

Correlation between the Serum Concentration of Vitamin A and Disease Severity in Patients Carrying p.G90D in RHO, the Most Frequent Gene Associated with Dominant Retinitis Pigmentosa: Implications for Therapy with Vitamin A


 ,
,
Abstract
1. Introduction
2. Results
2.1. Correlation between Serum Vitamin A Concentration and Age
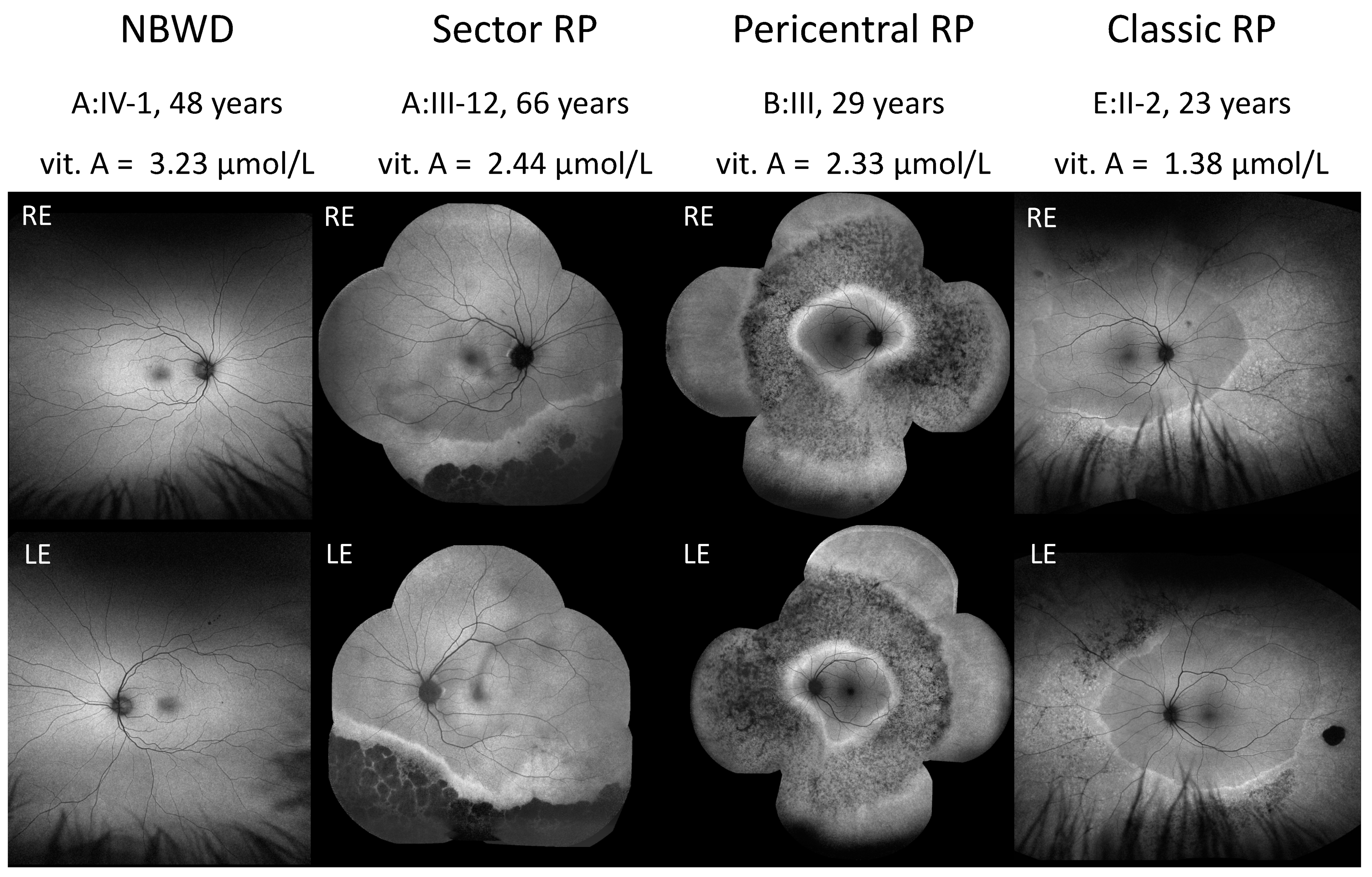
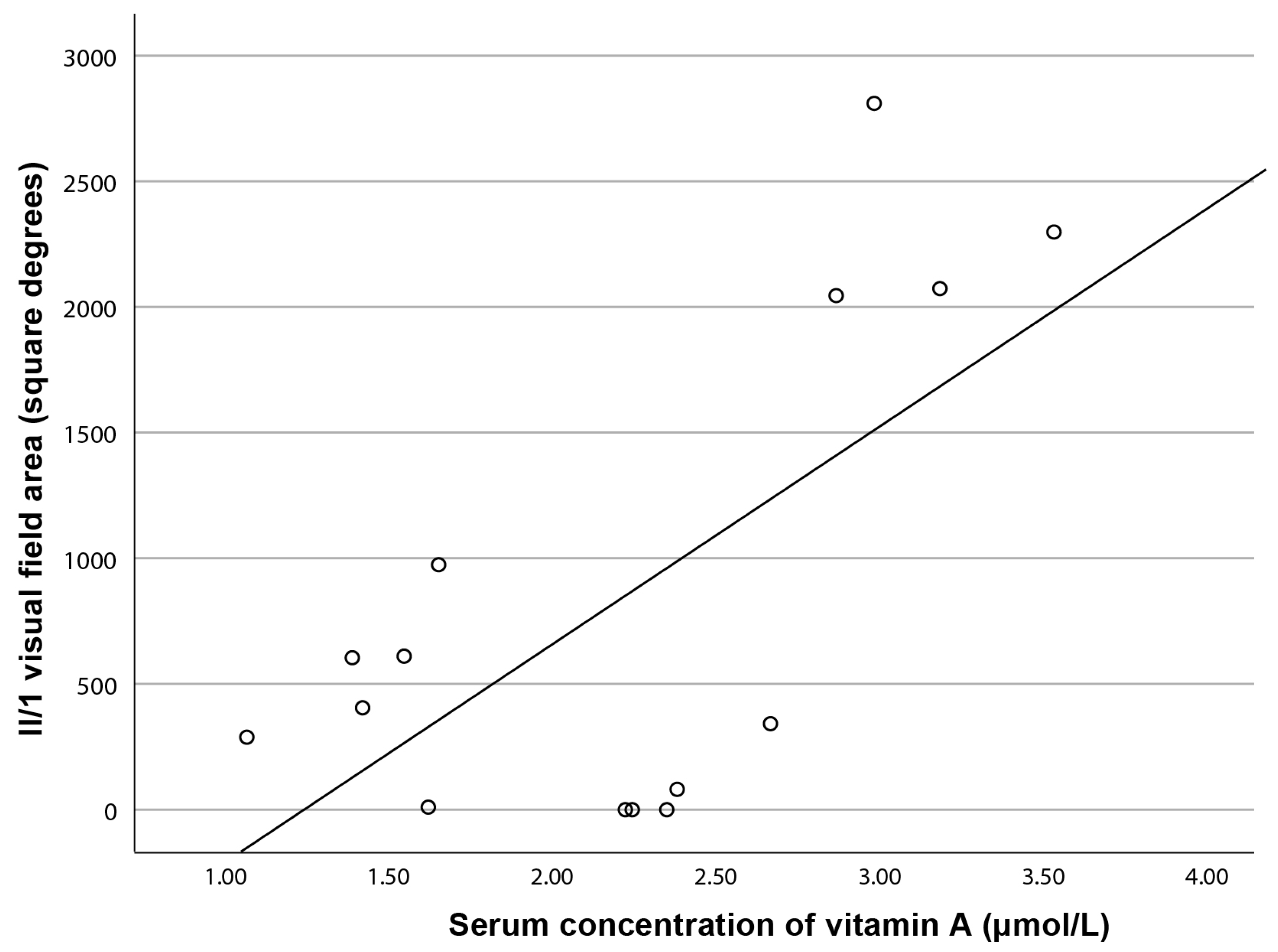
2.2. Correlation between Serum Vitamin A Concentration and Phenotype
3. Discussion
3.1. Correlation between Serum Concentration of Vitamin A and Age
3.2. Correlation between Serum Concentration of Vitamin A and Phenotype
3.3. The Use of Vitamin A as a Treatment Strategy
3.4. Possible Role of Vitamin A in Retinal Degeneration in RHO p.G90D Carriers
4. Materials and Methods
4.1. Patients
4.2. Genetic and Bioinformatic Analysis
4.3. Clinical Examination
4.4. Phenotype Classification
4.5. Measurement of Serum Vitamin A Concentration
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RHO | Rhodopsin gene |
| RP | Retinitis pigmentosa |
| NBWD | Night blindness without degeneration |
| CSNB | Congenital stationary night blindness |
| GCPR | G-protein coupled receptor |
| FAF | Fundus autofluorscence imaging |
| RE | Right eye |
| LE | Left eye |
| ERG | Electroretinography |
| RPE | Retinal pigment epithelium |
| RBP | Retinal binding protein |
| STRA6 | Retinoic acid 6 |
| CRBP1 | Cellular retinol -binding protein 1 |
| LRAT | Retinol:lecithin acyltransferase |
| RPE65 | Retinoid isomerohydrolase |
| CRALBP | Cellular retinaldehyde-binding protein |
| IRBP | Interphotoreceptor retinoid-binding protein |
| IU | International Unit |
| WT | Wild-type |
| DNA | Deoxyribonucleic acid |
| BWA | Burrows-Wheeler aligner |
| GATK | Genome analysis toolkit |
| CONIFER | Copy number inference from exome reads |
| GnomAD | Genome aggregation database |
| ACMG/AMP | American College of Medical Genetics and Genomics/Association for Molecular Pathology |
| OCT | Optical coherence tomography |
| DA | Dark adapted |
| LA | Light adapted |
| HPLC | High-performance liquid chromatography |
References
- Verbakel, S.K.; van Huet, R.A.C.; Boon, C.J.F.; den Hollander, A.I.; Collin, R.W.J.; Klaver, C.C.W.; Hoyng, C.B.; Roepman, R.; Klevering, B.J. Non-syndromic retinitis pigmentosa. Prog. Retin. Eye Res. 2018, 66, 157–186. [Google Scholar] [CrossRef]
