

Ozone as Redox Bioregulator in Preventive Medicine: The Molecular and Pharmacological Basis of the Low-Dose Ozone Concept—A Review

Abstract
:1. Introduction
1.1. Prevention through Room and Surface Disinfection
1.2. From Empirical Findings to Science
2. Preclinical Trials in Animal and Cell Models
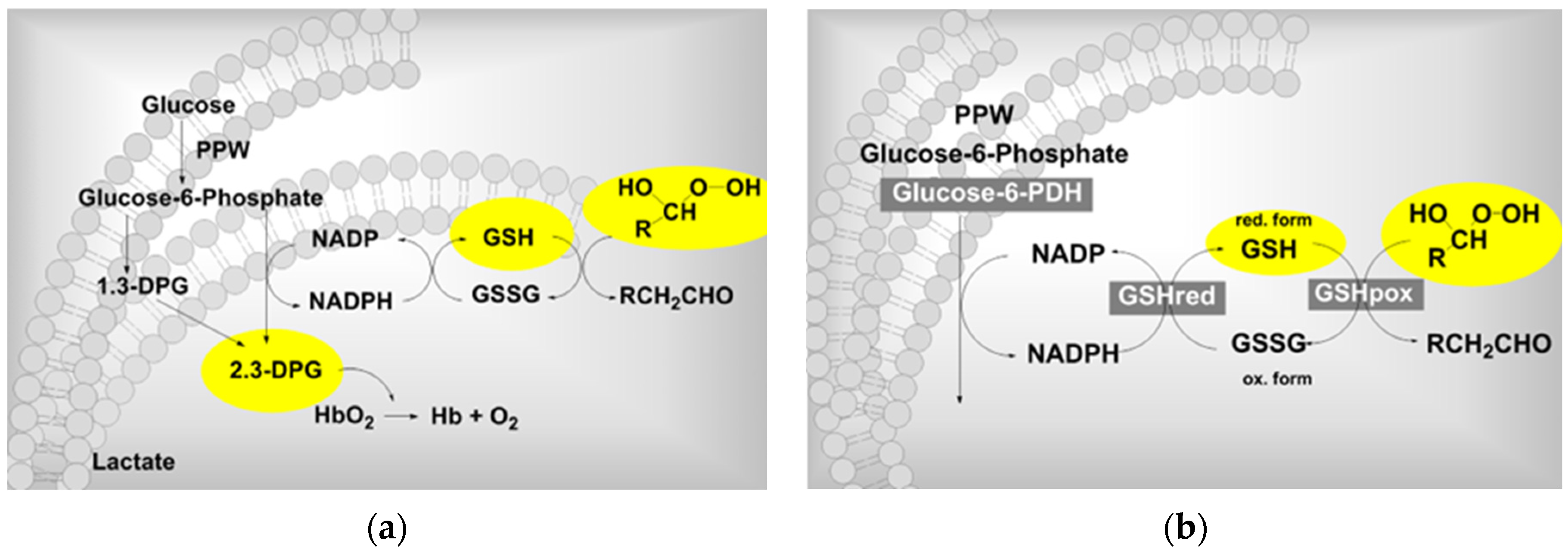
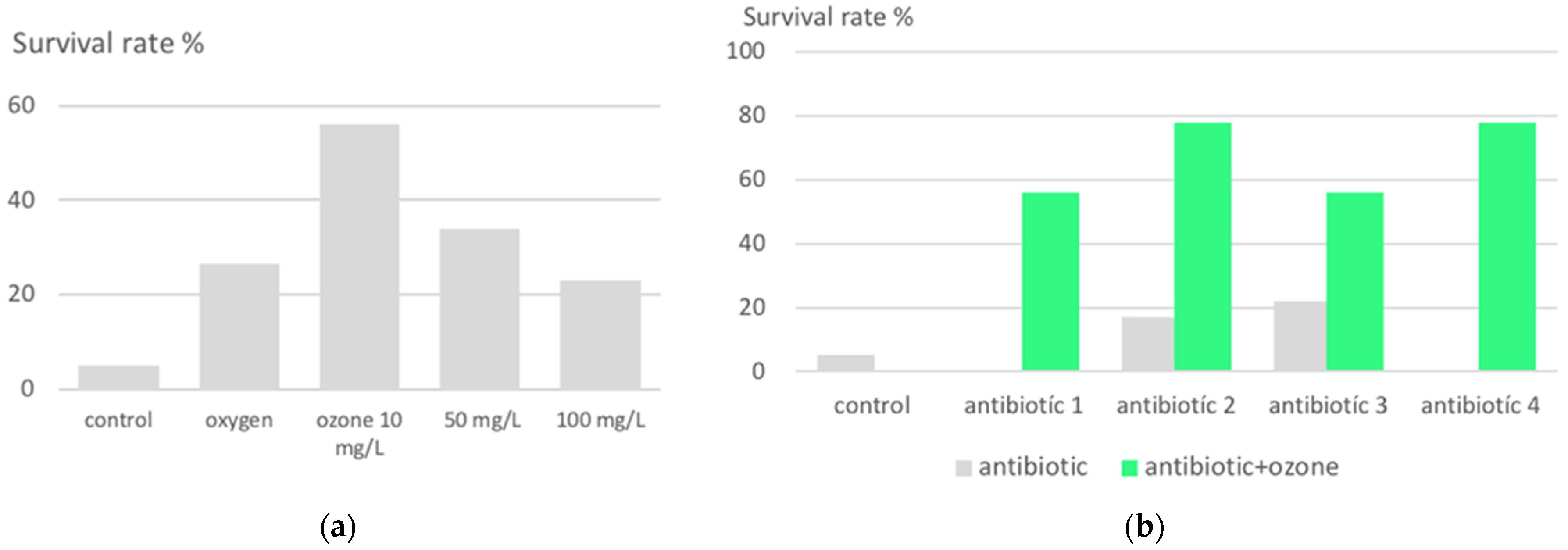
2.1. Growth Inhibition of Plasmodium Falciparum in Ozone-Pretreated Red Blood Cells (RBC)
2.2. Protection against Lethal Peritonitis by Oxidative Preconditioning with Ozone in Animal Models
3. Low-Dose Ozone Concept in Preventive Medicine
4. Clinical Trials and Reports
4.1. Prevention against COVID-19
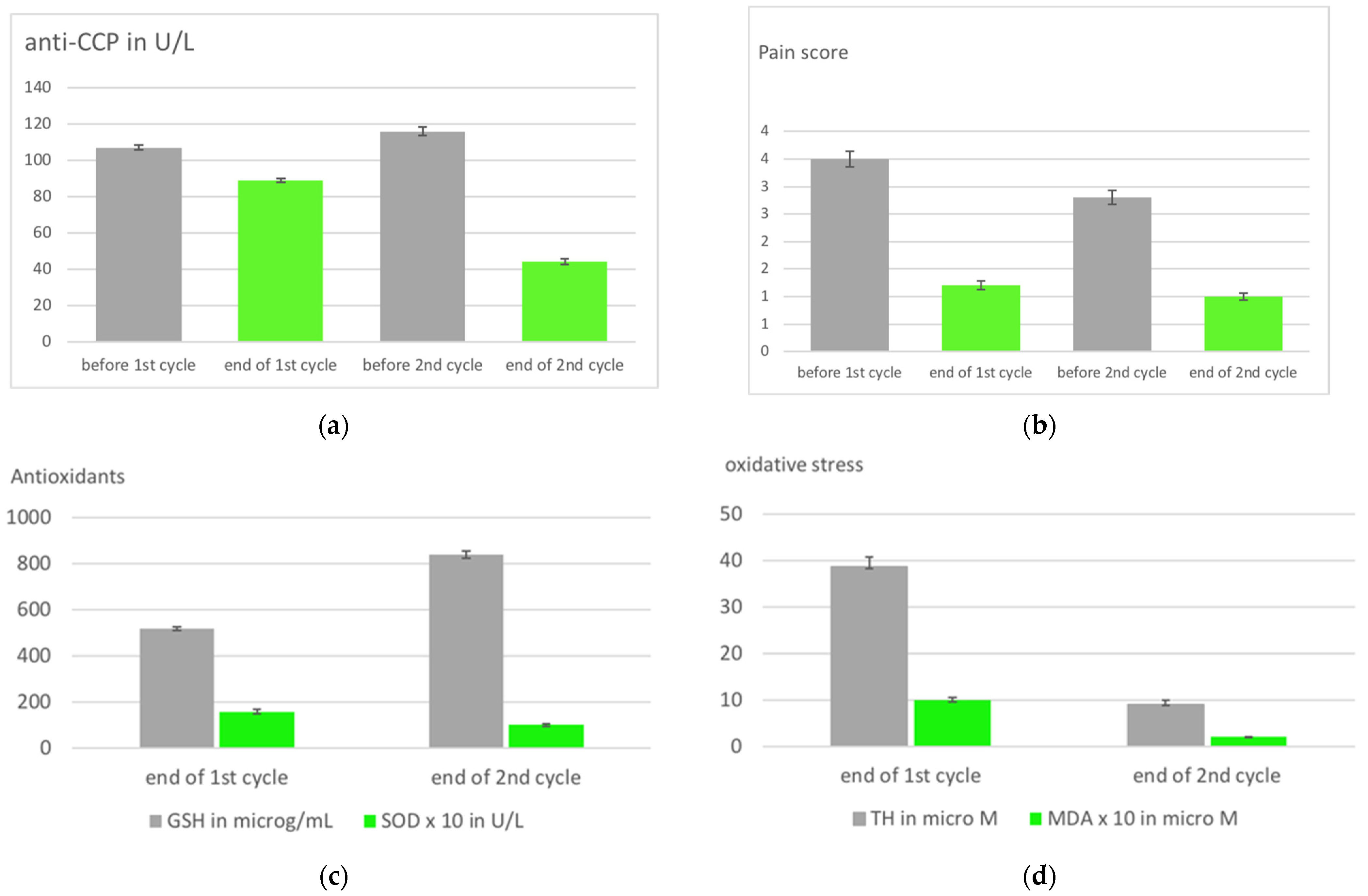
4.2. Oxidative Preconditioning in Rheumatoid Arthritis Patients with a Second Cycle of Ozone Treatment
4.3. Reference Substances
4.4. Involvement of the Innate Immune System
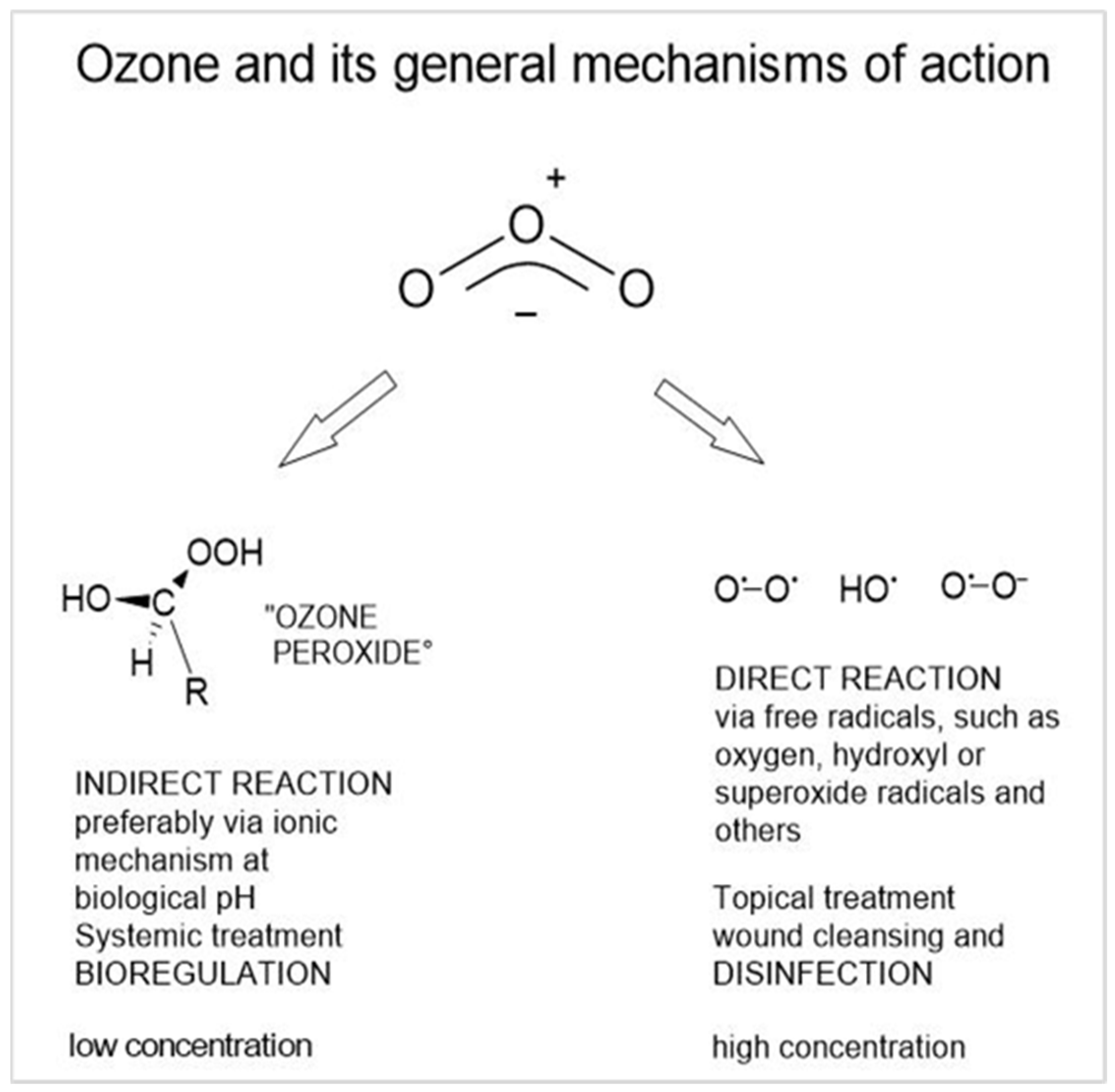
5. Mechanism of Action of Medical Ozone in Preventive Medicine
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schalekamp, M. Alles über Ozon, seine Vor- und Nachteile bei der Trinkwasserversorgung. (All about ozone, its advantages and disadvantages in drinking water supply). OzoNachrichten 1983, 2, 74–82. [Google Scholar]
