
Constipation Mitigation by Rhubarb Extract in Middle-Aged Adults Is Linked to Gut Microbiome Modulation: A Double-Blind Randomized Placebo-Controlled Trial
 , ,
, ,  , , and
, , and 
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics of Volunteers
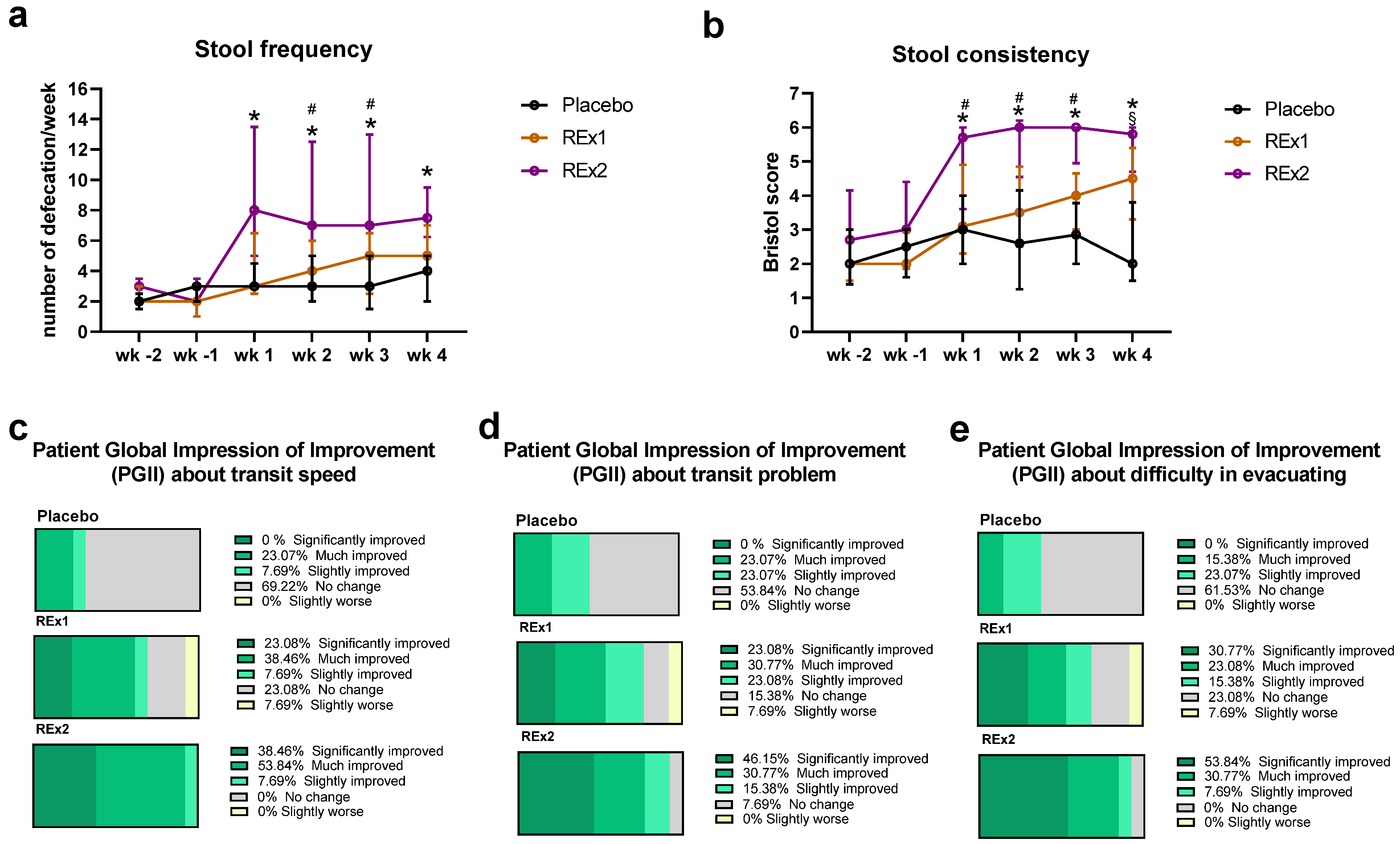
2.2. Rhubarb Extract Supplementation Improved Intestinal Transit without Changing Dietary Habits or Safety Parameters
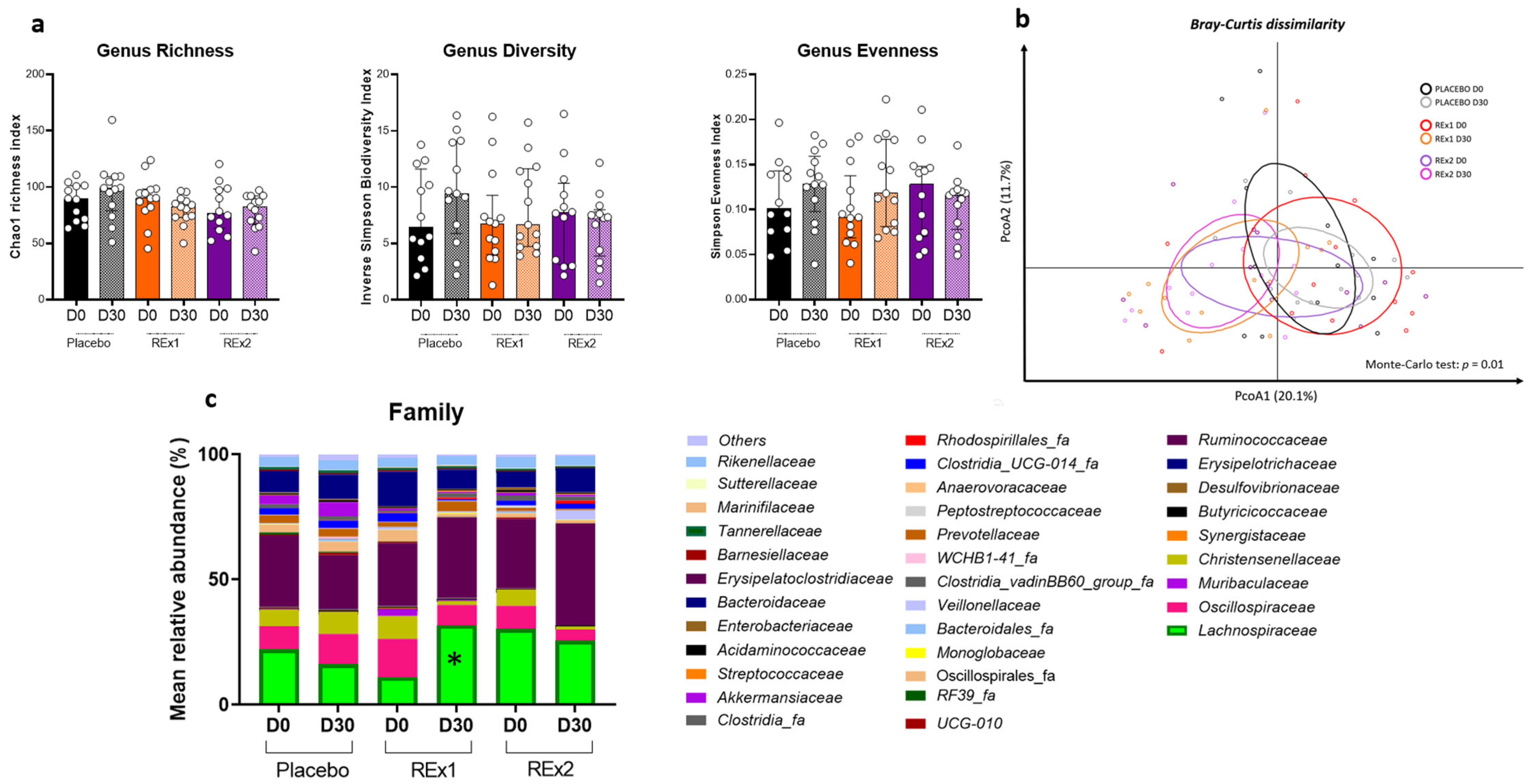
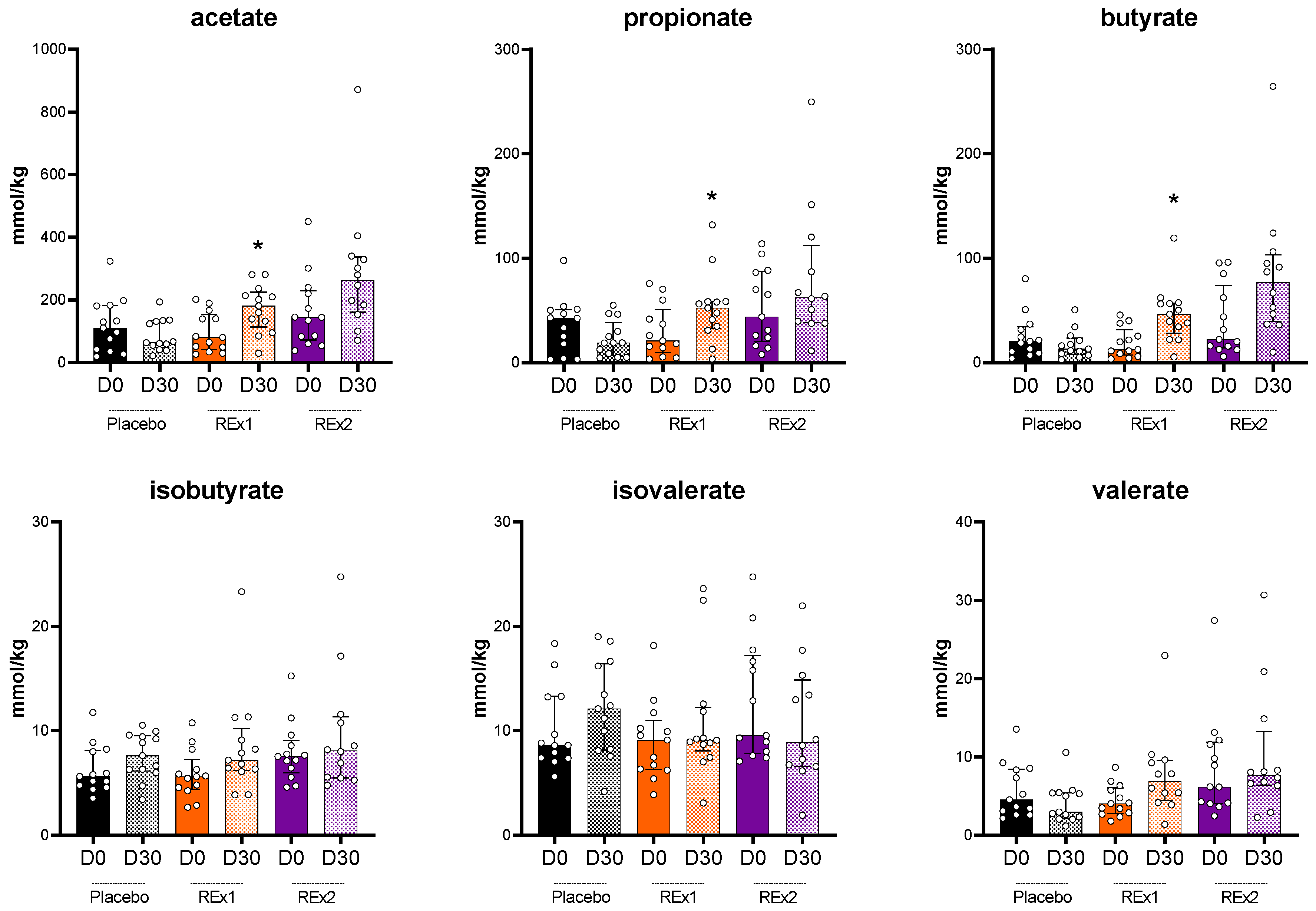
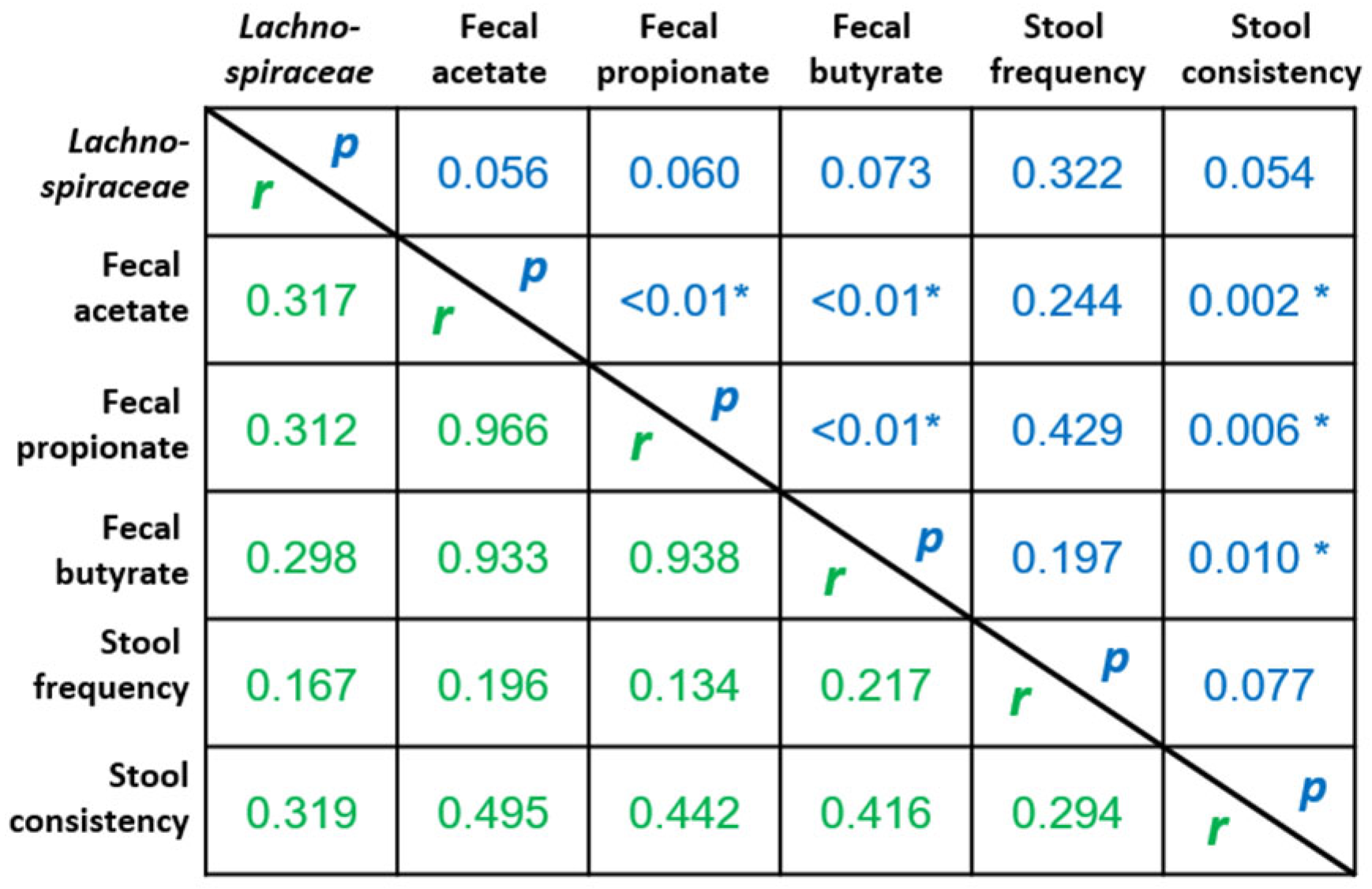
2.3. Rhubarb Extract Supplementation Induces Changes in Gut Microbiome
3. Discussion
4. Materials and Methods
4.1. Power Analysis and Sample Size
4.2. Clinical Study
4.3. Intervention
4.4. Transit Characteristics
4.5. Plasma Analysis
4.6. Quality of Life Assessment
4.7. Gut Microbiota Analyses
4.8. Fecal Short Chain Fatty Acid
4.9. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yarullina, D.R.; Shafigullin, M.U.; Sakulin, K.A.; Arzamastseva, A.A.; Shaidullov, I.F.; Markelova, M.I.; Grigoryeva, T.V.; Karpukhin, O.Y.; Sitdikova, G.F. Characterization of gut contractility and microbiota in patients with severe chronic constipation. PLoS ONE 2020, 15, e0235985. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.M.; Simrén, M.; Farmer, A.D.; Dinning, P.G.; Carrington, E.V.; Benninga, M.A.; Burgell, R.E.; Dimidi, E.; Fikree, A.; Ford, A.C.; et al. Chronic constipation in adults: Contemporary perspectives and clinical challenges. 1: Epidemiology, diagnosis, clinical associations, pathophysiology and investigation. Neurogastroenterol. Motil. 2020, 33, e14050. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, P.C.; Marcobal, A.; Ursell, L.K.; Larauche, M.; Duboc, H.; Earle, K.A.; Sonnenburg, E.D.; Ferreyra, J.A.; Higginbottom, S.K.; Million, M.; et al. Complex Interactions Among Diet, Gastrointestinal Transit, and Gut Microbiota in Humanized Mice. Gastroenterology 2013, 144, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Werth, B.L.; Christopher, S.