- Russell, S.; Bennett, J.; Wellman, J.A.; Chung, D.C.; Yu, Z.-F.; Tillman, A.; Wittes, J.; Pappas, J.; Elci, O.; McCague, S.; et al. Efficacy and safety of voretigene neparvovec (AAV2-hRPE65v2) in patients with RPE65-mediated inherited retinal dystrophy: A randomised, controlled, open-label, phase 3 trial. Lancet 2017, 390, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Berson, E.L.; Rosner, B.; Sandberg, M.A.; Hayes, K.C.; Nicholson, B.W.; Weigel-DiFranco, C.; Willett, W. A randomized trial of vitamin A and vitamin E supplementation for retinitis pigmentosa. Arch. Ophthalmol. 1993, 111, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Berson, E.L.; Rosner, B.; Sandberg, M.A.; Weigel-DiFranco, C.; Moser, A.; Brockhurst, R.J.; Hayes, K.C.; Johnson, C.A.; Anderson, E.J.; Gaudio, A.R.; et al. Clinical trial of docosahexaenoic acid in patients with retinitis pigmentosa receiving vitamin A treatment. Arch. Ophthalmol. 2004, 122, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- Berson, E.L.; Rosner, B.; Sandberg, M.A.; Weigel-DiFranco, C.; Brockhurst, R.J.; Hayes, K.C.; Johnson, E.J.; Anderson, E.J.; Johnson, C.A.; Gaudio, A.R.; et al. Clinical trial of lutein in patients with retinitis pigmentosa receiving vitamin A. Arch. Ophthalmol. 2010, 128, 403–411. [Google Scholar] [CrossRef]
- Berson, E.L.; Rosner, B.; Sandberg, M.A.; Weigel-DiFranco, C.; Willett, W.C. ω-3 intake and visual acuity in patients with retinitis pigmentosa receiving vitamin A. Arch. Ophthalmol. 2012, 130, 707–711. [Google Scholar] [CrossRef]
- Berson, E.L.; Weigel-DiFranco, C.; Rosner, B.; Gaudio, A.R.; Sandberg, M.A. Association of Vitamin A Supplementation With Disease Course in Children With Retinitis Pigmentosa. JAMA Ophthalmol. 2018, 136, 490–495. [Google Scholar] [CrossRef]
- Schwartz, S.G.; Wang, X.; Chavis, P.; Kuriyan, A.E.; Abariga, S.A. Vitamin A and fish oils for preventing the progression of retinitis pigmentosa. Cochrane Database Syst. Rev. 2020, 6, CD008428. [Google Scholar] [CrossRef]
- Naash, M.I.; Wu, T.; Chakraborty, D.; Fliesler, S.J.; Ding, X.; Nour, M.; Peachey, N.S.; Lem, J.; Qtaishat, N.; Al-Ubaidi, M.R.; et al. Retinal abnormalities associated with the G90D mutation in opsin. J. Comp. Neurol. 2004, 478, 149–163. [Google Scholar] [CrossRef]
- Kawamura, S.; Colozo, A.T.; Ge, L.; Muller, D.J.; Park, P.S.-H. Structural, energetic, and mechanical perturbations in rhodopsin mutant that causes congenital stationary night blindness. J. Biol. Chem. 2012, 287, 21826–21835. [Google Scholar] [CrossRef]
