
Decreased Expression of Estrogen Receptors Is Associated with Tumorigenesis in Papillary Thyroid Carcinoma

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
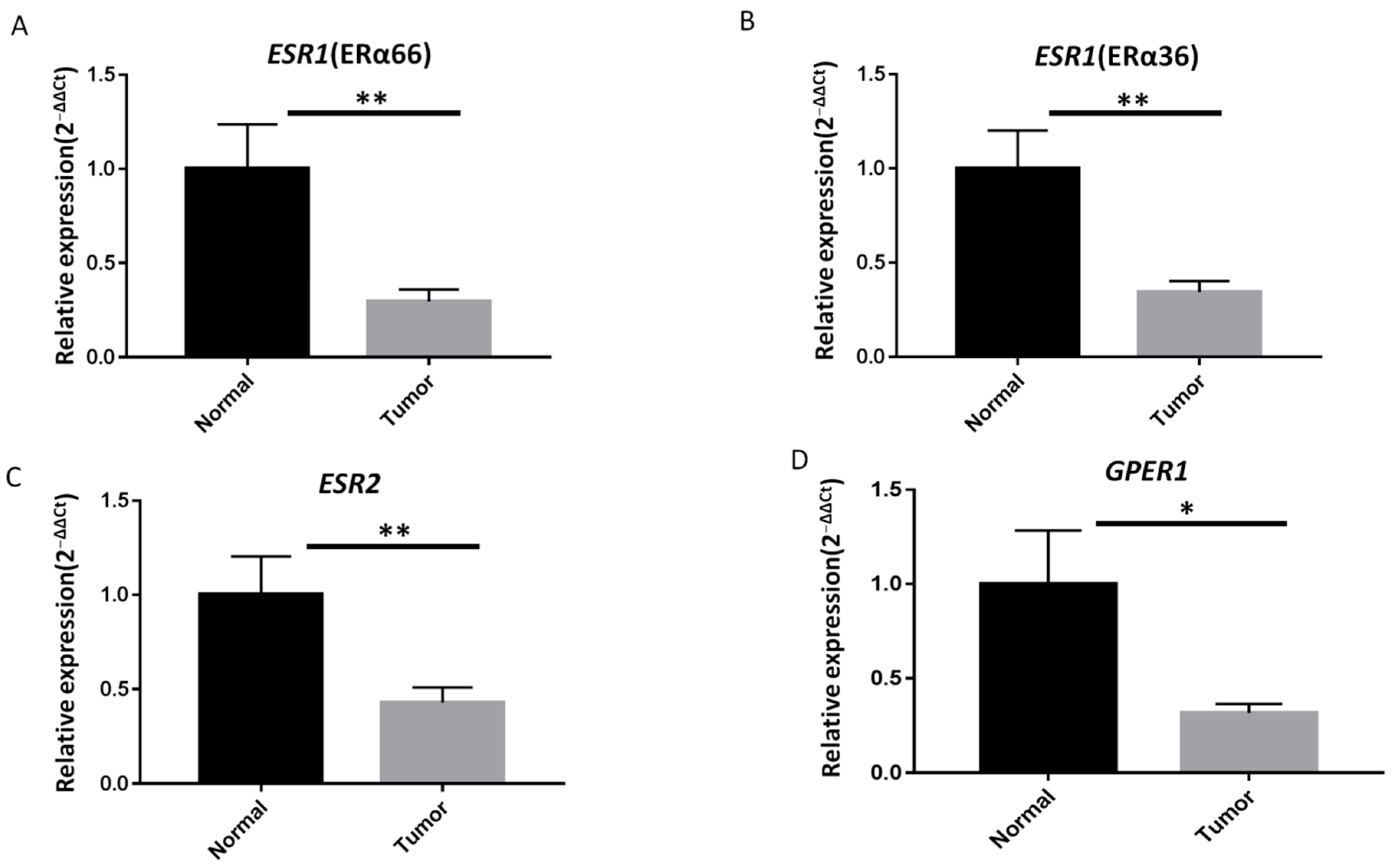
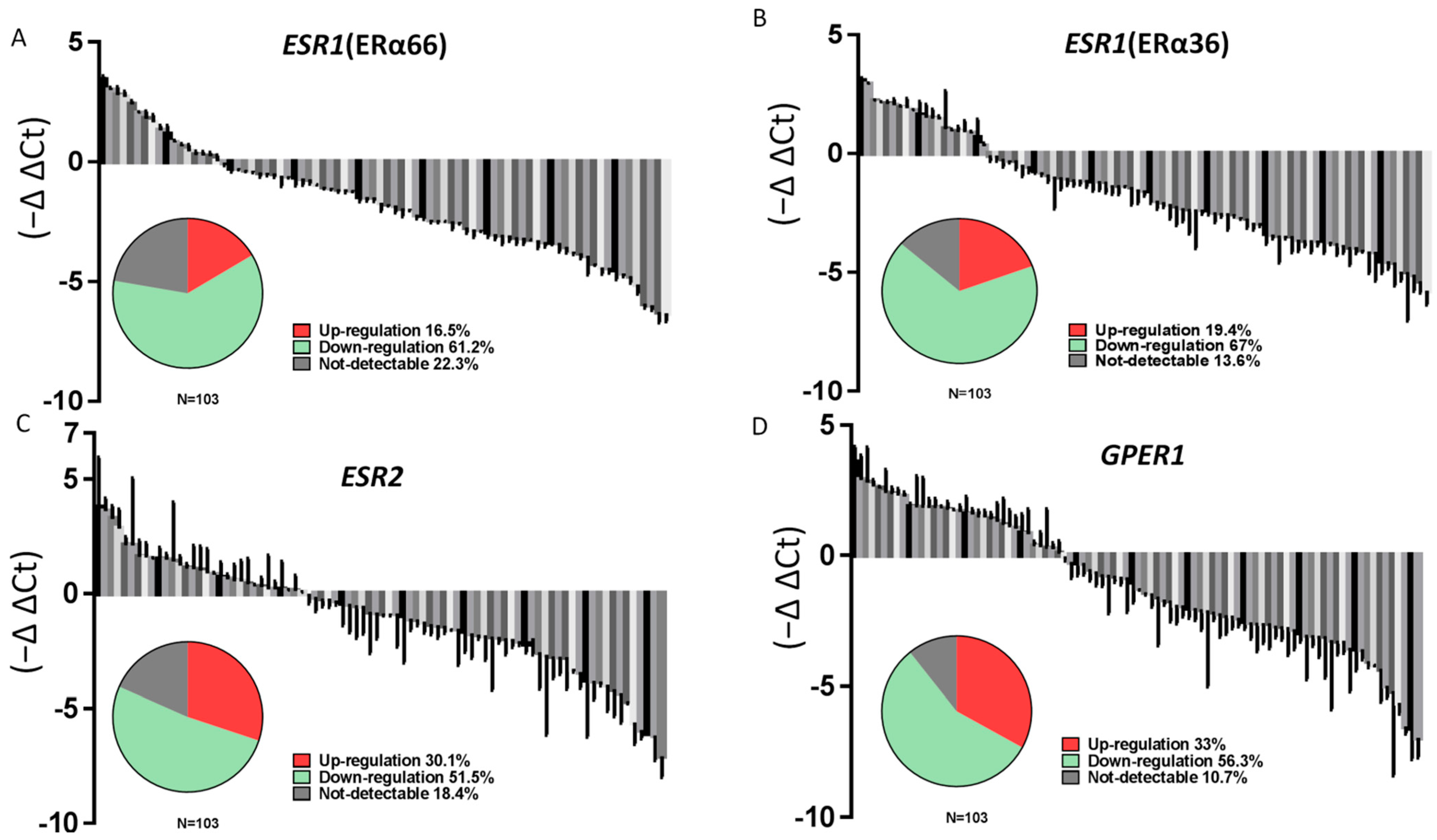
2.2. ER Expression Is Lower in PTC Specimes Than in Adjacent Normal Thyroid Tissues
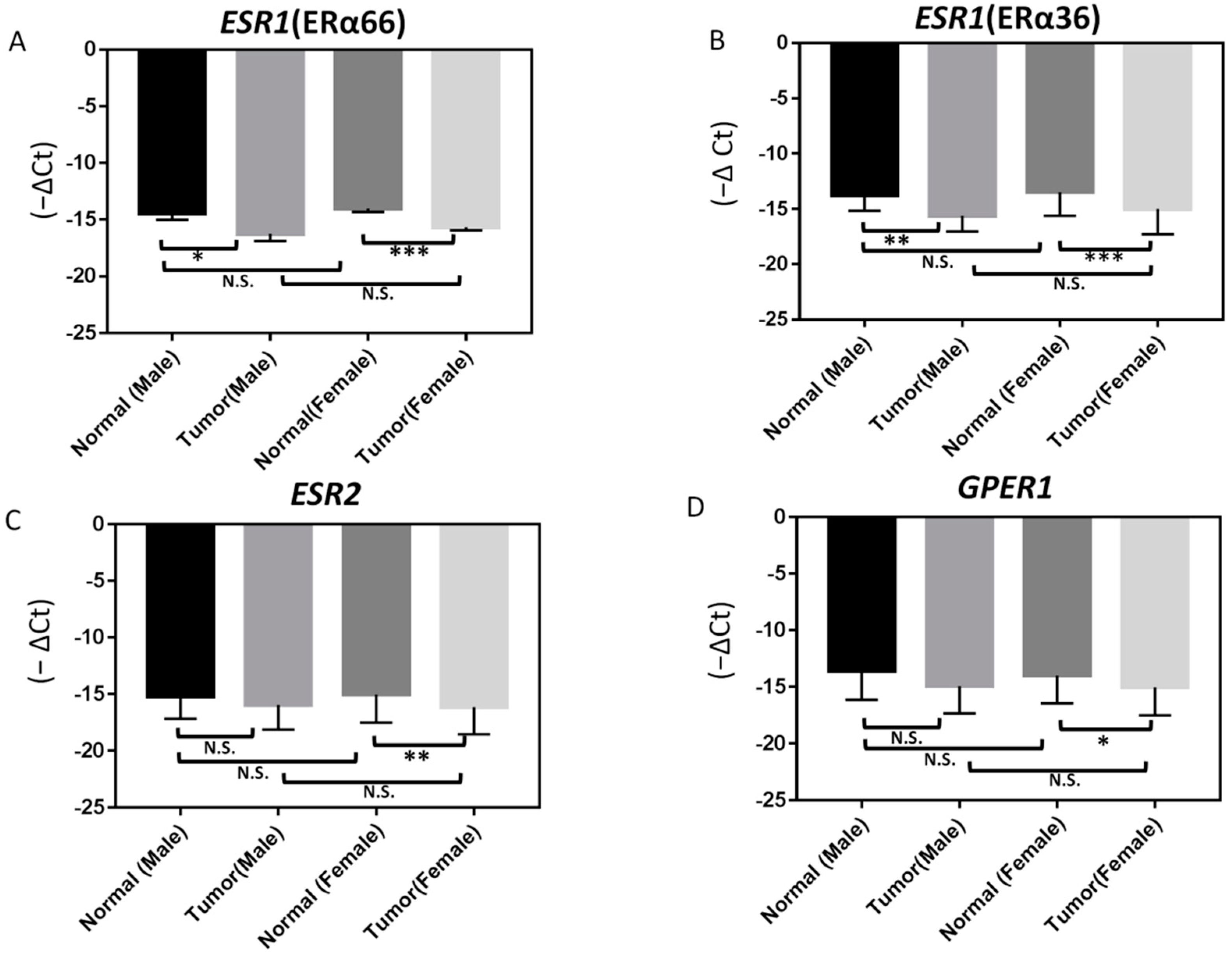
2.3. Correlation of ER Expression with Clinicopathological Characteristics in PTC
3. Discussion
4. Materials and Methods
4.1. Tumor Samples and Patient Information
4.2. RNA Extraction and Quantitative Reverse Transcription Polymerase Chain Reaction (RT-qPCR)
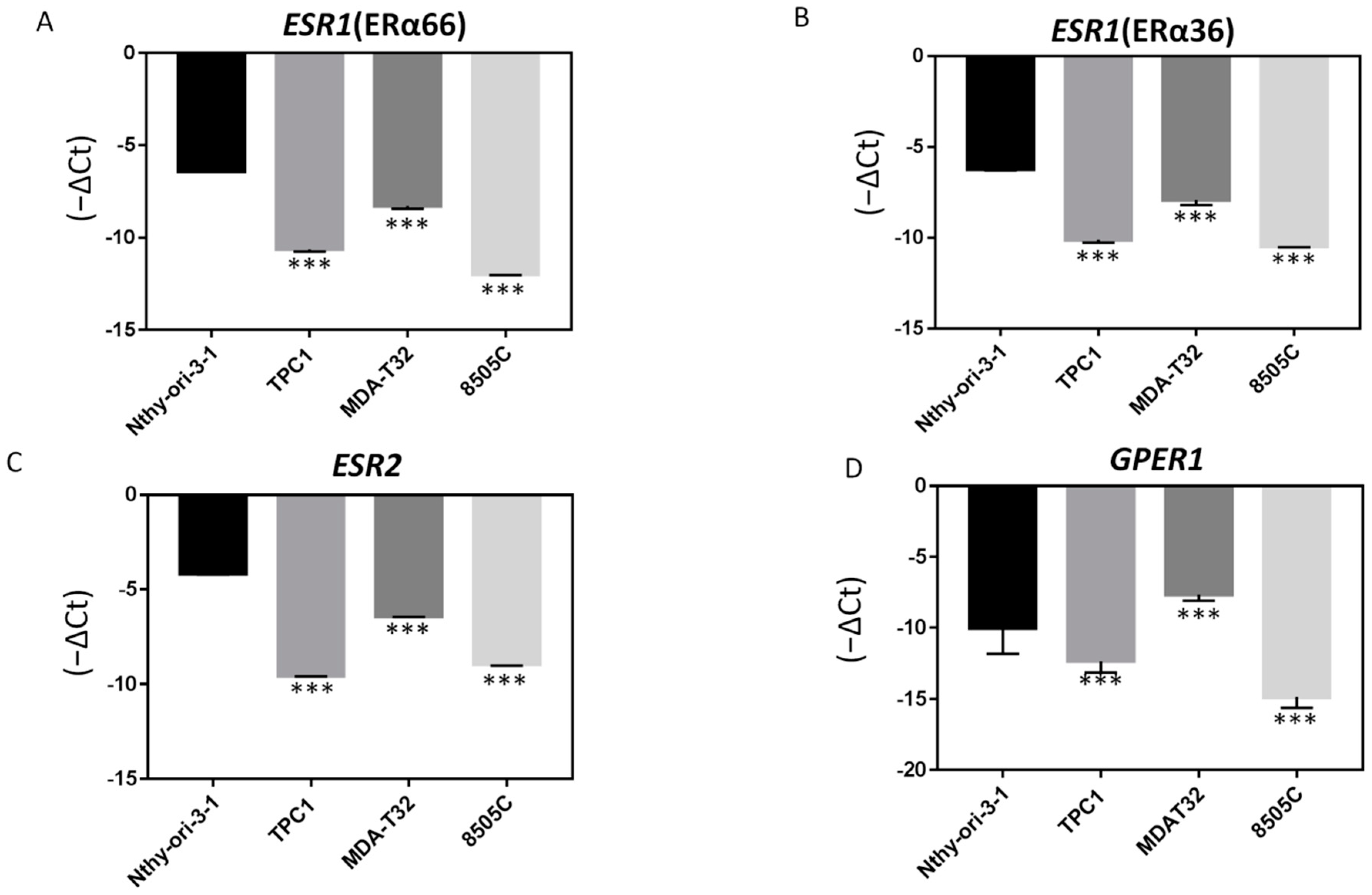
4.3. Thyroid Cancer Cell Culture
4.4. Bioinformatics Analysis
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahbari, R.; Zhang, L.; Kebebew, E. Thyroid cancer gender disparity. Future Oncol. 2010, 6, 1771–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, D.S.; Gharib, H. Epidemiology of thyroid nodules. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 901–911. [Google Scholar] [CrossRef]
- Hay, I.D.; Bergstralh, E.J.; Goellner, J.R.; Ebersold, J.R.; Grant, C.S. Predicting outcome in papillary thyroid carcinoma: Development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 1993, 114, 1050–1057; discussion 1057–1058. [Google Scholar]
- Guo, K.; Wang, Z. Risk factors influencing the recurrence of papillary thyroid carcinoma: A systematic review and meta-analysis. Int. J. Clin. Exp. Pathol. 2014, 7, 5393–5403. [Google Scholar] [PubMed]
