
Calprotectin and Imbalances between Acute-Phase Mediators Are Associated with Critical Illness in COVID-19

 ,
,  , ,
, , 
 and
and
Abstract
:1. Introduction
2. Results
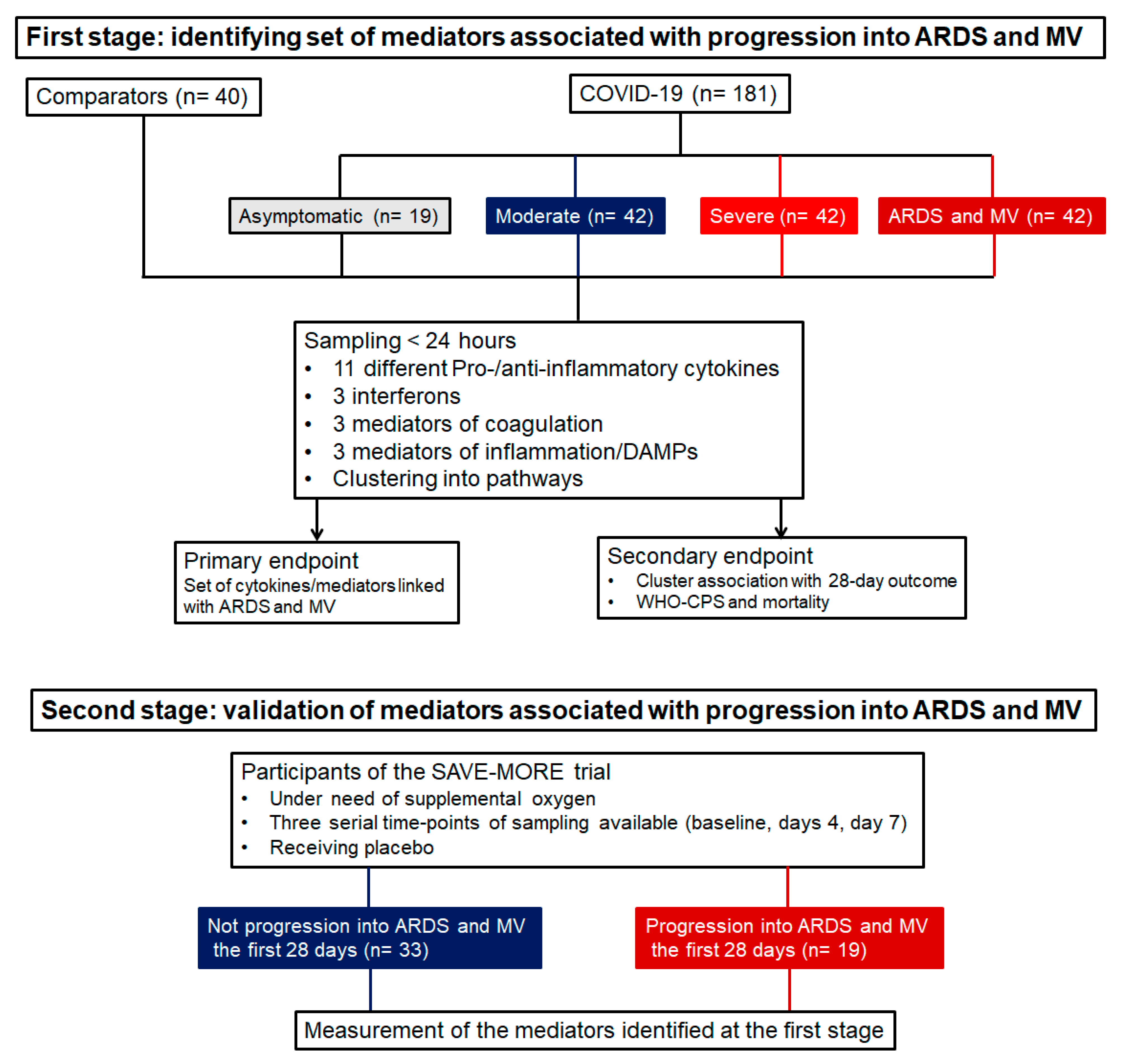
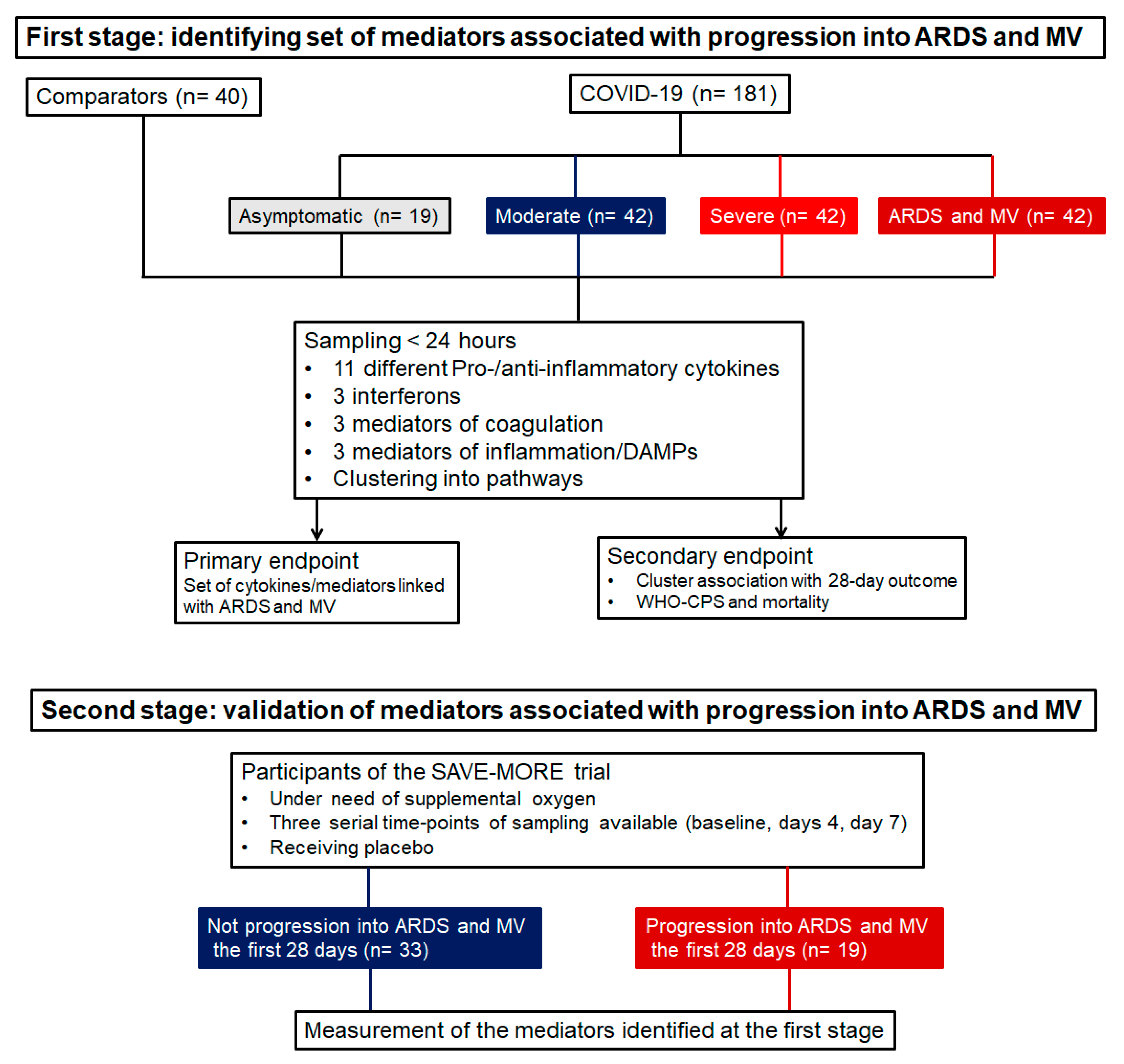
2.1. Study Participants
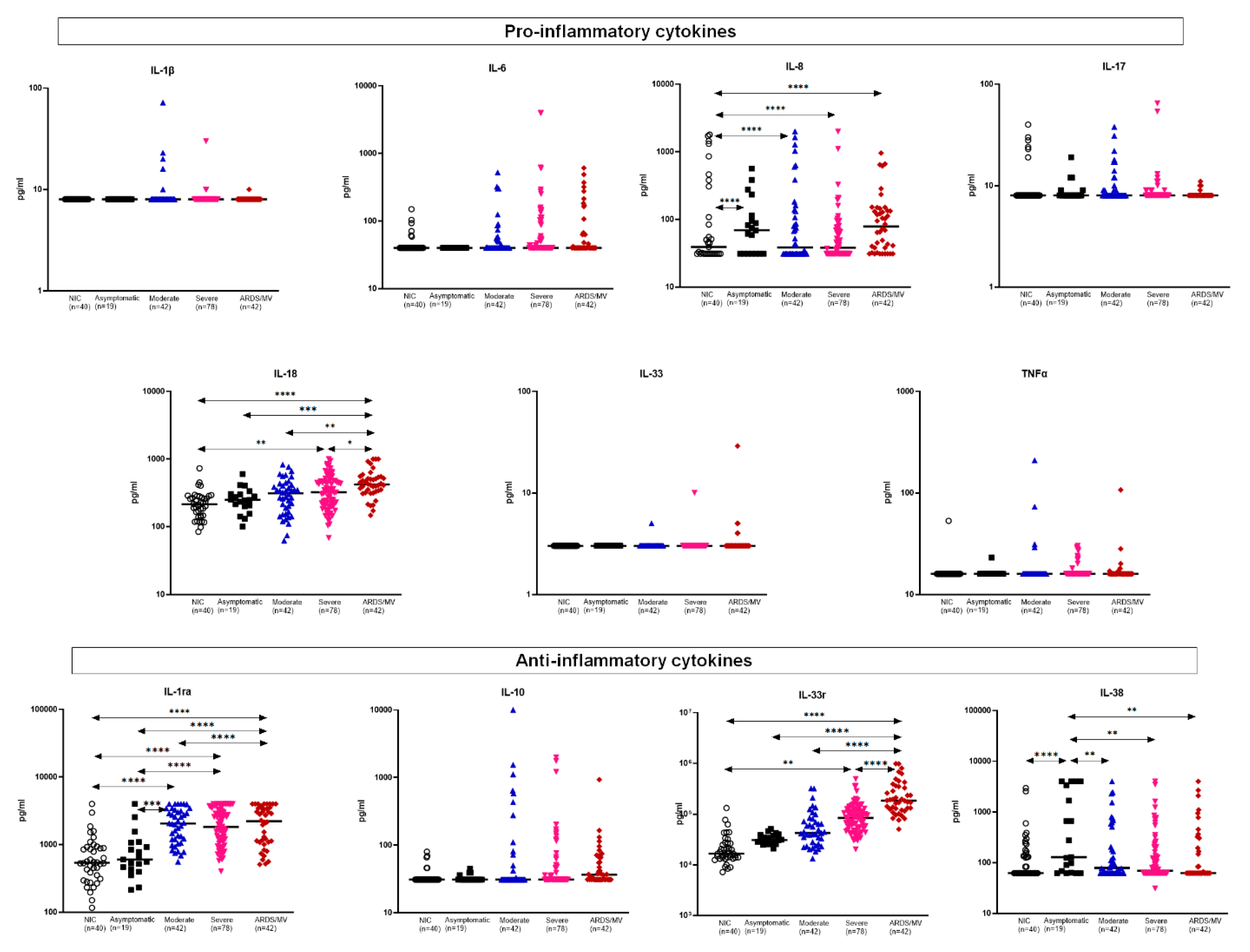
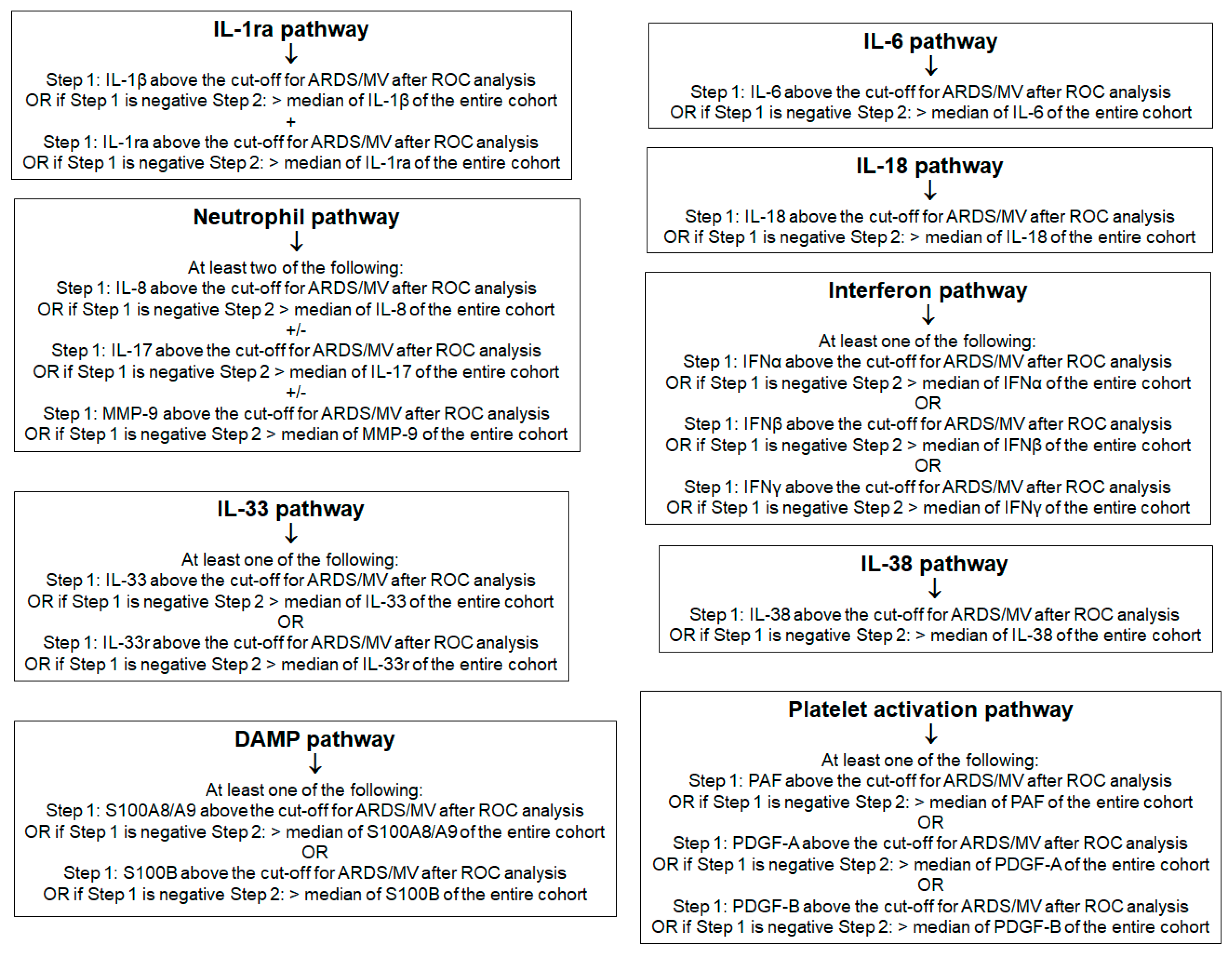
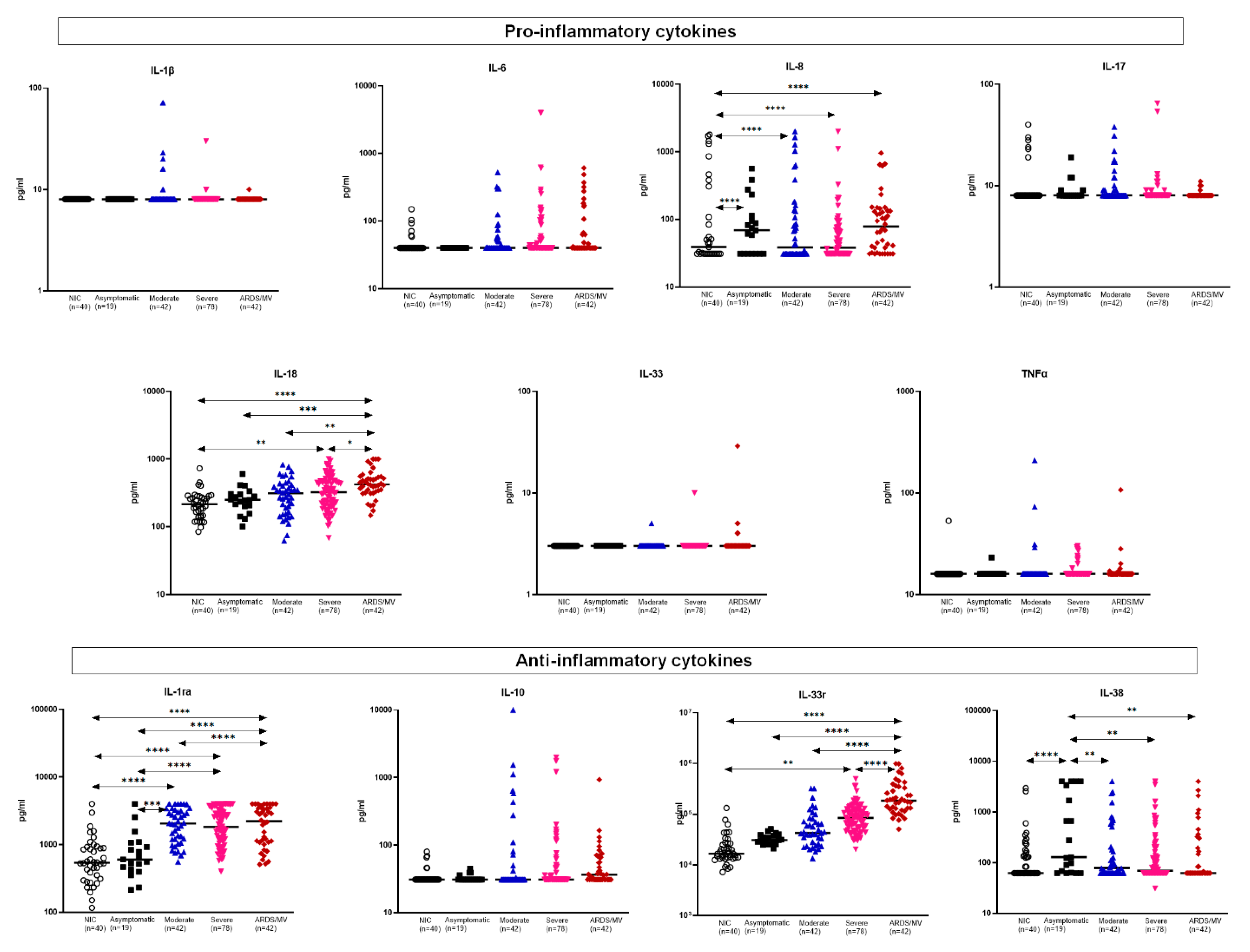
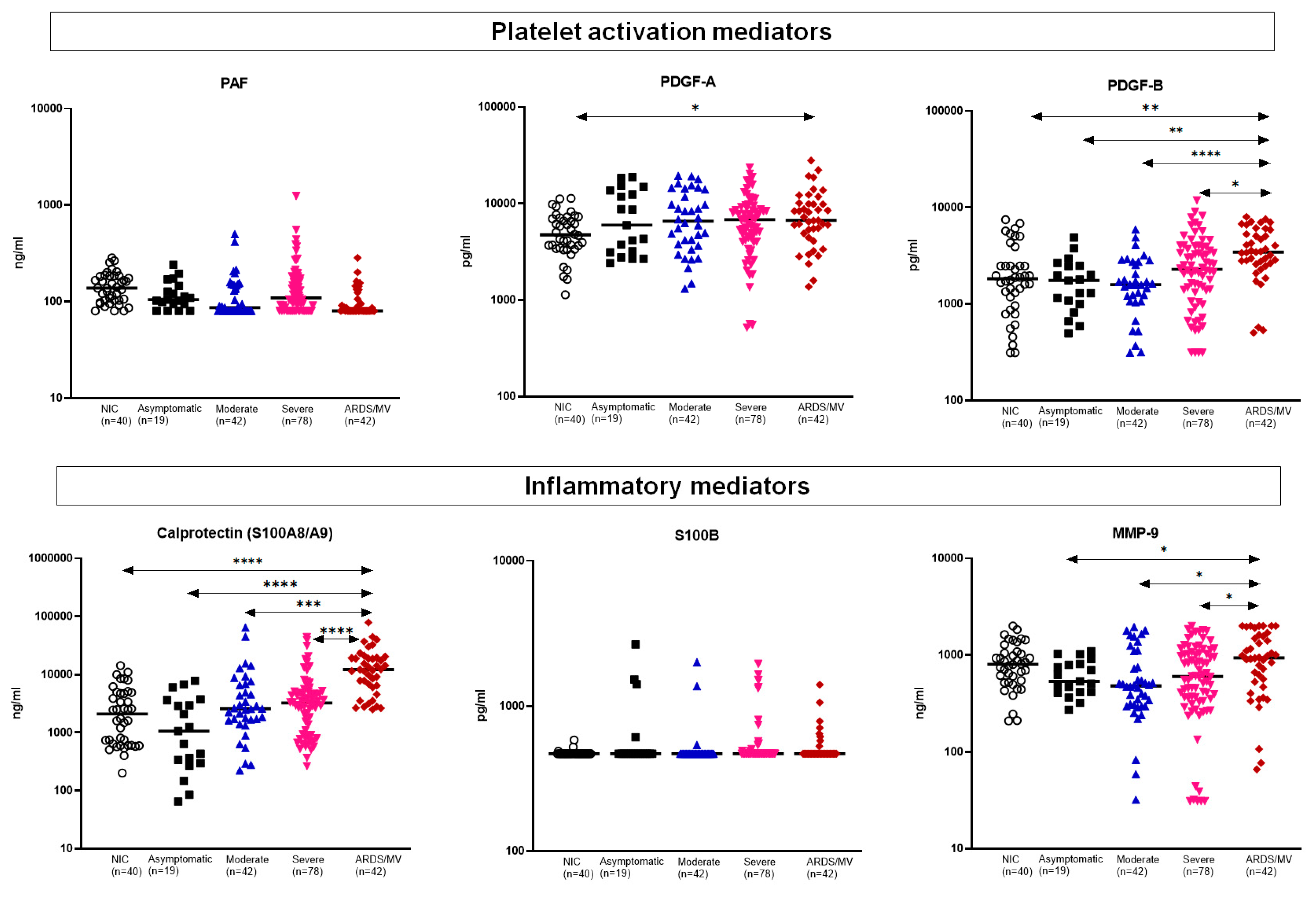
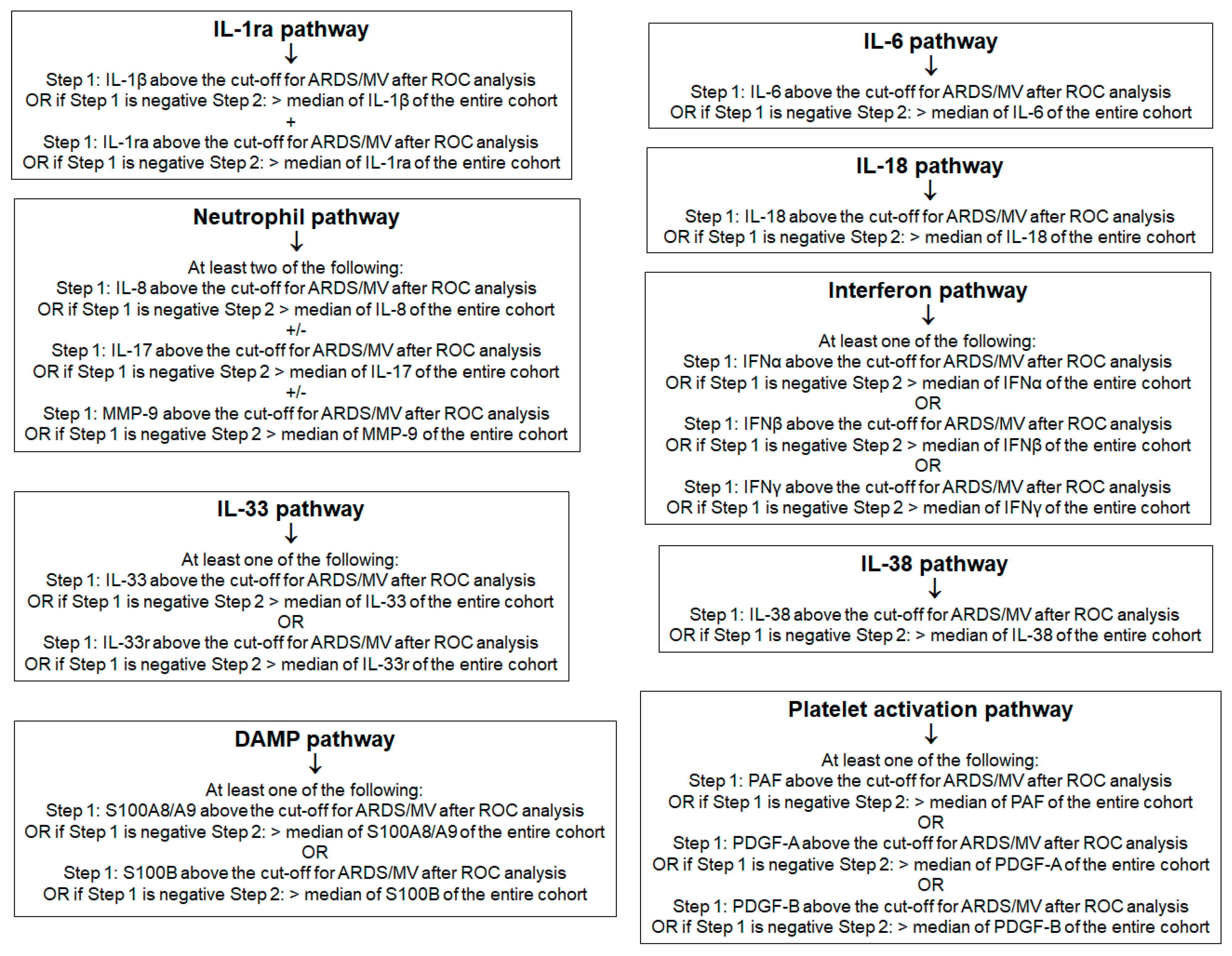
2.2. First Stage: Presence of Inflammation-Associated Mediators
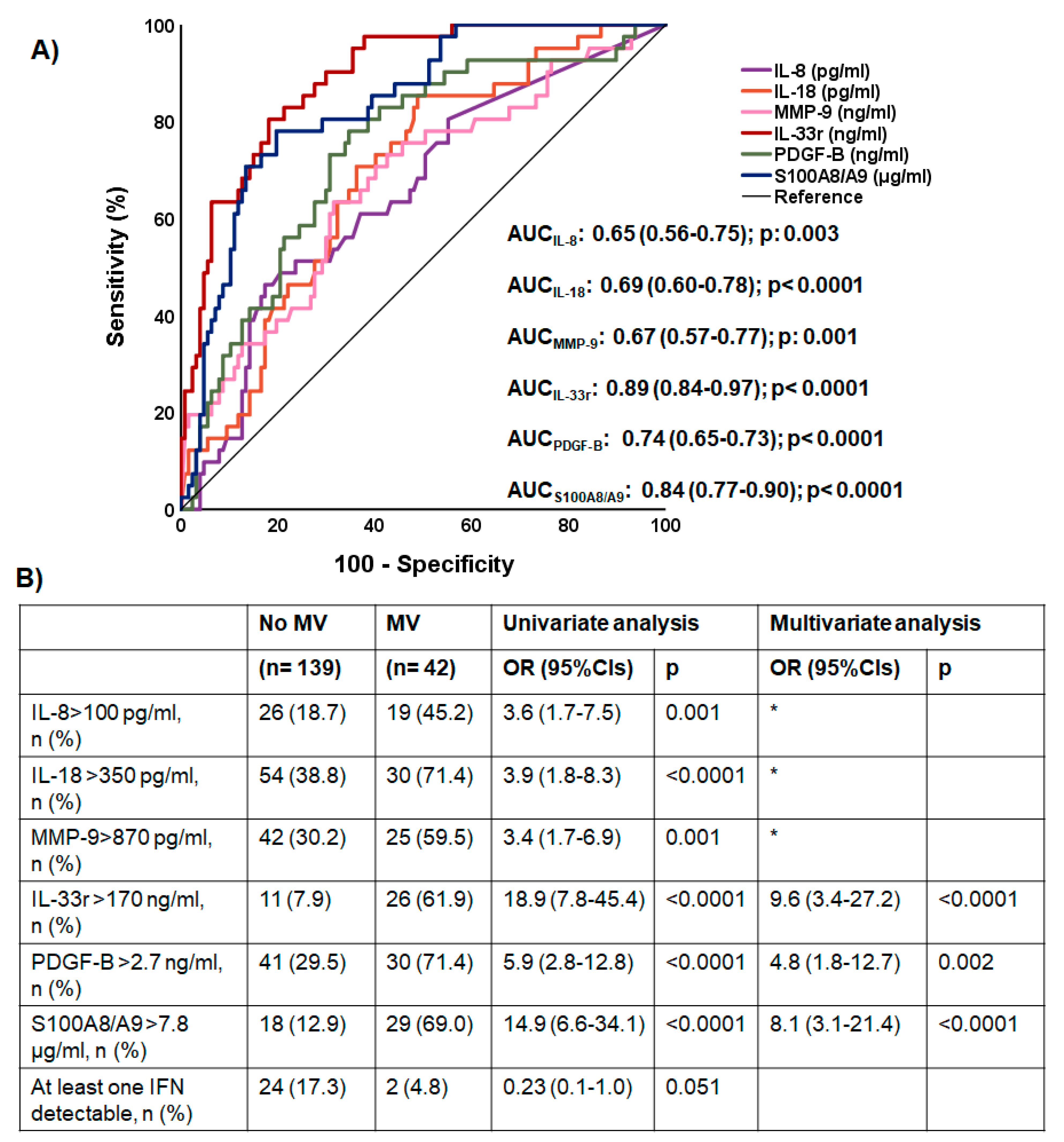
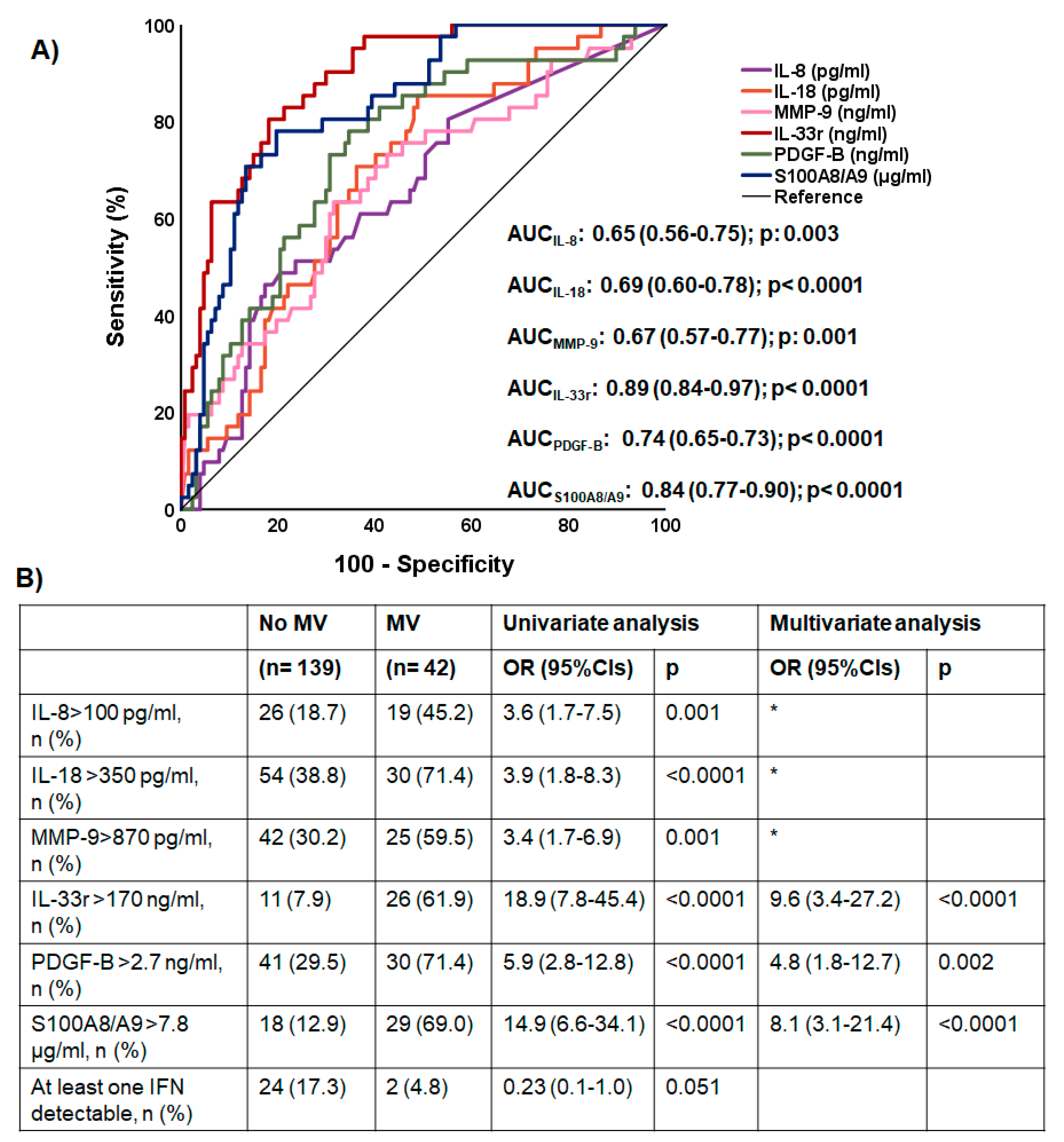
2.3. First Stage: Associations between Inflammatory Mediators and Progression into Acute Respiratory Distress Syndrome (ARDS) Necessitating Mechanical Ventilation (MV)
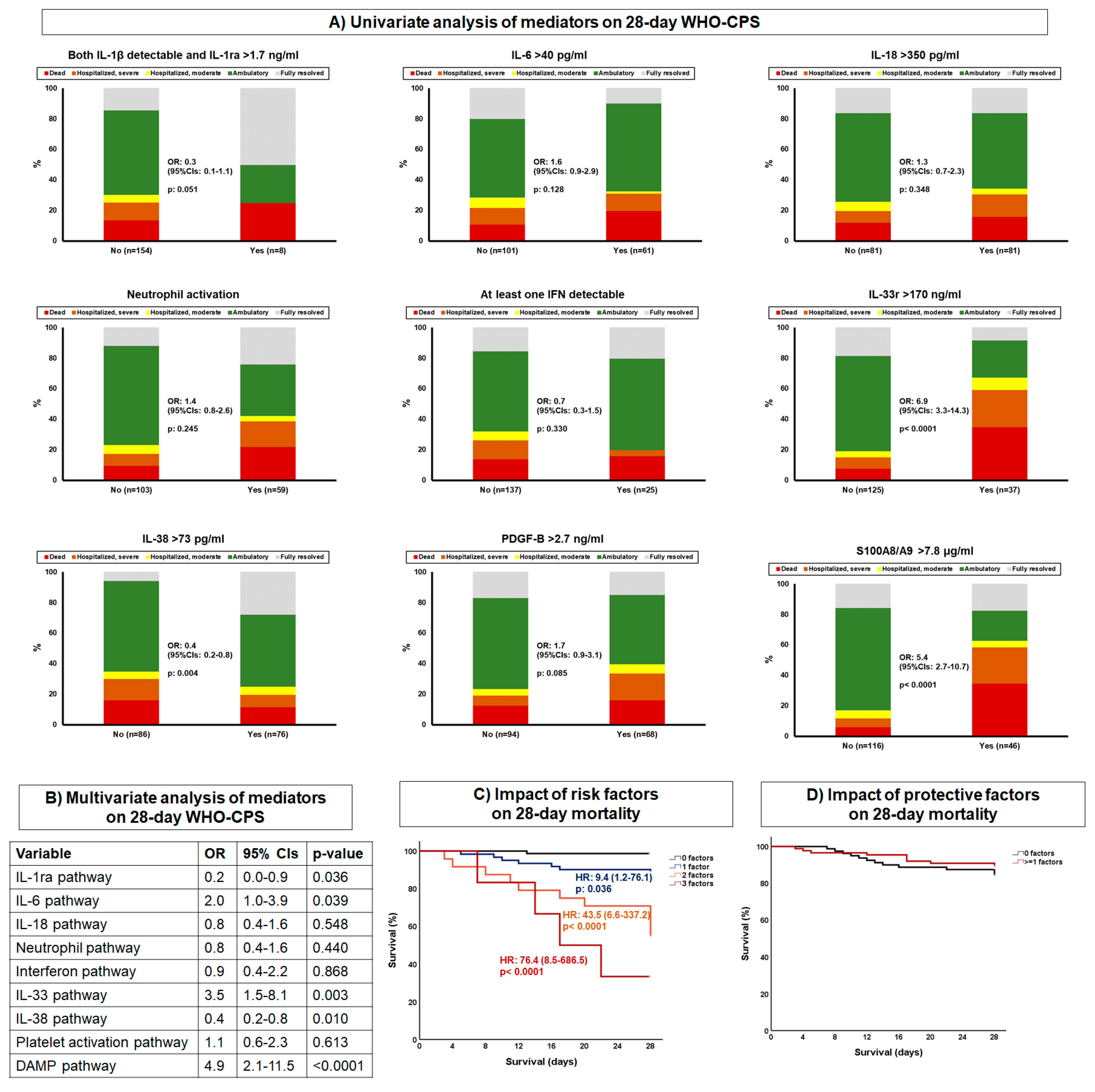
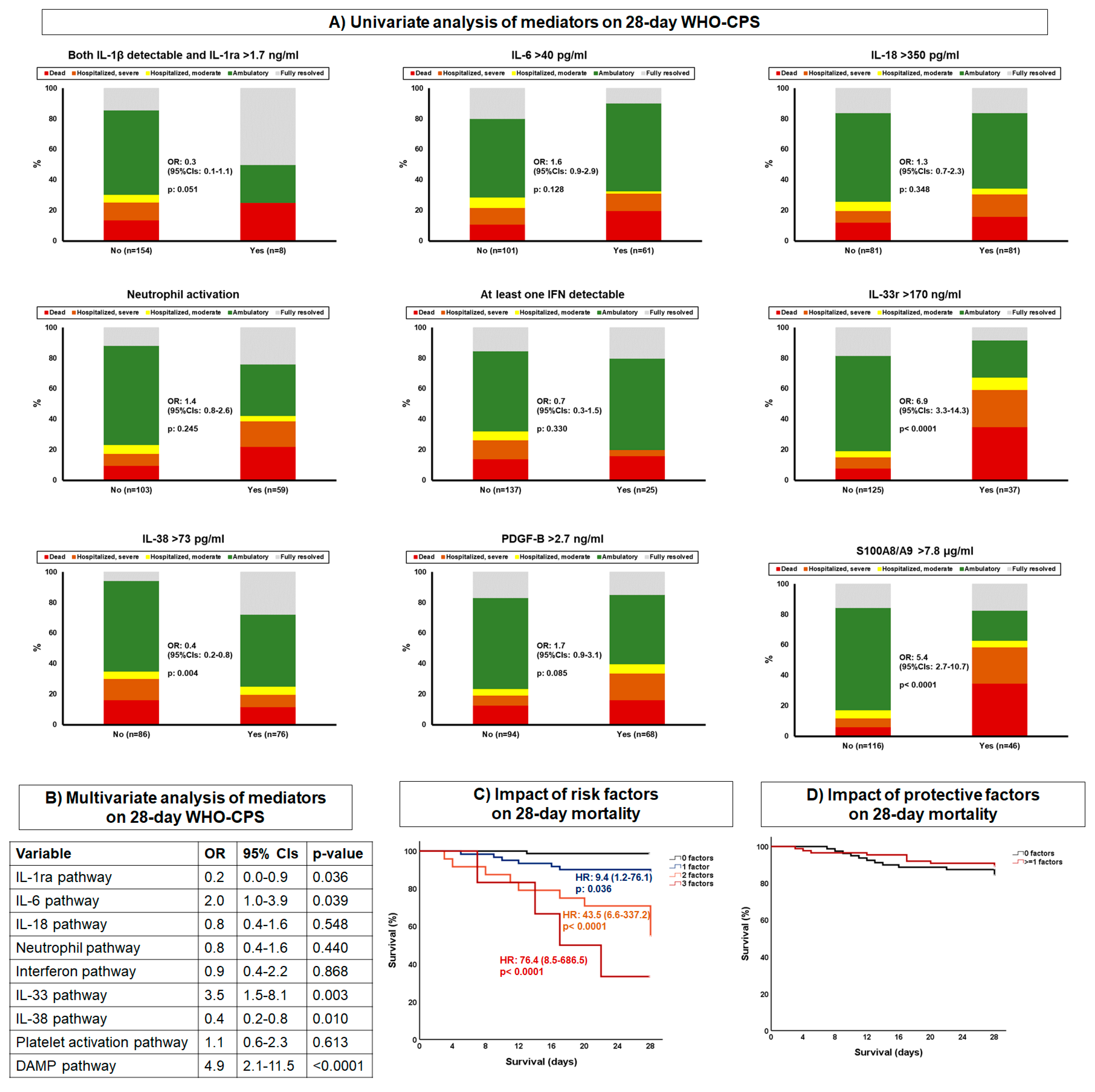
2.4. First Stage: Associations between Biomarkers and 28-Day Mortality
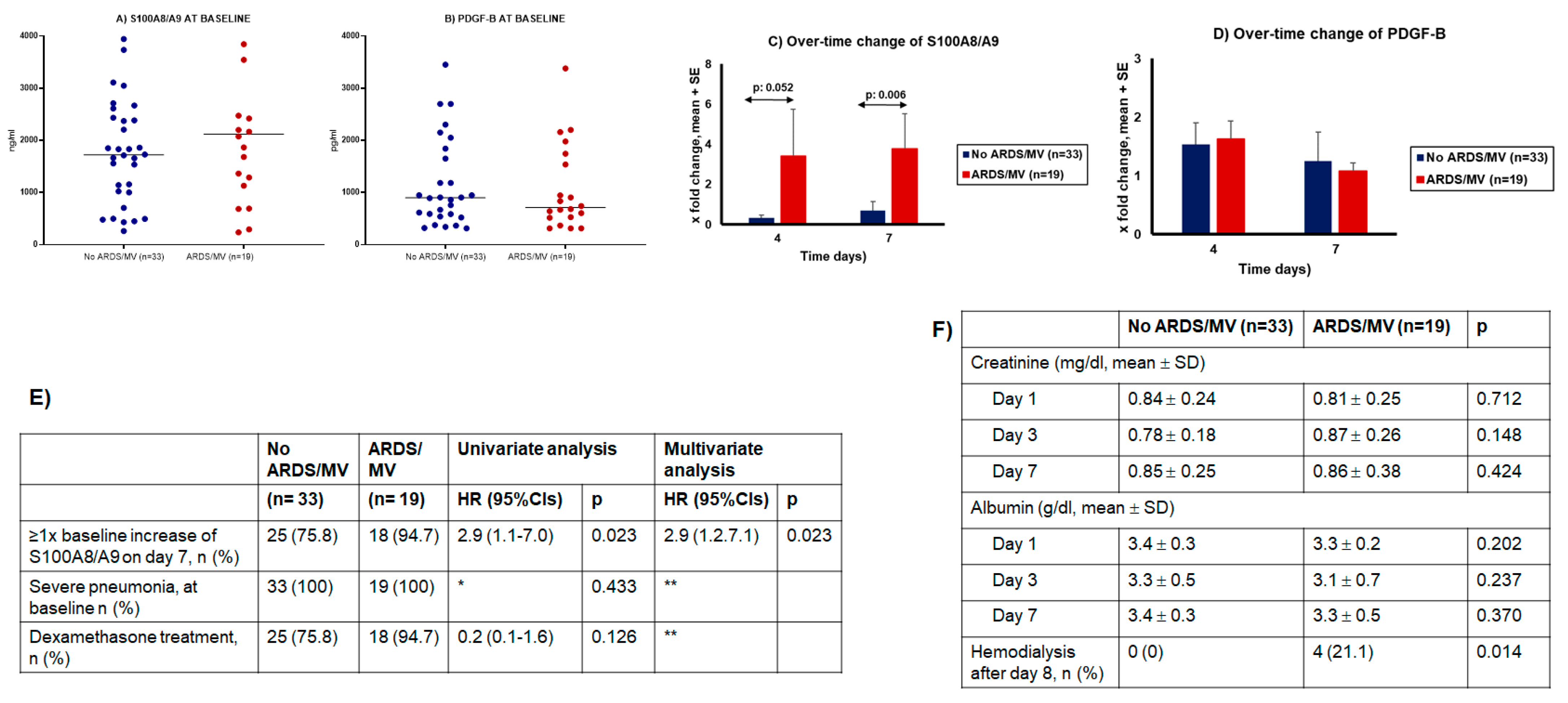
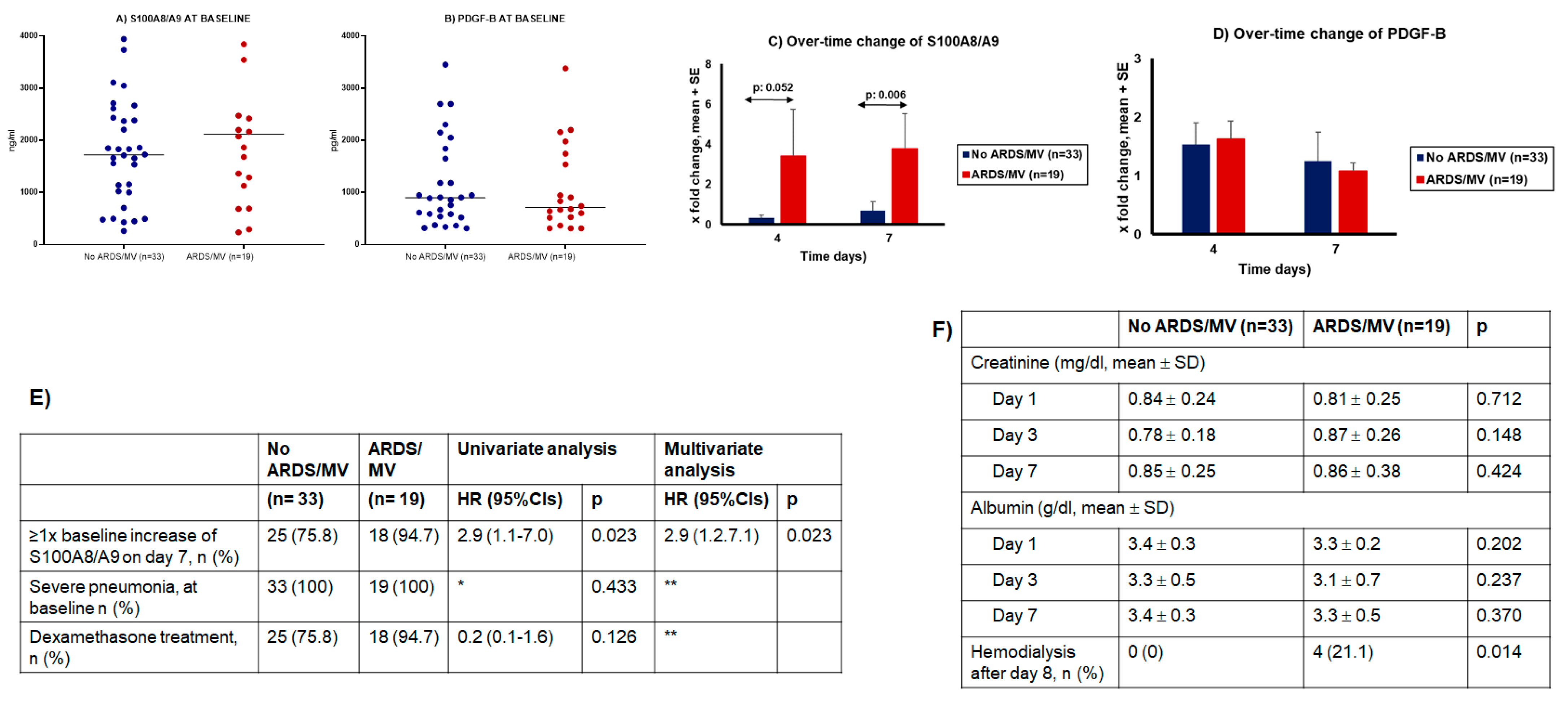
2.5. Second Stage: Validation of the Role of S100A8/A9 (Calprotectin) in Progression into ARDS Necessitating MV
3. Discussion
4. Methods
4.1. Patient Cohorts
4.2. Laboratory Assays
4.3. Study Endpoints
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tai, W.; He, L.; Zhang, X.; Pu, J.; Voronin, D.; Jiang, S.; Zou, Y.; Du, L. Characterization of the receptor-binding domain (RBD) of 2019 novel coronavirus: Implication for development of RBD protein as a viral attachment inhibitor and vaccine. Cell. Mol. Immunol. 2020, 17, 613–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canna, S.W.; Cron, R.Q. Highways to hell: Mechanism-based management of cytokine storm syndromes. J. Allergy Clin. Immunol. 2020, 146, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.B.; June, C.H. Cytokine release syndrome in severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [Green Version]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, E.M.; Katsaounou, P.; et al. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe 2020, 27, 992–1000. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Brodin, P. Immune determinants of COVID-19 disease presentation and severity. Nat. Med. 2021, 27, 28–33. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136. [Google Scholar] [CrossRef]
- Malik, I.A.; Ramadori, G. Interleukin-6-production is responsible for induction of hepatic synthesis of several chemokines as acute-phase mediators in two animal models: Possible significance for interpretation of laboratory changes in severely ill patients. Biology 2022, 11, 470. [Google Scholar] [CrossRef]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Capone, M.; Vanni, A.; Spinicci, M.; Mencarini, J.; Caporale, R.; Peruzzi, B.; Antonelli, A.; et al. Impaired immune cell cytotoxicity in severe COVID-19 is IL-6 dependent. J. Clin. Investig. 2020, 130, 4694–4703. [Google Scholar] [CrossRef]
- Conti, P.; Caraffa, A.; Gallenga, C.E.; Ross, R.; Kritas, S.K.; Frydas, I.; Younes, A.; Ronconi, G. Coronavirus-19 (SARS-CoV-2) induces acute severe lung inflammation via IL-1 causing cytokine storm in COVID-19: A promising inhibitory strategy. J. Biol. Regul. Homeost. Agents 2020, 34, 1971–1975. [Google Scholar] [PubMed]
- Silvin, A.; Chapuis, N.; Dunsmore, G.; Goubet, A.G.; Dubuisson, A.; Derosa, L.; Almire, C.; Hénon, C.; Kosmider, O.; Droin, N.; et al. Elevated calprotectin and abnormal myeloid cell subsets discriminate severe from mild COVID-19. Cell 2020, 182, 1401–1418. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Poulakou, G.; Milionis, H.; Metallidis, S.; Adamis, G.; Tsiakos, K.; Fragkou, A.; Rapti, A.; Damoulari, D.; Fantoni, M.; et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen activator receptor: A double-blind, randomized controlled phase 3 trial. Nat. Med. 2021, 27, 1752–1760. [Google Scholar] [CrossRef]
