Abstract
Eosinophils play a key role in airway inflammation in many diseases, such as allergic and non-allergic asthma, chronic rhinosinusitis with nasal polyps, and chronic obstructive pulmonary disease. In these chronic disabling conditions, eosinophils contribute to tissue damage, repair, remodeling, and disease persistence through the production a variety of mediators. With the introduction of biological drugs for the treatment of these respiratory diseases, the classification of patients based on clinical characteristics (phenotype) and pathobiological mechanisms (endotype) has become mandatory. This need is particularly evident in severe asthma, where, despite the great scientific efforts to understand the immunological pathways underlying clinical phenotypes, the identification of specific biomarkers defining endotypes or predicting pharmacological response remains unsatisfied. In addition, a significant heterogeneity also exists among patients with other airway diseases. In this review, we describe some of the immunological differences in eosinophilic airway inflammation associated with severe asthma and other airway diseases and how these factors might influence the clinical presentation, with the aim of clarifying when eosinophils play a key pathogenic role and, therefore, represent the preferred therapeutic target.
1. Introduction
Eosinophils are the key actor in airway inflammation in many conditions such as allergic and non-allergic asthma, chronic rhinosinusitis with nasal polyps (CRSwNP), and in chronic obstructive pulmonary disease (COPD). In these disorders, eosinophils contribute to tissue damage, repair, remodeling, and disease persistence through the production of a variety of mediators, including basic proteins (major basic protein, eosinophil cationic protein, eosinophil peroxidase, and eosinophil-derived neurotoxin), chemokines (CCL5, CCL11, CCL13), cytokines (interleukin (IL)-2, IL-3, IL-4, IL-5, IL-10, IL-12, IL-13, IL-16, IL-25), and growth factors (tumor necrosis factor, transforming growth factor α/β) [1,2]. IL-5 is the key factor responsible for eosinophils accumulation, activation, and terminal differentiation from hematopoietic progenitor cells in both the bone marrow and airways (in situ eosinophilopoiesis), and it is principally secreted by T-helper cell type 2 (Th2) lymphocytes and innate lymphoid cells–type 2 (ILC-2). The knowledge of molecular pathways sustaining the production of IL-5 and, consequently, of eosinophilia in respiratory disease is essential information to choose the most effective biological treatment for each patient. Five monoclonal antibodies (mAb) targeting some molecules participating in type 2 (T2) inflammation (i.e., anti-IL4/13, anti-IL-5, anti-IL-5Rα, anti-IgE, anti-thymic stromal lymphopoietin (TSLP)) are now available for severe asthma and some of them are also indicated for CRSwNP. Moreover, some clinical trials targeting eosinophilic inflammation in COPD are currently ongoing. In order to sharpen the biological drug choice, patient classification based on clinical characteristics (phenotyping) and pathobiological mechanisms (endotyping) has become mandatory [3]. The importance of selecting tailored treatments according to the patients’ features has been deeply investigated by many research groups, especially in severe asthma (SA) [4]. Several phenotypes of SA have been identified according to the age of disease onset, the number of previous exacerbations, the cell types dominating the inflammatory picture, and some comorbidities [5]. According to the expression of type 2 cytokines (IL-4, IL-5, and IL-13), SA has been classified as type 2-high (eosinophilic, T2-high) or type 2-low (non-eosinophilic, T2-low) phenotype [6,7].
T2-high asthma encompasses several asthma subtypes, such as early-onset allergic, late-onset eosinophilic asthma, and aspirin-exacerbated asthma [5]. The secretion of T2 cytokines can be driven by two non-mutually exclusive pathways. The first is sustained by Th2 cells activated by inhaled aeroallergens (allergen-specific IgE) in genetically susceptible individuals. The second is mediated by the ILC-2 upon stimulation with epithelial-secreted alarmins, such as TSLP, IL-25, and IL-33 [8,9].
The pathobiology of T2-low asthma is thought to be characterized by neutrophilic inflammation driven by Th1 and/or Th1/17 cell activation [5].
Although T2-high asthma is typically associated with eosinophils, their presence does not automatically mean that they play the most relevant pathogenetic role and that their ablation will be accompanied by a clinical response. Similarly, in subjects with systemic eosinophilia the presence of the atopic state does not guarantee an effective response to mAbs designed for patients with atopic asthma (e.g., anti-IgE or anti-IL4R). However, it is equally true that biological treatment can often lead to clinical remission of asthma [10], suggesting that the expected outcome of treatment can be achieved by targeting the specific drivers (endotypes) of the disease.
In this review, we describe some of the immunological differences in eosinophilic airway inflammation associated with SA and other airway diseases and how these factors might influence clinical presentation, with the aim of clarifying when eosinophils play a key pathogenic role and, therefore, represent the preferred therapeutic target.
2. Eosinophilopoiesis
Eosinophil development and maturation largely occur in the bone marrow from CD34+ hematopoietic precursors upon stimulation with IL-3, GM-CSF, and IL-5, which bind to receptors sharing a common beta chain.
IL-5 receptor, formed by a unique binging α chain (IL-5Rα), is upregulated on CD34+ cells at an early stage in eosinophil-lineage-committed progenitor cells (EoP) [11]. IL-5 plays a central role in the production, mobilization, activation, recruitment, and survival of eosinophils at the site of inflammation [12]. The expression of IL-5Rα on EoP is increased in the bone marrow of atopic asthmatics suggesting that, in atopic subjects, EoP are primed to promptly respond to IL-5 [13].
In addition to Th2 lymphocytes and ILC-2s, further sources of IL-5 are EoPs, invariant natural killer T cells, and mast cells [14]. However, IL-5 can be released by eosinophils themselves in an auto/paracrine manner [15].
Eosinophils recruitment from the blood into organs and tissues are favored by some chemokines, such as CCL5 (RANTES), CCL7 (MCP3), CCL11 (eotaxin 1), CCL13 (MCP-4), CCL15, CCL24, and CCL26. These chemokines act as eosinophil chemoattractant and bind to the CCR3 chemokine receptor, along with type 2 receptors (DP2 or CRTH2) and its ligand prostaglandin (PG) D2, orchestrating synergistically with IL-5 the migration of eosinophils from blood to the lungs [2,16,17].
There are data supporting the view that local maturational processes sustain the development of eosinophilia in the lung. Indeed, anti-CCR3 treatment has been reported to be insufficient to clear luminal airway eosinophils in moderately SA, likely because the treatment did not attenuate local eosinophil differentiation reflected in the lack of effect of the drug on sputum levels of either EoPs or mature eosinophils [18].
Th2 cells favor eosinophil activation and survival by releasing primarily IL-5 [19]. These data support the view that in situ eosinophilopoiesis promotes the development of lung eosinophilia and suggest that targeting local IL-5-driven expansion of EoPs may be an important approach to control persistent airway eosinophilia and clinical response to anti-eosinophil treatments in SA [20,21].
3. Eosinophils and Bronchial Asthma
3.1. Eosinophils in Type 2-High Asthma Phenotype
T2-high asthma phenotype as compared to T2-low phenotype is associated with higher blood eosinophil count, a greater expression of IL-5 in airway mucosa, more severe airway hyper-responsiveness, larger total serum IgE, and higher fractional exhaled nitric oxide (FeNO) [22].
IL-5 and IL-4/IL-13 are considered the key drivers of type 2 pathways underlying eosinophilic airway inflammation in asthma.
In allergic asthma, in genetically predisposed individuals, naïve CD4+ T cells are activated via presentation of allergens by dendritic cells differentiating into Th2 cells. Th2 cells produce cytokines, such as IL-4, IL-5, and IL-13, and lead to IgE switching from B cells, airway eosinophilia, and mucous hypersecretion [23]. In eosinophilic non-allergic asthma, the interaction of environmental pollutants, microbes, and glycolipids with airway epithelium induce the release of IL-33, TLSP, and IL-25 [24]. These epithelial-derived alarmins promote, in an antigen-independent manner, a T2-mediated inflammation by acting on ILC-2 cells, which, when activated, secrete high amounts of IL-5 and IL-13 that orchestrate the accumulation, activation, and differentiation of EoP in peripheral tissues [25]. The key pathogenetic role played by eosinophils in bronchial asthma is supported by some observation. Asthma severity correlates with the level of blood and airway eosinophils, and, in addition, treatments reducing sputum eosinophils level are able to reduce asthma exacerbations and spare corticosteroid use in patients with severe asthma [26].
FeNO and blood and sputum eosinophil count have been reported to predict T2-high phenotype in SA [27]. Indeed, these biomarkers are being used to select SA candidates to receive targeted T2 therapies such as anti-IL-5 or anti-IL-5Rα treatment and to anticipate the therapeutic response. Interestingly, in a non-selected population of SA, there was an overall discrepancy in the coexpression of biomarkers related to IL-5 and IL-13 pathways, suggesting the existence of distinct subtypes of T2-high SA [28]. Nonetheless, all the biological drugs available to date for the treatment of T2-high phenotype have shown a better response at the increasing number in blood eosinophil levels. However, considering only the number of circulating eosinophils in order to identify patients with eosinophilic-driven airway inflammation can often be misleading. Indeed, there is evidence for the existence of several eosinophil endotypes derived from different signals perceived by the developing progenitors of eosinophils. Data from mouse models, also confirmed in asthmatic patients, show that among asthma phenotypes there may be a different expression of eosinophil subpopulation differing from their localization (parenchymal/peribronchial), cellular density profiles (hypodense/normodense), asthma endotypes (allergic/non allergic eosinophilic), surface adhesion capacity, and responsiveness to IL-5 [29]. In addition, regulatory and inflammatory subsets of eosinophils have also been documented in a murine model of eosinophilic esophagitis [30,31] (Figure 1).
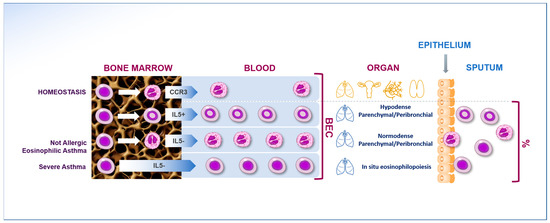
Figure 1.
Eosinophil endotypes derived from different signals perceived by the developing progenitors of eosinophils. There may be a different expression of eosinophil subpopulation differing from their localization (parenchymal/peribronchial and in situ), cellular density profiles (hypodense/normodense), asthma endotypes (allergic/non-allergic eosinophilic), and responsiveness to IL-5.
The ability to distinguish systemic eosinophilia with pathogenetic relevance in the airways from systemic non-inflammatory eosinophilia as an epiphenomenon linked to specific/non-specific stimuli promoting the production of Th2 cytokines helps to define whether eosinophils drive the disease.
3.2. Eosinophils in Type 2-Low Asthma Phenotype
In type 2-low asthma, the upregulation of T2 immune pathways (e.g., IL-4 and IL-13) and eosinophilic inflammation characteristic of type 2-high phenotype are classically absent, contributing to the poor response to corticosteroids [32]. Although the pathogenesis of type 2-low asthma is not completely elucidated, the following mechanisms have been suggested to play a role in this subtype of asthma: (i) type 1 (IFN-mediated) and type 3 (IL-17-mediated) immune pathways together with airway neutrophilia; (ii) pauci-granulocytic mechanisms; (iii) systemic inflammation associated with IL-6, obesity, and metabolic dysfunction [32]. In particular, murine models show that IL-17 contributes to neutrophilic airway inflammation, bronchial hyper-responsiveness, mucus hypersecretion, airway obstruction, and corticosteroid resistance [33,34,35]. In addition, levels of Th17-derived IL-17 in the airway and peripheral blood correlate with disease severity [34,36]. Despite this evidence, recent studies demonstrate that patients with severe type 2-low asthma do not respond to anti-IL-17 treatments [37].
