
The Benefits of Fibrinolysis Combined with Venous Systemic Oxygen Persufflation (VSOP) in a Rat Model of Donation after Circulatory Death and Orthotopic Liver Transplantation


 , and
, and
Abstract
:1. Introduction
2. Results
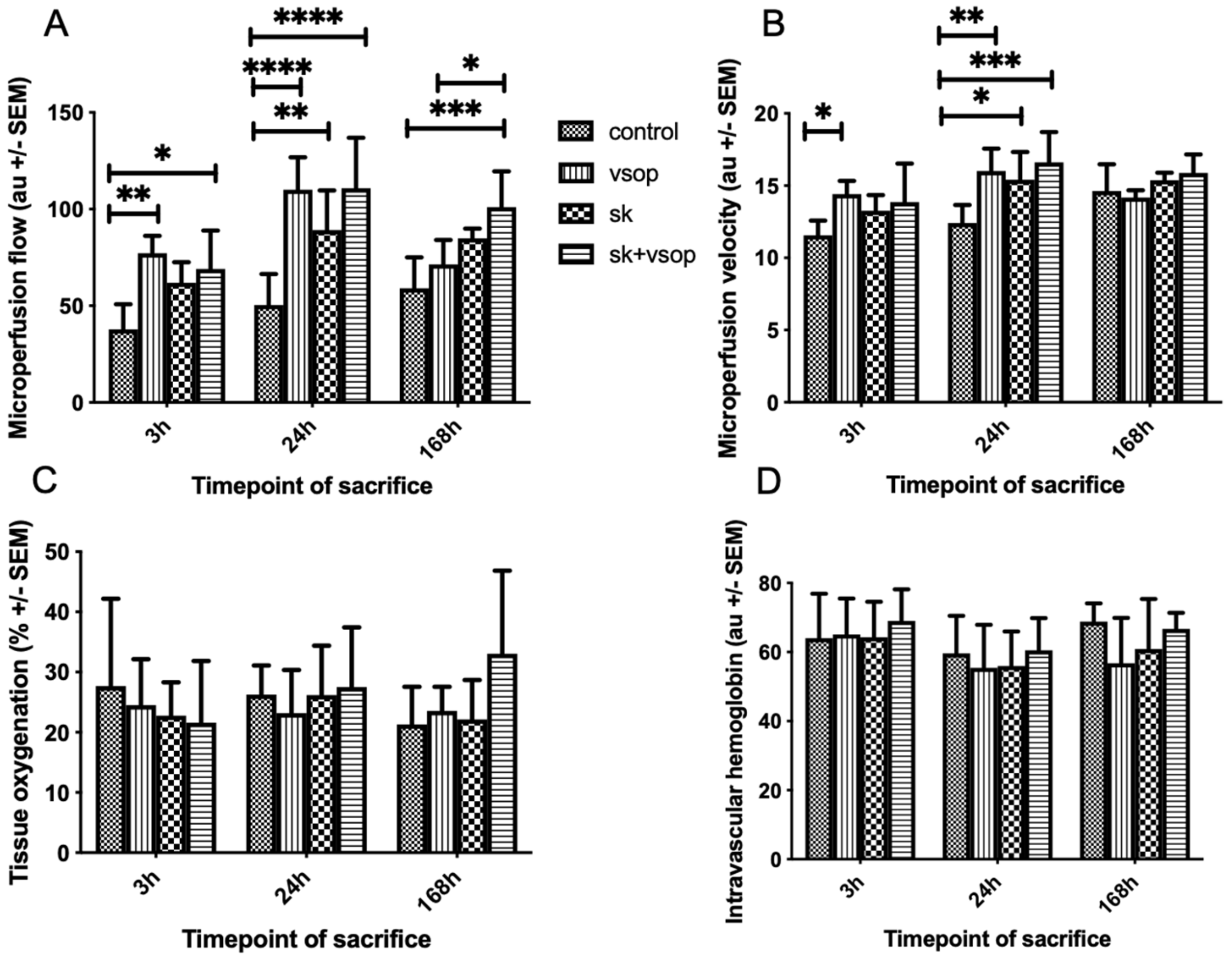
2.1. Evaluation of Microcirculatory Perfusion
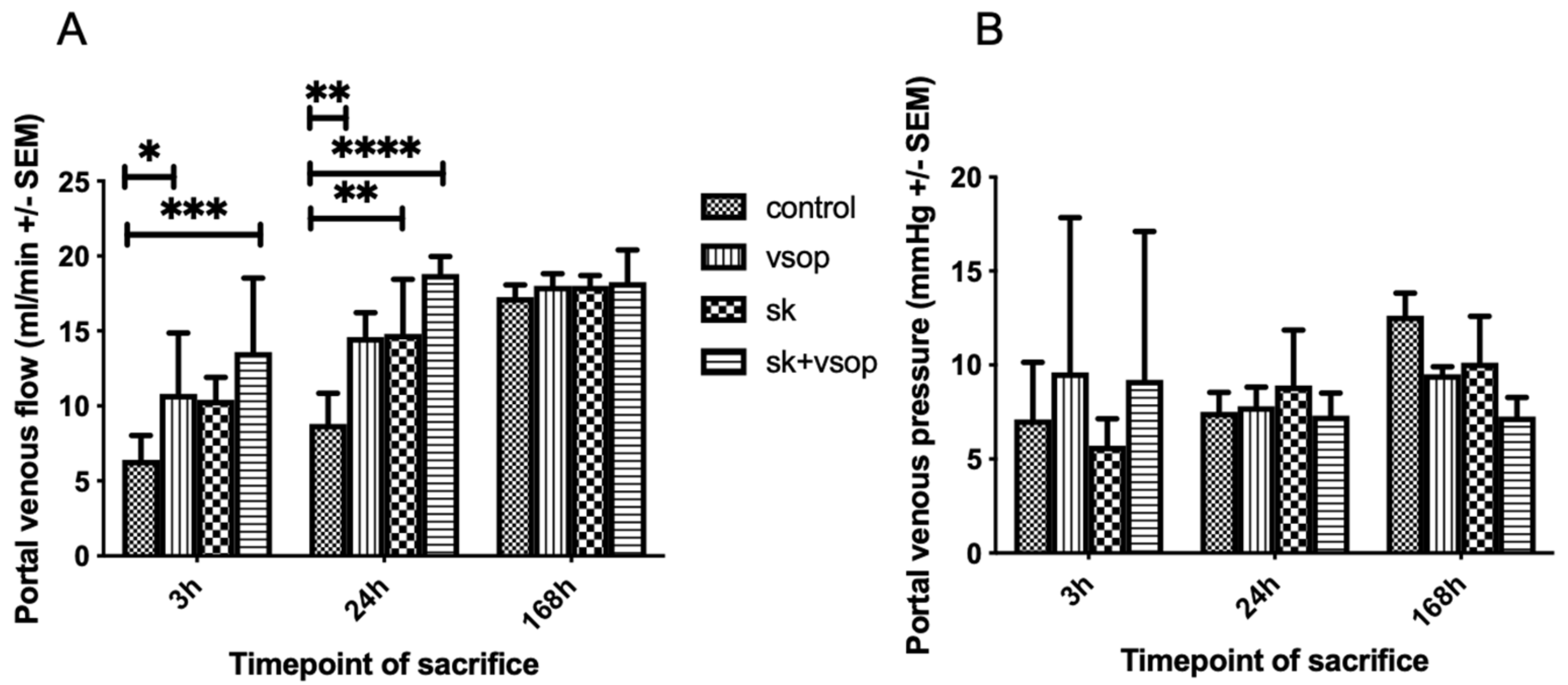
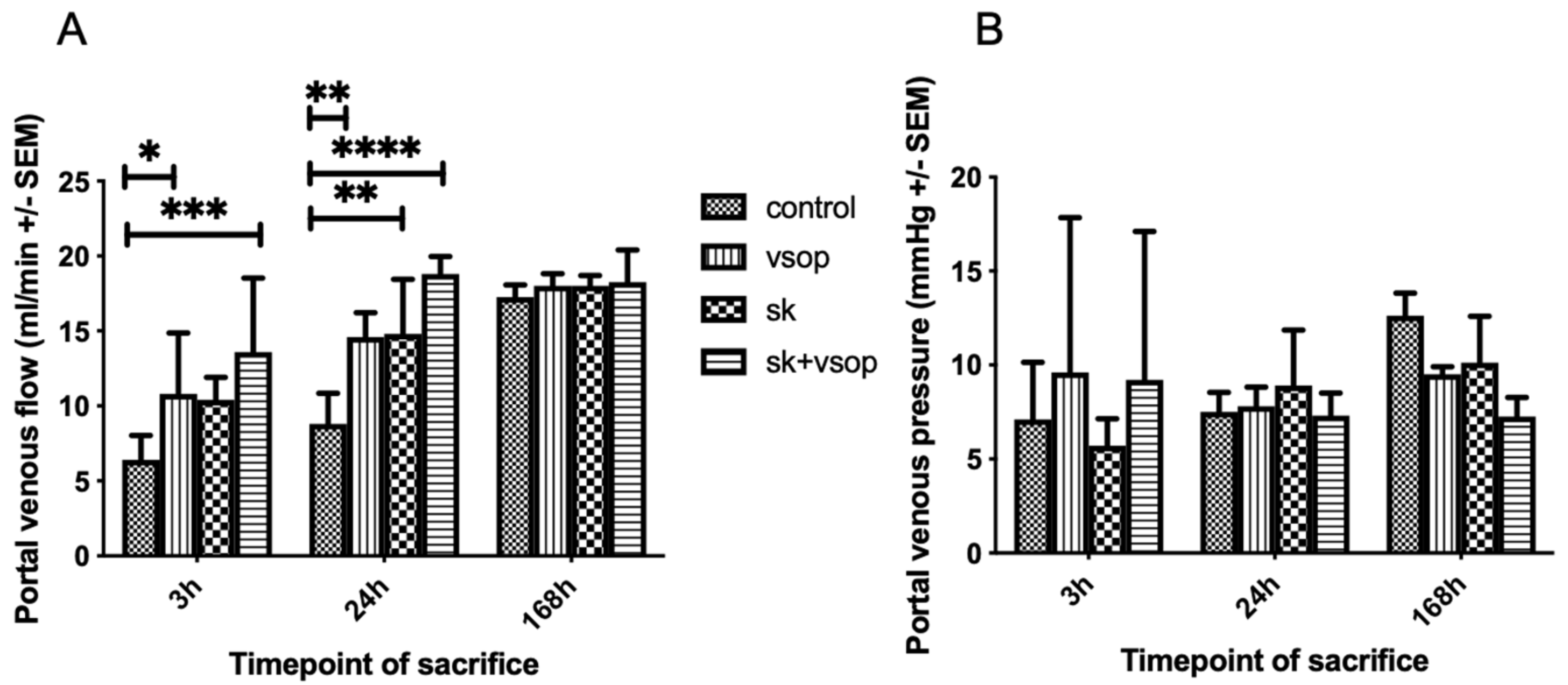
2.2. Evaluation of Portal Circulation
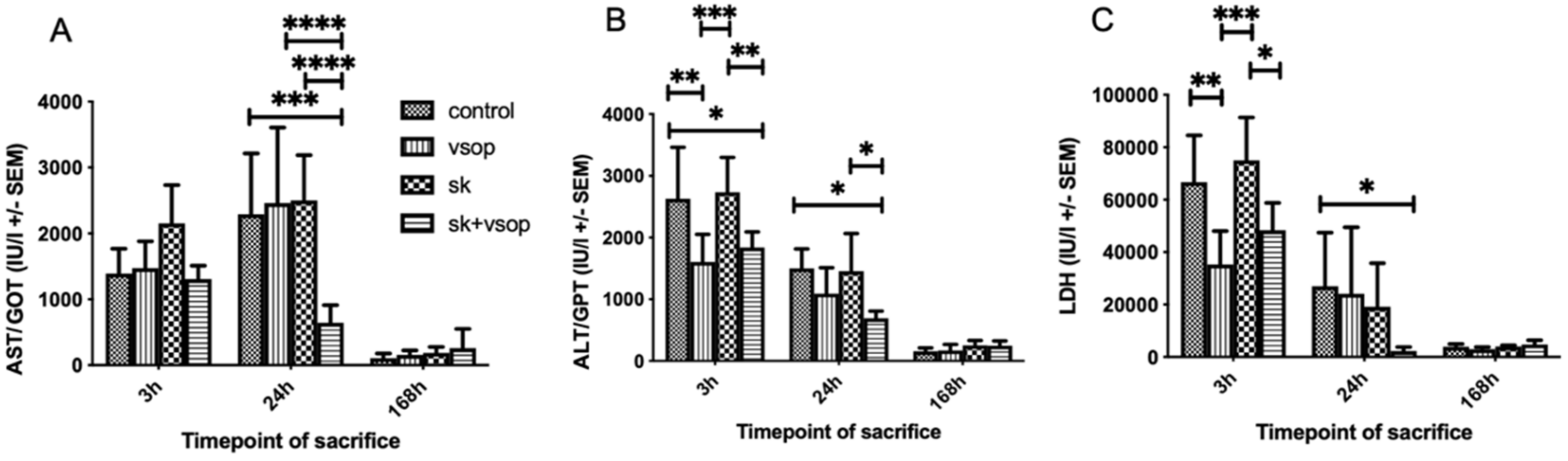
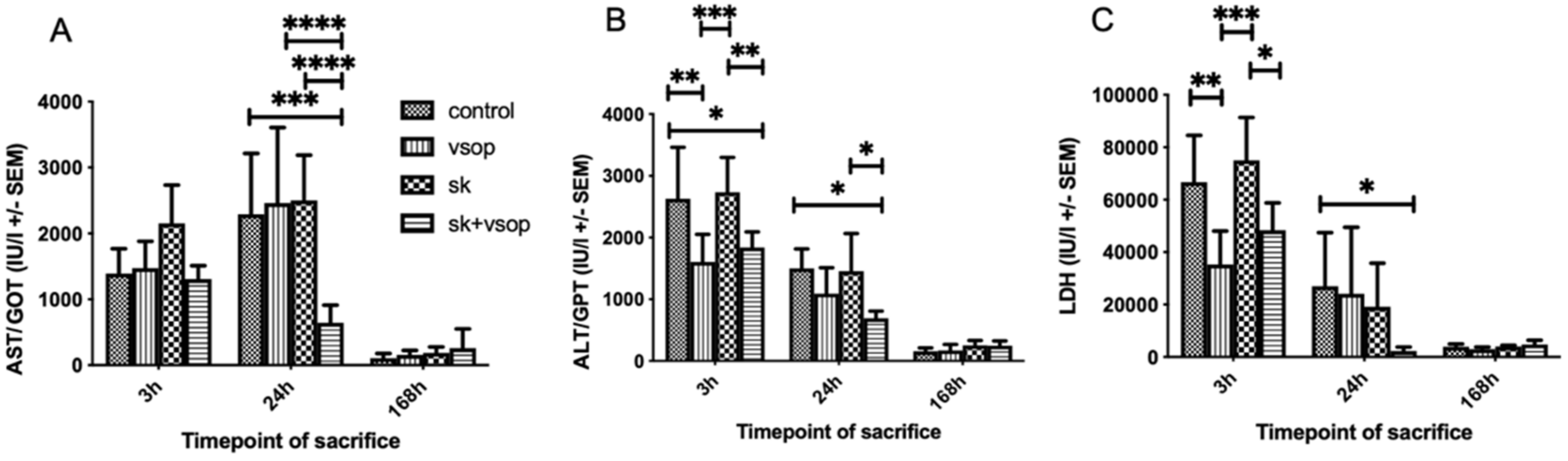
2.3. Serum GOT/AST, GPT/ALT, and LDH Measurements
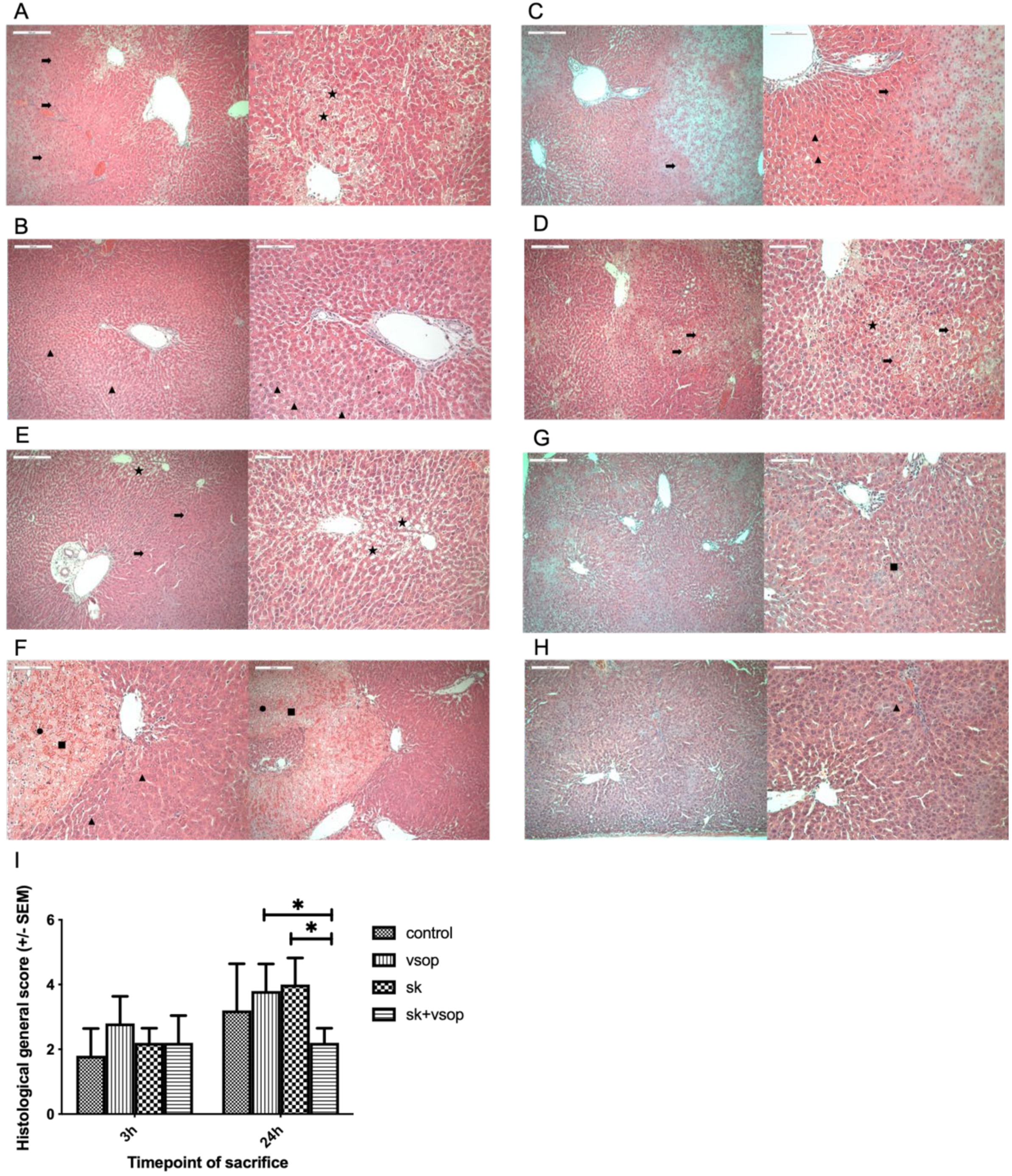
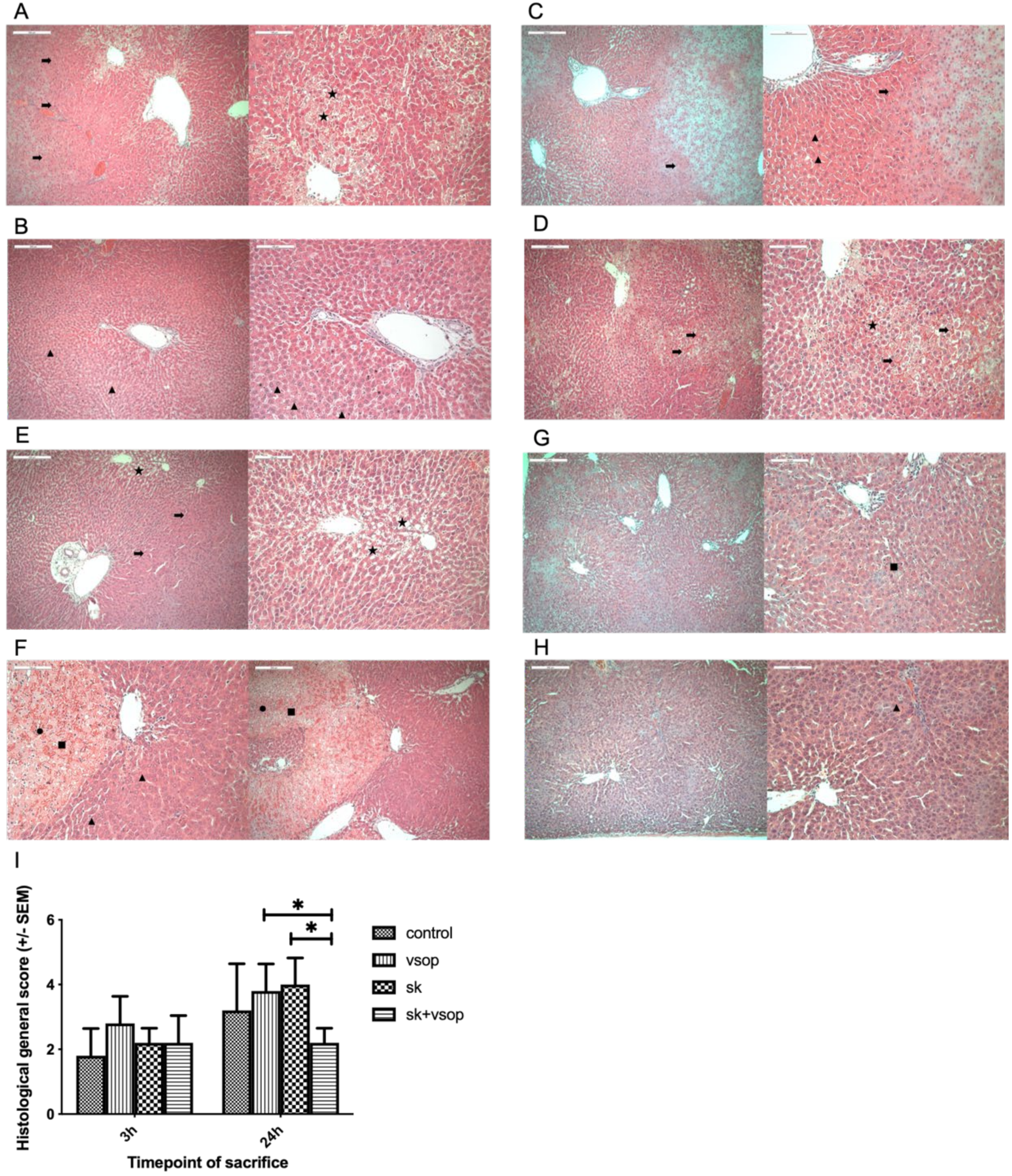
2.4. Histopathological Analysis
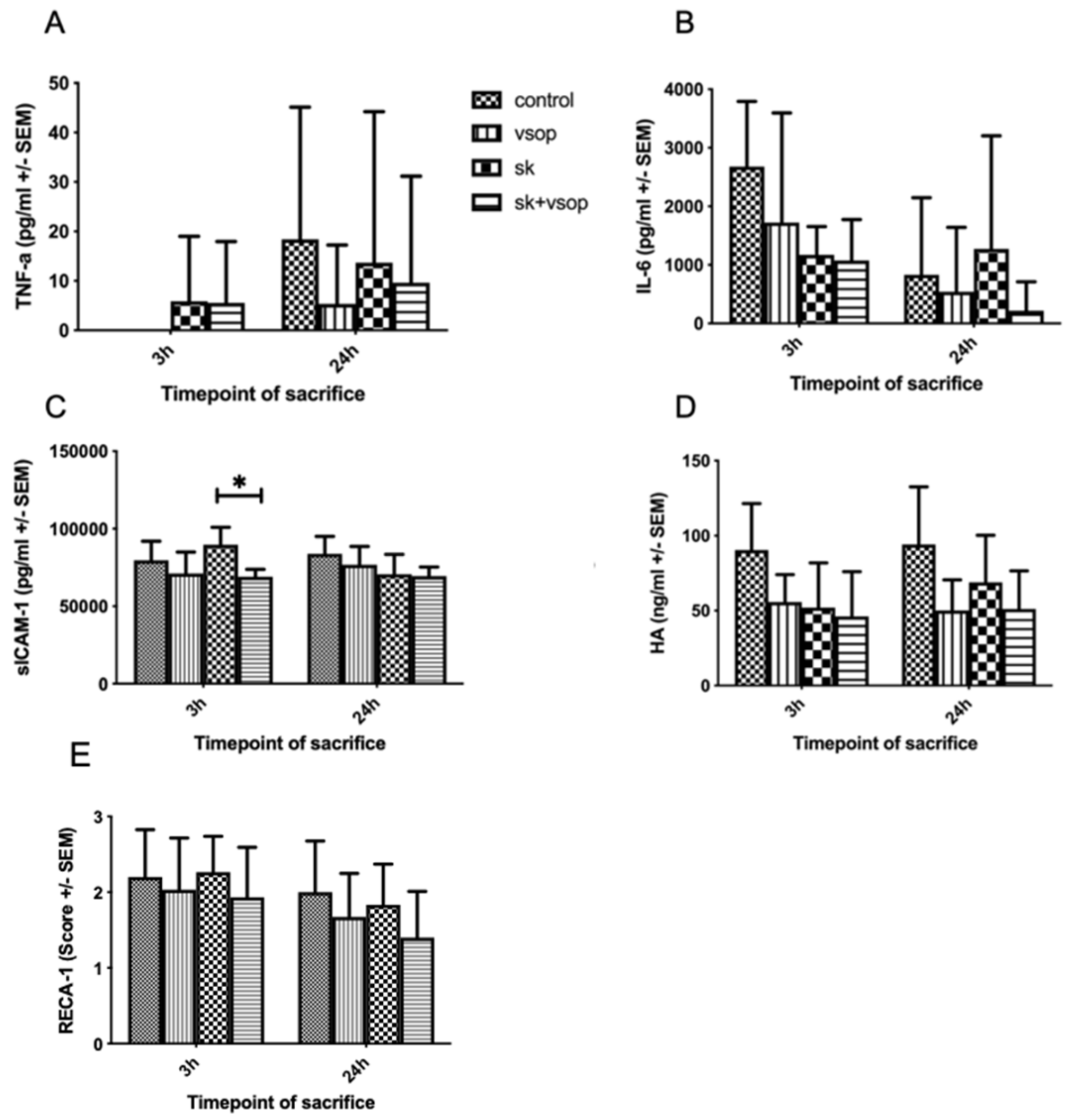
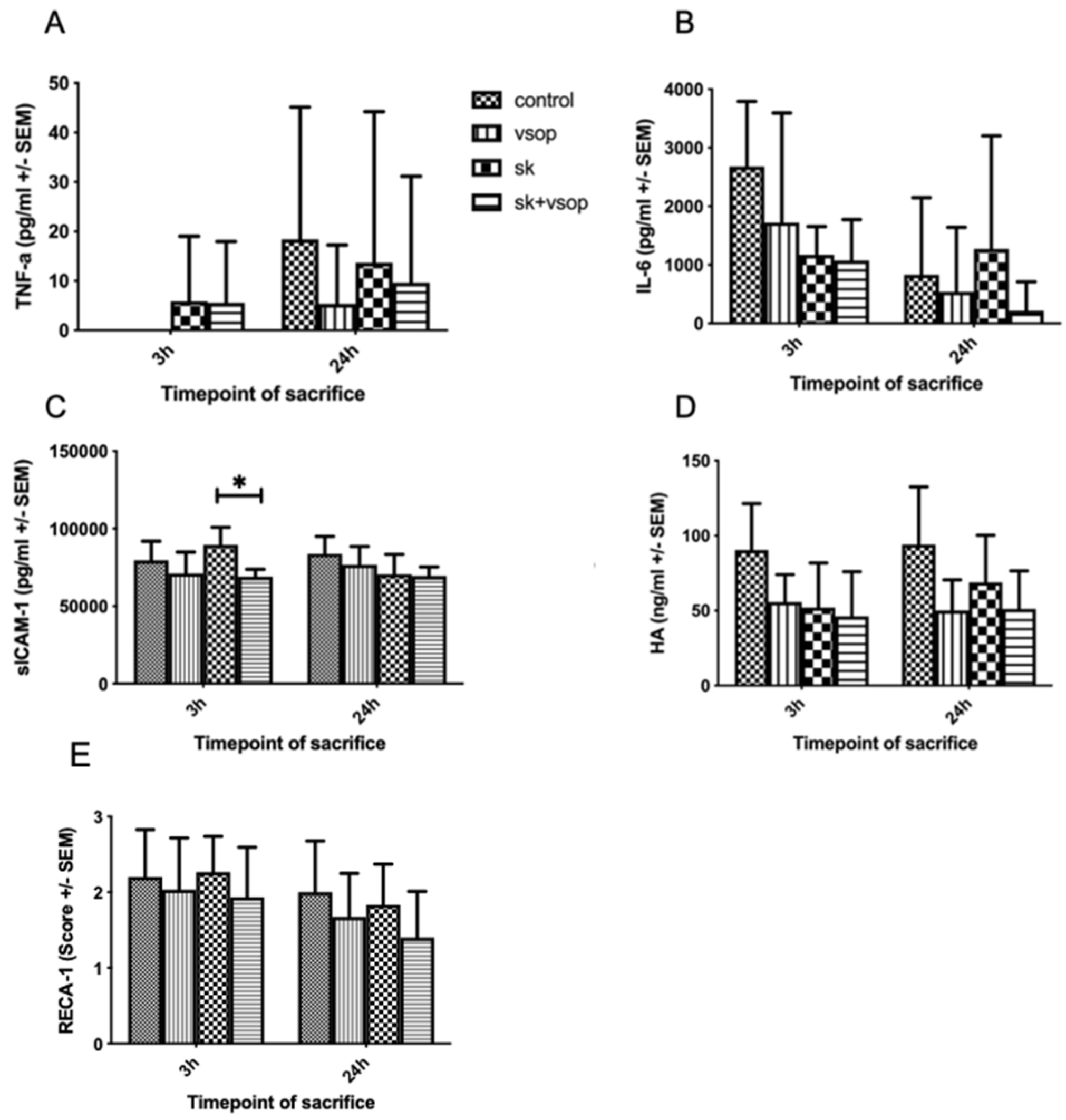
2.5. Serum TNF-α, IL-6, sICAM-1, HA and Immunohistochemical Analysis of RECA-1 Staining
3. Discussion
4. Materials and Methods
4.1. Animals
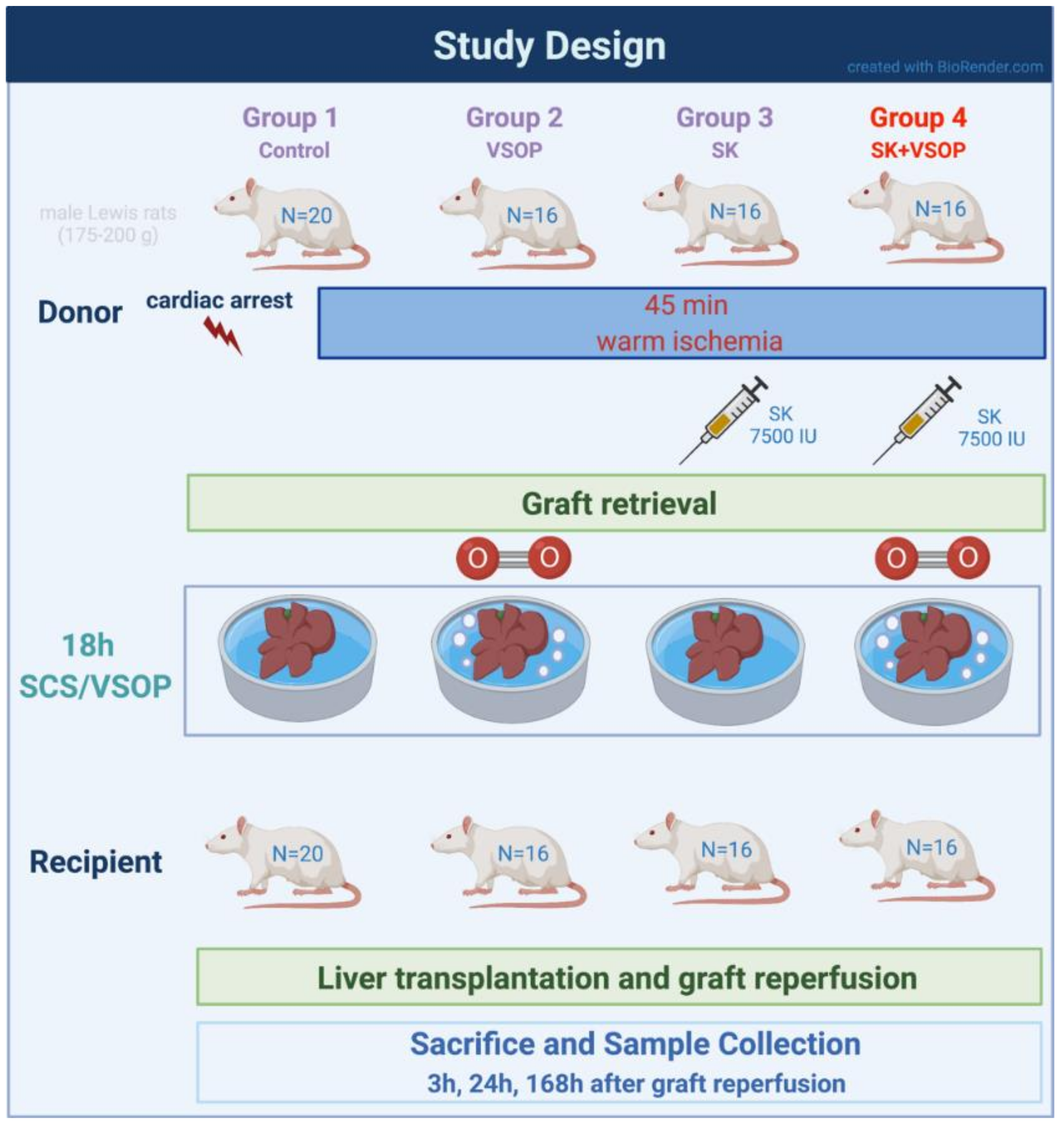
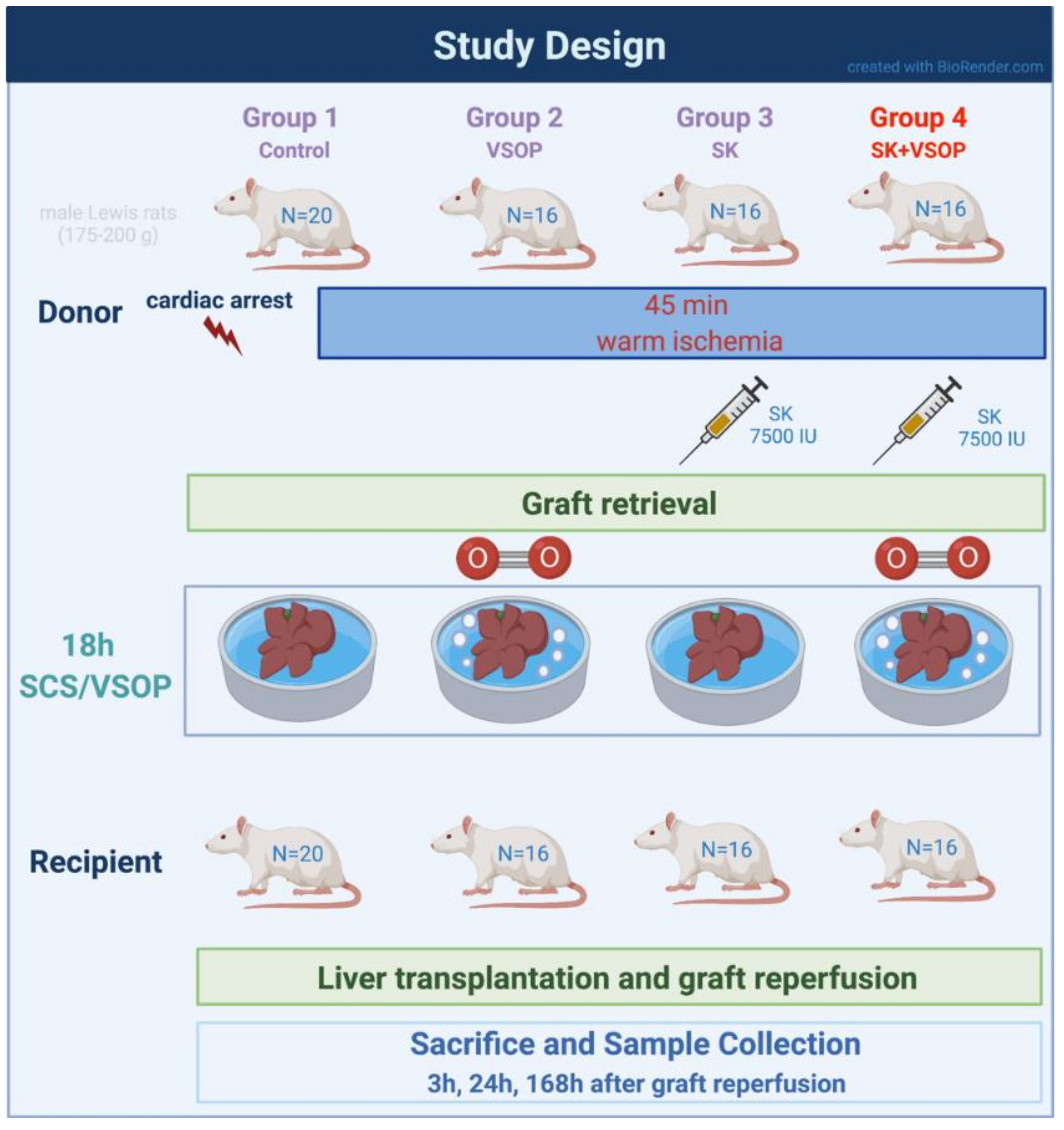
4.2. Experimental Groups and Design
4.3. Surgical Techniques
4.3.1. Donor Procedure
4.3.2. Ex Vivo Graft Preparation after Retrieval
4.3.3. Recipient Procedure
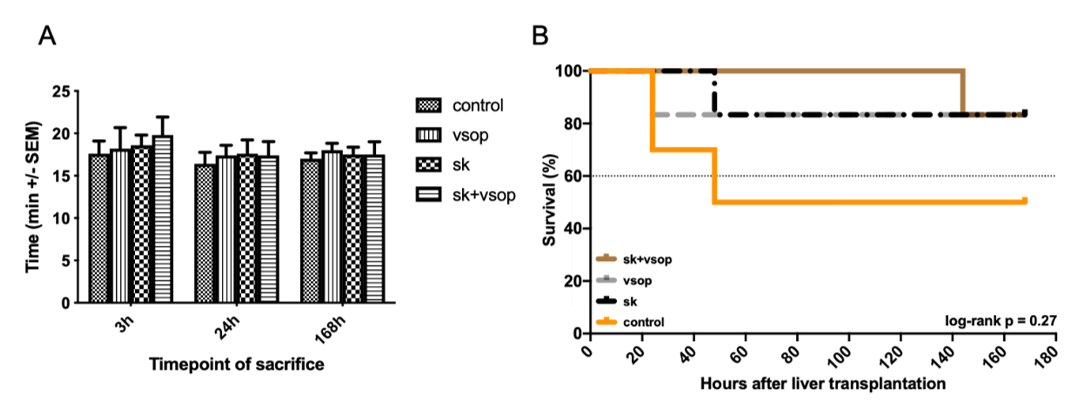
4.4. Anhepatic Time and Survival Estimate
4.5. Evaluation of Microcirculatory Perfusion
4.6. Evaluation of Portal Circulation
4.7. Serum GOT/AST, GPT/ALT, and LDH Measurements
4.8. Histopathological Analysis
4.9. ELISA Measurements of TNF-α, IL-6, sICAM-1, HA, and Immunohistochemical Analysis of RECA-1 Staining
4.10. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- White, S.A.; Prasad, K.R. Liver Transplantation from Non-Heart Beating Donors. BMJ 2006, 332, 376–377. [Google Scholar] [CrossRef]
