
Axitinib Rechallenge Restores the Anticancer Effect after Nivolumab: A Case Report

 , , and
, , and
Abstract
1. Introduction
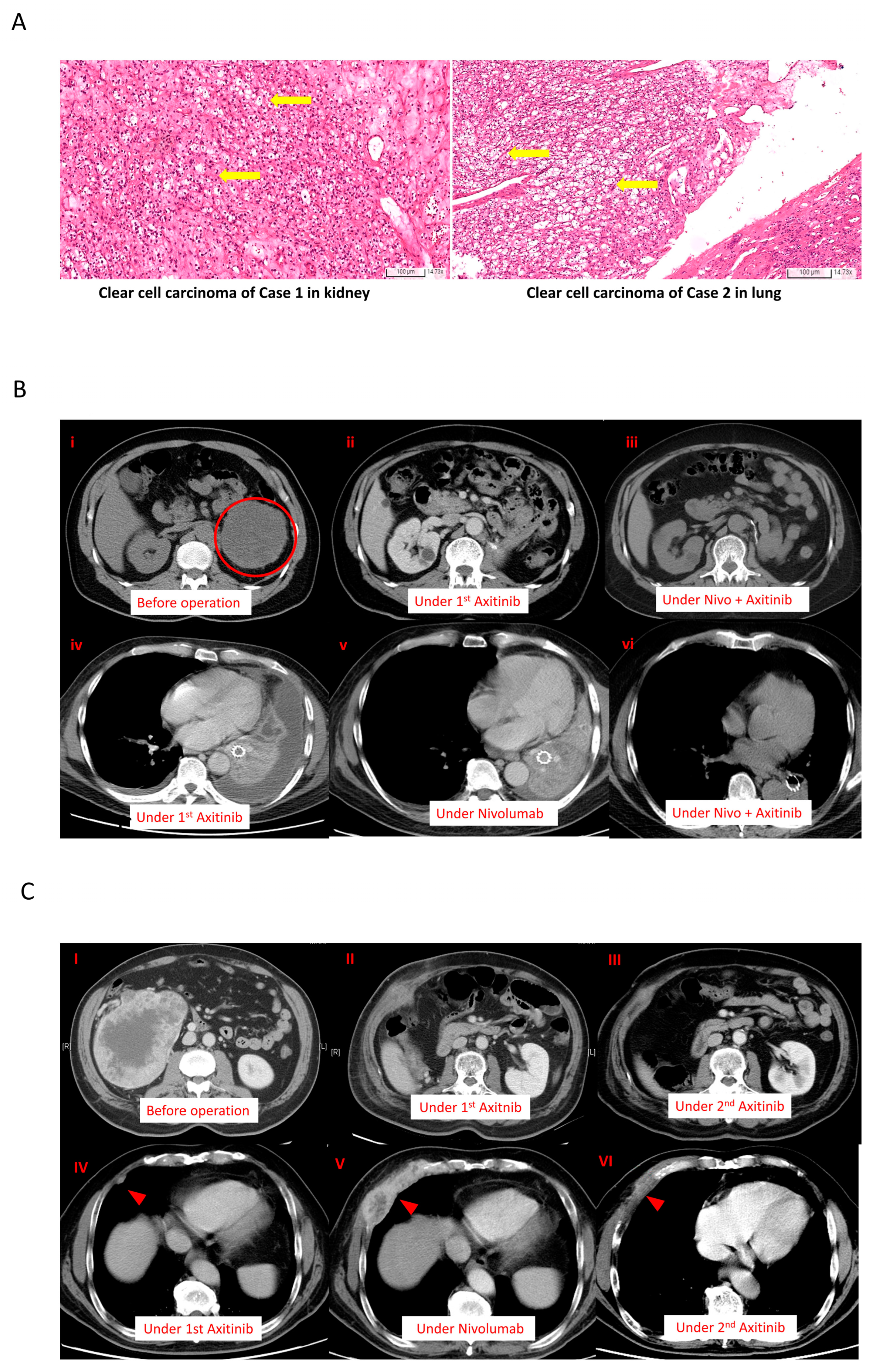
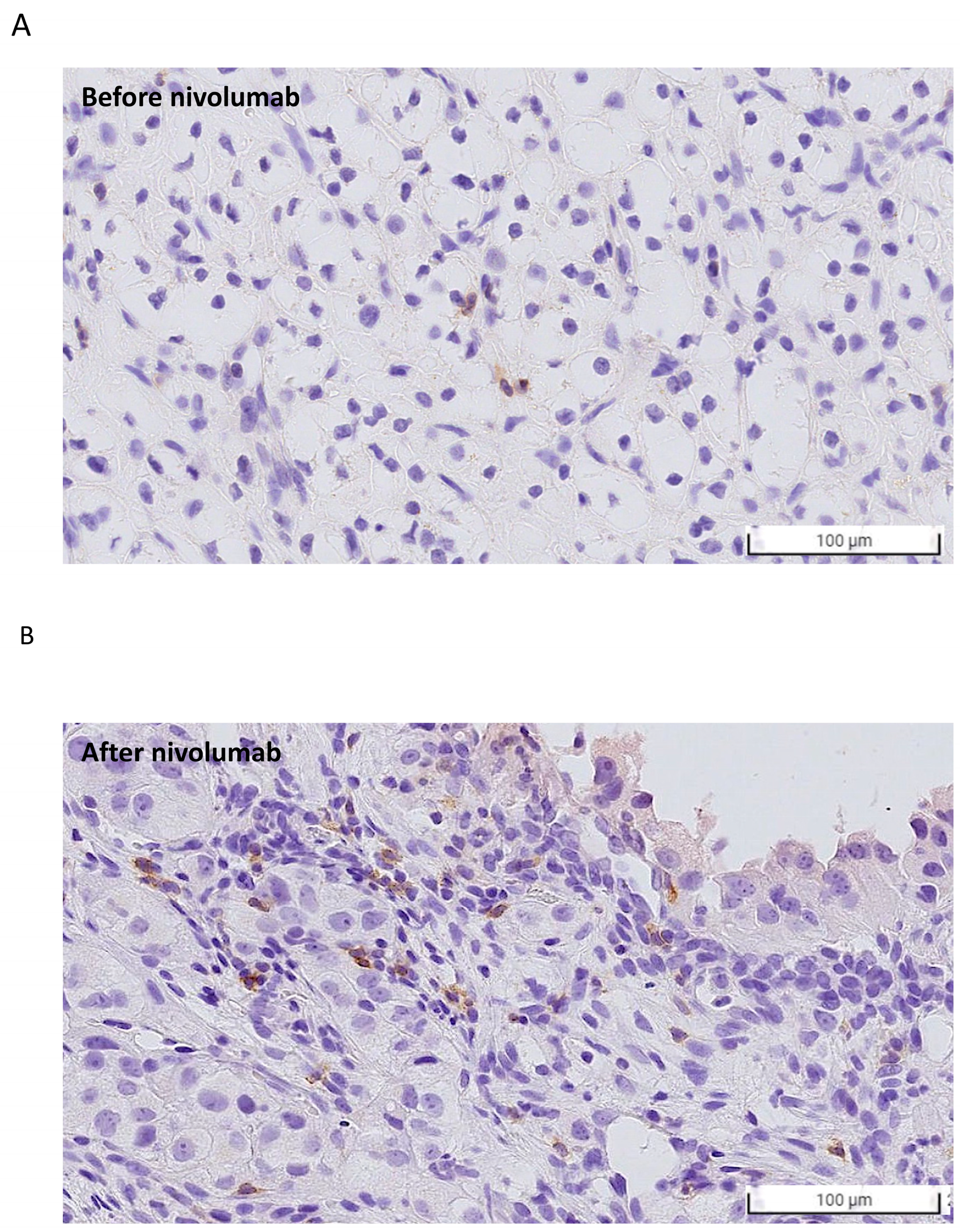
2. Case Description
3. Discussion
4. Conclusions
5. Method
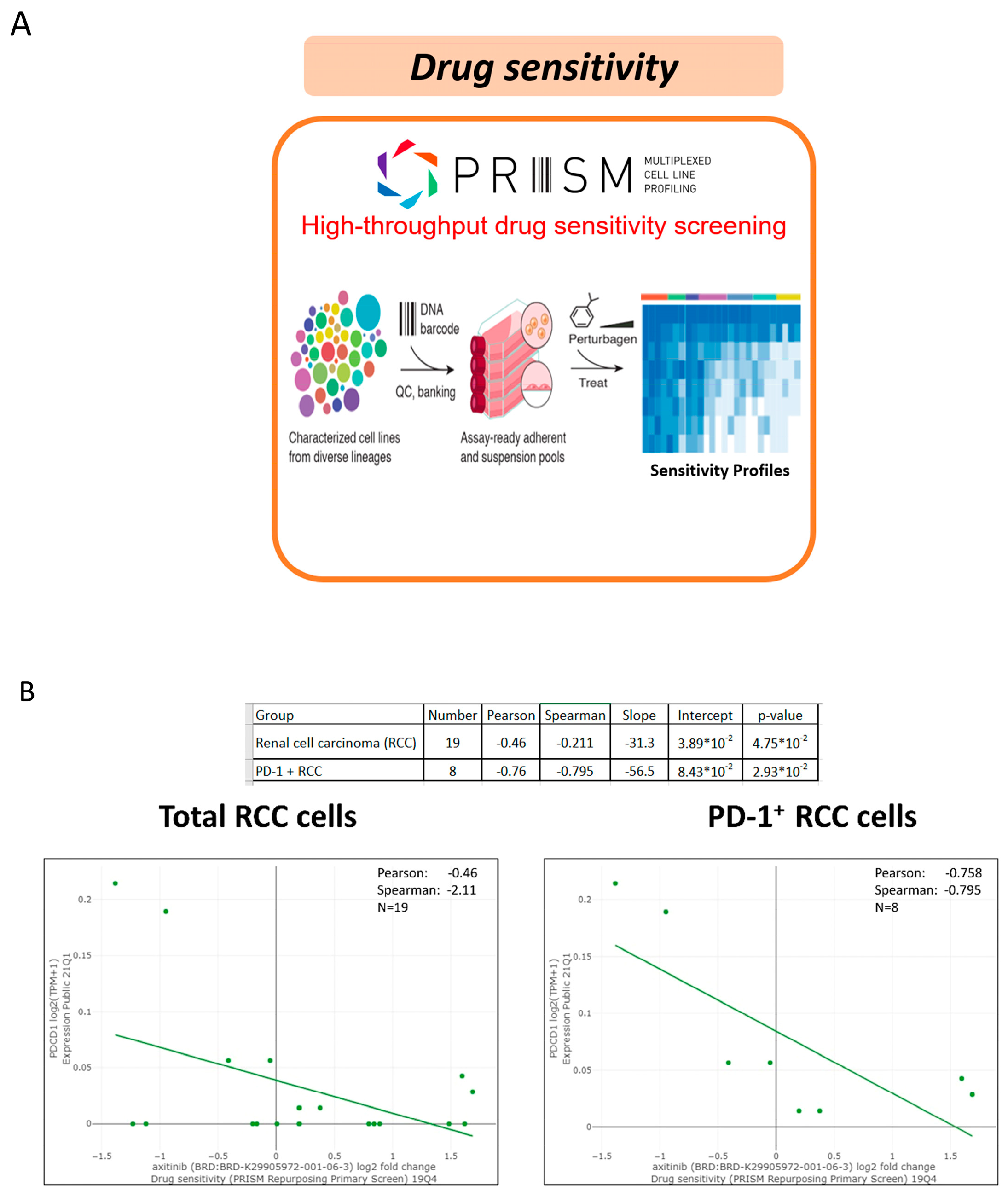
5.1. PRISM Method
5.2. Lymphocyte Activation Test
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Motzer, R.J.; Jonasch, E.; Boyle, S.; Carlo, M.I.; Manley, B.; Agarwal, N.; Alva, A.; Beckermann, K.; Choueiri, T.K.; Costello, B.A.; et al. NCCN Guidelines Insights: Kidney Cancer, Version 1.2021. J. Natl. Compr. Cancer Netw. 2020, 18, 1160–1170. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Plimack, E.R.; Soulières, D.; Waddell, T.; Stus, V.; Gafanov, R.; Nosov, D.; Pouliot, F.; Melichar, B.; Vynnychenko, I.; et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Shah, A.Y.; Rasco, D.; Rao, A.; Taylor, M.H.; Di Simone, C.; Hsieh, J.J.; Pinto, A.; Shaffer, D.R.; Sarrio, R.G.; et al. Lenvatinib plus pembrolizumab in patients with either treatment-naive or previously treated metastatic renal cell carcinoma (Study 111/KEYNOTE-146): A phase 1b/2 study. Lancet Oncol. 2021, 22, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Psutka, S.P.; Parikh, A.B.; Li, M.; Collier, K.; Miah, A.; Mori, S.V.; Hinkley, M.; Tykodi, S.S.; Hall, E.; et al. Combining immune checkpoint inhibition plus tyrosine kinase inhibition as first and subsequent treatments for metastatic renal cell carcinoma. Cancer Med. 2022, 11, 3106–3114. [Google Scholar] [CrossRef] [PubMed]