- McAlear, S.D.; Kraft, T.W.; Gross, A.K. 1 rhodopsin mutations in congenital night blindness. Adv. Exp. Med. Biol. 2010, 664, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Kisselev, O.G. Focus on molecules: Rhodopsin. Exp. Eye Res. 2005, 81, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Katayama, K.; Takeyama, Y.; Enomoto, A.; Imai, H.; Kandori, H. Disruption of Hydrogen-Bond Network in Rhodopsin Mutations Cause Night Blindness. J. Mol. Biol. 2020, 432, 5378–5389. [Google Scholar] [CrossRef] [PubMed]
- Saari, J.C. Vitamin A and Vision. In The Biochemistry of Retinoid Signaling II; Springer: Berlin/Heidelberg, Germany, 2016; Volume 81, pp. 231–259. [Google Scholar] [CrossRef]
- Xiao, T.; Xu, K.; Zhang, X.; Xie, Y.; Li, Y. Sector Retinitis Pigmentosa caused by mutations of the RHO gene. Eye 2019, 33, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Karali, M.; Testa, F.; Brunetti-Pierri, R.; Di Iorio, V.; Pizzo, M.; Mellillo, P.; Barillari, M.R.; Torella, A.; Musacchia, F.; D’Angello, L.; et al. Clinical and Genetic Analysis of a European Cohort with Pericentral Retinitis Pigmentosa. Int. J. Mol. Sci. 2019, 21, 86. [Google Scholar] [CrossRef] [PubMed]
- Kobal, N.; Krašovec, T.; Šuštar, M.; Volk, M.; Peterlin, B.; Hawlina, M.; Fakin, A. Stationary and Progressive Phenotypes Caused by the p.G90D Mutation in Rhodopsin Gene. Int. J. Mol. Sci. 2021, 22, 2133. [Google Scholar] [CrossRef]
- Georgiou, M.; Grewal, P.S.; Narayan, A.; Alser, M.; Ali, N.; Fujinami, K.; Webster, A.R.; Michaelides, M. Sector Retinitis Pigmentosa: Extending the Molecular Genetics Basis and Elucidating the Natural History. Am. J. Ophthalmol. 2021, 221, 299–310. [Google Scholar] [CrossRef]
- Coussa, R.G.; Basali, D.; Maeda, A.; DeBenedictis, M.; Traboulsi, E.I. Sector retinitis pigmentosa: Report of ten cases and a review of the literature. Mol. Vis. 2019, 25, 869–889. [Google Scholar]
- Sibulesky, L.; Hayes, K.C.; Pronczuk, A.; Weigel-DiFranco, C.; Rosner, B.; Berson, E.L. Safety of <7500 RE (<25000 IU) vitamin A daily in adults with retinitis pigmentosa. Am. J. Clin. Nutr. 1999, 69, 656–663. [Google Scholar] [CrossRef]
- Campbell, D.A.; Tonks, E.L. Biochemical findings in human retinitis pigmentosa with particular relation to vitamin a deficiency. Br. J. Ophthalmol. 1962, 46, 151–164. [Google Scholar] [CrossRef][Green Version]
