
Mechanism Underlying Metformin Action and Its Potential to Reduce Gastric Cancer Risk



Abstract

1. Introduction
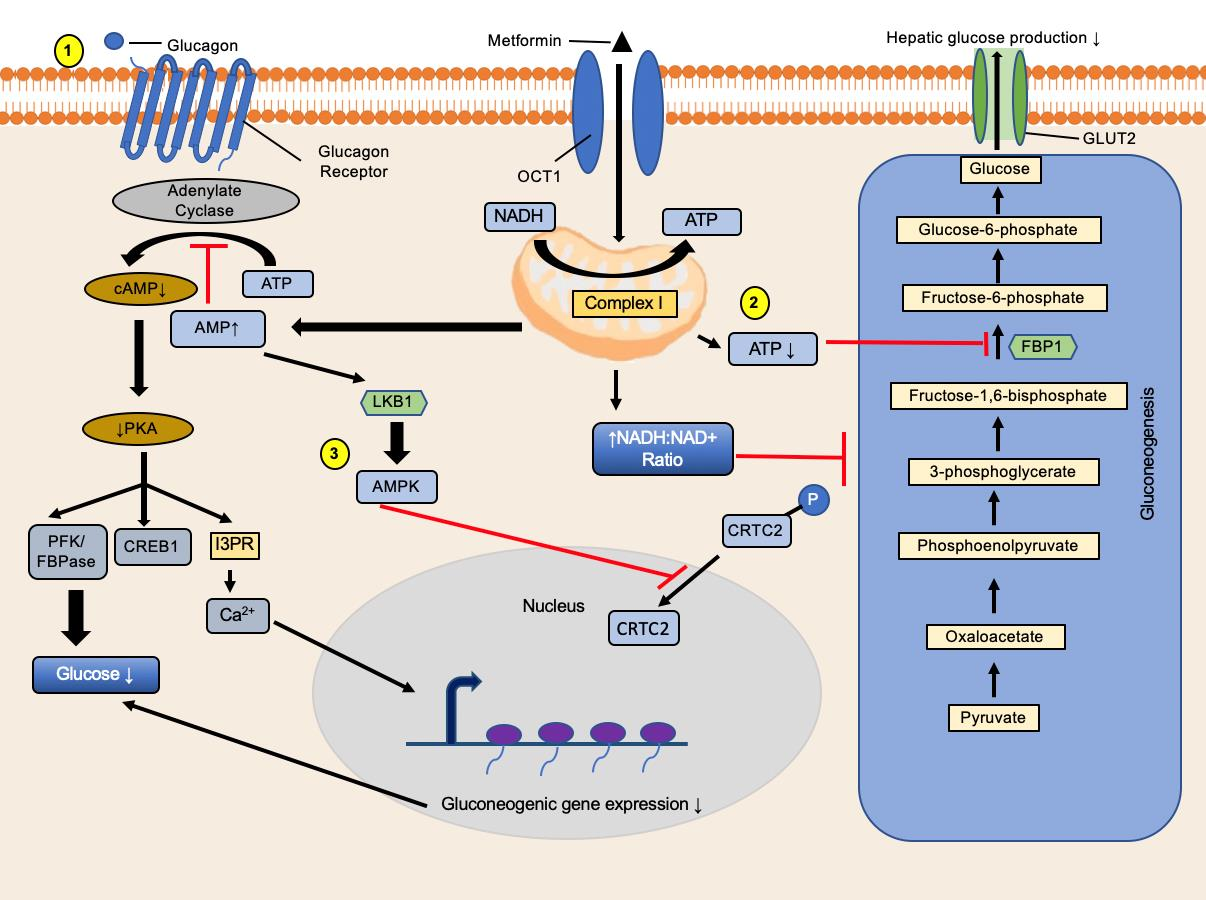
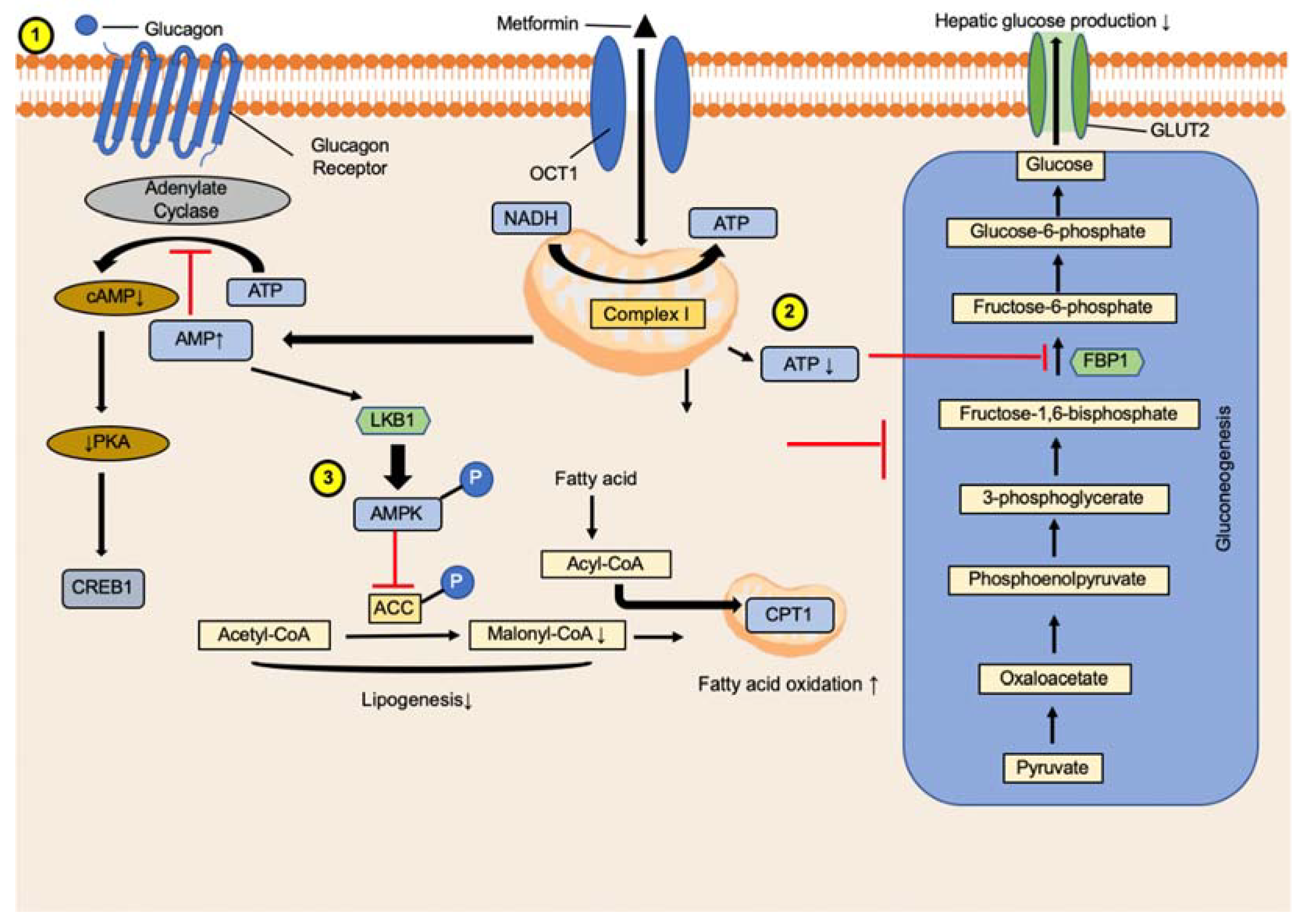
2. Metformin Mechanism of Action and Diabetes Mellitus
3. Clinical Use of Metformin
3.1. Metformin Use Reduces GC Risk in Patients with Diabetes
3.2. Metformin and GC Prevention
3.3. Metformin Use in GC Treatment
4. Repositioning (Repurposing) of Metformin for Cancer Inhibition
5. Metformin Use Alters Microbiota Composition
6. Metformin and Adverse Effects
7. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.S.; Badgwell, B.D. Current treatment and recent progress in gastric cancer. CA Cancer J. Clin. 2021, 71, 264–279. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.P.; El-Serag, H.B. Burden of gastric cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Sagaert, X.; Topal, B.; Haustermans, K.; Prenen, H. Gastric cancer. Lancet 2016, 388, 2654–2664. [Google Scholar] [CrossRef]
- Šterbenc, A.; Jarc, E.; Poljak, M.; Homan, M. Virulence genes. World J. Gastroenterol. 2019, 25, 4870–4884. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, S. Diabetes mellitus carries a risk of gastric cancer: A meta-analysis. World J. Gastroenterol. 2013, 19, 6902–6910. [Google Scholar] [CrossRef]
- Zhou, X.L.; Xue, W.H.; Ding, X.F.; Li, L.F.; Dou, M.M.; Zhang, W.J.; Lv, Z.; Fan, Z.R.; Zhao, J.; Wang, L.X. Association between metformin and the risk of gastric cancer in patients with type 2 diabetes mellitus: A meta-analysis of cohort studies. Oncotarget 2017, 8, 55622–55631. [Google Scholar] [CrossRef]
- Cheung, K.S.; Chan, E.W.; Chen, L.; Seto, W.K.; Wong, I.C.K.; Leung, W.K. Diabetes increases risk of gastric cancer after. Diabetes Care 2019, 42, 1769–1775. [Google Scholar] [CrossRef]
- Zhou, J.; Massey, S.; Story, D.; Li, L. Metformin: An old drug with new applications. Int. J. Mol. Sci. 2018, 19, 2863. [Google Scholar] [CrossRef]
- Lv, Z.; Guo, Y. Metformin and its benefits for various diseases. Front. Endocrinol. 2020, 11, 191. [Google Scholar] [CrossRef]
- Foretz, M.; Guigas, B.; Viollet, B. Understanding the glucoregulatory mechanisms of metformin in type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2019, 15, 569–589. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.A.; Chu, Q.; Xie, J.; Foretz, M.; Viollet, B.; Birnbaum, M.J. Biguanides suppress hepatic glucagon signalling by decreasing production of cyclic amp. Nature 2013, 494, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, E. Metformin-induced mitochondrial complex i inhibition: Facts, uncertainties, and consequences. Front. Endocrinol. 2018, 9, 753. [Google Scholar] [CrossRef] [PubMed]
- Oakhill, J.S.; Scott, J.W.; Kemp, B.E. Ampk functions as an adenylate charge-regulated protein kinase. Trends Endocrinol. Metab. 2012, 23, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.; Johnstone, S.R.; Dickerson, K.; Leiper, F.C.; Fryer, L.G.; Neumann, D.; Schlattner, U.; Wallimann, T.; Carlson, M.; Carling, D. Lkb1 is the upstream kinase in the amp-activated protein kinase cascade. Curr. Biol. 2003, 13, 2004–2008. [Google Scholar] [CrossRef]
