
Current Progress of Platelet-Rich Derivatives in Cartilage and Joint Repairs



 ,
,  , and
, and
Abstract
1. Introduction
2. Evolution of Platelet-Rich Derivatives
2.1. Fibrin Glue
2.2. Platelet-Rich Plasma (PRP)
2.3. Platelet-Rich Fibrin (PRF)
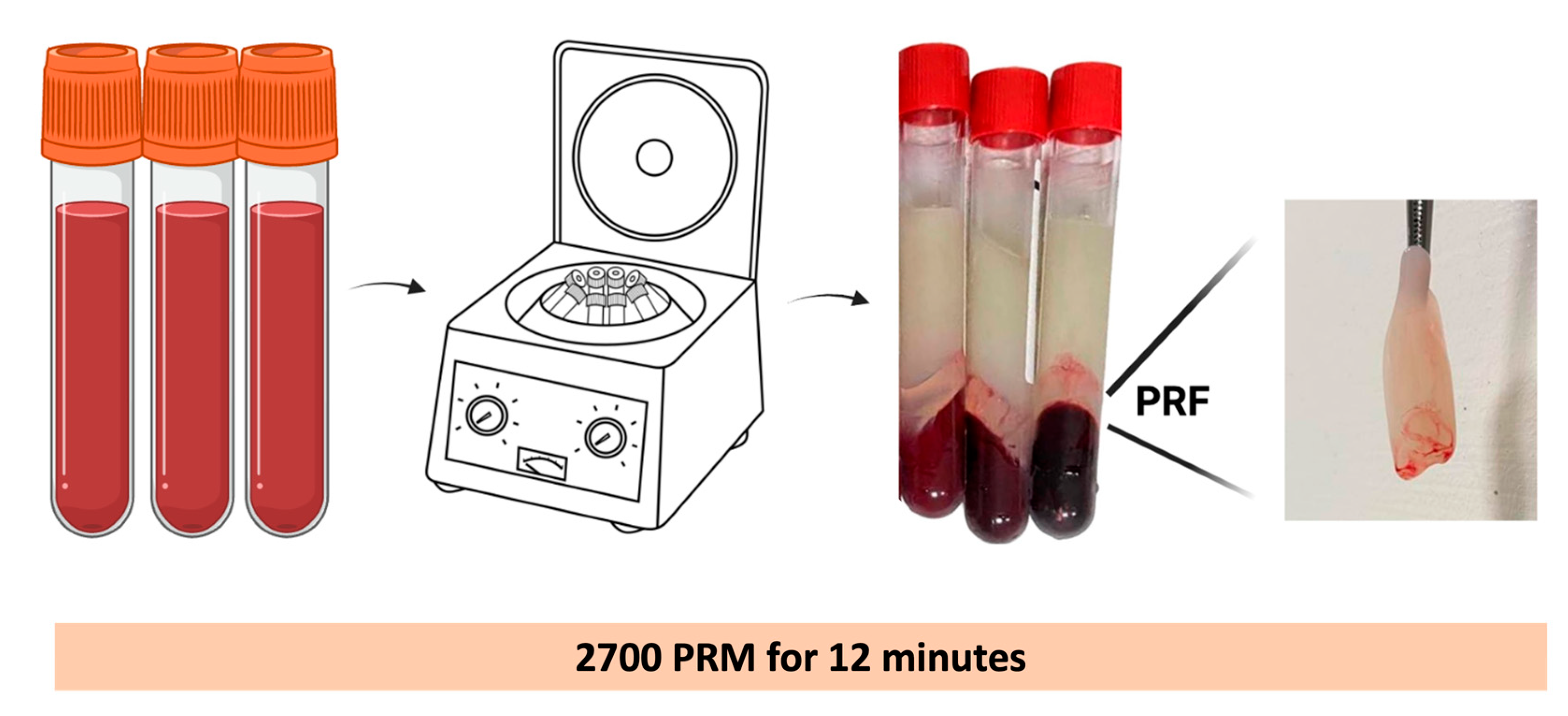
2.3.1. PRF Preparation
2.3.2. Components of PRF
3. Clinical Application
3.1. Oral and Maxillofacial Surgery
3.2. Musculoskeletal Disorders
3.2.1. Repair and Regeneration of Cartilage
3.2.2. Meniscal Repair
3.2.3. Repair and Regeneration of Tendons
3.2.4. Repair Ligament
4. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matras, H. Effect of various fibrin preparations on reimplantations in the rat skin. Osterr. Z. Stomatol. 1970, 67, 338–359. [Google Scholar] [PubMed]
- Marx, R.E.; Carlson, E.R.; Eichstaedt, R.M.; Schimmele, S.R.; Strauss, J.E.; Georgeff, K.R. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1998, 85, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Deppermann, C.; Kubes, P. Start a fire, kill the bug: The role of platelets in inflammation and infection. Innate Immun. 2018, 24, 335–348. [Google Scholar] [CrossRef]
- Boswell, S.G.; Cole, B.J.; Sundman, E.A.; Karas, V.; Fortier, L.A. Platelet-rich plasma: A milieu of bioactive factors. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 429–439. [Google Scholar] [CrossRef]
- Choukroun, J.; Adda, F.; Schoeffler, C.; Vervelle, A. Une opportunité en paro-implantologie: Le PRF. Implantodontie 2001, 42, e62. [Google Scholar]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Trandafilovic, M.; Stojanovic, P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Med. Wars 2021, 16, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e45–e50. [Google Scholar] [CrossRef]
- Vinaya Kumar, R.; Shubhashini, N. Platelet rich fibrin: A new paradigm in periodontal regeneration. Cell Tissue Bank. 2013, 14, 453–463. [Google Scholar] [CrossRef]
- Masuki, H.; Okudera, T.; Watanebe, T.; Suzuki, M.; Nishiyama, K.; Okudera, H.; Nakata, K.; Uematsu, K.; Su, C.Y.; Kawase, T. Growth factor and pro-inflammatory cytokine contents in platelet-rich plasma (PRP), plasma rich in growth factors (PRGF), advanced platelet-rich fibrin (A-PRF), and concentrated growth factors (CGF). Int. J. Implant. Dent. 2016, 2, 19. [Google Scholar] [CrossRef] [PubMed]
- Esfahrood, Z.R.; Ardakani, M.T.; Shokri, M.; Shokri, M. Effects of leukocyte-platelet-rich fibrin and advanced platelet-rich fibrin on the viability and migration of human gingival fibroblasts. J. Indian Soc. Periodontol. 2020, 24, 15–19. [Google Scholar] [CrossRef]
- Bi, J.; Intriago, M.F.B.; Koivisto, L.; Jiang, G.; Häkkinen, L.; Larjava, H. Leucocyte- and platelet-rich fibrin regulates expression of genes related to early wound healing in human gingival fibroblasts. J. Clin. Periodontol. 2020, 47, 851–862. [Google Scholar] [CrossRef]
- Ghanaati, S.; Booms, P.; Orlowska, A.; Kubesch, A.; Lorenz, J.; Rutkowski, J.; Landes, C.; Sader, R.; Kirkpatrick, C.; Choukroun, J. Advanced platelet-rich fibrin: A new concept for cell-based tissue engineering by means of inflammatory cells. J. Oral Implant. 2014, 40, 679–689. [Google Scholar] [CrossRef]
- Tunalı, M.; Özdemir, H.; Küçükodacı, Z.; Akman, S.; Fıratlı, E. In vivo evaluation of titanium-prepared platelet-rich fibrin (T-PRF): A new platelet concentrate. Br. J. Oral Maxillofac. Surg. 2013, 51, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Tunalı, M.; Özdemir, H.; Küçükodacı, Z.; Akman, S.; Yaprak, E.; Toker, H.; Fıratlı, E. A novel platelet concentrate: Titanium-prepared platelet-rich fibrin. Biomed. Res. Int. 2014, 2014, 209548. [Google Scholar] [CrossRef] [PubMed]
- Shashank, B.; Bhushan, M. Injectable Platelet-Rich Fibrin (PRF): The newest biomaterial and its use in various dermatological conditions in our practice: A case series. J. Cosmet. Dermatol. 2021, 20, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Hassan, H.; Quinlan, D.J.; Ghanem, A. Injectable platelet-rich fibrin for facial rejuvenation: A prospective, single-center study. J. Cosmet. Dermatol. 2020, 19, 3213–3221. [Google Scholar] [CrossRef]
- Grecu, A.F.; Reclaru, L.; Ardelean, L.C.; Nica, O.; Ciucă, E.M.; Ciurea, M.E. Platelet-Rich Fibrin and its Emerging Therapeutic Benefits for Musculoskeletal Injury Treatment. Medicina 2019, 55, 141. [Google Scholar] [CrossRef]
- Kartika, R.W.; Alwi, I.; Suyatna, F.D.; Yunir, E.; Waspadji, S.; Immanuel, S.; Bardosono, S.; Sungkar, S.; Rachmat, J.; Hediyati, M.; et al. Wound Healing in Diabetic Foot Ulcer Patients Using Combined Use of Platelet Rich Fibrin and Hyaluronic Acid, Platelet Rich Fibrin and Placebo: An Open Label, Randomized Controlled Trial. Acta Med. Indones 2021, 53, 268–275. [Google Scholar]
