
Overview of First-Line and Second-Line Pharmacotherapies for Osteoarthritis with Special Focus on Intra-Articular Treatment





Abstract
:1. Introduction
2. OA and Pain
3. The First-Line Therapy of Osteoarthritis
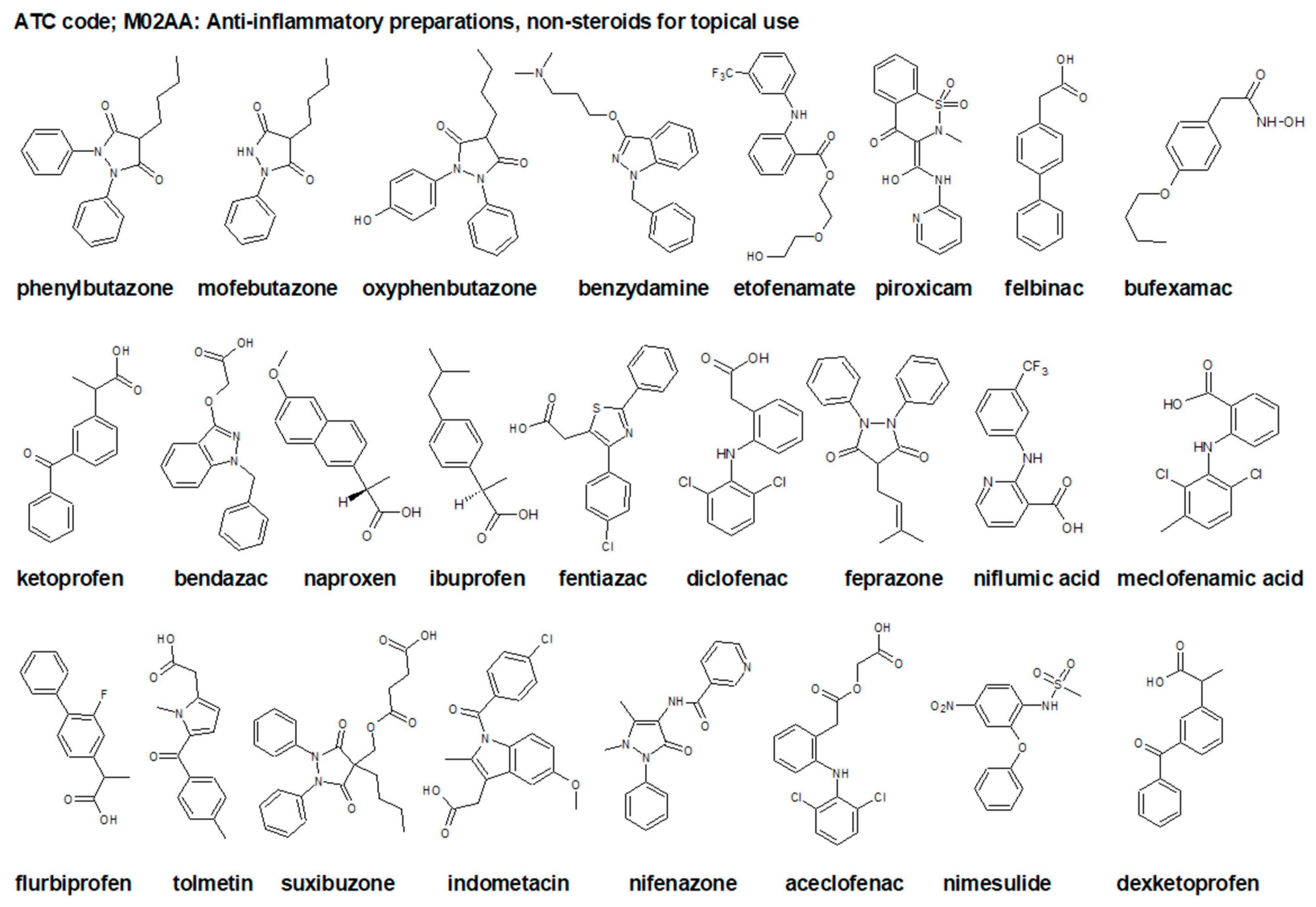
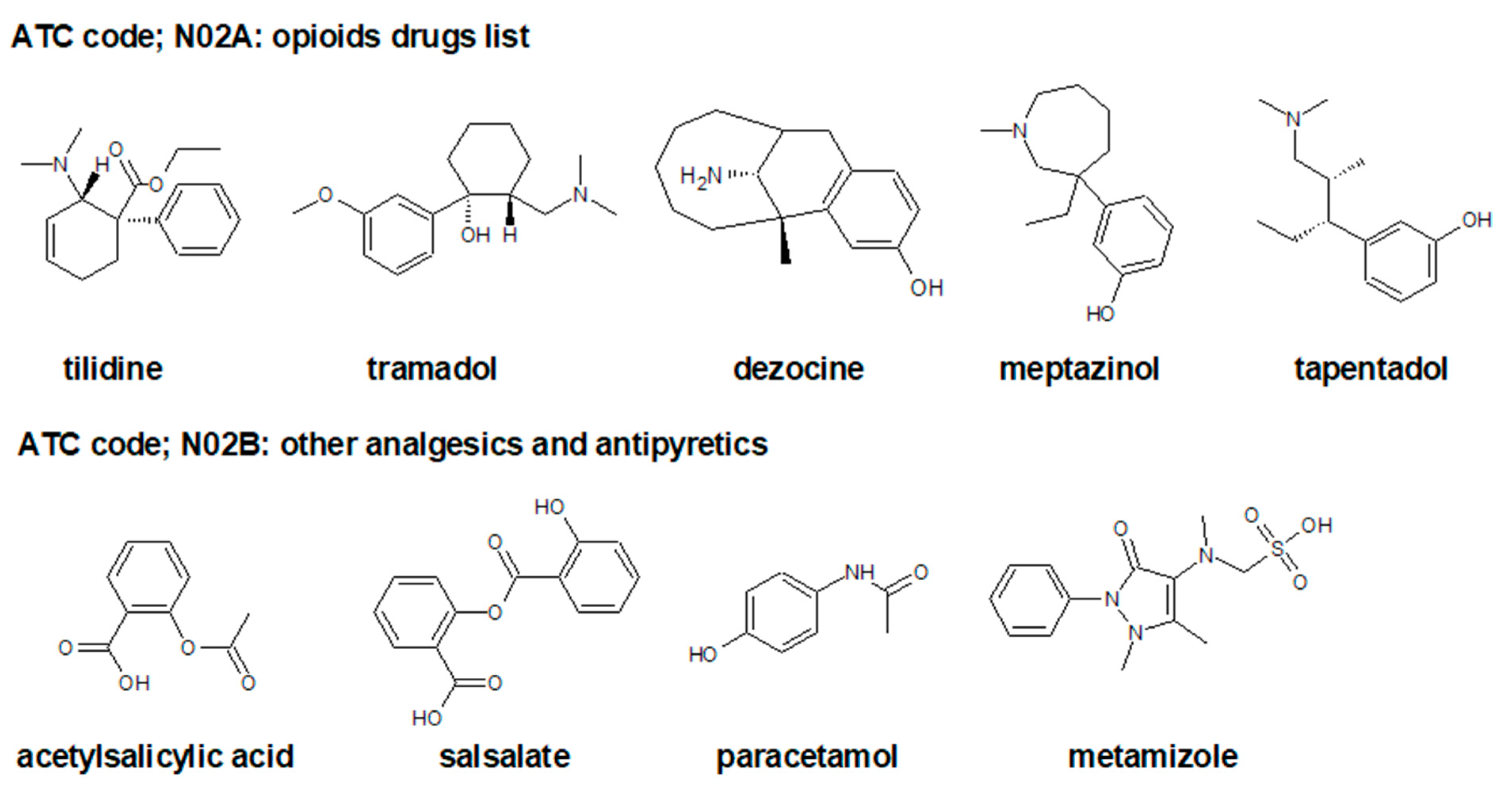
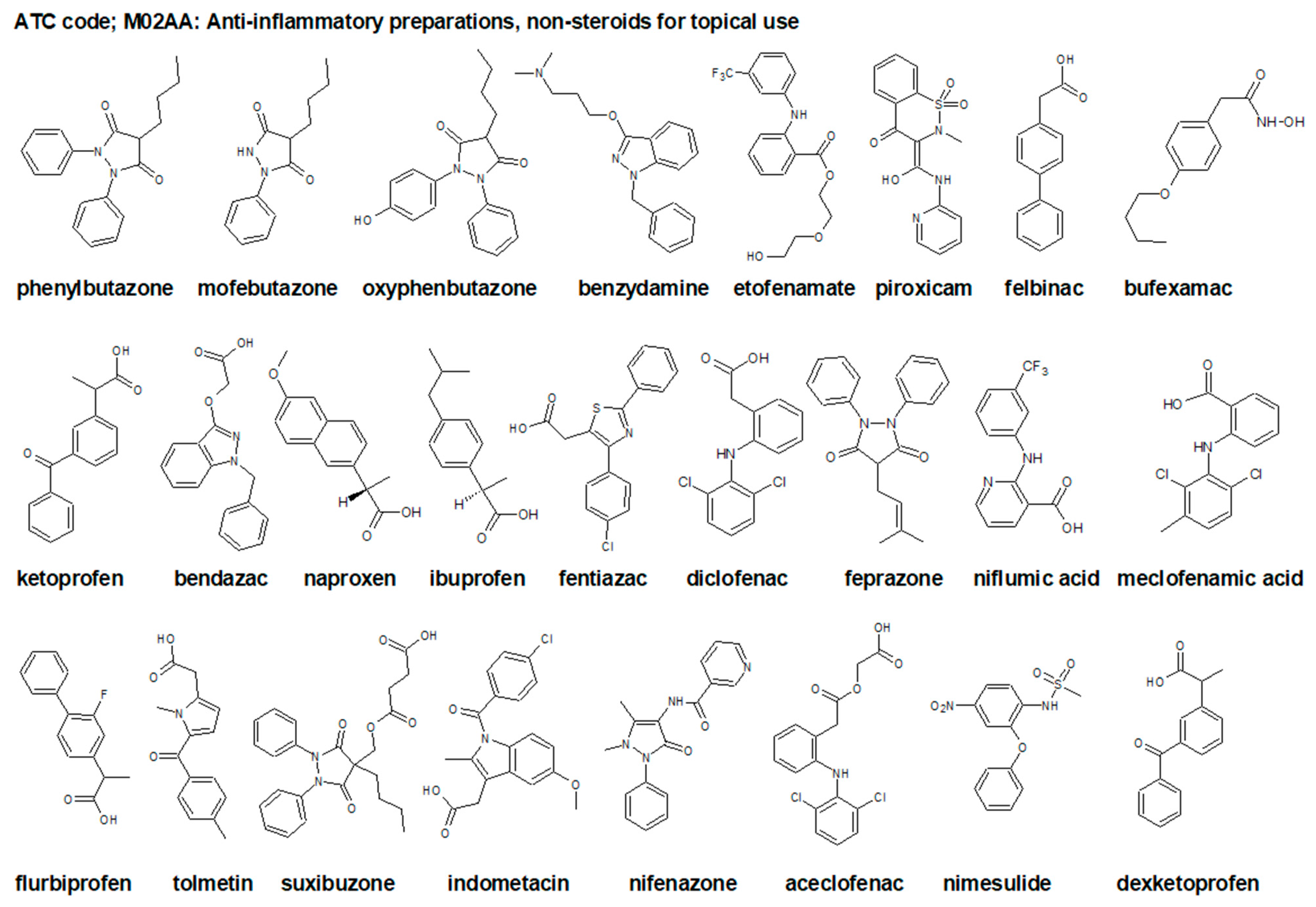
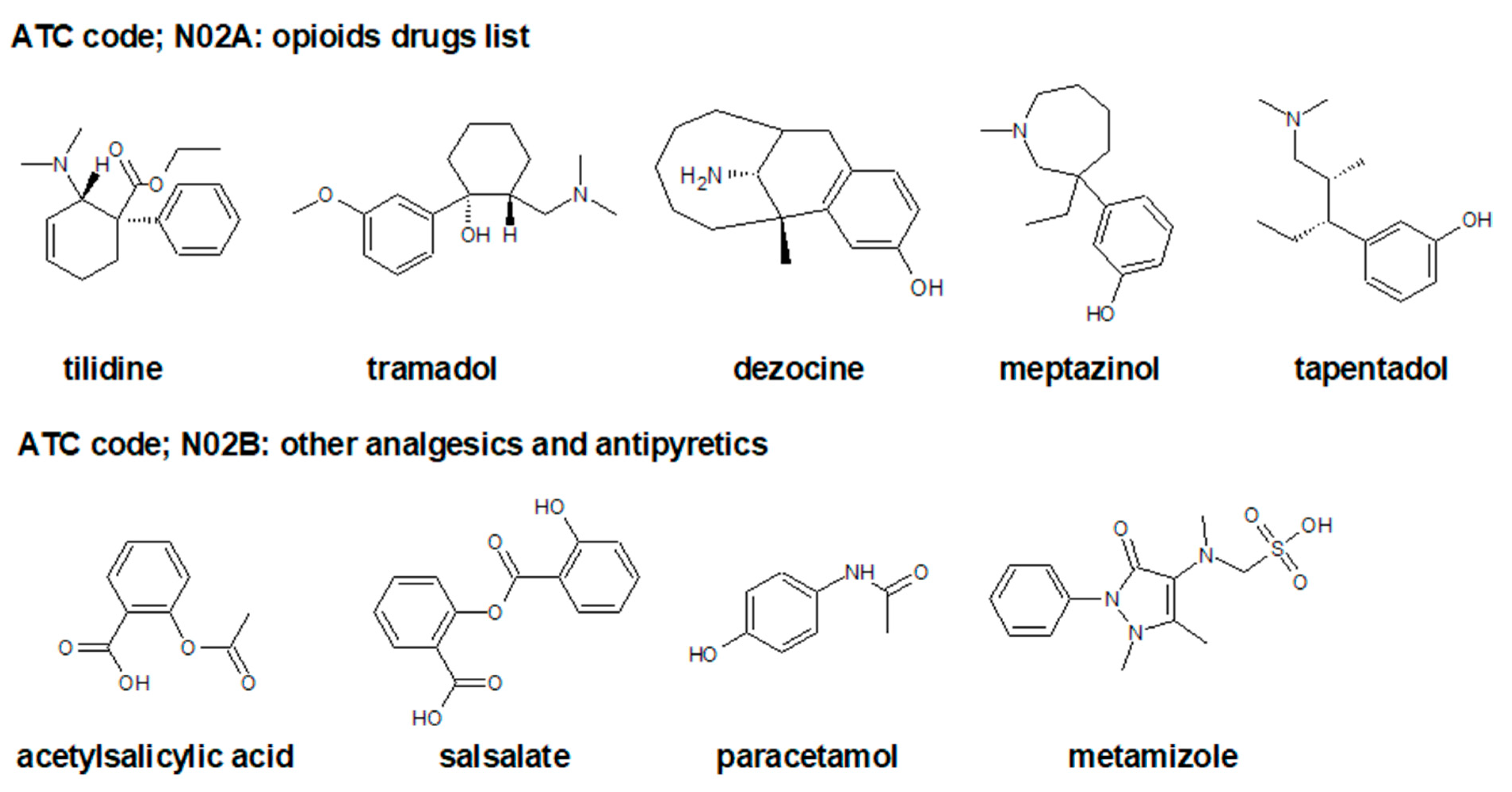
3.1. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
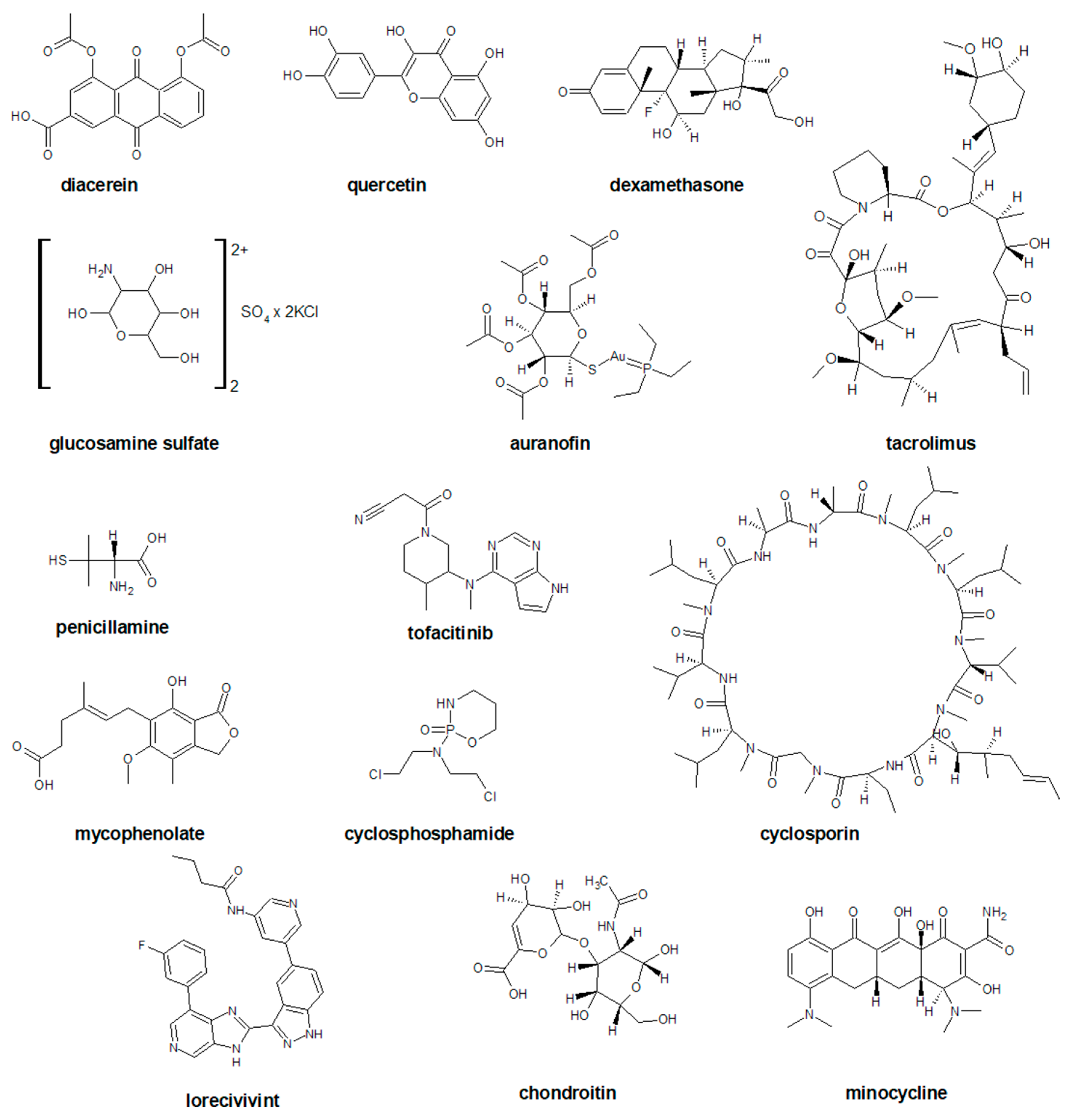
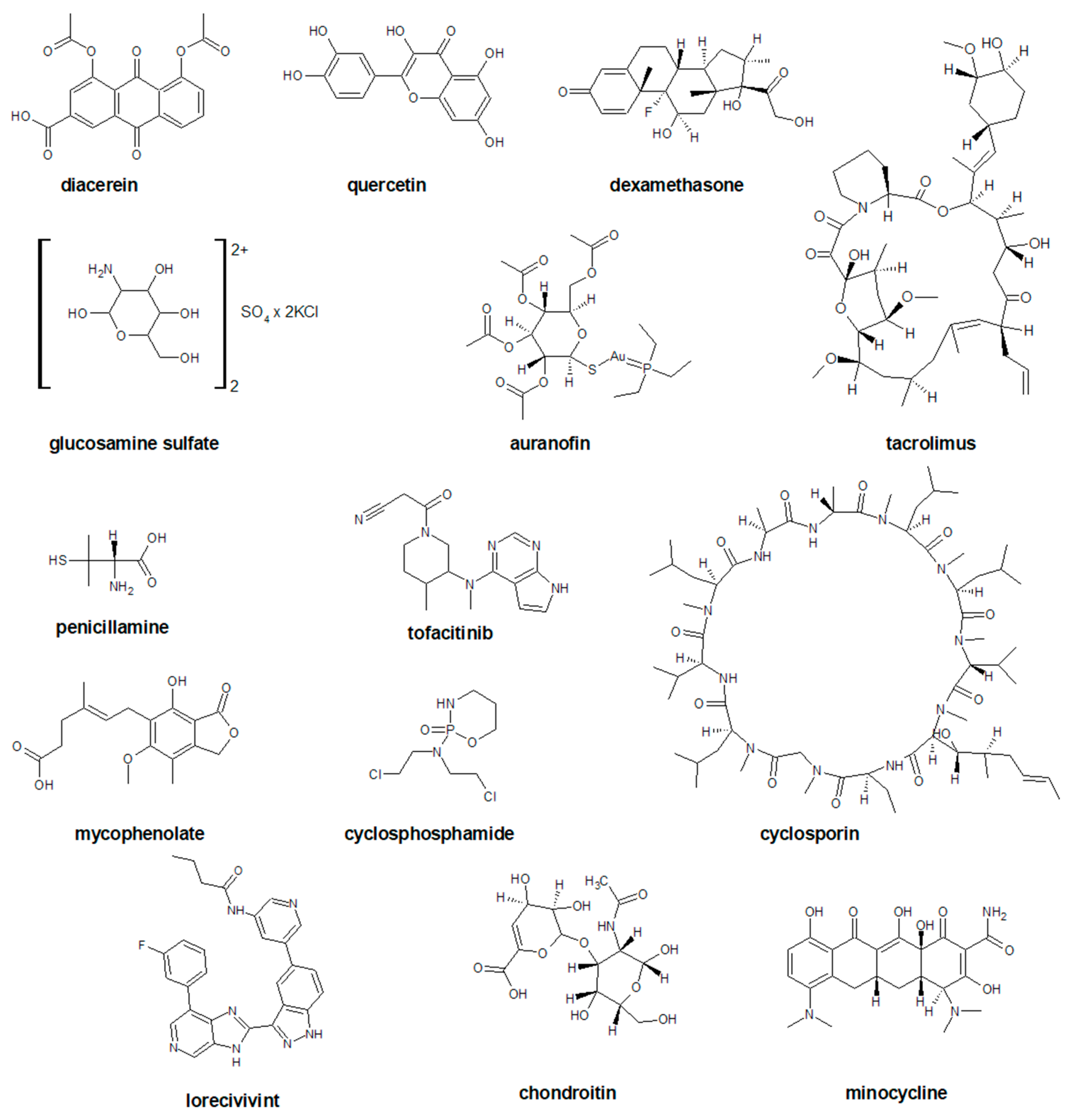
3.2. Disease Modifying Drugs for Osteoarthritis (DMOADs)
3.3. Symptomatic Slow-Acting Drugs for Osteoarthritis (SYSADOA)
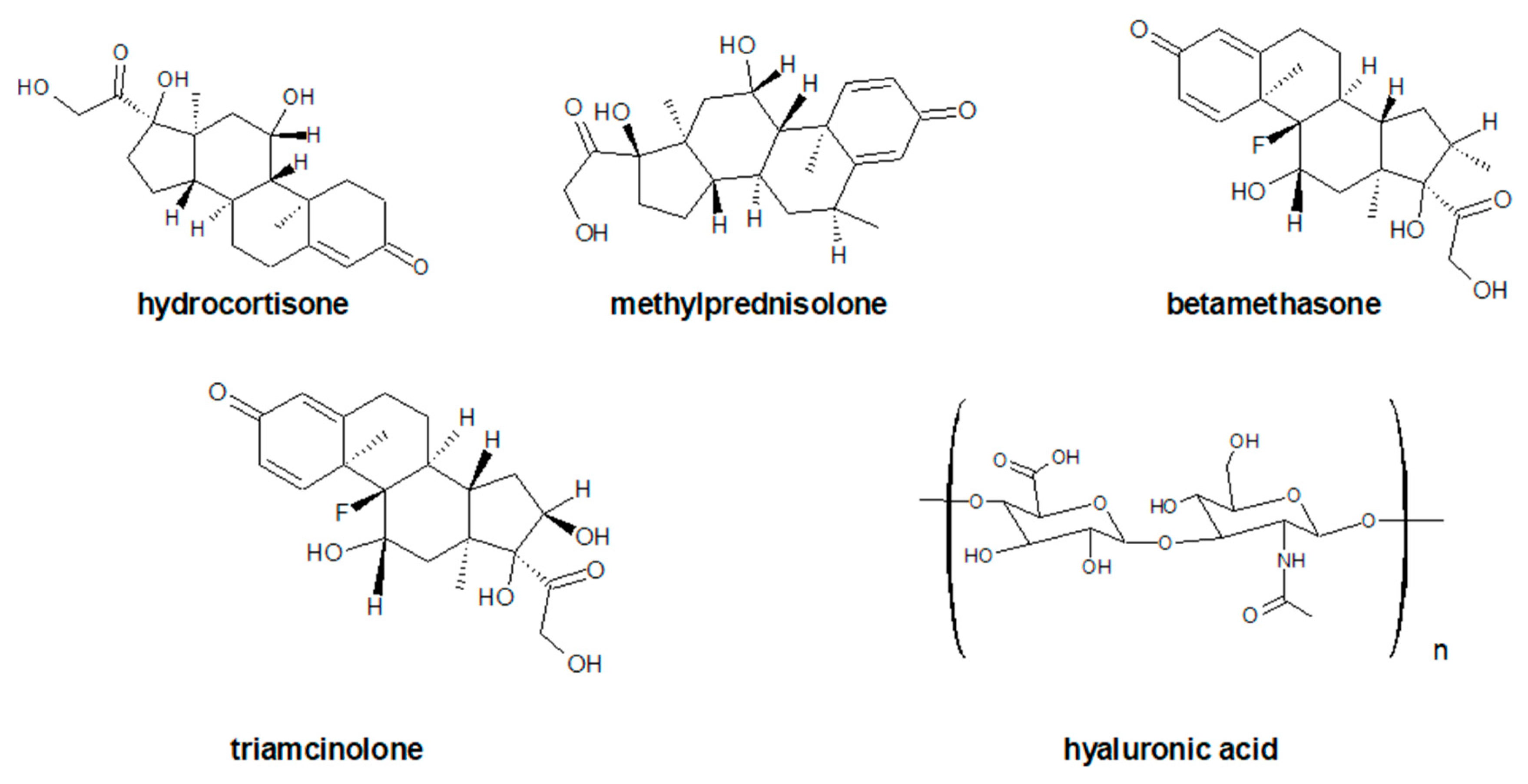
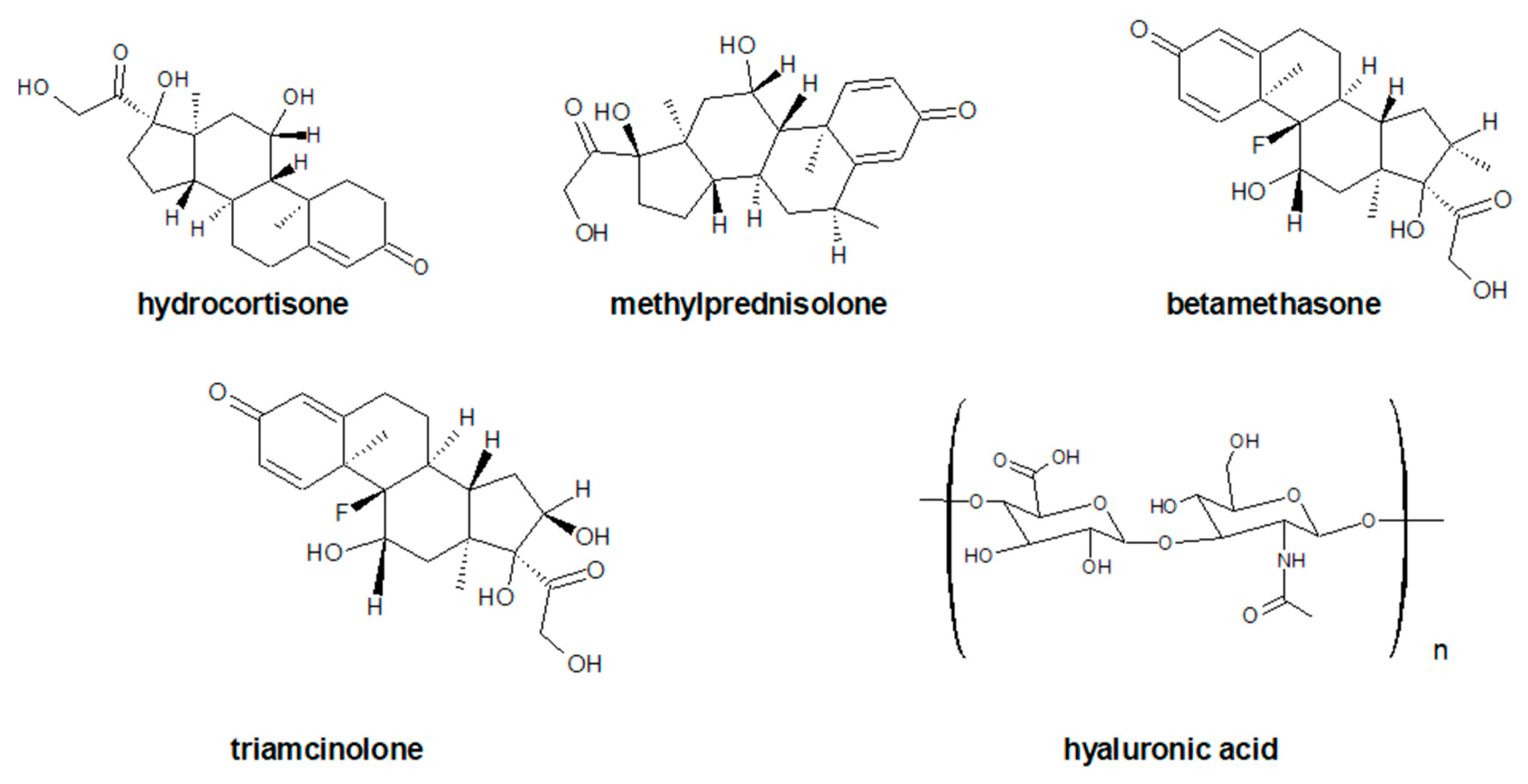
3.4. Glucorticosteroid Therapy and Viscosuplemmentation
4. Platelet-Rich Plasma (PRP)/Platelet-Rich Fibrin (PRF) as Second Line Treatment
4.1. PRP as Source of GF
4.2. PRP as Source of Cytokines
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACLT | Anterior Cruciate Ligament Transection |
| ATC | Anatomical Therapeutic Chemical Classification System |
| AAOS | The American Academic of Orthopaedic Surgeons |
| ACR | The American College of Rheumatology |
| BDNF | Brain-Derived Neurotrophic Factor |
| BMP | Bone Morphogenetic Proteins |