- Czigany, Z.; Lurje, I.; Tolba, R.H.; Neumann, U.P.; Tacke, F.; Lurje, G. Machine Perfusion for Liver Transplantation in the Era of Marginal Organs-New Kids on the Block. Liver Int. 2019, 39, 228–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czigany, Z.; Tacke, F.; Lurje, G. Evolving Trends in Machine Liver Perfusion: Comments on Clinical End Points and Selection Criteria. Gastroenterology 2019, 157, 1166–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, R.M.; Youngner, S.J. Time Is of the Essence: The Pressing Need for Comprehensive Non-Heart-Beating Cadaveric Donation Policies. Transplant. Proc. 1995, 27, 2913–2917, discussion 2917-2921. [Google Scholar] [PubMed]
- Czigany, Z.; Lurje, I.; Schmelzle, M.; Schöning, W.; Öllinger, R.; Raschzok, N.; Sauer, I.M.; Tacke, F.; Strnad, P.; Trautwein, C.; et al. Ischemia-Reperfusion Injury in Marginal Liver Grafts and the Role of Hypothermic Machine Perfusion: Molecular Mechanisms and Clinical Implications. J. Clin. Med. 2020, 9, 846. [Google Scholar] [CrossRef] [Green Version]
- Czigany, Z.; Schöning, W.; Ulmer, T.F.; Bednarsch, J.; Amygdalos, I.; Cramer, T.; Rogiers, X.; Popescu, I.; Botea, F.; Froněk, J.; et al. Hypothermic Oxygenated Machine Perfusion (HOPE) for Orthotopic Liver Transplantation of Human Liver Allografts from Extended Criteria Donors (ECD) in Donation after Brain Death (DBD): A Prospective Multicentre Randomised Controlled Trial (HOPE ECD-DBD). BMJ Open 2017, 7, e017558. [Google Scholar] [CrossRef]
- Czigany, Z.; Pratschke, J.; Froněk, J.; Guba, M.; Schöning, W.; Raptis, D.A.; Andrassy, J.; Kramer, M.; Strnad, P.; Tolba, R.H.; et al. Hypothermic Oxygenated Machine Perfusion Reduces Early Allograft Injury and Improves Post-Transplant Outcomes in Extended Criteria Donation Liver Transplantation from donation after brain death: Results from a Multicenter Randomized Controlled Trial (HOPE ECD-DBD). Ann. Surg. 2021, 274, 705–712. [Google Scholar] [CrossRef]
- Casavilla, A.; Ramirez, C.; Shapiro, R.; Nghiem, D.; Miracle, K.; Fung, J.J.; Starzl, T.E. Liver and Kidney Transplantation from Non-Heart Beating Donors: The Pittsburgh Experience. Transplant. Proc. 1995, 27, 710–712. [Google Scholar]