- Cieslik-Bielecka, A.; Choukroun, J.; Odin, G.; Dohan Ehrenfest, D.M. L-PRP/L-PRF in esthetic plastic surgery, regenerative medicine of the skin and chronic wounds. Curr. Pharm. Biotechnol. 2012, 13, 1266–1277. [Google Scholar] [CrossRef]
- Kumar, K.R.; Genmorgan, K.; Abdul Rahman, S.M.; Rajan, M.A.; Kumar, T.A.; Prasad, V.S. Role of plasma-rich fibrin in oral surgery. J. Pharm. Bioallied Sci. 2016, 8 (Suppl. S1), S36–S38. [Google Scholar] [CrossRef]
- Fan, Y.; Perez, K.; Dym, H. Clinical Uses of Platelet-Rich Fibrin in Oral and Maxillofacial Surgery. Dent. Clin. N. Am. 2020, 64, 291–303. [Google Scholar] [CrossRef]
- Tashnizi, M.A.; Alamdari, D.H.; Khayami, M.E.; Rahimi, H.R.; Moeinipour, A.; Amouzeshi, A.; Seifalian, A.M. Treatment of non-healing sternum wound after open-heart surgery with allogenic platelet-rich plasma and fibrin glue-preliminary outcomes. Indian J. Plast. Surg. 2013, 46, 538–542. [Google Scholar] [CrossRef]
- Silver, F.H.; Wang, M.-C.; Pins, G.D. Preparation and use of fibrin glue in surgery. Biomaterials 1995, 16, 891–903. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e37–e44. [Google Scholar] [CrossRef] [PubMed]
- Tayapongsak, P.; O’Brien, D.A.; Monteiro, C.B.; Arceo-Diaz, L.Y. Autologous fibrin adhesive in mandibular reconstruction with particulate cancellous bone and marrow. J. Oral Maxillofac. Surg. 1994, 52, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Goczyńska, P.; Lasocka, J.; Lachert, E. Fibrin glues—The current state of knowledge. J. Transfus. Med. 2021, 14, 214–224. [Google Scholar] [CrossRef]
- Raja, V.S.; Naidu, E.M. Platelet-rich fibrin: Evolution of a second-generation platelet concentrate. Indian J. Dent. Res. 2008, 19, 42. [Google Scholar] [CrossRef]
- Ehrenfest, D.M.D.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte-and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Jia, Y.; Zhai, G.; Wang, E.; Li, P. Efficacy of local hemostatic agents after endoscopic submucosal dissection: A meta-analysis. Minim. Invasive Ther. Allied Technol. 2022, 31, 1017–1025. [Google Scholar] [CrossRef]
- Habib Bedwani, N.A.R.; Kelada, M.; Smart, N.; Szydlo, R.; Patten, D.K.; Bhargava, A. Glue versus mechanical mesh fixation in laparoscopic inguinal hernia repair: Meta-analysis and trial sequential analysis of randomized clinical trials. Br. J. Surg. 2021, 108, 14–23. [Google Scholar] [CrossRef]
- Mungroop, T.H.; van der Heijde, N.; Busch, O.R.; de Hingh, I.H.; Scheepers, J.J.; Dijkgraaf, M.G.; Groot Koerkamp, B.; Besselink, M.G.; van Eijck, C.H.; on behalf of the Dutch Pancreatic Cancer Group. Randomized clinical trial and meta-analysis of the impact of a fibrin sealant patch on pancreatic fistula after distal pancreatectomy: CPR trial. BJS Open 2021, 5, zrab001. [Google Scholar] [CrossRef]
- Koopman, J.E.; Duraku, L.S.; de Jong, T.; de Vries, R.B.M.; Michiel Zuidam, J.; Hundepool, C.A. A systematic review and meta-analysis on the use of fibrin glue in peripheral nerve repair: Can we just glue it? J. Plast. Reconstr. Aesthetic Surg. 2022, 75, 1018–1033. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.C.; Fideles, S.O.M.; Pomini, K.T.; Bellini, M.Z.; Pereira, E.; Reis, C.H.B.; Pilon, J.P.G.; de Marchi, M.; Trazzi, B.F.M.; da Silva, W.S.; et al. Potential of Fibrin Glue and Mesenchymal Stem Cells (MSCs) to Regenerate Nerve Injuries: A Systematic Review. Cells 2022, 11, 221. [Google Scholar] [CrossRef] [PubMed]
- Whitman, D.H.; Berry, R.L.; Green, D.M. Platelet gel: An autologous alternative to fibrin glue with applications in oral and maxillofacial surgery. J. Oral Maxillofac. Surg. 1997, 55, 1294–1299. [Google Scholar] [CrossRef] [PubMed]
- Giannobile, W. Periodontal tissue engineering by growth factors. Bone 1996, 19, S23–S37. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Platelet-rich plasma: Evidence to support its use. J. Oral Maxillofac. Surg. 2004, 62, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Jameson, C.A. Autologous platelet concentrate for the production of platelet gel. Lab. Med. 2007, 38, 39–42. [Google Scholar] [CrossRef]
- Weibrich, G.; Kleis, W.K.; Hafner, G.; Hitzler, W.; Wagner, W. Comparison of platelet, leukocyte, and growth factor levels in point-of-care platelet-enriched plasma, prepared using a modified Curasan kit, with preparations received from a local blood bank. Clin. Oral Implant. Res. 2003, 14, 357–362. [Google Scholar] [CrossRef]