| CBx | Cannabinoid Receptors Type x |
| CDC kinaze x | Cyclin-Dependent Kinase Type x |
| CTGF | Connective Tissue Growth Factor |
| DMOAD | Disease-Modifying Drugs for Osteoarthritis |
| EGF | Epidermal Growth Factor |
| EMA | The European Medicines Agency |
| EULAR | The European League Against Rheumatism |
| FDA | The US Food and Drug Administration |
| FGF | Fibroblast Growth Factor |
| GF | Growth Factor |
| GS | Glucocorticosteroid |
| HA | Hyaluronic Acid |
| HGF | Hepatocyte Growth Factor |
| IA HA | Intra-Articular Hyaluronic Acid |
| IGF | Insulin-Like Growth Factor |
| IL-x | Interleukin Type x |
| IFN-γ | Interferons Type II |
| IP-10 | Interferon-Γ-Inducible Protein 10, CXCL10 |
| OA | Osteoarthritis |
| NT-x | Neurotrophin Type x |
| NFG | Nerve Growth Factor |
| NF-κB | Nuclear Factor of Kappa Light Chain Enhancer of Activated B Cells |
| NSAID | Non-Steroidal Anti-Inflammatory Drugs |
| MIBO | Minimum Information for Studies Evaluating Biologics in Orthopedics |
| MFAT | Micro-Fragmented Adipose Tissue |
| MMP-9 | Matrix Metalloproteinase-9 |
| OARSI | The Osteoarthritis Research Society International |
| PDGF | Platelet-Derived Growth Factor |
| PLT | Platelets |
| PPI | Proton Pump Inhibitors |