- Stephensen, C.B.; Gildengorin, G. Serum retinol, the acute phase response, and the apparent misclassification of vitamin A status in the third National Health and Nutrition Examination Survey. Am. J. Clin. Nutr. 2000, 72, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Penniston, K.L.; Tanumihardjo, S.A. The acute and chronic toxic effects of vitamin A. Am. J. Clin. Nutr. 2006, 83, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Orban, T.; Palczewska, G.; Palczewski, K. Retinyl ester storage particles (retinosomes) from the retinal pigmented epithelium resemble lipid droplets in other tissues. J. Biol. Chem. 2011, 286, 17248–17258. [Google Scholar] [CrossRef] [PubMed]
- Frey, S.K.; Vogel, S. Vitamin A metabolism and adipose tissue biology. Nutrients 2011, 3, 27–39. [Google Scholar] [CrossRef]
- Chytil, F. The lungs and vitamin A. Am. J. Physiol. 1992, 262, L517–L527. [Google Scholar] [CrossRef]
- Sajovic, J.; Meglič, A.; Glavač, D.; Markelj, Š.; Hawlina, M.; Fakin, A. The Role of Vitamin A in Retinal Diseases. Int. J. Mol. Sci. 2022, 23, 1014. [Google Scholar] [CrossRef]
- Carazo, A.; Macakova, K.; Matušova, K.; Kujovska Krčmova, L.; Protti, M.; Mladenka, P. Vitamin A Update: Forms, Sources, Kinetics, Detection, Function, Deficiency, Therapeutic Use and Toxicity. Nutrients 2021, 13, 1703. [Google Scholar] [CrossRef]
- Blaner, W.S.; Li, Y.; Brun, P.-J.; Yuen, J.J.; Lee, S.-A.; Clugston, R.D. Vitamin A Absorption, Storage and Mobilization. Subcell Biochem. 2016, 81, 95–125. [Google Scholar] [CrossRef]
- Choi, E.H.; Daruwalla, A.; Suh, S.; Leinonen, H.; Palczewski, K. Retinoids in the visual cycle: Role of the retinal G protein-coupled receptor. J. Lipid Res. 2021, 62, 100040. [Google Scholar] [CrossRef]
- Kawaguchi, R.; Yu, J.; Honda, J.; Hu, J.; Whitelegge, J.; Ping, P.; Wiita, P.; Bok, D.; Sun, H. A membrane receptor for retinol binding protein mediates cellular uptake of vitamin A. Science 2007, 315, 820–825. [Google Scholar] [CrossRef]
- Kawaguchi, R.; Yu, J.; Wiita, P.; Sun, H. An essential ligand-binding domain in the membrane receptor for retinol-binding protein revealed by large-scale mutagenesis and a human polymorphism. J. Biol. Chem. 2008, 283, 15160–15168. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.; Widjaja-Adhi, M.A.K.; Palczewski, G.; von Lintig, J. Transport of vitamin A across blood-tissue barriers is facilitated by STRA6. FASEB J. 2016, 30, 2985–2995. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, R.; Zhong, M.; Kassai, M.; Ter-Stepanian, M.; Sun, H. STRA6-catalyzed vitamin A influx, efflux, and exchange. J. Membr. Biol. 2012, 245, 731–745. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, M.; Sivaprasadarao, A.; DeSousa, M.M.; Findlay, J.B. The transfer of retinol from serum retinol-binding protein to cellular retinol-binding protein is mediated by a membrane receptor. J. Biol. Chem. 1998, 273, 3336–3342. [Google Scholar] [CrossRef] [PubMed]
- Saari, J.C. Vitamin A metabolism in rod and cone visual cycles. Annu. Rev. Nutr. 2012, 32, 125–145. [Google Scholar] [CrossRef]
- Sears, A.E.; Palczewski, K. Lecithin:Retinol Acyltransferase: A Key Enzyme Involved in the Retinoid (visual) Cycle. Biochemistry 2016, 55, 3082–3091. [Google Scholar] [CrossRef]
- Perusek, L.; Maeda, T. Vitamin A derivatives as treatment options for retinal degenerative diseases. Nutrients 2013, 5, 2646–2666. [Google Scholar] [CrossRef]
- Harrison, E.H. Mechanisms of Transport and Delivery of Vitamin A and Carotenoids to the Retinal Pigment Epithelium. Mol. Nutr. Food Res. 2019, 63, e1801046. [Google Scholar] [CrossRef]
- Zeng, S.; Zhang, T.; Madigan, M.C.; Fernando, N.; Aggio-Bruce, R.; Zhou, F.; Pierce, M.; Chen, Y.; Huang, L.; Natoli, R.; et al. Interphotoreceptor Retinoid-Binding Protein (IRBP) in Retinal Health and Disease. Front. Cell. Neurosci. 2020, 14, 577935. [Google Scholar] [CrossRef]
- Sandberg, M.A.; Rosner, B.; Weigel-DiFranco, C.; Dryja, T.P.; Berson, E.L. Disease course of patients with X-linked retinitis pigmentosa due to RPGR gene mutations. Investig. Ophthalmol. Vis. Sci. 2007, 48, 1298–1304. [Google Scholar] [CrossRef]
- Campbell, D.A.; Harrison, R.; Tonks, E.L. Retinitis pigmentosa: Vitamin a serum levels in relation to clinical findings. Exp. Eye Res. 1964, 3, 412–426. [Google Scholar] [CrossRef]
- Zhao, Y.; Feng, K.; Liu, R.; Pan, J.; Zhang, L.; Lu, X. Vitamins and Mineral Supplements for Retinitis Pigmentosa. J. Ophthalmol. 2019, 2019, 8524607. [Google Scholar] [CrossRef] [PubMed]
- Jevnikar, K.; Šuštar, M.; Rotovnik Kozjek, N.; Štrucl, A.M.; Markelj, Š.; Hawlina, M.; Fakin, A. Disruption of the outer segments of the photoreceptors on optical coherence tomography as a feature of vitamin A deficiency. Retin. Cases Brief Rep. 2022, 16, 658–662. [Google Scholar] [CrossRef]
- Saenz-de-Viteri, M.; Sádaba, L.M. Optical Coherence Tomography Assessment Before and After Vitamin Supplementation in a Patient with Vitamin A Deficiency: A Case Report and Literature Review. Medicine 2016, 95, e2680. [Google Scholar] [CrossRef] [PubMed]