- Lucarelli, E.; Beretta, R.; Dozza, B.; Tazzari, P.; O’Connel, S.; Ricci, F.; Pierini, M.; Squarzoni, S.; Pagliaro, P.; Oprita, E. A recently developed bifacial platelet-rich fibrin matrix. Eur. Cell Mater. 2010, 20, 13–23. [Google Scholar] [CrossRef]
- Saluja, H.; Dehane, V.; Mahindra, U. Platelet-Rich fibrin: A second generation platelet concentrate and a new friend of oral and maxillofacial surgeons. Ann. Maxillofac. Surg. 2011, 1, 53. [Google Scholar] [CrossRef]
- Charrier, J.; Monteil, J.; Albert, S.; Collon, S.; Bobin, S.; Dohan, D.E. Relevance of Choukroun’s Platelet-Rich Fibrin (PRF) and SMAS flap in primary reconstruction after superficial or subtotal parotidectomy in patients with focal pleiomorphic adenoma: A new technique. Rev. Laryngol.-Otol.-Rhinol. 2008, 129, 313–318. [Google Scholar]
- Bergeson, A.G.; Tashjian, R.Z.; Greis, P.E.; Crim, J.; Stoddard, G.J.; Burks, R.T. Effects of platelet-rich fibrin matrix on repair integrity of at-risk rotator cuff tears. Am. J. Sports Med. 2012, 40, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Sclafani, A.P. Safety, efficacy, and utility of platelet-rich fibrin matrix in facial plastic surgery. Arch. Facial Plast. Surg. 2011, 13, 247–251. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Lin, Y.; Hu, X.; Zhang, Y.; Wu, H. A comparative study of platelet-rich fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 707–713. [Google Scholar] [CrossRef]
- Kuo, T.-F.; Lin, M.-F.; Lin, Y.-H.; Lin, Y.-C.; Su, R.-J.; Lin, H.-W.; Chan, W.P. Implantation of platelet-rich fibrin and cartilage granules facilitates cartilage repair in the injured rabbit knee: Preliminary report. Clinics 2011, 66, 1835–1838. [Google Scholar] [CrossRef]
- Simonpieri, A.; Del Corso, M.; Vervelle, A.; Jimbo, R.; Inchingolo, F.; Sammartino, G.; M Dohan Ehrenfest, D. Current knowledge and perspectives for the use of platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) in oral and maxillofacial surgery part 2: Bone graft, implant and reconstructive surgery. Curr. Pharm. Biotechnol. 2012, 13, 1231–1256. [Google Scholar] [CrossRef] [PubMed]
- Kanayama, T.; Sigetomi, T.; Sato, H.; Yokoi, M. Crestal approach sinus floor elevation in atrophic posterior maxilla using only platelet rich fibrin as grafting material: A computed tomography evaluation of 2 cases. J. Oral Maxillofac. Surg. Med. Pathol. 2014, 26, 519–525. [Google Scholar] [CrossRef]
- Del Corso, M.; Dohan Ehrenfest, D. Immediate implantation and peri-implant Natural Bone Regeneration (NBR) in the severely resorbed posterior mandible using Leukocyte-and Platelet-Rich Fibrin (L-PRF): A 4-year follow-up. Poseido 2013, 1, 109–116. [Google Scholar]
- Kang, Y.-H.; Jeon, S.H.; Park, J.-Y.; Chung, J.-H.; Choung, Y.-H.; Choung, H.-W.; Kim, E.-S.; Choung, P.-H. Platelet-rich fibrin is a Bioscaffold and reservoir of growth factors for tissue regeneration. Tissue Eng. Part A 2011, 17, 349–359. [Google Scholar] [CrossRef]
- Wu, C.L.; Lee, S.S.; Tsai, C.H.; Lu, K.H.; Zhao, J.H.; Chang, Y.C. Platelet-rich fibrin increases cell attachment, proliferation and collagen-related protein expression of human osteoblasts. Aust. Dent. J. 2012, 57, 207–212. [Google Scholar] [CrossRef]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.-O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part V: Histologic evaluations of PRF effects on bone allograft maturation in sinus lift. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Hauser, F.; Gaydarov, N.; Badoud, I.; Vazquez, L.; Bernard, J.-P.; Ammann, P. Clinical and histological evaluation of postextraction platelet-rich fibrin socket filling: A prospective randomized controlled study. Implant Dent. 2013, 22, 295–303. [Google Scholar] [CrossRef]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.-O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e56–e60. [Google Scholar] [CrossRef] [PubMed]
- Whiteheart, S.W. Platelet granules: Surprise packages. Blood 2011, 118, 1190–1191. [Google Scholar] [CrossRef]
- Mihaylova, Z.; Mitev, V.; Stanimirov, P.; Isaeva, A.; Gateva, N.; Ishkitiev, N. Use of platelet concentrates in oral and maxillofacial surgery: An overview. Acta Odontol. Scand. 2017, 75, 1–11. [Google Scholar] [CrossRef]
- Gunning, W.T. The Platelet Delta Granule and Its Role in Hemostasis. Microsc. Microanal. 2003, 9, 1362–1363. [Google Scholar] [CrossRef]