- Stanisic, V.; Lonard, D.M.; O’Malley, B.W. Modulation of steroid hormone receptor activity. Prog. Brain Res. 2010, 181, 153–176. [Google Scholar] [PubMed]
- Chou, C.K.; Chi, S.Y.; Chou, F.F.; Huang, S.C.; Wang, J.H.; Chen, C.C.; Kang, H.Y. Aberrant Expression of Androgen Receptor Associated with High Cancer Risk and Extrathyroidal Extension in Papillary Thyroid Carcinoma. Cancers 2020, 12, 1109. [Google Scholar] [CrossRef] [PubMed]
- Mangelsdorf, D.J.; Thummel, C.; Beato, M.; Herrlich, P.; Schutz, G.; Umesono, K.; Blumberg, B.; Kastner, P.; Mark, M.; Chambon, P.; et al. The nuclear receptor superfamily: The second decade. Cell 1995, 83, 835–839. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.G.; Zeng, Q.; Tse, G.M. Estrogen and its receptors in cancer. Med. Res. Rev. 2008, 28, 954–974. [Google Scholar] [CrossRef]
- Derwahl, M.; Nicula, D. Estrogen and its role in thyroid cancer. Endocr. Relat. Cancer 2014, 21, T273–T283. [Google Scholar] [CrossRef] [PubMed]
- Manole, D.; Schildknecht, B.; Gosnell, B.; Adams, E.; Derwahl, M. Estrogen promotes growth of human thyroid tumor cells by different molecular mechanisms. J. Clin. Endocrinol. Metab. 2001, 86, 1072–1077. [Google Scholar] [CrossRef]
- Lee, M.L.; Chen, G.G.; Vlantis, A.C.; Tse, G.M.; Leung, B.C.; van Hasselt, C.A. Induction of thyroid papillary carcinoma cell proliferation by estrogen is associated with an altered expression of Bcl-xL. Cancer J. 2005, 11, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Halon, A.; Nowak-Markwitz, E.; Maciejczyk, A.; Pudelko, M.; Gansukh, T.; Gyorffy, B.; Donizy, P.; Murawa, D.; Matkowski, R.; Spaczynski, M.; et al. Loss of estrogen receptor beta expression correlates with shorter overall survival and lack of clinical response to chemotherapy in ovarian cancer patients. Anticancer Res. 2011, 31, 711–718. [Google Scholar] [PubMed]
- Mauro, L.V.; Dalurzo, M.; Carlini, M.J.; Smith, D.; Nunez, M.; Simian, M.; Lastiri, J.; Vasallo, B.; Bal de Kier Joffe, E.; Pallotta, M.G.; et al. Estrogen receptor beta and epidermal growth factor receptor as early-stage prognostic biomarkers of non-small cell lung cancer. Oncol. Rep. 2010, 24, 1331–1338. [Google Scholar] [PubMed] [Green Version]
- Tallini, G.; Garcia-Rostan, G.; Herrero, A.; Zelterman, D.; Viale, G.; Bosari, S.; Carcangiu, M.L. Downregulation of p27KIP1 and Ki67/Mib1 labeling index support the classification of thyroid carcinoma into prognostically relevant categories. Am. J. Surg. Pathol. 1999, 23, 678–685. [Google Scholar] [CrossRef]
- Heikkila, A.; Hagstrom, J.; Maenpaa, H.; Louhimo, J.; Siironen, P.; Heiskanen, I.; Haglund, C.; Arola, J. Loss of estrogen receptor Beta expression in follicular thyroid carcinoma predicts poor outcome. Thyroid 2013, 23, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Folkerd, E.; Dowsett, M. Sex hormones and breast cancer risk and prognosis. Breast 2013, 22, S38–S43. [Google Scholar] [CrossRef]
