
An Exploratory Study Using Next-Generation Sequencing to Identify Prothrombotic Variants in Patients with Cerebral Vein Thrombosis

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Results
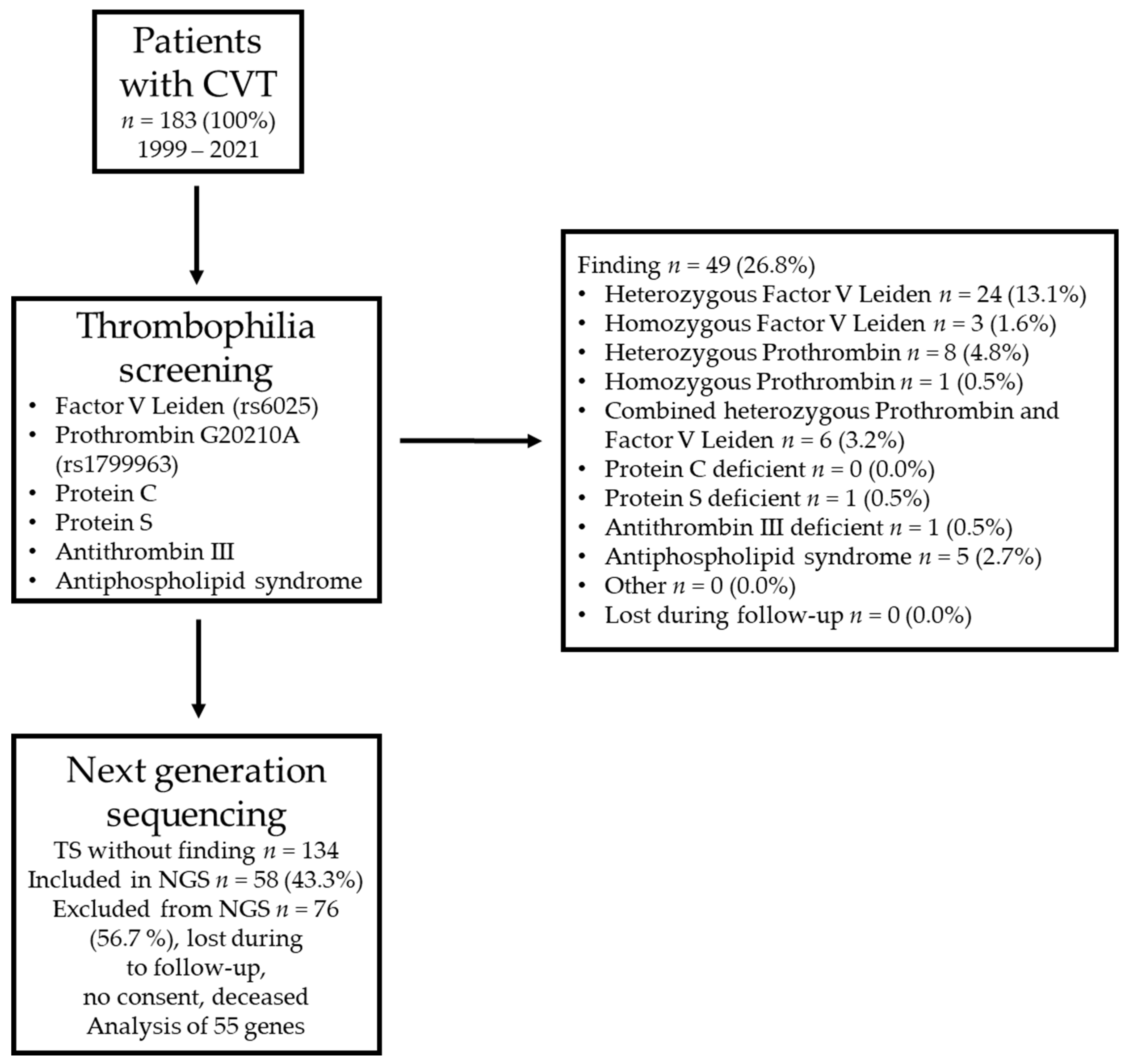
2.1. Initial Thrombophilia Screening
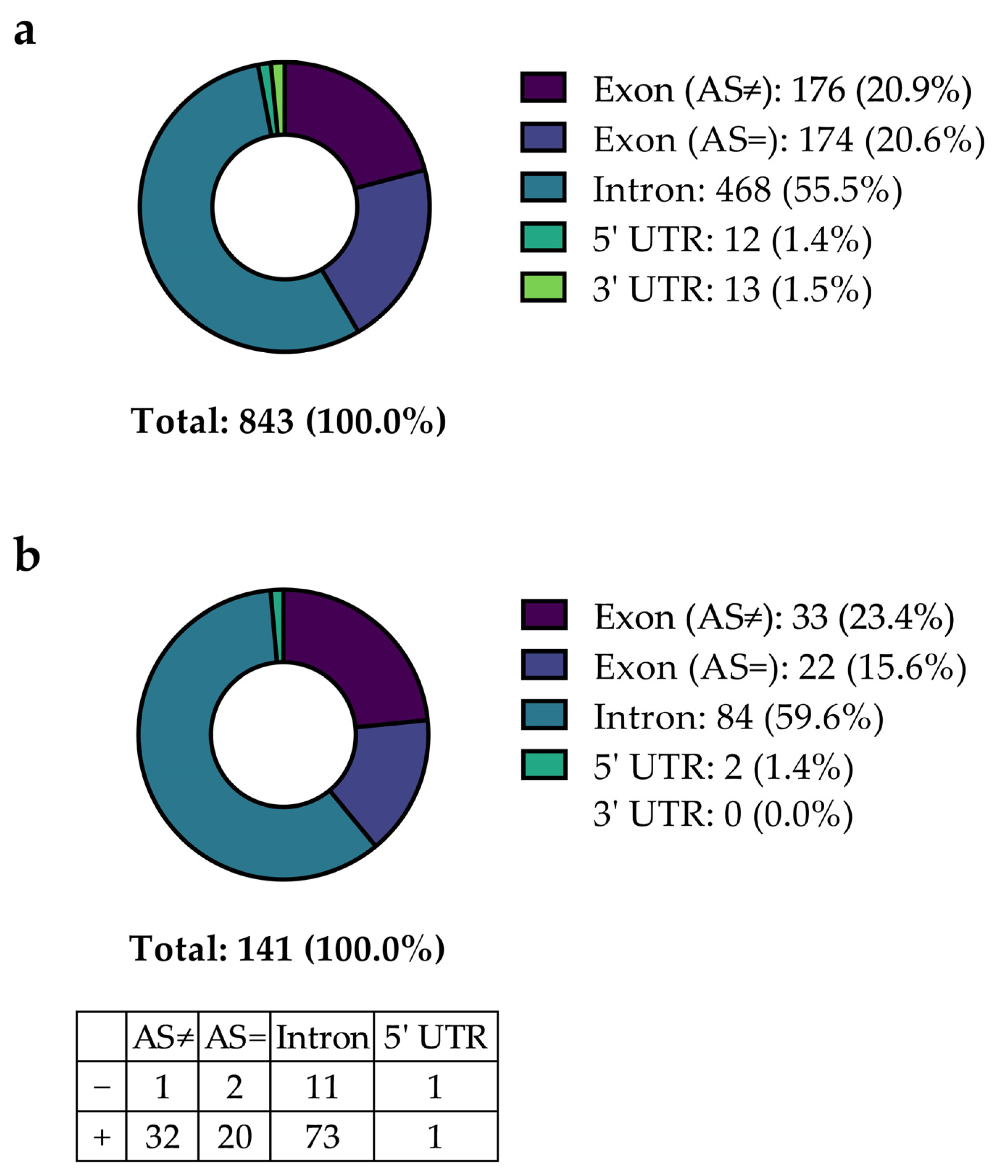
2.2. Analysis of NGS Data
3. Discussion
4. Materials and Methods
4.1. Patient Cohort and Sampling Approach
4.2. Initial Thrombophilia Screening
4.3. NGS
4.4. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bousser, M.-G.; Ferro, J.M. Cerebral venous thrombosis: An update. Lancet Neurol. 2007, 6, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, L.; Squitieri, M.; Cohen, H.; Cowley, P.; Werring, D.J. Cerebral venous thrombosis: A practical guide. Pract. Neurol. 2020, 20, 356–367. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, J.M.; Zuurbier, S.M.; Stam, J. Declining mortality in cerebral venous thrombosis: A systematic review. Stroke 2014, 45, 1338–1341. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, R.; Ken-Dror, G.; Martinelli, I.; Grandone, E.; Hiltunen, S.; Lindgren, E.; Margaglione, M.; Le Cam Duchez, V.; Bagan Triquenot, A.; Zedde, M.; et al. Age of onset of cerebral venous thrombosis: The BEAST study. Eur. Stroke J. 2023, 8, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Ferro, J.M.; Canhão, P.; Stam, J.; Bousser, M.-G.; Barinagarrementeria, F. ISCVT Investigators Prognosis of cerebral vein and dural sinus thrombosis: Results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke 2004, 35, 664–670. [Google Scholar] [CrossRef]
- Saposnik, G.; Barinagarrementeria, F.; Brown, R.D.; Bushnell, C.D.; Cucchiara, B.; Cushman, M.; Deveber, G.; Ferro, J.M.; Tsai, F.Y. Diagnosis and Management of Cerebral Venous Thrombosis: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2011, 42, 1158–1192. [Google Scholar] [CrossRef]
- Ferro, J.M.; Bousser, M.-G.; Canhão, P.; Coutinho, J.M.; Crassard, I.; Dentali, F.; di Minno, M.; Maino, A.; Martinelli, I.; Masuhr, F.; et al. European Stroke Organization guideline for the diagnosis and treatment of cerebral venous thrombosis—Endorsed by the European Academy of Neurology. Eur. Stroke J. 2017, 2, 195–221. [Google Scholar] [CrossRef]
- Miranda, B.; Aaron, S.; Arauz, A.; Barinagarrementeria, F.; Borhani-Haghighi, A.; Carvalho, M.; Conforto, A.B.; Coutinho, J.M.; Stam, J.; Canhão, P.; et al. The benefit of EXtending oral antiCOAgulation treatment (EXCOA) after acute cerebral vein thrombosis (CVT): EXCOA-CVT cluster randomized trial protocol. Int. J. Stroke 2018, 13, 771–774. [Google Scholar] [CrossRef]
