
How the Analysis of the Pathogenetic Variants of DDR Genes Will Change the Management of Prostate Cancer Patients

 , ,
, ,  ,
,
Abstract
1. Premise
- -
- A shift from a clear distinction between the management of hormone-sensitive prostate cancer (HSPC) and the management of castration-resistant prostate cancer (CRPC) to a merger of the two phases. At present, the management of metastatic castration-resistant prostate cancer (mCRPC) represents a second line of therapy, sharing several of the recommended drugs for metastatic hormone-sensitive prostate cancer (mHSPC).
- -
- The concept of the anticipation of therapies as the main goal achieved, leading, in particular, to the use of both docetaxel and androgen receptor signaling inhibitors (ARSi) from the mCRPC to the mHSPC phase.
- -
- Short metastatic-free survival
- -
- Short cancer-specific survival
- -
- The prediction of responses to PARP inhibitors and to platinum salts
2. DDR Analysis: Prognostic Role and Prediction of Response to Therapy
2.1. Incidence
2.2. Prognostic Role in Non-Metastatic PC
2.3. Prognostic Role in Metastatic PC
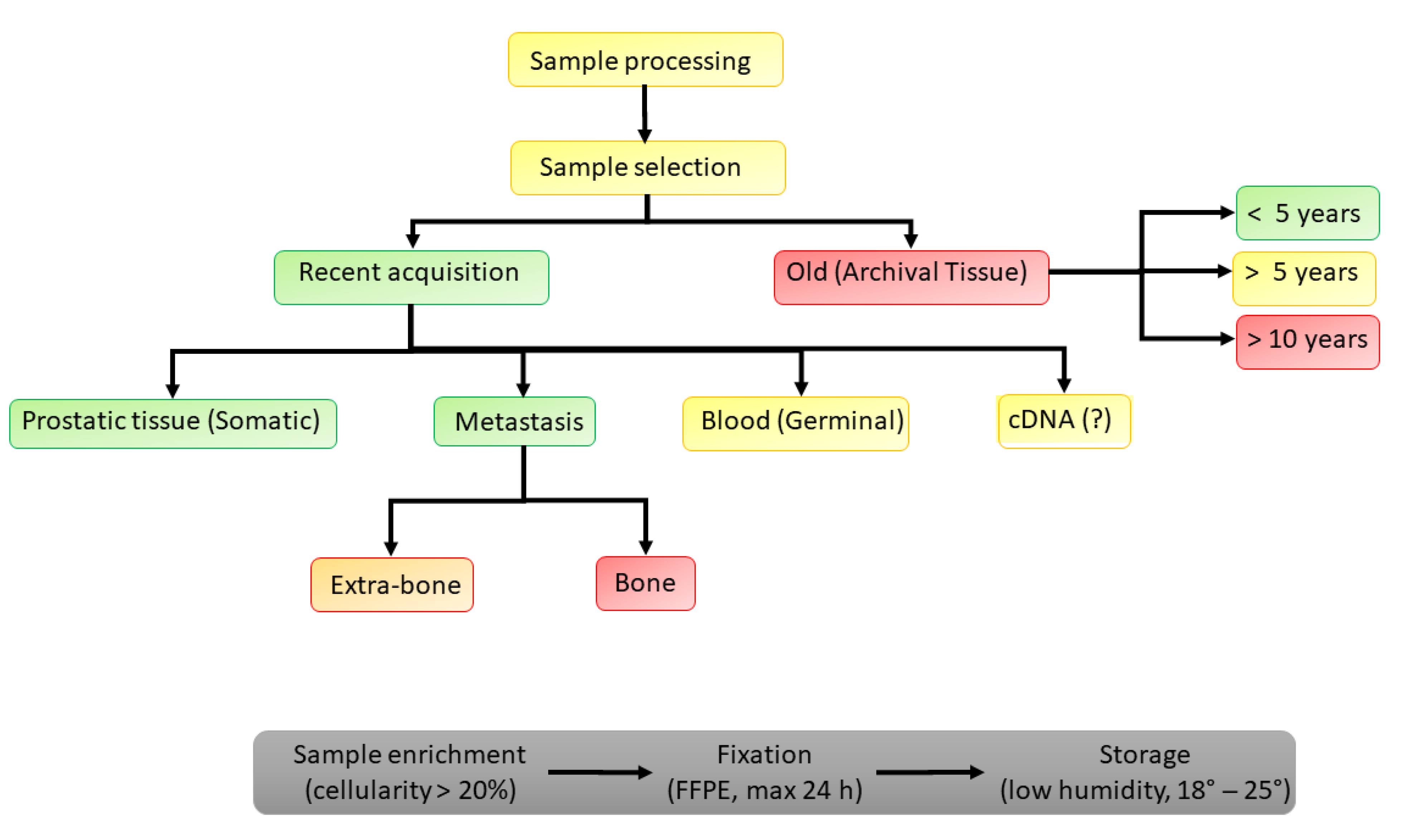
3. DDR Analysis: How to Perform
3.1. Recent vs. Archived Somatic Samples
3.2. Somatic vs. Germline Analysis in PC
- -
- Non-pathogenetic variants (probability of pathogenicity (PP) of < 0.001)
- -
- Likely not pathogenic or of little clinical significance (PP: 0.001–0.049)
- -
- Uncertain significance (PP: 0.05–0.949)
- -
- Likely pathogenic (PP: 0.95–0.99)
- -
- Pathogenic (PP of > 0.99).