- Alimohammadi, M.; Naderia, M. Effectiveness of Ozone Gas on Airborne Virus Inactivation in Enclosed Spaces: A Review Study. Ozone Sci. Eng. 2021, 43, 21–31. [Google Scholar] [CrossRef]
- Loeb, B. Ozone: Science & Engineering Thirty Years of Progress. Ozone Sci. Eng. 2009, 31, 379–392. [Google Scholar] [CrossRef]
- Martins, R.B.; Castro, I.A.; Pontelli, M.; Souza, J.P.; Lima, T.M.; Rezende Melo, R.S.; Zen Siqueira, J.P.; Caetano, M.H.; Arruda, E.; Gottardo de Almeida, M.T. SARS-CoV-2 Inactivation by Ozonated Water: A Preliminary Alternative for Environmental Disinfection. Ozone Sci. Eng. 2021, 43, 108–111. [Google Scholar] [CrossRef]
- Inagaki, H.; Akatsuki, S.; Sudaryatma, P.E.; Sugiyama, H.; Okabayashi, T.; Fujimoto, S. Rapid Inactivation of SARS-CoV-2 with Ozonated Water. Ozone Sci. Eng. 2021, 43, 208–212. [Google Scholar] [CrossRef]
- Tizaoui, C. Ozone: A Potential Oxidant for COVID-19 Virus (SARS-CoV-2). Ozone Sci. Eng 2020, 42, 378–385. [Google Scholar] [CrossRef]
- Hudson, J.B.; Sharma, M.; Vimalanathan, S. Development of a Practical Method for Using Ozone Gas as a Virus Decontaminating Agent. Ozone Sci. Eng. 2009, 31, 216–223. [Google Scholar] [CrossRef]
- Morrison, C.; Atkinson, A.; Zamyadi, A.; Kibuye, F.; McKie, M.; Hogard, S.; Mollica, P.; Jasim, S.; Wert, E.C. Critical Review and Research Needs of Ozone Applications Related to Virus Inactivation: Potential Implications for SARS-CoV-2. Ozone Sci. Eng. 2021, 43, 2–20. [Google Scholar] [CrossRef]