- Daniels, N.A.; Nielson, C.M.; Hoffman, A.R.; Bauer, D.C.; Osteoporotic Fractures In Men Study, G. Sex hormones and the risk of incident prostate cancer. Urology 2010, 76, 1034–1040. [Google Scholar] [CrossRef] [Green Version]
- Casper, J.; Zweig, A.S.; Villarreal, C.; Tyner, C.; Speir, M.L.; Rosenbloom, K.R.; Raney, B.J.; Lee, C.M.; Lee, B.T.; Karolchik, D.; et al. The UCSC Genome Browser database: 2018 update. Nucleic Acids Res. 2018, 46, D762–D769. [Google Scholar] [CrossRef] [Green Version]
- Bardin, A.; Boulle, N.; Lazennec, G.; Vignon, F.; Pujol, P. Loss of ERbeta expression as a common step in estrogen-dependent tumor progression. Endocr. Relat. Cancer 2004, 11, 537–551. [Google Scholar] [CrossRef] [Green Version]
- Magri, F.; Capelli, V.; Gaiti, M.; Villani, L.; Zerbini, F.; La Manna, L.; Rotondi, M.; Chiovato, L. ER-alpha and ER-beta expression in differentiated thyroid cancer: Relation with tumor phenotype across the TNM staging and peri-tumor inflammation. Endocrine 2015, 49, 429–435. [Google Scholar] [CrossRef]
- Chen, G.G.; Vlantis, A.C.; Zeng, Q.; van Hasselt, C.A. Regulation of cell growth by estrogen signaling and potential targets in thyroid cancer. Curr. Cancer Drug Targets 2008, 8, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.J.; Qiu, Y.B.; Jiang, R.; Xu, M.; Zhao, L.; Chen, G.G.; Liu, Z.M. Concomitant high expression of ERalpha36, EGFR and HER2 is associated with aggressive behaviors of papillary thyroid carcinomas. Sci. Rep. 2017, 7, 12279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.; Zhang, X.B.; Zhang, X.L.; Fu, W.L. Methylation status of oestrogen receptor alpha-A: A predictor of prognosis in leukaemias. Biosci. Rep. 2010, 30, 217–222. [Google Scholar] [CrossRef]
