
Altered Gene Expression of IL-35 and IL-36α in the Skin of Patients with Atopic Dermatitis
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Demographic Data
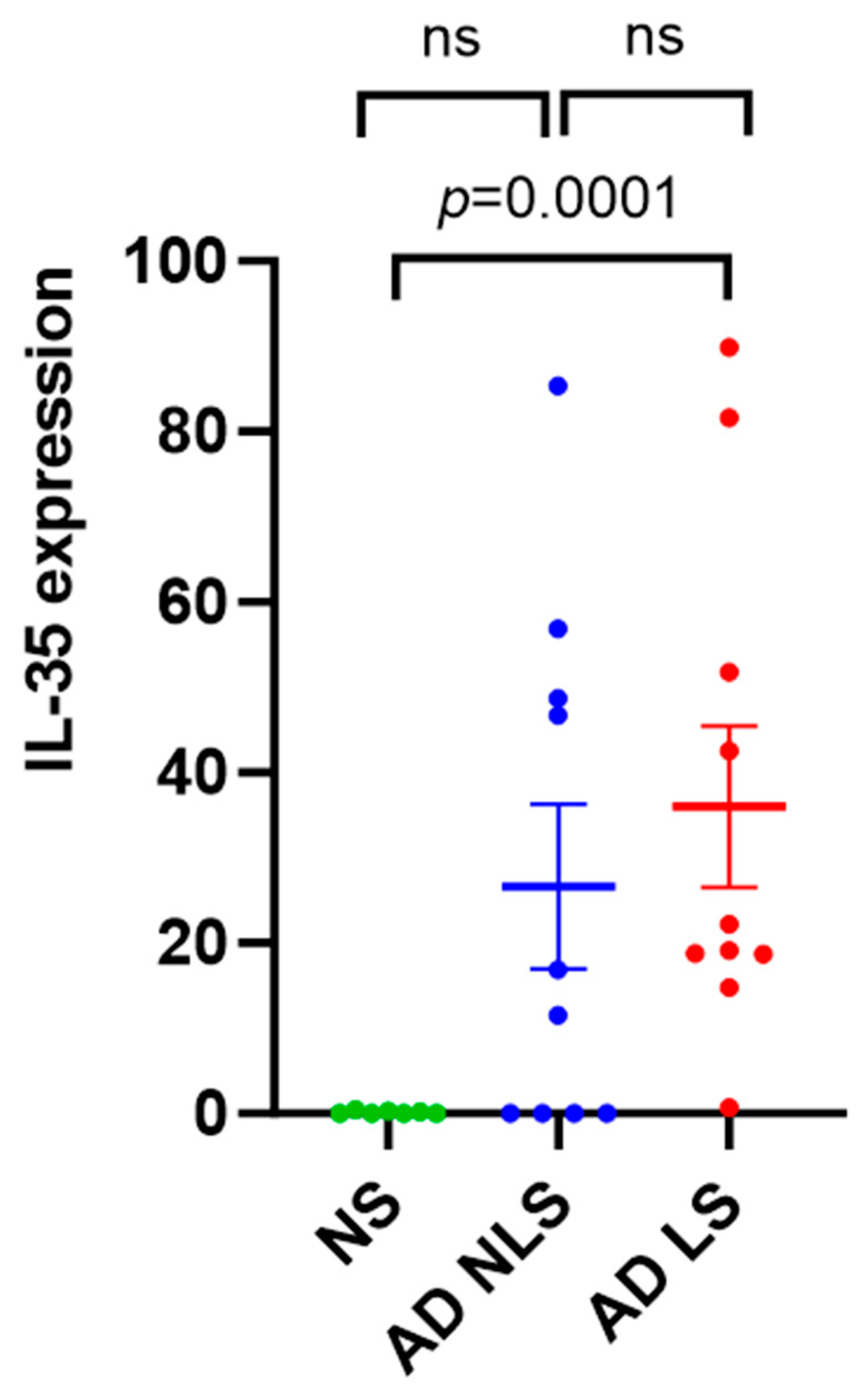
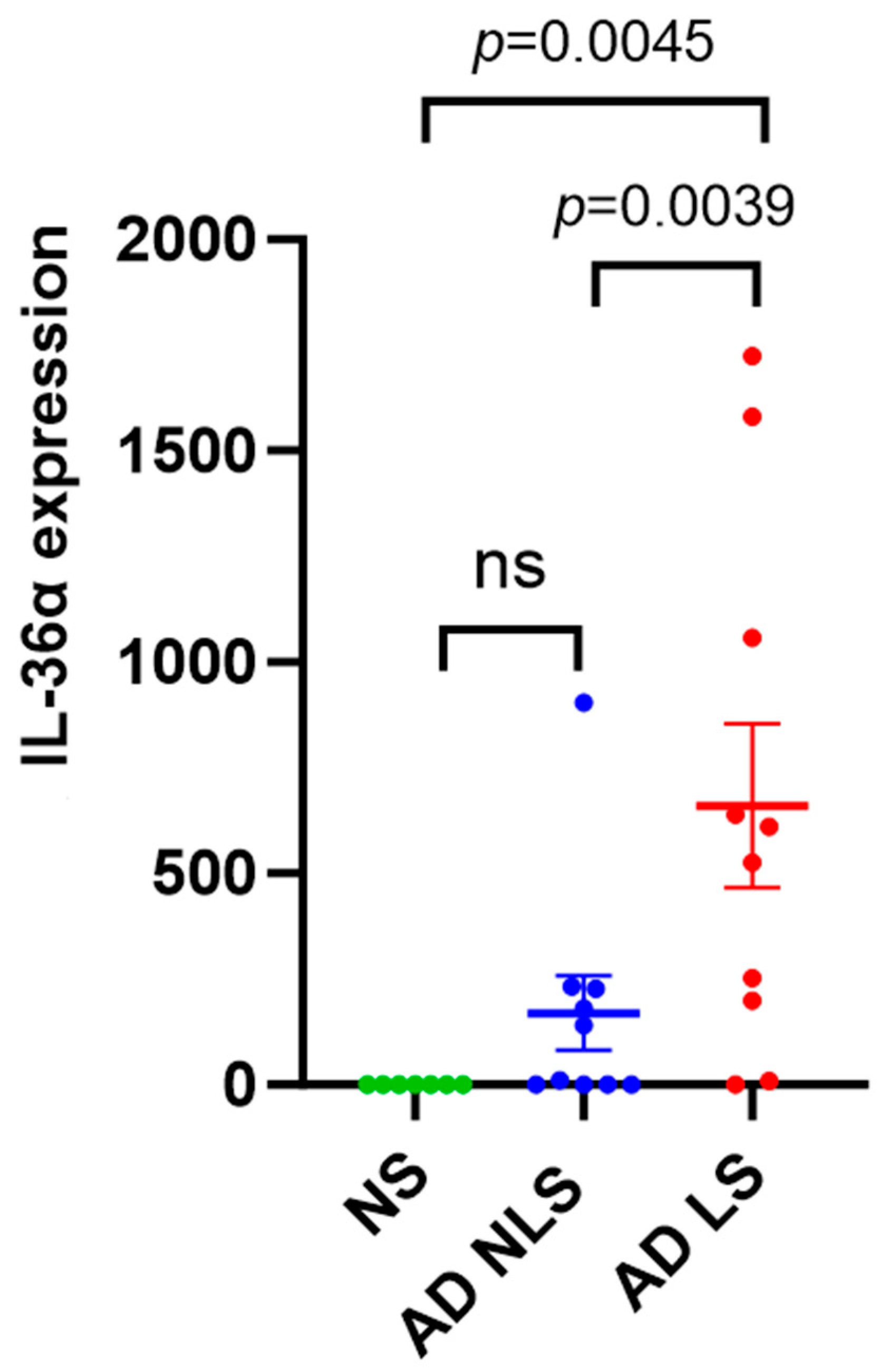
2.2. The Expression Level of IL-35 and IL-36α in Tape Strips from Lesional AD Skin, Nonlesional AD Skin, and Healthy Control Skin
2.3. Correlations of the Expression Level of IL-35 and IL-36α with Clinical Features of AD
3. Discussion
4. Material and Methods
4.1. Patients
4.2. Determination of AD Severity
4.3. Tissue Sampling and Analysis
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sroka-Tomaszewska, J.; Trzeciak, M. Molecular Mechanisms of Atopic Dermatitis Pathogenesis. Int. J. Mol. Sci. 2021, 22, 4130. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.; Jaworski, J.C.; Simpson, E.L.; Boguniewicz, M.; Russell, J.J.; Block, J.K.; Tofte, S.; Dunn, J.D.; Feldman, S.R.; Clark, A.R.; et al. Major Comorbidities of Atopic Dermatitis: Beyond Allergic Disorders. Am. J. Clin. Dermatol. 2018, 19, 821–838. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I. Comorbidities and the impact of atopic dermatitis. Ann. Allergy Asthma Immunol. 2019, 123, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Facheris, P.; Jeffery, J.; Del Duca, E.; Guttman-Yassky, E. The translational revolution in atopic dermatitis: The paradigm shift from pathogenesis to treatment. Cell. Mol. Immunol. 2023, 20, 448–474. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kim, S.E.; Shin, K.O.; Park, K.; Lee, S.E. Dupilumab Therapy Improves Stratum Corneum Hydration and Skin Dysbiosis in Patients with Atopic Dermatitis. Allergy Asthma Immunol. Res. 2021, 13, 762. [Google Scholar] [CrossRef] [PubMed]
- Deleuran, M.; Thaçi, D.; Beck, L.A.; de Bruin-Weller, M.; Blauvelt, A.; Forman, S.; Bissonnette, R.; Reich, K.; Soong, W.; Hussain, I.; et al. Dupilumab shows long-term safety and efficacy in patients with moderate to severe atopic dermatitis enrolled in a phase 3 open-label extension study. J. Am. Acad. Dermatol. 