- Hoigne, L.; Bader, H. Ozonation of Water: Selectivity and Rate of Oxidation of Solutes. Ozone Sci. Eng. 1979, 1, 73–85. [Google Scholar] [CrossRef]
- Viebahn-Haensler, R.; León Fernández, O.S. Ozone in Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action In Chronic Inflammatory Diseases. Int. J. Mol. Sci. 2021, 22, 7890. [Google Scholar] [CrossRef]
- Schulz, S.; Rodriguez, Z.; Mutters, R.; Bette, M.; Hoffmann, S. Die lethale postoperative Peritonitis im Tiermodell. Infektprophylaxe und Therapie durch Kombination von Ozon und Antibiotika. (The lethal post-operative peritonitis in an animal model. Infection prophylaxis and therapy by combination of ozone and antibiotics). In Ozon-Handbuch. Grundlagen-Prävention-Therapie (Ozone-Handbook, Basics-Prevention-Therapy); Viebahn-Hänsler, R., Knoch, H.G., Eds.; Ecomed: Landsberg am Lech, Germany, 2000. [Google Scholar]
- Foglieni, C.; Fulgenzi, A.; Belloni, D.; Sciorati, C.; Ferrero, E.; Ferrero, M.E. Ozonated autohemotherapy: Protection of kidneys from ischemia in rats subjected to unilateral nephrectomy. BMC Nephrol. 2011, 12, 61. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Roche, L.; Riera-Romo, M.; Mesta, F.; Hernández-Matos, Y.; Barrios, J.M.; Martínez-Sánchez, G.; Al-Dalaien, S.M. Medical ozone promotes Nrf2 phosphorylation reducing oxidative stress and proinflammatory cytokines in multiple sclerosis patients. Eur. J. Pharmacol. 2017, 811, 148–154. [Google Scholar] [CrossRef]
- León Fernández, O.S.; Viebahn-Haensler, R.; López Cabreja, G.; Serrano Espinosa, I.; Hernández Matos, Y.; Delgado Roche, L.; Tamargo Santos, B.; Takon Oru, G.; Polo Vega, J.C. Medical Ozone Increases Methotrexate Clinical Response and Improves Cellular Redox Balance in Patients with Rheumatoid Arthritis. Eur. J. Pharmacol. 2016, 789, 313–318. [Google Scholar] [CrossRef]
- León Fernández, O.S.; Takon Oru, G.; Viebahn-Hänsler, R.; López Cabreja, L.; Serrano Espinosa, I.; García Fernández, E. Medical ozone arrests oxidative damage progression and regulates vasoactive mediator levels in older patients (60–70 years) with oxidative etiology diseases. Front. Physiol. 2022, 13, 1029805. [Google Scholar] [CrossRef]
- Clavo, B.; Rodríguez-Esparragó, F.; Rodríguez-Abreu, D.; Llontop, P.; Aguiar-Bujanda, D.; Santana-Rodríguez, N. Modulation of Oxidative Stress by Ozone Therapy in the Prevention and Treatment of Chemotherapy-Induced Toxicity: Review and Prospects. Antioxidants 2019, 8, 588. [Google Scholar] [CrossRef]
- Martínez-Sánchez, G. Ozone Therapy for Prevention and Treatment of COVID-19. J. Explor. Res. Pharmacol. 2022, 7, 189–194. [Google Scholar] [CrossRef]