| PRF | Platelet-Rich Fibrin |
| PRP | Platelet-Rich Plasma |
| PsA | Psoriatic Arthritis |
| RCT | Randomized Controlled Trials |
| RANK-L | Receptor Activator for Nuclear Factor Κ B Ligand |
| RA | Rheumatoid Arthritis |
| SA | Septic Arthritis |
| SMADx | The SMAD type x Transcription Factors; The SMAD is an acronym from The Fusion Of Caenorhabditis Elegans Sma Genes And The Drosophila Mad, Mothers Against Decapentaplegic |
| SYSADOA | Symptomatic Slow-Acting Drugs For Osteoarthritis |
| TGF-x | Transforming Growth Factor Type x |
| TNFx | Tumor Necrosis Factor Type x |
| WOMAC | Western Ontario And McMaster Universities Osteoarthritis Index |
| Wnt | Wingless-Like Glycoproteins |
| VEGF | Vascular Endothelial Growth Factor |
References
- International Classification of Diseases. Available online: https://www.icd10data.com/ICD10CM/Codes/M00-M99/M05-M14/M06-/M06.9 (accessed on 10 January 2022).
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Neidhart, S.; Neidhart, M. Rheumatoid arthritis and the concept of autoimmune disease. Int. J. Clin. Rheumatol. 2019, 14, 75. [Google Scholar]
- International Classification of Diseases. Available online: https://www.icd10data.com/ICD10CM/Codes/M00-M99/M15-M19 (accessed on 10 January 2022).
