
Incidental Bystander or Essential Culprit: A Systematic Review of Bacterial Significance in the Pathogenesis of Breast Implant-Associated Anaplastic Large Cell Lymphoma
 , , ,
, , , 
Abstract
:1. Introduction
2. Method
2.1. Eligibility Criteria
- Female adult population 18 years and above
- Female with BIA-ALCL or suspicion of BIA-ALCL
- Animal, cadaveric, or experimental studies on BIA-ALCL
- Studies on BIA-ALCL investigating BF or bacteria
- Studies in English and studies translated to English
- Editorials, commentary reports, abstracts, and letters to the editors
- Studies conducted in patients with history of non-Hodgkin lymphoma or Hodgkin lymphoma
2.2. Search Strategy
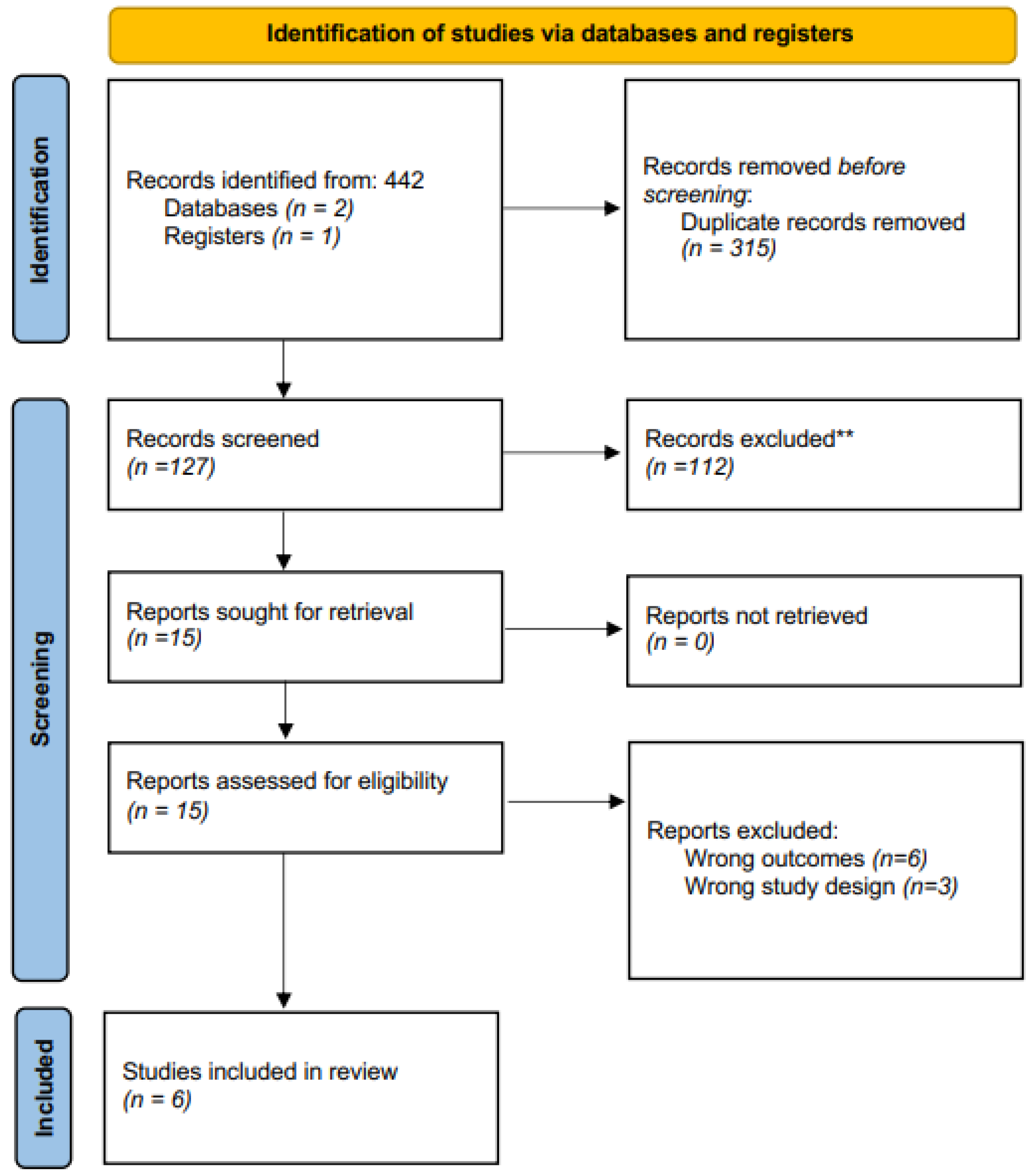
2.3. Study Selection
2.4. Data Extraction/Synthesis
2.5. Outcomes
2.6. Quality Assessment
2.7. Statistical Analysis
3. Results
3.1. Results—Clinical
3.1.1. Summary of Method—Clinical
3.1.2. Summary of Results—Clinical
3.2. Results—Experimental
3.2.1. Summary of Method—Experimental
3.2.2. Summary of Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Keech, J.A., Jr.; Creech, B.J. Anaplastic T-cell lymphoma in proximity to a saline-filled breast implant. Plast. Reconstr. Surg. 1997, 100, 554–555. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- Medical Device Reports of Breast Implant-Associated Anaplastic Large Cell Lymphoma. 2022. Available online: https://www.fda.gov/medical-devices/breast-implants/medical-device-reports-breast-implant-associated-anaplastic-large-cell-lymphoma (accessed on 4 December 2023).
