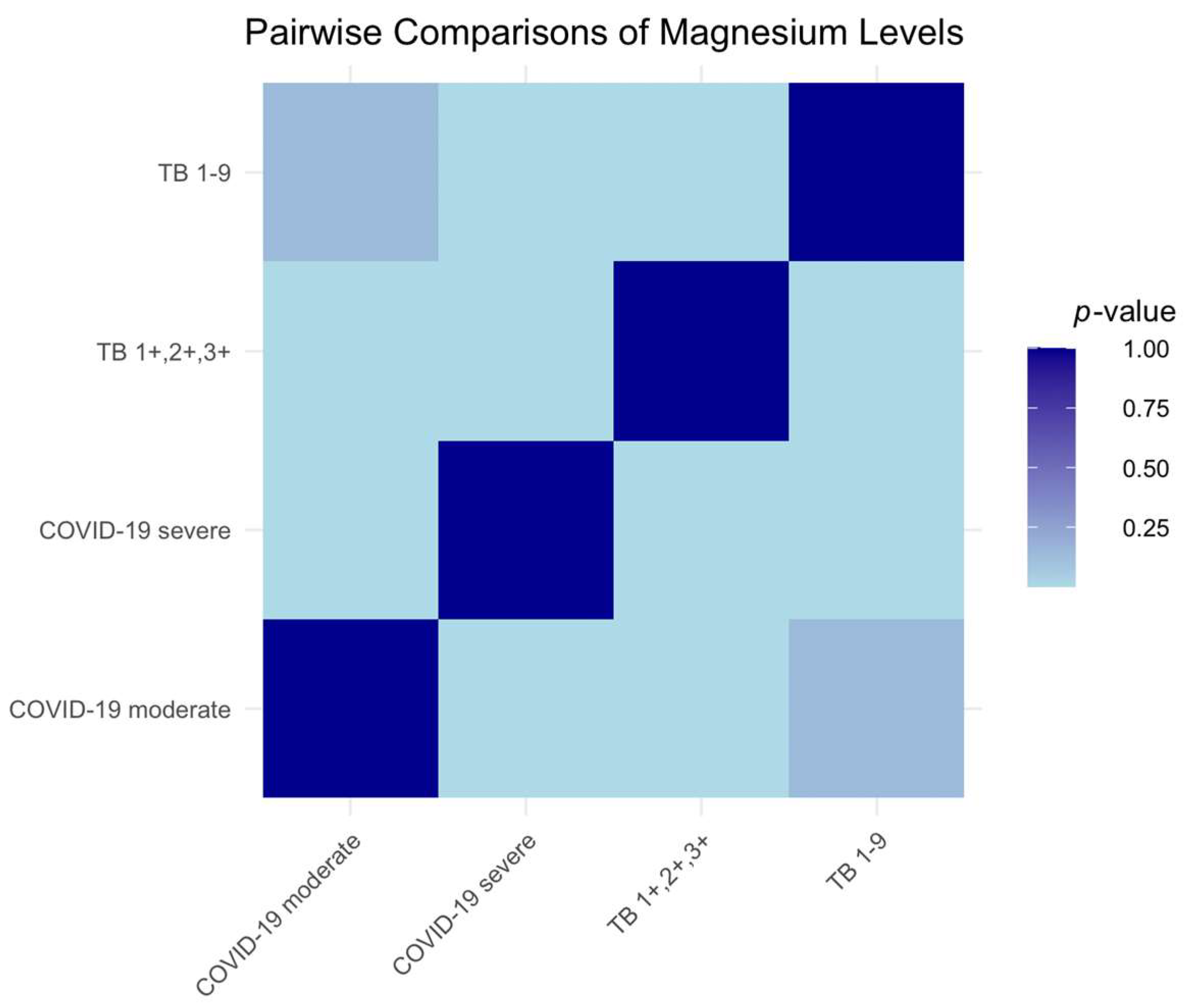
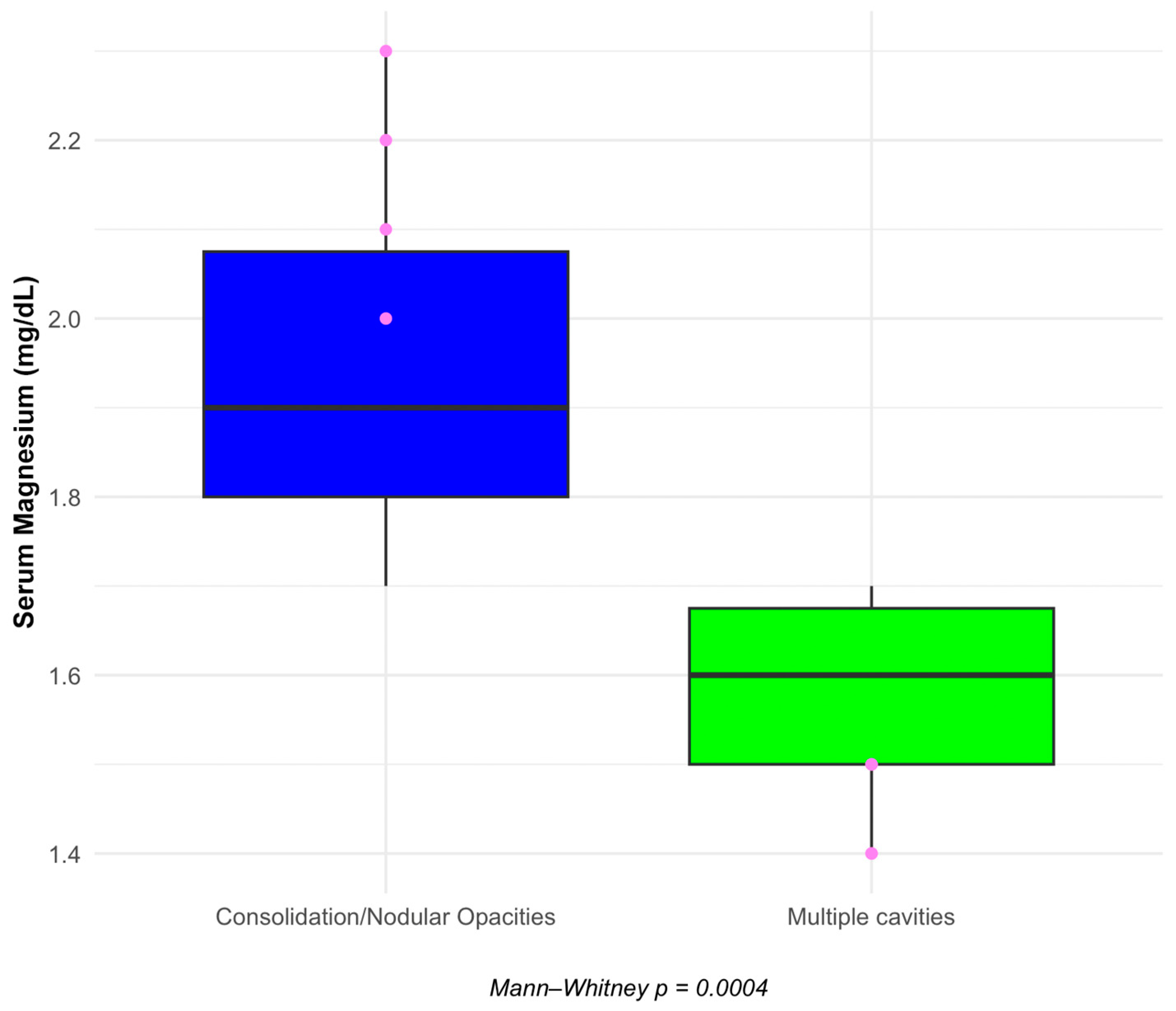
Additionally, we observed a highly significant difference in serum magnesium levels between the same patient groups. Those with more severe TB pathology, as denoted by the presence of multiple cavities, also demonstrated lower levels of serum magnesium, hinting