- Shaw, R.J.; Lamia, K.A.; Vasquez, D.; Koo, S.H.; Bardeesy, N.; Depinho, R.A.; Montminy, M.; Cantley, L.C. The kinase lkb1 mediates glucose homeostasis in liver and therapeutic effects of metformin. Science 2005, 310, 1642–1646. [Google Scholar] [CrossRef]
- Foretz, M.; Hébrard, S.; Leclerc, J.; Zarrinpashneh, E.; Soty, M.; Mithieux, G.; Sakamoto, K.; Andreelli, F.; Viollet, B. Metformin inhibits hepatic gluconeogenesis in mice independently of the lkb1/ampk pathway via a decrease in hepatic energy state. J. Clin. Investig. 2010, 120, 2355–2369. [Google Scholar] [CrossRef]
- Zhou, G.; Myers, R.; Li, Y.; Chen, Y.; Shen, X.; Fenyk-Melody, J.; Wu, M.; Ventre, J.; Doebber, T.; Fujii, N.; et al. Role of amp-activated protein kinase in mechanism of metformin action. J. Clin. Investig. 2001, 108, 1167–1174. [Google Scholar] [CrossRef]
- Fullerton, M.D.; Galic, S.; Marcinko, K.; Sikkema, S.; Pulinilkunnil, T.; Chen, Z.P.; O’Neill, H.M.; Ford, R.J.; Palanivel, R.; O’Brien, M.; et al. Single phosphorylation sites in acc1 and acc2 regulate lipid homeostasis and the insulin-sensitizing effects of metformin. Nat. Med. 2013, 19, 1649–1654. [Google Scholar] [CrossRef]
- Wu, T.; Xie, C.; Wu, H.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Metformin reduces the rate of small intestinal glucose absorption in type 2 diabetes. Diabetes Obes. Metab. 2017, 19, 290–293. [Google Scholar] [CrossRef]
- McCreight, L.J.; Bailey, C.J.; Pearson, E.R. Metformin and the gastrointestinal tract. Diabetologia 2016, 59, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Koffert, J.P.; Mikkola, K.; Virtanen, K.A.; Andersson, A.D.; Faxius, L.; Hällsten, K.; Heglind, M.; Guiducci, L.; Pham, T.; Silvola, J.M.U.; et al. Metformin treatment significantly enhances intestinal glucose uptake in patients with type 2 diabetes: Results from a randomized clinical trial. Diabetes Res. Clin. Pract. 2017, 131, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Yi, F.; Sun, J.; Lim, G.E.; Fantus, I.G.; Brubaker, P.L.; Jin, T. Cross talk between the insulin and wnt signaling pathways: Evidence from intestinal endocrine l cells. Endocrinology 2008, 149, 2341–2351. [Google Scholar] [CrossRef] [PubMed]
- Beysen, C.; Murphy, E.J.; Deines, K.; Chan, M.; Tsang, E.; Glass, A.; Turner, S.M.; Protasio, J.; Riiff, T.; Hellerstein, M.K. Effect of bile acid sequestrants on glucose metabolism, hepatic de novo lipogenesis, and cholesterol and bile acid kinetics in type 2 diabetes: A randomised controlled study. Diabetologia 2012, 55, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Borg, M.J.; Bound, M.; Grivell, J.; Sun, Z.; Jones, K.L.; Horowitz, M.; Rayner, C.K.; Wu, T. Comparative effects of proximal and distal small intestinal administration of metformin on plasma glucose and glucagon-like peptide-1, and gastric emptying after oral glucose, in type 2 diabetes. Diabetes Obes. Metab. 2019, 21, 640–647. [Google Scholar] [CrossRef]