- Cotlarciuc, I.; Marjot, T.; Khan, M.S.; Hiltunen, S.; Haapaniemi, E.; Metso, T.M.; Putaala, J.; Zuurbier, S.M.; Brouwer, M.C.; Passamonti, S.M.; et al. Towards the genetic basis of cerebral venous thrombosis—The BEAST Consortium: A study protocol: Table 1. BMJ Open 2016, 6, e012351. [Google Scholar] [CrossRef]
- Simeoni, I.; Stephens, J.C.; Hu, F.; Deevi, S.V.V.; Megy, K.; Bariana, T.K.; Lentaigne, C.; Schulman, S.; Sivapalaratnam, S.; Vries, M.J.A.; et al. A high-throughput sequencing test for diagnosing inherited bleeding, thrombotic, and platelet disorders. Blood 2016, 127, 2791–2803. [Google Scholar] [CrossRef]
- Downes, K.; Megy, K.; Duarte, D.; Vries, M.; Gebhart, J.; Hofer, S.; Shamardina, O.; Deevi, S.V.V.; Stephens, J.; Mapeta, R.; et al. Diagnostic high-throughput sequencing of 2396 patients with bleeding, thrombotic, and platelet disorders. Blood 2019, 134, 2082–2091. [Google Scholar] [CrossRef]
- Reed, F.A.; Akey, J.M.; Aquadro, C.F. Fitting background-selection predictions to levels of nucleotide variation and divergence along the human autosomes. Genome Res. 2005, 15, 1211–1221. [Google Scholar] [CrossRef]
- Li, X.; Cui, L.; Li, Y.; Zhu, L.; Wang, C.; Liu, J.; Fang, S. Prevalence and geographical variation of Factor V Leiden in patients with cerebral venous thrombosis: A meta-analysis. PLoS ONE 2018, 13, e0203309. [Google Scholar] [CrossRef]
- Marjot, T.; Yadav, S.; Hasan, N.; Bentley, P.; Sharma, P. Genes associated with adult cerebral venous thrombosis. Stroke 2011, 42, 913–918. [Google Scholar] [CrossRef]
- Joly, B.S.; Coppo, P.; Veyradier, A. Thrombotic thrombocytopenic purpura. Blood 2017, 129, 2836–2846. [Google Scholar] [CrossRef]
- Plautz, W.E.; Raval, J.S.; Dyer, M.R.; Rollins-Raval, M.A.; Zuckerbraun, B.S.; Neal, M.D. ADAMTS13: Origins, applications, and prospects. Transfusion 2018, 58, 2453–2462. [Google Scholar] [CrossRef]
- Kremer Hovinga, J.A.; Coppo, P.; Lämmle, B.; Moake, J.L.; Miyata, T.; Vanhoorelbeke, K. Thrombotic thrombocytopenic purpura. Nat. Rev. Dis. Prim. 2017, 3, 17020. [Google Scholar] [CrossRef]
- Wang, Y.; Ni, H. Fibronectin maintains the balance between hemostasis and thrombosis. Cell. Mol. Life Sci. 2016, 73, 3265–3277. [Google Scholar] [CrossRef]
- Mosher, D.F. Cross-linking of cold-insoluble globulin by fibrin-stabilizing factor. J. Biol. Chem. 1975, 250, 6614–6621. [Google Scholar] [CrossRef]