- Wei, J.; Han, B.; Mao, X.Y.; Wei, M.J.; Yao, F.; Jin, F. Promoter methylation status and expression of estrogen receptor alpha in familial breast cancer patients. Tumour Biol. 2012, 33, 413–420. [Google Scholar] [CrossRef]
- Ramos, E.A.; Camargo, A.A.; Braun, K.; Slowik, R.; Cavalli, I.J.; Ribeiro, E.M.; Pedrosa Fde, O.; de Souza, E.M.; Costa, F.F.; Klassen, G. Simultaneous CXCL12 and ESR1 CpG island hypermethylation correlates with poor prognosis in sporadic breast cancer. BMC Cancer 2010, 10, 23. [Google Scholar] [CrossRef] [Green Version]
- Prossnitz, E.R.; Barton, M. Signaling, physiological functions and clinical relevance of the G protein-coupled estrogen receptor GPER. Prostaglandins Other Lipid Mediat. 2009, 89, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Weber, R.; Bertoni, A.P.; Bessestil, L.W.; Brum, I.S.; Furlanetto, T.W. Decreased Expression of GPER1 Gene and Protein in Goiter. Int. J. Endocrinol. 2015, 2015, 869431. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, X.; Shen, P.; Loggie, B.W.; Chang, Y.; Deuel, T.F. A variant of estrogen receptor-{alpha}, hER-{alpha}36: Transduction of estrogen- and antiestrogen-dependent membrane-initiated mitogenic signaling. Proc. Natl. Acad. Sci. USA 2006, 103, 