- Mahler, M.; Meron, P.L.; Infantino, M.; Buhler, K.A.; Fritzler, M.J. Circulating calprotectin as a biomarker of COVID-19 severity. Expert Rev. Clin. Immunol. 2021, 17, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Mao, Q.; Wang, C.; Wen, W.; Zhou, M.; Tanj, J.; Chen, C.; Cheng, Y.; Wu, Q.; Zhang, X.; Feng, Z.; et al. A meta-analysis of the association between calprotectin and the severity of COVID-19. J. Infect. 2021, 84, e31–e33. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Long, X.; Xu, Q.; Tan, J.; Wang, X.; Cao, Y.; Wei, J.; Luo, H.; Zhu, H.; Huang, L.; et al. Elevated serum levels of S100A8/A9 and HMGB1 at hospital admission are correlated with inferior clinical outcomes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 992–994. [Google Scholar] [CrossRef] [PubMed]
- Bauer, W.; Diehl-Wiesenecker, E.; Ulke, J.; Galtung, N.; Havelka, A.; Hegel, J.K.; Tauber, R.; Somasundaram, R.; Kappert, K. Outcome prediction by serum calprotectin in patients with COVID-19 in the emergency department. J. Infect. 2021, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Mentzer, A.J.; James, T.; Yongya, M.; Cox, S.; Paddon, K.; Shine, B.; Bowen, J.; Novak, A.; Knight, J.C.; Fullerton, J.N. Serum calprotectin is not an independent predictor of severe COVID-19 in ambulatory adult patients. J. Infect. 2022, 84, e27–e33. [Google Scholar] [CrossRef]
- Shi, H.; Zuo, Y.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Woodward, W.; Lezak, S.P.; Lugogo, N.L.; et al. Neutrophil calprotectin identifies severe pulmonary disease in COVID-19. J. Leukoc. Biol. 2021, 109, 67–72. [Google Scholar] [CrossRef]
- Huang, W.; Li, M.; Luo, G.; Wu, X.; Su, B.; Zhao, L.; Zhang, S.; Chen, X.; Jia, M.; Zhu, J.; et al. The inflammatory factors associated with disease severity to predict COVID-19 progression. J. Immunol. 2021, 206, 1597–1608. [Google Scholar] [CrossRef]
