
Novel Arylpiperazine Derivatives of Salicylamide with α1-Adrenolytic Properties Showed Antiarrhythmic and Hypotensive Properties in Rats

 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. The Tested Compounds Showed High to Moderate Affinity for α1-Adrenergic Receptors
2.2. The Tested Compounds Showed Prophylactic Antiarrhythmic Activity in the Arrhythmia Model Induced by Adrenaline, but Not by Calcium Chloride or Aconitine in Rats
2.3. The Tested Compounds Showed Therapeutic Antiarrhythmic Activity in the Adrenaline-Induced Arrhythmia Model in Rats
2.4. The Tested Compounds Did Not Influence the ECG Parameters in Rats (Except for JJGW02 and JJGW11, Which Decreased the Heart Rate Significantly)
2.5. The Tested Compounds Decreased Blood Pressure in the Normotensive Rats
2.6. The Tested Compounds Reversed the Pressor Effect of Methoxamine in Rats
3. Discussion
4. Materials and Methods
4.1. Drugs
4.2. Animals
4.3. Radioligand Binding Assay
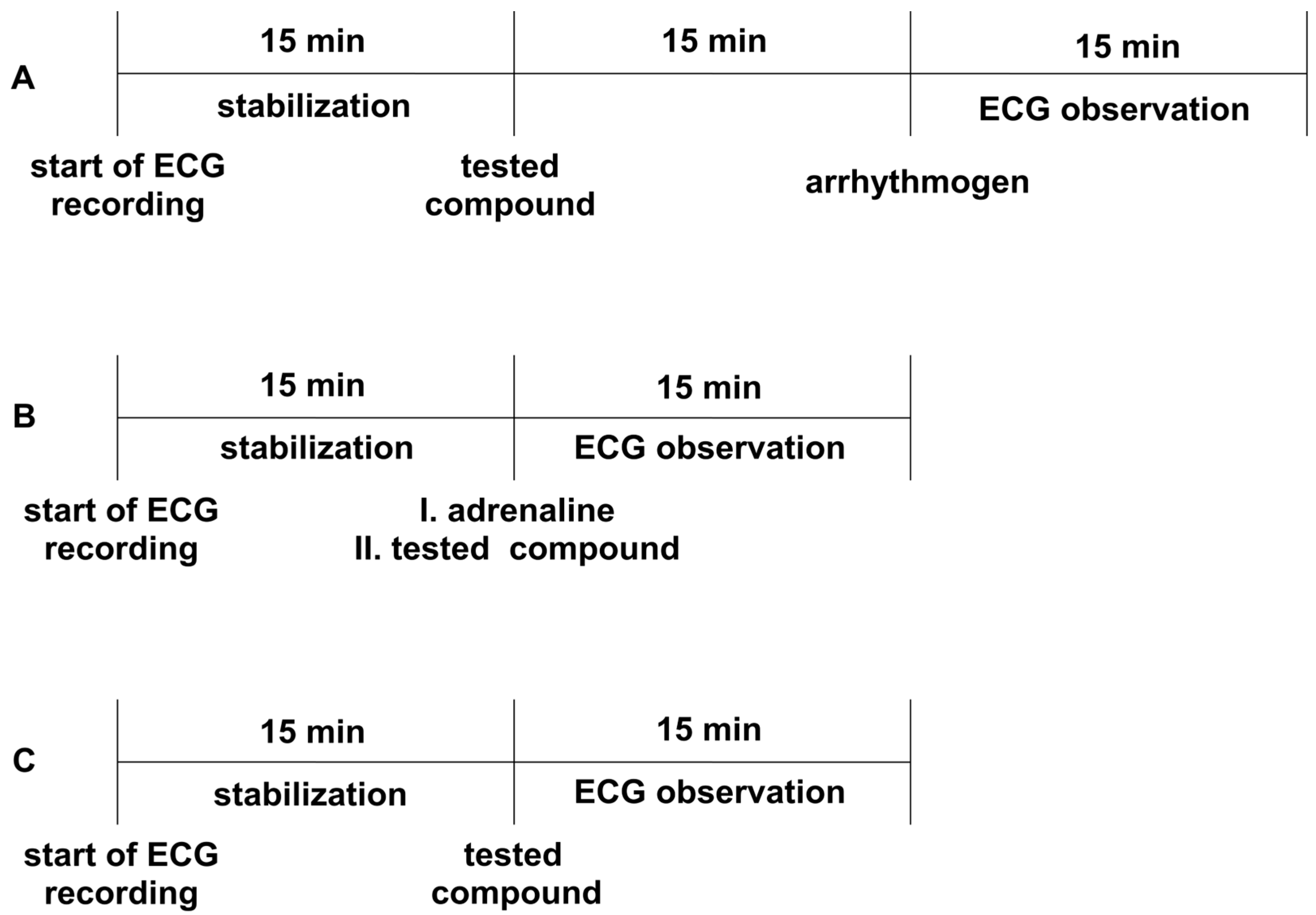
4.4. Prophylactic Antiarrhythmic Activity in Adrenaline-, Aconitine-, and Calcium Chloride-Induced Arrhythmia
4.5. Therapeutic Antiarrhythmic Activity in Adrenaline-Induced Arrhythmia
4.6. The Effect on a Normal Electrocardiogram in Rats
4.7. ECG Waveform Analysis
4.8. The Influence on Blood Pressure in the Normotensive Rats
4.9. The Influence on Blood Vasopressor Response in Rats
4.10. Statistic Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 8 November 2022).
- American Heart Association. What Is an Arrhythmia? Available online: https://www.heart.org/en/health-topics/arrhythmia/about-arrhythmia (accessed on 8 November 2022).