-A. Laxative Use in the Community: A Literature Review. J. Clin. Med. 2021, 10, 143. [Google Scholar] [CrossRef]
- Gallegos-Orozco, J.F.; Foxx-Orenstein, A.E.; Sterler, S.M.; Stoa, J.M. Chronic Constipation in the Elderly. Am. J. Gastroenterol. 2012, 107, 18–25. [Google Scholar] [CrossRef]
- Wei, L.; Luo, Y.; Zhang, X.; Liu, Y.; Gasser, M.; Tang, F.; Ouyang, W.-W.; Wei, H.; Lu, S.; Yang, Z.; et al. Topical therapy with rhubarb navel plasters in patients with chronic constipation: Results from a prospective randomized multicenter study. J. Ethnopharmacol. 2020, 264, 113096. [Google Scholar] [CrossRef]
- Régnier, M.; Rastelli, M.; Morissette, A.; Suriano, F.; Le Roy, T.; Pilon, G.; Delzenne, N.M.; Marette, A.; Van Hul, M.; Cani, P.D. Rhubarb Supplementation Prevents Diet-Induced Obesity and Diabetes in Association with Increased Akkermansia muciniphila in Mice. Nutrients 2020, 12, 2932. [Google Scholar] [CrossRef]
- Neyrinck, A.M.; Etxeberria, U.; Taminiau, B.; Daube, G.; Van Hul, M.; Everard, A.; Cani, P.D.; Bindels, L.B.; Delzenne, N.M. Rhubarb extract prevents hepatic inflammation induced by acute alcohol intake, an effect related to the modulation of the gut microbiota. Mol. Nutr. Food Res. 2016, 61, 1500899. [Google Scholar] [CrossRef]
- Estaquio, C.; Kesse-Guyot, E.; Deschamps, V.; Bertrais, S.; Dauchet, L.; Galan, P.; Hercberg, S.; Castetbon, K. Adherence to the French Programme National Nutrition Santé Guideline Score Is Associated with Better Nutrient Intake and Nutritional Status. J. Am. Diet. Assoc. 2009, 109, 1031–1041. [Google Scholar] [CrossRef]