- Pecheniuk, N.M.; Elias, D.J.; Deguchi, H.; Averell, P.M.; Griffin, J.H. Elevated plasma fibronectin levels associated with venous thromboembolism. Thromb. Haemost. 2008, 100, 224–228. [Google Scholar] [CrossRef]
- Patten, J.; Wang, K. Fibronectin in development and wound healing. Adv. Drug Deliv. Rev. 2021, 170, 353–368. [Google Scholar] [CrossRef]
- Vaz-Drago, R.; Custódio, N.; Carmo-Fonseca, M. Deep intronic mutations and human disease. Hum. Genet. 2017, 136, 1093–1111. [Google Scholar] [CrossRef] [PubMed]
- Vihinen, M. When a Synonymous Variant Is Nonsynonymous. Genes 2022, 13, 1485. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.M.; Catto, A.J.; Grant, P.J. Association of the alpha-fibrinogen Thr312Ala polymorphism with poststroke mortality in subjects with atrial fibrillation. Circulation 1999, 99, 2423–2426. [Google Scholar] [CrossRef]
- Carter, A.M.; Catto, A.J.; Kohler, H.P.; Ariëns, R.A.; Stickland, M.H.; Grant, P.J. Alpha-fibrinogen Thr312Ala polymorphism and venous thromboembolism. Blood 2000, 96, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- Standeven, K.F.; Grant, P.J.; Carter, A.M.; Scheiner, T.; Weisel, J.W.; Ariëns, R.A.S. Functional analysis of the fibrinogen Aalpha Thr312Ala polymorphism: Effects on fibrin structure and function. Circulation 2003, 107, 2326–2330. [Google Scholar] [CrossRef]
- Rasmussen-Torvik, L.J.; Cushman, M.; Tsai, M.Y.; Zhang, Y.; Heckbert, S.R.; Rosamond, W.D.; Folsom, A.R. The association of alpha-fibrinogen Thr312Ala polymorphism and venous thromboembolism in the LITE study. Thromb. Res. 2007, 121, 1–7. [Google Scholar] [CrossRef]
- Le Gal, G.; Delahousse, B.; Lacut, K.; Malaviolle, V.; Regina, S.; Blouch, M.-T.; Couturaud, F.; Mottier, D.; Oger, E.; Gruel, Y.; et al. Fibrinogen Aalpha-Thr312Ala and factor XIII-A Val34Leu polymorphisms in idiopathic venous thromboembolism. Thromb. Res. 2007, 121, 333–338. [Google Scholar] [CrossRef]
- Lotta, L.A.; Wang, M.; Yu, J.; Martinelli, I.; Yu, F.; Passamonti, S.M.; Consonni, D.; Pappalardo, E.; Menegatti, M.; Scherer, S.E.; et al. Identification of genetic risk variants for deep vein thrombosis by multiplexed next-generation sequencing of 186 hemostatic/pro-inflammatory genes. BMC Med. Genomics 2012, 5, 7. [Google Scholar] [CrossRef]
- Klajmon, A.; Chmiel, J.; Ząbczyk, M.; Pociask, E.; Wypasek, E.; Malinowski, K.P.; Undas, A.; Natorska, J. Fibrinogen β chain and FXIII polymorphisms affect fibrin clot properties in acute pulmonary embolism. Eur. J. Clin. Investig. 2022, 52, e13718. [Google Scholar] [CrossRef]