- Jiménez-Castro, M.B.; Cornide-Petronio, M.E.; Gracia-Sancho, J.; Peralta, C. Inflammasome-Mediated Inflammation in Liver Ischemia-Reperfusion Injury. Cells 2019, 8, 1131. [Google Scholar] [CrossRef] [Green Version]
- Czigany, Z.; Bleilevens, C.; Beckers, C.; Stoppe, C.; Möhring, M.; Fülöp, A.; Szijarto, A.; Lurje, G.; Neumann, U.P.; Tolba, R.H. Limb Remote Ischemic Conditioning of the Recipient Protects the Liver in a Rat Model of Arterialized Orthotopic Liver Transplantation. PLoS ONE 2018, 13, e0195507. [Google Scholar] [CrossRef]
- Czigany, Z.; Craigie, E.C.; Lurje, G.; Song, S.; Yonezawa, K.; Yamamoto, Y.; Minor, T.; Tolba, R.H. Adenosine A2a Receptor Stimulation Attenuates Ischemia-Reperfusion Injury and Improves Survival in A Porcine Model of DCD Liver Transplantation. Int. J. Mol. Sci. 2020, 21, 6747. [Google Scholar] [CrossRef] [PubMed]
- Czigany, Z.; Hata, K.; Lai, W.; Schwandt, T.; Yamamoto, Y.; Uemoto, S.; Tolba, R.H. A Dual Protective Effect of Intestinal Remote Ischemic Conditioning in a Rat Model of Total Hepatic Ischemia. J. Clin. Med. 2019, 8, 1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czigány, Z.; Turóczi, Z.; Kleiner, D.; Lotz, G.; Homeyer, A.; Harsányi, L.; Szijártó, A. Neural Elements behind the Hepatoprotection of Remote Perconditioning. J. Surg. Res. 2015, 193, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Czigány, Z.; Turóczi, Z.; Ónody, P.; Harsányi, L.; Lotz, G.; Hegedüs, V.; Szijártó, A. Remote Ischemic Perconditioning Protects the Liver from Ischemia-Reperfusion Injury. J. Surg. Res. 2013, 185, 605–613. [Google Scholar] [CrossRef]
- Minor, T.; Saad, S.; Nagelschmidt, M.; Kötting, M.; Fu, Z.; Paul, A.; Isselhard, W. Successful Transplantation of Porcine Livers after Warm Ischemic Insult in Situ and Cold Preservation Including Postconditioning with Gaseous Oxygen. Transplantation 1998, 65, 1262–1264. [Google Scholar] [CrossRef]