Eosinophilic and neutrophilic asthma are not mutually exclusive subtypes. The concomitance of activation of type 2 immune pathways in these patients may sometimes occur, further worsening the clinical and functional outcome. Indeed, in the airway of patients with SA, eosinophils can accumulate together with neutrophilic count increase [38]. In addition, the inflammation pattern may change in the same patient over time. In a large retrospective study [39], the authors analyzed 1786 consecutive sputum cell counts from 1139 patients with airway disease, reporting changes in the cellular nature of airway inflammation among consecutive exacerbations in 48% of the patients. The existence of a dynamic interplay between type 2-high and type 2-low pathways in different phases of airway inflammation is supported also by the identification in the circulation of patients with bronchial asthma of a subset of T cells (Th17/Th2 cells) that can secrete both IL-4 and IL-17 [40]. These findings strengthen the hypothesis that different inflammatory phenotypes can coexist in one patient and alternate according to the different stages of the disease.
3.3. Early-Onset Allergic Disease vs. Late-Onset Eosinophilic Airway Disease
Approximately 40–50% of all patients with asthma develop the disease during childhood (early-onset asthma). Generally, these patients are atopic with multiple sensitizations to allergens [41]. High total IgE, high FeNO levels, and increased sputum and blood eosinophils characterize patients with severe early allergic asthma. In these cases, airflow limitation and airway remodeling could appear early.
Late-onset eosinophilic asthma phenotype, often non-allergic, is present in about 25% of SA patients and present persistent airflow limitation, accelerated decline of lung function, often requiring high doses of inhaled corticosteroids (ICS) or being refractory to oral corticosteroids (OCS) treatment [42]. Another recognizable clinical characteristic, especially in severe late-onset asthma, is the concomitance of CRSwNP [43] and blood eosinophils count [44,45]. It has been suggested that ILC-2 activation plays a role in both early-onset allergic asthma and in the late-onset asthma with CRSwNP phenotype [46].
It has been widely demonstrated that in the late-onset eosinophilic phenotype, the presence of allergy does not represent a factor impacting the efficacy of the anti-eosinophilic therapeutic approach [47,48], demonstrating how this eosinophil-driven phenotype is untied to allergenic stimuli and therefore could not be effectively modulated using drugs targeting T2 inflammatory cytokines (anti IL-5 and IL-4/13) or anti-IgE. This observation resembles the immunological phenotype switch observed in patients with eosinophilic esophagitis in which children seem to respond more to target food elimination than adults [49]. Discrepancies in response between children and adults may suggest a decreasing pathogenic role of IgE in the transition from childhood to adulthood.
3.4. Current and Novel Biomarkers of Eosinophilic Airway Inflammation
The new therapeutic frontiers in SA reflect the need to identify reliable biomarkers capable of identifying different phenotypes and endotypes of asthmatics to guide the therapeutic choice. Table 1 summarizes the main molecules studied so far for this purpose.

Table 1.
Current and potential future biomarkers for severe asthma.
Blood eosinophil count is a commonly used indicator of T2 inflammation in routinary clinical practice. It is easily measured and reproducible. In addition, it has been shown to correlate with risk of exacerbations in patients with SA [68]. Moreover, eosinophils levels ranging from 150 to 400 cell/µL can also predict the response to treatment with mAbs, targeting the IL-5 pathway. The MENSA and DREAM studies pointed out that patients with levels of eosinophils ≥ 150 cell/µL have a better response to mepolizumab (mAb targeting IL-5) [69,70]. Otherwise, in SIROCCO and CALIMA studies, patients with severe asthma and eosinophils ≥ 300 cell/µL had a better response to benralizumab (mAb targeting IL-Rα) [71,72]. Finally, studies conducted with the use of reslizumab (mAb targeting IL-5) showed a reduction in exacerbation rate and improvement in lung function in patients with eosinophils ≥ 400 cells/µL [52]. However, eosinophils as a biomarker have low specificity since they can be elevated in several autoimmune and atopic diseases. In addition, non-respiratory diseases influence B-Eos count but not FeNO or CRP. Male sex, obesity, certain races/ethnicities, and current smoking are individual characteristics or exposures that are associated with higher B-Eos counts [73]. Moreover, a single determination of blood eosinophil count is often inadequate. Indeed, the Global Initiative for Asthma (GINA) guidelines suggest the need for at least three measurements to identify eosinophilic asthma phenotype [74,75]. In addition, based on the International Severe Asthma Registry (ISAR), patients with SA are classified as eosinophilic phenotype, based not only on blood eosinophil count but also on some clinical features (i.e., OCS dependency, presence of CRSwNP, elevated FeNO, and late onset of the disease) [76]. These clinical features are closely associated with the eosinophilic asthma phenotype because their prevalence increase as the number of blood eosinophils increases, thus suggesting that they may be directly linked with the eosinophilic phenotype and be predictor of successful response to anti-eosinophilic treatment [47,48,49,77,78,79]. Another key point is given by the fact that some scientific evidence has shown discordance between blood and sputum eosinophil count, particularly observed in OCS-dependent asthmatics [80]. These findings do not support the role of absolute eosinophil count as the only biomarker for anti-IL-5 mAb treatment response. This discordance is likely due to in situ eosinophilopoiesis, resulting from incomplete neutralization of IL-5 produced in airways by ILC-2 cells. Moreover, in a retrospective study on 508 asthmatics with successful sputum induction, Schleich et al. [81] investigated the prevalence and characteristics of patients with concordant and discordant systemic and bronchial eosinophilia. Asthmatics with isolated systemic eosinophilia (7%) had similar characteristics as non-eosinophilic asthmatics. The group with concordant systemic and airway eosinophilia (19%) showed remarkable male predominance, and had the lowest airway caliber, asthma control, and quality of life, and the highest airway hyper-responsiveness, exacerbation rate, and FeNO.
FeNO is an indirect biomarker of airway type 2 inflammation, and its production is enhanced by the IL-13 and IL-4 pathways that promote the activity of NO synthase [82,83,84,85]. Eosinophilic inflammation is highly probable with FeNO levels above 50 ppb and unlikely when FeNO levels are below 25 ppb [86]. From a clinical perspective, FeNO has a potential role in guiding adjustments in dosing ICS, with a reduction in exacerbation rate [86]. Furthermore, FeNO levels are higher in naïve corticosteroids patients, so it can be used as an indicator of poor patient compliance.
FeNO levels also correlate with the therapeutic response to dupilumab (anti-interleukin-4 receptor α mAbs that blocks both interleukin-4 and interleukin-13 signaling) since several studies showed that FeNO levels decreased during treatment with this drug [87,88]. Contrarily, FeNO is not affected by biologics targeting IL-5 as mepolizumab. Indeed, mepolizumab has been shown to decrease consistently the blood and sputum eosinophil count in patients with eosinophilic asthma, with no effect on FeNO levels [89]. FeNO is considered a biomarker of T2-driven airway inflammation. Although it correlates with airway eosinophilia in steroid-naïve patients, it can be independent from eosinophils and therefore not helpful in monitoring the response to anti-IL-5 mAb [90]. However, the prognostic and predictive value of FeNO as a biomarker may have several limits, as it can be influenced by several confounders, including age, height, sex, and recent respiratory infections [70]. In addition, FeNO is strongly associated with atopy and may be increased in the absence of eosinophilic inflammation [91,92].
Current and previous evidence have suggested FeNO as a surrogate marker for sputum eosinophilia [93]. Contrariwise, low FeNO despite high sputum eosinophils has been reported in some adult asthmatic patients [94]. Other evidence about the decoupling of FeNO from sputum eosinophilia came from a study by Wenzel et al., in which no improvement in the levels of blood or sputum eosinophilia was found with dupilumab despite the decrease in other biomarkers such as FeNO and the improvement of forced expiratory volume in 1 s (FEV1) [25]. In the study by Crespo et al. [12], a discrepancy between FeNO and sputum eosinophil count was observed in about 42% of patients. Of these patients, 73.9% with a predominance of non-allergic asthma had a FeNO <50 ppb and high eosinophil count. The remaining patients with a predominance of atopy and pauci-granulocytic inflammatory phenotype (26.1%) had FeNO ≥50 ppb and normal sputum eosinophilic count.
The causes of these observations are not completely elucidated. A possible explanation may be found in the differences between molecular pathways leading to increase in FeNO and recruitment and activation of eosinophils. Overall, given the above conflicting evidence, further ad hoc studies are needed to clarify whether FeNO could be effectively considered in the near future for routine use as a biomarker of airway eosinophilia in different clinical and healthcare settings (i.e., community, hospital, rehabilitation) [95,96].
Another molecule that has been proposed as surrogate marker of Th2 inflammation in SA is periostin, an extracellular matrix proteinase, produced by bronchial epithelial cells in response to IL-4 and IL-13. Periostin is also implied in asthma airway remodeling, as it promotes activation of fibroblasts and has autocrine effects on the epithelial cells [57]. As a biomarker, higher levels of periostin correlate with higher exacerbation rate and poor asthma control [97]. Serum periostin levels respond partially to ICS therapy, possibly reflecting a reduction in airway inflammation and wall thickening in asthma [98]. In addition, biologics targeting IL-4/1L-13 (dupilumab) [99,100] and IL-13 (i.e., lebrikizumab) [101,102] have been shown to suppress serum periostin levels in asthma patients.
However, periostin has low specificity, since its levels are influenced by age and other disease as atopic dermatitis, scleroderma, cancer, and diabetic nephropathy [74].
T2-high asthma phenotype hosts up to 70% of SA patients and occurs in both allergic and non-allergic asthma. Owing to difference in blood eosinophil count [103], age at disease onset (early vs. late), clinical presentations (e.g., influence of allergy on symptoms), and presence of comorbidities (e.g., CRSwNP, atopic dermatitis, and obesity), T2-high asthma phenotype represents a highly heterogeneous group [43]. Thus, the conventional available biomarkers of T2 pathways (blood eosinophil count, FeNO, and serum IgE) are both individually or in combination unpowered to identify and rank the driver of the disease (e.g., IL-4, IL-5, IL-13, or IgE) [27]. The picture is further complicated because these biomarkers are not necessarily correlated with each other. In a study by Frossing et al. [28], the elevation in at least one biomarker was reported in 70% of patients with SA, while the simultaneous increase in all three biomarkers was observed in only 15%. The prevalence of elevation of each biomarker in isolation was reported in about 40% of the study group. However, the combined use of FeNO and blood eosinophils count should be recommended as they offer independent information in relation to risk for asthma morbidity [104].
This observation suggests that the degree of activation of different T2 pathways varies among patients, underscoring the importance of multiple domains characterization of T2 pathways in order to achieve better patient stratification.
4. Eosinophilic Airway Inflammation and Comorbidities
Upper and lower airways are considered a unified morphological and functional unit, and the connection existing between them has been observed for many years [105]. About 60% of patients with CRSwNP present comorbid asthma (with and without NSAID-exacerbated respiratory disease), predominantly atopic and not severe [106]. Accordingly, about 25% of patients with severe eosinophilic asthma have a comorbid CRSwNP [77].
Increased nasal polyposis and oral steroid courses for chronic rhinosinusitis (CRS) are reported in late-onset severe asthma as compared to early-onset asthma [107]. In CRS, as in asthma, the activation of ILC-2 cells leads to the release of cytokines (Il-9, Il-4, Il-5, and IL-13) stimulating a Th-2 inflammatory response [108,109]. As for asthma, there are different inflammatory phenotypes and endotypes of CRS. Diverse immune cells and inflammatory mediators orchestrate this heterogeneous disease spectrum, which comprises CRSwNP and CRS without nasal polyps (CsNP) [110,111,112]. Two distinct phenotypes of CRSwNP have been described, one with eosinophilic CRS (ECRSwNP) and one with non-eosinophilic CRS (NECRSwNP). ECRSwNP is a disabling condition associated with severe eosinophilic infiltration and more severe sinus inflammation on sinus CT scan and nasal endoscopy compared to those with NECRSwNP [113]. Tissue eosinophilia was also a predictor of nasal polyp recurrence following surgery, another indicator of more recalcitrant disease. The diagnosis of ECRS is made by examination of a biopsy specimen or resected tissue [114]. Moreover, for determining the severity of ECRS several factors have been proposed, including peripheral blood eosinophil, ethmoid sinus-predominant involvement on CT scans, and the presence of complications (current asthma or a history of asthma, aspirin intolerance, and/or NSAID allergy). On the other side, blood and sputum eosinophil levels in patients with asthma are directly correlated with sinus mucosal thickening osteitis and are associated with increasing number of prior sinus surgery, lending further support to the hypothesis that similar inflammatory processes [115] mediate both asthma and CRS.