- Gabay, O. Osteoarthritis: New perspectives. J. Spine 2012, 1, e101. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Yuan, M.; Meng, H.; Wang, A.; Guo, Q.; Wang, Y.; Peng, J. Basic science and clinical application of platelet-rich plasma for cartilage defects and osteoarthritis: A review. Osteoarthr. Cartil. 2013, 21, 1627–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Zhao, L.; Chen, D. Growth factor signalling in osteoarthritis. Growth Factors 2018, 36, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Szwedowski, D.; Szczepanek, J.; Paczesny, Ł.; Pękała, P.; Zabrzyński, J.; Kruczyński, J. Genetics in Cartilage Lesions: Basic Science and Therapy Approaches. IJMS 2020, 21, 5430. [Google Scholar] [CrossRef] [PubMed]
- Denk, F.; Bennett, D.L.; McMahon, S.B. Nerve growth factor and pain mechanisms. Annu. Rev. Neurosci. 2017, 40, 307–325. [Google Scholar] [CrossRef] [PubMed]
- Abramson, S.B. Nitric oxide in inflammation and pain associated with osteoarthritis. Arthritis Res. Ther. 2008, 10, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malemud, C.J. The biological basis of osteoarthritis: State of the evidence. Curr. Opin. Rheumatol. 2015, 27, 289. [Google Scholar] [CrossRef] [PubMed]
- Van Der Kraan, P.M. Differential role of transforming growth factor-beta in an osteoarthritic or a healthy joint. J. Bone Metab. 2018, 25, 65. [Google Scholar] [CrossRef]
- Glazier, R.H.; Dalby, D.M.; Badley, E.M.; Hawker, G.A.; Bell, M.J.; Buchbinder, R.; Lineker, S.C. Management of common musculoskeletal problems: Survey of Ontario primary care physicians. CMAJ 1998, 158, 1037–1040. [Google Scholar] [PubMed]
- Gnylorybov, A.M.; Ter-Vartanian, S.K.; Golovach, I.Y.; Vyrva, O.E.; Burianov, O.A.; Yesirkepova, G.S.; Irismetov, M.E.; Rizamuhamedova, M.Z.; Vardanyan, V.S.; Ginosyan, K.V. Expert Opinion on the Extensive Use of Prescription Crystalline Glucosamine Sulfate in the Multimodal Treatment of Osteoarthritis in Ukraine, Kazakhstan, Uzbekistan, and Armenia. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2020, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rasheed Kayani, R.; Shamim, R.; Sultana Munir, S.; Sultana, M.; Nazir, S.U.R.; Riaz, H.; Nazir, T.; Maaz Ali, M.; Islam, A. Medicinal Plants and Nonsteroidal Anti-inflammatory Drugs (NSAIDs) in Treatment of Arthritis: A Literature Review. Altern. Ther. Health Med. 2021; online ahead of print. [Google Scholar] [PubMed]
- Nahhas, C.R.; Fuller, B.C.; Hannon, C.P.; Gerlinger, T.L.; Nam, D.; Della Valle, C.J. Which Nonsurgical Treatments Do Patients Believe Are Most Effective for Hip and Knee Arthritis? JAAOS Glob. Res. Rev. 2020, 4, e20. [Google Scholar] [CrossRef]
- Sun, Y.; Zuo, Z.; Kuang, Y. An emerging target in the battle against osteoarthritis: Macrophage polarization. IJMS 2020, 21, 8513. [Google Scholar] [CrossRef]
- Kim, J.H.; Jin, H.M.; Kim, K.; Song, I.; Youn, B.U.; Matsuo, K.; Kim, N. The mechanism of osteoclast differentiation induced by IL-1. J. Immunol. 2009, 183, 1862–1870. [Google Scholar] [CrossRef]
- Sims, J.E.; Smith, D.E. The IL-1 family: Regulators of immunity. Nat. Rev. Immunol. 2010, 10, 89–102. [Google Scholar] [CrossRef]
- Sims, N.A.; Lorenzo, J.A. Local regulators of bone: Interleukin-1, tumor necrosis factor, interferons, the IL-6 family, and additional cytokines. In Principles of Bone Biology; Elsevier: Amsterdam, The Netherlands, 2020; pp. 1205–1246. [Google Scholar]
- Lorenzo, J.A. The Role of Interleukin-6 in Bone. J. Endocr. Soc. 2020, 4, bvaa112. [Google Scholar] [CrossRef]
- Meguid, M.H.A.; Hamad, Y.H.; Swilam, R.S.; Barakat, M.S. Relation of interleukin-6 in rheumatoid arthritis patients to systemic bone loss and structural bone damage. Rheumatol. Int. 2013, 33, 697–703. [Google Scholar] [CrossRef]
- Ciafrè, S.; Ferraguti, G.; Tirassa, P.; Iannitelli, A.; Ralli, M.; Greco, A.; Chaldakov, G.N.; Rosso, P.; Fico, E.; Messina, M.P. Nerve growth factor in the psychiatric brain. Riv. Psichiatr. 2020, 55, 4–15. [Google Scholar]
- Wise, B.L.; Seidel, M.F.; Lane, N.E. The evolution of nerve growth factor inhibition in clinical medicin. Nat. Rev. Rheumatol. 2021, 17, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Oneto, P.; Etulain, J. PRP in wound healing applications. Platelets 2021, 32, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Daste, C.; Kirren, Q.; Akoum, J.; Lefèvre-Colau, M.-M.; Rannou, F.; Nguyen, C. Physical activity for osteoarthritis: Efficiency and review of recommandations. Jt. Bone Spine 2021, 88, 105207. [Google Scholar] [CrossRef] [PubMed]
- Jevsevar, D.S.; Brown, G.A.; Jones, D.L.; Matzkin, E.G.; Manner, P.A.; Mooar, P.; Schousboe, J.T.; Stovitz, S.; Sanders, J.O.; Bozic, K.J.; et al. The American Academy of Orthopaedic Surgeons Evidence-Based Guideline on: Treatment of Osteoarthritis of the Knee, 2nd Edition. JBJS 2013, 95, 1885–1886. [Google Scholar] [CrossRef] [PubMed]
- Quinn, R.H.; Murray, J.; Pezold, R.; Hall, Q. Management of osteoarthritis of the hip: Evidence-based clinical practice guideline. J. Am. Acad. Orthop. Surg. 2017, 26, e434–e436. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.; Vaysbrot, E.; Arden, N.; Bennell, K.; Bierma-Zeinstra, S.; Kraus, V.; Lohmander, L.S.; Abbott, J.; Bhandari, M. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarth. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geenen, R.; Overman, C.L.; Christensen, R.; Åsenlöf, P.; Capela, S.; Huisinga, K.L.; Husebø, M.E.P.; Köke, A.J.; Paskins, Z.; Pitsillidou, I.A. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Ann. Rheum. Dis. 2018, 77, 797–807. [Google Scholar] [CrossRef] [Green Version]
- Anatomical Therapeutic Chemical Classification System. Available online: https://www.whocc.no/atc_ddd_index/?code=M&showdescription=no (accessed on 10 January 2022).
- Anatomical Therapeutic Chemical Classification System. Available online: https://www.atccode.com/M02A (accessed on 10 January 2022).
- Anatomical Therapeutic Chemical Classification System. Available online: https://www.atccode.com/M02AA (accessed on 10 January 2022).
- Akram, M.; Daniyal, M.; Sultana, S.; Owais, A.; Akhtar, N.; Zahid, R.; Said, F.; Bouyahya, A.; Ponomarev, E.; Shariat, M.A. Traditional and modern management strategies for rheumatoid arthritis. Clin. Chim. Acta 2021, 512, 142–155. [Google Scholar] [CrossRef]
- Pflugbeil, S.; Böckl, K.; Pongratz, R.; Leitner, M.; Graninger, W.; Ortner, A. Drug interactions in the treatment of rheumatoid arthritis and psoriatic arthritis. Rheumatol. Int. 2020, 40, 511–521. [Google Scholar] [CrossRef] [Green Version]
- Smolen, J.; Steiner, G. Therapeutic strategies for rheumatoid arthritis. Nat. Rev. Drug Discov. 2003, 2, 473–488. [Google Scholar] [CrossRef]
- Anatomical Therapeutic Chemical Classification System. Available online: https://www.atccode.com/N02BE (accessed on 10 January 2022).
- Esh, C.J.; Chrismas, B.C.; Mauger, A.R.; Taylor, L. Pharmacological hypotheses: Is acetaminophen selective in its cyclooxygenase inhibition? Pharm. Res. Perspect. 2021, 9, e00835. [Google Scholar] [CrossRef] [PubMed]
- Sodano, F.; Lazzarato, L.; Rolando, B.; Spyrakis, F.; De Caro, C.; Magliocca, S.; Marabello, D.; Chegaev, K.; Gazzano, E.; Riganti, C. Paracetamol–Galactose Conjugate: A Novel Prodrug for an Old Analgesic Drug. Mol. Pharm. 2019, 16, 4181–4189. [Google Scholar] [CrossRef] [PubMed]
- Anatomical Therapeutic Chemical Classification System. Available online: https://www.atccode.com/N02BA (accessed on 10 January 2022).
- Greener, B.; Archibald, S.J.; Hodkinson, M. Hydrogen bonding interactions in amorphous salicyl salicylate. Angew. Chem. Int. Ed. 2000, 39, 3601–3604. [Google Scholar] [CrossRef]
- WebMD Health Corp. Available online: https://www.webmd.com/drugs/2/drug-8704/salsalate-oral/details (accessed on 10 January 2022).
- Drug Index A to, Z. Available online: https://www.drugs.com/mtm/salsalate.html (accessed on 10 January 2022).
- Singleton, P., Jr. Salsalate: Its role in the management of rheumatic disease. Clin. Ther. 1980, 3, 80–102. [Google Scholar] [PubMed]
- Mohandoss, S.; Edison, T.N.J.I.; Atchudan, R.; Palanisamy, S.; Prabhu, N.M.; Napoleon, A.A.; You, S.; Lee, Y.R. Ultrasonic-assisted efficient synthesis of inclusion complexes of salsalate drug and β-cyclodextrin derivatives for potent biomedical applications. J. Mol. Liq. 2020, 319, 114358. [Google Scholar] [CrossRef]
- Yoo, C.-G.; Lee, S.; Lee, C.-T.; Kim, Y.W.; Han, S.K.; Shim, Y.-S. Effect of acetylsalicylic acid on endogenous IκB kinase activity in lung epithelial cells. Am. J. Physiol. Lung C 2001, 280, L3–L9. [Google Scholar] [CrossRef] [PubMed]
- Yeasmin, F.; Choi, H.W. Natural Salicylates and Their Roles in Human Health. IJMS 2020, 21, 9049. [Google Scholar] [CrossRef]
- Amann, R.; Peskar, B.A. Anti-Inflammatory effects of aspirin and sodium salicylate. Eur. J. Pharmacol. 2002, 447, 1–9. [Google Scholar] [CrossRef]
- Honvo, G.; Reginster, J.-Y.; Rabenda, V.; Geerinck, A.; Mkinsi, O.; Charles, A.; Rizzoli, R.; Cooper, C.; Avouac, B.; Bruyère, O. Safety of symptomatic slow-acting drugs for osteoarthritis: Outcomes of a systematic review and meta-analysis. Drugs Aging 2019, 36, 65–99. [Google Scholar] [CrossRef] [Green Version]
- Patrono, C.; Patrignani, P.; Rodríguez, L.A.G. Cyclooxygenase-Selective inhibition of prostanoid formation: Transducing biochemical selectivity into clinical read-outs. J. Clin. Investig. 2001, 108, 7–13. [Google Scholar] [CrossRef]
- Puljak, L.; Marin, A.; Vrdoljak, D.; Markotic, F.; Utrobicic, A.; Tugwell, P. Celecoxib for osteoarthritis. Cochrane Database Syst. Rev. 2017, 5, CD009865. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, B.R.; Pereira, T.V.; Saadat, P.; Rudnicki, M.; Iskander, S.M.; Bodmer, N.S.; Bobos, P.; Gao, L.; Kiyomoto, H.D.; Montezuma, T. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and hip osteoarthritis: Network meta-analysis. BMJ 2021, 375, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Revel, F.B.; Fayet, M.; Hagen, M. Topical diclofenac, an efficacious treatment for osteoarthritis: A narrative review. Rheumatol. Ther. 2020, 7, 217–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Anatomical Therapeutic Chemical Classification System. Available online: https://www.whocc.no/atc_ddd_index/?code=M01AC&showdescription=no (accessed on 10 January 2022).
- Csifo, E.; Nagy, E.E.; Horvath, E.; Farr, A.; Muntean, D.-L. Mid-Term effects of meloxicam on collagen type II degradation in a rat osteoarthritis model induced by iodoacetate. Farmacia 2015, 63, 556–560. [Google Scholar]
- Wen, Z.-H.; Tang, C.-C.; Chang, Y.-C.; Huang, S.-Y.; Chen, C.-H.; Wu, S.-C.; Hsieh, S.-P.; Hsieh, C.-S.; Wang, K.-Y.; Lin, S.-Y. Intra-Articular injection of the selective cyclooxygenase-2 inhibitor meloxicam (Mobic) reduces experimental osteoarthritis and nociception in rats. Osteoarthr. Cartil. 2013, 21, 1976–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, R.; Hochberg, M.; Gibofsky, A.; Jaros, M.; Young, C. Efficacy and safety of low-dose SoluMatrix meloxicam in the treatment of osteoarthritis pain: A 12-week, phase 3 study. Curr. Med. Res. Opin. 2015, 31, 2331–2343. [Google Scholar] [CrossRef] [Green Version]
- Anatomical Therapeutic Chemical Classification System. Available online: https://www.atccode.com/N02 (accessed on 10 January 2022).