- Aleman, T.S.; Garrity, S.T.; Brucker, A.J. Retinal structure in vitamin A deficiency as explored with multimodal imaging. Doc. Ophthalmol. 2013, 127, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Chow, C.C.; Mieler, W.F. Vitamin A deficiency and xerophthalmic fundus in autoimmune hepatitis and cirrhosis. Retin. Cases Brief Rep. 2014, 8, 164–166. [Google Scholar] [CrossRef]
- Colozo, A.T.; Vasudevan, S.; Park, P.S. Retinal degeneration in mice expressing the constitutively active G90D rhodopsin mutant. Hum. Mol. Genet. 2020, 29, 881–891. [Google Scholar] [CrossRef]
- Zvyaga, T.A.; Fahmy, K.; Siebert, F.; Sakmar, T.P. Characterization of the mutant visual pigment responsible for congenital night blindness: A biochemical and Fourier-transform infrared spectroscopy study. Biochemistry 1996, 35, 7536–7545. [Google Scholar] [CrossRef]
- Sieving, P.A.; Fowler, M.L.; Bush, R.A.; Machida, S.; Calvert, P.D.; Green, D.G.; Makino, C.L.; McHenry, C.L. Constitutive “light” adaptation in rods from G90D rhodopsin: A mechanism for human congenital nightblindness without rod cell loss. J. Neurosci. 2001, 21, 5449–5460. [Google Scholar] [CrossRef]
- DePristo, M.A.; Banks, E.; Poplin, R.; Garimella, K.V.; Maguire, J.R.; Hartl, C.; Philippakis, A.A.; del Angel, G.; Rivas, M.A.; Hanna, M.; et al. A framework for variation discovery and genotyping using next-generation DNA sequencing data. Nat. Genet. 2011, 43, 491–498. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Meynert, A.M.; Ansari, M.; FitzPatrick, D.R.; Taylor, M.S. Variant detection sensitivity and biases in whole genome and exome sequencing. BMC Bioinform. 2014, 15, 247. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, D.L.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; Holder, G.E.; Tzekov, R.; Bach, M. ISCEV Standard for full-field clinical electroretinography (2015 update). Doc. Ophthalmol. 2015, 130, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.C.; Bach, M.; Brigell, M.; Keating, D.; Kondo, M.; Lyons, J.S.; Marmor, M.F.; McCulloch, D.L.; Palmowski-Wolfe, A.M. ISCEV standard for clinical multifocal electroretinography (mfERG) (2011 edition). Doc. Ophthalmol. 2012, 124, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bach, M.; Brigell, M.G.; Hawlina, M.; Holder, G.E.; Johnson, M.A.; McCulloch, D.L.; Meigen, T.; Viswanathan, S. ISCEV standard for clinical pattern electroretinography (PERG): 2012 update. Doc. Ophthalmol. 2013, 126, 1–7. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID (Centre ID) | Age When Examined (Years) | Sex | Phenotype | Serum Concentration of Vitamin A (µmol/L) | Normal Range of Serum Concentration of Vitamin A for Age (µmol/L) |