- Sansome, D.J.; Xie, C.; Veedfald, S.; Horowitz, M.; Rayner, C.K.; Wu, T. Mechanism of glucose-lowering by metformin in type 2 diabetes: Role of bile acids. Diabetes Obes. Metab. 2020, 22, 141–148. [Google Scholar] [CrossRef]
- Tseng, C.H. The relationship between diabetes mellitus and gastric cancer and the potential benefits of metformin: An extensive review of the literature. Biomolecules 2021, 11, 1022. [Google Scholar] [CrossRef]
- Tseng, C.-H.; Tseng, F.-H. Diabetes and gastric cancer: The potential links. World J. Gastroenterol. 2014, 20, 1701–1711. [Google Scholar] [CrossRef]
- Tseng, C.-H. Metformin reduces gastric cancer risk in patients with type 2 diabetes mellitus. Aging 2016, 8, 1636. [Google Scholar] [CrossRef]
- Kim, Y.I.; Kim, S.Y.; Cho, S.J.; Park, J.H.; Choi, I.J.; Lee, Y.J.; Lee, E.K.; Kook, M.C.; Kim, C.G.; Ryu, K.W.; et al. Long-term metformin use reduces gastric cancer risk in type 2 diabetics without insulin treatment: A nationwide cohort study. Aliment. Pharmacol. Ther. 2014, 39, 854–863. [Google Scholar] [CrossRef]
- Valent, F. Diabetes mellitus and cancer of the digestive organs: An italian population-based cohort study. J. Diabetes Complicat. 2015, 29, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-K.; Jung, M.; Jung, I.; Heo, S.J.; Jeong, Y.H.; An, J.Y.; Kim, H.-I.; Cheong, J.-H.; Hyung, W.J.; Noh, S.H.; et al. Cumulative metformin use and its impact on survival in gastric cancer patients after gastrectomy. Ann. Surg. 2016, 263, 96–102. [Google Scholar] [CrossRef]
- De Jong, R.G.; Burden, A.M.; de Kort, S.; van Herk-Sukel, M.P.; Vissers, P.A.; Janssen, P.K.; Haak, H.R.; Masclee, A.A.; de Vries, F.; Janssen-Heijnen, M.L. No decreased risk of gastrointestinal cancers in users of metformin in the netherlands; a time-varying analysis of metformin exposure. Cancer Prev. Res. 2017, 10, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.S.; Chan, E.W.; Wong, A.Y.S.; Chen, L.; Seto, W.K.; Wong, I.C.K.; Leung, W.K. Metformin use and gastric cancer risk in diabetic patients after helicobacter pylori eradication. J. Natl. Cancer Inst. 2018, 111, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, O.; Couttenier, A.; Vaes, E.; Cardwell, C.R.; De Schutter, H.; Robert, A. Impact of metformin on gastric adenocarcinoma survival: A belgian population based study. Cancer Epidemiol. 2018, 53, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Dulskas, A.; Patasius, A.; Linkeviciute-Ulinskiene, D.; Zabuliene, L.; Smailyte, G. A cohort study of antihyperglycemic medication exposure and survival in patients with gastric cancer. Aging 2019, 11, 7197–7205. [Google Scholar] [CrossRef]
- Zheng, J.; Xie, S.-H.; Santoni, G.; Lagergren, J. Metformin use and risk of gastric adenocarcinoma in a swedish population-based cohort study. Br. J. Cancer 2019, 121, 877–882. [Google Scholar] [CrossRef]
- Chung, W.-S.; Le, P.-H.; Kuo, C.-J.; Chen, T.-H.; Kuo, C.-F.; Chiou, M.-J.; Chou, W.-C.; Yeh, T.-S.; Hsu, J.-T. Impact of metformin use on survival in patients with gastric cancer and diabetes mellitus following gastrectomy. Cancers 2020, 12, 2013. [Google Scholar] [CrossRef]