9063–9068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertoni, A.P.S.; Manfroi, P.A.; Tomedi, J.; Assis-Brasil, B.M.; de Souza Meyer, E.L.; Furlanetto, T.W. The gene expression of GPER1 is low in fresh samples of papillary thyroid carcinoma (PTC), and in silico analysis. Mol. Cell. Endocrinol. 2021, 535, 111397. [Google Scholar] [CrossRef]
- Zhao, Y.; Yang, Z.; Miao, Y.; Fan, M.; Zhao, X.; Wei, Q.; Ma, B. G protein-coupled estrogen receptor 1 inhibits the epithelial-mesenchymal transition of goat mammary epithelial cells via NF-kappaB signalling pathway. Reprod. Domest. Anim. 2021, 56, 1137–1144. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Dong, W.; Li, J.; Zhang, H.; Shan, Z.; Teng, W. Differential expression patterns and clinical significance of estrogen receptor-alpha and beta in papillary thyroid carcinoma. BMC Cancer 2014, 14, 383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturniolo, G.; Zafon, C.; Moleti, M.; Castellvi, J.; Vermiglio, F.; Mesa, J. Immunohistochemical Expression of Estrogen Receptor-alpha and Progesterone Receptor in Patients with Papillary Thyroid Cancer. Eur. Thyroid J. 2016, 5, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Qi, W.; Zhang, P.; Guan, H.; Wang, L. Expression of the estrogen receptor alpha, progesterone receptor and epidermal growth factor receptor in papillary thyroid carcinoma tissues. Oncol. Lett. 2015, 10, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, C.K.; Chen, R.F.; Chou, F.F.; Chang, H.W.; Chen, Y.J.; Lee, Y.F.; Yang, K.D.; Cheng, J.T.; Huang, C.C.; Liu, R.T. miR-146b