- Yasuoka, S.; Yuasa, T.; Fujiwara, R.; Komai, Y.; Numao, N.; Yamamoto, S.; Kondo, Y.; Yonese, J. Efficacy and Safety of Axitinib Therapy After Nivolumab for Patients with Metastatic Renal Cell Cancer. Anticancer. Res. 2020, 40, 6493–6497. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Hara, T.; Terakawa, T.; Harada, K.; Fujisawa, M. Efficacy of axitinib rechallenge in metastatic renal cell carcinoma. Int. J. Urol. 2021, 28, 702–703. [Google Scholar] [CrossRef] [PubMed]
- Azuma, T.; Sugihara, T.; Honda, S.; Yoshizaki, U.; Niimi, F.; Tsuru, I.; Kume, H. Metastatic renal cell carcinoma regains sensitivity to tyrosine kinase inhibitor after nivolumab treatment: A case report. Oncol. Lett. 2019, 17, 4011–4015. [Google Scholar] [CrossRef] [PubMed]
- Vano, Y.A.; Elaidi, R.; Bennamoun, M.; Chevreau, C.; Borchiellini, D.; Pannier, D.; Maillet, D.; Gross-Goupil, M.; Tournigand, C.; Laguerre, B.; et al. Nivolumab, nivolumab-ipilimumab, and VEGFR-tyrosine kinase inhibitors as first-line treatment for metastatic clear-cell renal cell carcinoma (BIONIKK): A biomarker-driven, open-label, non-comparative, randomised, phase 2 trial. Lancet Oncol. 2022, 23, 612–624. [Google Scholar] [CrossRef] [PubMed]
- Corsello, S.M.; Nagari, R.T.; Spangler, R.D.; Rossen, J.; Kocak, M.; Bryan, J.G.; Humeidi, R.; Peck, D.; Wu, X.; Tang, A.A.; et al. Discovering the anticancer potential of non-oncology drugs by systematic viability profiling. Nat. Cancer 2020, 1, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Mannan, A.M.; Yvone, G.M.; Ross, K.N.; Zhang, Y.L.; Marton, M.A.; Taylor, B.R.; Crenshaw, A.; Gould, J.Z.; Tamayo, P.; et al. High-throughput identification of genotype-specific cancer vulnerabilities in mixtures of barcoded tumor cell lines. Nat. Biotechnol. 