- Ciferri, S.; Emiliani, C.; Guglielmini, G.; Orlacchio, A.; Nenci, G.G.; Gresele, P. Platelets release their lysosomal content in vivo in humans upon activation. Thromb. Haemost. 2000, 83, 157–164. [Google Scholar] [CrossRef]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Marques, L.F.; Stessuk, T.; Camargo, I.C.C.; Sabeh Junior, N.; Santos, L.D.; Ribeiro-Paes, J.T. Platelet-rich plasma (PRP): Methodological aspects and clinical applications. Platelets 2015, 26, 101–113. [Google Scholar] [CrossRef]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Stojanovic, P. Platelet rich plasma: A short overview of certain bioactive components. Open Med. 2016, 11, 242–247. [Google Scholar] [CrossRef]
- Knezevic, N.N.; Candido, K.D.; Desai, R.; Kaye, A.D. Is platelet-rich plasma a future therapy in pain management? Med. Clin. 2016, 100, 199–217. [Google Scholar] [CrossRef]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood J. Am. Soc. Hematol. 2011, 117, 3720–3732. [Google Scholar] [CrossRef] [PubMed]
- Artlett, C.M. The IL-1 family of cytokines. Do they have a role in scleroderma fibrosis? Immunol. Lett. 2018, 195, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e51–e55. [Google Scholar] [CrossRef]
- Karin, M.; Clevers, H. Reparative inflammation takes charge of tissue regeneration. Nature 2016, 529, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Xue, X.; Falcon, D.M. The role of immune cells and cytokines in intestinal wound healing. Int. J. Mol. Sci. 2019, 20, 6097. [Google Scholar] [CrossRef]
- Sokol, C.L.; Barton, G.M.; Farr, A.G.; Medzhitov, R. A mechanism for the initiation of allergen-induced T helper type 2 responses. Nat. Immunol. 2008, 9, 310–318. [Google Scholar] [CrossRef]
- Salmon-Ehr, V.; Ramont, L.; Godeau, G.; Birembaut, P.; Guenounou, M.; Bernard, P.; Maquart, F.-X. Implication of interleukin-4 in wound healing. Lab. Investig. 2000, 80, 1337–1343. [Google Scholar] [CrossRef]
- Brockmann, L.; Giannou, A.D.; Gagliani, N.; Huber, S. Regulation of TH17 cells and associated cytokines in wound healing, tissue regeneration, and carcinogenesis. Int. J. Mol. Sci. 2017, 18, 1033. [Google Scholar] [CrossRef]
- Bai, M.Y.; Wang, C.W.; Wang, J.Y.; Lin, M.F.; Chan, W.P. Three-dimensional structure and cytokine distribution of platelet-rich fibrin. Clinics 2017, 72, 116–124. [Google Scholar] [CrossRef]
- Bai, M.-Y.; Chuang, M.-H.; Lin, M.-F.; Tang, S.-L.; Wong, C.-C.; Chan, W.P. Relationships of Age and Sex with Cytokine Content and Distribution in Human Platelet Fibrin Gels. Sci. Rep. 2018, 8, 10642. [Google Scholar] [CrossRef]
- Ravi, S.; Santhanakrishnan, M. Mechanical, chemical, structural analysis and comparative release of PDGF-AA from L-PRF, A-PRF and T-PRF—An in vitro study. Biomater. Res. 2020, 24, 16. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.C.; Kuo, T.F.; Yang, T.L.; Tsuang, Y.H.; Lin, M.F.; Chang, C.H.; Lin, Y.H.; Chan, W.P. Platelet-Rich Fibrin Facilitates Rabbit Meniscal Repair by Promoting Meniscocytes Proliferation, Migration, and Extracellular Matrix Synthesis. Int. J. Mol. Sci. 2017, 18, 1722. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.C.; Chen, C.H.; Chan, W.P.; Chiu, L.H.; Ho, W.P.; Hsieh, F.J.; Chen, Y.T.; Yang, T.L. Single-Stage Cartilage Repair Using Platelet-Rich Fibrin Scaffolds With Autologous Cartilaginous Grafts. Am. J. Sports Med. 2017, 45, 3128–3142. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.C.; Ou, K.L.; Lin, Y.H.; Lin, M.F.; Yang, T.L.; Chen, C.H.; Chan, W.P. Platelet-Rich Fibrin Facilitates One-Stage Cartilage Repair by Promoting Chondrocytes Viability, Migration, and Matrix Synthesis. Int. J. Mol. Sci. 2020, 21, 577. [Google Scholar] [CrossRef]
- Ghoneim, N.I.; Mansour, N.A.; Elmaghraby, S.A.; Abdelsameaa, S.E. Treatment of temporomandibular joint disc displacement using arthrocentesis combined with injectable platelet rich fibrin versus arthrocentesis alone. J. Dent. Sci. 2022, 17, 468–475. [Google Scholar] [CrossRef]
- Kütük, N.; Baş, B.; Soylu, E.; Gönen, Z.B.; Yilmaz, C.; Balcioğlu, E.; Özdamar, S.; Alkan, A. Effect of Platelet-Rich Plasma on Fibrocartilage, Cartilage, and Bone Repair in Temporomandibular Joint. J. Oral Maxillofac. Surg. 2014, 72, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Giacomello, M.; Mortellaro, C.; Viganoni, C.; Crimella, A.; Fossati, J.; Lauritano, D. PRGF® endoret injections for temporomandibular joint osteoarthritis treatment: A one-year follow-up. J. Biol. Regul. Homeost. Agents 2019, 33 (Suppl. S2), 215–222. [Google Scholar]