- Alessandri-Bonetti, M.; Jeong, T.; Vaienti, L.; De La Cruz, C.; Gimbel, M.L.; Nguyen, V.T.; Egro, F.M. The Role of Microorganisms in the Development of Breast Implant-Associated Anaplastic Large Cell Lymphoma. Pathogens 2023, 12, 313. [Google Scholar] [CrossRef] [PubMed]
- Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL). 2023. Available online: https://www.plasticsurgery.org/patient-safety/breast-implant-safety/bia-alcl-summary (accessed on 4 December 2023).
- Wang, G.; Zhao, R.; Bi, R.; Xie, H. Subcutaneous Face and Neck lift: A Traditional Method with Definite Effects Among Asians. Aesthetic Surg. J. 2021, 41, NP1890–NP1903. [Google Scholar] [CrossRef] [PubMed]
- DeCoster, R.C.; Lynch, E.B.; Bonaroti, A.R.; Miranda, R.N.; Hunt, K.K.; Clemens, M.W. Breast Implant–Associated Anaplastic Large Cell Lymphoma. Clin. Plast. Surg. 2021, 48, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.D.; Quatman, C.E.; Manring, M.; Siston, R.A.; Flanigan, D.C. How to write a systematic review. Am. J. Sports Med. 2013, 42, 2761–2768. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung and Blood Institute. Study Quality Assessment Tools. 2019. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 4 December 2023).