- Ariëns, R.A.; Philippou, H.; Nagaswami, C.; Weisel, J.W.; Lane, D.A.; Grant, P.J. The factor XIII V34L polymorphism accelerates thrombin activation of factor XIII and affects cross-linked fibrin structure. Blood 2000, 96, 988–995. [Google Scholar] [CrossRef]
- Schroeder, V.; Chatterjee, T.; Kohler, H.P. Influence of blood coagulation factor XIII and FXIII Val34Leu on plasma clot formation measured by thrombelastography. Thromb. Res. 2001, 104, 467–474. [Google Scholar] [CrossRef]
- Van Hylckama Vlieg, A.; Komanasin, N.; Ariëns, R.A.S.; Poort, S.R.; Grant, P.J.; Bertina, R.M.; Rosendaal, F.R. Factor XIII Val34Leu polymorphism, factor XIII antigen levels and activity and the risk of deep venous thrombosis. Br. J. Haematol. 2002, 119, 169–175. [Google Scholar] [CrossRef]
- de la Red, G.; Tàssies, D.; Espinosa, G.; Monteagudo, J.; Bové, A.; Plaza, J.; Cervera, R.; Reverter, J.-C. Factor XIII-A subunit Val34Leu polymorphism is associated with the risk of thrombosis in patients with antiphospholipid antibodies and high fibrinogen levels. Thromb. Haemost. 2009, 101, 312–316. [Google Scholar] [CrossRef]
- Kattula, S.; Bagoly, Z.; Tóth, N.K.; Muszbek, L.; Wolberg, A.S. The factor XIII-A Val34Leu polymorphism decreases whole blood clot mass at high fibrinogen concentrations. J. Thromb. Haemost. 2020, 18, 885–894. [Google Scholar] [CrossRef]
- Balogh, I.; Szôke, G.; Kárpáti, L.; Wartiovaara, U.; Katona, E.; Komáromi, I.; Haramura, G.; Pfliegler, G.; Mikkola, H.; Muszbek, L. Val34Leu polymorphism of plasma factor XIII: Biochemistry and epidemiology in familial thrombophilia. Blood 2000, 96, 2479–2486. [Google Scholar] [CrossRef]
- Endler, G.; Funk, M.; Haering, D.; Lalouschek, W.; Lang, W.; Mirafzal, M.; Wagner, O.; Mannhalter, C. Is the factor XIII 34Val/Leu polymorphism a protective factor for cerebrovascular disease? Br. J. Haematol. 2003, 120, 310–314. [Google Scholar] [CrossRef]
- Kupis, R.W.; Goldman-Mazur, S.; Polak, M.; Ząbczyk, M.; Undas, A. Faster fibrin clot degradation characterizes patients with central pulmonary embolism at a low risk of recurrent peripheral embolism. Sci. Rep. 2019, 9, 72. [Google Scholar] [CrossRef]
- Siudut, J.; Grela, M.; Wypasek, E.; Plens, K.; Undas, A. Reduced plasma fibrin clot permeability and susceptibility to lysis are associated with increased risk of postthrombotic syndrome. J. Thromb. Haemost. 2016, 14, 784–793. [Google Scholar] [CrossRef]