- Xie, A.; Nie, L.; Shen, G.; Cui, Z.; Xu, P.; Ge, H.; Tan, Q. The application of autologous platelet-rich plasma gel in cartilage regeneration. Mol. Med. Rep. 2014, 10, 1642–1648. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chien, C.-S.; Ho, H.-O.; Liang, Y.-C.; Ko, P.-H.; Sheu, M.-T.; Chen, C.-H. Incorporation of exudates of human platelet-rich fibrin gel in biodegradable fibrin scaffolds for tissue engineering of cartilage. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100B, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Taufik, S.A.; Dirja, B.T.; Utomo, D.N.; Usman, M.A.; Sakti, M.; Saleh, M.R.; Hatta, M.; Budu. Double membrane platelet-rich fibrin (PRF)—Synovium succeeds in regenerating cartilage defect at the knee: An experimental study on rabbit. Heliyon 2023, 9, e13139. [Google Scholar] [CrossRef] [PubMed]
- Smyth, N.A.; Murawski, C.D.; Fortier, L.A.; Cole, B.J.; Kennedy, J.G. Platelet-rich plasma in the pathologic processes of cartilage: Review of basic science evidence. Arthroscopy 2013, 29, 1399–1409. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Yuan, M.; Meng, H.Y.; Wang, A.Y.; Guo, Q.Y.; Wang, Y.; Peng, J. Basic science and clinical application of platelet-rich plasma for cartilage defects and osteoarthritis: A review. Osteoarthr. Cartil. 2013, 21, 1627–1637. [Google Scholar] [CrossRef] [PubMed]
- Mustafa Abd El, R.; Xuzhu, W.; Si, M.; Jihua, C.; Abdel Basit Mohamed, A.-A.; Mekkawy, M.N.H.; Shahram, G.; Joseph, C.; Elisa, C.; Yufeng, Z.; et al. Injectable-platelet rich fibrin using the low speed centrifugation concept improves cartilage regeneration when compared to platelet-rich plasma. Platelets 2019, 30, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, C.; Filardo, G.; Mariani, E.; Kon, E.; Marcacci, M.; Pereira Ruiz, M.T.; Facchini, A.; Grigolo, B. Comparison of Platelet-Rich Plasma Formulations for Cartilage Healing: An in Vitro Study. JBJS 2014, 96, 423–429. [Google Scholar] [CrossRef]
- Spreafico, A.; Chellini, F.; Frediani, B.; Bernardini, G.; Niccolini, S.; Serchi, T.; Collodel, G.; Paffetti, A.; Fossombroni, V.; Galeazzi, M.; et al. Biochemical investigation of the effects of human platelet releasates on human articular chondrocytes. J. Cell. Biochem. 2009, 108, 1153–1165. [Google Scholar] [CrossRef]
- Wang, M.; Gao, W. Fixation of platelet-rich plasma and fibrin gels on knee cartilage defects after microfracture with arthroscopy. Int. Orthop. 2022, 46, 1761–1766. [Google Scholar] [CrossRef]
- Raeissadat, S.A.; Rayegani, S.M.; Ahangar, A.G.; Abadi, P.H.; Mojgani, P.; Ahangar, O.G. Efficacy of intra-articular injection of a newly developed plasma rich in growth factor (PRGF) versus hyaluronic acid on pain and function of patients with knee osteoarthritis: A single-blinded randomized clinical trial. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2017, 10, 1179544117733452. [Google Scholar] [CrossRef]
- Bottegoni, C.; Dei Giudici, L.; Salvemini, S.; Chiurazzi, E.; Bencivenga, R.; Gigante, A. Homologous platelet-rich plasma for the treatment of knee osteoarthritis in selected elderly patients: An open-label, uncontrolled, pilot study. Ther. Adv. Musculoskelet. Dis. 2016, 8, 35–41. [Google Scholar] [CrossRef]
- Gobbi, A.; Lad, D.; Karnatzikos, G. The effects of repeated intra-articular PRP injections on clinical outcomes of early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 2170–2177. [Google Scholar] [CrossRef]
- Vaquerizo, V.; Plasencia, M.Á.; Arribas, I.; Seijas, R.; Padilla, S.; Orive, G.; Anitua, E. Comparison of intra-articular injections of plasma rich in growth factors (PRGF-Endoret) versus Durolane hyaluronic acid in the treatment of patients with symptomatic osteoarthritis: A randomized controlled trial. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1635–1643. [Google Scholar] [CrossRef]
- Cheeva-Akrapan, V.; Turajane, T. The 36-Month Survival Analysis of Conservative Treatment Using Platelet-Rich Plasma Enhanced With Injectable Platelet-Rich Fibrin in Patients With Knee Osteoarthritis. Cureus 2023, 15, e35632. [Google Scholar] [CrossRef] [PubMed]
- Andersson-Molina, H.; Karlsson, H.; Rockborn, P. Arthroscopic partial and total meniscectomy: A long-term follow-up study with matched controls. Arthroscopy 2002, 18, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Lindhorst, E.; Vail, T.P.; Guilak, F.; Wang, H.; Setton, L.A.; Vilim, V.; Kraus, V.B. Longitudinal characterization of synovial fluid biomarkers in the canine meniscectomy model of osteoarthritis. J. Orthop. Res. 2000, 18, 269–280. [Google Scholar] [CrossRef]
- Narita, A.; Takahara, M.; Sato, D.; Ogino, T.; Fukushima, S.; Kimura, Y.; Tabata, Y. Biodegradable gelatin hydrogels incorporating fibroblast growth factor 2 promote healing of horizontal tears in rabbit meniscus. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 255–263. [Google Scholar] [CrossRef]