There is still no standardized process to establish the most appropriate therapy for asthmatic patients with nasal polyps. What is emerging quite clear from both randomized and real-world evidence studies is that, more than an asthma comorbidity, the presence of nasal polyposis is a hallmark of late-onset eosinophilic asthma identifying a phenotype particularly responsive to anti-eosinophilic therapy with improvement of quality of life, lung function, and reduction in asthma exacerbations [116]. The presence of CRSwNP in patients with SA is accompanied by a more extensive eosinophilic inflammation and therefore it can benefit more from a direct anti-eosinophilic approach [117].
Anti-IL-5 and anti-IL-5Rα in real-life studies have shown to significantly reduce eosinophils number in nasal polyps, the latter with a complete reduction in eosinophils- and neutrophils-infiltrated cells, with a significant reduction in the nasal polyp score (NPS) after 6 months [118]. However, despite a significant improvement in nasal symptomatology, as assessed by the Sinonasal Outcome Test 22 (SNOT-22) questionnaire, achieved by these anti-eosinophilic drugs, as for other biologics, not all patients showed significant clinical improvement based on computed tomography (CT) and endoscopic results. The variability in the therapeutic response observed in these patients is linked to the great heterogeneity of the disease and further investigations aimed at better characterizing and phenotyping of CRSwNP are necessary.
Another comorbidity which should be actively investigated and treated as a possible trigger factor of uncontrolled asthma is gastroesophageal reflux disease (GERD) [119,120]. This condition should also be ruled out before SA is diagnosed and biologic therapy is started. Both eosinophilic type 2 inflammatory changes and neutrophilic inflammation have been described in patients with GERD [120,121].
Obesity has been associated to airway inflammation and is generally considered a feature of late-onset non-eosinophilic asthma [122]. However, some studies have reported higher levels of airway IL-5 and eosinophils in obese patients in general [123], and the Severe Asthma Research Program (SARP) has also identified a group of predominantly females with severe late-onset asthma, obesity, and increased sputum eosinophils [124]. Therefore, obesity may be associated to both eosinophilic and neutrophilic asthma.
The role of eosinophils is under investigation in several other chronic respiratory conditions including allergic fungal airway disease and chronic idiopathic eosinophilic pneumonia [1,125,126,127].
Systemic hypereosinophilic diseases including eosinophilic granulomatosis with polyangiitis (EGPA) can also be associated with airway inflammation and severe asthma [119,128,129]. An early identification of these disabling diseases is essential as they require a multidisciplinary approach and systemic corticosteroids and/or immune-suppressant therapies.
5. Eosinophils and Chronic Obstructive Pulmonary Disease
In recent years, understanding of the pathogenetic mechanisms involved in COPD has greatly increased [130]. Indeed, the awareness of the wide range of inflammatory patterns that can be observed in this disabling condition led to the identification of more personalized rehabilitation and pharmacological approaches [131,132,133,134,135], with a potential role for biologically targeted therapies. The inflammatory pattern in COPD is extremely variegated. In most of the cases, the inflammatory environment in the airways of COPD patients is dominated by neutrophils, cytotoxic CD8+ T cells, and alveolar macrophages [136]. However, eosinophils may also play a key role in a subset of COPD patients [2,137].
In fact, several studies have shown that eosinophils may be involved in the inflammatory response in COPD, as under certain circumstances, inflammatory cues promote eosinophil recruitment to the lungs, where secretion of a variety of chemokines and cytotoxic granular products contributes to inflammation [138].
Increased levels of eosinophils can be detected in the sputum of approximately one-third of COPD patients, overcoming the old-fashioned concept that eosinophilia is a feature that can be used for distinguishing COPD from asthmatic patients [139,140]. In addition, sputum eosinophilia is particularly increased during COPD exacerbations [140]. Additionally noteworthy is that blood and/or sputum eosinophilia is a biomarker of beneficial responses to inhaled or systemic glucocorticoids for preventing or treating the exacerbations, respectively [2,141]. Evidence from the Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-Points (ECLIPSE) study have shed light on the prevalence of eosinophilic inflammation in COPD patients, pointing out that the elevation of eosinophils in COPD patients is intermittent rather than constant [142]. Indeed, 37.4% of patients with COPD had blood eosinophil counts persistently elevated (≥2%) over a three-year follow-up period, whereas 49% had intermittent elevation of these cells. In addition, the authors described some common features among COPD patients with eosinophil counts persistently ≥2% (i.e., older age, male gender, fewer current smokers, higher FEV1% predicted, higher fat-free mass index, fewer symptoms, and lower BODE (body mass index, airflow obstruction, dyspnoea, exercise capacity index) [142]. Interestingly, in the ECLIPSE study, although the subjects with high blood eosinophil counts had better clinical characteristics at baseline, they also showed increased rate of emphysema progression, further confirming the pathogenetic role of this cell in airway inflammation, tissue damage, and remodeling [142,143]. In addition, exploring the relationship between lung function and sputum eosinophilia, several studies have shown a link between airway obstruction and eosinophilic lung inflammation. Indeed, a higher concentration of both eosinophils and their products, such as eosinophil cationic protein, have been related to worse lung function, as expressed by lower FEV1 values [144].
The above reported findings about the persistence of eosinophilia in COPD patients are also in contrast with data from the Acute Exacerbation and Respiratory Infections in COPD (AERIS) study, which reported persistent blood eosinophilia ≥2% in most of their cohort (58%) over 1 year [145].
A few studies have attempted to establish a relationship between eosinophils blood count and the development of pneumonia in COPD patients, considering also the antimicrobial defense role of these cells, with mixed results. Some authors report no difference in pneumonia incidence between COPD patients with low and high eosinophils levels [146], while other research groups found that patients with higher eosinophils levels (≥2%) had slightly fewer episodes of pneumonia [141,147].
In conclusion, further studies are needed to better elucidate the fluctuation of eosinophils levels in COPD patients and correlate them with lung function and clinical outcome in long-term follow-up.
6. Target Therapies in Eosinophilic Airway Disease
6.1. Eosinophils and Oral Corticosteroid Dependence
OCS dependence is reported in a subset of SA phenotype that, although representing only a small proportion of the asthmatic population, requires personalized treatment because of its increased morbidity, hospitalization, and mortality.
These patients remain symptomatic and present persistent airway eosinophilia despite treatment with high-dose ICS and OCS. Several cellular and molecular mechanisms related to immunological dysregulation, genetic and environmental factors, or respiratory infections have been related to OCS insensitivity in asthma [148].
Eosinophils, during their migration from the bone marrow to tissues and then to airway lumen, undergo phenotypic changes in response to tissue microenvironmental cues, including altered morphology, enhanced responsiveness to cytokines, different susceptibility to chemotactic mediators, and various degrees of cellular activation, likely acquiring a different susceptibility to pharmacological treatments [149,150,151]. So, indirect anti-eosinophil approaches may not be completely effective in reducing eosinophil number at all degrees of asthma severity, in all compartments and/or for all T2-high phenotypes [152]. In a recent real-life clinical study, suboptimal responses were observed in 42.8% of 250 moderate-to-severe asthmatic patients treated with anti-IL-5 mAbs (i.e., mepolizumab, reslizumab). In that study, daily prednisone requirement, sinus disease, and late-onset asthma diagnoses were the strongest predictors of suboptimal response. Importantly, after 4 months of treatment, reduced blood and sputum eosinophil values were available in 129 patients: 65 patients were suboptimal responders and in 78% of them sputum eosinophil value was >3% [153]. These data, on the one hand confirm the strong correlation between sputum eosinophilia and OCS dependence, and on the other hand, are in line with the observation of the incomplete reduction in eosinophils in blood and tissues in IL-5 or IL5-Rα knockout mouse model, suggesting that IL-5 may not be the only driver of eosinophilia [154].
Tissue eosinophils may be resilient to some extent against anti-IL-5 therapies because molecules other than IL-5, such as IL-3 and GM-CSF, can sustain them. The latter was also identified as a predictor of suboptimal response for anti-IL-5 mAbs treatment [153].
These data are in contrast with what has been observed in 18 patients with SA and elevated blood eosinophils who relied on OCS therapy to control their disease. In this subset of patients, anti-IL-Rα (benralizumab) showed a significant reduction in both circulating and sputum numbers of mature eosinophils and EoP cells, suggesting that targeting IL-5Rα+ cells decreases EoP cell numbers both systemically and within the airways, thereby attenuating the potential IL-5–driven in situ eosinophilopoietic processes that may contribute to persistent airway eosinophilia in patients with severe, prednisone-dependent asthma [155]. Collectively, these data support the substantial difference existing between a direct and indirect approach to eosinophils.
6.2. Biological Therapies and Eosinophilic Inflammation in Severe Asthma
In recent years, a wide range of mAbs targeting IgE or type 2 cytokines have been proved to be highly effective and safe in reducing symptoms and exacerbation in patients with severe allergic and eosinophilic asthma [156]. However, these therapies are not suitable for about half of patients with severe asthma who often present with non-allergic, non-eosinophilic type 2-low asthma [60,157,158]. For this reason, in the era of precision medicine, investigating the different pathways involved in the different endotypes of asthma can help identify new targeted therapies (Table 2).
Table 2.
Current and future biological therapies for type 2-high severe asthma.
In SA, the identification of specific biomarkers has become the basis for a personalized approach that has replaced the conventional treatment based on corticosteroids and bronchodilators drugs. However, the response to biologics targeting T2 pathways is variable and often unpredictable. Although the origin of this variability is multifactorial, the differences in baseline patient characteristics and the complexity and heterogeneity of biological pathways orchestrating T2 responses are the major determinants. The role played by individual cytokines in T2 inflammatory processes is variable as each of them may be involved to a greater or lesser extent in the initiation, maintenance, and amplification of the inflammatory process. A further complication derives from the fact that in the individual patient, the cytokines and the cells on which they act can vary during the course of the disease and in the different target organs. As a consequence, targeting a single cytokine generally does not result in complete abrogation of the inflammatory response in a large majority of patients.
The selection of the most appropriate biologic for each patient should be made on the basis of the patient’s clinical characteristics (atopy, blood eosinophil count, sputum eosinophil count, and FeNO level) and taking into account the patient’s comorbidities (CRS, atopic dermatitis, urticaria, and obesity) [168].
Patients with asthma that is clearly driven by a clinical history of allergies (rather than just an elevated IgE level) are candidates for anti-IgE therapy.
In subjects with severe T2 eosinophilic phenotype asthma, the presence of comorbidities affecting the upper airways increases as peripheral eosinophilia increases and, therefore, patients with these characteristics may benefit more from treatment with IL-5/Rα, even if the anti-IL-4/13 and anti-IgE treatment are recommended as first-line treatments in these patients. However, in asthmatic patients with overlapping phenotypes, the choice of the biological drug able to guarantee the best therapeutic response is still an unsolved problem.
6.3. Biological Therapies and Eosinophilic Inflammation in CRSwNP
Several mAb targeting T2 inflammation (IL-4Rα, IgE, and IL5/Rα) have been approved or are currently in phase 3 clinical trial as add-on therapy for CRSwNP. Dupilumab was the first Food and Drug Administration (FDA)-approved biologic agent in the United States and Europe for the treatment of CRSwNP. Two wide, double-blind, placebo-controlled, international phase 3 studies (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52) enrolling 724 patients with refractory CRSwNP, assessed the efficacy and safety of dupilumab (300 mg every 2 weeks or 4 weeks subcutaneously) in improving nasal symptoms, disease specific quality of life, use of systemic corticosteroids, and/or the need for nasal polyp surgery [106].