is highly expressed in adult papillary thyroid carcinomas with high risk features including extrathyroidal invasion and the BRAF(V600E) mutation. Thyroid 2010, 20, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Features | n (%) |
|---|---|
| Age at the time of diagnosis (years) | 47.18 ± 12.82 |
| Sex (male/female) | 21/82 |
| Tumor size (cm) | 1.90 ± 1.10 |
| Lymph node metastasis | 38 (36.8%) |
| Extrathyroidal extension | 30 (29.1%) |
| Tumor staging (AJCC) a | |
| Low-risk | 93 (90.2%) |
| High-risk | 10 (9.7%) |
| Distant metastasis | 1 (0.97%) |
| Clinical Features | ERα66 | ERα36 | ERβ | GPER1 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 2−(ΔΔCt) | p | 2−(ΔΔCt) | p | 2−(ΔΔCt) | p | 2−(ΔΔCt) | p | ||
| Age (years) | <55 | 1.77 ± 0.28 | 0.60 | 1.94 ± 0.22 | 0.59 | 1.11 ± 0.29 | 0.09 | 1.89 ± 0.31 | 0.63 |
| ≥55 | 1.23 ± 0.21 | 2.49 ± 0.44 | 0.66 ± 0.14 | 2.31 0.83 | |||||
| Sex | Feale | 1.67 ± 0.23 | 0.47 | 1.44 ± 0.23 | 0.06 | 1.10 ± 0.24 | 0.44 | 1.68 ± 0.25 | 0.40 |
| Male | 1.25 ± 0.30 | 0.8 ± 0.43 | 0.99 ± 0.22 | 2.24 ± 0.64 | |||||
| Lymph node metastasis | Absent | 1.43 ± 0.24 | 0.36 | 1.95 ± 0.20 | 0.49 | 1.21 ± 0.35 | 0.74 | 2.22 ± 0.50 | 0.70 |
| Present | 1.84 ± 0.33 | 1.76 ± 0.42 | 0.95 ± 0.15 | 1.79 ± 0.39 | |||||
| Extrathyroidal extension | Absent | 1.76 ± 0.27 | 0.79 | 1.06 ± 0.22 | 0.16 | 0.83 ± 0.12 | 0.12 | 2.2 ± 0.45 | 0.04 b |
| Present | 1.03 ± 0.16 | 1.8 ± 0.45 | 1.65 ± 0.62 | 0.97 ± 0.22 | |||||
