
Psoriasis and Systemic Inflammatory Disorders

Abstract
1. Introduction
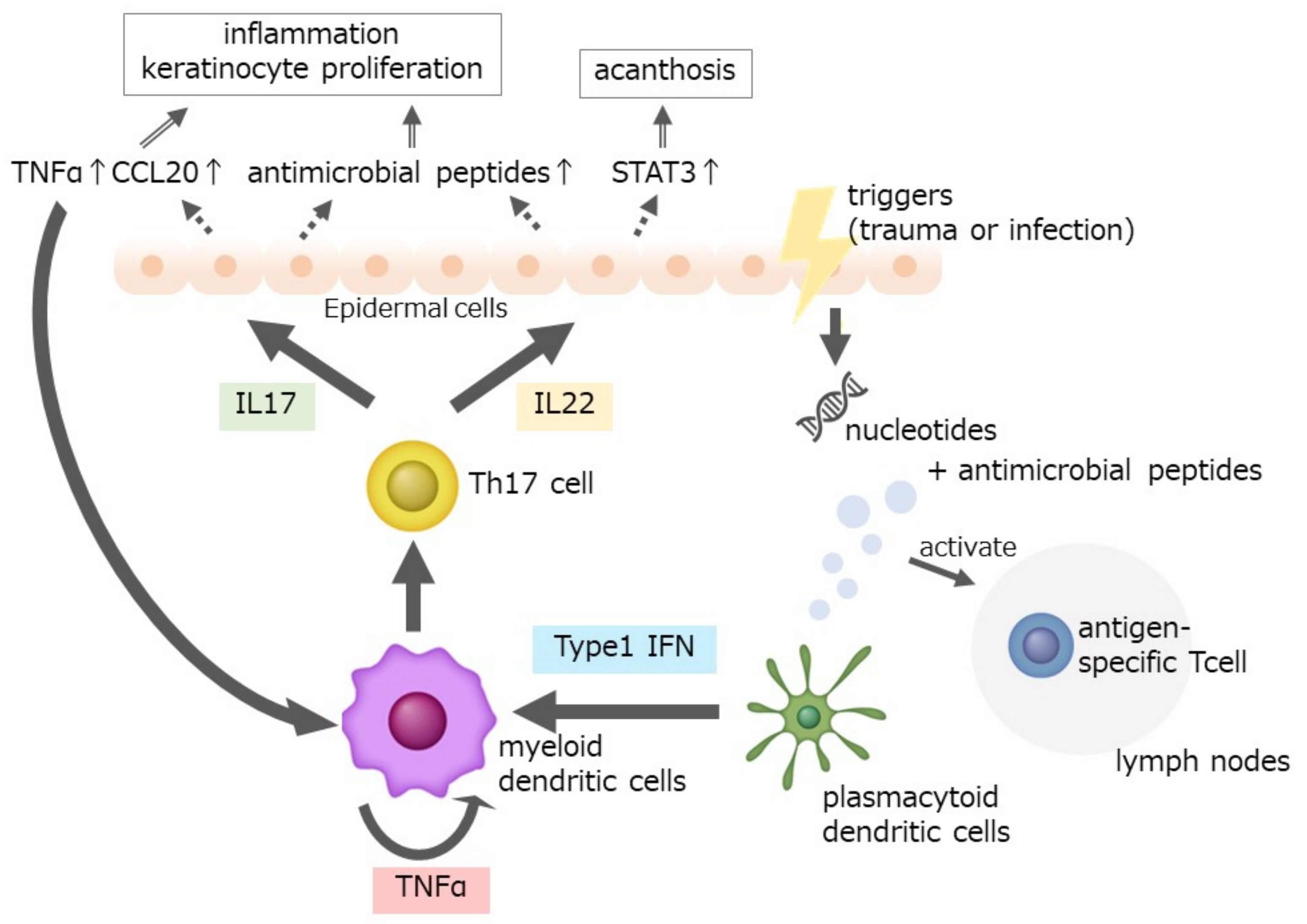
2. The Pathogenesis of Psoriasis
3. Cerebrocardiovascular Diseases
4. Osteoporosis
5. Liver Dysfunction
6. Renal Dysfunction
7. Psychological Disorders
8. Hypothyroidism
9. Alzheimer’s Disease (AD)
10. Chronic Rhinosinusitis
11. Endometriosis
12. Uveitis
13. Gut Inflammation
14. Chronic Obstructive Pulmonary Disease (COPD)
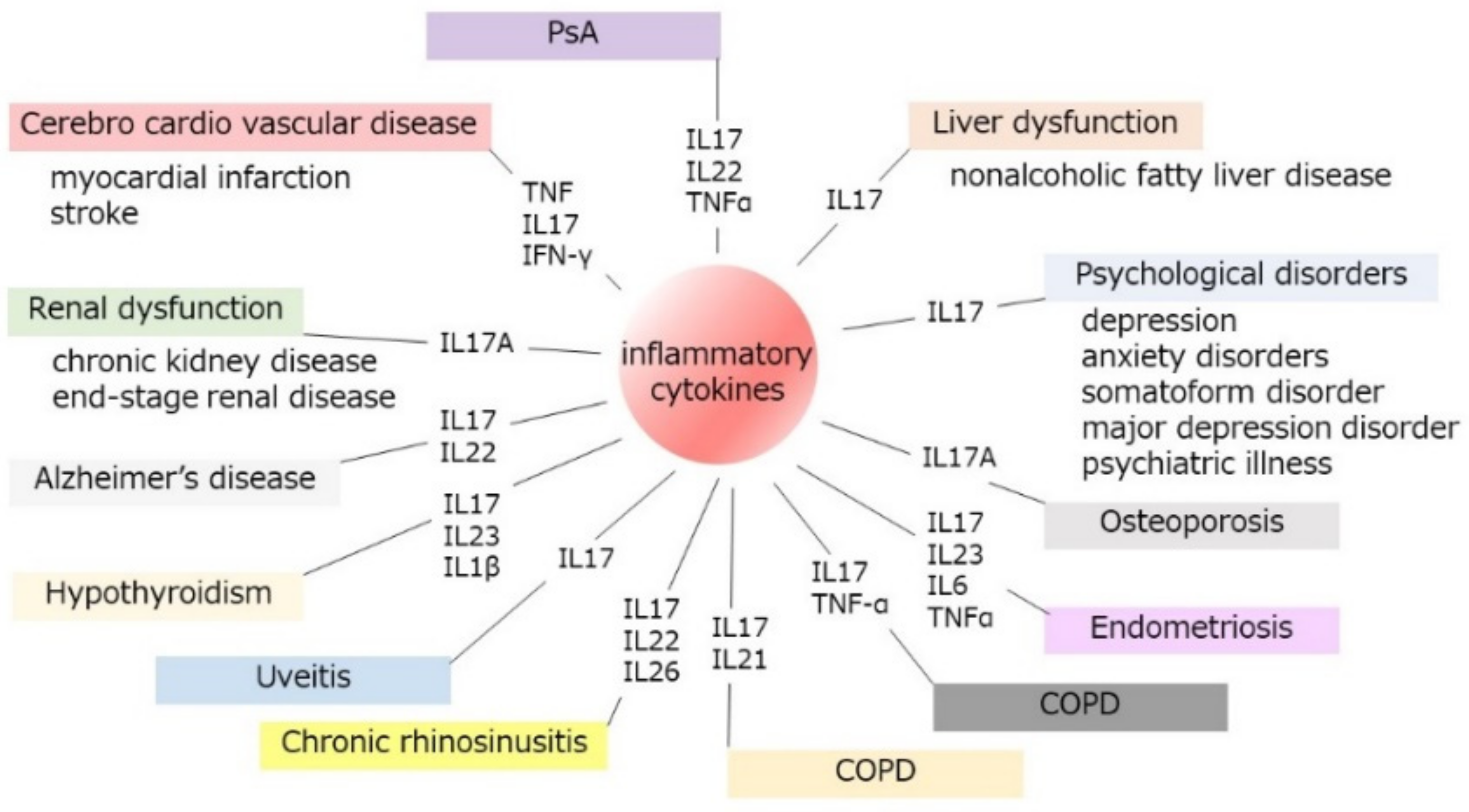
15. Whole Interaction of Psoriasis to Systemic Organ Inflammation
16. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dainichi, T.; Kitoh, A.; Otsuka, A.; Nakajima, S.; Nomura, T.; Kaplan, D.H.; Kabashima, K. The epithelial immune microenvironment (EIME) in atopic dermatitis and psoriasis. Nat. Immunol. 2018, 19, 1286–1298. [Google Scholar] [CrossRef] [PubMed]
- Sawada, Y.; Gallo, R.L. Role of Epigenetics in the Regulation of Immune Functions of the Skin. J. Investig. Dermatol. 2021, 141, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Tomura, M.; Honda, T.; Tanizaki, H.; Otsuka, A.; Egawa, G.; Tokura, Y.; Waldmann, H.; Hori, S.; Cyster, J.G.; Watanabe, T.; et al. Activated regulatory T cells are the major T cell type emigrating from the skin during a cutaneous immune response in mice. J. Clin. Investig. 2010, 120, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Gray, E.E.; Ramírez-Valle, F.; Xu, Y.; Wu, S.; Wu, Z.; Karjalainen, K.E.; Cyster, J.G. Deficiency in IL-17-committed Vγ4(+) γδ T cells in a spontaneous Sox13-mutant CD45.1(+) congenic mouse substrain provides protection from dermatitis. Nat. Immunol. 2013, 14, 584–592. [Google Scholar] [CrossRef]
- Hawkes, J.E.; Chan, T.C.; Krueger, J.G. Psoriasis pathogenesis and the development of novel targeted immune therapies. J. Allergy Clin. Immunol. 2017, 140, 645–653. [Google Scholar] [CrossRef]
- Knabel, M.; Mudaliar, K. Histopathologic features of inverse psoriasis. J. Cutan. Pathol. 2022, 49, 246–251. [Google Scholar] [CrossRef]
- Karbach, S.; Hobohm, L.; Wild, J.; Münzel, T.; Gori, T.; Wegner, J.; Steinbrink, K.; Wenzel, P.; Keller, K. Impact of Psoriasis on Mortality Rate and Outcome in Myocardial Infarction. J. Am. Heart Assoc. 2020, 9, e016956. [Google Scholar] [CrossRef]
- Kathuria, P.; Gordon, K.B.; Silverberg, J.I. Association of psoriasis and psoriatic arthritis with osteoporosis and pathological fractures. J. Am. Acad. Dermatol. 2017, 76, 1045–1053.e3. [Google Scholar] [CrossRef]
- FitzGerald, O.; Ogdie, A.; Chandran, V.; Coates, L.C.; Kavanaugh, A.; Tillett, W.; Leung, Y.Y.; deWit, M.; Scher, J.U.; Mease, P.J. Psoriatic arthritis. Nat. Rev. Dis. Primers 2021, 7, 59. [Google Scholar] [CrossRef]
- Setoyama, A.; Sawada, Y.; Saito-Sasaki, N.; Ohmori, S.; Omoto, D.; Yamamoto, K.; Yoshioka, H.; Okada, E.; Nakamura, M. Psoriasis epidemiology screening tool (PEST) is useful for the detection of psoriatic arthritis in the Japanese population. Sci. Rep. 2021, 11, 16146. [Google Scholar] [CrossRef]
- Cai, J.; Cui, L.; Wang, Y.; Li, Y.; Zhang, X.; Shi, Y. Cardiometabolic Comorbidities in Patients With Psoriasis: Focusing on Risk, Biological Therapy, and Pathogenesis. Front. Pharmacol. 2021, 12, 774808. [Google Scholar] [CrossRef]
- Davidovici, B.B.; Sattar, N.; Prinz, J.; Puig, L.; Emery, P.; Barker, J.N.; van de Kerkhof, P.; Ståhle, M.; Nestle, F.O.; Girolomoni, G.; et al. Psoriasis and systemic inflammatory diseases: Potential mechanistic links between skin disease and co-morbid conditions. J. Investig. Dermatol. 2010, 130, 1785–1796. [Google Scholar] [CrossRef]
- Korman, N.J. Management of psoriasis as a systemic disease: What is the evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef]
- Boehncke, W.H.; Brembilla, N.C. Autoreactive T-Lymphocytes in Inflammatory Skin Diseases. Front. Immunol. 2019, 10, 1198. [Google Scholar] [CrossRef]
- Lande, R.; Gregorio, J.; Facchinetti, V.; Chatterjee, B.; Wang, Y.H.; Homey, B.; Cao, W.; Wang, Y.H.; Su, B.; Nestle, F.O.; et al. Plasmacytoid dendritic cells sense self-DNA coupled with antimicrobial peptide. Nature 2007, 449, 564–569. [Google Scholar] [CrossRef]