at a potential role of this electrolyte in the pathophysiology of TB.
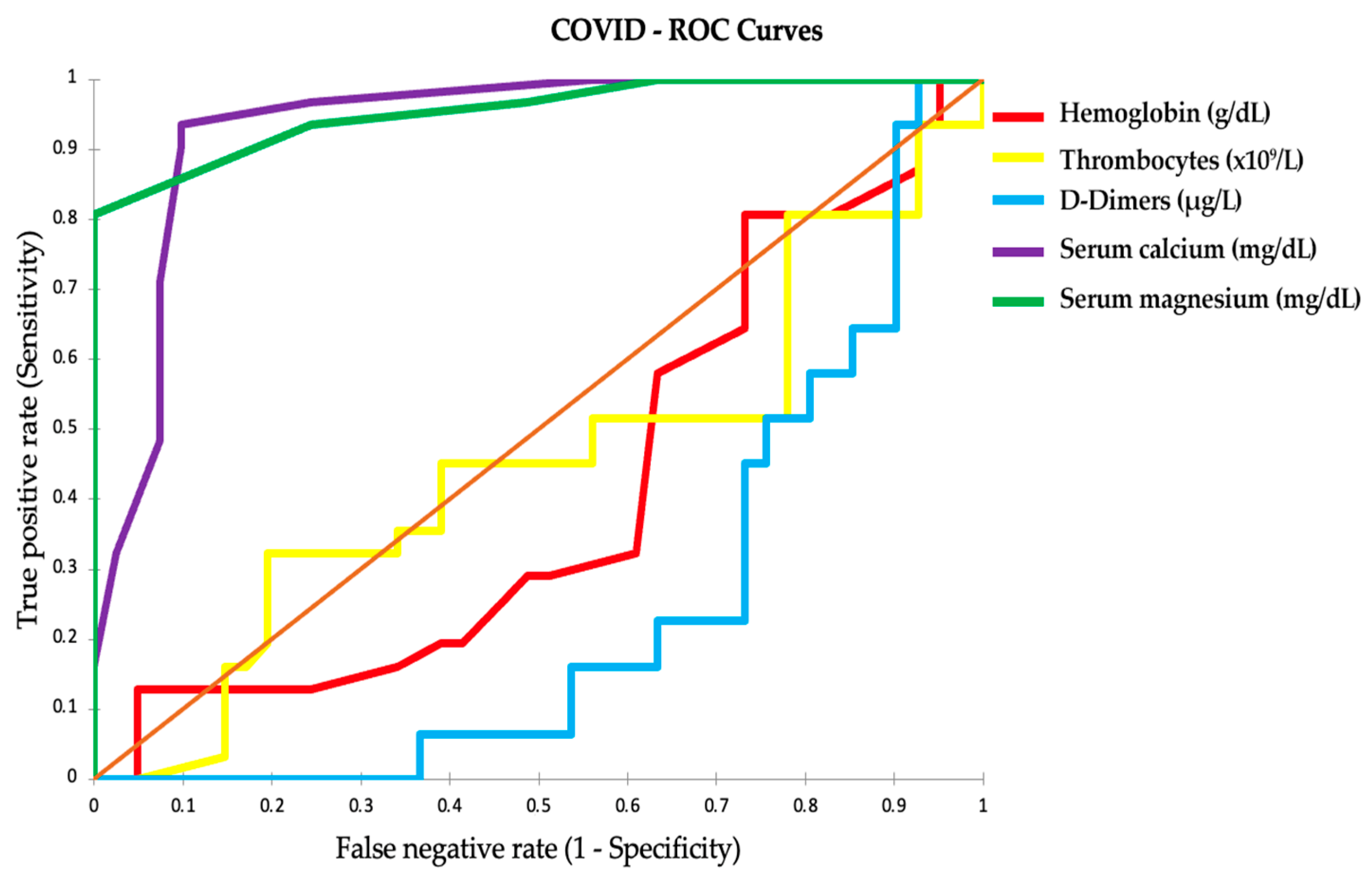
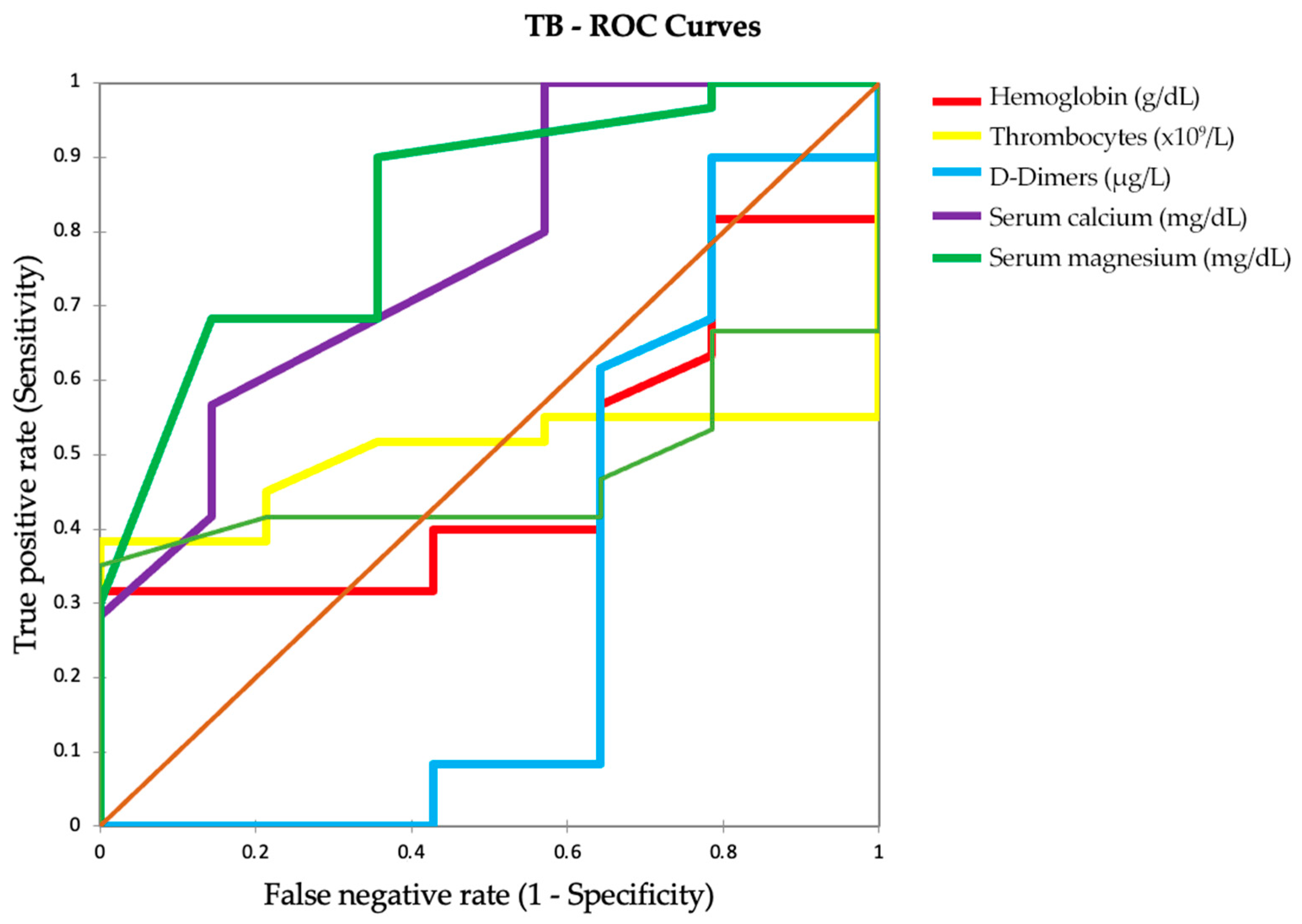
Our analysis extended to assessing various clinical parameters through ROC curves to distinguish between severe and moderate COVID-19 cases. The results pointed to serum calcium and serum magnesium as highly accurate predictors of disease severity, with AUC values close to 1. These electrolytes, D-dimer levels, and pulmonary function test results emerged as potential biomarkers of disease severity in COVID-19, with the latter offering additional insights into respiratory function impairment associated with the infection.