Some of the strongest evidence regarding the effectiveness of mepolizumab in improving nasal polyp size and nasal obstruction in CRSwNP, which have led to the approval of the drug for this disabling condition, came from the SYNAPSE study [169].
In this randomized, double-blind, placebo-controlled, parallel group study, the effect of subcutaneous mepolizumab was evaluated in 407 adult patients with highly symptomatic CRSwNP uncontrolled by previous surgery and treated with intranasal steroids. The treatment demonstrated significant improvement in terms of size of nasal polyps and nasal obstruction at week 52 compared with placebo.
In a study conducted in 44 subjects with severe eosinophilic asthma and CRSwNP, mepolizumab administered for one year achieved clinical improvement in both asthma and rhinosinusitis. In addition, the mean percent of eosinophil count in nasal cytology, as compared to baseline, significantly decreased after 6 and 12 months of treatment, suggesting that clinical efficacy of mepolizumab is related to reduced inflammation at tissue level [170]. Similar results have been reported by Walter et al. [171].
Omalizumab has also shown significant superiority to placebo in the POLYP I (n = 138) and POLYP II (n = 127) phase 3 trials conducted over a treatment period of 24 weeks followed by a 4-week follow-up period [159], and it is currently indicated as an add-on therapy with intranasal corticosteroids when this treatment does not provide adequate disease control.
Benralizumab has shown promising results in the phase 3 OSTRO study, including 413 randomized patients with severe CRSwNP (207 in the benralizumab group and 206 in the placebo group), demonstrating a reduction in nasal polyps score and improved nasal symptoms as nasal obstruction and difficulty with sense of smell [172]. Another phase 3 trial evaluating efficacy and safety of benralizumab in ECRSwNP (ORCHID; NCT04157335) is currently ongoing. A prospective observational study (NCT03369574) aimed at monitoring CRS symptoms in asthma patients undergoing treatment with reslizumab, evaluating the potential benefit on CRS symptoms, has been withdrawn.
No documented study in CRSwNP is presently available for mAb targeting IL-13, tralokinumab, and lebrikizumab.
6.4. Biological Therapies and Eosinophilic Inflammation in Chronic Obstructive Pulmonary Disease
Although there is evidence supporting the existence of eosinophilic inflammation in a subgroup of COPD patients, findings from phase 2 and 3 trials evaluating the efficacy of T2-targeted therapies in COPD have been disappointing as compared to those in asthma patients [137].
A pilot randomized clinical trial (NCT01463644) evaluating 18 subjects treated with mepolizumab given once a month intravenously at the dose of 750 mg for 6 months versus placebo, demonstrated a reduction in blood and sputum eosinophils, without any significant change in FEV1, diffusing capacity of the lung for carbon monoxide values, radiological evidence of remodeling, COPD Assessment Test, Chronic Respiratory Disease Questionnaire, and exacerbation rate [173]. Other phase 3, randomized, double-blind, parallel-group trials, namely METREX (NCT02105961) and METREO (NCT02105948), compared the efficacy of subcutaneous injection of mepolizumab given, respectively, at the dose of 100 or 300 mg every 4 weeks in patients with eosinophilic-phenotype COPD patients with history of moderate or severe exacerbations [174]. The authors reported a lower annual rate of moderate or severe exacerbations than placebo among patients with higher blood eosinophil counts at screening, with no differences in patient-reported outcomes and/or lung-function end points [174].
A randomized, double-blind, placebo-controlled, phase 2a study investigated efficacy and safety of benralizumab subcutaneously, every 4 weeks (three doses), then every 8 weeks (five doses) over 48 weeks in a cohort of 101 patients with moderate-to-severe COPD and a sputum eosinophil count of 3·0% or more within the previous year, reporting no significant reduction in the rate of acute exacerbations [175]. Similarly, the TERRANOVA (NCT02155660) and GALATHEA (NCT02138916) randomized placebo-controlled studies analyzed the effect of benralizumab (30 or 100 mg in GALATHEA; 10, 30, or 100 mg in TERRANOVA every 4 weeks for the first three doses and then every 8 weeks) versus placebo on the annualized COPD exacerbation rate in patients with blood eosinophil counts ≤220/mm3 gave disappointing results [176].
Other biological drugs investigated in moderate-severe COPD patients with T2 inflammation are dupilumab, for which two clinical trials are currently ongoing (NCT04456673; NCT03930732) and lebrikizumab (VALETA, NCT02546700), which have been completed, but the results are not yet available. The details of these studies are available at the website www.clincaltrials.gov. No documented study in COPD is currently available for reslizumab and tralokinumab.
Collectively, this evidence demonstrates that the role of eosinophils in COPD is more complex than in asthma. Therefore, in order to obtain a substantial improvement in patients’ outcome and respiratory function tests, it would be necessary to act on multiple pathways or cells other than eosinophils, such as T and B cells, macrophages, basophils, and mast cells.
7. Conclusions
In recent years, understanding the role of eosinophil as the driver of pathology in respiratory diseases has increased. The role of eosinophils as biomarkers of T2 inflammation is now established. Furthermore, new eosinophil-targeting therapies have been developed, allowing for better management and therapeutic care of patients. However, the full immunological differences across the spectrum of T2 eosinophilic inflammation and how these differences might influence the clinical presentation and evolution of the diseases are not completely known. Further studies should help understand the contribution of eosinophils in respiratory diseases.
Author Contributions
M.M. (Mauro Mormile) and I.M. conceived and designed the study, interpreted literature data, and drafted the manuscript. S.F. and F.W.R. acquired literature data. L.L. and P.A. interpreted literature data and performed critical revisions. A.d.P. drafted the manuscript and performed critical revisions. M.M. (Mauro Maniscalco) supervised the project, interpreted literature data, and drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partially supported by the “Ricerca Corrente” funding scheme of the Ministry of Health, Italy.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were generated or analyzed for this review article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wechsler, M.E.; Munitz, A.; Ackerman, S.J.; Drake, M.G.; Jackson, D.J.; Wardlaw, A.J.; Dougan, S.K.; Berdnikovs, S.; Schleich, F.; Matucci, A.; et al. Eosinophils in Health and Disease: A State-of-the-Art Review. Mayo Clin. Proc. 2021, 96, 2694–2707. [Google Scholar] [CrossRef] [PubMed]
- Mycroft, K.; Krenke, R.; Gorska, K. Eosinophils in COPD-Current Concepts and Clinical Implications. J. Allergy Clin. Immunol. Pract. 2020, 8, 2565–2574. [Google Scholar] [CrossRef] [PubMed]
- Carr, T.F.; Berdnikovs, S.; Simon, H.U.; Bochner, B.S.; Rosenwasser, L.J. Eosinophilic bioactivities in severe asthma. World Allergy Organ. J. 2016, 9, 21. [Google Scholar] [CrossRef]
- Israel, E.; Reddel, H.K. Severe and Difficult-to-Treat Asthma in Adults. N. Engl. J. Med. 2017, 377, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, M.E.; Lee, F.E.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin. Rev. Allergy Immunol. 2019, 56, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, S.G.; Lloyd, C.M. Eosinophils in the pathogenesis of allergic airways disease. Cell Mol. Life Sci 2007, 64, 1269–1289. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaian, F.; Ledford, D.K.; Casale, T.B. Biologic and New Therapies in Asthma. Immunol. Allergy Clin. N. Am. 2017, 37, 329–343. [Google Scholar] [CrossRef]
- Fahy, J.V. Type 2 inflammation in asthma—Present in most, absent in many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef]
- McGregor, M.C.; Krings, J.G.; Nair, P.; Castro, M. Role of Biologics in Asthma. Am. J. Respir. Crit. Care Med. 2019, 199, 433–445. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Bafadhel, M.; Busse, W.W.; Casale, T.B.; Kocks, J.W.H.; Pavord, I.D.; Szefler, S.J.; Woodruff, P.G.; de Giorgio-Miller, A.; Trudo, F.; et al. An expert consensus framework for asthma remission as a treatment goal. J. Allergy Clin. Immunol. 2020, 145, 757–765. [Google Scholar] [CrossRef]
- Mori, Y.; Iwasaki, H.; Kohno, K.; Yoshimoto, G.; Kikushige, Y.; Okeda, A.; Uike, N.; Niiro, H.; Takenaka, K.; Nagafuji, K.; et al. Identification of the human eosinophil lineage-committed progenitor: Revision of phenotypic definition of the human common myeloid progenitor. J. Exp. Med. 2009, 206, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Crespo, A.; Giner, J.; Torrejon, M.; Belda, A.; Mateus, E.; Granel, C.; Torrego, A.; Ramos-Barbon, D.; Plaza, V. Clinical and inflammatory features of asthma with dissociation between fractional exhaled nitric oxide and eosinophils in induced sputum. J. Asthma 2016, 53, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Sehmi, R.; Howie, K.; Sutherland, D.R.; Schragge, W.; O’Byrne, P.M.; Denburg, J.A. Increased levels of CD34+ hemopoietic progenitor cells in atopic subjects. Am. J. Respir. Cell Mol. Biol. 1996, 15, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Molofsky, A.B.; Nussbaum, J.C.; Liang, H.E.; Van Dyken, S.J.; Cheng, L.E.; Mohapatra, A.; Chawla, A.; Locksley, R.M. Innate lymphoid type 2 cells sustain visceral adipose tissue eosinophils and alternatively activated macrophages. J. Exp. Med. 2013, 210, 535–549. [Google Scholar] [CrossRef]