- Eysenck, H.J. Systematic Reviews: Meta-analysis and its problems. BMJ 1994, 309, 789–792. [Google Scholar] [CrossRef]
- Greco, T.; Zangrillo, A.; Biondi-Zoccai, G.; Landoni, G. Meta-analysis: Pitfalls and hints. Heart Lung Vessel. 2013, 5, 219–225. [Google Scholar]
- Nordmann, A.J.; Kasenda, B.; Briel, M. Meta-analyses: What they can and cannot do. Swiss Med. Wkly. 2012, 142, w13518. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Patsopoulos, N.A.; Rothstein, H.R. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ 2008, 336, 1413–1415. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, A.; Pepe, G.; Giarnieri, E.; Cippitelli, C.; Bonifacino, A.; Mattei, M.; Martelli, M.; Falasca, C.; Cox, M.C.; Santino, I.; et al. Cytological diagnostic features of late breast implant seromas: From reactive to anaplastic large cell lymphoma. PLoS ONE 2017, 12, e0181097. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Jacombs, A.; Vickery, K.; Merten, S.L.; Pennington, D.G.; Deva, A.K. Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: Implications for breast implant–associated lymphoma. Plast. Reconstr. Surg. 2015, 135, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Johani, K.; Almatroudi, A.; Vickery, K.; Van Natta, B.; Kadin, M.E.; Brody, G.; Clemens, M.; Cheah, C.Y.; Lade, S.; et al. Bacterial Biofilm Infection Detected in Breast Implant—Associated Anaplastic Large-Cell Lymphoma. Plast. Reconstr. Surg. 2016, 137, 1659–1669. [Google Scholar] [CrossRef] [PubMed]
- Mempin, M.; Hu, H.; Vickery, K.; Kadin, M.E.; Prince, H.M.; Kouttab, N.; Morgan, J.W.; Adams, W.P.; Deva, A.K. Gram-Negative Bacterial Lipopolysaccharide Promotes Tumor Cell Proliferation in Breast Implant-Associated Anaplastic Large-Cell Lymphoma. Cancers 2021, 13, 5298. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.N.; Hanson, B.M.; Pinkner, C.L.; Simar, S.R.; Pinkner, J.S.; Parikh, R.; Clemens, M.W.; Hultgren, S.J.; Myckatyn, T.M. Insights into the Microbiome of Breast Implants and Periprosthetic Tissue in Breast Implant-Associated Anaplastic Large Cell Lymphoma. Sci. Rep. 2019, 9, 10393. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, P.; Deva, A.K.; Prince, H.M. Breast Implant-Associated Anaplastic Large Cell Lymphoma. Curr. Hematol. Malign. Rep. 2018, 13, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Lajevardi, S.S.; Rastogi, P.; Isacson, D.; Deva, A.K. What are the likely causes of breast implant associated anaplastic large cell lymphoma (BIA-ALCL)? JPRAS Open 2022, 32, 34–42. [Google Scholar] [CrossRef]
- Tevis, S.E.; Hunt, K.K.; Miranda, R.N.; Lange, C.; Butler, C.E.; Clemens, M.W. Differences in Human Leukocyte Antigen Expression Between Breast Implant–Associated Anaplastic Large Cell Lymphoma Patients and the General Population. Aesthetic Surg. J. 2019, 39, 1065–1070. [Google Scholar] [CrossRef]
- Salter, S.J.; Cox, M.J.; Turek, E.M.; Calus, S.T.; Cookson, W.O.; Moffatt, M.F.; Turner, P.; Parkhill, J.; Loman, N.J.; Walker, A.W. Reagent and laboratory contamination can critically impact sequence-based microbiome analyses. BMC Biol. 2014, 12, 87. [Google Scholar] [CrossRef]
- Wally, N.; Schneider, M.; Thannesberger, J.; Kastner, M.T.; Bakonyi, T.; Indik, S.; Rattei, T.; Bedarf, J.; Hildebrand, F.; Law, J.; et al. Plasmid DNA contaminant in molecular reagents. Sci. Rep. 2019, 9, 1652. [Google Scholar] [CrossRef]
- Epps, M.T.; Langsdon, S.; Pels, T.K.; Noyes, V.; Levine, D.; Thurston, T.E.; Spratt, H.G.; Brzezienski, M.A. Pocket Irrigation and Technique During Reconstructive Surgery. Ann. Plast. Surg. 2019, 82, S427–S432. [Google Scholar] [CrossRef] [PubMed]
- Jewell, M.L.; Bionda, N.; Moran, A.V.; Bevels, E.J.; Jewell, H.L.; Hariri, S.; Leung, B.K. In Vitro Evaluation of Common Antimicrobial Solutions Used for Breast Implant Soaking and Breast Pocket Irrigation—Part 2: Efficacy Against Biofilm-Associated Bacteria. Aesthetic Surg. J. 2021, 41, 1252–1262. [Google Scholar] [CrossRef] [PubMed]