Overall, our findings emphasize the importance of monitoring serum calcium and serum magnesium levels in patients with TB and COVID-19 and suggest that these electrolytes, along with specific clinical parameters, could serve as significant indicators of disease severity, with potential implications for patient management and treatment strategies.
Based on a retrospective study by Zhou et al. [
20], involving 127 patients confirmed with COVID-19, a clear correlation was established between the severity of COVID-19 and low serum calcium levels. Their findings indicate that both mild/moderate and severe/critical cases of COVID-19 exhibited low serum calcium levels in the early stages of the infection. Notably, the severe/critical cases demonstrated significantly lower serum calcium levels than the mild/moderate cases at these early stages. Zhou et al. also observed that low serum calcium levels were associated with severe/critical multiorgan injuries, especially in the mild/moderate patient group. Furthermore, they found a correlation between changes in serum calcium levels and the pro-inflammatory cytokine IL-6 across both mild/moderate and severe/critical cases.
This study highlights the prevalence of low serum calcium as a common abnormality in COVID-19 patients, particularly those in severe or critical condition. This underscores the importance of serum calcium as a potential early-stage biomarker for assessing COVID-19 severity, linking it to multiorgan injuries and elevated levels of pro-inflammatory cytokines like IL-6.
These findings are consistent with those of our study, where patients with more severe forms of COVID-19 exhibited significantly lower serum calcium and serum magnesium levels. Our study expands upon Zhou et al.’s work by suggesting the potential of these electrolytes as biomarkers of disease severity in COVID-19. This broader scope encompasses the implications of electrolyte imbalances in COVID-19, reinforcing the clinical importance of monitoring these levels in patients with this disease.
Our results also support the study conducted by Alemzadeh et al. [
21], published in 2021, which systematically reviewed and meta-analyzed data on the impact of serum calcium levels on COVID-19 outcomes. Their investigation included 25 articles, revealing that 59% of COVID-19 patients experienced hypocalcemia. They found significant associations between hypocalcemia and the severity of COVID-19 (
p = 0.002), increased mortality (odds ratio (OR) = 6.99), extended hospitalization (
p < 0.001), and a higher likelihood of admission to the intensive care unit (OR = 5.09). Additionally, they observed a direct correlation between low serum calcium levels and elevated D-dimer levels (
p = 0.02) and reduced lymphocyte counts (
p = 0.007). Consequently, they concluded that lower serum calcium levels are linked to higher mortality and complications in COVID-19 patients, suggesting that serum calcium should be considered as a prognostic factor for disease severity and included in the initial patient assessments.
Guziejko et al. [
22] found no significant differences in PFTs between COVID-19 convalescents and a healthy control group. Still, they highlighted that COVID-19 patients with a persistent cough had decreased lung function parameters. At the same time, our study showed significant differences in FEV1 and FVC values among patients with severe and moderate COVID-19 and different TB stages. Both studies underscore the importance of PFTs in the follow-up of patients who have suffered from COVID-19, albeit with other implications. Our study suggests a need for differentiated follow-up strategies based on the severity of COVID-19 and TB. At the same time, Guziejko et al. recommend PFT for patients with persistent symptoms like cough, regardless of the initial severity of their COVID-19 infection.