- Nestle, F.O.; Conrad, C.; Tun-Kyi, A.; Homey, B.; Gombert, M.; Boyman, O.; Burg, G.; Liu, Y.J.; Gilliet, M. Plasmacytoid predendritic cells initiate psoriasis through interferon-alpha production. J. Exp. Med. 2005, 202, 135–143. [Google Scholar] [CrossRef]
- Greb, J.E.; Goldminz, A.M.; Elder, J.T.; Lebwohl, M.G.; Gladman, D.D.; Wu, J.J.; Mehta, N.N.; Finlay, A.Y.; Gottlieb, A.B. Psoriasis. Nat. Rev. Dis. Primers 2016, 2, 16082. [Google Scholar] [CrossRef]
- Yoshiki, R.; Kabashima, K.; Honda, T.; Nakamizo, S.; Sawada, Y.; Sugita, K.; Yoshioka, H.; Ohmori, S.; Malissen, B.; Tokura, Y.; et al. IL-23 from Langerhans cells is required for the development of imiquimod-induced psoriasis-like dermatitis by induction of IL-17A-producing γδ T cells. J. Investig. Dermatol. 2014, 134, 1912–1921. [Google Scholar] [CrossRef]
- Von Stebut, E.; Reich, K.; Thaçi, D.; Koenig, W.; Pinter, A.; Körber, A.; Rassaf, T.; Waisman, A.; Mani, V.; Yates, D.; et al. Impact of Secukinumab on Endothelial Dysfunction and Other Cardiovascular Disease Parameters in Psoriasis Patients over 52 Weeks. J. Investig. Dermatol. 2019, 139, 1054–1062. [Google Scholar] [CrossRef]
- Fry, L.; Baker, B.S.; Powles, A.V.; Fahlen, A.; Engstrand, L. Is chronic plaque psoriasis triggered by microbiota in the skin? Br. J. Dermatol. 2013, 169, 47–52. [Google Scholar] [CrossRef]
- Ueharaguchi, Y.; Honda, T.; Kusuba, N.; Hanakawa, S.; Adachi, A.; Sawada, Y.; Otsuka, A.; Kitoh, A.; Dainichi, T.; Egawa, G.; et al. Thromboxane A(2) facilitates IL-17A production from Vγ4(+) γδ T cells and promotes psoriatic dermatitis in mice. J. Allergy Clin. Immunol. 2018, 142, 680–683.e2. [Google Scholar] [CrossRef]
- Saito-Sasaki, N.; Sawada, Y.; Mashima, E.; Yamaguchi, T.; Ohmori, S.; Yoshioka, H.; Haruyama, S.; Okada, E.; Nakamura, M. Maresin-1 suppresses imiquimod-induced skin inflammation by regulating IL-23 receptor expression. Sci. Rep. 2018, 8, 5522. [Google Scholar] [CrossRef]
- Sawada, Y.; Nakatsuji, T.; Dokoshi, T.; Kulkarni, N.N.; Liggins, M.C.; Sen, G.; Gallo, R.L. Cutaneous innate immune tolerance is mediated by epigenetic control of MAP2K3 by HDAC8/9. Sci. Immunol. 2021, 6, eabe1935. [Google Scholar] [CrossRef]
- Anderson, J.L.; Morrow, D.A. Acute Myocardial Infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H.; Boehncke, S.; Schön, M.P. Managing comorbid disease in patients with psoriasis. BMJ 2010, 340, b5666. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H.; Boehncke, S. Cardiovascular mortality in psoriasis and psoriatic arthritis: Epidemiology, pathomechanisms, therapeutic implications, and perspectives. Curr. Rheumatol. Rep. 2012, 14, 343–348. [Google Scholar] [CrossRef]
- Boehncke, W.H. Systemic Inflammation and Cardiovascular Comorbidity in Psoriasis Patients: Causes and Consequences. Front. Immunol. 2018, 9, 579. [Google Scholar] [CrossRef]
- Von Stebut, E.; Boehncke, W.H.; Ghoreschi, K.; Gori, T.; Kaya, Z.; Thaci, D.; Schäffler, A. IL-17A in Psoriasis and Beyond: Cardiovascular and Metabolic Implications. Front. Immunol. 2019, 10, 3096. [Google Scholar] [CrossRef]
- Ahlehoff, O.; Gislason, G.H.; Jørgensen, C.H.; Lindhardsen, J.; Charlot, M.; Olesen, J.B.; Abildstrøm, S.Z.; Skov, L.; Torp-Pedersen, C.; Hansen, P.R. Psoriasis and risk of atrial fibrillation and ischaemic stroke: A Danish Nationwide Cohort Study. Eur. Heart J. 2012, 33, 2054–2064. [Google Scholar] [CrossRef]
- Kimball, A.B.; Guerin, A.; Latremouille-Viau, D.; Yu, A.P.; Gupta, S.; Bao, Y.; Mulani, P. Coronary heart disease and stroke risk in patients with psoriasis: Retrospective analysis. Am. J. Med. 2010, 123, 350–357. [Google Scholar] [CrossRef]
- Choi, H.; Uceda, D.E.; Dey, A.K.; Abdelrahman, K.M.; Aksentijevich, M.; Rodante, J.A.; Elnabawi, Y.A.; Reddy, A.; Keel, A.; Erb-Alvarez, J.; et al. Treatment of Psoriasis with Biologic Therapy Is Associated With Improvement of Coronary Artery Plaque Lipid-Rich Necrotic Core: Results From a Prospective, Observational Study. Circ. Cardiovasc Imaging 2020, 13, e011199. [Google Scholar] [CrossRef]
- Jatwani, S.; Jatwani, K.; Tiwari, P.; Wadhwa, N.; Chugh, K. Trends in hospitalisations and inpatient mortality from acute myocardial infarction among patients with psoriatic arthritis: An analysis of nationwide inpatient sample 2004–2014. Clin. Exp. Rheumatol. 2021, 39, 790–794. [Google Scholar]