- Guo, Q.; Zhao, Y.; Li, J.; Liu, J.; Yang, X.; Guo, X.; Kuang, M.; Xia, H.; Zhang, Z.; Cao, L.; et al. Induction of alarmin S100A8/A9 mediates activation of aberrant neutrophils in the pathogenesis of COVID-19. Cell Host Microbe 2021, 29, 222–235. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Hong, X.Y.; Li, Y.; Chen, W.; Ye, G.; Li, Y.; Luo, Y. Serum-soluble ST2 as a novel biomarker reflecting inflammatory status and illness severity in patients with COVID-19. Biomark. Med. 2020, 14, 1619–1629. [Google Scholar] [CrossRef]
- Stanczak, M.A.; Sanin, D.E.; Apostolova, P.; Nerz, G.; Lampaki, D.; Hofmann, M.; Steinmann, D.; Krohn-Grimberghe, M.; Thimme, R.; Mittler, G.; et al. IL-33 expression in response to SARS-CoV-2 correlates with seropositivity in COVID-19 convalescent individuals. Nat. Commun. 2021, 12, 2133. [Google Scholar] [CrossRef] [PubMed]
- Munitz, A.; Erdy-Boltzer, L.; Itan, M.; Tur-Kaspa, R.; Dicker, D.; Marcoviu, D.; Goren, M.G.; Mor, M.; Lev, S.; Gottesman, T.; et al. Rapid seroconversion and persistent functional IgG antibodies in severe COVID-19 patients correlates with an IL-12p70 and IL-33 signature. Sci. Rep. 2021, 11, 3461. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Ge, Y.; Sun, J. IL-33 in COVID-19: Friend or foe? Cell. Mol. Immunol. 2021, 18, 1602–1604. [Google Scholar] [CrossRef] [PubMed]
- Taracanova, A.; Alevizos, M.; Karagkouni, A.; Weng, Z.; Norwitz, E.; Conit, P.; Leeman, S.E.; Theoharides, T.C. SP and IL-33 together markedly enhance TNF synthesis and secretion from human mast cells mediated by the interaction of their receptors. Proc. Natl. Acad. Sci. USA 2017, 114, E4002–E4009. [Google Scholar] [CrossRef] [Green Version]