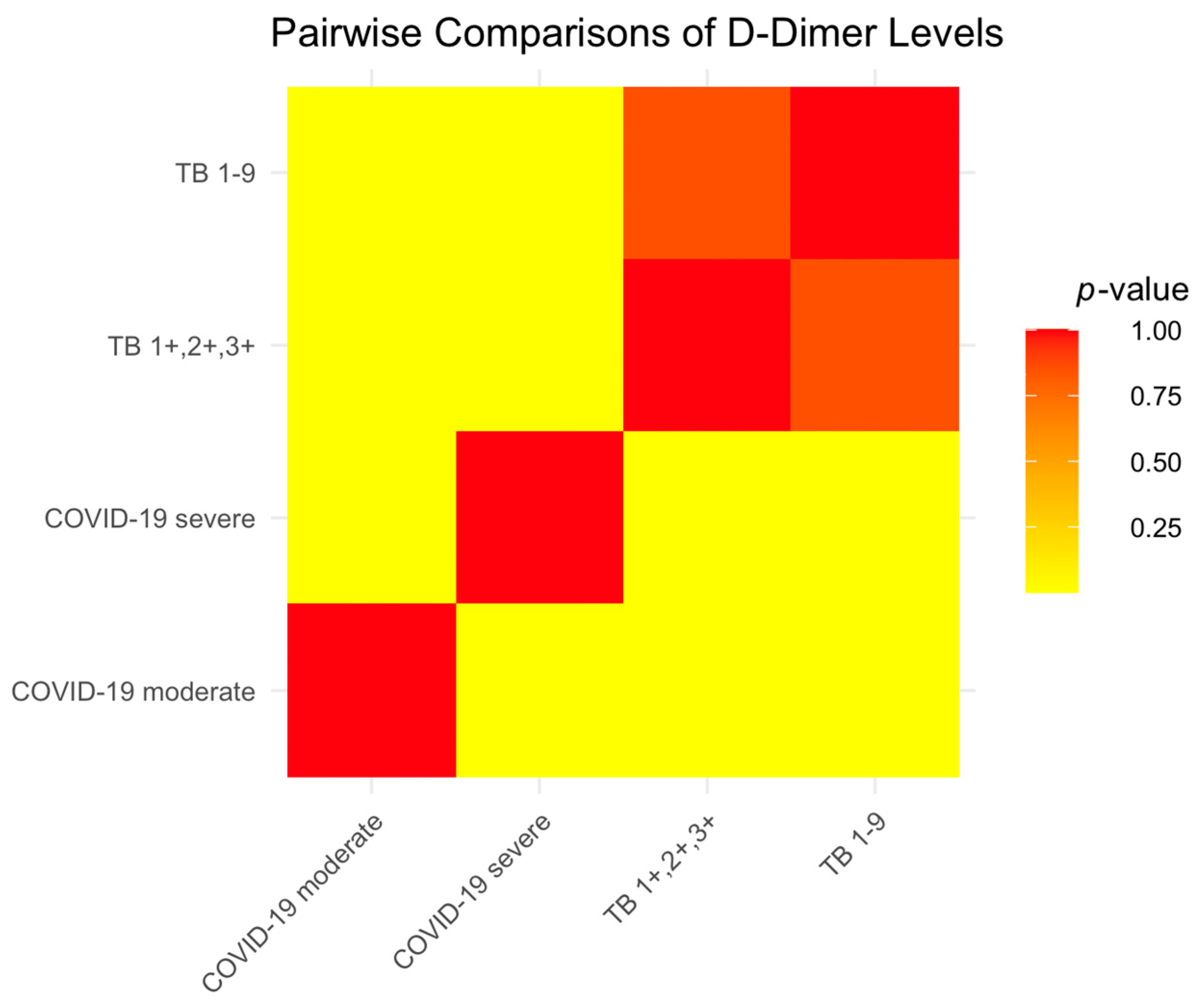
Coagulation abnormalities in COVID-19 patients often lead to the progression of the disease towards severe conditions and potentially fatal outcomes, a process marked by increased D-dimer levels and the formation of thrombi in both veins and arteries—elevated D-dimer in COVID-19 results from excessive clotting and low oxygen levels in the blood. Additionally, an increase in D-dimer levels is commonly seen in patients with severe COVID-19 and is significantly linked to higher mortality rates. As D-dimer is a breakdown product of fibrin, its presence serves as an indicator for the likelihood of pulmonary embolism and deep venous thrombosis (DVT) [
23,
24,
25].
The D-dimer levels observed in our study of COVID-19 patients were consistent with these established findings. We observed elevated D-dimer levels, particularly in patients with severe COVID-19, which is consistent with the model that higher D-dimer levels are associated with more severe disease and higher mortality risk. Consistent with its role as a fibrin degradation product, the elevated D-dimer levels in our cohort also suggest an increased risk of thrombotic complications such as pulmonary embolism and deep vein thrombosis, reinforcing its utility as a critical biomarker in the management of COVID-19.
The study by Baquri and Kora [
26] investigating the relationship between serum magnesium levels and pulmonary tuberculosis severity showed significant results. They observed a marked decrease in serum magnesium levels in patients with TB, which became more pronounced in the advanced stages of the disease. Their research concluded that serum magnesium levels were inversely correlated with TB severity, indicating its potential as a valuable biomarker for assessing disease progression. This inverse relationship suggests that the need for serum magnesium supplementation may increase as TB progresses, highlighting a potential area for therapeutic intervention.