- Sugita, J.; Fujiu, K.; Nakayama, Y.; Matsubara, T.; Matsuda, J.; Oshima, T.; Liu, Y.; Maru, Y.; Hasumi, E.; Kojima, T.; et al. Cardiac macrophages prevent sudden death during heart stress. Nat. Commun. 2021, 12, 1910. [Google Scholar] [CrossRef] [PubMed]
- Kowey, P.R. Pharmacological Effects of Antiarrhythmic Drugs: Review and Update. Arch. Intern. Med. 1998, 158, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Dan, G.A.; Martinez-Rubio, A.; Agewall, S.; Boriani, G.; Borggrefe, M.; Gaita, F.; Van Gelder, I.; Gorenek, B.; Kaski, J.C.; Kjeldsen, K.; et al. Antiarrhythmic drugs–clinical use and clinical decision making: A consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology (ESC) Working Group on Cardiovascular Pharmacology, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and International Society of Cardiovascular Pharmacotherapy (ISCP). EP Eur. 2018, 20, 731–732. [Google Scholar] [CrossRef]
- Alegret, J.M.; Viñolas, X.; Grande, Á.; Castellanos, E.; Asso, A.; Tercedor, L.; Carmona, J.R.; Medina, O.; Alberola, A.G.; Fidalgo, M.L.; et al. Clinical Effectiveness of Antiarrhythmic Treatment After Electrical Cardioversion in Patients Without Structural Heart Disease. Rev. Española Cardiol. 2008, 61, 1274–1279. [Google Scholar] [CrossRef] [PubMed]
- Valembois, L.; Audureau, E.; Takeda, A.; Jarzebowski, W.; Belmin, J.; Lafuente-Lafuente, C. Antiarrhythmics for maintaining sinus rhythm after cardioversion of atrial fibrillation. Cochrane Database Syst. Rev. 2019, 9, 1–193. [Google Scholar] [CrossRef]
- King, G.S.; Goyal, A.; Grigorova, Y.; Hashmi, M.F. Antiarrhythmic Medications. Semin. Dial. 2022, 3, 33–38. [Google Scholar] [CrossRef]
- Mankad, P.; Kalahasty, G. Antiarrhythmic Drugs: Risks and Benefits. Med. Clin. N. Am. 2019, 103, 821–834. [Google Scholar] [CrossRef]
- Larson, J.; Rich, L.; Deshmukh, A.; Judge, E.C.; Liang, J.J. Pharmacologic Management for Ventricular Arrhythmias: Overview of Anti-Arrhythmic Drugs. J. Clin. Med. 2022, 11, 3233. [Google Scholar] [CrossRef]
- Geng, M.; Lin, A.; Nguyen, T.P. Revisiting Antiarrhythmic Drug Therapy for Atrial Fibrillation: Reviewing Lessons Learned and Redefining Therapeutic Paradigms. Front. Pharmacol. 2020, 11, 581837. [Google Scholar] [CrossRef]
- Zimetbaum, P. Antiarrhythmic Drug Therapy for Atrial Fibrillation. Circulation 2012, 125, 381–389. [Google Scholar] [CrossRef]
- Claro, J.C.; Candia, R.; Rada, G.; Baraona, F.; Larrondo, F.; Letelier, L.M. Amiodarone versus other pharmacological interventions for prevention of sudden cardiac death. Cochrane Database Syst. Rev. 2015, 2015, 1–84. [Google Scholar] [CrossRef]
- Hamilton, D.; Nandkeolyar, S.; Lan, H.; Desai, P.; Evans, J.; Hauschild, C.; Choksi, D.; Abudayyeh, I.; Contractor, T.; Hilliard, A. Amiodarone: A Comprehensive Guide for Clinicians. Am. J. Cardiovasc. Drugs 2020, 20, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Gil, J.; Marmelo, B.; Abreu, L.; Antunes, H.; Dos Santos, L.F.; Cabral, J.C. Propafenone Overdose: From Cardiogenic Shock to Brugada Pattern. Arq. Bras. Cardiol. 2018, 110, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Savage, R.D.; Visentin, J.D.; Bronskill, S.E.; Wang, X.; Gruneir, A.; Giannakeas, V.; Guan, J.; Lam, K.; Luke, M.J.; Read, S.H.; et al. Evaluation of a Common Prescribing Cascade of Calcium Channel Blockers and Diuretics in Older Adults with Hypertension. JAMA Intern. Med. 2020, 180, 643. [Google Scholar] [CrossRef] [PubMed]
- Rosen, M.R.; Wit, A.L. Arrhythmogenic actions of antiarrhythmic drugs. Am. J. Cardiol. 1987, 59, E10–E18. [Google Scholar] [CrossRef]
- Nattel, S. Experimental evidence for proarrhythmic mechanisms of antiarrhythmic drugs. Cardiovasc. Res. 1998, 37, 567–577. [Google Scholar] [CrossRef]
- Zipes, D.P. Proarrhythmic effects of antiarrhythmic drugs. Am. J. Cardiol. 1987, 59, E26–E31. [Google Scholar] [CrossRef]