- Ngaage, L.M.M.C.M.B.; Elegbede, A.; Brao, K.B.; Chopra, K.; Gowda, A.U.; Nam, A.J.; Ernst, R.K.; Shirtliff, M.E.; Harro, J.; Rasko, Y.M. The Efficacy of Breast Implant Irrigant Solutions: A Comparative Analysis Using an In Vitro Model. Plast. Reconstr. Surg. 2020, 146, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Culbertson, E.J.; Felder-Scott, C.; Deva, A.K.; E Greenberg, D.; Adams, W.P. Optimizing Breast Pocket Irrigation: The Breast Implant–Associated Anaplastic Large Cell Lymphoma (BIA-ALCL) Era. Aesthetic Surg. J. 2019, 40, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Swanson, E. The Limitations of Three-Dimensional Simulations in Breast Augmentation. Aesthetic Surg. J. 2015, 35, Np62-4. [Google Scholar] [CrossRef] [PubMed]
- Dang, T.; Yim, N.; Tummala, S.; Parsa, A.A.; Parsa, F.D. Povidone-Iodine versus antibiotic irrigation in breast implant surgery: Revival of the ideal solution. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Darouiche, R.O.; Wall, M.J.; Itani, K.M.; Otterson, M.F.; Webb, A.L.; Carrick, M.M.; Miller, H.J.; Awad, S.S.; Crosby, C.T.; Mosier, M.C.; et al. Chlorhexidine–Alcohol versus Povidone–Iodine for Surgical-Site Antisepsis. N. Engl. J. Med. 2010, 362, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Makihara, S.; Kariya, S.; Okano, M.; Naito, T.; Tsumura, M.; Nishizaki, K. Orbital complications of infected mucocele in the paranasal sinuses. Auris Nasus Larynx 2020, 47, 990–995. [Google Scholar] [CrossRef]
- Jongsma, T.E.; Puylaert, J.B. Infection of a malignant appendiceal mucocele masquerading as an appendiceal abscess: Role of preoperative sonography and CT. J. Clin. Ultrasound 2009, 37, 236–238. [Google Scholar] [CrossRef]
- Rangarathnam, C.; Linscheid, R.L. Infected mucous cyst of the finger. J. Hand Surg. 1984, 9, 245–247. [Google Scholar] [CrossRef]
- Eichenfield, D.Z.; Sprague, J.; Eichenfield, L.F. Management of Acne Vulgaris. JAMA 2021, 326, 2055–2067. [Google Scholar] [CrossRef]
- Clemens, M.W.; Medeiros, L.J.; Butler, C.E.; Hunt, K.K.; Fanale, M.A.; Horwitz, S.; Weisenburger, D.D.; Liu, J.; Morgan, E.A.; Kanagal-Shamanna, R.; et al. Complete Surgical Excision Is Essential for the Management of Patients with Breast Implant–Associated Anaplastic Large-Cell Lymphoma. J. Clin. Oncol. 2016, 34, 160–168. [Google Scholar] [CrossRef]
- Patzelt, M.; Zarubova, L.; Klener, P.; Barta, J.; Benkova, K.; Brandejsova, A.; Trneny, M.; Gürlich, R.; Sukop, A. Anaplastic Large-Cell Lymphoma Associated with Breast Implants: A Case Report of a Transgender Female. Aesthetic Plast. Surg. 2017, 42, 451–455. [Google Scholar] [CrossRef]

{kind=link}
| Title | First Author Last Name/Year | Type of Study | Total Population | Total Sample | Age of Population (Mean) | Time till Diagnosis (Years) | Total Case of BIA-ALCL | Type of Implants | NIH Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|
| Cytological diagnostic features of late breast implant seromas: From reactive to anaplastic large cell lymphoma | Di Napoli, 2017 [15] | Clinical | 50 | 67 | 23–75 | 5.83 ± 1.42 | 5 | 4 Biocell texture silicon implants, 1 Polyurethane- coated silicone | Good |
| Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: implications for breast implant-associated lymphoma. | Hu, 2015 [16] | In Vivo (pig) | 3 | 24 | N/A * | 0.73 | 0 | 12 textured vs. 12 smooth | Good |
| Clinical | 34 | 57 | N/A | N/A | 0 | Smooth implant | |||
| Bacterial Biofilm Infection Detected in Breast Implant-Associated Anaplastic Large-Cell Lymphoma. | Hu, 2016 [17] | Clinical | 84 | 88 | 52.7 (BIA-ALCL only), 43.8 (capsule patients) | 8.8 (BIA-ALCL only), 7.4 (capsule patients) | 22 | 13 textured, 9 unknown | Good |