- Sherief, L.M.; Zakaria, M.; Soliman, B.K.; Kamal, N.M.; Alharthi, S.A.; Abosabie, S.A.; Abdelazeem, M. Cerebral sinuses thrombosis prior to the diagnosis of acute lymphoblastic leukemia in a child: A case report. SAGE Open Med. Case Rep. 2022, 10. [Google Scholar] [CrossRef]
- Huang, J.; Li, X.; Shi, X.; Zhu, M.; Wang, J.; Huang, S.; Huang, X.; Wang, H.; Li, L.; Deng, H.; et al. Platelet integrin αIIbβ3: Signal transduction, regulation, and its therapeutic targeting. J. Hematol. Oncol. 2019, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Feng, D.; Lindpaintner, K.; Larson, M.G.; Rao, V.S.; O’Donnell, C.J.; Lipinska, I.; Schmitz, C.; Sutherland, P.A.; Silbershatz, H.; D’Agostino, R.B.; et al. Increased platelet aggregability associated with platelet GPIIIa PlA2 polymorphism: The Framingham Offspring Study. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 1142–1147. [Google Scholar] [CrossRef] [PubMed]
- Goodall, A.H.; Curzen, N.; Panesar, M.; Hurd, C.; Knight, C.J.; Ouwehand, W.H.; Fox, K.M. Increased binding of fibrinogen to glycoprotein IIIa-proline33 (HPA-1b, PlA2, Zwb) positive platelets in patients with cardiovascular disease. Eur. Heart J. 1999, 20, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, K.V.; Goldschmidt-Clermont, P.J.; Roos, C.; Bray, P.F. The PlA2 polymorphism of integrin β3 enhances outside-in signaling and adhesive functions. J. Clin. Investig. 2000, 105, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Undas, A.; Brummel, K.; Musial, J.; Mann, K.G.; Szczeklik, A. PlA2 polymorphism of β3 integrins is associated with enhanced thrombin generation and impaired antithrombotic action of aspirin at the site of microvascular injury. Circulation 2001, 104, 2666–2672. [Google Scholar] [CrossRef]
- Podolnikova, N.P.; Yermolenko, I.S.; Fuhrmann, A.; Lishko, V.K.; Magonov, S.; Bowen, B.; Enderlein, J.; Podolnikov, A.V.; Ros, R.; Ugarova, T.P. Control of integrin alphaIIb beta3 outside-in signaling and platelet adhesion by sensing the physical properties of fibrin(ogen) substrates. Biochemistry 2010, 49, 68–77. [Google Scholar] [CrossRef]
- Kumar, S.; Wang, Y.; Hedayati, M.; Fleissner, F.; Rausch, M.K.; Parekh, S.H. Structural control of fibrin bioactivity by mechanical deformation. Proc. Natl. Acad. Sci. USA 2022, 119, e2117675119. [Google Scholar] [CrossRef]
- Medina, P.; Navarro, S.; Estellés, A.; Vayá, A.; Woodhams, B.; Mira, Y.; Villa, P.; Migaud-Fressart, M.; Ferrando, F.; Aznar, J.; et al. Contribution of polymorphisms in the endothelial protein C receptor gene to soluble endothelial protein C receptor and circulating activated protein C levels, and thrombotic risk. Thromb. Haemost. 2004, 91, 905–911. [Google Scholar] [CrossRef]