2020, 82, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Cork, M.J.; Eckert, L.; Simpson, E.L.; Armstrong, A.; Barbarot, S.; Puig, L.; Girolomoni, G.; de Bruin-Weller, M.; Wollenberg, A.; Kataoka, Y.; et al. Dupilumab improves patient-reported symptoms of atopic dermatitis, symptoms of anxiety and depression, and health-related quality of life in moderate-to-severe atopic dermatitis: Analysis of pooled data from the randomized trials SOLO 1 and SOLO 2. J. Dermatol. Treat. 2020, 31, 606–614. [Google Scholar] [CrossRef]
- Miniotti, M.; Ribero, S.; Mastorino, L.; Ortoncelli, M.; Gelato, F.; Bailon, M.; Trioni, J.; Stefan, B.; Quaglino, P.; Leombruni, P. Long-term psychological outcome of patients with moderate-to-severe atopic dermatitis continuously treated with Dupilumab: Data up to 3 years. Exp. Dermatol. 2023, 32, 852–858. [Google Scholar] [CrossRef]
- Mastorino, L.; Duò, V.L.C.; Vecco, C.; Gelato, F.; Giordano, S.; Roccuzzo, G.; Cavaliere, G.; Avallone, G.; Ortoncelli, M.; Ribero, S.; et al. Impact of comorbidities in the response of atopic patients treated with dupilumab: A real-life study up to 36 weeks. J. Eur. Acad. Dermatol. Venereol. 2022, 36, E1021–E1023. [Google Scholar] [CrossRef]
- Klonowska, J.; Gleń, J.; Nowicki, R.J.; Trzeciak, M. New Cytokines in the Pathogenesis of Atopic Dermatitis—New Therapeutic Targets. Int. J. Mol. Sci. 2018, 19, 3086. [Google Scholar] [CrossRef]
- Zysk, W.; Gleń, J.; Trzeciak, M. Current Insight into the Role of IL-35 and Its Potential Involvement in the Pathogenesis and Therapy of Atopic Dermatitis. Int. J. Mol. Sci. 2022, 23, 15709. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Yano, H.; Workman, C.J.; Vignali, D.A.A. Interleukin-35: Structure, Function and Its Impact on Immune-Related Diseases. J. Interf. Cytokine Res. 2021, 41, 391–406. [Google Scholar] [CrossRef] [PubMed]
- Gürkan, A.; Yücel, A.A.; Sönmez, C.; Keleş, Ş.; Bostancı, İ. Serum Cytokine Profiles in Infants with Atopic Dermatitis. Acta Dermatovenerol. Croat. 2016, 24, 268–273. [Google Scholar] [PubMed]
- Kiwan, A.H.; Mohamed, H.A.K.; Hashim, O.A.E.; Abd-Elraheem, S.I.; Alkhrsawy, A.M. Pro-Inflammatory versus Anti-Inflammatory cytokines in atopic dermatitis patients: A case control study. J. Cosmet. Dermatol. 2022, 21, 6163–6168. [Google Scholar] [CrossRef] [PubMed]