- Wu, J.J.; Poon, K.Y.; Channual, J.C.; Shen, A.Y. Association between tumor necrosis factor inhibitor therapy and myocardial infarction risk in patients with psoriasis. Arch. Dermatol. 2012, 148, 1244–1250. [Google Scholar] [CrossRef]
- Persson, R.; Hagberg, K.W.; Qian, Y.; Vasilakis-Scaramozza, C.; Jick, S. The risk of myocardial infarction, stroke, and revascularization among patients with psoriasis treated with apremilast compared with biologics and disease-modifying antirheumatic drugs: A cohort study in the US MarketScan database. J. Am. Acad. Dermatol. 2020, 83, 271–274. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Shin, D.B.; Duffin, K.C.; Armstrong, A.W.; Blauvelt, A.; Tyring, S.K.; Menter, A.; Gottlieb, S.; Lockshin, B.N.; Simpson, E.L.; et al. A Randomized Placebo-Controlled Trial of Secukinumab on Aortic Vascular Inflammation in Moderate-to-Severe Plaque Psoriasis (VIP-S). J. Investig. Dermatol. 2020, 140, 1784–1793.e2. [Google Scholar] [CrossRef]
- Mehta, N.N.; Teague, H.L.; Swindell, W.R.; Baumer, Y.; Ward, N.L.; Xing, X.; Baugous, B.; Johnston, A.; Joshi, A.A.; Silverman, J.; et al. IFN-γ and TNF-α synergism may provide a link between psoriasis and inflammatory atherogenesis. Sci. Rep. 2017, 7, 13831. [Google Scholar] [CrossRef]
- Eid, R.E.; Rao, D.A.; Zhou, J.; Lo, S.F.; Ranjbaran, H.; Gallo, A.; Sokol, S.I.; Pfau, S.; Pober, J.S.; Tellides, G. Interleukin-17 and interferon-gamma are produced concomitantly by human coronary artery-infiltrating T cells and act synergistically on vascular smooth muscle cells. Circulation 2009, 119, 1424–1432. [Google Scholar] [CrossRef]
- Karbach, S.; Croxford, A.L.; Oelze, M.; Schüler, R.; Minwegen, D.; Wegner, J.; Koukes, L.; Yogev, N.; Nikolaev, A.; Reißig, S.; et al. Interleukin 17 drives vascular inflammation, endothelial dysfunction, and arterial hypertension in psoriasis-like skin disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2658–2668. [Google Scholar] [CrossRef]
- Garshick, M.S.; Barrett, T.J.; Wechter, T.; Azarchi, S.; Scher, J.U.; Neimann, A.; Katz, S.; Fuentes-Duculan, J.; Cannizzaro, M.V.; Jelic, S.; et al. Inflammasome Signaling and Impaired Vascular Health in Psoriasis. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 787–798. [Google Scholar] [CrossRef]
- Garshick, M.S.; Tawil, M.; Barrett, T.J.; Salud-Gnilo, C.M.; Eppler, M.; Lee, A.; Scher, J.U.; Neimann, A.L.; Jelic, S.; Mehta, N.N.; et al. Activated Platelets Induce Endothelial Cell Inflammatory Response in Psoriasis via COX-1. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1340–1351. [Google Scholar] [CrossRef]
- Verma, D.; Fekri, S.Z.; Sigurdardottir, G.; Bivik Eding, C.; Sandin, C.; Enerbäck, C. Enhanced Inflammasome Activity in Patients with Psoriasis Promotes Systemic Inflammation. J. Investig. Dermatol. 2021, 141, 586–595.e5. [Google Scholar] [CrossRef]
- Vila, L.; Cullaré, C.; Solá, J.; Puig, L.; de Castellarnau, C.; de Moragas, J.M. Cyclooxygenase activity is increased in platelets from psoriatic patients. J. Investig. Dermatol. 1991, 97, 922–926. [Google Scholar] [CrossRef]
- Garshick, M.S.; Ward, N.L.; Krueger, J.G.; Berger, J.S. Cardiovascular Risk in Patients With Psoriasis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2021, 77, 1670–1680. [Google Scholar] [CrossRef]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Paskins, Z.; Whittle, R.; Abdul Sultan, A.; Muller, S.; Blagojevic-Bucknall, M.; Helliwell, T.; Packham, J.; Hider, S.; Roddy, E.; Mallen, C. Risk of fragility fracture among patients with late-onset psoriasis: A UK population-based study. Osteoporos. Int. 2018, 29, 1659–1664. [Google Scholar] [CrossRef]
- Ogdie, A.; Harter, L.; Shin, D.; Baker, J.; Takeshita, J.; Choi, H.K.; Love, T.J.; Gelfand, J.M. The risk of fracture among patients with psoriatic arthritis and psoriasis: A population-based study. Ann. Rheum. Dis. 2017, 76, 882–885. [Google Scholar] [CrossRef]
- Kastelan, D.; Kastelan, M.; Massari, L.P.; Korsic, M. Possible association of psoriasis and reduced bone mineral density due to increased TNF-alpha and IL-6 concentrations. Med. Hypotheses 2006, 67, 1403–1405. [Google Scholar] [CrossRef]