- Yamauchi, J.; Schramm, R.; Richter, S.; Vollmar, B.; Menger, M.D.; Minor, T. Improvement of Microvascular Graft Equilibration and Preservation in Non-Heart-Beating Donors by Warm Preflush with Streptokinase1. Transplantation 2003, 75, 449–453. [Google Scholar] [CrossRef]
- Tolba, R.H.; Yonezawa, K.; Song, S.; Burger, C.; Minor, T. Synergistic Value of Fibrinolysis and Hypothermic Aerobic Preservation with Oxygen in the Protection of Livers from Non–Heart-Beating Donors: An Experimental Model. Transplant. Proc. 2004, 36, 2927–2930. [Google Scholar] [CrossRef]
- Daemen, J.W.; Kootstra, G.; Wijnen, R.M.; Yin, M.; Heineman, E. Nonheart-Beating Donors: The Maastricht Experience. Clin. Transpl. 1994, 27, 303–316. [Google Scholar]
- Kootstra, G.; Kievit, J.K.; Heineman, E. The Non Heart-Beating Donor. Br. Med. Bull. 1997, 53, 844–853. [Google Scholar] [CrossRef] [Green Version]
- Abt, P.L.; Desai, N.M.; Crawford, M.D.; Forman, L.M.; Markmann, J.W.; Olthoff, K.M.; Markmann, J.F. Survival Following Liver Transplantation from Non-Heart-Beating Donors. Ann. Surg. 2004, 239, 87–92. [Google Scholar] [CrossRef]
- Richter, S.; Yamauchi, J.-I.; Minor, T.; Vollmar, B.; Menger, M.D. Effect of warm ischemia time and organ perfusion technique on liver microvascular preservation in a non-heart-beating rat model. Transplantation 2000, 69, 20. [Google Scholar] [CrossRef] [PubMed]
- Vollmar, B.; Glasz, J.; Leiderer, R.; Post, S.; Menger, M.D. Hepatic Microcirculatory Perfusion Failure Is a Determinant of Liver Dysfunction in Warm Ischemia-Reperfusion. Am. J. Pathol. 1994, 145, 1421–1431. [Google Scholar] [PubMed]
- Yamauchi, J.-I.; Richter, S.; Vollmar, B.; Menger, M.D.; Minor, T. Warm preflush with streptokinase improves microvascular procurement and tissue integrity in liver graft retrieval from non-heart-beating donors. Transplantation 2000, 69, 1780–1784. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, J.; Richter, S.; Vollmar, B.; Menger, M.D.; Minor, T. Microcirculatory Perfusion Pattern during Harvest of Livers from Non–Heart-Beating Donors: Beneficial Effect of Warm Preflush with Streptokinase. Transplant. Proc. 2000, 32, 21–22. [Google Scholar] [CrossRef]