- Saposnik, B.; Reny, J.-L.; Gaussem, P.; Emmerich, J.; Aiach, M.; Gandrille, S. A haplotype of the EPCR gene is associated with increased plasma levels of sEPCR and is a candidate risk factor for thrombosis. Blood 2004, 103, 1311–1318. [Google Scholar] [CrossRef]
- Qu, D.; Wang, Y.; Song, Y.; Esmon, N.L.; Esmon, C.T. The Ser219-->Gly dimorphism of the endothelial protein C receptor contributes to the higher soluble protein levels observed in individuals with the A3 haplotype. J. Thromb. Haemost. 2006, 4, 229–235. [Google Scholar] [CrossRef]
- Reiner, A.P.; Carty, C.L.; Jenny, N.S.; Nievergelt, C.; Cushman, M.; Stearns-Kurosawa, D.J.; Kurosawa, S.; Kuller, L.H.; Lange, L.A. PROC, PROCR and PROS1 polymorphisms, plasma anticoagulant phenotypes, and risk of cardiovascular disease and mortality in older adults: The Cardiovascular Health Study. J. Thromb. Haemost. 2008, 6, 1625–1632. [Google Scholar] [CrossRef]
- Karabıyık, A.; Yılmaz, E.; Eğin, Y.; Akar, N. The Effects of Endothelial Protein C Receptor Gene Polymorphisms on the Plasma sEPCR Level in Venous Thrombosis Patients. Turk. Soc. Haematol. 2012, 29, 55–62. [Google Scholar] [CrossRef]
- Anastasiou, G.; Politou, M.; Rallidis, L.; Grouzi, E.; Karakitsos, P.; Merkouri, E.; Travlou, A.; Gialeraki, A. Endothelial Protein C Receptor Gene Variants and Risk of Thrombosis. Clin. Appl. Thromb. Hemost. 2016, 22, 199–204. [Google Scholar] [CrossRef]
- España, F.; Vayá, A.; Mira, Y.; Medina, P.; Estellés, A.; Villa, P.; Falcó, C.; Aznar, J. Low level of circulating activated protein C is a risk factor for venous thromboembolism. Thromb. Haemost. 2001, 86, 1368–1373. [Google Scholar]
- Dennis, J.; Johnson, C.Y.; Adediran, A.S.; de Andrade, M.; Heit, J.A.; Morange, P.-E.; Trégouët, D.-A.; Gagnon, F. The endothelial protein C receptor (PROCR) Ser219Gly variant and risk of common thrombotic disorders: A HuGE review and meta-analysis of evidence from observational studies. Blood 2012, 119, 2392–2400. [Google Scholar] [CrossRef]
- Li, Y.-Y.; Wu, J.-J.; Yang, X.-X.; Geng, H.-Y.; Gong, G.; Kim, H.J. EPCR Gene Ser219Gly Polymorphism and Venous Thromboembolism: A Meta-Analysis of 9,494 Subjects. Front. Physiol. 2017, 8, 339. [Google Scholar] [CrossRef]
- Lindström, S.; Wang, L.; Smith, E.N.; Gordon, W.; van Hylckama Vlieg, A.; de Andrade, M.; Brody, J.A.; Pattee, J.W.; Haessler, J.; Brumpton, B.M.; et al. Genomic and transcriptomic association studies identify 16 novel susceptibility loci for venous thromboembolism. Blood 2019, 134, 1645–1657. [Google Scholar] [CrossRef]