- Sharma, A.; Shah, M.; Sane, H.; Gokulchandran, N.; Paranjape, A.; Khubchandani, P.; Captain, J.; Shirke, S.; Kulkarni, P. Intravenous ozonized saline therapy as prophylaxis for healthcare workers (HCWs) in a dedicated COVID-19 hospital in India. A retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3632–3639. [Google Scholar]
- Shah, M.; Captain, J.; Ganu, G. Immunity Prophylaxis with Ozone Therapy. Review Report. J. Ozone Ther. 2020, 7, 86–88. [Google Scholar] [CrossRef]
- Orscelik, A.; Karaaslan, B.; Agiragac, B.; Solmaz, I.; Parpucu, M. Could the minor autohemotherapy be a complementary therapy for healthcare professionals to prevent COVID-19 infection? Ann. Med. Res. 2021, 28, 1863–1869. [Google Scholar] [CrossRef]
- Chaijadi, D.; Hendradiana, A.; Tjahjono, P.D.; Kusumaningsih, E.; Hariyanto; Siagian, C.; Atmadja, D.S.; Viebahn-Hänsler, R. The Role of Ozone Therapy as Adjuvant in the Management of Covid-19 in Indonesia. In Proceedings of the IOA 26th Ozone World Congress and Exhibition, Milan, Italy, 2–7 July 2023. [Google Scholar]
- Gencer-Aalay, K.; Sahin, T. Could ozone therapy be used to prevent COVID-19? Marmara Med. J. 2022, 35, 196–201. Available online: https://dergipark.org.tr/tr/pub/marumj (accessed on 30 May 2022).