| Gram-Negative Bacterial Lipopolysaccharide Promotes Tumor Cell Proliferation in Breast Implant-Associated Anaplastic Large-Cell Lymphoma. | Mempin, 2021 [18] | In vitro | Tumor cell line: 16 patients PBMC: 12 patients with BIACL, 3 controls | N/A | 43.8 years | 7 | 16 | 8 Silimed polyurethane (textured), 6 Allergan Biocell (textured), 1 Mentor Siltex (textured), 2 Nagor, 1 McGhan, 2 polyimplant prostheses | Good |
| Insights into the Microbiome of Breast Implants and Periprosthetic Tissue in Breast Implant-Associated Anaplastic Large Cell Lymphoma. | Walker, 2019 [19] | Clinical | 9 | 58 | 51.7 ± 11.4 years | 9.3 ± 2.0 | 7 | Textured implants | Good |
| Breast Implant-Associated Anaplastic Large Cell Lymphoma: Defining Future Research Priorities | DeCoster, 2021 [7] | Clinical | 24 | 18 | N/A | 1–28 | 18 | Textured silicon implants | Good |
| Title | Method Biofilm/BIA-ALCL Identification |
|---|---|
| Cytological diagnostic features of late breast implant seromas: From reactive to anaplastic large cell lymphoma [15] | From 61 reactive late seromas, 21 samples underwent aerobic, anaerobic, and fungal cultures, incubated in a brain–heart infusion broth and fluid thioglycolate medium, then spread on various agar plates. Post 24 h incubation at 37 °C, samples with no bacterial growth after 48 h were deemed negative. Cell-block and FFPE specimens underwent immunohistochemistry and molecular T-cell receptor analysis, with PCR products analyzed via a genetic analyzer. Capsulectomy specimens from five BI-ALCL patients were collected post-diagnosis. |
| Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: implications for breast implant-associated lymphoma [16] | Capsule or implant samples (50 or 100 mg) were digested using proteinase K and lysozyme, followed by genomic DNA extraction via phenol/chloroform and ethanol precipitation. Bacterial counts were determined by qPCR of the 16S rRNA gene. T- and B-cell quantities in capsules or on implants were ascertained by qPCR of specific genes. Bacteria and lymphocyte counts were calculated per milligram of capsule. Real-time qPCR involved a mix with cycling conditions of 95 °C for 10 min, followed by 40 cycles. Biofilm presence was confirmed by scanning electron microscopy, and lymphocytic infiltration was analyzed using monoclonal antibodies and confocal laser scanning microscopy. |
| Bacterial Biofilm Infection Detected in Breast Implant-Associated Anaplastic Large-Cell Lymphoma [17] | Samples (50–100 mg) from 26 breast implant-associated ALCL and 62 non-tumor capsules were digested using proteinase K and lysozyme, followed by genomic DNA extraction. Bacterial DNA was quantified using qPCR of the 16S rRNA gene, with the 18S rRNA gene as a reference. Bacterial count per milligram of tissue was based on the 18S rRNA gene’s average copies. Real-time qPCR involved a 25 μL mix with specific cycling conditions. Bacterial species were identified in 19 ALCL and 12 non-tumor samples, plus 3 contralateral breast samples, using FLX amplicon pyrosequencing and analyzed by QIIME software (Ver 1.3.0) (Boulder, CO, USA). The bacterial composition and abundance were compared using one-way ANOVA. Non-tumor capsules were fixed in glutaraldehyde, and ALCL samples were prepared from formalin-fixed, paraffin-embedded blocks, dehydrated, and examined under a scanning electron microscope. Bacterial aggregates were located using fluorescence in situ hybridization with specific probes. |