- Nánási, P.P.; Pueyo, E.; Virág, L. Editorial: Perspectives of Antiarrhythmic Drug Therapy: Disappointing Past, Current Efforts, and Faint Hopes. Front. Pharmacol. 2020, 11, 1116. [Google Scholar] [CrossRef]
- Camm, A.J. Hopes and disappointments with antiarrhythmic drugs. Int. J. Cardiol. 2017, 237, 71–74. [Google Scholar] [CrossRef]
- Oluwole Fagbemi, S.; Chi, L.; Lucchesi, B.R. Antifibrillatory and profibrillatory actions of selected class I antiarrhythmic agents. J. Cardiovasc. Pharmacol. 1993, 21, 709–719. [Google Scholar] [CrossRef]
- Kirchhof, P.F.; Larissa Fabritz, C.; Franz, M.R. Postrepolarization refractoriness versus conduction slowing caused by class I antiarrhythmic drugs: Antiarrhythmic and proarrhythmic effects. Circulation 1998, 97, 2567–2574. [Google Scholar] [CrossRef] [PubMed]
- Skibsbye, L.; Ravens, U. Mechanism of Proarrhythmic Effects of Potassium Channel Blockers. Card. Electrophysiol. Clin. 2016, 8, 395–410. [Google Scholar] [CrossRef]
- Kahlon, S.S.; Sikandar, R.; Tejovath, S.; Nair, S.; Hassan, D.; Patel, K.K.; Peddemul, A.; Mostafa, J.A. Diagnosing Torsades De Pointes Based on Correlation to QT Interval: A Systematic Review. Cureus 2022, 14, e27833. [Google Scholar] [CrossRef] [PubMed]
- Belardinelli, L.; Giles, W.R.; Rajamani, S.; Karagueuzian, H.S.; Shryock, J.C. Cardiac late Na+ current: Proarrhythmic effects, roles in long QT syndromes, and pathological relationship to CaMKII and oxidative stress. Heart Rhythm 2015, 12, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, D.J. Drug-induced proarrhythmic effects: Assessment of changes in QT interval. Br. J. Clin. Pharmacol. 2000, 50, 297–302. [Google Scholar] [CrossRef]
- Priori, S.G.; Napolitano, C.; Schwartz, P.J. Cardiac receptor activation and arrhythmogenesis. Eur. Heart J. 1993, 14 (Suppl. E), 20–26. [Google Scholar] [CrossRef]
- Kurz, T.; Yamada, K.A.; DaTorre, S.D.; Corr, P.B. Alpha 1-adrenergic system and arrhythmias in ischaemic heart disease. Eur. Heart J. 1991, 12 (Suppl. F), 88–98. [Google Scholar] [CrossRef]
- Molinoff, P.B. Alpha- and beta-adrenergic receptor subtypes properties, distribution and regulation. Drugs 1984, 28 (Suppl. 2), 1–15. [Google Scholar] [CrossRef]
- Adolfo García-Sáinz, J. Alpha 1-adrenergic action: Receptor subtypes, signal transduction and regulation. Cell. Signal. 1993, 5, 539–547. [Google Scholar] [CrossRef]
- Jensen, B.C.; Swigart, P.M.; De Marco, T.; Hoopes, C.; Simpson, P.C. {alpha}1-Adrenergic receptor subtypes in nonfailing and failing human myocardium. Circ. Heart Fail. 2009, 2, 654–663. [Google Scholar] [CrossRef]
- Zhang, J.; Simpson, P.C.; Jensen, B.C. Cardiac α1A-adrenergic receptors: Emerging protective roles in cardiovascular diseases. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H725–H733. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, T.D.; Jensen, B.C.; Baker, A.J.; Simpson, P.C. Cardiac alpha1-adrenergic receptors: Novel aspects of expression, signaling mechanisms, physiologic function, and clinical importance. Pharmacol. Rev. 2013, 66, 308–333. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.M. Adrenergic receptors: Structure and function. Cleve. Clin. J. Med. 1990, 57, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Pustovit, K.B.; Samoilova, D.V.; Abramochkin, D.V.; Filatova, T.S.; Kuzmin, V.S. α1-adrenergic receptors accompanied by GATA4 expression are related to proarrhythmic conduction and automaticity in rat interatrial septum. J. Physiol. Biochem. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, A.D.; Filatova, T.S.; Abramochkin, D.V.; Atkinson, A.; Dobrzynski, H.; Kokaeva, Z.G.; Merzlyak, E.M.; Pustovit, K.B.; Kuzmin, V.S. Attenuation of inward rectifier potassium current contributes to the α1-adrenergic receptor-induced proarrhythmicity in the caval vein myocardium. Acta Physiol. 2021, 231, e13597. [Google Scholar] [CrossRef]