- Shin, K.H.; Lee, H.; Kang, S.; Ko, Y.-J.; Lee, S.-Y.; Park, J.-H.; Bae, J.-H. Effect of Leukocyte-Rich and Platelet-Rich Plasma on Healing of a Horizontal Medial Meniscus Tear in a Rabbit Model. BioMed Res. Int. 2015, 2015, 179756. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.W.; Hadeed, M.M.; Werner, B.C.; Diduch, D.R.; Carson, E.W.; Miller, M.D. Platelet-rich Plasma in Meniscal Repair: Does Augmentation Improve Surgical Outcomes? Clin. Orthop. Relat. Res. 2015, 473, 1665–1672. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, D.; Akizuki, S.; Takizawa, T.; Omae, S.; Kato, H. Compact platelet-rich fibrin scaffold to improve healing of patellar tendon defects and for medial collateral ligament reconstruction. Knee 2013, 20, 545–550. [Google Scholar] [CrossRef]
- Weng, P.W.; Chen, C.H.; Lin, Y.C.; Chen, K.H.; Yeh, Y.Y.; Lai, J.M.; Chiang, C.J.; Wong, C.C. Platelet-Rich Fibrin-Augmented Gap-Bridging Strategy in Rabbit Anterior Cruciate Ligament Repair. Am. J. Sports Med. 2023, 51, 642–655. [Google Scholar] [CrossRef]
- Beyzadeoglu, T.; Pehlivanoglu, T.; Yildirim, K.; Buldu, H.; Tandogan, R.; Tuzun, U. Does the Application of Platelet-Rich Fibrin in Anterior Cruciate Ligament Reconstruction Enhance Graft Healing and Maturation? A Comparative MRI Study of 44 Cases. Orthop. J. Sports Med. 2020, 8, 2325967120902013. [Google Scholar] [CrossRef]
- Sánchez, M.; Anitua, E.; Azofra, J.; Prado, R.; Muruzabal, F.; Andia, I. Ligamentization of tendon grafts treated with an endogenous preparation rich in growth factors: Gross morphology and histology. Arthroscopy 2010, 26, 470–480. [Google Scholar] [CrossRef]
- Eggli, S.; Kohlhof, H.; Zumstein, M.; Henle, P.; Hartel, M.; Evangelopoulos, D.S.; Bonel, H.; Kohl, S. Dynamic intraligamentary stabilization: Novel technique for preserving the ruptured ACL. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1215–1221. [Google Scholar] [CrossRef]
- Hurley, E.T.; Lim Fat, D.; Moran, C.J.; Mullett, H. The efficacy of platelet-rich plasma and platelet-rich fibrin in arthroscopic rotator cuff repair: A meta-analysis of randomized controlled trials. Am. J. Sports Med. 2019, 47, 753–761. [Google Scholar] [CrossRef]
- Han, C.; Na, Y.; Zhu, Y.; Kong, L.; Eerdun, T.; Yang, X.; Ren, Y. Is platelet-rich plasma an ideal biomaterial for arthroscopic rotator cuff repair? A systematic review and meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2019, 14, 183. [Google Scholar] [CrossRef]
- Liu, C.-J.; Yu, K.-L.; Bai, J.-B.; Tian, D.-H.; Liu, G.-L. Platelet-rich plasma injection for the treatment of chronic Achilles tendinopathy: A meta-analysis. Medicine 2019, 98, e15278. [Google Scholar] [CrossRef] [PubMed]
- Grassi, A.; Napoli, F.; Romandini, I.; Samuelsson, K.; Zaffagnini, S.; Candrian, C.; Filardo, G. Is platelet-rich plasma (PRP) effective in the treatment of acute muscle injuries? A systematic review and meta-analysis. Sports Med. 2018, 48, 971–989. [Google Scholar] [CrossRef] [PubMed]
- Maisel-Campbell, A.L.; Ismail, A.; Reynolds, K.A.; Poon, E.; Serrano, L.; Grushchak, S.; Farid, C.; West, D.P.; Alam, M. A systematic review of the safety and effectiveness of platelet-rich plasma (PRP) for skin aging. Arch. Dermatol. Res. 2019, 312, 301–315. [Google Scholar] [CrossRef] [PubMed]
- Marchitto, M.C.; Qureshi, A.; Marks, D.; Awosika, O.; Rengifo-Pardo, M.; Ehrlich, A. Emerging Nonsteroid-Based Procedural Therapies for Alopecia Areata: A Systematic Review. Dermatol. Surg. 2019, 45, 1484–1506. [Google Scholar] [CrossRef]
- Schiavone, G.; Paradisi, A.; Ricci, F.; Abeni, D. Injectable platelet-, leukocyte-, and fibrin-rich plasma (iL-PRF) in the management of androgenetic alopecia. Dermatol. Surg. 2018, 44, 1183–1190. [Google Scholar] [CrossRef]
- Mao, G.; Zhang, G.; Fan, W. Platelet-Rich Plasma for Treating Androgenic Alopecia: A Systematic Review. Aesthetic Plast. Surg. 2019, 43, 1326–1336. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Wolford, L.M.; Ellis III, E.; Neff, A. The Hierarchy of Different Treatments for Arthrogenous Temporomandibular Disorders: A Network Meta-Analysis of Randomized Clinical Trials. J. Cranio-Maxillofac. Surg. 2019, 48, 9–23. [Google Scholar] [CrossRef]
- Catapano, M.; Catapano, J.; Borschel, G.; Alavania, S.M.; Robinson, L.R.; Mittal, N. Effectiveness of platelet rich plasma injections for non-surgical management of carpal tunnel syndrome: A systematic review and meta-analysis of randomized controlled trials. Arch. Phys. Med. Rehabil. 2019, 101, 897–906. [Google Scholar] [CrossRef]
- Hu, Z.; Qu, S.; Zhang, J.; Cao, X.; Wang, P.; Huang, S.; Shi, F.; Dong, Y.; Wu, J.; Tang, B. Efficacy and Safety of Platelet-Rich Plasma for Patients with Diabetic Ulcers: A Systematic Review and Meta-analysis. Adv. Wound Care 2019, 8, 298–308. [Google Scholar] [CrossRef]