- Pezzati, D. Strategies to Optimize the Use of Marginal Donors in Liver Transplantation. World J. Hepatol. 2015, 7, 2636. [Google Scholar] [CrossRef]
- Minor, T.; Klauke, H.; Vollmar, B.; Menger, M.D.; Isselhard, W. Rat Liver Transplantation after Long-Term Preservation by Venous Systemic Oxygen Persufflation. Transplant. Proc. 1997, 29, 410–411. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving Bioscience Research Reporting: The ARRIVE Guidelines for Reporting Animal Research. PLoS Biol. 2010, 8, e1000412. [Google Scholar] [CrossRef] [PubMed]
- Czigány, Z.; Iwasaki, J.; Yagi, S.; Nagai, K.; Szijártó, A.; Uemoto, S.; Tolba, R.H. Improving Research Practice in Rat Orthotopic and Partial Orthotopic Liver Transplantation: A Review, Recommendation, and Publication Guide. Eur. Surg. Res. 2015, 55, 119–138. [Google Scholar] [CrossRef]
- Morton, D.; Griffiths, P. Guidelines on the Recognition of Pain, Distress and Discomfort in Experimental Animals and an Hypothesis for Assessment. Vet. Rec. 1985, 116, 431–436. [Google Scholar] [CrossRef]
- Kanzler, S.; Rix, A.; Czigany, Z.; Tanaka, H.; Fukushima, K.; Kögel, B.; Pawlowsky, K.; Tolba, R.H. Recommendation for Severity Assessment Following Liver Resection and Liver Transplantation in Rats: Part I. Lab. Anim. 2016, 50, 459–467. [Google Scholar] [CrossRef]
- Nagai, K.; Yagi, S.; Uemoto, S.; Tolba, R.H. Surgical Procedures for a Rat Model of Partial Orthotopic Liver Transplantation with Hepatic Arterial Reconstruction. J. Vis. Exp. 2013, 73, e4376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagi, S.; Doorschodt, B.M.; Afify, M.; Klinge, U.; Kobayashi, E.; Uemoto, S.; Tolba, R.H. Improved Preservation and Microcirculation with POLYSOL After Partial Liver Transplantation in Rats. J. Surg. Res. 2011, 167, e375–e383. [Google Scholar] [CrossRef] [PubMed]