- Huang, C.D.; Wang, C.H.; Liu, C.Y.; Lin, S.M.; Chou, C.L.; Liu, W.T.; Lin, H.C.; Kuo, H.P. Eosinophils from asthmatics release IL-5 in an autocrine fashion to prevent apoptosis through upregulation of Bcl-2 expression. J. Asthma 2005, 42, 395–403. [Google Scholar] [CrossRef]
- Nussbaum, J.C.; Van Dyken, S.J.; von Moltke, J.; Cheng, L.E.; Mohapatra, A.; Molofsky, A.B.; Thornton, E.E.; Krummel, M.F.; Chawla, A.; Liang, H.E.; et al. Type 2 innate lymphoid cells control eosinophil homeostasis. Nature 2013, 502, 245–248. [Google Scholar] [CrossRef]
- Smit, J.J.; Lukacs, N.W. A closer look at chemokines and their role in asthmatic responses. Eur. J. Pharmacol. 2006, 533, 277–288. [Google Scholar] [CrossRef]
- Neighbour, H.; Boulet, L.P.; Lemiere, C.; Sehmi, R.; Leigh, R.; Sousa, A.R.; Martin, J.; Dallow, N.; Gilbert, J.; Allen, A.; et al. Safety and efficacy of an oral CCR3 antagonist in patients with asthma and eosinophilic bronchitis: A randomized, placebo-controlled clinical trial. Clin. Exp. Allergy 2014, 44, 508–516. [Google Scholar] [CrossRef]
- Southworth, T.; Van Geest, M.; Singh, D. Type-2 airway inflammation in mild asthma patients with high blood eosinophils and high fractional exhaled nitric oxide. Clin. Transl. Sci. 2021, 14, 1259–1264. [Google Scholar] [CrossRef]
- Nagase, H.; Ueki, S.; Fujieda, S. The roles of IL-5 and anti-IL-5 treatment in eosinophilic diseases: Asthma, eosinophilic granulomatosis with polyangiitis, and eosinophilic chronic rhinosinusitis. Allergol. Int. 2020, 69, 178–186. [Google Scholar] [CrossRef]
- Walsh, G.M. Anti-IL-5 monoclonal antibodies for the treatment of asthma: An update. Expert Opin. Biol. Ther. 2020, 20, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, P.G.; Modrek, B.; Choy, D.F.; Jia, G.; Abbas, A.R.; Ellwanger, A.; Koth, L.L.; Arron, J.R.; Fahy, J.V. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am. J. Respir. Crit. Care Med. 2009, 180, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Humeniuk, P.; Dubiela, P.; Hoffmann-Sommergruber, K. Dendritic Cells and Their Role in Allergy: Uptake, Proteolytic Processing and Presentation of Allergens. Int. J. Mol. Sci. 2017, 18, 1491. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.A.; Barlow, J.L.; McKenzie, A.N. Innate lymphoid cells--how did we miss them? Nat. Rev. Immunol. 2013, 13, 75–87. [Google Scholar] [CrossRef]
- Wenzel, S.; Ford, L.; Pearlman, D.; Spector, S.; Sher, L.; Skobieranda, F.; Wang, L.; Kirkesseli, S.; Rocklin, R.; Bock, B.; et al. Dupilumab in persistent asthma with elevated eosinophil levels. N. Engl. J. Med. 2013, 368, 2455–2466. [Google Scholar] [CrossRef]
- Bel, E.H.; Ten Brinke, A. New Anti-Eosinophil Drugs for Asthma and COPD: Targeting the Trait! Chest 2017, 152, 1276–1282. [Google Scholar] [CrossRef]
- Pavlidis, S.; Takahashi, K.; Ng Kee Kwong, F.; Xie, J.; Hoda, U.; Sun, K.; Elyasigomari, V.; Agapow, P.; Loza, M.; Baribaud, F.; et al. “T2-high” in severe asthma related to blood eosinophil, exhaled nitric oxide and serum periostin. Eur. Respir. J. 2019, 53. [Google Scholar] [CrossRef]
- Frossing, L.; Silberbrandt, A.; Von Bulow, A.; Backer, V.; Porsbjerg, C. The Prevalence of Subtypes of Type 2 Inflammation in an Unselected Population of Patients with Severe Asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 1267–1275. [Google Scholar] [CrossRef]
- Pelaia, C.; Paoletti, G.; Puggioni, F.; Racca, F.; Pelaia, G.; Canonica, G.W.; Heffler, E. Interleukin-5 in the Pathophysiology of Severe Asthma. Front. Physiol. 2019, 10, 1514. [Google Scholar] [CrossRef]
- Racca, F.; Pellegatta, G.; Cataldo, G.; Vespa, E.; Carlani, E.; Pelaia, C.; Paoletti, G.; Messina, M.R.; Nappi, E.; Canonica, G.W.; et al. Type 2 Inflammation in Eosinophilic Esophagitis: From Pathophysiology to Therapeutic Targets. Front. Physiol. 2021, 12, 815842. [Google Scholar] [CrossRef]
- Blanchard, C.; Simon, D.; Schoepfer, A.; Straumann, A.; Simon, H.U. Eosinophilic esophagitis: Unclear roles of IgE and eosinophils. J. Intern. Med. 2017, 281, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, A.M.; Chipps, B.E.; Holguin, F.; Woodruff, P.G. T2-”Low” Asthma: Overview and Management Strategies. J. Allergy Clin. Immunol. Pract. 2020, 8, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.; Humbert, M.; Buhl, R.; Cruz, A.A.; Inoue, H.; Korom, S.; Hanania, N.A.; Nair, P. Revisiting Type 2-high and Type 2-low airway inflammation in asthma: Current knowledge and therapeutic implications. Clin. Exp. Allergy 2017, 47, 161–175. [Google Scholar] [CrossRef] [PubMed]
- McKinley, L.; Alcorn, J.F.; Peterson, A.; Dupont, R.B.; Kapadia, S.; Logar, A.; Henry, A.; Irvin, C.G.; Piganelli, J.D.; Ray, A.; et al. TH17 cells mediate steroid-resistant airway inflammation and airway hyperresponsiveness in mice. J. Immunol. 2008, 181, 4089–4097. [Google Scholar] [CrossRef] [PubMed]
- Margelidon-Cozzolino, V.; Tsicopoulos, A.; Chenivesse, C.; de Nadai, P. Role of Th17 Cytokines in Airway Remodeling in Asthma and Therapy Perspectives. Front. Allergy 2022, 3, 806391. [Google Scholar] [CrossRef]
- Bhakta, N.R.; Woodruff, P.G. Human asthma phenotypes: From the clinic, to cytokines, and back again. Immunol. Rev. 2011, 242, 220–232. [Google Scholar] [CrossRef]
- Busse, W.W.; Holgate, S.; Kerwin, E.; Chon, Y.; Feng, J.; Lin, J.; Lin, S.L. Randomized, double-blind, placebo-controlled study of brodalumab, a human anti-IL-17 receptor monoclonal antibody, in moderate to severe asthma. Am. J. Respir. Crit. Care Med. 2013, 188, 1294–1302. [Google Scholar] [CrossRef]
- Fahy, J.V. Eosinophilic and neutrophilic inflammation in asthma: Insights from clinical studies. Proc. Am. Thorac. Soc. 2009, 6, 256–259. [Google Scholar] [CrossRef]
- D’Silva, L.; Cook, R.J.; Allen, C.J.; Hargreave, F.E.; Parameswaran, K. Changing pattern of sputum cell counts during successive exacerbations of airway disease. Respir. Med. 2007, 101, 2217–2220. [Google Scholar] [CrossRef]
- Cosmi, L.; Maggi, L.; Santarlasci, V.; Capone, M.; Cardilicchia, E.; Frosali, F.; Querci, V.; Angeli, R.; Matucci, A.; Fambrini, M.; et al. Identification of a novel subset of human circulating memory CD4(+) T cells that produce both IL-17A and IL-4. J. Allergy Clin. Immunol. 2010, 125, 222–230.e1-4. [Google Scholar] [CrossRef]
- Di Spigna, G.; Ladogana, P.; Covelli, B.; Ricciardone, M.; Salzano, S.; Spalletti Cernia, D.; Mormile, I.; Varriale, G.; Catapano, O.; Spadaro, G.; et al. Component resolved diagnosis by recombinant allergens in patients with allergies to inhalants. J. Biol. Regul. Homeost Agents 2020, 34, 1729–1737. [Google Scholar] [PubMed]
- Chung, L.P.; Upham, J.W.; Bardin, P.G.; Hew, M. Rational oral corticosteroid use in adult severe asthma: A narrative review. Respirology 2020, 25, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Laidlaw, T.M.; Mullol, J.; Woessner, K.M.; Amin, N.; Mannent, L.P. Chronic Rhinosinusitis with Nasal Polyps and Asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Bakakos, A.; Loukides, S.; Bakakos, P. Severe Eosinophilic Asthma. J. Clin. Med. 2019, 8, 1375. [Google Scholar] [CrossRef]
- Lefaudeux, D.; De Meulder, B.; Loza, M.J.; Peffer, N.; Rowe, A.; Baribaud, F.; Bansal, A.T.; Lutter, R.; Sousa, A.R.; Corfield, J.; et al. U-BIOPRED clinical adult asthma clusters linked to a subset of sputum omics. J. Allergy Clin. Immunol. 2017, 139, 1797–1807. [Google Scholar] [CrossRef]
- McKenzie, A.N. Type-2 innate lymphoid cells in asthma and allergy. Ann. Am. Thorac. Soc. 2014, 11 (Suppl. S5), S263–S270. [Google Scholar] [CrossRef]
- Jackson, D.J.; Humbert, M.; Hirsch, I.; Newbold, P.; Garcia Gil, E. Ability of Serum IgE Concentration to Predict Exacerbation Risk and Benralizumab Efficacy for Patients with Severe Eosinophilic Asthma. Adv. Ther. 2020, 37, 718–729. [Google Scholar] [CrossRef]
- Pelaia, C.; Crimi, C.; Benfante, A.; Caiaffa, M.F.; Calabrese, C.; Carpagnano, G.E.; Ciotta, D.; D’Amato, M.; Macchia, L.; Nolasco, S.; et al. Therapeutic Effects of Benralizumab Assessed in Patients with Severe Eosinophilic Asthma: Real-Life Evaluation Correlated with Allergic and Non-Allergic Phenotype Expression. J. Asthma Allergy 2021, 14, 163–173. [Google Scholar] [CrossRef]
- Spergel, J.M.; Andrews, T.; Brown-Whitehorn, T.F.; Beausoleil, J.L.; Liacouras, C.A. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Ann. Allergy Asthma Immunol. 2005, 95, 336–343. [Google Scholar] [CrossRef]
- Medrek, S.K.; Parulekar, A.D.; Hanania, N.A. Predictive Biomarkers for Asthma Therapy. Curr. Allergy Asthma Rep. 2017, 17, 69. [Google Scholar] [CrossRef]
- Van Hulst, G.; Bureau, F.; Desmet, C.J. Eosinophils as Drivers of Severe Eosinophilic Asthma: Endotypes or Plasticity? Int. J. Mol. Sci. 2021, 22, 10150. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, J.; Hoyte, F.C.L.; Phipatanakul, W.; Silver, J.; Howarth, P.; Lugogo, N.L. Allergic and eosinophilic asthma in the era of biomarkers and biologics: Similarities, differences and misconceptions. Ann. Allergy Asthma Immunol. 2022, 129, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Woolnough, K.; Wardlaw, A.J. Eosinophilia in Pulmonary Disorders. Immunol. Allergy Clin. North. Am. 2015, 35, 477–492. [Google Scholar] [CrossRef] [PubMed]