- Kotake, S.; Udagawa, N.; Takahashi, N.; Matsuzaki, K.; Itoh, K.; Ishiyama, S.; Saito, S.; Inoue, K.; Kamatani, N.; Gillespie, M.T.; et al. IL-17 in synovial fluids from patients with rheumatoid arthritis is a potent stimulator of osteoclastogenesis. J. Clin. Investig. 1999, 103, 1345–1352. [Google Scholar] [CrossRef]
- Shukla, P.; Mansoori, M.N.; Singh, D. Efficacy of anti-IL-23 monotherapy versus combination therapy with anti-IL-17 in estrogen deficiency induced bone loss conditions. Bone 2018, 110, 84–95. [Google Scholar] [CrossRef]
- Brunt, E.M.; Wong, V.W.; Nobili, V.; Day, C.P.; Sookoian, S.; Maher, J.J.; Bugianesi, E.; Sirlin, C.B.; Neuschwander-Tetri, B.A.; Rinella, M.E. Nonalcoholic fatty liver disease. Nat. Rev. Dis. Primers 2015, 1, 15080. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Barba, E.; Girolomoni, G. Non-alcoholic fatty liver disease fibrosis score in patients with psoriasis. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Targher, G.; Zoppini, G.; Girolomoni, G. Non-alcoholic fatty liver disease in patients with chronic plaque psoriasis. J. Hepatol. 2009, 51, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Candia, R.; Ruiz, A.; Torres-Robles, R.; Chávez-Tapia, N.; Méndez-Sánchez, N.; Arrese, M. Risk of non-alcoholic fatty liver disease in patients with psoriasis: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 656–662. [Google Scholar] [CrossRef]
- Romero-Pérez, D.; Belinchón-Romero, I.; Bellot, P.; Francés, R.; Marco, F.; Ramos-Rincón, J.M. Nonalcoholic fatty liver disease puts patients with psoriasis at greater cardiovascular risk. Australas. J. Dermatol. 2019, 60, e304–e310. [Google Scholar] [CrossRef]
- Campanati, A.; Ganzetti, G.; Di Sario, A.; Damiani, A.; Sandroni, L.; Rosa, L.; Benedetti, A.; Offidani, A. The effect of etanercept on hepatic fibrosis risk in patients with non-alcoholic fatty liver disease, metabolic syndrome, and psoriasis. J. Gastroenterol. 2013, 48, 839–846. [Google Scholar] [CrossRef]
- He, B.; Wu, L.; Xie, W.; Shao, Y.; Jiang, J.; Zhao, Z.; Yan, M.; Chen, Z.; Cui, D. The imbalance of Th17/Treg cells is involved in the progression of nonalcoholic fatty liver disease in mice. BMC Immunol. 2017, 18, 33. [Google Scholar] [CrossRef]
- Li, F.; Hao, X.; Chen, Y.; Bai, L.; Gao, X.; Lian, Z.; Wei, H.; Sun, R.; Tian, Z. The microbiota maintain homeostasis of liver-resident γδT-17 cells in a lipid antigen/CD1d-dependent manner. Nat. Commun. 2017, 7, 13839. [Google Scholar] [CrossRef]
- Rau, M.; Schilling, A.K.; Meertens, J.; Hering, I.; Weiss, J.; Jurowich, C.; Kudlich, T.; Hermanns, H.M.; Bantel, H.; Beyersdorf, N.; et al. Progression from Nonalcoholic Fatty Liver to Nonalcoholic Steatohepatitis Is Marked by a Higher Frequency of Th17 Cells in the Liver and an Increased Th17/Resting Regulatory T Cell Ratio in Peripheral Blood and in the Liver. J. Immunol. 2016, 196, 97–105. [Google Scholar] [CrossRef]
- Tang, Y.; Bian, Z.; Zhao, L.; Liu, Y.; Liang, S.; Wang, Q.; Han, X.; Peng, Y.; Chen, X.; Shen, L.; et al. Interleukin-17 exacerbates hepatic steatosis and inflammation in non-alcoholic fatty liver disease. Clin. Exp. Immunol. 2011, 166, 281–290. [Google Scholar] [CrossRef]
- Gomes, A.L.; Teijeiro, A.; Burén, S.; Tummala, K.S.; Yilmaz, M.; Waisman, A.; Theurillat, J.P.; Perna, C.; Djouder, N. Metabolic Inflammation-Associated IL-17A Causes Non-alcoholic Steatohepatitis and Hepatocellular Carcinoma. Cancer Cell 2016, 30, 161–175. [Google Scholar] [CrossRef]
- Rolla, S.; Alchera, E.; Imarisio, C.; Bardina, V.; Valente, G.; Cappello, P.; Mombello, C.; Follenzi, A.; Novelli, F.; Carini, R. The balance between IL-17 and IL-22 produced by liver-infiltrating T-helper cells critically controls NASH development in mice. Clin. Sci. 2016, 130, 193–203. [Google Scholar] [CrossRef]
- Romagnani, P.; Remuzzi, G.; Glassock, R.; Levin, A.; Jager, K.J.; Tonelli, M.; Massy, Z.; Wanner, C.; Anders, H.J. Chronic kidney disease. Nat. Rev. Dis. Primers 2017, 3, 17088. [Google Scholar] [CrossRef]
- Jabbar-Lopez, Z.K.; Weatherhead, S.C.; Reynolds, N.J. Kidney disease in moderate-to-severe psoriasis: A critical appraisal. Br. J. Dermatol. 2016, 174, 267–270. [Google Scholar] [CrossRef]