- Kuz’min, V.S.; Kobylina, A.A.; Pustovit, K.B.; Ivanova, A.D.; Abramochkin, D.V. MicroRNA miR-133a-3p Facilitates Adrenergic Proarrhythmic Ectopy in Rat Pulmonary Vein Myocardium by Increasing cAMP Content. Bull. Exp. Biol. Med. 2022, 172, 671–675. [Google Scholar] [CrossRef]
- Groszek, G.; Nowak-Król, A.; Wdowik, T.; Świerczyński, D.; Bednarski, M.; Otto, M.; Walczak, M.; Filipek, B. Synthesis and adrenolytic activity of 1-(1H-indol-4-yloxy)-3-(2-(2-methoxy phenoxy)ethylamino)propan-2-ol analogs and its enantiomers. Part 2. Eur. J. Med. Chem. 2009, 44, 5103–5111. [Google Scholar] [CrossRef]
- Groszek, G.; Bajek, A.; Bis, A.; Nowak-Król, A.; Bednarski, M.; Siwek, A.; Filipek, B. Synthesis and adrenolytic activity of new propanolamines. Molecules 2010, 15, 3887–3904. [Google Scholar] [CrossRef]
- Groszek, G.; Bednarski, M.; Dybała, M.; Filipek, B. Synthesis and adrenolytic activity of 1-(1H-indol-4-yloxy)-3-{[2-(2-methoxyphenoxy)ethyl]amino}propan-2-ol and its enantiomers. Part 1. Eur. J. Med. Chem. 2009, 44, 809–817. [Google Scholar] [CrossRef]
- Bednarski, M.; Otto, M.; Dudek, M.; Kołaczkowski, M.; Bucki, A.; Siwek, A.; Groszek, G.; Maziarz, E.; Wilk, P.; Sapa, J. Synthesis and Pharmacological Activity of a New Series of 1-(1H-Indol-4-yloxy)-3-(2-(2-methoxyphenoxy)ethylamino)propan-2-ol Analogs. Arch. Pharm. 2016, 349, 211–223. [Google Scholar] [CrossRef]
- Richer, L.P.; Vinet, A.; Kus, T.; Cardinal, R.; Ardell, J.L.; Armour, J.A. Alpha-adrenoceptor blockade modifies neurally induced atrial arrhythmias. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R1175–R1180. [Google Scholar] [CrossRef] [PubMed]
- Dabrowska, B.; Pruszczyk, P.; Dabrowski, A.; Feltynowski, T.; Wocial, B.; Januszewicz, W. Influence of α-adrenergic blockade on ventricular arrhythmias, QTc interval and heart rate variability in phaeochromocytoma. J. Hum. Hypertens. 1995, 9, 925–929. [Google Scholar] [PubMed]
- Penjišević, J.Z.; Šukalović, V.B.; Andrić, D.B.; Suručić, R.; Kostić-Rajačić, S.V. The Therapeutic Potential of 2-{[4-(2-methoxyphenyl)piperazin-1-yl]alkyl}-1H-benzo[d]imidazoles as Ligands for Alpha1-Adrenergic Receptor—Comparative In Silico and In Vitro Study. Appl. Biochem. Biotechnol. 2022, 194, 3749–3764. [Google Scholar] [CrossRef]
- Martin Grisar, J.; Claxton, G.P.; Bare, T.M.; Dage, R.C.; Cheng, H.C.; Woodward, J.K. Salicylamide derivatives related to medroxalol with alpha- and beta-adrenergic antagonist and antihypertension activity. J. Med. Chem. 1981, 24, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Clifton, J.E.; Collins, I.; Hallett, P.; Hartley, D.; Lunts, L.H.C.; Wicks, P.D. Arylethanolamines derived from salicylamide with alpha- and beta-adrenoceptor blocking activities. Preparation of labetalol, its enantiomers, and related salicylamides. J. Med. Chem. 1982, 25, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Brittain, R.T.; Drew, G.M.; Levy, G.P. The alpha- and beta-adrenoceptor blocking potencies of labetalol and its individual stereoisomers in anaesthetized dogs and in isolated tissues. Br. J. Pharmacol. 1982, 77, 105–114. [Google Scholar] [CrossRef]
- Cheng, Y.; Prusoff, W.H. Relationship between the inhibition constant (K1) and the concentration of inhibitor which causes 50 per cent inhibition (I50) of an enzymatic reaction. Biochem. Pharmacol. 1973, 22, 3099–3108. [Google Scholar] [CrossRef]
- Litchfield, J.T.; Wilcoxon, F. A simplified method of evaluating dose-effect experiments. J. Pharmacol. Exp. Ther. 1949, 96, 99–113. [Google Scholar] [PubMed]
- De Clerck, F.; Van de Water, A.; D’Aubioul, J.; Hua, R.L.; Van Rossem, K.; Hermans, A.; Van Ammel, K. In vivo measurement of QT prolongation, dispersion and arrhythmogenesis: Application to the preclinical cardiovascular safety pharmacology of a new chemical entity. Fundam. Clin. Pharmacol. 2002, 16, 125–140. [Google Scholar] [CrossRef]
- Biolo, A.; Rosa, A.S.; Mazzotti, N.G.; Martins, S.; Belló-Klein, A.; Rohde, L.E.; Clausell, N. The role of adrenergic receptor polymorphisms in heart failure. Braz. J. Med. Biol. Res. 2006, 39, 1281–1290. [Google Scholar] [CrossRef]