- Cho, M.H.; Yoo, T.G.; Jeong, S.-M.; Shin, D.W. Association of aspirin, metformin, and statin use with gastric cancer incidence and mortality: A nationwide cohort study. Cancer Prev. Res. 2021, 14, 95–104. [Google Scholar] [CrossRef]
- MacArthur, T.A.; Harmsen, W.S.; Mandrekar, J.; Abraha, F.; Grotz, T.E. Association of common medications and the risk of early-onset gastric cancer: A population-based matched study. J. Cancer Epidemiol. 2021, 2021, 2670502. [Google Scholar] [CrossRef]
- McFarland, M.S.; Cripps, R. Diabetes mellitus and increased risk of cancer: Focus on metformin and the insulin analogs. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2010, 30, 1159–1178. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Chen, R.; Yu, J.; Li, N.; Ke, R.; Luo, L.; Zou, J.; Zhang, J.; Zhang, K.; Lu, N.; et al. Clinical significance and role of lkb1 in gastric cancer. Mol. Med. Rep. 2016, 13, 249–256. [Google Scholar] [CrossRef][Green Version]
- Kato, K.; Gong, J.; Iwama, H.; Kitanaka, A.; Tani, J.; Miyoshi, H.; Nomura, K.; Mimura, S.; Kobayashi, M.; Aritomo, Y.; et al. The antidiabetic drug metformin inhibits gastric cancer cell proliferation in vitro and in vivo. Mol. Cancer Ther. 2012, 11, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Han, G.; Gong, H.; Wang, Y.; Guo, S.; Liu, K. Ampk/mtor-mediated inhibition of survivin partly contributes to metformin-induced apoptosis in human gastric cancer cell. Cancer Biol. Ther. 2015, 16, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Ryan, B.M.; O’Donovan, N.; Duffy, M.J. Survivin: A new target for anti-cancer therapy. Cancer Treat. Rev. 2009, 35, 553–562. [Google Scholar] [CrossRef]
- Chang, H.R.; Nam, S.; Kook, M.C.; Kim, K.T.; Liu, X.; Yao, H.; Jung, H.R.; Lemos, R., Jr.; Seo, H.H.; Park, H.S.; et al. Hnf4α is a therapeutic target that links ampk to wnt signalling in early-stage gastric cancer. Gut 2016, 65, 19–32. [Google Scholar] [CrossRef]
- Salomon, D.S.; Brandt, R.; Ciardiello, F.; Normanno, N. Epidermal growth factor-related peptides and their receptors in human malignancies. Crit. Rev. Oncol. Hematol. 1995, 19, 183–232. [Google Scholar] [CrossRef]
- Chen, H.X.; Sharon, E. Igf-1r as an anti-cancer target--trials and tribulations. Chin. J. Cancer 2013, 32, 242–252. [Google Scholar] [CrossRef]
- Sarfstein, R.; Friedman, Y.; Attias-Geva, Z.; Fishman, A.; Bruchim, I.; Werner, H. Metformin downregulates the insulin/igf-i signaling pathway and inhibits different uterine serous carcinoma (usc) cells proliferation and migration in p53-dependent or -independent manners. PLoS ONE 2013, 8, e61537. [Google Scholar] [CrossRef]
- Gao, C.; Cai, S.; He, Y. Metformin plus tyrosine kinase inhibitors in epidermal growth factor receptor-mutated non-small cell lung cancer. JAMA Oncol. 2020, 6, 782. [Google Scholar] [CrossRef]