|---|---|---|---|---|---|
| A:III-10 * (642) | 71 | M | Classic RP | 1.68 | 1.05–2.8 |
| A:III-11 * (645) | 65 | M | Sector RP | 2.93 | 1.05–2.8 |
| A:III-12 * (604) | 63 | F | Sector RP | 2.44 | 1.05–2.8 |
| A:III-13 (1031) | 54 | M | Sector RP | 3.04 | 1.05–2.8 |
| A:III-14 * (760) | 55 | M | Sector RP | 3.56 | 1.05–2.8 |
| A:III-17 * (653) | 65 | M | Classic RP | 2.74 | 1.05–2.8 |
| A:IV-1 * (117) | 48 | M | NBWD | 3.23 | 1.05–2.8 |
| A:IV-4 * (1030) | 39 | M | Classic RP | 2.42 | 1.05–2.8 |
| A:IV-5 * (644) | 36 | M | Classic RP | 2.48 | 1.05–2.8 |
| A:IV-8 (1033) | 30 | F | NBWD | 2.01 | 1.05–2.8 |
| A:IV-17 * (652) | 38 | F | Classic RP | 2.1 | 1.05–2.8 |
| A:IV-19 (1034) | 39 | F | NBWD | 1.11 | 1.05–2.8 |
| A:V-1 * (1032) | 17 | M | NBWD | 1.44 | 0.91–2.51 |
| A:V-4 (1030) | 10 | F | Classic RP | 0.89 | 0.91–1.71 |
| B:III-3 * (610) | 29 | M | Pericentral RP | 2.33 | 1.05–2.8 |
| C:I-1 * (580) | 66 | F | Classic RP | 2.34 | 1,05–2,8 |
| C:II-2 * (612) | 40 | M | Classic RP | 1.56 | 1.05–2.8 |
| C:III-2 * (874) | 8 | M | NBWD | 1.64 | 0.91–1.71 |
| D:II-1 (1020) | 73 | M | Classic RP | 2.47 | 1.05–2.8 |
| D:II-2 (1021) | 65 | F | Classic RP | 2.32 | 1.05–2.8 |
| D:II-3 (1974) | 59 | M | Classic RP | 1.78 | 1.05–2.8 |
| D:III-1 (951) | 44 | M | Classic RP | 2.62 | 1.05–2.8 |
| D:IV-1 (950) | 14 | F | NBWD | 1.95 | 0.91–2.51 |
| E:I-1 (658) | 57 | F | Classic RP | 1.53 | 1.05–2.8 |
| E:I-2 (431) | 63 | M | Classic RP | 1.23 | 1.05–2.8 |
| E:II-1 (1058) | 34 | F | Classic RP | 0.92 | 1.05–2.8 |
| E:II-2 (1067) | 23 | M | Classic RP | 1.38 | 1.05–2.8 |
| E:II-3 (1068) | 13 | F | NBWD | 1.32 | 0.91–2.51 |
| F:I-1 (1961) | 48 | F | Classic RP | 1.75 | 1.05–2.8 |
| G:I-1 (1049) | 56 | F | Classic RP | 2.25 (s) | 1.05–2.8 |
| B | S.E. | Wald | df | Sig. | Exp(B) | |
|---|---|---|---|---|---|---|
| Serum concentration of vitamin A | −1.730 | 0.839 | 4.249 | 1 | 0.039 * | 0.177 |
| Age | 0.065 | 0.030 | 4.759 | 1 | 0.029 * | 1.068 |
| Constant | 1.367 | 1.434 | 0.908 | 1 | 0.353 | 3.923 |
| Phenotype | Main Features | Auxiliary Features |
|---|---|---|