- -
- test all metastatic PCs (either hormone-sensitive (HS) or castration-resistant (CR))
- -
- test all PCs with a significant family history of PC or hereditary breast and ovarian cancer syndrome and Lynch syndrome
- -
- in PC cases with somatic mutations, perform germline evaluations in all related family members
- -
- in nmPC, use the reflex test with an initial analysis of priority genes, followed by expanded panels with a particular focus on BRCA2
3.3. cDNA
4. PARP Inhibitors as Tailored Therapy
5. Answers Achieved, Open Questions, and Future Perspectives
5.1. Answers Achieved
- -
- The incidence of germline PVs in HRR genes among men with mPC varies between 11% and 33%, which is significantly higher than that of nmPC, and the BRCA2 PVs were more frequent when compared to other HRRs.
- -
- The determination of somatic or germline HRR PVs and, in particular, BRCA2, is able to define a tailored therapy with PARP inhibitors in mCRPC that progresses after first-line therapy, with significant improvements in rPFS and OS. This point reached recommendations from international guidelines and approval from the FDA and EMA for olaparib and rucaparib.
5.2. Open Questions
- -
- Conflicting results remain when comparing the somatic determination of HRRs between the primary site from prostate biopsy or prostatectomy and the biopsy on metastases (some studies found an incidence of 10% in primary tumors and 27% in metastatic samples, whereas others found similar detection rates between prostate biopsies (27%) and those of metastases (32%)) [13,14,15].
- -
- Somatic determination on a metastatic site, in particular, bone, may be associated with various biases (in 30% of cases), as well as possible side effects. On the other hand, the de novo determination on the prostate is not always possible at the time of the diagnosis of metastatic disease. The reliability of the analysis on paraffin preparations is conditioned by the temporal distance (good if <5 years and bad if >10 years).
- -
- Data on the use of circulating free DNA are still incomplete.
5.3. Future Perspectives
- -
- A geneticist will be included in our multidisciplinary groups on PC.
- -
- The prognostic value of HRR PVs will also be used in selected high-risk cases with non-metastatic stages to better arrange controls and therapeutic primary options.
- -
- The role of HRR genes other than BRCA2 will be better characterized, and new tailored therapies will be considered on the basis of defects other than BRCA.
- -
- The anticipation in the use of PARP inhibitors (HSPC) will be investigated.
- -
- The crosstalk between AR and DNA repair will be used to conduce to new combination strategies using ARSi plus PARP inhibitors or better therapeutic sequences (Table 2).
6. Conclusions
- -
- Test all mPC patients (either hormone-sensitive or castration-resistant) for somatic and germline HRR PVs. The use of this analysis in high-risk nmPC patients or for those with a significant family history of PC must be carefully discussed.
- -
- Use both germline and somatic tests and large gene panels with priority for BRCA2, leaving the determination of circulating free DNA in cases in which the somatic or germline determination is not suitable or reliable. Somatic determination on the primary site (prostate, when available) or on historic paraffin preparations with a temporal distance of no longer than 5 years should be preferred to metastatic site biopsies. The analysis must be performed in a specialized laboratory, following the criteria for evidence-based networks for the interpretation of PVs [16].