- Wang, W.M.; Yang, S.S.; Shao, S.H.; Nie, H.Q.; Zhang, J.; Su, T. Metformin downregulates the expression of epidermal growth factor receptor independent of lowering blood glucose in oral squamous cell carcinoma. Front. Endocrinol. 2022, 13, 828608. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Gong, W.; Zhou, Y.; Fan, R.; Wu, Y.; Pei, W.; Sun, S.; Xu, X.; Jiang, H. Metformin up-regulated mir-107 expression and enhanced the inhibitory effect of mir-107 on gastric cancer growth. Transl. Cancer Res. 2020, 9, 2941–2950. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Xiang, Y.; Li, T.; Huang, Y.; Wang, J.; Zhang, H.M.; Li, H.H.; Dai, Z.T.; Li, J.P.; Li, H.; et al. Metformin and mir-365 synergistically promote the apoptosis of gastric cancer cells via mir-365-pten-ampk axis. Pathol. Res. Pract. 2022, 230, 153740. [Google Scholar] [CrossRef] [PubMed]
- Chiurillo, M.A. Role of the wnt/β-catenin pathway in gastric cancer: An in-depth literature review. World J. Exp. Med. 2015, 5, 84–102. [Google Scholar] [CrossRef]
- Valaee, S.; Shamsara, M.; Yaghoobi, M.M. Metformin is a novel suppressor for vimentin in human gastric cancer cell line. Int. J. Mol. Cell. Med. 2021, 10, 200–206. [Google Scholar]
- Tseng, H.H.; Chen, Y.Z.; Chou, N.H.; Chen, Y.C.; Wu, C.C.; Liu, L.F.; Yang, Y.F.; Yeh, C.Y.; Kung, M.L.; Tu, Y.T.; et al. Metformin inhibits gastric cancer cell proliferation by regulation of a novel loc100506691-chac1 axis. Mol. Ther. Oncolytics 2021, 22, 180–194. [Google Scholar] [CrossRef]
- Zhou, J.; Zhi, X.; Wang, L.; Wang, W.; Li, Z.; Tang, J.; Wang, J.; Zhang, Q.; Xu, Z. Linc00152 promotes proliferation in gastric cancer through the egfr-dependent pathway. J. Exp. Clin. Cancer Res. 2015, 34, 135. [Google Scholar] [CrossRef]
- Courtois, S.; Durán, R.V.; Giraud, J.; Sifré, E.; Izotte, J.; Mégraud, F.; Lehours, P.; Varon, C.; Bessède, E. Metformin targets gastric cancer stem cells. Eur. J. Cancer 2017, 84, 193–201. [Google Scholar] [CrossRef]
- Zou, J.; Li, C.; Jiang, S.; Luo, L.; Yan, X.; Huang, D.; Luo, Z. Ampk inhibits smad3-mediated autoinduction of tgf-β1 in gastric cancer cells. J. Cell. Mol. Med. 2021, 25, 2806–2815. [Google Scholar] [CrossRef]
- Jauvain, M.; Courtois, S.; Lehours, P.; Bessède, E. Metformin modifies the gut microbiota of mice infected with. Pharmaceuticals 2021, 14, 329. [Google Scholar] [CrossRef]
- Jandhyala, S.M.; Talukdar, R.; Subramanyam, C.; Vuyyuru, H.; Sasikala, M.; Nageshwar Reddy, D. Role of the normal gut microbiota. World J. Gastroenterol. 2015, 21, 8787–8803. [Google Scholar] [CrossRef]
- Belcheva, A.; Irrazabal, T.; Robertson, S.J.; Streutker, C.; Maughan, H.; Rubino, S.; Moriyama, E.H.; Copeland, J.K.; Surendra, A.; Kumar, S. Gut microbial metabolism drives transformation of msh2-deficient colon epithelial cells. Cell 2014, 158, 288–299. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, J.; Xin, Y.; Geng, C.; Tian, Z.; Yu, X.; Dong, Q. Bacterial overgrowth and diversification of microbiota in gastric cancer. Eur. J. Gastroenterol. Hepatol. 2016, 28, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Vinasco, K.; Mitchell, H.M.; Kaakoush, N.O.; Castaño-Rodríguez, N. Microbial carcinogenesis: Lactic acid bacteria in gastric cancer. Biochim. Biophys. Acta Rev. Cancer 2019, 1872, 188309. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Esteve, E.; Tremaroli, V.; Khan, M.T.; Caesar, R.; Mannerås-Holm, L.; Ståhlman, M.; Olsson, L.M.; Serino, M.; Planas-Fèlix, M.; et al. Metformin alters the gut microbiome of individuals with treatment-naive type 2 diabetes, contributing to the therapeutic effects of the drug. Nat. Med. 2017, 23, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Hong, X.; Wang, J.; Sun, T.; Yu, T.; Yu, Y.; Fang, J.; Xiong, H. Metformin elicits antitumour effect by modulation of the gut microbiota and rescues fusobacterium nucleatum-induced colorectal tumourigenesis. eBioMedicine 2020, 61, 103037. [Google Scholar] [CrossRef]
- Zhou, Q.; Zhang, Y.; Wang, X.; Yang, R.; Zhu, X.; Chen, C.; Yuan, H.; Yang, Z.; Sun, L. Gut bacteria. Nutr. Metab. 2020, 17, 90. [Google Scholar] [CrossRef]
- Bahmani, S.; Azarpira, N.; Moazamian, E. Anti-colon cancer activity of bifidobacterium metabolites on colon cancer cell line sw742. Turk. J. Gastroenterol. 2019, 30, 835–842. [Google Scholar] [CrossRef]
- Yang, J.; Zhou, X.; Liu, X.; Ling, Z.; Ji, F. Role of the gastric microbiome in gastric cancer: From carcinogenesis to treatment. Front. Microbiol. 2021, 12, 641322. [Google Scholar] [CrossRef]
- Forslund, K.; Hildebrand, F.; Nielsen, T.; Falony, G.; Le Chatelier, E.; Sunagawa, S.; Prifti, E.; Vieira-Silva, S.; Gudmundsdottir, V.; Krogh Pedersen, H. Disentangling type 2 diabetes and metformin treatment signatures in the human gut microbiota. Nature 2015, 528, 262–266. [Google Scholar] [CrossRef]
- Aroda, V.R.; Edelstein, S.L.; Goldberg, R.B.; Knowler, W.C.; Marcovina, S.M.; Orchard, T.J.; Bray, G.A.; Schade, D.S.; Temprosa, M.G.; White, N.H. Long-term metformin use and vitamin b12 deficiency in the diabetes prevention program outcomes study. J. Clin. Endocrinol. Metab. 2016, 101, 1754–1761. [Google Scholar] [CrossRef] [PubMed]
- Al-Abri, S.; Hayashi, S.; Thoren, K.; Olson, K. Metformin overdose-induced hypoglycemia in the absence of other antidiabetic drugs. Clin. Toxicol. 2013, 51, 444–447. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.; Fleming, G.A.; Chen, K.; Bicsak, T.A. Metformin-associated lactic acidosis: Current perspectives on causes and risk. Metabolism 2016, 65, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Pasquel, F.J.; Hinedi, Z.; Umpierrez, G.E.; Klein, R.; Adigweme, A.; Coralli, R.; Pimentel, J.L.; Lopez, F.A. Metformin-associated lactic acidosis. Am. J. Med. Sci. 2015, 349, 263–267. [Google Scholar] [CrossRef]
- Miralles-Linares, F.; Puerta-Fernandez, S.; Bernal-Lopez, M.R.; Tinahones, F.J.; Andrade, R.J.; Gomez-Huelgas, R. Metformin-induced hepatotoxicity. Diabetes Care 2012, 35, e21. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author and Study Year | Study Location | Effect of Statins on GC | Joint Effect of Other Drugs | Presence of H. pylori | Reference |
|---|---|---|---|---|---|