- Ungprasert, P.; Raksasuk, S. Psoriasis and risk of incident chronic kidney disease and end-stage renal disease: A systematic review and meta-analysis. Int. Urol. Nephrol. 2018, 50, 1277–1283. [Google Scholar] [CrossRef]
- Chiu, H.Y.; Huang, H.L.; Li, C.H.; Yin, Y.J.; Chen, H.A.; Hsu, S.T.; Lin, S.J.; Tsai, T.F.; Ho, S.Y. Increased risk of glomerulonephritis and chronic kidney disease in relation to the severity of psoriasis, concomitant medication, and comorbidity: A nationwide population-based cohort study. Br. J. Dermatol. 2015, 173, 146–154. [Google Scholar] [CrossRef]
- Lee, E.; Han, J.H.; Bang, C.H.; Yoo, S.A.; Han, K.D.; Kim, H.N.; Park, Y.M.; Lee, J.Y.; Lee, J.H. Risk of End-Stage Renal Disease in Psoriatic Patients: Real-World Data from a Nationwide Population-Based Cohort Study. Sci. Rep. 2019, 9, 16581. [Google Scholar] [CrossRef]
- Veronesi, G.; Guglielmo, A.; Gardini, A.; Sacchelli, L.; Loi, C.; Patrizi, A.; Bardazzi, F. Biological therapy in patients with psoriasis: What we know about the effects on renal function. Dermatol. Ther. 2022, 35, e15202. [Google Scholar] [CrossRef]
- Chung, B.H.; Kim, K.W.; Sun, I.O.; Choi, S.R.; Park, H.S.; Jeon, E.J.; Kim, B.M.; Choi, B.S.; Park, C.W.; Kim, Y.S.; et al. Increased interleukin-17 producing effector memory T cells in the end-stage renal disease patients. Immunol. Lett. 2012, 141, 181–189. [Google Scholar] [CrossRef]
- Lavoz, C.; Matus, Y.S.; Orejudo, M.; Carpio, J.D.; Droguett, A.; Egido, J.; Mezzano, S.; Ruiz-Ortega, M. Interleukin-17A blockade reduces albuminuria and kidney injury in an accelerated model of diabetic nephropathy. Kidney Int. 2019, 95, 1418–1432. [Google Scholar] [CrossRef]
- Mehrotra, P.; Patel, J.B.; Ivancic, C.M.; Collett, J.A.; Basile, D.P. Th-17 cell activation in response to high salt following acute kidney injury is associated with progressive fibrosis and attenuated by AT-1R antagonism. Kidney Int. 2015, 88, 776–784. [Google Scholar] [CrossRef]
- Odobasic, D.; Gan, P.Y.; Summers, S.A.; Semple, T.J.; Muljadi, R.C.; Iwakura, Y.; Kitching, A.R.; Holdsworth, S.R. Interleukin-17A promotes early but attenuates established disease in crescentic glomerulonephritis in mice. Am. J. Pathol. 2011, 179, 1188–1198. [Google Scholar] [CrossRef]
- Oh, J.; Jung, K.J.; Kim, T.G.; Kim, H.W.; Jee, S.H.; Lee, M.G. Risk of psychiatric diseases among patients with psoriasis in Korea: A 12-year nationwide population-based cohort study. J. Dermatol. 2021, 48, 1763–1771. [Google Scholar] [CrossRef]
- Egeberg, A.; Thyssen, J.P.; Wu, J.J.; Skov, L. Risk of first-time and recurrent depression in patients with psoriasis: A population-based cohort study. Br. J. Dermatol. 2019, 180, 116–121. [Google Scholar] [CrossRef]
- Brandon, T.G.; Manos, C.K.; Xiao, R.; Ogdie, A.; Weiss, P.F. Pediatric psoriatic arthritis: A population-based cohort study of risk factors for onset and subsequent risk of inflammatory comorbidities. J. Psoriasis. Psoriatic Arthritis 2018, 3, 131–136. [Google Scholar] [CrossRef]
- Egeberg, A.; Khalid, U.; Gislason, G.H.; Mallbris, L.; Skov, L.; Hansen, P.R. Association between depression and risk of atrial fibrillation and stroke in patients with psoriasis: A Danish nationwide cohort study. Br. J. Dermatol. 2015, 173, 471–479. [Google Scholar] [CrossRef]
- Strober, B.; Gooderham, M.; de Jong, E.; Kimball, A.B.; Langley, R.G.; Lakdawala, N.; Goyal, K.; Lawson, F.; Langholff, W.; Hopkins, L.; et al. Depressive symptoms, depression, and the effect of biologic therapy among patients in Psoriasis Longitudinal Assessment and Registry (PSOLAR). J. Am. Acad. Dermatol. 2018, 78, 70–80. [Google Scholar] [CrossRef]
- Westfall, S.; Caracci, F.; Zhao, D.; Wu, Q.L.; Frolinger, T.; Simon, J.; Pasinetti, G.M. Microbiota metabolites modulate the T helper 17 to regulatory T cell (Th17/Treg) imbalance promoting resilience to stress-induced anxiety- and depressive-like behaviors. Brain Behav. Immun. 2021, 91, 350–368. [Google Scholar] [CrossRef]
- Kim, J.; Suh, Y.H.; Chang, K.A. Interleukin-17 induced by cumulative mild stress promoted depression-like behaviors in young adult mice. Mol. Brain 2021, 14, 11. [Google Scholar] [CrossRef]
- Roberts, C.G.; Ladenson, P.W. Hypothyroidism. Lancet 2004, 363, 793–803. [Google Scholar] [CrossRef]