- Taracanova, A.; Tsilioni, I.; Conti, P.; Norwitz, E.R.; Leemanm, S.E.; Theoharidesm, T.C. Substance P and IL-33 administered together stimulate a marked secretion of IL-1beta from human mast cells, inhibited by methoxyluteolin. Proc. Natl. Acad. Sci. USA 2018, 115, E9381–E9390. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Dinarello, C.A.; Molgora, M.; Garlandam, C. Interleukin-1 and related cytokines in the regulation of inflammation and immunity. Immunity 2019, 50, 778–795. [Google Scholar] [CrossRef] [Green Version]
- van de Veerdonk, F.L.; de Graaf, D.M.; Joosten, L.A.; Dinarello, C.A. Biology of IL-38 and its role in disease. Immunol. Rev. 2018, 281, 191–196. [Google Scholar] [CrossRef]
- Kwak, A.; Lee, Y.; Kim, H.; Kim, S. Intracellular interleukin (IL)-1 family cytokine processing enzyme. Arch. Pharm. Res. 2016, 39, 1556–1564. [Google Scholar] [CrossRef] [PubMed]
- Tsilioni, I.; Pantazopoulos, H.; Conti, P.; Leeman, S.E.; Theoharides, T.C. IL-38 inhibits microglial inflammatory mediators and is decreased in amygdala of children with autism spectrum disorder. Proc. Natl. Acad. Sci. USA 2020, 117, 16475–16480. [Google Scholar] [CrossRef] [PubMed]
- Laing, A.G.; Lorenc, A.; Del Moline Del Barrio, I.; Das, A.; Fish, M.; Monin, L.; Muñoz-Ruiz, M.; McKenzie, D.R.; Hayday, T.S.; Francos-Quijorna, I.; et al. A dynamic COVID-19 immune signature includes associations with poor prognosis. Nat. Med. 2021, 26, 1623–1635. [Google Scholar] [CrossRef] [PubMed]
- Dalekos, G.N.; Stefos, A.; Georgiadou, S.; Lygoura, V.; Michail, A.; Ntaios, G.; Smakidou, A.; Giannoulis, G.; Gabeta, S.; Vlychou, M.; et al. Lessons from pathophysiology: Use of individualized combination treatments with immune interventional agents to tackle severe respiratory failure in patients with COVID-19. Eur. J. Intern. Med. 2021, 88, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, E.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; van Bentum-Puijk, W.; Berry, L.R.; et al. Interleukin-6 receptor antagonists in critically ill patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar]