| Kim, 2014 | Korea | Metformin use for >3 years was associated with a significant 43% reduction in GC risk among those who did not use insulin | GC risk might be doubled in insulin users while compared to nonuser, disregarding metformin use | NA † | [30] |
| Valent, 2015 | Italy | Metformin prescription reduced risk of most types of digestive cancer | NA | - ‡ | [31] |
| Lee, 2016 | Korea | Metformin use for more than 6 months decreases recurrence, cancer-specific mortality, and all-cause mortality in diabetic patients with gastrectomy | NA | NA | [32] |
| Tseng, 2016 | Taiwan | Metformin significantly reduces GC risk, especially for patients prescribed more than 2 years | Independent of insulin, sulfonylurea, meglitinide, acarbose, rosiglitazone, pioglitazone, and statin | +/− ¶ | [29] |
| de Jong, 2017 | Netherlands | No significant difference between metformin users and other NIADs users | NA | - | [33] |
| Cheung, 2018 | Hong Kong | In H. pylori-eradicated patients, metformin use exhibited a 51% reduction in GC risk, and associated with dose- and duration-gradients | Independent with glycemic control | - | [34] |
| Lacroix, 2018 | Belgium | Metformin use reduces all-cause mortality but not for cancer-specific mortality | NA | NA | [35] |
| Dulskas, 2019 | Lithuania | No significant effect on survival in patients prescribed metformin | Insulin | NA | [36] |
| Zheng, 2019 | Sweden | Metformin use does not reduce GC risk in both diabetic population and common-medication population | No significant difference in combination of other anti-diabetic drugs | - | [37] |
| Chung, 2020 | Taiwan | Metformin prolonged cancer-specific survival in GC stage III patients | NA | NA | [38] |
| Cho, 2021 | Korea | Metformin reduced mortality among diabetic and nondiabetic populations with use for ≥547.5 cDDD-days | Aspirin and statin | NA | [39] |
| MacArthur, 2021 | Olmsted County, Minnesota | No protective effect of metformin against early onset GC | NA | +/− | [40] |
| Author and Study Year | Experiment | Target or Mechanism | Reference |
|---|---|---|---|
| Ryan, 2009 | Review strategies to target survivin in cancer cells | Survivin is one of the most cancer-specified proteins and is upregulated in nearly all human tumors | [45] |
| Kato, 2012 | Dose–response of metformin vs. viability and cyclins in MKN1, MKN45, and MKN74 human GC cell lines and tumor growth of inoculated GC cell line in nude mice | Metformin decreases the expression of cyclins thus can inhibit tumor growth by arresting G1 cell-cycle in vivo | [43] |
| Zhou, 2015 | Linc00152 expression and interaction protein identification | Linc00152 promotes proliferation in GC through the EGFR-dependent pathway | [57] |
| Chang, 2016 | Integrative analysis of transcriptomic profiles of tumors and their matched noncancerous samples. The candidate genes were validated by inhibition using RNA interference | AMPKα downregulates HNF4α, resulting in cyclin downregulation, cell cycle arrest, and tumor growth inhibition | [46] |
| Courtois, 2017 | Study the metformin effects on proliferation and tumorigenic properties of primary cell culture from patients and established GC cell lines | Metformin leads to tumor growth delay and decreases cancer stem cell’s renewal ability | [58] |