- Steinmeyer, J.; Bock, F.; Stöve, J.; Jerosch, J.; Flechtenmacher, J. Pharmacological treatment of knee osteoarthritis: Special considerations of the new German guideline. Orthop. Rev. 2018, 10, 147–152. [Google Scholar] [CrossRef]
- Hermann, W.; Lambova, S.; Muller-Ladner, U. Current treatment options for osteoarthritis. Curr. Rheumatol. Rev. 2018, 14, 108–116. [Google Scholar] [CrossRef]
- Alcaraz, M.J.; Guillén, M.I.; Ferrándiz, M.L. Emerging therapeutic agents in osteoarthritis. Biochem. Pharmacol. 2019, 165, 4–16. [Google Scholar] [CrossRef]
- Ghouri, A.; Conaghan, P.G. Prospects for therapies in osteoarthritis. Calcif. Tissue Int. 2021, 109, 339–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckstein, F.; Hochberg, M.C.; Guehring, H.; Moreau, F.; Ona, V.; Bihlet, A.R.; Byrjalsen, I.; Andersen, J.R.; Daelken, B.; Guenther, O. Long-Term structural and symptomatic effects of intra-articular sprifermin in patients with knee osteoarthritis: 5-year results from the FORWARD study. Ann. Rheum. Dis. 2021, 80, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Oo, W.M.; Little, C.; Duong, V.; Hunter, D.J. The development of disease-modifying therapies for osteoarthritis (DMOADs): The evidence to date. Drug Des. Dev. Ther. 2021, 15, 2921–2945. [Google Scholar] [CrossRef] [PubMed]
- Almezgagi, M.; Zhang, Y.; Hezam, K.; Shamsan, E.; Gamah, M.; Al-Shaebi, F.; Abbas, A.; Shoaib, M.; Saif, B.; Han, Y.; et al. Diacerein: Recent insight into pharmacological activities and molecular pathways. Biomed. Pharmacother. 2020, 131, 110594. [Google Scholar] [CrossRef] [PubMed]
- Zúñiga-Romero, A.; Ponce-Chávez, M.K.; Gauthereau-Torres, M.Y.; Ortega-Varela, L.F. Combination of diacerhein and antiepileptic drugs after local peripheral, and oral administration in the rat formalin test. Drug Develop. Res. 2014, 75, 510–520. [Google Scholar] [CrossRef]
- Gadotti, V.M.; Martins, D.F.; Pinto, H.F.; Oliveira, G.; Kaster, M.P.; Quintão, N.L.M.; Santos, A.R.S. Diacerein decreases visceral pain through inhibition of glutamatergic neurotransmission and cytokine signaling in mice. Pharmacol. Biochem. Behav. 2012, 102, 549–554. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, M.D.; Cidral-Filho, F.J.; Winkelmann-Duarte, E.C.; Cargnin-Ferreira, E.; Calixto, J.B.; Dutra, R.C.; Santos, A.R.S. Diacerein reduces joint damage, pain behavior and inhibits transient receptor potential vanilloid 1, matrix metalloproteinase and glial cells in rat spinal cord. Int. J. Rheum. Dis. 2017, 20, 1337–1349. [Google Scholar] [CrossRef]
- Zhang, Q.; Cao, D.-L.; Zhang, Z.-J.; Jiang, B.-C.; Gao, Y.-J. Chemokine CXCL13 mediates orofacial neuropathic pain via CXCR5/ERK pathway in the trigeminal ganglion of mice. J. Neuroinflamm. 2016, 13, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Petrosino, S.; Ahmad, A.; Marcolongo, G.; Esposito, E.; Allarà, M.; Verde, R.; Cuzzocrea, S.; Di Marzo, V. Diacerein is a potent and selective inhibitor of palmitoylethanolamide inactivation with analgesic activity in a rat model of acute inflammatory pain. Pharm. Res. 2015, 91, 9–14. [Google Scholar] [CrossRef]
- Chen, Y.; Sun, H.; Yao, X.; Yu, Y.; Tian, T.; Xu, W.; Zhou, Y.; Ouyang, H. Pharmaceutical therapeutics for articular regeneration and restoration: State-of-the-Art technology for screening small molecular drugs. Cell. Mol. Life Sci. 2021, 78, 8127–8155. [Google Scholar] [CrossRef]
- Hu, Y.; Gui, Z.; Zhou, Y.; Xia, L.; Lin, K.; Xu, Y. Quercetin alleviates rat osteoarthritis by inhibiting inflammation and apoptosis of chondrocytes, modulating synovial macrophages polarization to M2 macrophages. Free Radic. Biol. Med. 2019, 145, 146–160. [Google Scholar] [CrossRef] [PubMed]
- Kestler, H.A.; Kühl, M. Generating a Wnt switch: It’s all about the right dosage. J. Cell Biol. 2011, 193, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Novicky, A.; Caetano-Silva, S.P.; Javaheri, B.; Pitsillides, A.A. The Mechanics of Skeletal Development. In Developmental Biology and Musculoskeletal Tissue Engineering; Academic Press: Cambridge, MA, USA, 2018; pp. 25–51. [Google Scholar] [CrossRef]
- Coryell, P.R.; Diekman, B.O.; Loeser, R.F. Mechanisms and therapeutic implications of cellular senescence in osteoarthritis. Nat. Rev. Rheumatol. 2021, 17, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Cherifi, C.; Monteagudo, S.; Lories, R.J. Promising targets for therapy of osteoarthritis: A review on the Wnt and TGF-β signalling pathways. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211006959. [Google Scholar] [CrossRef]
- Lee, B.; Parvizi, J.; Bramlet, D.; Romness, D.W.; Guermazi, A.; Noh, M.; Sodhi, N.; Khlopas, A.; Mont, M.A. Results of a phase II study to determine the efficacy and safety of genetically engineered allogeneic human chondrocytes expressing TGF-β1. J. Knee Surg. 2020, 33, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Webber, H.C.; Bermudez, J.Y.; Sethi, A.; Clark, A.F.; Mao, W. Crosstalk between TGFβ and Wnt signaling pathways in the human trabecular meshwork. Exp. Eye Res. 2016, 148, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Guehring, H.; Moreau, F.; Daelken, B.; Ladel, C.; Guenther, O.; Bihlet, A.R.; Wirth, W.; Eckstein, F.; Hochberg, M.; Conaghan, P.G. The Effects of sprifermin on symptoms and structure in a subgroup at risk of progression in the FORWARD knee osteoarthritis trial. Semin. Arthrittis Rheum. 2021, 51, 450–456. [Google Scholar] [CrossRef]
- Yazici, Y.; McAlindon, T.E.; Gibofsky, A.; Lane, N.E.; Clauw, D.; Jones, M.; Bergfeld, J.; Swearingen, C.J.; DiFrancesco, A.; Simsek, I. Lorecivivint, a Novel Intraarticular CDC-like Kinase 2 and Dual-Specificity Tyrosine Phosphorylation-Regulated Kinase 1A Inhibitor and Wnt Pathway Modulator for the Treatment of Knee Osteoarthritis: A Phase II Randomized Trial. Arthritis Rheumatol. 2020, 72, 1694–1706. [Google Scholar] [CrossRef]
- Sabha, M.; Siaton, B.C.; Hochberg, M.C. Lorecivivint, an intra-articular potential disease-modifying osteoarthritis drug. Expert Opin. Investig. Drug. 2020, 29, 1339–1346. [Google Scholar] [CrossRef]
- Chevalier, X.; Conrozier, T.; Richette, P. Desperately looking for the right target in osteoarthritis: The anti-IL-1 strategy. Arthritis Res. Ther. 2011, 13, 124. [Google Scholar] [CrossRef] [Green Version]
- Kloppenburg, M.; Peterfy, C.; Haugen, I.K.; Kroon, F.; Chen, S.; Wang, L.; Liu, W.; Levy, G.; Fleischmann, R.M.; Berenbaum, F. Phase IIa, placebo-controlled, randomised study of lutikizumab, an anti-interleukin-1α and anti-interleukin-1β dual variable domain immunoglobulin, in patients with erosive hand osteoarthritis. Ann. Rheum. Dis. 2019, 78, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, R.M.; Bliddal, H.; Blanco, F.J.; Schnitzer, T.J.; Peterfy, C.; Chen, S.; Wang, L.; Feng, S.; Conaghan, P.G.; Berenbaum, F. A Phase II Trial of Lutikizumab, an Anti–Interleukin-1α/β Dual Variable Domain Immunoglobulin, in Knee Osteoarthritis Patients with Synovitis. Arthrit. Rheumatol. 2019, 71, 1056–1069. [Google Scholar] [CrossRef] [PubMed]
- Richette, P.; Latourte, A.; Sellam, J.; Wendling, D.; Piperno, M.; Goupille, P.; Pers, Y.-M.; Eymard, F.; Ottaviani, S.; Ornetti, P. Efficacy of tocilizumab in patients with hand osteoarthritis: Double blind, randomised, placebo-controlled, multicentre trial. Ann. Rheum. Dis. 2021, 80, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, X.; Goupille, P.; Beaulieu, A.; Burch, F.; Bensen, W.; Conrozier, T.; Loeuille, D.; Kivitz, A.J.; Silver, D.; Appleton, B. Intraarticular injection of anakinra in osteoarthritis of the knee: A multicenter, randomized, double-blind, placebo-controlled study. Arthrit. Care Res. 2009, 61, 344–352. [Google Scholar] [CrossRef]
- Aitken, D.; Laslett, L.L.; Pan, F.; Haugen, I.K.; Otahal, P.; Bellamy, N.; Bird, P.; Jones, G. A randomised double-blind placebo-controlled crossover trial of HUMira (adalimumab) for erosive hand OsteoaRthritis–the HUMOR trial. Osteoarthr. Cartil. 2018, 26, 880–887. [Google Scholar] [CrossRef] [Green Version]
- Kloppenburg, M.; Ramonda, R.; Bobacz, K.; Kwok, W.-Y.; Elewaut, D.; Huizinga, T.W.; Kroon, F.P.; Punzi, L.; Smolen, J.S.; Vander Cruyssen, B. Etanercept in patients with inflammatory hand osteoarthritis (EHOA): A multicentre, randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2018, 77, 1757–1764. [Google Scholar] [CrossRef]
- Oo, W.M.; Hunter, D.J. Disease modification in osteoarthritis: Are we there yet? Clin. Exp. Rheumatol. 2019, 37 (Suppl. 120), 135–140. [Google Scholar]
- Hunter, D.J. Pharmacologic therapy for osteoarthritis—The era of disease modification. Nat. Rev. Rheumatol. 2011, 7, 13–22. [Google Scholar] [CrossRef]
- Zegels, B.; Crozes, P.; Uebelhart, D.; Bruyère, O.; Reginster, J.-Y. Equivalence of a single dose (1200 mg) compared to a three-time a day dose (400 mg) of chondroitin 4&6 sulfate in patients with knee osteoarthritis. Results of a randomized double blind placebo controlled study. Osteoarthr. Cartil. 2013, 21, 22–27. [Google Scholar]
- Roman-Blas, J.A.; Castañeda, S.; Sánchez-Pernaute, O.; Largo, R.; Herrero-Beaumont, G.; CS/GS Combined Therapy Study Group; Blanco, F.J.; Gómez, R.B.; Burlato, M.C.; González, C.G. Combined treatment with chondroitin sulfate and glucosamine sulfate shows no superiority over placebo for reduction of joint pain and functional impairment in patients with knee osteoarthritis: A six-month multicenter, randomized, double-blind, placebo-controlled clinical trial. Arthritis Rheumatol. 2017, 69, 77–85. [Google Scholar]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.; Arden, N.; Berenbaum, F.; Bierma-Zeinstra, S.; Hawker, G.; Henrotin, Y.; Hunter, D.; Kawaguchi, H. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godwin, M.; Dawes, M. Intra-Articular steroid injections for painful knees. Systematic review with meta-analysis. Can. Fam. Physician 2004, 50, 241–248. [Google Scholar] [PubMed]
- Arroll, B.; Goodyear-Smith, F. Corticosteroid injections for osteoarthritis of the knee: Meta-Analysis. BJM 2004, 328, 869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellamy, N.; Campbell, J.; Welch, V.; Gee, T.L.; Bourne, R.; Wells, G.A. Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst. Rev. 2006, 2, CD005321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creamer, P. Intra-Articular corticosteroid treatment in osteoarthritis. Curr. Opin. Orthop. 2000, 11, 66–70. [Google Scholar] [CrossRef]
- Habib, G.S. Systemic effects of intra-articular corticosteroids. Clin. Rheumatol. 2009, 28, 749–756. [Google Scholar] [CrossRef]