- Recovery Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Panagopoulos, P.; Metallidis, S.; Dalekos, G.N.; Poulakou, G.; Gatselis, N.; Karakike, E.; Saridaki, M.; Loli, G.; Stefos, A.; et al. An open label trial of anakinra to prevent respiratory failure in COVID-19. eLife 2021, 10, e66125. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2022, 384, 693–704. [Google Scholar]
- Sinha, S.; Rosin, N.L.; Arora, R.; Labit, E.; Jaffer, A.; Cao, L.; Farias, R.; Nguyen, A.P.; de Almeida, L.G.N.; Dufour, A.; et al. Dexamethasone modulates immature neutrophils and interferon reprogramming in severe COVID-19. Nat. Med. 2022, 28, 201–211. [Google Scholar] [CrossRef]
- Tsiakos, K.; Tsakiris, A.; Tsibris, G.; Voutsinas, P.M.; Panagopoulos, P.; Kosmidou, A.; Petrakis, V.; Gravvani, A.; Gkavogianni, T.; Klouras, E.; et al. Early start of clarithromycin is associated with better outcome in COVID-19 of moderate severity: The ACHIEVE open-label single-arm trial. Infect. Dis. Ther. 2021, 10, 2333–2351. [Google Scholar] [CrossRef]
- Karakike, E.; Dalekos, G.N.; Koutsodimitropoulos, I.; Saridaki, I.; Poutzitaki, C.; Papathanakos, G.; Kotsaki, A.; Chalvatzis, S.; Dimakopoulou, V.; Vechlidis, N.; et al. ESCAPE: An open-label trial of personalized immunotherapy in critically ill COVID-19 patients. J. Innate Immun. 2021, 14, 218–228. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparators | Asymptomatic | Moderate | Severe | ARDS and MV | |
|---|---|---|---|---|---|
| Number | 40 | 19 | 42 | 78 | 42 |
| Age (years) mean ± SD | 58.3 ± 15.8 | 59.5 ± 10.8 | 55.3 ± 14.8 | 61.4 ± 13.9 | 64.9 ± 12.8 |
| Male gender, n (%) | 28 (70) | 12 (63.2) | 25 (59.5) | 56 (71.8) | 35 (83.3) |
| SOFA, mean ± SD | NA | NA | 0.9 ± 0.9 | 2.3 ± 1.6 | 6.5 ± 2.5 |