- Streidl, T.; Karkossa, I.; Segura Muñoz, R.R.; Eberl, C.; Zaufel, A.; Plagge, J.; Schmaltz, R.; Schubert, K.; Basic, M.; Schneider, K.M.; et al. The Gut Bacterium Extibacter Muris Produces Secondary Bile Acids and Influences Liver Physiology in Gnotobiotic Mice. Gut Microbes 2021, 13, 1854008. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Approx. Areas without Lesions | Hemorrhage | Congestion | Inflammatory Cell Infiltration | Necrosis | Degenerative Changes | Biliary Epithelial Proliferation | Sinu. Endothelial/ Kupffer Cell Activation | General Score | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Granulocytes | Macrophages | Mononuclear Cells (Other) | Fatty Degeneration | Granularity of Cytoplasm | |||||||||
| 3 h | Control | 50 | 1 | 4 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 2 |
| 70 | 1 | 3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | ||
| 95 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| 85 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | ||
| 60 | 1 | 4 | 1 | 1 | 1 | 2 | 3 | 3 | 1 | 1 | 3 | ||
| Mean/SD | 72 +/− 18 | 1 | 3 +/− 1 | 1 | 1 | 1 | 1.2 +/− 0.44 | 1.4 +/− 0.89 | 1.8 +/− 0.84 | 1 | 1 | 1.8 +/− 0.84 | |
| 3 h | SK | 40 | 1 | 3 | 1 | 1 | 1 | 1 | 2 | 3 | 1 | 3 | 2 |
| 60 | 1 | 3 | 1 | 1 | 1 | 1 | 2 | 4 | 1 | 1 | 3 | ||
| 75 | 1 | 3 | 1 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 2 | ||
| 60 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | ||
| 75 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 3 | 1 | 1 | 2 | ||
| Mean/SD | 62 +/− 14 | 1 | 2.6 +/− 0.55 | 1 | 1 | 1 | 1 | 1.6 +/− 0.55 | 3 +/− 0.71 | 1 | 1.4 +/− 0.89 | 2.2 +/− 0.45 | |
| SK + VSOP | 40 | 2 | 4 | 2 | 1 | 1 | 2 | 2 | 2 | 1 | 1 | 3 | |
| 3 h | 70 | 1 | 3 | 1 | 1 | 1 | 2 | 2 | 2 | 1 | 1 | 3 | |
| 85 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | ||
| 80 | 1 | 3 | 1 | 1 | 1 | 1 | 3 | 2 | 1 | 1 | 2 | ||