- Vastarella, M.; Megna, M.; Lupoli, G.A.; Napolitano, M.; Gallo, L.; Balato, A.; Tasso, M.; Costa, L.; Fabbrocini, G.; Peluso, R. Is there any association between psoriasis, psoriatic arthritis and thyroid autoimmunity? Australas. J. Dermatol. 2021, 62, e207–e211. [Google Scholar] [CrossRef] [PubMed]
- Nanba, T.; Watanabe, M.; Inoue, N.; Iwatani, Y. Increases of the Th1/Th2 cell ratio in severe Hashimoto’s disease and in the proportion of Th17 cells in intractable Graves’ disease. Thyroid 2009, 19, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; You, R.; Yu, N.; Gong, Y.; Qu, C.; Zhang, Y.; Lu, G.; Huang, Y.; Zhang, H.; Gao, Y.; et al. Increased proportions of Tc17 cells and NK cells may be risk factors for disease progression in Hashimoto’s thyroiditis. Int. Immunopharmacol. 2016, 40, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Yang, Y.; Zhang, Y.; Song, S.; Zhang, L.; Ma, L.; Yang, T.; Liu, H. Macrophage migration inhibitory factor interacting with Th17 cells may be involved in the pathogenesis of autoimmune damage in Hashimoto’s thyroiditis. Mediators. Inflamm. 2015, 2015, 621072. [Google Scholar] [CrossRef]
- Konca Degertekin, C.; Aktas Yilmaz, B.; Balos Toruner, F.; Kalkanci, A.; Turhan Iyidir, O.; Fidan, I.; Yesilyurt, E.; Cakır, N.; Kustimur, S.; Arslan, M. Circulating Th17 cytokine levels are altered in Hashimoto’s thyroiditis. Cytokine 2016, 80, 13–17. [Google Scholar] [CrossRef]
- Salazar-Viedma, M.; Vergaño-Salazar, J.G.; Pastenes, L.; D’Afonseca, V. Simulation Model for Hashimoto Autoimmune Thyroiditis Disease. Endocrinology 2021, 162, bqab190. [Google Scholar] [CrossRef]
- Hayashi, F.; Watanabe, M.; Nanba, T.; Inoue, N.; Akamizu, T.; Iwatani, Y. Association of the -31C/T functional polymorphism in the interleukin-1beta gene with the intractability of Graves’ disease and the proportion of T helper type 17 cells. Clin. Exp. Immunol. 2009, 158, 281–286. [Google Scholar] [CrossRef]
- Olivieri, A.N.; Iafusco, D.; Mellos, A.; Zanfardino, A.; Mauro, A.; Granato, C.; Gicchino, M.F.; Prisco, F.; Perrone, L. Refractory rheumatoid factor positive polyarthritis in a female adolescent already suffering from type 1 diabetes mellitus and Hashimoto’s thyroiditis successfully treated with etanercept. Ital. J. Pediatr. 2013, 39, 64. [Google Scholar] [CrossRef][Green Version]
- Knopman, D.S.; Amieva, H.; Petersen, R.C.; Chételat, G.; Holtzman, D.M.; Hyman, B.T.; Nixon, R.A.; Jones, D.T. Alzheimer disease. Nat. Rev. Dis. Primers 2021, 7, 33. [Google Scholar] [CrossRef]
- Kim, M.; Park, H.E.; Lee, S.H.; Han, K.; Lee, J.H. Increased risk of Alzheimer’s disease in patients with psoriasis: A nationwide population-based cohort study. Sci. Rep. 2020, 10, 6454. [Google Scholar] [CrossRef]
- Zhou, M.; Xu, R.; Kaelber, D.C.; Gurney, M.E. Tumor Necrosis Factor (TNF) blocking agents are associated with lower risk for Alzheimer’s disease in patients with rheumatoid arthritis and psoriasis. PLoS ONE 2020, 15, e0229819. [Google Scholar] [CrossRef]
- Oberstein, T.J.; Taha, L.; Spitzer, P.; Hellstern, J.; Herrmann, M.; Kornhuber, J.; Maler, J.M. Imbalance of Circulating T(h)17 and Regulatory T Cells in Alzheimer’s Disease: A Case Control Study. Front. Immunol. 2018, 9, 1213. [Google Scholar] [CrossRef]
- Zhang, J.; Ke, K.F.; Liu, Z.; Qiu, Y.H.; Peng, Y.P. Th17 cell-mediated neuroinflammation is involved in neurodegeneration of aβ1-42-induced Alzheimer’s disease model rats. PLoS ONE 2013, 8, e75786. [Google Scholar] [CrossRef]
- Cristiano, C.; Volpicelli, F.; Lippiello, P.; Buono, B.; Raucci, F.; Piccolo, M.; Iqbal, A.J.; Irace, C.; Miniaci, M.C.; Perrone Capano, C.; et al. Neutralization of IL-17 rescues amyloid-β-induced neuroinflammation and memory impairment. Br. J. Pharmacol. 2019, 176, 3544–3557. [Google Scholar] [CrossRef]
- Xu, J.J.; Guo, S.; Xue, R.; Xiao, L.; Kou, J.N.; Liu, Y.Q.; Han, J.Y.; Fu, J.J.; Wei, N. Adalimumab ameliorates memory impairments and neuroinflammation in chronic cerebral hypoperfusion rats. Aging 2021, 13, 14001–14014. [Google Scholar] [CrossRef]
- Bachert, C.; Marple, B.; Schlosser, R.J.; Hopkins, C.; Schleimer, R.P.; Lambrecht, B.N.; Bröker, B.M.; Laidlaw, T.; Song, W.J. Adult chronic rhinosinusitis. Nat. Rev. Dis. Primers 2020, 6, 86. [Google Scholar] [CrossRef]