- Mohtashami, L.; Amiri, M.S.; Ayati, Z.; Ramezani, M.; Jamialahmadi, T.; Emami, S.A.; Sahebkar, A. Ethnobotanical Uses, Phytochemistry and Pharmacology of Different Rheum Species (Polygonaceae): A Review. In Pharmacological Properties of Plant-Derived Natural Products and Implications for Human Health; Springer International Publishing: Cham, Switzerland, 2021; pp. 309–352. [Google Scholar] [CrossRef]
- Marciniak, C.M.; Lee, J.; Jesselson, M.; Gaebler-Spira, D. Cross-Sectional Study of Bowel Symptoms in Adults With Cerebral Palsy: Prevalence and Impact on Quality of Life. Arch. Phys. Med. Rehabil. 2015, 96, 2176–2183. [Google Scholar] [CrossRef]
- Belsey, J.; Greenfield, S.M.; Candy, D.; Geraint, M. Systematic review: Impact of constipation on quality of life in adults and children. Aliment. Pharmacol. Ther. 2010, 31, 938–949. [Google Scholar] [CrossRef]
- Rao, S.S.C.; Lichtlen, P.; Habibi, S. Effects of Lubiprostone, an Intestinal Secretagogue, on Electrolyte Homeostasis in Chronic Idiopathic and Opioid-induced Constipation. J. Clin. Gastroenterol. 2020, 55, 512–519. [Google Scholar] [CrossRef]
- Arakelyan, A.; Petrkova, J.; Hermanova, Z.; Boyajyan, A.; Lukl, J.; Petrek, M. Serum Levels of the MCP-1 Chemokine in Patients With Ischemic Stroke and Myocardial Infarction. Mediat. Inflamm. 2005, 2005, 175–179. [Google Scholar] [CrossRef]
- Quigley, E.M.M. Microflora Modulation of Motility. J. Neurogastroenterol. Motil. 2011, 17, 140–147. [Google Scholar] [CrossRef]
- Quigley, E.M.M. The enteric microbiota in the pathogenesis and management of constipation. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 119–126. [Google Scholar] [CrossRef]
- Khalif, I.L.; Quigley, E.M.M.; Konovitch, E.A.; Maximova, I.D. Alterations in the colonic flora and intestinal permeability and evidence of immune activation in chronic constipation. Dig. Liver Dis. 2005, 37, 838–849. [Google Scholar] [CrossRef]