- Sachen, K.L.; Greving, C.N.A.; Towne, J.E. Role of IL-36 cytokines in psoriasis and other inflammatory skin conditions. Cytokine 2022, 156, 155897. [Google Scholar] [CrossRef] [PubMed]
- Tsoi, L.C.; Rodriguez, E.; Stölzl, D.; Wehkamp, U.; Sun, J.; Gerdes, S.; Sarkar, M.K.; Hübenthal, M.; Zeng, C.; Uppala, R.; et al. Progression of acute-to-chronic atopic dermatitis is associated with quantitative rather than qualitative changes in cytokine responses. J. Allergy Clin. Immunol. 2020, 145, 1406–1415. [Google Scholar] [CrossRef]
- Otobe, S.; Sugaya, M.; Nakajima, R.; Oka, T.; Takahashi, N.; Kabasawa, M.; Miyagaki, T.; Asano, Y.; Sato, S. Increased interleukin-36γ expression in skin and sera of patients with atopic dermatitis and mycosis fungoides/Sézary syndrome. J. Dermatol. 2018, 45, 468–471. [Google Scholar] [CrossRef]
- Suárez-Fariñas, M.; Ungar, B.; da Rosa, J.C.; Ewald, D.A.; Rozenblit, M.; Gonzalez, J.; Xu, H.; Zheng, X.; Peng, X.; Estrada, Y.D.; et al. RNA sequencing atopic dermatitis transcriptome profiling provides insights into novel disease mechanisms with potential therapeutic implications. J. Allergy Clin. Immunol. 2015, 135, 1218–1227. [Google Scholar] [CrossRef]
- Komaki, R.; Miyagaki, T.; Tanaka, M.; Nakajima, K.; Okano, T.; Takeuchi, S.; Kadono, T. Increased Interleukin-36β Expression Promotes Angiogenesis in Japanese Atopic Dermatitis. Int. J. Mol. Sci. 2023, 24, 11104. [Google Scholar] [CrossRef]
- Lang, C.C.V.; Renert-Yuval, Y.; Del Duca, E.; Pavel, A.B.; Wu, J.; Zhang, N.; Dubin, C.; Obi, A.; Chowdhoury, M.; Kim, M.; et al. Immune and barrier characterization of atopic dermatitis skin phenotype in Tanzanian patients. Ann. Allergy Asthma Immunol. 2021, 127, 334–341. [Google Scholar] [CrossRef]
- Liu, H.; Archer, N.K.; Dillen, C.A.; Wang, Y.; Ashbaugh, A.G.; Ortines, R.V.; Kao, T.; Lee, S.K.; Cai, S.S.; Miller, R.J.; et al. Staphylococcus aureus Epicutaneous Exposure Drives Skin Inflammation via IL-36-Mediated T Cell Responses. Cell Host Microbe 2017, 22, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Gresnigt, M.S.; van de Veerdonk, F.L. Biology of IL-36 cytokines and their role in disease. Semin. Immunol. 2013, 25, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Tawfik, S.S.; Baruah, K.P.; O’toole, E.A.; O’shaughnessy, R.F.L. Tape strips in dermatology research. Br. J. Dermatol. 2021, 185, 26–35. [Google Scholar] [CrossRef]