- -
- In mPC cases with somatic and germline BRCA PVs, offer a germline evaluation for all related family members after genetic counseling so as to conduct early cancer screening. The same germline evaluation is suggested in cases with high-risk nmPC patients with two or more relatives with a history of mammary, ovarian, or prostate neoplasms, or a history of early prostate cancer development (<55 years).
- -
- Consider a PARP inhibitor tailored therapy in cases with mCRPC that progresses after first-line therapy and that shows somatic and/or germline BRCA2 PVs.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-Repair Gene Mutations in Men with Metastatic Prostate Cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef] [PubMed]
- ICGC/TCGA. Pan-Cancer Analysis of Whole Genomes Consortium. Pan-cancer analysis of whole genomes. Nature 2020, 578, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Eeles, R.; Goh, C.; Castro, E.; Bancroft, E.; Guy, M.; Al Olama, A.A.; Easton, D.; Kote-Jarai, Z. The genetic epidemiology of prostate cancer and its clinical implications. Nat. Rev. Urol. 2014, 11, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, E.A.L.; Domati, F.; Guida, A.; Marchi, I.; Toss, A.; Barbieri, E.; Marcheselli, L.; Venturelli, M.; Piana, S.; Cirilli, C.; et al. BRCA mutation rate and characteristics of prostate tumor in breast and ovarian cancer families: Analysis of 6,591 Italian pedigrees. Cancer Biol. Med. 2021, 18, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://standuptocancer.org (accessed on 2 December 2022).
- Hussain, M.; Corcoran, C.; Sibilla, C.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Mateo, J.; Olmos, D.; Mehra, N.; et al. Tumor Genomic Testing for >4000 Men with Metastatic Castration-resistant Prostate Cancer in the Phase III Trial PROfound (Olaparib). Clin. Cancer Res. 2022, 28, 1518–1530. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Wu, J.; Gu, W.; Qin, X.; Dai, B.; Lin, G.; Gan, H.; Freedland, S.J.; Zhu, Y.; Ye, D. Germline DNA Repair Gene Mutation Landscape in Chinese Prostate Cancer Patients. Eur. Urol. 2019, 76, 280–283. [Google Scholar] [CrossRef]
- Page, E.C.; Bancroft, E.K.; Brook, M.N.; Assel, M.; Hassan Al Battat, M.; Thomas, S.; Taylor, N.; Chamberlain, A.; Pope, J.; Raghallaigh, H.N.; et al. Interim Results from the IMPACT Study: Evidence for Prostate-specific Antigen Screening in BRCA2 Mutation Carriers. Eur. Urol. 2019, 76, 831–842. [Google Scholar] [CrossRef]
- Carter, H.B.; Helfand, B.; Mamawala, M.; Wu, Y.; Landis, P.; Yu, H.; Wiley, K.; Na, R.; Shi, Z.; Petkewicz, J.; et al. Germline Mutations in ATM and BRCA1/2 Are Associated with Grade Reclassification in Men on Active Surveillance for Prostate Cancer. Eur. Urol. 2019, 75, 743–749. [Google Scholar] [CrossRef]
- Castro, E.; Goh, C.; Leongamornlert, D.; Saunders, E.; Tymrakiewicz, M.; Dadaev, T.; Govindasami, K.; Guy, M.; Ellis, S.; Frost, D.; et al. Effect of BRCA Mutations on Metastatic Relapse and Cause-specific Survival After Radical Treatment for Localised Prostate Cancer. Eur. Urol. 2015, 68, 186–193. [Google Scholar] [CrossRef]
- Martinez Chanza, N.; Bernard, B.; Barthelemy, P.; Accarain, A.; Paesmans, M.; Desmyter, L.; T’Kint de Roodenbeke, D.; Gil, T.; Sideris, S.; Roumeguere, T.; et al. Prevalence and clinical impact of tumor BRCA1 and BRCA2 mutations in patients presenting with localized or metastatic hormone-sensitive prostate cancer. Prostate Cancer Prostatic Dis. 2022, 25, 199–207. [Google Scholar] [CrossRef]