- Loewenthal, L.; Menzies-Gow, A. FeNO in Asthma. Semin Respir Crit. Care Med. 2022, 43, 635–645. [Google Scholar] [CrossRef]
- Kavanagh, J.E.; Hearn, A.P.; Jackson, D.J. A pragmatic guide to choosing biologic therapies in severe asthma. Breathe 2021, 17, 210144. [Google Scholar] [CrossRef]
- Sonnenberg-Riethmacher, E.; Miehe, M.; Riethmacher, D. Periostin in Allergy and Inflammation. Front. Immunol. 2021, 12, 722170. [Google Scholar] [CrossRef]
- Matsumoto, H. Role of serum periostin in the management of asthma and its comorbidities. Respir. Investig. 2020, 58, 144–154. [Google Scholar] [CrossRef]
- Milger, K.; Gotschke, J.; Krause, L.; Nathan, P.; Alessandrini, F.; Tufman, A.; Fischer, R.; Bartel, S.; Theis, F.J.; Behr, J.; et al. Identification of a plasma miRNA biomarker signature for allergic asthma: A translational approach. Allergy 2017, 72, 1962–1971. [Google Scholar] [CrossRef]
- Specjalski, K.; Niedoszytko, M. MicroRNAs: Future biomarkers and targets of therapy in asthma? Curr. Opin. Pulm. Med. 2020, 26, 285–292. [Google Scholar] [CrossRef]
- Adatia, A.; Vliagoftis, H. Challenges in severe asthma: Do we need new drugs or new biomarkers? Front. Med. 2022, 9, 921967. [Google Scholar] [CrossRef]
- Nakamura, Y.; Sugano, A.; Ohta, M.; Takaoka, Y. Docking analysis and the possibility of prediction efficacy for an anti-IL-13 biopharmaceutical treatment with tralokinumab and lebrikizumab for bronchial asthma. PLoS ONE 2017, 12, e0188407. [Google Scholar] [CrossRef] [PubMed]
- Pelaia, C.; Crimi, C.; Vatrella, A.; Tinello, C.; Terracciano, R.; Pelaia, G. Molecular Targets for Biological Therapies of Severe Asthma. Front. Immunol. 2020, 11, 603312. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Adcock, I.M. Precision medicine for the discovery of treatable mechanisms in severe asthma. Allergy 2019, 74, 1649–1659. [Google Scholar] [CrossRef] [PubMed]
- Jevnikar, Z.; Ostling, J.; Ax, E.; Calven, J.; Thorn, K.; Israelsson, E.; Oberg, L.; Singhania, A.; Lau, L.C.K.; Wilson, S.J.; et al. Unbiased Biomarkers in Prediction of Respiratory Disease Outcomes study, g., Epithelial IL-6 trans-signaling defines a new asthma phenotype with increased airway inflammation. J. Allergy Clin. Immunol. 2019, 143, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Santus, P.; Saad, M.; Damiani, G.; Patella, V.; Radovanovic, D. Current and future targeted therapies for severe asthma: Managing treatment with biologics based on phenotypes and biomarkers. Pharmacol. Res. 2019, 146, 104296. [Google Scholar] [CrossRef]
- Meyer, N.; Dallinga, J.W.; Nuss, S.J.; Moonen, E.J.; van Berkel, J.J.; Akdis, C.; van Schooten, F.J.; Menz, G. Defining adult asthma endotypes by clinical features and patterns of volatile organic compounds in exhaled air. Respir Res. 2014, 15, 136. [Google Scholar] [CrossRef]
- Brinkman, P.; Zee, A.M.; Wagener, A.H. Breathomics and treatable traits for chronic airway diseases. Curr. Opin. Pulm. Med. 2019, 25, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Fouka, E.; Domvri, K.; Gkakou, F.; Alevizaki, M.; Steiropoulos, P.; Papakosta, D.; Porpodis, K. Recent insights in the role of biomarkers in severe asthma management. Front. Med. 2022, 9, 992565. [Google Scholar] [CrossRef]
- Lugogo, N.; Domingo, C.; Chanez, P.; Leigh, R.; Gilson, M.J.; Price, R.G.; Yancey, S.W.; Ortega, H.G. Long-term Efficacy and Safety of Mepolizumab in Patients With Severe Eosinophilic Asthma: A Multi-center, Open-label, Phase IIIb Study. Clin. Ther. 2016, 38, 2058–2070.e1. [Google Scholar] [CrossRef]
- Pavord, I.D.; Afzalnia, S.; Menzies-Gow, A.; Heaney, L.G. The current and future role of biomarkers in type 2 cytokine-mediated asthma management. Clin. Exp. Allergy 2017, 47, 148–160. [Google Scholar] [CrossRef]
- Bleecker, E.R.; FitzGerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkstrom, V.; et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting beta(2)-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, J.M.; Bleecker, E.R.; Nair, P.; Korn, S.; Ohta, K.; Lommatzsch, M.; Ferguson, G.T.; Busse, W.W.; Barker, P.; Sproule, S.; et al. Benralizumab, an anti-interleukin-5 receptor alpha monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2016, 388, 2128–2141. [Google Scholar] [CrossRef] [PubMed]
- Amaral, R.; Jacinto, T.; Malinovschi, A.; Janson, C.; Price, D.; Fonseca, J.A.; Alving, K. The influence of individual characteristics and non-respiratory diseases on blood eosinophil count. Clin. Transl. Allergy 2021, 11, e12036. [Google Scholar] [CrossRef] [PubMed]
- Narendra, D.; Blixt, J.; Hanania, N.A. Immunological biomarkers in severe asthma. Semin. Immunol. 2019, 46, 101332. [Google Scholar] [CrossRef]
- Mauer, Y.; Taliercio, R.M. Managing adult asthma: The 2019 GINA guidelines. Cleve. Clin. J. Med. 2020, 87, 569–575. [Google Scholar] [CrossRef]
- Heaney, L.G.; Perez de Llano, L.; Al-Ahmad, M.; Backer, V.; Busby, J.; Canonica, G.W.; Christoff, G.C.; Cosio, B.G.; FitzGerald, J.M.; Heffler, E.; et al. Eosinophilic and Noneosinophilic Asthma: An Expert Consensus Framework to Characterize Phenotypes in a Global Real-Life Severe Asthma Cohort. Chest 2021, 160, 814–830. [Google Scholar] [CrossRef]
- Harrison, T.W.; Chanez, P.; Menzella, F.; Canonica, G.W.; Louis, R.; Cosio, B.G.; Lugogo, N.L.; Mohan, A.; Burden, A.; McDermott, L.; et al. Onset of effect and impact on health-related quality of life, exacerbation rate, lung function, and nasal polyposis symptoms for patients with severe eosinophilic asthma treated with benralizumab (ANDHI): A randomised, controlled, phase 3b trial. Lancet Respir. Med. 2021, 9, 260–274. [Google Scholar] [CrossRef]
- Kroegel, C.; Liu, M.C.; Hubbard, W.C.; Lichtenstein, L.M.; Bochner, B.S. Blood and bronchoalveolar eosinophils in allergic subjects after segmental antigen challenge: Surface phenotype, density heterogeneity, and prostanoid production. J. Allergy Clin. Immunol. 1994, 93, 725–734. [Google Scholar] [CrossRef]
- Nelson, R.K.; Bush, A.; Stokes, J.; Nair, P.; Akuthota, P. Eosinophilic Asthma. J. Allergy Clin. Immunol. Pract. 2020, 8, 465–473. [Google Scholar] [CrossRef]
- Kostikas, K.; Brindicci, C.; Patalano, F. Blood Eosinophils as Biomarkers to Drive Treatment Choices in Asthma and COPD. Curr. Drug. Targets 2018, 19, 1882–1896. [Google Scholar] [CrossRef]
- Schleich, F.N.; Manise, M.; Sele, J.; Henket, M.; Seidel, L.; Louis, R. Distribution of sputum cellular phenotype in a large asthma cohort: Predicting factors for eosinophilic vs neutrophilic inflammation. BMC Pulm. Med. 2013, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Maniscalco, M.; Sofia, M.; Pelaia, G. Nitric oxide in upper airways inflammatory diseases. Inflamm. Res. 2007, 56, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Quoc, Q.L.; Park, H.S. Biomarkers for Severe Asthma: Lessons From Longitudinal Cohort Studies. Allergy Asthma Immunol. Res. 2021, 13, 375–389. [Google Scholar] [CrossRef] [PubMed]
- de Laurentiis, G.; Maniscalco, M.; Cianciulli, F.; Stanziola, A.; Marsico, S.; Lundberg, J.O.; Weitzberg, E.; Sofia, M. Exhaled nitric oxide monitoring in COPD using a portable analyzer. Pulm. Pharmacol. Ther. 2008, 21, 689–693. [Google Scholar] [CrossRef]
- Heffler, E.; Carpagnano, G.E.; Favero, E.; Guida, G.; Maniscalco, M.; Motta, A.; Paoletti, G.; Rolla, G.; Baraldi, E.; Pezzella, V.; et al. Fractional Exhaled Nitric Oxide (FENO) in the management of asthma: A position paper of the Italian Respiratory Society (SIP/IRS) and Italian Society of Allergy, Asthma and Clinical Immunology (SIAAIC). Multidiscip. Respir. Med. 2020, 15, 36. [Google Scholar] [CrossRef]
- Diamant, Z.; Vijverberg, S.; Alving, K.; Bakirtas, A.; Bjermer, L.; Custovic, A.; Dahlen, S.E.; Gaga, M.; Gerth van Wijk, R.; Giacco, S.D.; et al. Toward clinically applicable biomarkers for asthma: An EAACI position paper. Allergy 2019, 74, 1835–1851. [Google Scholar] [CrossRef]
- Pavord, I.D.; Deniz, Y.; Corren, J.; Casale, T.B.; FitzGerald, J.M.; Izuhara, K.; Daizadeh, N.; Ortiz, B.; Johnson, R.R.; Harel, S.; et al. Baseline FeNO Independently Predicts the Dupilumab Response in Patients With Moderate-to-Severe Asthma. J. Allergy Clin. Immunol. Pract. 2022, 11, 1213–1220.e2. [Google Scholar] [CrossRef]
- Pavord, I.D.; Siddiqui, S.; Papi, A.; Corren, J.; Sher, L.D.; Bardin, P.; Langton, D.; Park, H.S.; Rice, M.S.; Deniz, Y.; et al. Dupilumab Efficacy in Patients Stratified by Baseline Treatment Intensity and Lung Function. J. Asthma Allergy 2020, 13, 701–711. [Google Scholar] [CrossRef]
- Haldar, P.; Brightling, C.E.; Hargadon, B.; Gupta, S.; Monteiro, W.; Sousa, A.; Marshall, R.P.; Bradding, P.; Green, R.H.; Wardlaw, A.J.; et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N. Engl. J. Med. 2009, 360, 973–984. [Google Scholar] [CrossRef]
- George, L.; Brightling, C.E. Eosinophilic airway inflammation: Role in asthma and chronic obstructive pulmonary disease. Ther Adv. Chronic Dis. 2016, 7, 34–51. [Google Scholar] [CrossRef]