- Keurentjes, A.J.; Jakasa, I.; Kezic, S. Research Techniques Made Simple: Stratum Corneum Tape Stripping. J. Investig. Dermatol. 2021, 141, 1129–1133. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.E.; Goleva, E.; Kim, P.S.; Norquest, K.; Bronchick, C.; Taylor, P.; Leung, D.Y. Side-by-Side Comparison of Skin Biopsies and Skin Tape Stripping Highlights Abnormal Stratum Corneum in Atopic Dermatitis. J. Investig. Dermatol. 2019, 139, 2387–2389. [Google Scholar] [CrossRef] [PubMed]
- Bieber, T. Interleukin-13: Targeting an underestimated cytokine in atopic dermatitis. Allergy 2020, 75, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Mai, J.; Virtue, A.; Yin, Y.; Gong, R.; Sha, X.; Gutchigian, S.; Frisch, A.; Hodge, I.; Jiang, X.; et al. IL-35 Is a Novel Responsive Anti-inflammatory Cytokine—A New System of Categorizing Anti-inflammatory Cytokines. PLoS ONE 2012, 7, e33628. [Google Scholar] [CrossRef]
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef]
- Fania, L.; Moretta, G.; Antonelli, F.; Scala, E.; Abeni, D.; Albanesi, C.; Madonna, S. Multiple Roles for Cytokines in Atopic Dermatitis: From Pathogenic Mediators to Endotype-Specific Biomarkers to Therapeutic Targets. Int. J. Mol. Sci. 2022, 23, 2684. [Google Scholar] [CrossRef]
- Owczarczyk-Saczonek, A.; Czerwińska, J.; Orylska, M.; Placek, W. Evaluation of selected mechanisms of immune tolerance in psoriasis. Adv. Dermatol. Allergol. 2019, 36, 319–328. [Google Scholar] [CrossRef]
- Agrawal, R.; Wisniewski, J.A.; Woodfolk, J.A. The Role of Regulatory T Cells in Atopic Dermatitis. Pathog. Manag. Atopic Dermat. 2011, 41, 112–124. [Google Scholar] [CrossRef]
- Szegedi, A.; Baráth, S.; Nagy, G.; Szodoray, P.; Gál, M.; Sipka, S.; Bagdi, E.; Banham, A.; Krenács, L. Regulatory T cells in atopic dermatitis: Epidermal dendritic cell clusters may contribute to their local expansion. Br. J. Dermatol. 2009, 160, 984–993. [Google Scholar] [CrossRef] [PubMed]