- Crous-Bou, M.; Harrington, L.B.; Kabrhel, C. Environmental and Genetic Risk Factors Associated with Venous Thromboembolism. Semin. Thromb. Hemost. 2016, 42, 808–820. [Google Scholar] [CrossRef]
- Lane, D.A.; Grant, P.J. Role of hemostatic gene polymorphisms in venous and arterial thrombotic disease. Blood 2000, 95, 1517–1532. [Google Scholar] [CrossRef]
- Simsek, E.; Yesilyurt, A.; Pinarli, F.; Eyerci, N.; Ulus, A.T. Combined genetic mutations have remarkable effect on deep venous thrombosis and/or pulmonary embolism occurence. Gene 2014, 536, 171–176. [Google Scholar] [CrossRef]
- Almawi, W.Y.; Tamim, H.; Kreidy, R.; Timson, G.; Rahal, E.; Nabulsi, M.; Finan, R.R.; Irani-Hakime, N. A case control study on the contribution of factor V-Leiden, prothrombin G20210A, and MTHFR C677T mutations to the genetic susceptibility of deep venous thrombosis. J. Thromb. Thrombolysis 2005, 19, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Bremond-Gignac, D.; Daruich, A.; Gallet, M.; Menoud, P.A.; Nowomiejska, K.; Rejdak, R.; Behar-Cohen, F.; Benkhalifa, M.; Copin, H. Central retinal vein occlusion in otherwise healthy children and adolescents: Association With Multigenetic Variants of Thrombophilia. Retina 2020, 40, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Carare, R.O. Cerebral Vessels: An Overview of Anatomy, Physiology, and Role in the Drainage of Fluids and Solutes. Front. Neurol. 2020, 11, 611485. [Google Scholar] [CrossRef] [PubMed]
- Soylu, A.; Tokaç, M.; Cora, T.; Düzenli, M.A.; Acar, H. Platelet glycoprotein Ibalpha gene polymorphism and massive or submassive pulmonary embolism. J. Thromb. Thrombolysis 2009, 27, 259–266. [Google Scholar] [CrossRef]
- Afshar-Kharghan, V.; Li, C.Q.; Khoshnevis-Asl, M.; López, J.A. Kozak sequence polymorphism of the glycoprotein (GP) Ibalpha gene is a major determinant of the plasma membrane levels of the platelet GP Ib-IX-V complex. Blood 1999, 94, 186–191. [Google Scholar] [CrossRef]
- Cadroy, Y.; Sakariassen, K.S.; Charlet, J.P.; Thalamas, C.; Boneu, B.; Sie, P. Role of 4 platelet membrane glycoprotein polymorphisms on experimental arterial thrombus formation in men. Blood 2001, 98, 3159–3161. [Google Scholar] [CrossRef]
- Schneppenheim, R.; Hellermann, N.; Brehm, M.A.; Klemm, U.; Obser, T.; Huck, V.; Schneider, S.W.; Denis, C.V.; Tischer, A.; Auton, M.; et al. The von Willebrand factor Tyr2561 allele is a gain-of-function variant and a risk factor for early myocardial infarction. Blood 2019, 133, 356–365. [Google Scholar] [CrossRef]