- Fleming, L.; Tsartsali, L.; Wilson, N.; Regamey, N.; Bush, A. Longitudinal relationship between sputum eosinophils and exhaled nitric oxide in children with asthma. Am. J. Respir. Crit. Care Med. 2013, 188, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.; Raza, A.; Karmaus, W.; Mitchell, F.; Grundy, J.; Kurukulaaratchy, R.J.; Arshad, S.H.; Roberts, G. Influence of atopy and asthma on exhaled nitric oxide in an unselected birth cohort study. Thorax 2010, 65, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Wagener, A.H.; de Nijs, S.B.; Lutter, R.; Sousa, A.R.; Weersink, E.J.; Bel, E.H.; Sterk, P.J. External validation of blood eosinophils, FE(NO) and serum periostin as surrogates for sputum eosinophils in asthma. Thorax 2015, 70, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Corren, J.; Pham, T.H.; Garcia Gil, E.; Salapa, K.; Ren, P.; Parnes, J.R.; Colice, G.; Griffiths, J.M. Baseline type 2 biomarker levels and response to tezepelumab in severe asthma. Allergy 2022, 77, 1786–1796. [Google Scholar] [CrossRef]
- Bersuch, E.; Graf, F.; Renner, E.D.; Jung, A.; Traidl-Hoffmann, C.; Lauener, R.; Roduit, C. Lung function improvement and airways inflammation reduction in asthmatic children after a rehabilitation program at moderate altitude. Pediatr Allergy Immunol. 2017, 28, 768–775. [Google Scholar] [CrossRef] [PubMed]
- Clini, E.; Bianchi, L.; Foglio, K.; Porta, R.; Vitacca, M.; Ambrosino, N. Effect of pulmonary rehabilitation on exhaled nitric oxide in patients with chronic obstructive pulmonary disease. Thorax 2001, 56, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Habib, N.; Pasha, M.A.; Tang, D.D. Current Understanding of Asthma Pathogenesis and Biomarkers. Cells 2022, 11, 2764. [Google Scholar] [CrossRef]
- Hoshino, M.; Ohtawa, J.; Akitsu, K. Effect of treatment with inhaled corticosteroid on serum periostin levels in asthma. Respirology 2016, 21, 297–303. [Google Scholar] [CrossRef]
- Hamilton, J.D.; Harel, S.; Swanson, B.N.; Brian, W.; Chen, Z.; Rice, M.S.; Amin, N.; Ardeleanu, M.; Radin, A.; Shumel, B.; et al. Dupilumab suppresses type 2 inflammatory biomarkers across multiple atopic, allergic diseases. Clin. Exp. Allergy 2021, 51, 915–931. [Google Scholar] [CrossRef]
- Castro, M.; Corren, J.; Pavord, I.D.; Maspero, J.; Wenzel, S.; Rabe, K.F.; Busse, W.W.; Ford, L.; Sher, L.; FitzGerald, J.M.; et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N. Engl. J. Med. 2018, 378, 2486–2496. [Google Scholar] [CrossRef]
- Hanania, N.A.; Korenblat, P.; Chapman, K.R.; Bateman, E.D.; Kopecky, P.; Paggiaro, P.; Yokoyama, A.; Olsson, J.; Gray, S.; Holweg, C.T.; et al. Efficacy and safety of lebrikizumab in patients with uncontrolled asthma (LAVOLTA I and LAVOLTA II): Replicate, phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir. Med. 2016, 4, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Kudo, A. Clinical Applications Targeting Periostin. Adv. Exp. Med. Biol. 2019, 1132, 207–210. [Google Scholar] [PubMed]
- Mukherjee, M.; Sehmi, R.; Nair, P. Anti-IL5 therapy for asthma and beyond. World Allergy Organ. J. 2014, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Malinovschi, A.; Fonseca, J.A.; Jacinto, T.; Alving, K.; Janson, C. Exhaled nitric oxide levels and blood eosinophil counts independently associate with wheeze and asthma events in National Health and Nutrition Examination Survey subjects. J. Allergy Clin. Immunol. 2013, 132, 821–827.e1-5. [Google Scholar] [CrossRef] [PubMed]
- Kanda, A.; Kobayashi, Y.; Asako, M.; Tomoda, K.; Kawauchi, H.; Iwai, H. Regulation of Interaction between the Upper and Lower Airways in United Airway Disease. Med. Sci. 2019, 7, 27. [Google Scholar] [CrossRef]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef]
- John Staniorski, C.; Price, C.P.E.; Weibman, A.R.; Welch, K.C.; Conley, D.B.; Shintani-Smith, S.; Stevens, W.W.; Peters, A.T.; Grammer, L.; Lidder, A.K.; et al. Asthma onset pattern and patient outcomes in a chronic rhinosinusitis population. Int. Forum. Allergy Rhinol. 2018, 8, 495–503. [Google Scholar] [CrossRef]
- Licona-Limon, P.; Kim, L.K.; Palm, N.W.; Flavell, R.A. TH2, allergy and group 2 innate lymphoid cells. Nat. Immunol. 2013, 14, 536–542. [Google Scholar] [CrossRef]
- Toppila-Salmi, S.; van Drunen, C.M.; Fokkens, W.J.; Golebski, K.; Mattila, P.; Joenvaara, S.; Renkonen, J.; Renkonen, R. Molecular mechanisms of nasal epithelium in rhinitis and rhinosinusitis. Curr. Allergy Asthma Rep. 2015, 15, 495. [Google Scholar] [CrossRef]
- Van Zele, T.; Claeys, S.; Gevaert, P.; Van Maele, G.; Holtappels, G.; Van Cauwenberge, P.; Bachert, C. Differentiation of chronic sinus diseases by measurement of inflammatory mediators. Allergy 2006, 61, 1280–1289. [Google Scholar] [CrossRef]
- Van Bruaene, N.; Perez-Novo, C.A.; Basinski, T.M.; Van Zele, T.; Holtappels, G.; De Ruyck, N.; Schmidt-Weber, C.; Akdis, C.; Van Cauwenberge, P.; Bachert, C.; et al. T-cell regulation in chronic paranasal sinus disease. J. Allergy Clin. Immunol. 2008, 121, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.O.; Arebro, J.; Olze, H.; Forster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziaber, A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immunol. 2016, 137, 1449–1456. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, T.; Yoshikawa, M.; Asaka, D.; Okushi, T.; Matsuwaki, Y.; Otori, N.; Hama, T.; Moriyama, H. Mucosal eosinophilia and recurrence of nasal polyps—new classification of chronic rhinosinusitis. Rhinology 2011, 49, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, T.; Sakashita, M.; Haruna, T.; Asaka, D.; Takeno, S.; Ikeda, H.; Nakayama, T.; Seki, N.; Ito, S.; Murata, J.; et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: The JESREC Study. Allergy 2015, 70, 995–1003. [Google Scholar] [CrossRef]
- Mehta, V.; Campeau, N.G.; Kita, H.; Hagan, J.B. Blood and sputum eosinophil levels in asthma and their relationship to sinus computed tomographic findings. Mayo Clin. Proc. 2008, 83, 671–678. [Google Scholar] [CrossRef]
- Wenzel, S.E. Severe Adult Asthmas: Integrating Clinical Features, Biology, and Therapeutics to Improve Outcomes. Am. J. Respir. Crit. Care Med. 2021, 203, 809–821. [Google Scholar] [CrossRef]
- Bochner, B.S.; Stevens, W.W. Biology and Function of Eosinophils in Chronic Rhinosinusitis With or Without Nasal Polyps. Allergy Asthma Immunol. Res. 2021, 13, 8–22. [Google Scholar] [CrossRef]
- Matucci, A.; Bormioli, S.; Nencini, F.; Chiccoli, F.; Vivarelli, E.; Maggi, E.; Vultaggio, A. Asthma and Chronic Rhinosinusitis: How Similar Are They in Pathogenesis and Treatment Responses? Int. J. Mol. Sci. 2021, 22, 3340. [Google Scholar] [CrossRef]
- Porsbjerg, C.; Menzies-Gow, A. Co-morbidities in severe asthma: Clinical impact and management. Respirology 2017, 22, 651–661. [Google Scholar] [CrossRef]
- Mormile, M.M.I.; Palladino, F.; Molino, A.; Ruggiero, S.; Telesca, D.A.; Cappello, C.; Sivero, L. Gastro-esophageal reflux disease influence on asthma symptoms: Assessment of non-responder to the standard treatment. Minerva Pneumol. 2015, 54, 157–159. [Google Scholar]
- Paoletti, G.; Melone, G.; Ferri, S.; Puggioni, F.; Baiardini, I.; Racca, F.; Canonica, G.W.; Heffler, E.; Malipiero, G. Gastroesophageal reflux and asthma: When, how, and why. Curr. Opin. Allergy Clin. Immunol. 2021, 21, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Haldar, P.; Pavord, I.D.; Shaw, D.E.; Berry, M.A.; Thomas, M.; Brightling, C.E.; Wardlaw, A.J.; Green, R.H. Cluster analysis and clinical asthma phenotypes. Am. J. Respir. Crit. Care Med. 2008, 178, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Desai, D.; Newby, C.; Symon, F.A.; Haldar, P.; Shah, S.; Gupta, S.; Bafadhel, M.; Singapuri, A.; Siddiqui, S.; Woods, J.; et al. Elevated sputum interleukin-5 and submucosal eosinophilia in obese individuals with severe asthma. Am. J. Respir. Crit. Care Med. 2013, 188, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Moore, W.C.; Meyers, D.A.; Wenzel, S.E.; Teague, W.G.; Li, H.; Li, X.; D’Agostino, R. Jr.; Castro, M.; Curran-Everett, D.; Fitzpatrick, A.M.; et al. Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program. Am. J. Respir. Crit. Care Med. 2010, 181, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Elswood, T.R.; Turner, C.; Hornsby, J. Idiopathic chronic eosinophilic pneumonia: A differential diagnosis of lower respiratory tract infection. BMJ Case Rep. 2022, 15, e244458. [Google Scholar] [CrossRef] [PubMed]
- Mormile, I.; Mormile, M.; Rossi, F.W.; Williams, M.; Valente, T.; Candia, C.; Granata, F.; Rega, R.; Orlandi, M.; Matucci-Cerinic, M.; et al. Radiological patterns and pulmonary function values of lung involvement in primary Sjogren’s syndrome: A pilot analysis. Front. Med. 2022, 9, 998028. [Google Scholar] [CrossRef]
- Romano, R.; Borrelli, M.; Cirillo, E.; Giardino, G.; Spadaro, G.; Crescenzi, L.; Mormile, I.; Venditto, L.; Pignata, C.; Santamaria, F. Respiratory Manifestations in Primary Immunodeficiencies: Findings From a Pediatric and Adult Cohort. Arch. Bronconeumol. 2021, 57, 712–714. [Google Scholar] [CrossRef]
- Detoraki, A.; Tremante, E.; Poto, R.; Morelli, E.; Quaremba, G.; Granata, F.; Romano, A.; Mormile, I.; Rossi, F.W.; de Paulis, A.; et al. Real-life evidence of low-dose mepolizumab efficacy in EGPA: A case series. Respir. Res. 2021, 22, 185. [Google Scholar] [CrossRef]
- Mormile, I.; Petraroli, A.; Loffredo, S.; Rossi, F.W.; Mormile, M.; Del Mastro, A.; Spadaro, G.; de Paulis, A.; Bova, M. Episodic Angioedema with Hypereosinophilia (Gleich’s Syndrome): A Case Report and Extensive Review of the Literature. J. Clin. Med. 2021, 10, 1442. [Google Scholar] [CrossRef]
- ATS statement--Snowbird workshop on standardization of spirometry. Am. Rev. Respir. Dis. 1979, 119, 831–838.