| Insights into the Microbiome of Breast Implants and Periprosthetic Tissue in Breast Implant-Associated Anaplastic Large Cell Lymphoma [18] | In each case of breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL) and non-BIA-ALCL, an en bloc capsulectomy was performed. Specimens, including implant, capsule, skin, and parenchyma, underwent 16S rRNA microbiome sequencing, culturing, and imaging. Tissue and capsule samples were incubated for over 24 h at 37 °C. Visible microbial growth was isolated using a loop on BHI agar, with colonies identified through 16S Sanger sequencing. Homogeneous and heterogeneous colonies were processed for aerobic and anaerobic growth, with selected colonies sequenced. Biofilm samples were frozen for DNA extraction using the DNeasy PowerBiofilm kit. |
| Breast Implant-Associated Anaplastic Large Cell Lymphoma: Defining Future Research Priorities [7] | The diagnosis of breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL) involves three main steps. First, CD30+ cells are identified using immunohistochemistry, but this alone is not conclusive for BIA-ALCL as such cells can also be present in benign seromas. Second, flow cytometry is used to assess T-cell clonality, crucial for confirming T-cell lymphoma. Finally, histological examination is performed to detect large anaplastic lymphoma cells, a key factor in diagnosing BIA-ALCL. In cases without obvious lesions, a thorough approach involving multiple biopsies from different capsule areas is recommended to enhance diagnostic accuracy. |
| Title | Results |
|---|---|
| Cytological diagnostic features of late breast implant seromas: From reactive to anaplastic large cell lymphoma [15] | The lymphoma remained within the fibrous capsule around the implant, not spreading to nearby tissues. Only one case showed lymph node involvement at diagnosis. Four patients underwent surgical removal of the implant and capsule, whereas the fifth, with lymph node involvement, also received adjuvant chemotherapy, leading to complete remission. About 70% of cells in these samples were CD30-positive atypical neoplastic cells. One patient had a relapse, evidenced by a seroma containing mixed cells, including 10% large atypical cells. All cases showed a T-cell defective phenotype, predominantly CD4+, except for one CD8+ and one double-negative. Four cases presented monoclonal TRG rearrangement, and one was polyclonal. Of 61 seromas tested, 21 were cultured, showing various types including acute and mixed; 1 mixed seroma grew Pseudomonas aeruginosa and Klebsiella oxytoca, and 4 acute seromas grew Staphylococcus aureus and Serratia marcescens. Chronic and hemorrhagic seromas showed no pathogen growth. |
| Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: implications for breast implant-associated lymphoma [16] | In a four-year study, 57 periprosthetic capsules from 34 patients with Baker grade IV contracture were collected. All patients had textured implants. The capsules were analyzed using quantitative polymerase chain reaction to determine lymphocyte count, CD status, and bacterial count. All capsules contained biofilm bacteria, averaging 2.52 × 107 bacteria/mg of tissue. Implant textures varied: 34 Biocell, 14 Siltex, 5 Poly Implant Prothèse, and 4 polyurethane. T cells (CD4 + CD8a) outnumbered B cells significantly, and a correlation was noted between lymphocyte and bacterial count per milligram of tissue. Polyurethane implants showed a notably higher bacterial presence compared to other textures. |
| Bacterial Biofilm Infection Detected in Breast Implant-Associated Anaplastic Large-Cell Lymphoma [17]. | In a breast implant-associated ALCL study, five samples showed no bacteria via real-time quantitative polymerase chain reaction, with a significant inhibition of the human 18S rRNA gene’s reaction, suggesting PCR inhibitors’ presence. One negative sample, part of a pair from the same tumor, contrasted with its counterpart showing normal gene augmentation. The other 21 ALCL and 62 non-tumor samples displayed considerable bacterial 16S rRNA gene presence, averaging 4.7 × 106 and 4.9 × 106 bacteria/mg of tissue, respectively. Samples from the contralateral breasts had significantly fewer bacteria. Microbiome analysis of 19 ALCL samples revealed a predominance of Ralstonia spp., also noted in contralateral samples, whereas Staphylococcus spp. was common in non-tumor specimens. Fluorescent in situ hybridization in 11 ALCL samples detected Ralstonia spp. in 10, confirmed in half, and identified in all via pyrosequencing. |