- Falzoni, W.; Senvaitis, M.I.; Iwasa, S. COVID-19 prophylaxis with ozone therapy. Acupunct. Electro-Ther. Res. 2021, 46, 35–36. [Google Scholar]
- Medina, J.G. Comparative analysis of 2 groups of people according to age and sex, vaccinated triple versus covid-19, were subjected to quantitative analysis of antibodies and B lymphocytes after ozone therapy. J. Ozone Ther. 2022, 6, 11–12. [Google Scholar] [CrossRef]
- Krishna, S.; Bustamante, L.; Haynes, R.K.; Staines, H.M. Artemisinins: Their growing importance in medicine. Trends Pharmacol. Sci. 2008, 29, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Lell, B.; Viebahn, R.; Kremsner, P. The activity of ozone against plasmodium falciparum. Ozone Sci. Eng. 2001, 23, 89–93. [Google Scholar] [CrossRef]
- Travagli, F.; Zanardi, I.; Silvietti, A.; Bocci, V. A physicochemical investigation on the effects of ozone on blood. Int. J. Biol. Macromol. 2007, 41, 504–511. [Google Scholar] [CrossRef]
- Bocci, V.; Luzzi, E.; Corradeschi, F.; Paulesu, L.; Rossi, R.; Cardaioli, E.; Di Simplicio, P. Studies on the Biological Effects of Ozone: 4. Cytokine Production and Glutathione Levels in Human Erythrocytes. J. Boil. Regul. Homeost. Agents 1993, 7, 133–138. [Google Scholar]
- Schulz, S.; Rodriguez, Z.; Mutters, R.; Menendez, S.; Bette, M. Repetitive pneumoperitoneum with ozonized oxygen as a preventive in lethal polymicrobial sepsis in rats. Eur. Surg. Res. 2003, 35, 26–34. [Google Scholar] [CrossRef]
- Zamora, Z.B.; Borrego, A.; Lopez, O.Y.; Delgado, R.; Gonzalez, R.; Menendez, S.; Hernandez, F.; Schulz, S. Effects of Ozone Oxidative Preconditioning on TNF-α Release and Antioxidant-Prooxidant Intracellular Balance in Mice During Endotoxic Shock. Mediat. Inflamm. 2005, 2005, 634736. [Google Scholar] [CrossRef]
- Bette, M.; Nuessing, R.M.; Mutters, R.; Zamora, Z.B.; Menendez, S.; Schulz, S. Efficiency of tazobactam/piperacillin in lethal peritonitis is enhanced after preconditioning of rats with O3/O2-pneumoperitoneum. SHOCK 2006, 25, 23–29. [Google Scholar] [CrossRef]
- Viebahn-Haensler, R.; León Fernández, O.S.; Fahmy, Z. Ozone in medicine: The low-dose ozone concept. Guidelines and treatment strategies. Ozone Sci. Eng. 2012, 34, 408–424. [Google Scholar] [CrossRef]
- Léon, O.S.; Menendéz, S.; Merino, N.; Castillo, R.; Sam, S.; Pérez, L.; Cruz, E.; Bocci, V. Ozone oxidative preconditioning: A protection against cellular damage by free radicals. Mediat. Inflamm. 1998, 7, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Peralta, C.; León, O.S.; Xaus, C.; Prats, N.; Sala Planell, E.; Puig-Parellada, P.; Gelpí, E.; Roselló-Catafau, J. Protective effect of ozone treatment on the injury associated with hepatic ischemia-reperfusion: Antioxidant-prooxidant balance. Free Radic. Res. 1999, 31, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Candelario-Jalil, S.; Al-Dalain, M.; Fernández, O.S.; Menéndez, S.; Pérez-Davison, G.; Merino, N.; Sam, S.; Ajamieh, H.H. Oxidative preconditioning affords protection against carbon tetrachloride-induced glycogen depletion and oxidative stress in rats, animal model. J. Appl. Toxicol. 2001, 21, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Borrego, A.; Zamora, Z.B.; Gonzalez, R.; Romay, C.; Menendez, S.; Hernandez, F.; Montero, T.; Rojas, E. Protection by ozone preconditioning is mediated by the antioxidant system in cisplatin-induced nephrotoxicity in rats. Mediators Inflamm. 2004, 13, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Wolff, H. Textbook Das Medizinische Ozon; Verlag für Medizin: Heidelberg, Germany, 1979. [Google Scholar]
- Takon Oru, G.; Viebahn-Haensler, R.; García Fernández, E.; Alvarez Almiñaque, D.; Polo Vega, J.C.; Tamargo Santos, B.; López Cabreja, G.; Serrano Espinosa, I.; Tabares Nápoles, N.; León Fernández, O.S. Medical Ozone Effects and Innate Immune Memory in Rheumatoid Arthritis Patients Treated with Methotrexate+Ozone After a Second Cycle of Ozone Exposure. Chronic Pain Manag. 2019, 2, 114. [Google Scholar] [CrossRef]
- Criegee, R.; Lohaus, G. Über das Ozonid des 1.2-Dimethyl-cyclopentens-(1) (II. Mitteil. über den Verlauf der Ozonspaltung). Chem. Berichte 1953, 86, 1–4. [Google Scholar] [CrossRef]
- Von Sonntag, C.; Von Gunten, U. Chemistry of Ozone in Water and Wastewater Treatment: From Basic Principles to Applications; IWA Publishing: London, UK, 2012; Chapter 6; 302p, Available online: https://iwaponline.com/ebooks/book/465/Chemistry-of-Ozone-in-Water-and-Wastewater (accessed on 1 January 2020).