- Sherry, S.T.; Ward, M.H.; Kholodov, M.; Baker, J.; Phan, L.; Smigielski, E.M.; Sirotkin, K. dbSNP: The NCBI database of genetic variation. Nucleic Acids Res. 2001, 29, 308–311. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 8 February 2023).
- Newcombe, R.G. Interval estimation for the difference between independent proportions: Comparison of eleven methods. Stat. Med. 1998, 17, 873–890. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variants | Act. Freq. CVT (%) | Calc. Freq. CVT (%) | Calc. Freq. NCBI (%) | p Value |
|---|---|---|---|---|
| FGA (rs6050) + F13A1 (rs5985) | 15.52 | 10.61 | 6.03 | <0.001 |
| FGA (rs6050) + ITGB3 (rs5918) | 9.48 | 5.62 | 3.87 | 0.004 |
| FGA (rs6050) + PROCR (rs867186) | 7.76 | 4.99 | 2.44 | 0.001 |
| ITGB3 (rs5918) + F13A1 (rs5985) | 11.21 | 4.55 | 3.81 | 0.001 |
| PROCR (rs867186) + F13A1 (rs5985) | 5.17 | 4.04 | 2.39 | 0.024 |
| PROCR (rs867186) + ITGB3 (rs5918) | 2.59 | 2.14 | 1.54 | 0.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kramer, R.A.; Zimmermann, R.; Strobel, J.; Achenbach, S.; Ströbel, A.M.; Hackstein, H.; Messerer, D.A.C.; Schneider, S. An Exploratory Study Using Next-Generation Sequencing to Identify Prothrombotic Variants in Patients with Cerebral Vein Thrombosis. Int. J. Mol. Sci. 2023, 24, 7976. https://doi.org/10.3390/ijms24097976
Kramer RA, Zimmermann R, Strobel J, Achenbach S, Ströbel AM, Hackstein H, Messerer DAC, Schneider S. An Exploratory Study Using Next-Generation Sequencing to Identify Prothrombotic Variants in Patients with Cerebral Vein Thrombosis. International Journal of Molecular Sciences. 2023; 24(9):7976. https://doi.org/10.3390/ijms24097976
Chicago/Turabian StyleKramer, Robert Anton, Robert Zimmermann, Julian Strobel, Susanne Achenbach, Armin Michael Ströbel, Holger Hackstein, David Alexander Christian Messerer, and Sabine Schneider. 2023. "An Exploratory Study Using Next-Generation Sequencing to Identify Prothrombotic Variants in Patients with Cerebral Vein Thrombosis" International Journal of Molecular Sciences 24, no. 9: 7976. https://doi.org/10.3390/ijms24097976
APA StyleKramer, R. A., Zimmermann, R., Strobel, J., Achenbach, S., Ströbel, A. M., Hackstein, H., Messerer, D. A. C., & Schneider, S. (2023). An Exploratory Study Using Next-Generation Sequencing to Identify Prothrombotic Variants in Patients with Cerebral Vein Thrombosis. International Journal of Molecular Sciences, 24(9), 7976. https://doi.org/10.3390/ijms24097976