- Li, A.; Wang, H.; Yu, Z.; Zhang, G.; Feng, S.; Liu, L.; Gao, Y. Platelet-rich plasma vs corticosteroids for elbow epicondylitis: A systematic review and meta-analysis. Medicine 2019, 98, e18358. [Google Scholar] [CrossRef] [PubMed]
- Houck, D.A.; Kraeutler, M.J.; Thornton, L.B.; McCarty, E.C.; Bravman, J.T. Treatment of lateral epicondylitis with autologous blood, platelet-rich plasma, or corticosteroid injections: A systematic review of overlapping meta-analyses. Orthop. J. Sports Med. 2019, 7, 2325967119831052. [Google Scholar] [CrossRef]
- Thompson, G.; Pearson, J.F. No attributable effects of PRP on greater trochanteric pain syndrome. N. Z. Med. J. 2019, 54, 22–32. [Google Scholar]
- Fitzpatrick, J.; Bulsara, M.K.; O’Donnell, J.; McCrory, P.R.; Zheng, M.H. The effectiveness of platelet-rich plasma injections in gluteal tendinopathy: A randomized, double-blind controlled trial comparing a single platelet-rich plasma injection with a single corticosteroid injection. Am. J. Sports Med. 2018, 46, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Charlesworth, J.; Fitzpatrick, J.; Perera, N.K.P.; Orchard, J. Osteoarthritis-a systematic review of long-term safety implications for osteoarthritis of the knee. BMC Musculoskelet. Disord. 2019, 20, 151. [Google Scholar] [CrossRef]
- Canellas, J.d.S.; Ritto, F.; Medeiros, P. Evaluation of postoperative complications after mandibular third molar surgery with the use of platelet-rich fibrin: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1138–1146. [Google Scholar] [CrossRef]
- Ortega-Mejia, H.; Estrugo-Devesa, A.; Saka-Herrán, C.; Ayuso-Montero, R.; López-López, J.; Velasco-Ortega, E. Platelet-Rich Plasma in Maxillary Sinus Augmentation: Systematic Review. Materials 2020, 13, 622. [Google Scholar] [CrossRef]
- Fortunato, L.; Bennardo, F.; Buffone, C.; Giudice, A. Is the application of platelet concentrates effective in the prevention and treatment of Medication-Related Osteonecrosis of the Jaw? A systematic review. J. Cranio-Maxillofac. Surg. 2020, 48, 268–285. [Google Scholar] [CrossRef] [PubMed]
- Andriolo, L.; Altamura, S.A.; Reale, D.; Candrian, C.; Zaffagnini, S.; Filardo, G. Nonsurgical treatments of patellar tendinopathy: Multiple injections of platelet-rich plasma are a suitable option: A systematic review and meta-analysis. Am. J. Sports Med. 2019, 47, 1001–1018. [Google Scholar] [CrossRef]
- Vander Doelen, T.; Jelley, W. Non-surgical treatment of patellar tendinopathy: A systematic review of randomized controlled trials. J. Sci. Med. Sport 2019, 23, 118–124. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Wu, Y.-C.; Tu, Y.-K.; Cheng, J.-W.; Tsai, W.-C.; Yu, T.-Y. Autologous Blood-Derived Products Compared With Corticosteroids for Treatment of Plantar Fasciopathy: A Systematic Review and Meta-Analysis. Am. J. Phys. Med. Rehabil. 2019, 98, 343–352. [Google Scholar] [CrossRef]
- Balli, G.; Ioannou, A.; Powell, C.A.; Angelov, N.; Romanos, G.E.; Soldatos, N. Ridge Preservation Procedures after Tooth Extractions: A Systematic Review. Int. J. Dent. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zumstein, M.A.; Rumian, A.; Thélu, C.É.; Lesbats, V.; O’Shea, K.; Schaer, M.; Boileau, P. SECEC Research Grant 2008 II: Use of platelet-and leucocyte-rich fibrin (L-PRF) does not affect late rotator cuff tendon healing: A prospective randomized controlled study. J. Shoulder Elb. Surg. 2016, 25, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Mariani, E.; Pulsatelli, L. Platelet concentrates in musculoskeletal medicine. Int. J. Mol. Sci. 2020, 21, 1328. [Google Scholar] [CrossRef]
- El Bagdadi, K.; Kubesch, A.; Yu, X.; Al-Maawi, S.; Orlowska, A.; Dias, A.; Booms, P.; Dohle, E.; Sader, R.; Kirkpatrick, C. Reduction of relative centrifugal forces increases growth factor release within solid platelet-rich-fibrin (PRF)-based matrices: A proof of concept of LSCC (low speed centrifugation concept). Eur. J. Trauma Emerg. Surg. 2017, 45, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Fadadu, P.P.; Mazzola, A.J.; Hunter, C.W.; Davis, T.T. Review of concentration yields in commercially available platelet-rich plasma (PRP) systems: A call for PRP standardization. Reg. Anesth. Pain Med. 2019, 44, 652–659. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Advantages of Platelet-Rich Fibrin | References |
|---|---|
| Preparation and application are easy and efficient | [46,47,48] |