- Roesner, L.M.; Floess, S.; Witte, T.; Olek, S.; Huehn, J.; Werfel, T. Foxp3+ regulatory T cells are expanded in severe atopic dermatitis patients. Allergy 2015, 70, 1656–1660. [Google Scholar] [CrossRef] [PubMed]
- Madonna, S.; Girolomoni, G.; Dinarello, C.A.; Albanesi, C. The Significance of IL-36 Hyperactivation and IL-36R Targeting in Psoriasis. Int. J. Mol. Sci. 2019, 20, 3318. [Google Scholar] [CrossRef] [PubMed]
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Prim. 2018, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Abramovits, W.; Proulx, É.S.-C.; Lee, P.; Guttman-Yassky, E.; Zovko, E.; Sigmund, R.; Willcox, J.; Bieber, T. Spesolimab, an anti-interleukin-36 receptor antibody, in patients with moderate-to-severe atopic dermatitis: Results from a multicentre, randomized, double-blind, placebo-controlled, phase IIa study. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Tsang, M.S.-M.; Sun, X.; Wong, C.K. The Role of New IL-1 Family Members (IL-36 and IL-38) in Atopic Dermatitis, Allergic Asthma, and Allergic Rhinitis. Curr. Allergy Asthma Rep. 2020, 20, 40. [Google Scholar] [CrossRef] [PubMed]
- Mikhaylov, D.B.; Del Duca, E.; Olesen, C.M.; He, H.; Wu, J.B.; Ungar, B.; Estrada, Y.B.; Zhang, N.; Chowdhury, M.; Clausen, M.-L.; et al. Transcriptomic Profiling of Tape-Strips From Moderate to Severe Atopic Dermatitis Patients Treated with Dupilumab. Dermatitis 2021, 32, S71–S80. [Google Scholar] [CrossRef]
- Pavel, A.B.; Renert-Yuval, Y.; Wu, J.; Del Duca, E.; Diaz, A.; Lefferdink, R.; Fang, M.M.; Canter, T.; Rangel, S.M.; Zhang, N.; et al. Tape strips from early-onset pediatric atopic dermatitis highlight disease abnormalities in nonlesional skin. Allergy 2021, 76, 314–325. [Google Scholar] [CrossRef]
- Andersson, A.M.; Sølberg, J.; Koch, A.; Skov, L.; Jakasa, I.; Kezic, S.; Thyssen, J.P. Assessment of biomarkers in pediatric atopic dermatitis by tape strips and skin biopsies. Allergy 2022, 77, 1499–1509. [Google Scholar] [CrossRef]