- Dunaway, S.; Yu, Q.; Larson, D.F. Effect of acute alpha adrenergic stimulation on cardiac function. Perfusion 2007, 22, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G. The paradox of α-adrenergic coronary vasoconstriction revisited. J. Mol. Cell. Cardiol. 2011, 51, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Lustyk, K.; Sałaciak, K.; Siwek, A.; Sapa, J.; Zaręba, P.; Gałuszka, A.; Pytka, K. The Antiarrhythmic and Hypotensive Effects of S-61 and S-73, the Pyrrolidin-2-one Derivatives with α1-Adrenolytic Properties. Int. J. Mol. Sci. 2022, 23, 10381. [Google Scholar] [CrossRef] [PubMed]
- Lustyk, K.; Sałaciak, K.; Siwek, A.; Filipek, B.; Sapa, J.; Marona, H.; Żelaszczyk, D.; Pytka, K. HBK-10, A Compound with α1-Adrenolytic Properties, Showed Antiarrhythmic and Hypotensive Effects in Rats. Pharmaceuticals 2022, 15, 1256. [Google Scholar] [CrossRef] [PubMed]
- Gautier, P.; Guillemare, E.; Djandjighian, L.; Marion, A.; Planchenault, J.; Bernhart, C.; Herbert, J.M.; Nisato, D. In vivo and in vitro characterization of the novel antiarrhythmic agent SSR149744C: Electrophysiological, anti-adrenergic, and anti-angiotensin II effects. J. Cardiovasc. Pharmacol. 2004, 44, 244–257. [Google Scholar] [CrossRef] [PubMed]
- Handzlik, J.; Szymańska, E.; Ndza, K.; Kubacka, M.; Siwek, A.; Mogilski, S.; Handzlik, J.; Filipek, B.; Kieć-Kononowicz, K. Pharmacophore models based studies on the affinity and selectivity toward 5-HT1A with reference to α1-adrenergic receptors among arylpiperazine derivatives of phenytoin. Bioorg. Med. Chem. 2011, 19, 1349–1360. [Google Scholar] [CrossRef]
- Handzlik, J.; Szymańska, E.; Wójcik, R.; Dela, A.; Jastrzebska-Wiesek, M.; Karolak-Wojciechowska, J.; Fruziński, A.; Siwek, A.; Filipek, B.; Kieć-Kononowicz, K. Synthesis and SAR-study for novel arylpiperazine derivatives of 5-arylidenehydantoin with α₁-adrenoceptor antagonistic properties. Bioorg. Med. Chem. 2012, 20, 4245–4257. [Google Scholar] [CrossRef]
- Rapacz, A.; Sapa, J.; Nowiński, L.; Mogilski, S.; Pytka, K.; Filipek, B.; Siwek, A.; Szkaradek, N.; Marona, H. Biofunctional studies of new 2-methoxyphenylpiperazine xanthone derivatives with α₁-adrenolytic properties. Pharmacol. Rep. 2015, 67, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.; Kiehn, J.; Katus, H.A.; Karle, C.A. Adrenergic regulation of the rapid component of the cardiac delayed rectifier potassium current, I(Kr), and the underlying hERG ion channel. Basic Res. Cardiol. 2004, 99, 279–287. [Google Scholar] [CrossRef]
- Pytka, K.; Lustyk, K.; Zmudzka, E.; Kotanska, M.; Siwek, A.; Zygmunt, M.; Dziedziczak, A.; Sniecikowska, J.; Olczyk, A.; Galuszka, A.; et al. Chemically Homogenous Compounds with Antagonistic Properties at All α1-Adrenoceptor Subtypes but not β1-Adrenoceptor Attenuate Adrenaline-Induced Arrhythmia in Rats. Front. Pharmacol. 2016, 7, 229. [Google Scholar] [CrossRef]
- Anderson, K.P. Sympathetic nervous system activity and ventricular tachyarrhythmias: Recent advances. Ann. Noninvasive Electrocardiol. 2003, 8, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Crumb, W.; Cavero, I. QT interval prolongation by non-cardiovascular drugs: Issues and solutions for novel drug development. Pharm. Sci. Technol. Today 1999, 2, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xu, T.Y.; Li, Y.; Chia, Y.C.; Buranakitjaroen, P.; Cheng, H.M.; Van Huynh, M.; Sogunuru, G.P.; Tay, J.C.; Wang, T.D.; et al. Role of α1-blockers in the current management of hypertension. J. Clin. Hypertens. 2022, 24, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- da Silva, S.B.; Feitosa, S.G.D.; de, L. Alves, S.M.; Santos, R.C.A.; dos Anjos, J.V.; Araújo, A.V. A Concise and Useful Guide to Understand How Alpha1 Adrenoceptor Antagonists Work. Mini Rev. Med. Chem. 2022, 22, 2383–2405. [Google Scholar] [CrossRef]