| Natural biomaterial, obtained by autologous blood sample. No risk of infection, immune rejection, or a reaction | [5,47] |
| Does not require bovine thrombin and anticoagulants | [24,49] |
| Fibrin’s three-dimensional architecture with growth factors is better suited for tissue regeneration | [50] |
| It can increase the healing rate | [51,52] |
| Decreased patient bleeding, discomfort, and pain after surgery | [47] |
| Disadvantages of Platelet-Rich Fibrin | |
| Autologous blood means the final amount is limited | [53] |
| Short handling time and fast degradation | [40] |
| Type | Process | Concentration | Fibrin | Safety and Risk | |||||
|---|---|---|---|---|---|---|---|---|---|
| Name | Blood Source | Time | Cost | Platelet | Leukocyte | Density | Cross-Infection | Immune Rejection | |
| Fibrin Glue | Tisseel | Commercial | Very Long | High | None | None | High | High | High |
| PPP | Autologous | Very Long | Very High | None | None | Low | Low | Low | |
| PRP | L-PRP | Autologous | Long | High | Low | High | Low | Low | Low |
| P-PRP | Autologous | Long | High | High | None | Low | Low | Low | |
| PRF | L-PRF | Autologous | Short | Very Low | High | Very High | High | None | None |
| Indication or Procedure | PRP | PRF |
|---|---|---|
| Achilles tendinopathy | PRP is not superior to placebo treatment [105] | |
| Acute muscle injuries | Abundance of high-quality evidence [106] | |
| Aging skin | Temporarily induce modest improvement in facial skin appearance, texture, and lines [107] | |
| Alopecia areata | Abundance of high-quality evidence [108] | Leukocyte PRF is superior to control treatment [109] |
| Androgenic alopecia | PRP is likely to reduce hair loss, increase hair diameter and density [110] | |
| Arthrogenous temporomandibular disorders | PRP is more effective than conservative treatments [111] | |
| Carpal tunnel syndrome | PRP represents a promising therapy for patients with mild to moderate CTS [112] | |
| Diabetic ulcers | PRP may improve ulcer healing [113] | |
| Elbow tendinopathy | PRP injections improved pain and function more effectively than corticosteroid injections at the long-term follow-up [114] PRP significantly improved pain and elbow function in the intermediate term (12–26 weeks) [115] | |
| Greater trochanteric pain syndrome | PRP is not superior to placebo treatment [116] A single PRP injection is superior to a single corticosteroid injection [117] | |
| Knee osteoarthritis | PRP injections have a low risk of harm and beneficial ≥12 month outcomes [118] | |
| Mandibular third molar surgery | Decrease in prevalence of alveolar osteitis [119] | |
| Maxillary sinus augmentation | Improves the healing period and bone formation [120] | |
| Medication-related osteonecrosis of the jaw | Abundance of high-quality evidence [121] | Abundance of high-quality evidence [121] |
| Patellar tendinopathy | Multiple injections of PRP obtained positive outcome [122] Pain relieving and functional improvement [123] | |
| Plantar fasciopathy | PRP may provide a long-term effect in relieving pain [124] | |
| Ridge preservation procedure | L-PRF reduced the magnitude of vertical and horizontal bone resorption [125] | |
| Rotator cuff tears | PRP treatment decreases the retear rate and improves the clinical outcomes [104] PRP improves patient outcomes [103] | L-PRF yields no beneficial effect in clinical outcome [126] PRF has no benefit in improving patient outcomes [103] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, M.-Y.; Vy, V.P.T.; Tang, S.-L.; Hung, T.N.K.; Wang, C.-W.; Liang, J.-Y.; Wong, C.-C.; Chan, W.P. Current Progress of Platelet-Rich Derivatives in Cartilage and Joint Repairs. Int. J. Mol. Sci. 2023, 24, 12608. https://doi.org/10.3390/ijms241612608
Bai M-Y, Vy VPT, Tang S-L, Hung TNK, Wang C-W, Liang J-Y, Wong C-C, Chan WP. Current Progress of Platelet-Rich Derivatives in Cartilage and Joint Repairs. International Journal of Molecular Sciences. 2023; 24(16):12608. https://doi.org/10.3390/ijms241612608
Chicago/Turabian StyleBai, Meng-Yi, Vu Pham Thao Vy, Sung-Ling Tang, Truong Nguyen Khanh Hung, Ching-Wei Wang, Jui-Yuan Liang, Chin-Chean Wong, and Wing P. Chan. 2023. "Current Progress of Platelet-Rich Derivatives in Cartilage and Joint Repairs" International Journal of Molecular Sciences 24, no. 16: 12608. https://doi.org/10.3390/ijms241612608
APA StyleBai, M.-Y., Vy, V. P. T., Tang, S.-L., Hung, T. N. K., Wang, C.-W., Liang, J.-Y., Wong, C.-C., & Chan, W. P. (2023). Current Progress of Platelet-Rich Derivatives in Cartilage and Joint Repairs. International Journal of Molecular Sciences, 24(16), 12608. https://doi.org/10.3390/ijms241612608