- Habib, G.; Bashir, M.; Jabbour, A. Increased blood glucose levels following intra-articular injection of methylprednisolone acetate in patients with controlled diabetes and symptomatic osteoarthritis of the knee. Ann. Rheum. Dis. 2008, 67, 1790–1791. [Google Scholar] [CrossRef]
- Nakazawa, F.; Matsuno, H.; Yudoh, K.; Watanabe, Y.; Katayama, R.; Kimura, T. Corticosteroid treatment induces chondrocyte apoptosis in an experimental arthritis model and in chondrocyte cultures. Clin. Exp. Rheumatol. 2002, 20, 773–782. [Google Scholar]
- Wernecke, C.; Braun, H.J.; Dragoo, J.L. The effect of intra-articular corticosteroids on articular cartilage: A systematic review. Orthop. J. Sports Med. 2015, 3, 2325967115581163. [Google Scholar] [CrossRef]
- Roecker, Z.; Quinlan, N.D.; Browne, J.A.; Werner, B.C. Risk of Periprosthetic infection following intra-articular corticosteroid injections after total knee arthroplasty. J. Arthroplast. 2020, 35, 1090–1094. [Google Scholar] [CrossRef]
- Marsland, D.; Mumith, A.; Barlow, I.W. Systematic review: The safety of intra-articular corticosteroid injection prior to total knee arthroplasty. Knee 2014, 21, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Bedard, N.A.; Pugely, A.J.; Elkins, J.M.; Duchman, K.R.; Westermann, R.W.; Liu, S.S.; Gao, Y.; Callaghan, J.J. The John N. Insall Award: Do intraarticular injections increase the risk of infection after TKA? Clin. Orthop. Relat. R. 2017, 475, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancienne, J.M.; Werner, B.C.; Luetkemeyer, L.M.; Browne, J.A. Does timing of previous intra-articular steroid injection affect the post-operative rate of infection in total knee arthroplasty? J. Arthroplast. 2015, 30, 1879–1882. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.J.; Hart, J.A.; Miller, M.D.; Altman, R.D.; Rosen, J.E. Hyaluronic acid viscosupplementation and osteoarthritis: Current uses and future directions. Am. J. Sports Med. 2009, 37, 1636–1644. [Google Scholar] [CrossRef]
- Wang, C.-T.; Lin, J.; Chang, C.-J.; Lin, Y.-T.; Hou, S.-M. Therapeutic effects of hyaluronic acid on osteoarthritis of the knee: A meta-analysis of randomized controlled trials. JBJS 2004, 86, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Hunter, D.J. Viscosupplementation for osteoarthritis of the knee. N. Engl. J. Med. 2015, 372, 10401047. [Google Scholar] [CrossRef]
- Marx, R.E. Platelet-Rich plasma (PRP): What is PRP and what is not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [Green Version]
- Gato-Calvo, L.; Magalhaes, J.; Ruiz-Romero, C.; Blanco, F.J.; Burguera, E.F. Platelet-Rich plasma in osteoarthritis treatment: Review of current evidence. Ther. Adv. Chronic. Dis. 2019, 10, 2040622319825567. [Google Scholar] [CrossRef] [Green Version]
- Lichtenfels, M.; Colomé, L.; Sebben, A.D.; Braga-Silva, J. Effect of platelet rich plasma and platelet rich fibrin on sciatic nerve regeneration in a rat model. Microsurgery 2013, 33, 383–390. [Google Scholar] [CrossRef]
- Eppley, B.L.; Pietrzak, W.S.; Blanton, M. Platelet-rich plasma: A review of biology and applications in plastic surgery. Plast. Reconst. Surg. 2006, 118, 147e–159e. [Google Scholar] [CrossRef] [Green Version]
- Mościcka, P.; Przylipiak, A. History of autologous platelet-rich plasma: A short review. J. Cosmet. Dermatol. 2021, 20, 2712–2714. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Aguirre, J.J.; Algorta, J.; Ayerdi, E.; Cabezas, A.I.; Orive, G.; Andia, I. Effectiveness of autologous preparation rich in growth factors for the treatment of chronic cutaneous ulcers. J. Biomed. Mater. Res. Part B Appl. Biomater. 2008, 84, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E. Plasma rich in growth factors: Preliminary results of use in the preparation of future sites for implants. Int. J. Oral Maxillofac. Implant. 1999, 14, 529–535. [Google Scholar]
- Filardo, G.; Previtali, D.; Napoli, F.; Candrian, C.; Zaffagnini, S.; Grassi, A. PRP injections for the treatment of knee osteoarthritis: A meta-analysis of randomized controlled trials. Cartilage 2021, 13 (Suppl. 1), 364S–375S. [Google Scholar] [CrossRef]
- Ahmad, H.S.; Farrag, S.E.; Okasha, A.E.; Kadry, A.O.; Ata, T.B.; Monir, A.A.; Shady, I. Clinical outcomes are associated with changes in ultrasonographic structural appearance after platelet-rich plasma treatment for knee osteoarthritis. Int. J. Rheum. Dis. 2018, 21, 960–966. [Google Scholar] [CrossRef]
- Hu, K.; Olsen, B.R.; Schmalz, G. Vascular Endothelial Growth Factor Control Mechanisms in Skeletal Growth and Repair. Dev. Dynam. 2017, 246, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Raeissadat, S.A.; Babaee, M.; Rayegani, S.M.; Hashemi, Z.; Hamidieh, A.A.; Mojgani, P.; Vanda, H.F. An overview of platelet products (PRP, PRGF, PRF, etc.) in the Iranian studies. Future Sci. OA 2017, 3, FSO231. [Google Scholar] [CrossRef] [Green Version]
- Roskoski, R., Jr. The role of small molecule platelet-derived growth factor receptor (PDGFR) inhibitors in the treatment of neoplastic disorders. Pharm. Res. 2018, 129, 65–83. [Google Scholar] [CrossRef]
- Van Der Kraan, P.M. The changing role of TGFβ in healthy, ageing and osteoarthritic joints. Nat. Rev. Rheumatol. 2017, 13, 155. [Google Scholar] [CrossRef]
- Nagao, M.; Hamilton, J.L.; Kc, R.; Berendsen, A.D.; Duan, X.; Cheong, C.W.; Li, X.; Im, H.-J.; Olsen, B.R. Vascular endothelial growth factor in cartilage development and osteoarthritis. Sci. Rep. UK 2017, 7, 1–16. [Google Scholar] [CrossRef]
- Zeng, F.; Harris, R.C. Epidermal growth factor, from gene organization to bedside. Semin. Cell Dev. Biol. 2014, 28, 2–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, L.F.; Stessuk, T.; Camargo, I.C.C.; Sabeh, N., Jr.; Santos, L.D.; Ribeiro-Paes, J.T. Platelet-Rich plasma (PRP): Methodological aspects and clinical applications. Platelets 2015, 26, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Yakar, S.; Werner, H.; Rosen, C.J. 40 YEARS OF IGF1: Insulin-Like growth factors: Actions on the skeleton. J. Mol. Endocrinol. 2018, 61, T115–T137. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Sakai, K.; Nakamura, T.; Matsumoto, K. Hepatocyte growth factor twenty years on: Much more than a growth factor. J. Gastroenterol. Hepatol. 2011, 26, 188–202. [Google Scholar] [CrossRef] [Green Version]
- Imamura, R.; Matsumoto, K. Hepatocyte growth factor in physiology and infectious diseases. Cytokine 2017, 98, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Jun, J.-I.; Lau, L.F. Taking aim at the extracellular matrix: CCN proteins as emerging therapeutic targets. Nat. Rev. Drug Discov. 2011, 10, 945–963. [Google Scholar] [CrossRef] [Green Version]
- Sampath, T.K.; Reddi, A.H. Discovery of Bone Morphogenetic Proteins—A Historical Perspective. Bone 2020, 140, 115548. [Google Scholar] [CrossRef]
- Gautschi, O.P.; Frey, S.P.; Zellweger, R. Bone morphogenetic proteins in clinical applications. ANZ J. Surg. 2007, 77, 626–631. [Google Scholar] [CrossRef]
- Bowen-Pope, D.F.; Raines, E.W. History of discovery: Platelet-Derived growth factor. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 2397–2401. [Google Scholar] [CrossRef] [Green Version]
- Betsholtz, C. Biology of platelet-derived growth factors in development. Birth Defects Res. Part C Embryo Today Rev. 2003, 69, 272–285. [Google Scholar] [CrossRef]
- Werner, S.; Grose, R. Regulation of wound healing by growth factors and cytokines. Physiol. Rev. 2003, 83, 835–870. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Wang, X.; Jiang, W.; Zhu, Y.; Hu, Y.; Zhao, Y.; Song, X.; Zhao, J.; Zhang, W.; Peng, J.; et al. Platelet-Rich Plasma Therapy in the Treatment of Diseases Associated with Orthopedic Injuries. Tissue Eng. Part A 2020, 26, 571–585. [Google Scholar] [CrossRef] [PubMed]
- Peter, I.; Wu, K.; Diaz, R.; Borg-Stein, J. Platelet-Rich plasma. Phys. Med. Rehabil. Clin. 2016, 27, 825–853. [Google Scholar]
- Yang, J.; Zhou, M.; Li, W.; Lin, F.; Shan, G. Preparation and Evaluation of Sustained Release Platelet-Rich Plasma-Loaded Gelatin Microspheres Using an Emulsion Method. ACS Omega 2020, 5, 27113–27118. [Google Scholar] [CrossRef]
- d’Hauterive, S.P.; Charlet-Renard, C.; Dubois, M.; Berndt, S.; Goffin, F.; Foidart, J.-M.; Geenen, V. Human endometrial leukemia inhibitory factor and interleukin-6: Control of secretion by transforming growth factor-β-related members. Neuroimmunomodulation 2005, 12, 157–163. [Google Scholar] [CrossRef]
- Szwedowski, D.; Szczepanek, J.; Paczesny, Ł.; Zabrzyński, J.; Gagat, M.; Mobasheri, A.; Jeka, S. The Effect of Platelet-Rich Plasma on the Intra-Articular Microenvironment in Knee Osteoarthritis. IJMS 2021, 22, 5492. [Google Scholar] [CrossRef]
- YiKim, I.; Kim, M.M.; Kim, S.-J. Transforming growth factor-β: Biology and clinical relevance. BMB Rep. 2005, 38, 1–8. [Google Scholar] [CrossRef]
- Murata, M.; Yudoh, K.; Masuko, K. The potential role of vascular endothelial growth factor (VEGF) in cartilage: How the angiogenic factor could be involved in the pathogenesis of osteoarthritis? Osteoarthr. Cartil. 2008, 16, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Hu, K.; Olsen, B.R. The roles of vascular endothelial growth factor in bone repair and regeneration. Bone 2016, 91, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Melincovici, C.S.; Boşca, A.B.; Şuşman, S.; Mărginean, M.; Mihu, C.; Istrate, M.; Moldovan, I.M.; Roman, A.L.; Mihu, C.M. Vascular endothelial growth factor (VEGF)—Key factor in normal and pathological angiogenesis. Rom. J. Morphol. Embryol. 2018, 59, 3950. [Google Scholar]
- Noguchi, T.; Kitaura, H.; Marahleh, A.; Ohori, F.; Nara, Y.; Pramusita, A.; Kinjo, R.; Ma, J.; Kanou, K.; Mizoguchi, I. Tumor necrosis factor-α enhances the expression of vascular endothelial growth factor in a mouse orthodontic tooth movement model. J. Den. Sci. 2021, 17, 415–420. [Google Scholar] [CrossRef]
- Da Silva Santos, E.; Nogueira, K.A.B.; Fernandes, L.C.C.; Martins, J.R.P.; Reis, A.V.F.; Neto, J.d.B.V.; da Silva, I., Jr.; Pessoa, C.; Petrilli, R.; Eloy, J.O. EGFR targeting for cancer therapy: Pharmacology and immunoconjugates with drugs and nanoparticles. Int. J. Pharm. 2020, 592, 120082. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Kot, A.; Lay, Y.A.E.; Fierro, F.A.; Chen, H.; Lane, N.E.; Yao, W. Acceleration of fracture healing by overexpression of basic fibroblast growth factor in the mesenchymal stromal cells. Stem Cell. Transl. Med. 2017, 6, 1880–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piszczorowicz, Ł.; Król, D.; Dyląg, S. Autologous platelet-rich plasma therapy—A promising method for tissue repair//regeneration in many medical fields. J. Transfus. Med. 2020, 13, 135–148. [Google Scholar] [CrossRef]