- Castro, E.; Goh, C.; Olmos, D.; Saunders, E.; Leongamornlert, D.; Tymrakiewicz, M.; Mahmud, N.; Dadaev, T.; Govindasami, K.; Guy, M.; et al. Germline BRCA mutations are associated with higher risk of nodal involvement, distant metastasis, and poor survival outcomes in prostate cancer. J. Clin. Oncol. 2013, 31, 1748–1757. [Google Scholar] [CrossRef] [PubMed]
- Annala, M.; Struss, W.J.; Warner, E.W.; Beja, K.; Vandekerkhove, G.; Wong, A.; Khalaf, D.; Seppälä, I.L.; So, A.; Lo, G.; et al. Treatment Outcomes and Tumor Loss of Heterozygosity in Germline DNA Repair-deficient Prostate Cancer. Eur. Urol. 2017, 72, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Lu, C.; Luber, B.; Liang, C.; Wang, H.; Chen, Y.; Silberstein, J.L.; Piana, D.; Lai, Z.; Chen, Y.; et al. Germline DNA-repair Gene Mutations and Outcomes in Men with Metastatic Castration-resistant Prostate Cancer Receiving First-line Abiraterone and Enzalutamide. Eur. Urol. 2018, 74, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Castro, E.; Romero-Laorden, N.; Del Pozo, A.; Lozano, R.; Medina, A.; Puente, J.; Piulats, J.M.; Lorente, D.; Saez, M.I.; Morales-Barrera, R.; et al. PROREPAIR-B: A Prospective Cohort Study of the Impact of Germline DNA Repair Mutations on the Outcomes of Patients with Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2019, 37, 490–503. [Google Scholar] [CrossRef]
- Giri, V.N.; Knudsen, K.E.; Kelly, W.K.; Cheng, H.H.; Cooney, K.A.; Cookson, M.S.; Dahut, W.; Weissman, S.; Soule, H.R.; Petrylak, D.P.; et al. Implementation of Germline Testing for Prostate Cancer: Philadelphia Prostate Cancer Consensus Conference 2019. J. Clin. Oncol. 2020, 38, 2798–2811. [Google Scholar] [CrossRef]
- Li, H.; Engel, C.; de la Hoya, M.; Peterlongo, P.; Yannoukakos, D.; Livraghi, L.; Radice, P.; Thomassen, M.; Hansen, T.V.O.; Gerdes, A.M.; et al. CIMBA Consortium. Risks of breast and ovarian cancer for women harboring pathogenic missense variants in BRCA1 and BRCA2 compared with those harboring protein truncating variants. Genet. Med. 2022, 24, 119–129. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Plon, S.E.; Eccles, D.M.; Easton, D.; Foulkes, W.D.; Genuardi, M.; Greenblatt, M.S.; Hogervorst, F.B.; Hoogerbrugge, N.; Spurdle, A.B.; Tavtigian, S.V.; et al. Sequence variant classification and reporting: Recommendations for improving the interpretation of cancer susceptibility genetic test results. Hum. Mutat. 2008, 29, 1282–1291. [Google Scholar] [CrossRef]
- Smith, M.R.; Scher, H.I.; Sandhu, S.; Efstathiou, E.; Lara, P.N., Jr.; Yu, E.Y.; George, D.J.; Chi, K.N.; Saad, F.; Ståhl, O.; et al. Niraparib in patients with metastatic castration-resistant prostate cancer and DNA repair gene defects (GALAHAD): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2022, 23, 362–373. [Google Scholar] [CrossRef]
- Torga, G.; Pienta, K.J. Patient-Paired Sample Congruence Between 2 Commercial Liquid Biopsy Tests. J. Am. Med. Assoc. Oncol. 2018, 4, 868–870. [Google Scholar] [CrossRef]
- Mateo, J.; Porta, N.; Bianchini, D.; McGovern, U.; Elliott, T.; Jones, R.; Syndikus, I.; Ralph, C.; Jain, S.; Varughese, M.; et al. Olaparib in patients with metastatic castration-resistant prostate cancer with DNA repair gene aberrations (TOPARP-B): A multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Abida, W.; Patnaik, A.; Campbell, D.; Shapiro, J.; Bryce, A.H.; McDermott, R.; Sautois, B.; Vogelzang, N.J.; Bambury, R.M.; Voog, E.; et al. Rucaparib in Men with Metastatic Castration-Resistant Prostate Cancer Harboring a BRCA1 or BRCA2 Gene Alteration. J. Clin. Oncol. 2020, 38, 3763–3772. [Google Scholar] [CrossRef] [PubMed]