- Keller, J.J.; Wu, C.S.; Lin, H.C. Increased risk of psoriasis following chronic rhinosinusitis without nasal polyps: A population-based matched-cohort study. Br. J. Dermatol. 2013, 168, 289–294. [Google Scholar] [CrossRef]
- Jiang, X.D.; Li, G.Y.; Li, L.; Dong, Z.; Zhu, D.D. The characterization of IL-17A expression in patients with chronic rhinosinusitis with nasal polyps. Am. J. Rhinol. Allergy 2011, 25, e171–e175. [Google Scholar] [CrossRef]
- Miljkovic, D.; Psaltis, A.; Wormald, P.J.; Vreugde, S. T regulatory and Th17 cells in chronic rhinosinusitis with polyps. Int. Forum. Allergy Rhinol. 2016, 6, 826–834. [Google Scholar] [CrossRef]
- Miljkovic, D.; Psaltis, A.J.; Wormald, P.J.; Vreugde, S. Chronic Rhinosinusitis with Polyps Is Characterized by Increased Mucosal and Blood Th17 Effector Cytokine Producing Cells. Front. Physiol. 2017, 8, 898. [Google Scholar] [CrossRef]
- Li, H.; Wang, Y.; Wang, J. Th17/Treg cells regulated by interleukin 6 in the pathogenesis of chronic rhinosinusitis with nasal polyps. Eur. Arch. Otorhinolaryngol. 2021. [Google Scholar] [CrossRef]
- Ramezanpour, M.; Moraitis, S.; Smith, J.L.; Wormald, P.J.; Vreugde, S. Th17 Cytokines Disrupt the Airway Mucosal Barrier in Chronic Rhinosinusitis. Mediat. Inflamm. 2016, 2016, 9798206. [Google Scholar] [CrossRef]
- Wang, M.; Zhang, N.; Zheng, M.; Li, Y.; Meng, L.; Ruan, Y.; Han, J.; Zhao, N.; Wang, X.; Zhang, L.; et al. Cross-talk between T(H)2 and T(H)17 pathways in patients with chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2019, 144, 1254–1264. [Google Scholar] [CrossRef]
- Zondervan, K.T.; Becker, C.M.; Koga, K.; Missmer, S.A.; Taylor, R.N.; Viganò, P. Endometriosis. Nat. Rev. Dis. Primers 2018, 4, 9. [Google Scholar] [CrossRef]
- Harris, H.R.; Costenbader, K.H.; Mu, F.; Kvaskoff, M.; Malspeis, S.; Karlson, E.W.; Missmer, S.A. Endometriosis and the risks of systemic lupus erythematosus and rheumatoid arthritis in the Nurses’ Health Study II. Ann. Rheum. Dis. 2016, 75, 1279–1284. [Google Scholar] [CrossRef]
- Harris, H.R.; Korkes, K.M.N.; Li, T.; Kvaskoff, M.; Cho, E.; Carvalho, L.F.; Qureshi, A.A.; Abrao, M.; Missmer, S.A. Endometriosis, psoriasis and psoriatic arthritis: A prospective cohort study. Am. J. Epidemiol. 2022. [Google Scholar] [CrossRef]
- Ahn, S.H.; Edwards, A.K.; Singh, S.S.; Young, S.L.; Lessey, B.A.; Tayade, C. IL-17A Contributes to the Pathogenesis of Endometriosis by Triggering Proinflammatory Cytokines and Angiogenic Growth Factors. J. Immunol. 2015, 195, 2591–2600. [Google Scholar] [CrossRef]
- Duplechain, A.; Conrady, C.D.; Patel, B.C.; Baker, S. Uveitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Braithwaite, T.; Adderley, N.J.; Subramanian, A.; Galloway, J.; Kempen, J.H.; Gokhale, K.; Cope, A.P.; Dick, A.D.; Nirantharakumar, K.; Denniston, A.K. Epidemiology of Scleritis in the United Kingdom From 1997 to 2018: Population-Based Analysis of 11 Million Patients and Association Between Scleritis and Infectious and Immune-Mediated Inflammatory Disease. Arthritis Rheumatol. 2021, 73, 1267–1276. [Google Scholar] [CrossRef]
- Egeberg, A.; Khalid, U.; Gislason, G.H.; Mallbris, L.; Skov, L.; Hansen, P.R. Association of Psoriatic Disease With Uveitis: A Danish Nationwide Cohort Study. JAMA Dermatol. 2015, 151, 1200–1205. [Google Scholar] [CrossRef]
- Amadi-Obi, A.; Yu, C.R.; Liu, X.; Mahdi, R.M.; Clarke, G.L.; Nussenblatt, R.B.; Gery, I.; Lee, Y.S.; Egwuagu, C.E. TH17 cells contribute to uveitis and scleritis and are expanded by IL-2 and inhibited by IL-27/STAT1. Nat. Med. 2007, 13, 711–718. [Google Scholar] [CrossRef]
- Yoshimura, T.; Sonoda, K.H.; Ohguro, N.; Ohsugi, Y.; Ishibashi, T.; Cua, D.J.; Kobayashi, T.; Yoshida, H.; Yoshimura, A. Involvement of Th17 cells and the effect of anti-IL-6 therapy in autoimmune uveitis. Rheumatology 2009, 48, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Zhou, R.; Luger, D.; Zhu, W.; Silver, P.B.; Grajewski, R.S.; Su, S.B.; Chan, C.C.; Adorini, L.; Caspi, R.R. Calcitriol suppresses antiretinal autoimmunity through inhibitory effects on the Th17 effector response. J. Immunol. 2009, 182, 4624–4632. [Google Scholar] [CrossRef] [PubMed]