- Ohkusa, T.; Koido, S.; Nishikawa, Y.; Sato, N. Gut Microbiota and Chronic Constipation: A Review and Update. Front. Med. 2019, 6, 19. [Google Scholar] [CrossRef]
- Zhu, L.; Liu, W.; Alkhouri, R.; Baker, R.D.; Bard, J.E.; Quigley, E.M.; Baker, S.S. Structural changes in the gut microbiome of constipated patients. Physiol. Genom. 2014, 46, 679–686. [Google Scholar] [CrossRef]
- Zhuang, M.; Shang, W.; Ma, Q.; Strappe, P.; Zhou, Z. Abundance of Probiotics and Butyrate-Production Microbiome Manages Constipation via Short-Chain Fatty Acids Production and Hormones Secretion. Mol. Nutr. Food Res. 2019, 63, e1801187. [Google Scholar] [CrossRef]
- Yang, L.; Wan, Y.; Li, W.; Liu, C.; Li, H.-F.; Dong, Z.; Zhu, K.; Jiang, S.; Shang, E.; Qian, D.; et al. Targeting intestinal flora and its metabolism to explore the laxative effects of rhubarb. Appl. Microbiol. Biotechnol. 2022, 106, 1615–1631. [Google Scholar] [CrossRef]
- Tang, T.; Wang, F.; Liu, J.; Ye, W.; Zhao, T.; Li, Z. Rhubarb alleviates acute lung injury by modulating gut microbiota dysbiosis in mice. Curr. Microbiol. 2022, 79, 116. [Google Scholar] [CrossRef]
- Jalanka, J.; Major, G.; Murray, K.; Singh, G.; Nowak, A.; Kurtz, C.; Silos-Santiago, I.; Johnston, J.M.; de Vos, W.M.; Spiller, R. The Effect of Psyllium Husk on Intestinal Microbiota in Constipated Patients and Healthy Controls. Int. J. Mol. Sci. 2019, 20, 433. [Google Scholar] [CrossRef] [PubMed]
- Vacca, M.; Celano, G.; Calabrese, F.M.; Portincasa, P.; Gobbetti, M.; De Angelis, M. The controversial role of human gut lachnospiraceae. Microorganisms 2020, 8, 573. [Google Scholar] [CrossRef] [PubMed]