- Chang, K.C. Hypertensive effects of methoxamine on arterial mechanics in rats: Analysis based on exponentially tapered T-tube model. Eur. J. Pharmacol. 1998, 350, 195–202. [Google Scholar] [CrossRef]
- Kowalski, P.; Jaśkowska, J.; Bojarski, A.J.; Duszyåska, B.; Bucki, A.; Koåaczkowski, M. Evaluation of 1-arylpiperazine derivative of hydroxybenzamides as 5-HT1A and 5-HT7 serotonin receptor ligands: An experimental and molecular modeling approach. J. Heterocycl. Chem. 2011, 48, 192–198. [Google Scholar] [CrossRef]
- Jaśkowska, J.; Drabczyk, A.K.; Śliwa, P.; Jodłowski, P.; Pindelska, E.; Kułaga, D.; Zaręba, P.; Majka, Z.; Siwek, A.; Wolak, M.; et al. Ultrasound assisted one-pot synthesis and preliminary in vitro studies of salicylamide arylpiperazines as dual 5-HT1A/5-HT7 ligands. J. Mol. Struct. 2022, 1275, 134585. [Google Scholar] [CrossRef]
- Zaręba, P.; Dudek, M.; Lustyk, K.; Siwek, A.; Starowicz, G.; Bednarski, M.; Nowiński, L.; Raźny, K.; Sapa, J.; Malawska, B.; et al. α-Adrenoceptor antagonistic and hypotensive properties of novel arylpiperazine derivatives of pyrrolidin-2-one. Bioorg. Med. Chem. 2015, 23, 2104–2111. [Google Scholar] [CrossRef]
- Szekeres, L.; Papp, J. “Experimental cardiac arrhythmias” in Experimental Production of Diseases, Part 3, Heart and Circulation, Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 1975. [Google Scholar]
- Sapa, J.; Nowaczyk, A.; Kulig, K. Antiarrhythmic and antioxidant activity of novel pyrrolidin-2-one derivatives with adrenolytic properties. Naunyn. Schmiedebergs. Arch. Pharmacol. 2011, 383, 13–25. [Google Scholar] [CrossRef]
- Savalia, S.; Acosta, E.; Emamian, V.; Savalia, S.; Acosta, E.; Emamian, V. Classification of Cardiovascular Disease Using Feature Extraction and Artificial Neural Networks. J. Biosci. Med. 2017, 5, 64–79. [Google Scholar] [CrossRef][Green Version]
- Ghorbani Afkhami, R.; Azarnia, G.; Tinati, M.A. Cardiac arrhythmia classification using statistical and mixture modeling features of ECG signals. Pattern Recognit. Lett. 2016, 70, 45–51. [Google Scholar] [CrossRef]
- Kubacka, M.; Mogilski, S.; Filipek, B.; Marona, H. The hypotensive activity and alpha1-adrenoceptor antagonistic properties of some aroxyalkyl derivatives of 2-methoxyphenylpiperazine. Eur. J. Pharmacol. 2013, 698, 335–344. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Adrenergic Receptors—pKi | |
|---|---|---|
| α1 a | α2 b | |
| JJGW01 | 8.40 ± 0.01 | 6.13 ± 0.02 |
| JJGW02 | 8.33 ± 0.02 | 6.20 ± 0.02 |
| JJGW03 | 8.11 ± 0.01 | 5.76 ± 0.02 |
| JJGW07 | 7.85 ± 0.01 | n.a. |
| JJGW11 | 8.07 ± 0.04 | n.a. |
| JJGW12 | 7.41 ± 0.01 | 6.11 ± 0.01 |
| Phentolamine | 8.05 ± 0.01 | - |
| Clonidine | - | 8.30 ± 0.01 |
| Treatment | Dose (mg/kg) | Fibrillations | Extrasystoles | Bradycardia | Blocks | Mortality |
|---|---|---|---|---|---|---|
| Adrenaline-induced arrhythmia | ||||||
| Control | - | - | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW01 | 0.25 | - | 4/6 | 2/6 | 4/6 | 1/6 |
| 0.1 | - | 5/6 | 3/6 | 5/6 | 0/6 | |
| 0.05 | - | 6/6 | 6/6 | 6/6 | 4/6 | |
| JJGW02 | 1 | - | 5/6 | 4/6 | 5/6 | 1/6 |
| 0.5 | - | 5/6 | 5/6 | 6/6 | 0/6 | |
| 0.25 | - | 5/6 | 5/6 | 5/6 | 3/6 | |
| JJGW03 | 1 | - | 4/5 | 1/5 | 4/5 | 0/5 |
| 0.5 | - | 4/5 | 4/5 | 5/5 | 4/5 | |
| 0.25 | - | 5/5 | 5/5 | 5/5 | 4/5 | |
| JJGW07 | 0.1 | - | 4/6 | 3/6 | 3/6 | 0/6 |
| 0.05 | - | 5/6 | 4/6 | 4/6 | 0/6 | |
| 0.02 | - | 5/6 | 6/6 | 6/6 | 3/6 | |
| JJGW11 | 0.5 | - | 3/6 | 2/6 | 1/6 | 1/6 |
| 0.25 | - | 6/6 | 0/6 | 6/6 | 0/6 | |
| 0.1 | - | 4/5 | 2/5 | 4/5 | 1/5 | |
| JJGW12 | 1 | - | 3/5 | 1/5 | 3/5 | 0/5 |
| 0.5 | - | 4/5 | 3/5 | 4/5 | 0/5 | |
| 0.25 | - | 6/6 | 5/6 | 6/6 | 3/6 | |
| Calcium chloride-induced arrhythmia | ||||||
| Control | - | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW01 | 5 | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW02 | 5 | 4/6 | 5/6 | 6/6 | 5/6 | 6/6 |
| JJGW03 | 5 | 4/6 | 6/6 | 6/6 | 6/6 | 5/6 |
| JJGW07 | 5 | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW11 | 5 | 6/6 | 5/6 | 6/6 | 6/6 | 6/6 |