- De Bono, J.S.; Mehra, N.; Scagliotti, G.V.; Castro, E.; Dorff, T.; Stirling, A.; Stenzl, A.; Fleming, M.T.; Higano, C.S.; Saad, F.; et al. Talazoparib monotherapy in metastatic castration-resistant prostate cancer with DNA repair alterations (TALAPRO-1): An open-label, phase 2 trial. Lancet Oncol. 2021, 22, 1250–1264. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Karanika, S.; Yang, G.; Wang, J.; Park, S.; Broom, B.M.; Manyam, G.C.; Wu, W.; Luo, Y.; Basourakos, S.; et al. Androgen receptor inhibitor-induced "BRCAness" and PARP inhibition are synthetically lethal for castration-resistant prostate cancer. Sci. Signal. 2017, 10, eaam7479. [Google Scholar] [CrossRef]
- Saad, F.; Thiery-Vuillemin, A.; Wiechno, P.; Alekseev, B.; Sala, N.; Jones, R.; Kocak, I.; Chiuri, V.E.; Jassem, J.; Fléchon, A.; et al. Patient-reported outcomes with olaparib plus abiraterone versus placebo plus abiraterone for metastatic castration-resistant prostate cancer: A randomised, double-blind, phase 2 trial. Lancet Oncol. 2022, 23, 1297–1307. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.N.; Rathkopf, D.E.; Smith, M.R.; Efstathiou, E.; Attard, G.; Olmos, D.; Lee, J.Y.; Small, E.J.; Gomes, A.J.; Roubaud, G.; et al. Phase 3 MAGNITUDE study: First results of niraparib (NIRA) with abiraterone acetate and prednisone (AAP) as first-line therapy in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) with and without homologous recombination repair (HRR) gene alterations. J. Clin. Oncol. 2022, 40, 12. [Google Scholar]



{kind=link}
{kind=link}
| Study | Study Design | Ethnicity | Incidence of DDR Gene PVs | Population | Outcomes Analyzed | Oncological Results in Carriers vs. No Carriers |
|---|---|---|---|---|---|---|
| Localized PC | ||||||
| Page E.C. et al., 2019. IMPACT study [8] | Prospective | Caucasian | Not applicable | PSA screening 902 BRCA-2 carriers 497 BRCA-2 no carriers | - PC incidence (rate per 1000 persons per year) -csPC | (19.4% vs. 12.0%; p = 0.03 (77% vs. 40%; p = 0.01) |
| Carter H.B. et al., 2019 [9] | Retrospective | Caucasian | All genes (BRCA1-2 plus ATM) - any upgrading (3.81%) - upgraded GG1 to ≥ 3 (5.10%) - upgraded GG1 to ≥ 2 (3.89%) | Active surveillance - 1211 patients | grade reclassification (GR) at 2, 5 and 10 years | (27%, 50% and 78% vs. 10%, 22% and 40%) |
| Castro E. et al., 2015 [10] | Retrospective | Caucasian | BRCA 1-2 (5.15) | 1302 patients with local or locally advanced PC treated with RT or RP - 67 carriers - 1235 no carriers | MFS at 3, 5, and 10 years CSS at 3.5 and 10 years | (90%, 72% and 50% vs. 97%, 94% and 84%, p < 0.001) (96%, 76% and 61% vs. 99%, 97% and 85%, p < 0.001) |
| Martinez Chanza N. et al., 2022 [11] | Retrospective | Caucasian | 3.5% | 258 patients with localized PC treated with RP or RT - 8 carriers - 250 no carriers | EFS MFS | 18.1 vs. 57 months (HR 1.73; 95% CI: 0.63–4.74; p = 0.28) 37 vs. 153 months (HR 2.77; 95% CI: 0.84–9.14; p = 0.08) |
| Castro E. et al., 2013 [12] | Retrospective | Caucasian | BRCA1-2 (3.81%) | 2019 patients at diagnosis - 79 carriers - 1940 no carriers | MFS CCS OS N+ | (77% v 93%; p = 0.0001) (82% v 96%; p = 9 × 10−8) (8.1 vs. 12.9 years; p = 1 × 10−7) (N1: 15% v 5%; p = 0.0005) |
| Metastatic PC | ||||||