| NBWD | Night blindness, normal visual field, normal fundus, normal FAF | Decreased or absent DA responses on ERG and normal LA responses on ERG |
| Sector RP | Night blindness, peripheral hypoautofluorescence on AF surrounded by a hyperautofluorescent line in the region of one or two quadrants | Partially constricted visual field, bone spicules in one or two quadrants, decreased DA and LA responses on ERG |
| Pericentral RP | Night blindness, annular area of retinal degeneration encompassed by a double hyperautofluorescent ring on FAF | Pericentral scotoma, retinal changes along the vascular arches |
| Classic RP | Night blindness, constricted visual field, concentric retinal degeneration delineated by a hyperautofluorescent ring on FAF | Bone spicules in three or four quadrants, decreased or absent DA and LA responses on the ERG |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krašovec, T.; Kobal, N.; Šuštar Habjan, M.; Volk, M.; Hawlina, M.; Fakin, A. Correlation between the Serum Concentration of Vitamin A and Disease Severity in Patients Carrying p.G90D in RHO, the Most Frequent Gene Associated with Dominant Retinitis Pigmentosa: Implications for Therapy with Vitamin A. Int. J. Mol. Sci. 2023, 24, 780. https://doi.org/10.3390/ijms24010780
Krašovec T, Kobal N, Šuštar Habjan M, Volk M, Hawlina M, Fakin A. Correlation between the Serum Concentration of Vitamin A and Disease Severity in Patients Carrying p.G90D in RHO, the Most Frequent Gene Associated with Dominant Retinitis Pigmentosa: Implications for Therapy with Vitamin A. International Journal of Molecular Sciences. 2023; 24(1):780. https://doi.org/10.3390/ijms24010780
Chicago/Turabian StyleKrašovec, Tjaša, Nina Kobal, Maja Šuštar Habjan, Marija Volk, Marko Hawlina, and Ana Fakin. 2023. "Correlation between the Serum Concentration of Vitamin A and Disease Severity in Patients Carrying p.G90D in RHO, the Most Frequent Gene Associated with Dominant Retinitis Pigmentosa: Implications for Therapy with Vitamin A" International Journal of Molecular Sciences 24, no. 1: 780. https://doi.org/10.3390/ijms24010780
APA StyleKrašovec, T., Kobal, N., Šuštar Habjan, M., Volk, M., Hawlina, M., & Fakin, A. (2023). Correlation between the Serum Concentration of Vitamin A and Disease Severity in Patients Carrying p.G90D in RHO, the Most Frequent Gene Associated with Dominant Retinitis Pigmentosa: Implications for Therapy with Vitamin A. International Journal of Molecular Sciences, 24(1), 780. https://doi.org/10.3390/ijms24010780