| Insights into the Microbiome of Breast Implants and Periprosthetic Tissue in Breast Implant-Associated Anaplastic Large Cell Lymphoma [19] | Staphylococcus spp., frequently found in cultures, was identified in both BIA-ALCL and control samples from the contralateral breast. The diversity and relative abundance of Gram-negative bacteria were similar between BIA-ALCL and control samples. Heat maps showed significant variations in bacterial composition across different materials like skin, breast, implant, and capsule. When comparing BIA-ALCL to control samples by material, Propionibacterium was the main driver of variability, alongside Staphylococcus, Altererythrobacter, and Stenotrophomonas, although this varied across sample types. Rare bacterial taxa, including Ralstonia in 8 samples and Brevundimonas in 31 samples, were present but did not differentiate BIA-ALCL samples from controls. Ralstonia was more common in non-ALCL controls, whereas Brevundimonas showed higher abundance in some contralateral control and BIA-ALCL skin samples. |
| Breast Implant-Associated Anaplastic Large Cell Lymphoma: Defining Future Research Priorities [7] | In a study focused on breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL), the intraoperative techniques used for breast implant placement in 24 patients were analyzed. Twelve of these patients underwent betadine irrigation at varying strengths, whereas seven were treated with different antibiotic irrigation combinations. Despite these measures, BIA-ALCL occurred in these patients. This study discovered 18 worldwide BIA-ALCL case clusters, each linked to a specific surgeon and involving multiple cases. Only in five clusters did the surgeon perform the original implantation, with the others involving secondary referral surgeons. Four of these surgeons had previously contributed to BIA-ALCL research and were recognized for their comprehensive implant practices, including diligent follow-up, proactive CD30 screening, and ongoing patient surveillance. |
| Title | Method Biofilm/BIA-ALCL Identification |
|---|---|
| Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: implications for breast implant-associated lymphoma [16] | Pig tissue samples (50 or 100 mg) were digested with proteinase K and lysozyme, and genomic DNA was extracted using phenol/chloroform and ethanol precipitation. Bacterial count was determined by real-time quantitative polymerase chain reaction of the 16S rRNA gene. T- and B-cell counts in the tissue were quantified using qPCR of CD3, CD4, CD8a, and CD79a genes. Bacterial and lymphocyte numbers were calculated per milligram of tissue, based on the average 18S gene copies. The qPCR analysis involved specific reaction mix and cycling conditions. Biofilm presence was visually confirmed via scanning electron microscopy, and lymphocytic infiltration was imaged using confocal microscopy with specific monoclonal antibodies. |
| Gram-Negative Bacterial Lipopolysaccharide Promotes Tumor Cell Proliferation in Breast Implant-Associated Anaplastic Large-Cell Lymphoma [18] | BIA-ALCL and TLBR cells were exposed to Phytohemagglutinin (PHA), lipopolysaccharide (LPS), Staphylococcal enterotoxin A (SEA), and toxic shock syndrome toxin-1 (TSST-1) to study apoptosis induced by biofilm secretion factors. Apoptotic stages were identified using a bivariate dot plot of Zombie UV versus Annexin V-FITC expressions. The analysis distinguished viable cells (Annexin V and Zombie UV negative), early apoptotic (Annexin V positive, Zombie UV negative), dead, and late apoptotic/necrotic cells (both markers positive). |