2016, 34, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Sarkis, J.; Assaf, J.; Alkassis, M. Biomarkers in renal cell carcinoma: Towards a more selective immune checkpoint inhibition. Transl. Oncol. 2021, 14, 101071. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, A.; Sepe, P.; Zattarin, E.; Mennitto, A.; Stellato, M.; Claps, M.; Guadalupi, V.; Verzoni, E.; De Braud, F.; Procopio, G. Predictive Biomarkers of Response to Immunotherapy in Metastatic Renal Cell Cancer. Front. Oncol. 2020, 10, 1644. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, A.; Solimando, A.G.; Kerscher, A.; Bittrich, M.; Kalogirou, C.; Kübler, H.; Rosenwald, A.; Bargou, R.; Kollmannsberger, P.; Schilling, B.; et al. SubgroupIndependent Mapping of Renal Cell Carcinoma-Machine Learning Reveals Prognostic Mitochondrial Gene Signature Beyond Histopathologic Boundaries. Front. Oncol. 2021, 11, 621278. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.A.; Sznol, M. Resistance mechanisms to checkpoint inhibitors. Curr. Opin. Immunol. 2021, 69, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yang, X.; Zhang, C.; Wang, Y.; Cheng, T.; Duan, L.; Tong, Z.; Tan, S.; Zhang, H.; Saw, P.E.; et al. Tumor cell-intrinsic PD-1 receptor is a tumor suppressor and mediates resistance to PD-1 blockade therapy. Proc. Natl. Acad. Sci. USA 2020, 117, 6640–6650. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.H.; Hung, S.I.; Yang, J.Y.; Su, S.C.; Huang, S.P.; Wei, C.Y.; Chin, S.W.; Chiou, C.C.; Chu, S.C.; Ho, H.C.; et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat. Med. 2008, 14, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Huang, H.; Li, T.; Gao, Q.; Song, Y.; Wang, Z. Axitinib Reverses Resistance to AntiProgrammed Cell Death-1 Therapy in a Patient with Renal Cell Carcinoma. Front. Immunol. 2021, 12, 728750. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 20190829 (Nivolumab Only, After Starting Treatment One Month) | ||
| Granzyme B | ||
| Drug | (pg/mL) | fold |
| PBS | 203.0 | 1.00 |
| Nivolumab | 408.8 | 2.01 |
| Ipilimumab | 219.2 | 1.08 |
| Pembrolizumab | 554.0 | 2.73 |
| PHA | 11,686.4 | 57.57 |
| 20200313 (Nivolumab and 2.5 mg Axitinib) | ||
| PBS | 102.5 | 1.00 |
| Nivolumab | 362.8 | 3.54 * |
| PHA | 20,368.0 | 198.79 |
| Study Type | Title | Efficacy | Compared with Our Cases | Reference |
|---|---|---|---|---|
| Case series | Efficacy of Axitinib After Nivolumab Failure in Metastatic Renal Cell Carcinoma (2020) | Efficacy of axitinib as a third-line therapy after the failure of a first-line VEGFR-TKI and a second-line nivolumab monotherapy for mRCC. The median PFS was 12.8 months, and the 1-year and OS rate was 71.6% | Similarities: The efficacy of axitinib after nivolumab would be better Differences: We focus on the efficacy of axitinib rechallenge after nivolumab | [6] |
| Case series | Efficacy of axitinib rechallenge in metastatic renal cell carcinoma (2021) | PFS in axitinib rechallenge: 3.3 months (95% CI 6.9–not reached_ OS in axitinib rechallenge: 21.8 months (95% CI 6.9–not reached | Similarities: The efficacy of the axitinib rechallenge was revealed in this study. The PFS is only 3.3 months Differences: We focus on the specific timing (after nivolumab) | [7] |