- Kon, R.; Ikarashi, N.; Nagoya, C.; Takayama, T.; Kusunoki, Y.; Ishii, M.; Ueda, H.; Ochiai, W.; Machida, Y.; Sugita, K.; et al. Rheinanthrone, a metabolite of sennoside A, triggers macrophage activation to decrease aquaporin-3 expression in the colon, causing the laxative effect of rhubarb extract. J. Ethnopharmacol. 2014, 152, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Leng-Peschlow, E. Acceleration of large intestine transit time in rats by sennosides and related compounds. J. Pharm. Pharmacol. 1986, 38, 369–373. [Google Scholar] [CrossRef]
- Staumont, G.; Fioramonti, J.; Frexinos, J.; Bueno, L. Changes in colonic motility induced by sennosides in dogs: Evidence of a prostaglandin mediation. Gut 1988, 29, 1180–1187. [Google Scholar] [CrossRef]
- McCrea, G.L.; Miaskowski, C.; Stotts, N.A.; Macera, L.; Varma, M.G. A Review of the Literature on Gender and Age Differences in the Prevalence and Characteristics of Constipation in North America. J. Pain Symptom Manag. 2009, 37, 737–745. [Google Scholar] [CrossRef]
- de Oliveira, E.P.; Burini, R.C. The impact of physical exercise on the gastrointestinal tract. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 533–538. [Google Scholar] [CrossRef]
- Lewis, S.J.; Heaton, K.W. Stool Form Scale as a Useful Guide to Intestinal Transit Time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Alyousif, Z.; Miller, J.L.; Sandoval, M.Y.; MacPherson, C.W.; Nagulesapillai, V.; Dahl, W.J. The effects of Bifidobacterium animalis ssp. lactis B94 on gastrointestinal wellness in adults with Prader-Willi syndrome: Study protocol for a randomized controlled trial. Trials 2018, 19, 256. [Google Scholar] [CrossRef]
- Mohebbi, M.; Dodd, S.; Dean, O.M.; Berk, M. Patient centric measures for a patient centric era: Agreement and convergent between ratings on The Patient Global Impression of Improvement (PGI-I) scale and the Clinical Global Impressions–Improvement (CGI-S) scale in bipolar and major depressive disorder. Eur. Psychiatry 2018, 53, 17–22. [Google Scholar] [CrossRef]