- Togi, S.; Togo, M.; Nagashima, S.; Kitai, Y.; Muromoto, R.; Kashiwakura, J.; Miura, T.; Matsuda, T. Implication of NFkB Activation of Ozone-Induced HO-1 Activation. BRP Rep. 2021, 4, 59–63. [Google Scholar] [CrossRef]
- Sies, H. Glutathione and Its Role in Cellular Functions. Free Radic. Biol. Med. 1999, 27, 916–921. [Google Scholar] [CrossRef]
- Sies, H. Oxidative Eustress: On Constant Alert for Redox Homeostasis. Redox Biol. 2021, 41, 101867. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Study | Results | Application Route | References |
|---|---|---|---|
| Medical ozone promotes Nrf2 phosphorylation reducing oxidative stress and proinflammatory cytokines in multiple sclerosis patients. | Secondary prevention GSH increase. | RI, 20 mg/L. | Delgado-Roche, L.; Riera-Romo, M.; Mesta, F.; Hernández-Matos, Y.; Barrios, J.M.; Martínez-Sánchez, G.; Al-Dalaien, S.M. 2017. [13]. |
| Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Clinical trial. | Statistical significant reduction of liver toxicity in patients with rheumatoid arthritis during MTX treatment. See text. | 10 rectal insufflations in 10 days. | León Fernández, O.S.; Viebahn-Haensler, R.; López Cabreja, G.; Serrano Espinosa, I.; Hernández Matos, Y.; Delgado Roche, L.; Tamargo Santos, B.; Takon Oru, G.; Polo Vega, J.C. 2016. [14]. |
| Medical ozone arrests oxidative damage progression and regulates vasoactive mediator levels in older patients (60–70 years) with oxidative etiology diseases. Controlled clinical study. | Positive influence on aging process. See text. | Rectal insufflation. | León Fernández, O. S., Takon Oru, G., Viebahn-Hänsler, R., López Cabreja, G., Serrano Espinosa, I., García Fernández, E. 2022. [15]. |
| Modulation of Oxidative Stress by Ozone Therapy in the Prevention and Treatment of Chemotherapy-Induced Toxicity: Review and Prospects. | Prevention from toxicity, mainly in animal models. | Systemic applications. | Clavo, B.; Rodríguez-Esparragó, F.; Rodríguez-Abreu, D.; Llontop, P.; Aguiar-Bujanda, D.; Santana-Rodríguez, N. 2019. [16]. |
| Type of Study | Results | Application Route | References |
|---|---|---|---|
| Ozone Therapy for Prevention and Treatment of COVID-19. Review. | 4 publications on prevention. | Different forms of application. | Martínez-Sánchez, G. 2022. [17]. |
| Intravenous ozonized saline therapy as prophylaxis for healthcare workers (HCWs) in a dedicated COVID-19 hospital in India. A retrospective study. | Less infections in the ozone group (4.6%) than in the control (14.03%). n = 64 (235). | Ozonized saline. | Sharma, A.; Shah, M.; Sane, H.; Gokulchandran, N.; Paranjape, A.; Khubchandani, P.; Captain, J.; Shirke, S.; Kulkarni, P. 2021. [18]. |
| Immunity Prophylaxis with Ozone Therapy. Review Report. | 2.19% incidence rate (n = 320). | Minor autohemotherapy. | Shah, M.; Captain, J.; Ganu, G. 2020. [19]. |
| Could the minor autohemotherapy be a complementary therapy for healthcare professionals to prevent COVID-19 infection? | (n = 73) No infection or positive test. | Minor autohemotherapy. | Orscelik, A.; Karaaslan, B.; Agiragac, B.; Solmaz, I.; Parpucu, M. 2021. [20]. |
| The Role of Ozone Therapy as Adjuvant in the Management of COVID-19 in Indonesia. Clinical trial. | See text. | MAH, RI, and vaginal insufflation. | Chaijadi, D.; Hendradiana, A.; Tjahjono, P.D.; Kusumaningsih, E.; Hariyanto.; Siagian, C.; Atmadja, D.S.; Viebahn-Hänsler, R. 2023. [21]. |