| CCI, mean ± SD | 1.0 ± 0.2 | 1.3 ± 1.9 | 2.3 ± 2.3 | 2.6 ± 2.1 | 2.4 ± 1.5 |
| Comorbidities, n (%) | |||||
| Type 2 diabetes mellitus | 0 (0) | 5 (26.3) | 13 (31.0) | 20 (25.6) | 6 (14.3) |
| Chronic heart failure | 0 (0) | 0 (0) | 3 (7.1) | 5 (5.1) | 0 (0) |
| Chronic renal disease | 0 (0) | 0 (0) | 2 (4.8) | 3 (3.8) | 2 (4.8) |
| Coronary heart disease | 0 (0) | 0 (0) | 5 (11.9) | 8 (10.3) | 6 (14.3) |
| Dyslipidemia | 0 (0) | 4 (21.1) | 14 (33.3) | 17 (21.8) | 4 (9.5) |
| Hypothyroidism | 0 (0) | 2 (10.5) | 7 (16.7) | 7 (9.0) | 3 (7.1) |
| Hypertension | 0 (0) | 2 (10.5) | 16 (38.1) | 24 (30.8) | 7 (16.7) |
| Stroke | 0 (0) | 0 (0) | 2 (4.8) | 1 (1.3) | 1 (2.4) |
| Atrial fibrillation | 0 (0) | 0 (0) | 2 (4.8) | 6 (7.7) | 3 (7.1) |
| COPD | 0 (0) | 0 (0) | 3 (7.1) | 2 (2.6) | 0 (0) |
| pO2/FiO2, mean ± SD | NA | NA | 397.5 ± 84.3 | 274.5 ± 103.8 | 127.1 ± 72.2 |
| White blood cell count, mean ± SD (/mm3) | NA | NA | 5394.3 ± 2379.8 | 7000.1 ± 2945.8 | 11,977.8 ± 6094.2 |
| CRP, median (IQR), mg/L | NA | NA | 4.9 (30.6) | 39.0 (80.1) | 82.9 (173.5) |
| Ferritin, median (IQR), ng/mL | NA | NA | 293.2 (534.2) | 485.3 (832.5) | 1189.5 (1686.8) |
| Administered drugs, n (%) | |||||
| β-lactamase inhibitor | NA | 0 (0) | 1 (2.4) | 21 (29.2) | 0 (0) |
| Ceftriaxone | NA | 0 (0) | 30 (71.4) | 41 (56.9) | 10 (23.8) |
| Ceftaroline | NA | 0 (0) | 0 (0) | 17 (23.6) | 10 (23.8) |
| Piperacillin/tazobactam | NA | 0 (0) | 8 (19.0) | 10 (13.9) | 16 (38.1) |
| Ceftaziidme/avibactam | NA | 0 (0) | 0 (0) | 0 (0) | 6 (14.3) |
| Glycopeptides/linezolid | NA | 0 (0) | 0 (0) | 3 (4.2) | 12 (28.6) |
| Remdesivir | NA | 0 (0) | 20 (47.6) | 30 (41.7) | 9 (21.4) |
| Dexamethasone | NA | 0 (0) | 4 (9.5) | 72 (100) | 42 (100) |
| Nor-adrenaline | NA | 0 (0) | 0 (0) | 0 (0) | 27 (64.3) |
| Furosemide | NA | 0 (0) | 0 (0) | 0 (0) | 29 (69.0) |