| Annala M. et al., 2017 [13] | Prospective | Caucasian | 7.5% | 133 patients with mCRPC treated with first-line therapy with docetaxel, abiraterone, or enzalutamide - 22 carriers - 113 no carriers | PFS on first-line AR target therapy PFS on first-line docetaxel | 3.3 months (95% CI: 2.7–3.9) vs. 6.2 (95% CI: 5.1–7.3), p = 0.01 7.2 months (95% CI: 5.6–8.7) vs. 8.0 (95% CI: 7.1–9.1), p = 0.127 |
| Antonarakis E. et al., 2018 [14] | Prospective | Caucasian | 12.8% | 172 patients with mCRPC treated with first-line therapy with abiraterone or enzalutamide - 22 carriers - 152 no carriers | PSA response rate PSA-PFS PFS OS | 77% vs. 59% (p = 0.158) median 10.2 vs. 7.6 months; [HR] 0.64, 95% CI: 0.39–1.04; p = 0.070 median 13.3 vs. 10.3 months; HR 0.67, 95% CI: 0.41–1.09; p = 0.107 median 41.1 vs. 28.3 months; HR 0.58, 95% CI: 0.30–1.11; p = 0.097 |
| Castro E. et al., 2019 PROREPAIR-B [15] | Prospective | Caucasian | 16.2% | 419 patients with mCRPC treated with first-line therapy with abiraterone or enzalutamide - 68 carriers - 351 no carriers | Time to mCRPC CCS CCS (only BRCA2) | 22.8 vs. 28.4 months; p = 0.007 23.3 vs. 33.2 months; HR, 1.32; 95% CI, 0.81 to 2.17, p = 0.264 17.4 vs. 33.2 months; HR, 2.10; 95% CI, 1.07 to 4.10; p = 0.027 |
| Answers Achieved | Future Perspectives |
|---|---|
| Incidence of PVs in HRR genes = 11–33%, higher in mPC than in nmPC | Include a geneticist in multidisciplinary groups on PC |
| BRCA2 PVs more frequent than other HRRs | Use of the prognostic analysis of HRR PVs in selected high-risk cases with nmPC |
| Somatic or germline HRR PVs define tailored therapy with PARP inhibitors in mCRPC | Anticipation in the use of PARP inhibitors from mCRPC to mHSPC |
| Somatic determination on primary site with a temporal distance of less than 5 years as preferred for HRR analysis | New combination strategies using ARSi plus PARP inhibitors |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sciarra, A.; Frisenda, M.; Bevilacqua, G.; Gentilucci, A.; Cattarino, S.; Mariotti, G.; Del Giudice, F.; Di Pierro, G.B.; Viscuso, P.; Casale, P.; et al. How the Analysis of the Pathogenetic Variants of DDR Genes Will Change the Management of Prostate Cancer Patients. Int. J. Mol. Sci. 2023, 24, 674. https://doi.org/10.3390/ijms24010674
Sciarra A, Frisenda M, Bevilacqua G, Gentilucci A, Cattarino S, Mariotti G, Del Giudice F, Di Pierro GB, Viscuso P, Casale P, et al. How the Analysis of the Pathogenetic Variants of DDR Genes Will Change the Management of Prostate Cancer Patients. International Journal of Molecular Sciences. 2023; 24(1):674. https://doi.org/10.3390/ijms24010674
Chicago/Turabian StyleSciarra, Alessandro, Marco Frisenda, Giulio Bevilacqua, Alessandro Gentilucci, Susanna Cattarino, Gianna Mariotti, Francesco Del Giudice, Giovanni Battista Di Pierro, Pietro Viscuso, Paolo Casale, and et al. 2023. "How the Analysis of the Pathogenetic Variants of DDR Genes Will Change the Management of Prostate Cancer Patients" International Journal of Molecular Sciences 24, no. 1: 674. https://doi.org/10.3390/ijms24010674
APA StyleSciarra, A., Frisenda, M., Bevilacqua, G., Gentilucci, A., Cattarino, S., Mariotti, G., Del Giudice, F., Di Pierro, G. B., Viscuso, P., Casale, P., Chung, B. I., Autorino, R., Crivellaro, S., & Salciccia, S. (2023). How the Analysis of the Pathogenetic Variants of DDR Genes Will Change the Management of Prostate Cancer Patients. International Journal of Molecular Sciences, 24(1), 674. https://doi.org/10.3390/ijms24010674