- Rausch Osthoff, A.K.; Beyer, S.; Gisi, D.; Rezek, S.; Schwank, A.; Meichtry, A.; Sievi, N.A.; Hess, T.; Wirz, M. Effect of counselling during pulmonary rehabilitation on self-determined motivation to be physically active for people with chronic obstructive pulmonary disease: A pragmatic RCT. BMC Pulm. Med. 2021, 21, 317. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zhang, Z.; Han, R.; Zhang, H.; Deng, J.; Chai, M. Effects of exercise-based home pulmonary rehabilitation on patients with chronic obstructive pulmonary disease: An overview of systematic review. PLoS ONE 2022, 17, e0277632. [Google Scholar] [CrossRef]
- Shui, L.L.; Cai, J.J.; Zhong, X.Q.; Li, Y.L.; He, M.R.; Chen, Y.J. Chronic Obstructive Pulmonary Disease Patients With High Peripheral Blood Eosinophil Counts Have Better Predicted Improvement in 6MWD After Rehabilitation: A PRELIMINARY STUDY. J. Cardiopulm. Rehabil. Prev. 2023, 43, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Moecke, D.P.; Zhu, K.; Gill, J.; Brar, S.; Petlitsyna, P.; Kirkham, A.; Girt, M.; Chen, J.; Peters, H.; Denson-Camp, H.; et al. Safety and Efficacy of Inpatient Pulmonary Rehabilitation for Patients Hospitalized with an Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-analyses. Ann. Am. Thorac. Soc. 2023, 20, 307–319. [Google Scholar] [CrossRef]
- Aldhahir, A.M.; Alqahtani, J.S.; AlDraiwiesh, I.A.; Alghamdi, S.M.; Alsulayyim, A.S.; Alqarni, A.A.; Alhotye, M.; Alwafi, H.; Siraj, R.; Alrajeh, A.; et al. Healthcare providers’ attitudes, beliefs and barriers to pulmonary rehabilitation for patients with chronic obstructive pulmonary disease in Saudi Arabia: A cross-sectional study. BMJ Open 2022, 12, e063900. [Google Scholar] [CrossRef] [PubMed]
- Kim, V.; Rogers, T.J.; Criner, G.J. New concepts in the pathobiology of chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2008, 5, 478–485. [Google Scholar] [CrossRef]
- Brightling, C.; Greening, N. Airway inflammation in COPD: Progress to precision medicine. Eur. Respir. J. 2019, 54, 1900651. [Google Scholar] [CrossRef]
- David, B.; Bafadhel, M.; Koenderman, L.; De Soyza, A. Eosinophilic inflammation in COPD: From an inflammatory marker to a treatable trait. Thorax 2021, 76, 188–195. [Google Scholar] [CrossRef]
- Eltboli, O.; Bafadhel, M.; Hollins, F.; Wright, A.; Hargadon, B.; Kulkarni, N.; Brightling, C. COPD exacerbation severity and frequency is associated with impaired macrophage efferocytosis of eosinophils. BMC Pulm. Med. 2014, 14, 112. [Google Scholar] [CrossRef]
- Leigh, R.; Pizzichini, M.M.; Morris, M.M.; Maltais, F.; Hargreave, F.E.; Pizzichini, E. Stable COPD: Predicting benefit from high-dose inhaled corticosteroid treatment. Eur. Respir. J. 2006, 27, 964–971. [Google Scholar] [CrossRef]
- Pavord, I.D. Blood Eosinophil-directed Management of Airway Disease. The Past, Present, and Future. Am. J. Respir. Crit. Care Med. 2020, 202, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Kolsum, U.; Brightling, C.E.; Locantore, N.; Agusti, A.; Tal-Singer, R.; investigators, E. Eosinophilic inflammation in COPD: Prevalence and clinical characteristics. Eur. Respir. J. 2014, 44, 1697–1700. [Google Scholar] [CrossRef] [PubMed]
- Mormile, I.; Mormile, M.; Rea, G.; Petraroli, A.; Barbieri, V.; de Paulis, A.; Rossi, F.W. Spontaneous Pneumo-Mediastinum in a Post-COVID-19 Patient with Systemic Sclerosis. Healthcare 2022, 10, 529. [Google Scholar] [CrossRef] [PubMed]
- Lams, B.E.; Sousa, A.R.; Rees, P.J.; Lee, T.H. Subepithelial immunopathology of the large airways in smokers with and without chronic obstructive pulmonary disease. Eur. Respir. J. 2000, 15, 512–516. [Google Scholar] [CrossRef]
- Kim, V.L.; Coombs, N.A.; Staples, K.J.; Ostridge, K.K.; Williams, N.P.; Wootton, S.A.; Devaster, J.M.; Aris, E.; Clarke, S.C.; Tuck, A.C.; et al. Impact and associations of eosinophilic inflammation in COPD: Analysis of the AERIS cohort. Eur. Respir. J. 2017, 50, 1700853. [Google Scholar] [CrossRef]
- Cheng, S.L.; Lin, C.H. Effectiveness using higher inhaled corticosteroid dosage in patients with COPD by different blood eosinophilic counts. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2341–2348. [Google Scholar] [CrossRef]
- Pavord, I.D.; Lettis, S.; Anzueto, A.; Barnes, N. Blood eosinophil count and pneumonia risk in patients with chronic obstructive pulmonary disease: A patient-level meta-analysis. Lancet Respir. Med. 2016, 4, 731–741. [Google Scholar] [CrossRef]
- Henderson, I.; Caiazzo, E.; McSharry, C.; Guzik, T.J.; Maffia, P. Why do some asthma patients respond poorly to glucocorticoid therapy? Pharmacol. Res. 2020, 160, 105189. [Google Scholar] [CrossRef]
- Johansson, M.W. Eosinophil Activation Status in Separate Compartments and Association with Asthma. Front. Med. 2017, 4, 75. [Google Scholar] [CrossRef]
- Mukherjee, M.; Nair, P. Blood or sputum eosinophils to guide asthma therapy? Lancet Respir. Med. 2015, 3, 824–825. [Google Scholar] [CrossRef]
- Mesnil, C.; Raulier, S.; Paulissen, G.; Xiao, X.; Birrell, M.A.; Pirottin, D.; Janss, T.; Starkl, P.; Ramery, E.; Henket, M.; et al. Lung-resident eosinophils represent a distinct regulatory eosinophil subset. J. Clin. Investig. 2016, 126, 3279–3295. [Google Scholar] [CrossRef] [PubMed]
- Kanda, A.; Yun, Y.; Bui, D.V.; Nguyen, L.M.; Kobayashi, Y.; Suzuki, K.; Mitani, A.; Sawada, S.; Hamada, S.; Asako, M.; et al. The multiple functions and subpopulations of eosinophils in tissues under steady-state and pathological conditions. Allergol. Int. 2021, 70, 9–18. [Google Scholar] [CrossRef]
- Mukherjee, M.; Forero, D.F.; Tran, S.; Boulay, M.E.; Bertrand, M.; Bhalla, A.; Cherukat, J.; Al-Hayyan, H.; Ayoub, A.; Revill, S.D.; et al. Suboptimal treatment response to anti-IL-5 monoclonal antibodies in severe eosinophilic asthmatics with airway autoimmune phenomena. Eur. Respir. J. 2020, 56, 2000117. [Google Scholar] [CrossRef] [PubMed]
- Johnston, L.K.; Hsu, C.L.; Krier-Burris, R.A.; Chhiba, K.D.; Chien, K.B.; McKenzie, A.; Berdnikovs, S.; Bryce, P.J. IL-33 Precedes IL-5 in Regulating Eosinophil Commitment and Is Required for Eosinophil Homeostasis. J. Immunol. 2016, 197, 3445–3453. [Google Scholar] [CrossRef]
- Sehmi, R.; Smith, S.G.; Kjarsgaard, M.; Radford, K.; Boulet, L.P.; Lemiere, C.; Prazma, C.M.; Ortega, H.; Martin, J.G.; Nair, P. Role of local eosinophilopoietic processes in the development of airway eosinophilia in prednisone-dependent severe asthma. Clin. Exp. Allergy 2016, 46, 793–802. [Google Scholar] [CrossRef]
- Agache, I.; Rocha, C.; Pereira, A.; Song, Y.; Alonso-Coello, P.; Sola, I.; Beltran, J.; Posso, M.; Akdis, C.A.; Akdis, M.; et al. Efficacy and safety of treatment with omalizumab for chronic spontaneous urticaria: A systematic review for the EAACI Biologicals Guidelines. Allergy 2021, 76, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Hinks, T.S.C.; Levine, S.J.; Brusselle, G.G. Treatment options in type-2 low asthma. Eur. Respir. J. 2021, 57, 2000528. [Google Scholar] [CrossRef]
- Mormile, I.; Granata, F.; Detoraki, A.; Pacella, D.; Della Casa, F.; De Rosa, F.; Romano, A.; de Paulis, A.; Rossi, F.W. Predictive Response to Immunotherapy Score: A Useful Tool for Identifying Eligible Patients for Allergen Immunotherapy. Biomedicines 2022, 10, 971. [Google Scholar] [CrossRef]
- Gevaert, P.; Omachi, T.A.; Corren, J.; Mullol, J.; Han, J.; Lee, S.E.; Kaufman, D.; Ligueros-Saylan, M.; Howard, M.; Zhu, R.; et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J. Allergy Clin. Immunol. 2020, 146, 595–605. [Google Scholar] [CrossRef]
- Gon, Y.; Maruoka, S.; Mizumura, K. Omalizumab and IgE in the Control of Severe Allergic Asthma. Front. Pharmacol. 2022, 13, 839011. [Google Scholar] [CrossRef] [PubMed]
- Pavord, I.D.; Korn, S.; Howarth, P.; Bleecker, E.R.; Buhl, R.; Keene, O.N.; Ortega, H.; Chanez, P. Mepolizumab for severe eosinophilic asthma (DREAM): A multicentre, double-blind, placebo-controlled trial. Lancet 2012, 380, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Deeks, E.D.; Brusselle, G. Reslizumab in Eosinophilic Asthma: A Review. Drugs 2017, 77, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, J.E.; Hearn, A.P.; Dhariwal, J.; d’Ancona, G.; Douiri, A.; Roxas, C.; Fernandes, M.; Green, L.; Thomson, L.; Nanzer, A.M.; et al. Real-World Effectiveness of Benralizumab in Severe Eosinophilic Asthma. Chest 2021, 159, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Menzies-Gow, A.; Corren, J.; Bourdin, A.; Chupp, G.; Israel, E.; Wechsler, M.E.; Brightling, C.E.; Griffiths, J.M.; Hellqvist, A.; Bowen, K.; et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N. Engl. J. Med. 2021, 384, 1800–1809. [Google Scholar] [CrossRef]
- Rabe, K.F.; Celli, B.R.; Wechsler, M.E.; Abdulai, R.M.; Luo, X.; Boomsma, M.M.; Staudinger, H.; Horowitz, J.E.; Baras, A.; Ferreira, M.A.; et al. Safety and efficacy of itepekimab in patients with moderate-to-severe COPD: A genetic association study and randomised, double-blind, phase 2a trial. Lancet Respir. Med. 2021, 9, 1288–1298. [Google Scholar] [CrossRef]
- Wechsler, M.E.; Ruddy, M.K.; Pavord, I.D.; Israel, E.; Rabe, K.F.; Ford, L.B.; Maspero, J.F.; Abdulai, R.M.; Hu, C.C.; Martincova, R.; et al. Efficacy and Safety of Itepekimab in Patients with Moderate-to-Severe Asthma. N. Engl. J. Med. 2021, 385, 1656–1668. [Google Scholar] [CrossRef]
- Kosloski, M.P.; Kalliolias, G.D.; Xu, C.R.; Harel, S.; Lai, C.H.; Zheng, W.; Davis, J.D.; Kamal, M.A. Pharmacokinetics and pharmacodynamics of itepekimab in healthy adults and patients with asthma: Phase I first-in-human and first-in-patient trials. Clin. Transl. Sci. 2022, 15, 384–395. [Google Scholar] [CrossRef]
- Akar-Ghibril, N.; Casale, T.; Custovic, A.; Phipatanakul, W. Allergic Endotypes and Phenotypes of Asthma. J. Allergy Clin. Immunol. Pract. 2020, 8, 429–440. [Google Scholar] [CrossRef]
- Han, J.K.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.E.; Smith, S.G.; Martin, N.; Mayer, B.; Yancey, S.W.; et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 1141–1153. [Google Scholar] [CrossRef]
- Detoraki, A.; Tremante, E.; D’Amato, M.; Calabrese, C.; Casella, C.; Maniscalco, M.; Poto, R.; Brancaccio, R.; Boccia, M.; Martino, M.; et al. Mepolizumab improves sino-nasal symptoms and asthma control in severe eosinophilic asthma patients with chronic rhinosinusitis and nasal polyps: A 12-month real-life study. Ther Adv. Respir Dis 2021, 15, 17534666211009398. [Google Scholar] [CrossRef]
- Walter, S.; Ho, J.; Alvarado, R.; Smith, G.; Croucher, D.R.; Liang, S.; Grayson, J.W.; Mangussi-Gomes, J.; Van Es, S.L.; Earls, P.; et al. Mepolizumab decreases tissue eosinophils while increasing type-2 cytokines in eosinophilic chronic rhinosinusitis. Clin. Exp. Allergy 2022, 52, 1403–1413. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Han, J.K.; Desrosiers, M.Y.; Gevaert, P.; Heffler, E.; Hopkins, C.; Tversky, J.R.; Barker, P.; Cohen, D.; Emson, C.; et al. Efficacy and safety of benralizumab in chronic rhinosinusitis with nasal polyps: A randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2022, 149, 1309–1317.e12. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, A.; Kjarsgaard, M.; Capaldi, D.; Radford, K.; Aleman, F.; Boylan, C.; Altman, L.C.; Wight, T.N.; Parraga, G.; O’Byrne, P.M.; et al. A pilot randomised clinical trial of mepolizumab in COPD with eosinophilic bronchitis. Eur. Respir. J. 2017, 49, 1602486. [Google Scholar] [CrossRef]
- Pavord, I.D.; Chanez, P.; Criner, G.J.; Kerstjens, H.A.M.; Korn, S.; Lugogo, N.; Martinot, J.B.; Sagara, H.; Albers, F.C.; Bradford, E.S.; et al. Mepolizumab for Eosinophilic Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2017, 377, 1613–1629. [Google Scholar] [CrossRef]
- Brightling, C.E.; Bleecker, E.R.; Panettieri, R.A., Jr.; Bafadhel, M.; She, D.; Ward, C.K.; Xu, X.; Birrell, C.; van der Merwe, R. Benralizumab for chronic obstructive pulmonary disease and sputum eosinophilia: A randomised, double-blind, placebo-controlled, phase 2a study. Lancet Respir. Med. 2014, 2, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Criner, G.J.; Celli, B.R.; Brightling, C.E.; Agusti, A.; Papi, A.; Singh, D.; Sin, D.D.; Vogelmeier, C.F.; Sciurba, F.C.; Bafadhel, M.; et al. Benralizumab for the Prevention of COPD Exacerbations. N. Engl. J. Med. 2019, 381, 1023–1034. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).