| 90 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | ||
| Mean/SD | 73 +/− 19 | 1.2 +/− 0.45 | 2.8 +/− 0.84 | 1.2 +/− 0.45 | 1 | 1 | 1.4 +/− 0.55 | 2.2 +/− 0.45 | 2 | 1 | 1 | 2.2 +/− 0.84 | |
| VSOP | 90 | 1 | 3 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | |
| 3 h | 60 | 1 | 3 | 1 | 1 | 1 | 2 | 2 | 2 | 1 | 1 | 3 | |
| 60 | 2 | 4 | 3 | 1 | 1 | 4 | 2 | 3 | 1 | 1 | 4 | ||
| 60 | 1 | 3 | 1 | 1 | 1 | 3 | 2 | 3 | 1 | 2 | 3 | ||
| 85 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | ||
| Mean/SD | 71 +/− 15 | 1.2 +/− 0.45 | 3 +/− 0.71 | 1.4 +/− 0.89 | 1 | 1 | 2.2 +/− 1.30 | 2 | 2.4 +/− 0.55 | 1 | 1.2 +/− 0.45 | 2.8 +/− 0.84 | |
| Control | 95 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 2 | 1 | |
| 24 h | 60 | 1 | 4 | 3 | 2 | 1 | 3 | 3 | 3 | 2 | 3 | 4 | |
| 60 | 1 | 3 | 2 | 2 | 1 | 3 | 2 | 3 | 3 | 2 | 3 | ||
| 55 | 2 | 4 | 5 | 3 | 2 | 4 | 3 | 3 | 3 | 2 | 5 | ||
| 75 | 2 | 3 | 2 | 2 | 2 | 3 | 2 | 2 | 3 | 3 | 3 | ||
| Mean/SD | 69 +/− 16 | 1.4 +/− 0.55 | 3.2 +/− 0.84 | 2.6 +/− 1.52 | 2 +/− 0.71 | 1.4 +/− 0.55 | 2.8 +/− 1.10 | 2.4 +/− 0.55 | 2.6 +/− 0.55 | 2.4 +/− 0.90 | 2.4 +/− 0.55 | 3.2 +/− 1.44 | |
| SK | 40 | 2 | 4 | 3 | 2 | 2 | 5 | 3 | 3 | 3 | 2 | 5 | |
| 24 h | 60 | 2 | 4 | 4 | 2 | 2 | 4 | 3 | 3 | 3 | 2 | 4 | |
| 85 | 1 | 3 | 3 | 2 | 2 | 3 | 2 | 3 | 3 | 2 | 3 | ||
| 65 | 1 | 4 | 3 | 2 | 2 | 4 | 2 | 3 | 3 | 2 | 4 | ||
| Mean/SD | 63 +/− 18.48 | 1.5 +/− 0.58 | 3.75 +/− 0.5 | 3.25 +/− 0.5 | 2 | 2 | 4 +/− 0.82 | 2.5 +/− 0.58 | 3 | 3 | 2 | 4 +/− 0.82 | |
| SK + VSOP | 90 | 1 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 2 | |
| 24 h | 90 | 1 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 85 | 1 | 2 | 4 | 2 | 1 | 4 | 2 | 2 | 2 | 2 | 3 | ||
| 90 | 1 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| 95 | 1 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| Mean/SD | 90 +/− 3.54 | 1 | 2 | 2.2 +/− 1.1 | 1.6 +/− 0.55 | 1 | 2.4 +/− 0.9 | 2 | 2 | 2 | 1.8 +/− 0.45 | 2.2 +/− 0.45 | |