- Yakar, S.; Isaksson, O. Regulation of skeletal growth and mineral acquisition by the GH/IGF-1 axis: Lessons from mouse models. Growth Horm. IGF Res. 2016, 28, 26–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Zheng, Y.; Bai, J.; Shi, C.; Shi, X.; Shan, H.; Zhou, X. Hepatocyte growth factor overexpression promotes osteoclastogenesis and exacerbates bone loss in CIA mice. J. Orthop. Transl. 2021, 27, 9–16. [Google Scholar] [CrossRef]
- Yoneda, T.; Hiasa, M.; Okui, T.; Hata, K. Sensory nerves: A driver of the vicious cycle in bone metastasis? J. Bone Oncol. 2021, 30, 100387. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, N.; Zhang, Z.; Zhang, G.; Zhang, B. Connective tissue growth factor: From molecular understandings to drug discovery. Front. Cell Dev. Biol. 2020, 8, 1239. [Google Scholar] [CrossRef]
- Takigawa, M. CCN2: A master regulator of the genesis of bone and cartilage. J. Cell Commun. Signal. 2013, 7, 191–201. [Google Scholar] [CrossRef] [Green Version]
- Nishida, T.; Kubota, S.; Kojima, S.; Kuboki, T.; Nakao, K.; Kushibiki, T.; Tabata, Y.; Takigawa, M. Regeneration of defects in articular cartilage in rat knee joints by CCN2 (connective tissue growth factor). J. Bone Min. Res. 2004, 19, 1308–1319. [Google Scholar] [CrossRef]
- Katagiri, T.; Watabe, T. Bone morphogenetic proteins. Cold Spring Harb. Perspect. Biol. 2016, 8, a021899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, A.; Pelletier, M.H.; Yu, Y.; Walsh, W.R. Can platelet-rich plasma (PRP) improve bone healing? A comparison between the theory and experimental outcomes. Arch. Orthop. Traum. Su. 2013, 133, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Lima, F.S.; Stewart, J.L.; Canisso, I.F. Insights into nerve growth factor-β role in bovine reproduction-Review. Theriogenology 2020, 150, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Zabrzyński, J.; Zabrzyńska, A.; Grzanka, D. Tendon—Function-related structure, simple healing process and mysterious ageing. Folia Morphol. 2018, 77, 416–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szwedowski, D.; Jaworski, Ł.; Szwedowska, W.; Pękala, P.; Gagat, M. Neovascularization in Meniscus and Tendon Pathology as a Potential Mechanism in Regenerative Therapies: Special Reference to Platelet-Rich Plasma Treatment. Appl. Sci. 2021, 11, 8310. [Google Scholar] [CrossRef]
- Tol, J.L.; Spiezia, F.; Maffulli, N. Neovascularization in Achilles tendinopathy: Have we been chasing a red herring? Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1891–1894. [Google Scholar] [CrossRef] [Green Version]
- Stenken, J.A.; Poschenrieder, A.J. Bioanalytical chemistry of cytokines—A review. Anal. Chim. Act. 2015, 853, 95–115. [Google Scholar] [CrossRef]
- Akdis, M.; Burgler, S.; Crameri, R.; Eiwegger, T.; Fujita, H.; Gomez, E.; Klunker, S.; Meyer, N.; O’Mahony, L.; Palomares, O. Interleukins, from 1 to 37, and interferon-γ: Receptors, functions, and roles in diseases. J. Allergy Clin. Iimmunol. 2011, 127, 701–721.e70. [Google Scholar] [CrossRef]
- Cai, X.; Yuan, S.; Zeng, Y.; Wang, C.; Yu, N.; Ding, C. New Trends in Pharmacological Treatments for Osteoarthritis. Front. Pharmacol. 2021, 12, 701. [Google Scholar] [CrossRef]
- Vaillant, A.A.J.; Qurie, A. Interleukin. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Muñoz, J.; Akhavan, N.S.; Mullins, A.P.; Arjmandi, B.H. Macrophage polarization and osteoporosis: A review. Nutrients 2020, 12, 2999. [Google Scholar] [CrossRef]
- Pajarinen, J.; Lin, T.; Nabeshima, A.; Sato, T.; Gibon, E.; Jämsen, E.; Khan, T.N.; Yao, Z.; Goodman, S.B. Interleukin-4 repairs wear particle induced osteolysis by modulating macrophage polarization and bone turnover. J. Biomed. Mater. Res. A 2021, 109, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.-W.; Ren, B.; Wang, H.-W.; Zhang, X.; Yu, M.-Z.; Cheng, L.; Sang, Y.-H.; Cao, S.-S.; Thieringer, F.M.; Zhang, D. 3D-printed titanium implant combined with interleukin 4 regulates ordered macrophage polarization to promote bone regeneration and angiogenesis. Bone Jt. Res. 2021, 10, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Ross, E.A.; Devitt, A.; Johnson, J.R. Macrophages: The Good, the Bad, and the Gluttony. Front. Immunol. 2021, 12, 3234. [Google Scholar] [CrossRef] [PubMed]
- Karsenty, G.; Mera, P. Molecular bases of the crosstalk between bone and muscle. Bone 2018, 115, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Harmer, D.; Falank, C.; Reagan, M.R. Interleukin-6 interweaves the bone marrow microenvironment, bone loss, and multiple myeloma. Front. Endocrinol. 2019, 9, 788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggiolini, M.; Loetscher, P.; Moser, B. Interleukin-8 and the chemokine family. Int. J. Immunopharmacol. 1995, 17, 103–108. [Google Scholar] [CrossRef]
- Haga, Y.; Kanda, T.; Nakamoto, S.; Nakamura, M.; Sasaki, R.; Wu, S.; Yokosuka, O. Interferon induces interleukin 8 and bone marrow stromal cell antigen 2 expression, inhibiting the production of hepatitis B virus surface antigen from human hepatocytes. Biochem. Biophys. Res. Commun. 2017, 486, 858–863. [Google Scholar] [CrossRef]
- Cassano, J.M.; Kennedy, J.G.; Ross, K.A.; Fraser, E.J.; Goodale, M.B.; Fortier, L.A. Bone marrow concentrate and platelet-rich plasma differ in cell distribution and interleukin 1 receptor antagonist protein concentration. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 333–342. [Google Scholar] [CrossRef]
- Coniglio, S.J. Role of tumor-derived chemokines in osteolytic bone metastasis. Front. Endocrinol. 2018, 9, 313. [Google Scholar] [CrossRef]
- Verma, S.K.; Garikipati, V.N.; Krishnamurthy, P.; Schumacher, S.M.; Grisanti, L.A.; Cimini, M.; Cheng, Z.; Khan, M.; Yue, Y.; Benedict, C. Interleukin-10 inhibits bone marrow fibroblast progenitor cell–mediated cardiac fibrosis in pressure-overloaded myocardium. Circulation 2017, 136, 940–953. [Google Scholar] [CrossRef] [PubMed]
- Rios-Arce, N.D.; Dagenais, A.; Feenstra, D.; Coughlin, B.; Kang, H.J.; Mohr, S.; McCabe, L.R.; Parameswaran, N. Loss of interleukin-10 exacerbates early Type-1 diabetes-induced bone loss. J. Cell. Physiol. 2020, 235, 2350–2365. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, S.; Yokote, T.; Hiraoka, N.; Akioka, T.; Nishiwaki, U.; Miyoshi, T.; Iwaki, K.; Fumimoto, A.; Masuda, Y.; Hatooka, J. Transforming growth factor β–and interleukin 13–producing mast cells are associated with fibrosis in bone marrow. Hum. Pathol. 2017, 62, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Metzger, C.E.; Narayanan, S.A. The role of osteocytes in inflammatory bone loss. Front. Endocrinol. 2019, 10, 285. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, W.; Lim, S.-M.; Xu, L.; Jin, J.-O. Interleukin-10-Producing B Cells Help Suppress Ovariectomy-Mediated Osteoporosis. Immune Netw. 2020, 20, e50. [Google Scholar] [CrossRef]
- Lei, T.; Wang, M.; Zuo, C.; Xu, H. The Application Value of Interleukin-10 and Interleukin-15 in Osteoporosis. Open Access Libr. J. 2021, 8, 1–6. [Google Scholar] [CrossRef]
- Zhu, H.; Guo, J.; Shen, Y.; Dong, W.; Gao, H.; Miao, Y.; Li, C.; Zhang, Y. Functions and mechanisms of tumor necrosis factor-α and noncoding RNAs in bone-invasive pituitary adenomas. Clin. Cancer Res. 2018, 24, 5757–5766. [Google Scholar] [CrossRef] [Green Version]
- Fischer, J.; Hans, D.; Lamy, O.; Marques-Vidal, P.; Vollenweider, P.; Aubry-Rozier, B. “Inflammaging” and bone in the OsteoLaus cohort. Immun. Ageing 2020, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Tiemessen, K.M.; Bosker, F.J.; Wardenaar, K.J.; Lie, J.; Schoevers, R.A. Interleukin, tumor necrosis factor-α and C-reactive protein profiles in melancholic and non-melancholic depression: A systematic review. J. Psychosom. Res. 2018, 111, 58–68. [Google Scholar] [CrossRef]
- Abrams, G.D.; Frank, R.M.; Fortier, L.A.; Cole, B.J. Platelet-Rich plasma for articular cartilage repair. Sports Med. Arthrosc. 2013, 21, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Lin, L.; Wang, H.; Wei, X.; Fu, X.; Zhang, J.; Yu, C. Suppression of early experimental osteoarthritis by in vivo delivery of the adenoviral vector-mediated NF-κBp65-specific siRNA. Osteoarthr. Cartil. 2008, 16, 174–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.-R.; Park, K.M.; Joung, Y.K.; Park, K.D.; Do, S.H. Platelet-Rich plasma loaded hydrogel scaffold enhances chondrogenic differentiation and maturation with up-regulation of CB1 and CB2. J. Control. Release 2012, 159, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Mifune, Y.; Matsumoto, T.; Takayama, K.; Ota, S.; Li, H.; Meszaros, L.B.; Usas, A.; Nagamune, K.; Gharaibeh, B.; Fu, F. The effect of platelet-rich plasma on the regenerative therapy of muscle derived stem cells for articular cartilage repair. Osteoarthr. Cartil. 2013, 21, 175–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhillon, M.S.; Patel, S.; Bansal, T. Improvising PRP for use in osteoarthritis knee-upcoming trends and futuristic view. J. Clin. Orthop. Trauma 2019, 10, 32–35. [Google Scholar] [CrossRef]
- Wasterlain, A.S.; Braun, H.J.; Harris, A.H.; Kim, H.-J.; Dragoo, J.L. The systemic effects of platelet-rich plasma injection. Am. J. Sports Med. 2013, 41, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Szwedowski, D.; Dallo, I.; Irlandini, E.; Gobbi, A. Osteo-Core Plasty: A Minimally Invasive Approach for Subchondral Bone Marrow Lesions of the Knee. Arthrosc. Tech. 2020, 9, e1773–e1777. [Google Scholar] [CrossRef] [PubMed]
- Sheth, U.; Simunovic, N.; Klein, G.; Fu, F.; Einhorn, T.A.; Schemitsch, E.; Ayeni, O.R.; Bhandari, M. Efficacy of autologous platelet-rich plasma use for orthopaedic indications: A meta-analysis. JBJS 2012, 94, 298–307. [Google Scholar] [CrossRef]
- Dallo, I.; Szwedowski, D.; Mobasheri, A.; Irlandini, E.; Gobbi, A. Prospective Study Comparing Leukocyte-Poor Platelet-Rich Plasma Combined with Hyaluronic Acid and Autologous Microfragmented Adipose Tissue in Patients with Early Knee Osteoarthritis. Stem Cells Dev. 2021, 30, 651–659. [Google Scholar] [CrossRef]
- Karasavvidis, T.; Totlis, T.; Gilat, R.; Cole, B.J. Platelet-Rich plasma combined with hyaluronic acid improves pain and function compared with hyaluronic acid alone in knee osteoarthritis: A systematic review and meta-analysis. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 1277–1287. [Google Scholar] [CrossRef]
- Xu, T.; Yu, X.; Yang, Q.; Liu, X.; Fang, J.; Dai, X. Autologous micro-fragmented adipose tissue as stem cell-based natural scaffold for cartilage defect repair. Cell Transplant. 2019, 28, 1709–1720. [Google Scholar] [CrossRef]