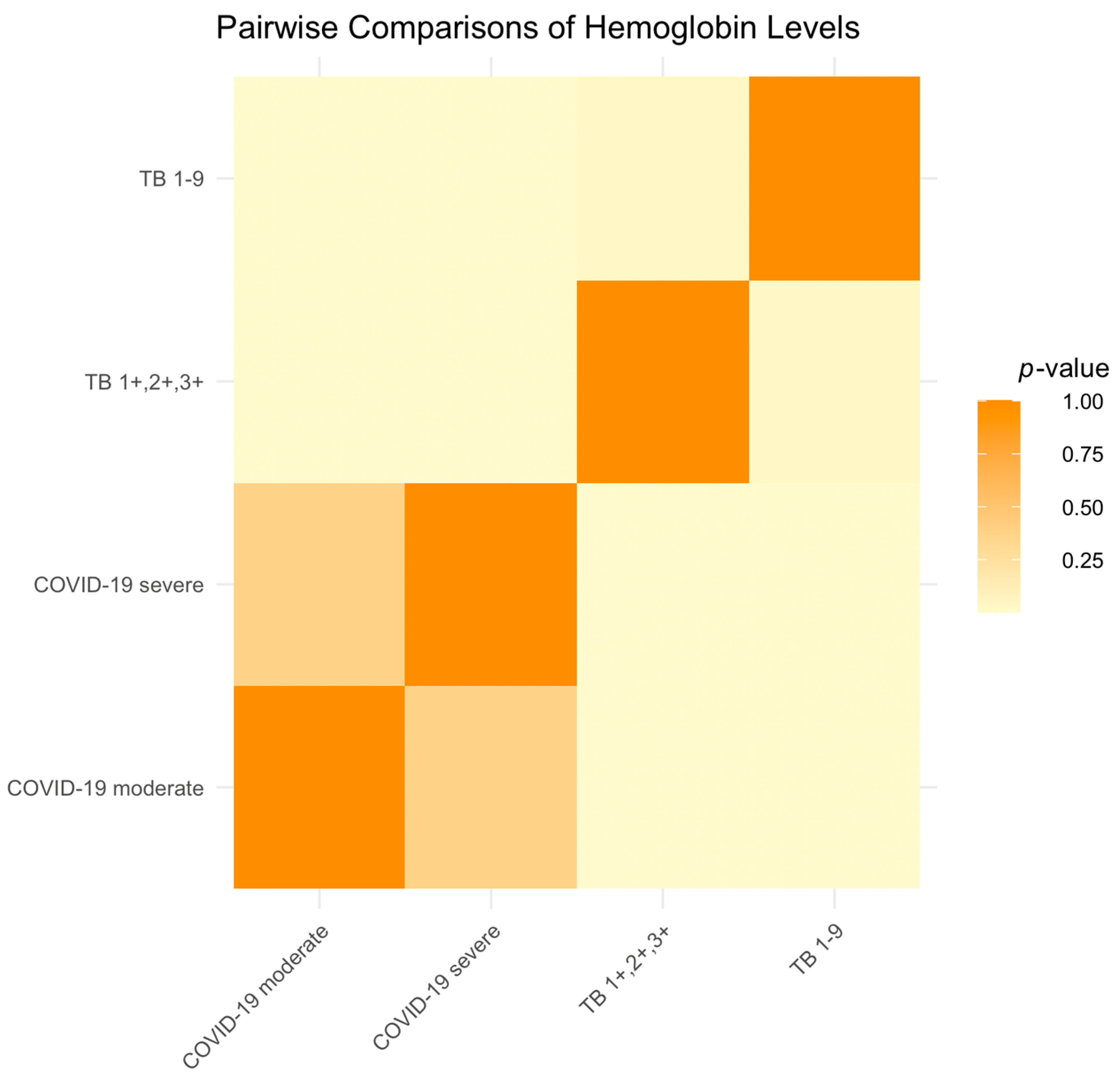
In comparison, our study investigated serum magnesium levels in different stages of TB, specifically in the TB 1-9 and TB1+,2+,3+ categories. Our findings revealed that while serum magnesium levels were lower in all TB patients, serum magnesium deficiency had a notable gradation correlating with the severity of TB. Patients in the TB1+,2+,3+ categories, representing more advanced stages of TB, exhibited more significant decreases in serum magnesium levels than those in the TB 1-9 category. This gradation further supports the hypothesis that serum magnesium levels could serve as an indicator of disease severity in TB patients. Our results are consistent with those of Baquri and Kora’s study, reinforcing the concept of serum magnesium levels as a potential biomarker of TB severity and suggesting the need for serum magnesium supplementation as part of TB treatment protocols, especially in more advanced cases.
The role of serum magnesium in the immune response, particularly its potential in mitigating disease severity, aligns with the observed decrease in serum magnesium levels in more advanced stages of TB in this study. This parallel suggests that serum magnesium deficiency might be a common thread in the progression of various infectious diseases, including TB and COVID-19.