- Schatteman, L.; Mielants, H.; Veys, E.M.; Cuvelier, C.; De Vos, M.; Gyselbrecht, L.; Elewaut, D.; Goemaere, S. Gut inflammation in psoriatic arthritis: A prospective ileocolonoscopic study. J. Rheumatol. 1995, 22, 680–683. [Google Scholar] [PubMed]
- Leppkes, M.; Becker, C.; Ivanov, I.I.; Hirth, S.; Wirtz, S.; Neufert, C.; Pouly, S.; Murphy, A.J.; Valenzuela, D.M.; Yancopoulos, G.D.; et al. RORgamma-expressing Th17 cells induce murine chronic intestinal inflammation via redundant effects of IL-17A and IL-17F. Gastroenterology 2009, 136, 257–267. [Google Scholar] [CrossRef]
- Fina, D.; Sarra, M.; Fantini, M.C.; Rizzo, A.; Caruso, R.; Caprioli, F.; Stolfi, C.; Cardolini, I.; Dottori, M.; Boirivant, M.; et al. Regulation of gut inflammation and th17 cell response by interleukin-21. Gastroenterology 2008, 134, 1038–1048. [Google Scholar] [CrossRef]
- Schmechel, S.; Konrad, A.; Diegelmann, J.; Glas, J.; Wetzke, M.; Paschos, E.; Lohse, P.; Göke, B.; Brand, S. Linking genetic susceptibility to Crohn’s disease with Th17 cell function: IL-22 serum levels are increased in Crohn’s disease and correlate with disease activity and IL23R genotype status. Inflamm. Bowel Dis. 2008, 14, 204–212. [Google Scholar] [CrossRef]
- Li, W.Q.; Han, J.L.; Chan, A.T.; Qureshi, A.A. Psoriasis, psoriatic arthritis and increased risk of incident Crohn’s disease in US women. Ann. Rheum. Dis. 2013, 72, 1200–1205. [Google Scholar] [CrossRef]
- Dreiher, J.; Weitzman, D.; Shapiro, J.; Davidovici, B.; Cohen, A.D. Psoriasis and chronic obstructive pulmonary disease: A case-control study. Br. J. Dermatol. 2008, 159, 956–960. [Google Scholar] [CrossRef]
- Chiang, Y.Y.; Lin, H.W. Association between psoriasis and chronic obstructive pulmonary disease: A population-based study in Taiwan. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 59–65. [Google Scholar] [CrossRef]
- Li, X.; Kong, L.; Li, F.; Chen, C.; Xu, R.; Wang, H.; Peng, S.; Zhou, M.; Li, B. Association between Psoriasis and Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis. PLoS ONE 2015, 10, e0145221. [Google Scholar] [CrossRef]
- Duan, M.C.; Tang, H.J.; Zhong, X.N.; Huang, Y. Persistence of Th17/Tc17 cell expression upon smoking cessation in mice with cigarette smoke-induced emphysema. Clin. Dev. Immunol. 2013, 2013, 350727. [Google Scholar] [CrossRef]
- Ito, J.T.; Cervilha, D.A.B.; Lourenço, J.D.; Gonçalves, N.G.; Volpini, R.A.; Caldini, E.G.; Landman, G.; Lin, C.J.; Velosa, A.P.P.; Teodoro, W.P.R.; et al. Th17/Treg imbalance in COPD progression: A temporal analysis using a CS-induced model. PLoS ONE 2019, 14, e0209351. [Google Scholar] [CrossRef]
- Chen, Y.; Kumar, R.K.; Thomas, P.S.; Herbert, C. Th1/17-Biased Inflammatory Environment Associated with COPD Alters the Response of Airway Epithelial Cells to Viral and Bacterial Stimuli. Mediat. Inflamm. 2019, 2019, 7281462. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inflammatory Diseases | The Influence of Psoriasis |
|---|---|
| Cerebrocardiovascular diseases | High risk [7,30,31,32,33] |
| Osteoporosis | High risk [8,46,47] |
| NAFLD | High risk [52,53,54,55] |
| Renal dysfunction | |
| Chronic kidney disease | Moderate risk [64,66] |
| End stage renal disease | High risk [65,67] |
| Psychological disorders | |
| Depression | Moderate risk [73,76] |
| Anxiety disorder | Moderate risk [73] |
| Somatoform disorder | Moderate risk [73] |
| Alzheimer’ disease | Moderate risk [90] |
| Chronic rhinosinusitis | High risk [97] |
| Endometriosis | High risk [106] |
| Uveitis | Moderate risk [110] |
| COPD | High risk [119,120,121] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tashiro, T.; Sawada, Y. Psoriasis and Systemic Inflammatory Disorders. Int. J. Mol. Sci. 2022, 23, 4457. https://doi.org/10.3390/ijms23084457
Tashiro T, Sawada Y. Psoriasis and Systemic Inflammatory Disorders. International Journal of Molecular Sciences. 2022; 23(8):4457. https://doi.org/10.3390/ijms23084457
Chicago/Turabian StyleTashiro, Tomoko, and Yu Sawada. 2022. "Psoriasis and Systemic Inflammatory Disorders" International Journal of Molecular Sciences 23, no. 8: 4457. https://doi.org/10.3390/ijms23084457
APA StyleTashiro, T., & Sawada, Y. (2022). Psoriasis and Systemic Inflammatory Disorders. International Journal of Molecular Sciences, 23(8), 4457. https://doi.org/10.3390/ijms23084457