| Title | Results |
|---|---|
| Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: implications for breast implant-associated lymphoma [16] | Ten capsular specimens from both smooth and textured implants were analyzed, with twenty samples undergoing quantitative polymerase chain reaction for bacterial 16S RNA gene detection. No significant difference was observed in bacterial count per milligram between smooth and textured implants (2.7 × 105 vs. 3.5 × 105 bacteria/mg). However, textured implants had significantly more attached bacteria (4.2 × 105 bacteria/mg) than smooth implants (1.52 × 103 bacteria/mg). Additionally, textured implants showed a higher lymphocyte count on their surface, with a 63-fold increase compared to smooth implants, mostly T cells. Scanning electron microscopy revealed numerous activated lymphocytes on textured implants, characterized by increased size and active replication, whereas smooth implants had minimal or no attached infiltrate. |
| Gram-Negative Bacterial Lipopolysaccharide Promotes Tumor Cell Proliferation in Breast Implant-Associated Anaplastic Large-Cell Lymphoma [18] | BIA-ALCL tumor cells and TLBR lines showed a stronger response to LPS than to Staphylococcal superantigens SEA, TSST-1, or PHA. Conversely, cutaneous ALCL cells and PBMCs from capsular contracture patients reacted more to PHA and Staphylococcal superantigens. Healthy control and BIA-ALCL patient-derived PBMCs also responded more to PHA. LPS stimulation increased the live cell count in BIA-ALCL and TLBR cells but did not affect cell viability or induce apoptosis. The proportions of live, dead, and apoptotic cells remained consistent across stimulated and non-stimulated cells, and between BIA-ALCL and TLBR cells. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foppiani, J.A.; Raska, O.; Taritsa, I.; Hernandez Alvarez, A.; Lee, D.; Escobar-Domingo, M.J.; Berger, J.; Klener, P.; Schuster, K.A.; Abdo, D.; et al. Incidental Bystander or Essential Culprit: A Systematic Review of Bacterial Significance in the Pathogenesis of Breast Implant-Associated Anaplastic Large Cell Lymphoma. Int. J. Mol. Sci. 2024, 25, 355. https://doi.org/10.3390/ijms25010355
Foppiani JA, Raska O, Taritsa I, Hernandez Alvarez A, Lee D, Escobar-Domingo MJ, Berger J, Klener P, Schuster KA, Abdo D, et al. Incidental Bystander or Essential Culprit: A Systematic Review of Bacterial Significance in the Pathogenesis of Breast Implant-Associated Anaplastic Large Cell Lymphoma. International Journal of Molecular Sciences. 2024; 25(1):355. https://doi.org/10.3390/ijms25010355
Chicago/Turabian StyleFoppiani, Jose A., Otakar Raska, Iulianna Taritsa, Angelica Hernandez Alvarez, Daniela Lee, Maria J. Escobar-Domingo, Josephine Berger, Pavel Klener, Kirsten A. Schuster, Daoud Abdo, and et al. 2024. "Incidental Bystander or Essential Culprit: A Systematic Review of Bacterial Significance in the Pathogenesis of Breast Implant-Associated Anaplastic Large Cell Lymphoma" International Journal of Molecular Sciences 25, no. 1: 355. https://doi.org/10.3390/ijms25010355
APA StyleFoppiani, J. A., Raska, O., Taritsa, I., Hernandez Alvarez, A., Lee, D., Escobar-Domingo, M. J., Berger, J., Klener, P., Schuster, K. A., Abdo, D., Clemens, M. W., & Lin, S. J. (2024). Incidental Bystander or Essential Culprit: A Systematic Review of Bacterial Significance in the Pathogenesis of Breast Implant-Associated Anaplastic Large Cell Lymphoma. International Journal of Molecular Sciences, 25(1), 355. https://doi.org/10.3390/ijms25010355