Moreover, the potential therapeutic applications of serum magnesium, as indicated in Guerrero-Romero et al.’s study on COVID-19, could be relevant for TB. Considering the decrease in serum magnesium levels in advanced TB, exploring serum magnesium supplementation might be beneficial in managing TB, similar to its proposed role in COVID-19.
In summary, Guerrero-Romero et al.’s [
27] study underscores the importance of serum magnesium in infectious diseases. It provides a valuable reference point for discussing our findings on serum magnesium levels in TB patients. It highlights the potential of serum magnesium not only as a biomarker for disease severity, but also as a possible therapeutic avenue in managing diseases like TB and COVID-19.
As stated in recent research [
28], it is essential to underline the critical importance of addressing the challenges posed by COVID-19 and TB management, mainly focusing on prevention.
In addition to our findings, it is pertinent to consider the insights from a study published last year [
29]. This study underscores the long-term health effects of COVID-19 and the significance of conducting extended follow-up studies. Similar to our observations, the study revealed a range of persistent symptoms in COVID-19 patients post-discharge, including fatigue, cough, and myalgia. Notably, it was reported that many patients experienced various post-discharge symptoms, with durations extending between 19 and 26 days. The study also pointed out that patients with severe forms of COVID-19 exhibited more severe lung diffusion impairment and abnormalities in lung imaging. This is consistent with our findings, where severe COVID-19 cases demonstrated lower serum calcium and serum magnesium levels, pointing towards an intricate relationship between disease severity and electrolyte imbalances.
Furthermore, the study’s findings on post-COVID-19 syndrome (long COVID-19) as a multisystem disease with a complex long-term impact resonate with our observations. These insights emphasize the need for comprehensive recovery programs and multidisciplinary collaboration to manage post-COVID-19 patient health effectively. This holistic approach is crucial for addressing the multifaceted challenges posed by both COVID-19 and TB, underscoring the need for vigilant monitoring and tailored treatment strategies for patients afflicted with these diseases.
In the context of our study’s findings, it is crucial to consider the complexities of diagnosing COVID-19, as highlighted by Marginean et al. [
30]. Given the pandemic’s urgency, this study stresses the importance of prompt recognition, isolation, and rapid treatment in cases of suspected COVID-19. It underscores the risks of delayed diagnosis and treatment due to the similarity of COVID-19 symptoms and imaging to those of other systemic conditions. Notably, this study points out that one in five patients with respiratory symptoms may be diagnosed with an alternative condition, underlining the complexity and potential for misdiagnosis in the clinical setting. This is particularly significant in our study, which examined electrolyte imbalances in tuberculosis and COVID-19 patients, as it emphasizes the need for thorough clinical and radiological evaluation to avoid misdiagnosis. The analysis further elaborates on the progression of COVID-19 pneumonia to ARDS, characterized by patchy ground-glass confluent areas and pulmonary condensations on HRCT. These insights are particularly relevant to our study’s findings, as they provide a deeper understanding of the diagnostic challenges and the critical need for accurate differentiation between TB, COVID-19, and other respiratory conditions.
A study by Udristoiu et al. [
31] explored the association of severe COVID-19 with various clinical parameters and comorbidities. It was found that severe COVID-19 was significantly correlated with several factors: CXR severity; respiratory function parameters like oxygen saturation and respiratory rate; cardiovascular function indicators such as systolic and diastolic blood pressure and cardiac frequency; associated diseases, including diabetes, cardiac and kidney disease, hypertension, autoimmune thyroiditis, and obesity; and the presence of symptoms like coughing, headache, shortness of breath, and others. Moreover, hematological analysis showed a decrease in white blood cells and lymphocytes in cases of severe disease. These findings provide a comprehensive view of the multifactorial nature of severe COVID-19 and underline the complexity of managing patients with such diverse clinical presentations. This resonates with our study’s findings on the electrolyte imbalances in tuberculosis and COVID-19 patients, further emphasizing the intricate interplay of various clinical factors in these diseases.
While speculative, it is plausible to consider that the COVID-19 pandemic may have affected the serum magnesium status of the Romanian population, thereby influencing their susceptibility to tuberculosis. This hypothesis warrants further investigation, considering Romania’s high TB incidence.
4. Materials and Methods
4.1. Study Design and Population
This prospective study aimed to investigate correlations in disease severity between TB and COVID-19 patients, specifically focusing on serum calcium and serum magnesium levels and various pulmonary function parameters, such as FEV1, FVC, MEF 50, and the FEV1/FVC ratio.
The research was conducted at the Pneumoftiziology Clinic of Victor Babes Hospital in Craiova, Romania, chosen for its extensive patient records and advanced facilities for detailed pulmonary function testing.
Data were collected from December 2021 to July 2023, a period selected to ensure a comprehensive sample size and to capture relevant data during key phases of the COVID-19 pandemic. The study included 146 patients: 72 diagnosed with COVID-19 and 74 with TB, providing a balanced comparison between these groups.