| Case report | Axitinib Reverses Resistance to Anti-Programmed Cell Death-1 Therapy in a Patient With Renal Cell Carcinoma (2022) | Axitinib successfully reversed primary resistance to anti-PD-1 therapy in a patient with RCC | Similarities: Axinitib can reverse the primary opposition to anti-PD-1 treatment Differences: In this study, anti-PD-1 treatment is the first line setting. | [8] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.-S.; Chang, P.-H.; Wang, D.-H.; Chen, C.-B.; Huang, C.-Y.F. Axitinib Rechallenge Restores the Anticancer Effect after Nivolumab: A Case Report. Int. J. Mol. Sci. 2023, 24, 12149. https://doi.org/10.3390/ijms241512149
Chang Y-S, Chang P-H, Wang D-H, Chen C-B, Huang C-YF. Axitinib Rechallenge Restores the Anticancer Effect after Nivolumab: A Case Report. International Journal of Molecular Sciences. 2023; 24(15):12149. https://doi.org/10.3390/ijms241512149
Chicago/Turabian StyleChang, Yueh-Shih, Pei-Hung Chang, Deng-Huang Wang, Chun-Bing Chen, and Chi-Ying F. Huang. 2023. "Axitinib Rechallenge Restores the Anticancer Effect after Nivolumab: A Case Report" International Journal of Molecular Sciences 24, no. 15: 12149. https://doi.org/10.3390/ijms241512149
APA StyleChang, Y.-S., Chang, P.-H., Wang, D.-H., Chen, C.-B., & Huang, C.-Y. F. (2023). Axitinib Rechallenge Restores the Anticancer Effect after Nivolumab: A Case Report. International Journal of Molecular Sciences, 24(15), 12149. https://doi.org/10.3390/ijms241512149