| Chen, 2020 | Identify potential metformin targets in cancer cells using bioinformatics analysis. Validate targets using miR-107 mimic and metformin treatment | Metformin increases miR-107 expression in the SGC-7901 GC cell line. MiR-107 inhibits tumor growth and invasion, inducing apoptosis and is related to cell-cycle arrest | [52] |
| Tseng, 2021 | Identify metformin targets using microarray data by treating several metformin concentrations. Validate the target genes using gene knockdown experiment | GC cells treated with metformin can decrease the oncogenic long noncoding RNA Loc100506691, while high Loc100506691 expression level is correlated with poor GC patient survival | [56] |
| Valaee, 2021 | Study metformin concentration vs. vimentin expression level in AGS cells. Assess vimentin function by siRNA (vim-siRNA) knockdown method | Vimentin is related to cancer metastasis and upregulated in epithelial-mesenchymal transition. Suppression of vimentin expression may have a beneficial effect on cancer survival. Metformin can be used to suppress vimentin expression | [55] |
| Zou, 2021 | Investigate TGF-β1 expression level and reporter gene activity vs. metformin treatment. The roles of Smad3 were determined by gene knockdown and deleting Smad3 binding sites in the TGF-β1 promoter region | AMPK suppression of TGF-β1 autoinduction is mediated through the inhibition of Smad3 phosphorylation and activation | [59] |
| Huang, 2022 | Assess apoptosis of GC cells and AMPK activity by metformin treatment. Analysis of metformin and miR-365, individually and combined, on the apoptosis of GC cells and the miR-365-PTEN-AMPK axis activity | Metformin can cooperate with miR-365 to promote GC cell apoptosis via the miR-365-PTEN-AMPK axis | [53] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lan, W.-H.; Lin, T.-Y.; Yeh, J.-A.; Feng, C.-L.; Hsu, J.-T.; Lin, H.-J.; Kuo, C.-J.; Lai, C.-H. Mechanism Underlying Metformin Action and Its Potential to Reduce Gastric Cancer Risk. Int. J. Mol. Sci. 2022, 23, 14163. https://doi.org/10.3390/ijms232214163
Lan W-H, Lin T-Y, Yeh J-A, Feng C-L, Hsu J-T, Lin H-J, Kuo C-J, Lai C-H. Mechanism Underlying Metformin Action and Its Potential to Reduce Gastric Cancer Risk. International Journal of Molecular Sciences. 2022; 23(22):14163. https://doi.org/10.3390/ijms232214163
Chicago/Turabian StyleLan, Wen-Hsi, Ting-Yu Lin, Jia-Ai Yeh, Chun-Lung Feng, Jun-Te Hsu, Hwai-Jeng Lin, Chia-Jung Kuo, and Chih-Ho Lai. 2022. "Mechanism Underlying Metformin Action and Its Potential to Reduce Gastric Cancer Risk" International Journal of Molecular Sciences 23, no. 22: 14163. https://doi.org/10.3390/ijms232214163
APA StyleLan, W.-H., Lin, T.-Y., Yeh, J.-A., Feng, C.-L., Hsu, J.-T., Lin, H.-J., Kuo, C.-J., & Lai, C.-H. (2022). Mechanism Underlying Metformin Action and Its Potential to Reduce Gastric Cancer Risk. International Journal of Molecular Sciences, 23(22), 14163. https://doi.org/10.3390/ijms232214163