| JJGW12 | 5 | 4/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| Aconitine-induced arrhythmia | ||||||
| Control | - | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW01 | 5 | 6/6 | 5/6 | 6/6 | 6/6 | 6/6 |
| JJGW02 | 5 | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW03 | 5 | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW07 | 5 | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 |
| JJGW11 | 5 | 4/6 | 5/6 | 6/6 | 6/6 | 6/6 |
| JJGW12 | 5 | 5/6 | 6/6 | 6/6 | 5/6 | 6/6 |
| Treatment | ED50 (mg/kg) |
|---|---|
| JJGW01 | 0.10 (0.03–0.36) |
| JJGW02 | 0.45 (0.11–1.77) |
| JJGW03 | 0.36 (0.08–1.56) |
| JJGW07 | 0.04 (0.01–0.15) |
| JJGW11 | 0.19 (0.08–0.45) |
| JJGW12 | 0.44 (0.10–1.98) |
| Treatment | Dose (mg/kg) | Bradycardia | Blocks | Mortality |
|---|---|---|---|---|
| Control | - | 6/6 | 5/6 | 4/6 |
| JJGW01 | 1 | 2/5 | 3/5 | 0/5 |
| JJGW02 | 5 | 2/6 | 1/6 | 1/6 |
| JJGW03 | 5 | 1/5 | 3/5 | 0/5 |
| JJGW07 | 1 | 1/5 | 2/5 | 0/5 |
| JJGW11 | 1 | 1/5 | 2/5 | 0/5 |
| JJGW12 | 5 | 6/6 | 6/6 | 6/6 |
| Treatment | Parameters | Time of Observation (min) | |||
|---|---|---|---|---|---|
| 0 | 5 | 10 | 15 | ||
| JJGW01 | PQ | 42.3 ± 3.4 | 42.3 ± 2.0 | 41.3 ± 2.4 | 41.0 ± 3.3 |
| QRS | 49.3 ± 7.8 | 46.7 ± 5.6 | 48.0 ± 4.2 | 50.3 ± 4.6 | |
| QTc | 196.0 ± 14.2 | 193.7 ± 14.9 | 186.6 ± 9.0 | 190.6 ± 14.5 | |
| HR | 311.8 ± 11.6 | 318.0 ± 28.5 | 324.6 ± 23.1 | 324.0 ± 23.1 | |
| JJGW02 | PQ | 42.6 ± 2.0 | 41.7 ± 1.8 | 42.2 ± 1.6 | 44.8 ± 5.9 |
| QRS | 36.0 ± 1.1 | 35.2 ± 1.2 | 36.1 ± 1.8 | 35.2 ± 0.7 | |
| QTc | 183.3 ± 7.1 | 175.4 ± 14.0 | 173.2 ± 15.7 | 175.1 ± 16.0 | |
| HR | 311.1 ± 24.4 | 278.7 ± 37.0 * | 265.0 ± 30.1 *** | 262.0 ± 37.3 *** | |
| JJGW03 | PQ | 41.6 ± 2.3 | 41.4 ± 1.6 | 40.2 ± 1.7 | 40.0 ± 0.5 |
| QRS | 39.6 ± 4.7 | 39.3 ± 3.9 | 40.8 ± 7.1 | 40.4 ± 5.2 | |
| QTc | 177.6 ± 12.0 | 188.7 ± 16.3 | 174.8 ± 7.3 | 178.1 ± 15.0 | |
| HR | 286.6 ± 45.7 | 289.1 ± 20.2 | 279.9 ± 15.7 | 271.9 ± 18.2 | |
| JJGW07 | PQ | 40.7 ± 2.1 | 40.0 ± 2.2 | 40.7 ± 3.7 | 40.7 ± 1.6 |
| QRS | 47.0 ± 6.3 | 49.7 ± 7.9 | 48.7 ± 7.2 | 48.7 ± 9.2 | |
| QTc | 196.5 ± 8.0 | 190.8 ± 4.2 | 196.3 ± 9.5 | 192.4 ± 7.5 | |
| HR | 328.7 ± 9.3 | 341.2 ± 11.5 | 333.2 ± 20.9 | 336.3 ± 20.9 | |
| JJGW11 | PQ | 45.8 ± 7.2 | 47.1 ± 5.7 | 47.4 ± 5.0 | 47.6 ± 5.1 |
| QRS | 38.5 ± 3.6 | 41.3 ± 3.0 | 42.4 ± 4.3 | 41.7 ± 5.4 | |
| QTc | 188.2 ± 12.3 | 197.3 ± 18.6 | 193.6 ± 22.0 | 184.1 ± 16.9 | |
| HR | 281.3 ± 50.8 | 266.5 ± 58.2 | 258.8 ± 55.0 ** | 252.4 ± 50.3 *** | |
| JJGW12 | PQ | 44.1 ± 6.2 | 43.6 ± 1.2 | 45.9 ± 2.4 | 45.5 ± 3.1 |
| QRS | 41.9 ± 2.1 | 44.5 ± 3.6 | 44.2 ± 2.3 | 45.2 ± 5.9 | |
| QTc | 190.8 ± 15.2 | 194.3 ± 16.8 | 190.3 ± 25.9 | 195.8 ± 25.5 | |
| HR | 254.6 ± 41.2 | 256.8 ± 47.1 | 255.2 ± 53.6 | 250.2 ± 51.5 | |
| Treatment | Dose (mg/kg) | Blood Pressure | Time of Observation (min) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 5 | 10 | 20 | 30 | 40 | 50 | 60 | |||
| Control | - | SBP | 127.5 ± 8.0 | 128.7 ± 8.6 | 126.2 ± 5.9 | 124.3 ± 5.7 | 120.5 ± 4.7 | 120.0 ± 7.0 | 123.5 ± 7.8 | 121.3 ± 7.4 |
| - | DBP | 92.2 ± 6.0 | 94.2 ± 5.7 | 92.2 ± 5.7 | 90.3 ± 5.9 | 88.8 ± 5.0 | 90.2 ± 11.4 | 87.3 ± 5.7 | 90.2 ± 11.9 | |
| JJGW01 | 0.5 | SBP | 130.7 ± 14.9 | 119.0 ± 13.4 | 115.7 ± 13.0 | 114.7 ± 8.8 | 114.5 ± 10.2 | 115.2 ± 12.6 | 116.8 ± 17.3 | 113.8 ± 16.1 |
| 1.0 | 112.5 ± 11.6 | 102.5 ± 9.5 d | 100.3 ± 10.4 d | 99.7 ± 11.3 c | 98.2 ± 10.4 c | 95.7 ± 13.3 c | 95.5 ± 11.2 d | 96.5 ± 10.6 c | ||
| 0.5 | DBP | 95.3 ± 12.6 | 88.5 ± 14.3 | 85.0 ± 13.6 | 84.8 ± 8.5 | 84.3 ± 6.9 | 86.0 ± 10.3 | 88.3 ± 15.3 | 86.8 ± 15.5 | |
| 1.0 | 87.7 ± 11.2 | 80.2 ± 10.8 | 79.0 ± 11.9 | 77.5 ± 12.1 | 75.7 ± 10.6 | 73.8 ± 14.0 a | 72.7 ± 11.6 | 73.2 ± 11.3 a | ||
| JJGW02 | 1.0 | SBP | 118.0 ± 10.5 | 113.7 ± 8.7 | 111.2 ± 6.4 | 109.7 ± 9.1 | 105.7 ± 7.5 | 107.7 ± 11.5 | 108.7 ± 12.9 | 111.0 ± 18.0 |