| Could ozone therapy be used to prevent COVID-19? Clinical trial. | 2 of 71 persons were tested positive. Retrospective, no control. 45% medical professionals. See text. | MAH, 10 treatments. | Gencer-Aalay, K.; Sahin, T. 2022. [22]. |
| COVID-19 prophylaxis with ozone therapy. | n = 9, good effect but no protection from further infection. | RI. | Falzoni, W.; Senvaitis, M.I.; Iwasa, S. 2021. [23]. |
| Comparative analysis of 2 groups of people according to age and sex, vaccinated triple versus COVID-19, were subjected to quantitative analysis of antibodies and B lymphocytes after ozone therapy. Clinical trial. | See text. | MAH. | Medina, J.G. 2022. [24]. |
| MAH | RI | Main Indications | |
|---|---|---|---|
| Ozone concentration | 10 to 40 μg/mL | 10 to 40 μg/mL | Chronic inflammatory diseases or diseases accompanied by inflammation, such as RA, angiopathy. Age-related diseases, chronic intestinal diseases. Prevention. |
| Volume | 50 to 100 mL | 150 to 300 mL | |
| Dose | 500 to 4000 μg | 1500 to 12,000 μg |
| Control Group, n = 52 | Ozone Group, n = 57 |
|---|---|
| 3 × vaccinated: n = 33 (63.5%); 2 × vaccinated: n = 19 (36.5%) | 3 × vaccinated: n = 31 (54.4%); 2 × vaccinated: n = 26 (45.6%) |
| female n = 33, male n = 19 age 20 to 55 | female n = 24, male n = 33 age 20 to 55 |
| MAH: 1 × per week, 8 treatments RI: 2 × per week during 2 weeks, then 1 × per week; 15–16 treatments |
| Injury Biomarkers: Oxidative Stress Markers | Protective Markers: Antioxidants | Clinical Parameters |
|---|---|---|
| TH (total hydroperoxides) | Total SOD (superoxide dismutase) CAT (catalase) | DAS (disease activity score) PAIN |
| MDA (malondialdehyde) AOOP (advanced oxidation protein products) | GSH (reduced glutathione) | HAQ: DI (health assessment disability questionnaire) |
| NO (nitrogen monoxide) | GGT (gamma glutamyl transferase) | Auto antibodies CCP (anti-cyclic citrullinated peptides) |
| Application | Ozone Concentration | Ozone Volume | Treatment Frequency |
|---|---|---|---|
| RI | 15–25 µg/mL In general: 10 to max. 40 µg/mL | 150–300 mL | twice per week, if possible prior to chemotherapy or antibiotics. At least once per week as adjuvant therapy two or 3 series per year with 10 treatments each. |
| MAH | 15–25 µg/mL In general: 10 to max. 40 µg/mL | 50 mL | 2 or 3 treatments per week, if possible prior to chemotherapy or antibiotics. At least once per week as adjuvant therapy or 2 to 3 series per year with 10 treatments each. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viebahn-Haensler, R.; León Fernández, O.S. Ozone as Redox Bioregulator in Preventive Medicine: The Molecular and Pharmacological Basis of the Low-Dose Ozone Concept—A Review. Int. J. Mol. Sci. 2023, 24, 15747. https://doi.org/10.3390/ijms242115747
Viebahn-Haensler R, León Fernández OS. Ozone as Redox Bioregulator in Preventive Medicine: The Molecular and Pharmacological Basis of the Low-Dose Ozone Concept—A Review. International Journal of Molecular Sciences. 2023; 24(21):15747. https://doi.org/10.3390/ijms242115747
Chicago/Turabian StyleViebahn-Haensler, Renate, and Olga Sonia León Fernández. 2023. "Ozone as Redox Bioregulator in Preventive Medicine: The Molecular and Pharmacological Basis of the Low-Dose Ozone Concept—A Review" International Journal of Molecular Sciences 24, no. 21: 15747. https://doi.org/10.3390/ijms242115747
APA StyleViebahn-Haensler, R., & León Fernández, O. S. (2023). Ozone as Redox Bioregulator in Preventive Medicine: The Molecular and Pharmacological Basis of the Low-Dose Ozone Concept—A Review. International Journal of Molecular Sciences, 24(21), 15747. https://doi.org/10.3390/ijms242115747