- Rutherford, C.; Brown, J.M.; Smith, I.; McGinnis, E.; Wilson, L.; Gilberts, R.; Brown, S.; Coleman, S.; Collier, H.; Nixon, J. A patient-reported pressure ulcer health-related quality of life instrument for use in prevention trials (PU-QOL-P): Psychometric evaluation. Health Qual. Life Outcomes 2018, 16, 227. [Google Scholar] [CrossRef]
- Aoun, S.M.; Deas, K.; Howting, D.; Lee, G. Exploring the Support Needs of Family Caregivers of Patients with Brain Cancer Using the CSNAT: A Comparative Study with Other Cancer Groups. PLoS ONE 2015, 10, e0145106. [Google Scholar] [CrossRef]
- Douny, C.; Dufourny, S.; Brose, F.; Verachtert, P.; Rondia, P.; Lebrun, S.; Marzorati, M.; Everaert, N.; Delcenserie, V.; Scippo, M.-L. Development of an analytical method to detect short-chain fatty acids by SPME-GC–MS in samples coming from an in vitro gastrointestinal model. J. Chromatogr. B 2019, 1124, 188–196. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Placebo (n = 13) | Re × 1 (n = 13) | Re × 2 (n = 13) | |
|---|---|---|---|
| Women/men N | 13/0 | 12/1 | 12/1 |
| Age (years old) | 57 ± 6 | 58 ± 6 | 58 ± 6 |
| Body weight (kg) | 65.1 ± 9.1 | 61.2 ± 10.7 | 68.1 ± 10.1 |
| BMI (kg/m2) | 24.0 ± 3.7 | 22.6 ± 2.9 | 25.4 ± 3.6 |
| SBP (mm Hg) | 117 ± 13 | 113 ± 10 | 114 ± 16 |
| DBP (mm Hg) | 75 ± 10 | 71 ± 7 | 75 ± 10 |
| ALAT (UI/L) | 21.6 ± 7.6 | 18.2 ± 7.3 | 20.7 ± 13.1 |
| ASAT (UI/L) | 22.7 ± 4.8 | 19.9 ± 4.4 | 21.9 ± 3.8 |
| Glycemia (g/l) | 0.94 ± 0.16 | 0.92 ± 0.08 | 0.92 ± 0.06 |
| Triglycerides (g/l) | 0.92 ± 0.54 | 0.78 ± 0.23 | 0.92 ± 0.23 |
| Cholesterol (g/l) | 2.28 ± 0.34 | 2.04 ± 0.34 | 2.25 ± 0.25 |
| Placebo (n = 13) | Re × 1 (n = 13) | Re × 2 (n = 13) | ||||
|---|---|---|---|---|---|---|
| D0 | D30 | D0 | D30 | D0 | D30 | |
| 65.1 ± 9.1 | 65.1 ± 9.0 | 61.2 ± 10.7 | 61.3 ± 10.5 | 68.1 ± 10.1 | 68.2 ± 10.2 | |