Our study classified TB patients based on the Ziehl–Neelsen staining method and the quantity of acid-fast bacilli (AFB) observed under light/bright-field microscopy. This method categorizes TB infections by counting the number of AFB per microscopic field [
32]. The classifications are as follows:
TB 1-9 (0): negative for TB. This is used when no AFB are observed across approximately 300 visual fields spanning two lengths of the slide. It is reported as “0”.
TB scanty positive (1-9): low positive. When 1 to 9 AFB are found within a single length, the count is noted with a “+” sign before the number (e.g., +1, +2, up to +9). This indicates a low but detectable level of TB bacilli.
TB1+,2+,3+ (ranging from 1+ to 3+):
TB1+ (10–99 AFB in 1 length): mildly positive. This is reported as “1+” when 10 to 99 AFB are found in a single length, indicating a mildly positive result for TB.
TB2+ (1–10 AFB per field in at least 50 fields): moderately positive. This category reports 1 to 10 AFB per field in at least 50 visual fields as “2+”. This suggests a moderate level of TB infection.
TB3+ (more than 10 AFB per field in at least 20 fields): highly positive. The “3+” category is assigned when there are more than 10 AFB per field in at least 20 fields, indicating a highly infectious stage of TB.
Radiological findings were also incorporated to complement the TB classification. Multiple cavities observed in radiology indicated TB 1-9, while consolidations or nodular opacities were associated with the TB 1+, 2+, and 3+ categories, providing a more comprehensive understanding of TB severity.
Regarding the severity of illness in adults with SARS-CoV-2, we used the Treatment Guidelines in Coronavirus Disease 2019 [
33].
Asymptomatic or pre-symptomatic infection: Patients who test positive for SARS-CoV-2 but without symptoms related to COVID-19.
Mild illness: Patients present signs and symptoms like fever, cough, and headache but do not experience shortness of breath, dyspnea, or abnormal chest imaging.
Moderate illness: Usually characterized by clinical or radiographic evidence of lower respiratory tract disease, with a measured oxygen saturation (SpO2) ≥ 94% in ambient air at sea level.
Severe illness: Patients experiencing one or more of the following: oxygen saturation below 94% in room air, PaO2/FiO2 ratio below 300 mm Hg, respiratory rate above 30 breaths/min, or lung infiltrates over 50%.
Critical illness: The most severe form includes patients experiencing respiratory failure, septic shock, multiple organ dysfunction, the need for mechanical ventilation, and shock.
4.2. Inclusion and Exclusion Criteria
Our inclusion criteria were patients aged 18 and older with confirmed diagnoses of TB or COVID-19; as per standard diagnostic procedures for TB, this typically includes a positive sputum test for Mycobacterium tuberculosis and chest radiography; for COVID-19, this includes a positive RT-PCR test or rapid antigen test confirming SARS-CoV-2 infection.
Patients were required to have comprehensive medical records, including detailed laboratory results for serum calcium and serum magnesium levels and complete pulmonary function test data. The exclusion criteria were patients with chronic respiratory diseases such as COPD or asthma, which could independently affect the pulmonary function test results, and those with known electrolyte imbalances from causes other than TB or COVID-19. Patients with incomplete medical records or missing essential study data, along with those undergoing treatments that significantly affect serum calcium or serum magnesium levels, were also excluded.
4.3. Data Collection and Parameters
Data were collected from the patients’ medical records at the Pneumoftiziology Clinic. These included laboratory reports and pulmonary function test results. The parameters assessed were as follows:
D-dimers: Quantified to assess clot formation and breakdown, providing insights into coagulation abnormalities in TB and COVID-19.
Serum calcium levels: Measured due to serum calcium’s critical role in cellular signaling and structural functions; abnormal levels may indicate underlying pathophysiological processes.
Serum magnesium levels: Assessed for their importance in biochemical reactions and overall bodily functions.
Pulmonary function tests: Included FEV1, FVC, MEF 50, and the FEV1/FVC ratio, providing comprehensive insights into respiratory impact.
4.4. Follow-Up
Follow-up evaluations at 1 and 6 months post-diagnosis were conducted to track patient progression and changes in health status. These evaluations included repeat pulmonary function tests, allowing for comparative analysis over these periods.
4.5. Statistical Analysis
Statistical analysis was performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA) and the XLSTAT add-on for MS Excel (Addinsoft SARL, Paris, France). Data were recorded using Microsoft Excel files and then statistically analyzed to find the relationships between the variables of interest for the two groups of patients.
We used the Anderson–Darling and Shapiro–Wilk tests to test the normality of the data. Because the study involved numerical comparisons between groups of patients that did not have a normal (i.e., Gaussian) distribution, the nonparametric Kruskal–Wallis test was primarily used, instead of the ANOVA test, to detect significant differences between the values in the compared data series. If statistically significant differences were detected between the analyzed groups, the Dunn procedure for pairwise comparisons was used to discover the groups with significant differences.



 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}