- He, H.; Bissonnette, R.; Wu, J.; Diaz, A.; Proulx, E.S.-C.; Maari, C.; Jack, C.; Louis, M.; Estrada, Y.; Krueger, J.G.; et al. Tape strips detect distinct immune and barrier profiles in atopic dermatitis and psoriasis. J. Allergy Clin. Immunol. 2021, 147, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Dyjack, N.; Goleva, E.; Rios, C.; Kim, B.E.; Bin, L.; Taylor, P.; Bronchick, C.; Hall, C.F.; Richers, B.N.; Seibold, M.A.; et al. Minimally invasive skin tape strip RNA sequencing identifies novel characteristics of the type 2–high atopic dermatitis disease endotype. J. Allergy Clin. Immunol. 2018, 141, 1298–1309. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.M.; Rajka, G. Diagnostic Features of Atopic Dermatitis. Acta Derm.-Venereol. 1980, 60, 44–47. [Google Scholar] [CrossRef]
- Chopra, R.; Vakharia, P.P.; Sacotte, R.; Patel, N.; Immaneni, S.; White, T.; Kantor, R.; Hsu, D.; Silverberg, J. Severity strata for Eczema Area and Severity Index (EASI), modified EASI, Scoring Atopic Dermatitis (SCORAD), objective SCORAD, Atopic Dermatitis Severity Index and body surface area in adolescents and adults with atopic dermatitis. Br. J. Dermatol. 2017, 177, 1316–1321. [Google Scholar] [CrossRef]
- Leshem, Y.A.; Hajar, T.; Hanifin, J.M.; Simpson, E.L. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: An interpretability study. Br. J. Dermatol. 2015, 172, 1353–1357. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | AD Patients (n = 10) | Healthy Controls (n = 7) |
|---|---|---|
| Sex, n (%) | ||
| Female | 4 (40.0%) | 3 (42.9%) |
| Male | 6 (60.0%) | 4 (57.1%) |
| Age, mean ± SD | 26 ± 13.5 | 30 ± 5.6 |
| AD severity according to SCORAD, n (%) | - | |
| Mild (SCORAD < 25) | 3 (33.3%) | |
| Moderate (SCORAD 25–50) | 5 (55.6%) | |
| Severe (SCORAD > 50) | 1 (11.1%) 1 | |
| AD severity according to EASI, n (%) | - | |
| Clear (EASI 0) | 0 (0.0%) | |
| Almost clear (EASI 0.1–1.0) | 0 (0.0%) | |
| Mild (EASI 1.1–7.0) | 0 (0.0%) | |
| Moderate (EASI 7.1–21.0) | 4 (40.0%) | |
| Severe (EASI 21.1–50.0) | 5 (50.0%) | |
| Very severe (EASI 50.1–72.0) | 1 (10.0%) | |
| Pruritus, mean ± SD | 6.0 ± 2.05 | - |
| Sleep loss, mean ± SD | 5.4 ± 2.8 | - |
| Atopic comorbidities, n (%) | - | |
| Allergic rhinitis | 5 (50.0%) | |