| Systolic blood pressure (mm Hg) | 117.3 ± 12.5 | 115.4 ± 13.0 | 112.5 ± 9.6 | 109.2 ± 14.0 | 114.2 ± 15.9 | 114.8 ± 15.7 |
| Diastolic blood pressure (mm Hg) | 75.0 ± 9.6 | 74.6 ± 7.5 | 70.9 ± 6.7 | 68.5 ± 6.6 | 75.0 ± 9.6 | 71.5 ± 11.4 |
| Alanine aminotransferase activity (U/L) | 21.6 ± 7.6 | 20.2 ± 5.1 | 18.2 ± 7.3 | 18.0 ± 8.4 | 20.7 ± 13.1 | 19.9 ± 7.8 |
| Aspartate aminotransferase activity (U/L) | 22.7 ± 4.8 | 22.3 ± 5.1 | 19.9 ± 4.4 | 21.9 ± 5.6 | 21.9 ± 3.8 | 21.6 ± 3.4 |
| Triglycerides (g/L) | 0.92 ± 0.54 | 0.87 ± 0.45 | 0.78 ± 0.23 | 0.85 ± 0.48 | 0.92 ± 0.23 | 0.96 ± 0.30 |
| Total cholesterol (g/L) | 2.28 ± 0.34 | 2.18 ± 0.25 | 2.04 ± 0.34 | 2.06 ± 0.36 | 2.25 ± 0.25 | 2.28 ± 0.34 |
| HDL-cholesterol (g/L) | 0.65 ± 0.18 | 0.63 ± 0.17 | 0.61 ± 0.16 | 0.61 ± 0.16 | 0.56 ± 0.08 | 0.56 ± 0.08 |
| LDL-cholesterol (g/L) | 1.44 ± 0.30 | 1.38 ± 0.24 | 1.28 ± 0.32 | 1.27 ± 0.33 | 1.50 ± 0.21 | 1.53 ± 0.26 |
| Glucose (g/L) | 0.94 ± 0.16 | 0.93 ± 0.13 | 0.92 ± 0.08 | 0.87 ± 0.12 | 0.92 ± 0.06 | 0.92 ± 0.09 |
| Potassium (mmol/L) | 4.13 ± 0.24 | 4.19 ± 0.28 | 4.27 ± 0.46 | 4.08 ± 0.39 | 4.14 ± 0.24 | 4.11 ± 0.34 |
| Hemoglobin (g/dL) | 13.6 ± 0.9 | 13.5 ± 0.9 | 13.5 ± 1.1 | 13.1 ± 1.1 | 13.9 ± 1.2 | 13.6 ± 1.0 |
| Leucocytes (G/L) | 5.91 ± 2.00 | 5.26 ± 1.75 * | 5.80 ± 1.15 | 5.92 ± 0.86 | 5.45 ± 1.27 | 5.30 ± 1.03 |
| Lymphocytes (G/L) | 1.83 ± 0.49 | 1.76 ± 0.39 | 1.82 ± 0.45 | 1.79 ± 0.39 | 1.94 ± 0.53 | 2.00 ± 0.48 |
| Monocytes (G/L) | 0.49 ± 0.13 | 0.45 ± 0.13 | 0.46 ± 0.08 | 0.49 ± 0.13 | 0.47 ± 0.14 | 0.46 ± 0.10 |
| TNFα (pg/mL) | 31.0 ± 33.8 | 35.9 ± 24.7 | 33.8 ± 22.3 | 41.7 ± 25.9 | 44.8 ± 34.2 | 55.4 ± 43.0 |
| MCP1 (pg/mL) | 197.6 ± 55.5 | 207.4 ± 62.5 | 215.0 ± 67.9 | 249.9 ± 103.6 * | 277.9 ± 92.1 | 273.2 ± 63.8 |
| IL1β (pg/mL) | 11.3 ± 17.9 | 15.8 ± 12.8 | 12.6 ± 12.0 | 16.2 ± 12.4 | 16.4 ± 17.7 | 22.1 ± 22.5 |