| Midazolam | NA | 0 (0) | 0 (0) | 0 (0) | 29 (69.0) |
| Fentanyl | NA | 0 (0) | 0 (0) | 0 (0) | 24 (57.1) |
| Propofol | NA | 0 (0) | 0 (0) | 0 (0) | 29 (69.0) |
| Dexmetomidine | NA | 0 (0) | 0 (0) | 0 (0) | 7 (16.7) |
| Cisatracurium | NA | 0 (0) | 0 (0) | 0 (0) | 7 (16.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kassianidis, G.; Siampanos, A.; Poulakou, G.; Adamis, G.; Rapti, A.; Milionis, H.; Dalekos, G.N.; Petrakis, V.; Sympardi, S.; Metallidis, S.; et al. Calprotectin and Imbalances between Acute-Phase Mediators Are Associated with Critical Illness in COVID-19. Int. J. Mol. Sci. 2022, 23, 4894. https://doi.org/10.3390/ijms23094894
Kassianidis G, Siampanos A, Poulakou G, Adamis G, Rapti A, Milionis H, Dalekos GN, Petrakis V, Sympardi S, Metallidis S, et al. Calprotectin and Imbalances between Acute-Phase Mediators Are Associated with Critical Illness in COVID-19. International Journal of Molecular Sciences. 2022; 23(9):4894. https://doi.org/10.3390/ijms23094894
Chicago/Turabian StyleKassianidis, Georgios, Athanasios Siampanos, Garyphalia Poulakou, George Adamis, Aggeliki Rapti, Haralampos Milionis, George N. Dalekos, Vasileios Petrakis, Styliani Sympardi, Symeon Metallidis, and et al. 2022. "Calprotectin and Imbalances between Acute-Phase Mediators Are Associated with Critical Illness in COVID-19" International Journal of Molecular Sciences 23, no. 9: 4894. https://doi.org/10.3390/ijms23094894
APA StyleKassianidis, G., Siampanos, A., Poulakou, G., Adamis, G., Rapti, A., Milionis, H., Dalekos, G. N., Petrakis, V., Sympardi, S., Metallidis, S., Alexiou, Z., Gkavogianni, T., Giamarellos-Bourboulis, E. J., & Theoharides, T. C. (2022). Calprotectin and Imbalances between Acute-Phase Mediators Are Associated with Critical Illness in COVID-19. International Journal of Molecular Sciences, 23(9), 4894. https://doi.org/10.3390/ijms23094894