- Russo, A.; Screpis, D.; Di Donato, S.; Bonetti, S.; Piovan, G.; Zorzi, C. Autologous micro-fragmented adipose tissue for the treatment of diffuse degenerative knee osteoarthritis: An update at 3 year follow-up. J. Exp. Orthop. 2018, 5, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Growth Factors/ References | Functions |
|---|---|
| PDGF [114,132,133,134,135,136,137] | The first growth factor to be approved for the treatment of human ulcers; Plays a significant role in blood vessel formation (angiogenesis process); Enhances proliferation of fibroblasts and their effectiveness in the production of extracellular matrix; Regulates cell growth and division; Helps in tissue remodeling and cellular differentiation; Helps in mesenchymal proliferation and directs the migration and differentiation; Promotes the healing of wounds. |
| TGF-β [12,122,138,139,140] | Controls proliferation process; Plays an important role in embryonic development, cell growth, cellular differentiation, hormone secretion, and immune function; Inhibits collagen synthesis and calcium release; An inducer of extracellular matrix proteins; Contributes to the reproductive process by enhancing endometrial proimplantatory LIF (Leukemia Inhibitory Factor). |
| VEGF [119,123,141,142,143,144] | Stimulates angiogenesis and vasculogenesis; Stimulates endothelial degradation and helps in the underlying basement membrane, migration into the surrounding tissue, proliferation and tube formation; Activates the synthesis of metalloproteinase; Initiates a macrophage-related angiogenic response in the inflammation stage; Important for the recruitment of blood vessels and osteoclasts in endochondral bone repair; Required for angiogenesis-osteogenesis coupling in intramembranous bone repair; Regulates osteoclasts in the remodeling stage; Useful in the treatment of impaired bone healing/regeneration. |
| EGF [124,145] | A protein that stimulates cell growth and differentiation by binding to its receptor (EGFR); Plays a substantial part in the maintenance of spermatogenesis. |
| FGF [120,146,147] | FGF-2, FGF-7, and FGF-10—crucial for wound healing; Involved in angiogenesis, wound healing, embryonic development, and various endocrine signaling pathways; Stimulates proliferation of various cells of mesodermal, ectodermal, and also endodermal origin; Helps in the regulation of many developmental processes, including morphogenesis, differentiation, cell proliferation, and migration during embryonic development. |
| IGF [126,148] | Growth hormone and its downstream mediator IGF construct a pleiotropic axis affecting growth, metabolism, and organ function; Exerts their effects on osteogenic cells via binding to their cognate receptor, leading to activation of an array of genes that mediate cellular differentiation and function; Interacts with skeletal regulators, such as sex steroids, thyroid hormone, and parathyroid hormone, to facilitate skeletal growth and metabolism; IGFs are produced in the liver; it bears on various reproductive processes and receives an essential role in the regulation of spermatogenesis; Regulates linear and radial bone growth and modeling during development; Protects the skeleton from age-related bone loss. |
| HGF [127,149,150] | Stimulates angiogenesis; Mitogenic for hepatocytes and endothelial cells; the key factor for tissue self-repair in animal models; protect liver, kidneys, lungs, heart, brain, and gastrointestinal mucosa, due to anti-apoptotic; and anti-inflammatory properties (as demonstrated on animal models); HGF neutralization at embryonic stage leads to hypoplasia; Cytotoxic effect on some cancer cells; One of the glucose controlling factors—preventive against hyperglycemia, stimulates insulin secretion Regulated osteoclastogenesis by JNK and AKT-GSK-3β-NFATc1 signalings. |
| CTGF [151,152,153] | Plays an important role in cell adhesion, migration, proliferation, angiogenesis, skeletal development and tissue repair; Stimulates cartilage regeneration; Promotes matrix mineralization Promotes the proliferation and differentiation of growth-plate chondrocytes, osteoblasts, and vascular endothelial cells, all of which play important roles in endochondral ossification; Promotes the formation of osteoclasts in vitro, which cells play an important role in the replacement of cartilage by bone during endochondral ossification; Promotes intramembranous ossification, regenerate cartilage and bone, and induce angiogenesis in vivo. |
| BMPs [131,154,155] | At least 20 BMPs have been identified; First discovered as proteins that induce ectopic bone formation; Known to be potent osteoinductive proteins involved in many of the processes related to bone formation and regeneration; Have unique activity in the demineralized bone matrix, which induces heterotopic bone formation in nonskeletal tissues, such as skeletal muscle and subcutaneous tissue; regulating cellular lineage commitment, morphogenesis, differentiation, proliferation, and apoptosis of various types of cells throughout the body; BMP-2 and BMP-7 are approved for clinical use in open fractures of long bones, non-unions, and spinal fusion. |
| NGF [9,156] | Ubiquitous seminal plasma protein in mammals; Substance is involved in regulating neuronal survival and differentiation; Acts as a pain mediator in mature mammals; Limits the regenerative capacity of the nervous system. |
| Cytokines/Reference | Functions |
|---|---|
| IL-1 [161,162,163] | Proinflammatory cytokine and pain mediator that acts as an endogenous pyrogen; Resulting in pain sensitization, bone resorption, and cartilage destruction; Family members include IL-1α, IL-1β, and IL-1ra (endogenous IL-1 receptor antagonist); Principal targets are macrophages, large granular lymphocytes, B cells, endothelium, fibroblasts, and astrocytes secrete IL-1; Acts on the hypothalamus to induce fever (also called an endogenous pyrogen); Operates on hepatocytes to increase the synthesis of specific serum proteins, such as amyloid A protein and fibrinogen; Causes fall in blood pressure or shock in large amounts; Causes lymphocyte activation, macrophage stimulation, increased leukocyte/endothelial adhesion, fever due to hypothalamus stimulation, and release of acute-phase proteins by the liver; Causes apoptosis in many cell types and cachexia; IL-1β plays important roles in inflammation and matrix degradation and is the primary target for reducing inflammation by manipulating IL-1ra; Corticosteroids inhibit the IL-1 effect. |
| IL-4 [164,165,166,167] | Intracellular anti-inflammatory cytokines; Specific cytokine modulating osteogenic capability; Primary effects include B-cell differentiation and stimulation of acute-phase proteins; Promotes mast cell proliferation in vivo; Promotes bone regeneration by causing the polarization of macrophage phenotype towards the anti-inflammatory M2, rather than the inflammatory M1 phenotype what promotes osteogenesis; Inhibits IFN gamma-mediated activation on macrophages; Promotes change in the cytokine microenvironment result in decreased osteoclast activity and increased osteoblast activity, resulting in the repair of bone Increases bone mineralization. |
| IL-6 [21,22,168,169] | Intracellular pro-inflammatory cytokines; The central mediators of osteoclast activity; appears, in part, to mediate the bone resorption–inducing effects of TNF-a and IL-l and osteoprotegerin (OPG); B lymphocytes and hepatocytes are its principal targets; Primary effects include B-cell differentiation and stimulation of acute-phase proteins. |
| IL-8 [170,171,172,173] | Stimulation of angiogenesis; Contributed to osteoclast formation; Principal targets are neutrophils, basophils, mast cells, macrophages, and keratinocytes; Plays a major part in infertility and is involved in mitogenesis, inhibition of angiogenesis, inflammation, chemotaxis, neutrophil degranulation, leukocyte activation, and calcium homeostasis. |
| IL-10 [161,174,175] | Intracellular anti-inflammatory cytokines; Principal targets are Th1 cells; Causes inhibition of IL-2 and interferon gamma; Decreases the antigen presentation, and MHC class II expression of dendritic cells; Costimulatory molecules on macrophages; Downregulates pathogenic Th17 cell responses; Inhibits the expression of many proinflammatory cytokines, chemokines, and chemokine receptors58 and mediates allergen tolerance in allergen-specific immunotherapy and after exposure to high doses of the allergen; Inhibits IL-12 production by macrophages; Promotes survival, proliferation, and differentiation of human B cells and increases the production of IgG4. |
| IL-13 [176,177] | Intracellular anti-inflammatory cytokines; Acts on monocytes, fibroblasts, epithelial cells and B cells; Significant effects are B-cell growth and differentiation, stimulates isotype switching to IgE. Causes increased mucus production by epithelial cells, increased collagen synthesis by fibroblasts and inhibits pro-inflammatory cytokine production; Works together with IL-4 in producing biologic effects associated with allergic inflammation and in defense against parasites. |
| IP-10 [174,175,178,179] | Proinflammatory cytokine; stimulate angiogenesis; Regulating osteoblast and osteoclast functions. |
| TNF-α [180,181,182] | Intracellular anti-inflammatory cytokines; Inflammation mediator; Stimulates the growth of fibroblasts; Promotes angiogenesis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowaczyk, A.; Szwedowski, D.; Dallo, I.; Nowaczyk, J. Overview of First-Line and Second-Line Pharmacotherapies for Osteoarthritis with Special Focus on Intra-Articular Treatment. Int. J. Mol. Sci. 2022, 23, 1566. https://doi.org/10.3390/ijms23031566
Nowaczyk A, Szwedowski D, Dallo I, Nowaczyk J. Overview of First-Line and Second-Line Pharmacotherapies for Osteoarthritis with Special Focus on Intra-Articular Treatment. International Journal of Molecular Sciences. 2022; 23(3):1566. https://doi.org/10.3390/ijms23031566
Chicago/Turabian StyleNowaczyk, Alicja, Dawid Szwedowski, Ignacio Dallo, and Jacek Nowaczyk. 2022. "Overview of First-Line and Second-Line Pharmacotherapies for Osteoarthritis with Special Focus on Intra-Articular Treatment" International Journal of Molecular Sciences 23, no. 3: 1566. https://doi.org/10.3390/ijms23031566
APA StyleNowaczyk, A., Szwedowski, D., Dallo, I., & Nowaczyk, J. (2022). Overview of First-Line and Second-Line Pharmacotherapies for Osteoarthritis with Special Focus on Intra-Articular Treatment. International Journal of Molecular Sciences, 23(3), 1566. https://doi.org/10.3390/ijms23031566