| IL8 (pg/mL) | 5.9 ± 4.7 | 7.1 ± 3.9 | 6.7 ± 4.1 | 8.2 ± 5.2 | 8.7 ± 6.6 | 10.4 ± 6.9 |
| IL10 (pg/mL) | 29.3 ± 53.8 | 29.2 ± 35.6 | 23.3 ± 26.0 | 30.2 ± 25.7 | 36.2 ± 40.7 | 49.3 ± 57.1 |
| IFNγ (pg/mL) | 27.4 ± 40.3 | 38.7 ± 30.4 | 29.9 ± 27.4 | 43.6 ± 37.5 | 48.2 ± 58.2 | 60.9 ± 56.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neyrinck, A.M.; Rodriguez, J.; Taminiau, B.; Herpin, F.; Cani, P.D.; Daube, G.; Bindels, L.B.; Delzenne, N.M. Constipation Mitigation by Rhubarb Extract in Middle-Aged Adults Is Linked to Gut Microbiome Modulation: A Double-Blind Randomized Placebo-Controlled Trial. Int. J. Mol. Sci. 2022, 23, 14685. https://doi.org/10.3390/ijms232314685
Neyrinck AM, Rodriguez J, Taminiau B, Herpin F, Cani PD, Daube G, Bindels LB, Delzenne NM. Constipation Mitigation by Rhubarb Extract in Middle-Aged Adults Is Linked to Gut Microbiome Modulation: A Double-Blind Randomized Placebo-Controlled Trial. International Journal of Molecular Sciences. 2022; 23(23):14685. https://doi.org/10.3390/ijms232314685
Chicago/Turabian StyleNeyrinck, Audrey M., Julie Rodriguez, Bernard Taminiau, Florent Herpin, Patrice D. Cani, Georges Daube, Laure B. Bindels, and Nathalie M. Delzenne. 2022. "Constipation Mitigation by Rhubarb Extract in Middle-Aged Adults Is Linked to Gut Microbiome Modulation: A Double-Blind Randomized Placebo-Controlled Trial" International Journal of Molecular Sciences 23, no. 23: 14685. https://doi.org/10.3390/ijms232314685
APA StyleNeyrinck, A. M., Rodriguez, J., Taminiau, B., Herpin, F., Cani, P. D., Daube, G., Bindels, L. B., & Delzenne, N. M. (2022). Constipation Mitigation by Rhubarb Extract in Middle-Aged Adults Is Linked to Gut Microbiome Modulation: A Double-Blind Randomized Placebo-Controlled Trial. International Journal of Molecular Sciences, 23(23), 14685. https://doi.org/10.3390/ijms232314685