| Tumor staging (AJCC) a | Low | 1.62 ± 0.22 | 0.60 | 1.1 ± 0.20 | 0.11 | 1.09 ± 0.23 | 0.76 | 1.86 ± 0.33 | 0.19 |
| High | 0.95 ± 0.23 | 2.7 ± 0.91 | 1.05 ± 0.36 | 0.90 ± 0.73 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, C.-K.; Chi, S.-Y.; Hung, Y.-Y.; Yang, Y.-C.; Fu, H.-C.; Wang, J.-H.; Chen, C.-C.; Kang, H.-Y. Decreased Expression of Estrogen Receptors Is Associated with Tumorigenesis in Papillary Thyroid Carcinoma. Int. J. Mol. Sci. 2022, 23, 1015. https://doi.org/10.3390/ijms23031015
Chou C-K, Chi S-Y, Hung Y-Y, Yang Y-C, Fu H-C, Wang J-H, Chen C-C, Kang H-Y. Decreased Expression of Estrogen Receptors Is Associated with Tumorigenesis in Papillary Thyroid Carcinoma. International Journal of Molecular Sciences. 2022; 23(3):1015. https://doi.org/10.3390/ijms23031015
Chicago/Turabian StyleChou, Chen-Kai, Shun-Yu Chi, Yi-Yung Hung, Yi-Chien Yang, Hung-Chun Fu, Jia-He Wang, Chueh-Chen Chen, and Hong-Yo Kang. 2022. "Decreased Expression of Estrogen Receptors Is Associated with Tumorigenesis in Papillary Thyroid Carcinoma" International Journal of Molecular Sciences 23, no. 3: 1015. https://doi.org/10.3390/ijms23031015
APA StyleChou, C.-K., Chi, S.-Y., Hung, Y.-Y., Yang, Y.-C., Fu, H.-C., Wang, J.-H., Chen, C.-C., & Kang, H.-Y. (2022). Decreased Expression of Estrogen Receptors Is Associated with Tumorigenesis in Papillary Thyroid Carcinoma. International Journal of Molecular Sciences, 23(3), 1015. https://doi.org/10.3390/ijms23031015