| 2.5 | 114.3 ± 15.7 | 103.2 ± 13.0 c | 104.2 ± 13.2 b | 102.8 ± 13.4 b | 103.7 ± 10.8 a | 106.5 ± 10.6 | 103.2 ± 9.4 b | 105.2 ± 9.7 a | ||
| 1.0 | DBP | 87.7 ± 14.9 | 82.7 ± 16.0 | 83.3 ± 10.3 | 80.0 ± 14.1 | 73.7 ± 10.6 | 75.0 ± 13.2 | 73.7 ± 13.9 | 76.7 ± 19.2 | |
| 2.5 | 84.8 ± 12.1 | 72.0 ± 9.4 c | 72.8 ± 11.6 b | 73.0 ± 9.6 b | 72.3 ± 8.1 a | 73.8 ± 9.4 a | 73.7 ± 8.7 | 73.7 ± 7.9 a | ||
| JJGW03 | 2.5 | SBP | 123.8 ± 17.4 | 112.5 ± 13.8 | 109.8 ± 13.5 | 108.8 ± 15.6 | 111.8 ± 20.5 | 111.2 ± 22.3 | 107.7 ± 19.7 | 109.2 ± 21.9 |
| 5.0 | 128.5 ± 8.6 | 108.0 ± 6.6 d | 104.3 ± 6.3 d | 101.3 ± 4.5 d | 102.3 ± 6.9 d | 104.3 ± 3.9b | 106.0 ± 7.9 c | 107.3 ± 6.1 b | ||
| 2.5 | DBP | 89.3 ± 15.6 | 83.3 ± 12.8 | 84.8 ± 14.7 | 86.0 ± 15.8 | 85.5 ± 14.7 | 83.7 ± 15.6 | 81.2 ± 15.0 | 79.5 ± 15.4 | |
| 5.0 | 101.5 ± 6.1 | 83.2 ± 5.0 a | 81.2 ± 4.0 a | 82.0 ± 4.2 | 83.5 ± 4.3 | 85.5 ± 5.8 | 86.7 ± 6.0 | 87.5 ± 6.3 | ||
| JJGW07 | 2.5 | SBP | 120.0 ± 9.3 | 116.5 ± 9.6 | 112.0 ± 9.7 | 110.2 ± 10.0 | 108.0 ± 10.8 | 106.3 ± 12.9 | 109.5 ± 9.1 | 112.0 ± 9.9 |
| 5.0 | 117.7 ± 2.6 | 113.8 ± 5.6 c | 109.5 ± 5.7c | 105.2 ± 6.3 d | 102.8 ± 6.9 d | 104.7 ± 5.7c | 104.7 ± 5.7 d | 104.3 ± 5.6 c | ||
| 2.5 | DBP | 92.7 ± 11.7 | 89.0 ± 11.9 | 84.7 ± 12.1 | 81.7 ± 13.0 | 80.2 ± 14.4 | 78.7 ± 16.1 | 77.5 ± 16.7 | 76.3 ± 18.0 | |
| 5.0 | 85.3 ± 4.1 | 88.5 ± 6.2 | 84.2 ± 6.7 | 81.2 ± 5.3 | 79.2 ± 5.3 | 80.3 ± 2.9 | 79.8 ± 2.5 | 80.0 ± 2.1 | ||
| JJGW11 | 1.0 | SBP | 118.2 ± 9.7 | 116.2 ± 8.5 | 113.8 ± 9.2 | 111.5 ± 10.4 | 111.0 ± 10.8 | 110.0 ± 11.5 | 110.3 ± 10.7 | 110.8 ± 10.6 |
| 2.5 | 116.7 ± 8.1 | 108.5 ± 8.7 b | 103.3 ± 9.5c | 102.3 ± 10.0 c | 101.3 ± 9.2 b | 103.0 ± 10.3 a | 103.5 ± 12.9 b | 100.2 ± 15.9 b | ||
| 1.0 | DBP | 86.8 ± 7.6 | 81.3 ± 14.4 | 82.0 ± 10.2 | 82.3 ± 8.8 | 83.0 ± 8.2 | 82.5 ± 8.4 | 81.7 ± 8.3 | 81.5 ± 8.4 | |
| 2.5 | 88.7 ± 10.4 | 84.7 ± 10.0 | 81.2 ± 8.6 | 78.5 ± 10.1 | 77.3 ± 9.9 | 79.2 ± 10.5 | 77.7 ± 12.9 | 73.0 ± 16.2 a | ||
| JJGW12 | 2.5 | SBP | 122.2 ± 15.6 | 120.7 ± 13.8 | 114.5 ± 10.6 | 109.7 ± 9.3 | 106.5 ± 13.1 | 108.8 ± 11.8 | 110.0 ± 7.5 | 110.5 ± 8.1 |
| 5.0 | 122.5 ± 11.9 | 120.7 ± 9.8 | 114.5 ± 9.1 | 112.8 ± 10.0 | 111.5 ± 10.4 | 113.0 ± 11.9 | 107.0 ± 12.7 a | 109.8 ± 12.2 | ||
| 2.5 | DBP | 95.0 ± 16.0 | 94.5 ± 16.5 | 87.5 ± 23.0 | 83.5 ± 22.4 | 84.0 ± 21.4 | 87.8 ± 16.7 | 89.3 ± 13.4 | 89.2 ± 13.9 | |
| 5.0 | 95.7 ± 6.0 | 87.7 ± 7.0 | 89.3 ± 8.1 | 88.5 ± 9.0 | 87.8 ± 8.8 | 87.8 ± 8.7 | 85.8 ± 8.1 | 86.7 ± 10.7 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żmudzka, E.; Lustyk, K.; Siwek, A.; Wolak, M.; Gałuszka, A.; Jaśkowska, J.; Kołaczkowski, M.; Sapa, J.; Pytka, K. Novel Arylpiperazine Derivatives of Salicylamide with α1-Adrenolytic Properties Showed Antiarrhythmic and Hypotensive Properties in Rats. Int. J. Mol. Sci. 2023, 24, 293. https://doi.org/10.3390/ijms24010293
Żmudzka E, Lustyk K, Siwek A, Wolak M, Gałuszka A, Jaśkowska J, Kołaczkowski M, Sapa J, Pytka K. Novel Arylpiperazine Derivatives of Salicylamide with α1-Adrenolytic Properties Showed Antiarrhythmic and Hypotensive Properties in Rats. International Journal of Molecular Sciences. 2023; 24(1):293. https://doi.org/10.3390/ijms24010293
Chicago/Turabian StyleŻmudzka, Elżbieta, Klaudia Lustyk, Agata Siwek, Małgorzata Wolak, Adam Gałuszka, Jolanta Jaśkowska, Marcin Kołaczkowski, Jacek Sapa, and Karolina Pytka. 2023. "Novel Arylpiperazine Derivatives of Salicylamide with α1-Adrenolytic Properties Showed Antiarrhythmic and Hypotensive Properties in Rats" International Journal of Molecular Sciences 24, no. 1: 293. https://doi.org/10.3390/ijms24010293
APA StyleŻmudzka, E., Lustyk, K., Siwek, A., Wolak, M., Gałuszka, A., Jaśkowska, J., Kołaczkowski, M., Sapa, J., & Pytka, K. (2023). Novel Arylpiperazine Derivatives of Salicylamide with α1-Adrenolytic Properties Showed Antiarrhythmic and Hypotensive Properties in Rats. International Journal of Molecular Sciences, 24(1), 293. https://doi.org/10.3390/ijms24010293