| Allergic conjunctivitis | 1 (10.0%) | |
| Asthma | 5 (10.0%) | |
| Eosinophilia, n (%) * | - | |
| Yes | 5 (55.6%) | |
| No | 4 (44.4%) 2 |
| SCORAD | EASI | VAS | Sleep | Eosinophilia | AR | AC | Asthma | |
|---|---|---|---|---|---|---|---|---|
| Nonlesional IL-35 | R = −0.89 | R = −0.90 | R = −0.33 | R = −0.22 | R = 0.52 | R = 0.03 | R = −0.06 | R = −0.03 |
| p = 0.004 | p = 0.002 | p = 0.358 | p = 0.540 | p = 0.190 | p = 1.0 | p = 1.0 | p = 1.0 | |
| Lesional IL-35 | R = −0.58 | R = −0.66 | R = −0.33 | R = −0.60 | R = 0.17 | R = −0.10 | R = −0.29 | R = 0.17 |
| p = 0.115 | p = 0.048 | p = 0.348 | p = 0.072 | p = 0.730 | p = 0.841 | p = 0.60 | p = 0.690 | |
| Nonlesional IL-36α | R = 0.02 | R = −0.04 | R = −0.18 | R = −0.006 | R = 0.0 | R = 0.10 | R = −0.41 | R = −0.59 |
| p = 0.980 | p = 0.932 | p = 0.623 | p = 0.993 | p = 1.0 | p = 0.841 | p = 0.40 | p = 0.095 | |
| Lesional IL-36α | R = 0.13 | R = 0.02 | R = −0.28 | R = 0.32 | R = 0.35 | R = −0.10 | R = −0.52 | R = −0.45 |
| p = 0.754 | p = 0.976 | p = 0.438 | p = 0.368 | p = 0.413 | p = 0.841 | p = 0.20 | p = 0.222 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zysk, W.; Sitko, K.; Tukaj, S.; Zaryczańska, A.; Trzeciak, M. Altered Gene Expression of IL-35 and IL-36α in the Skin of Patients with Atopic Dermatitis. Int. J. Mol. Sci. 2024, 25, 404. https://doi.org/10.3390/ijms25010404
Zysk W, Sitko K, Tukaj S, Zaryczańska A, Trzeciak M. Altered Gene Expression of IL-35 and IL-36α in the Skin of Patients with Atopic Dermatitis. International Journal of Molecular Sciences. 2024; 25(1):404. https://doi.org/10.3390/ijms25010404
Chicago/Turabian StyleZysk, Weronika, Krzysztof Sitko, Stefan Tukaj, Anna Zaryczańska, and Magdalena Trzeciak. 2024. "Altered Gene Expression of IL-35 and IL-36α in the Skin of Patients with Atopic Dermatitis" International Journal of Molecular Sciences 25, no. 1: 404. https://doi.org/10.3390/ijms25010404
APA StyleZysk, W., Sitko, K., Tukaj, S., Zaryczańska, A., & Trzeciak, M. (2024). Altered Gene Expression of IL-35 and IL-36α in the Skin of Patients with Atopic Dermatitis. International Journal of Molecular Sciences, 25(1), 404. https://doi.org/10.3390/ijms25010404