| VSOP | 75 | 1 | 3 | 3 | 2 | 1 | 4 | 2 | 3 | 2 | 2 | 4 | |
| 24 h | 40 | 2 | 4 | 3 | 2 | 1 | 4 | 2 | 3 | 2 | 2 | 5 | |
| 60 | 2 | 4 | 3 | 2 | 1 | 4 | 3 | 3 | 2 | 2 | 4 | ||
| 85 | 1 | 3 | 2 | 2 | 1 | 3 | 2 | 3 | 2 | 2 | 3 | ||
| 90 | 2 | 3 | 2 | 2 | 1 | 3 | 2 | 3 | 2 | 2 | 3 | ||
| Mean/SD | 70 +/− 20.31 | 1.6 +/− 0.55 | 3.4 +/− 0.55 | 2.6 +/− 0.55 | 2 | 1 | 3.6 +/− 0.55 | 2.2 +/− 0.45 | 3 | 2 | 2 | 3.8 +/− 0.84 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kröger, N.; Czigany, Z.; Jiang, J.; Afify, M.; Paschenda, P.; Nagai, K.; Yagi, S.; Tolba, R.H. The Benefits of Fibrinolysis Combined with Venous Systemic Oxygen Persufflation (VSOP) in a Rat Model of Donation after Circulatory Death and Orthotopic Liver Transplantation. Int. J. Mol. Sci. 2022, 23, 5272. https://doi.org/10.3390/ijms23095272
Kröger N, Czigany Z, Jiang J, Afify M, Paschenda P, Nagai K, Yagi S, Tolba RH. The Benefits of Fibrinolysis Combined with Venous Systemic Oxygen Persufflation (VSOP) in a Rat Model of Donation after Circulatory Death and Orthotopic Liver Transplantation. International Journal of Molecular Sciences. 2022; 23(9):5272. https://doi.org/10.3390/ijms23095272
Chicago/Turabian StyleKröger, Nadja, Zoltan Czigany, Jipin Jiang, Mamdouh Afify, Pascal Paschenda, Kazuyuki Nagai, Shintaro Yagi, and René H. Tolba. 2022. "The Benefits of Fibrinolysis Combined with Venous Systemic Oxygen Persufflation (VSOP) in a Rat Model of Donation after Circulatory Death and Orthotopic Liver Transplantation" International Journal of Molecular Sciences 23, no. 9: 5272. https://doi.org/10.3390/ijms23095272
APA StyleKröger, N., Czigany, Z., Jiang, J., Afify, M., Paschenda, P., Nagai, K., Yagi, S., & Tolba, R. H. (2022). The Benefits of Fibrinolysis Combined with Venous Systemic Oxygen Persufflation (VSOP) in a Rat Model of Donation after Circulatory Death and Orthotopic Liver Transplantation. International Journal of Molecular Sciences, 23(9), 5272. https://doi.org/10.3390/ijms23095272