
Addition of Synthetic Biomaterials to Deproteinized Bovine Bone Mineral (DBBM) for Bone Augmentation—A Preclinical In Vivo Study
 , , and
, , and
Abstract
:1. Introduction
2. Results
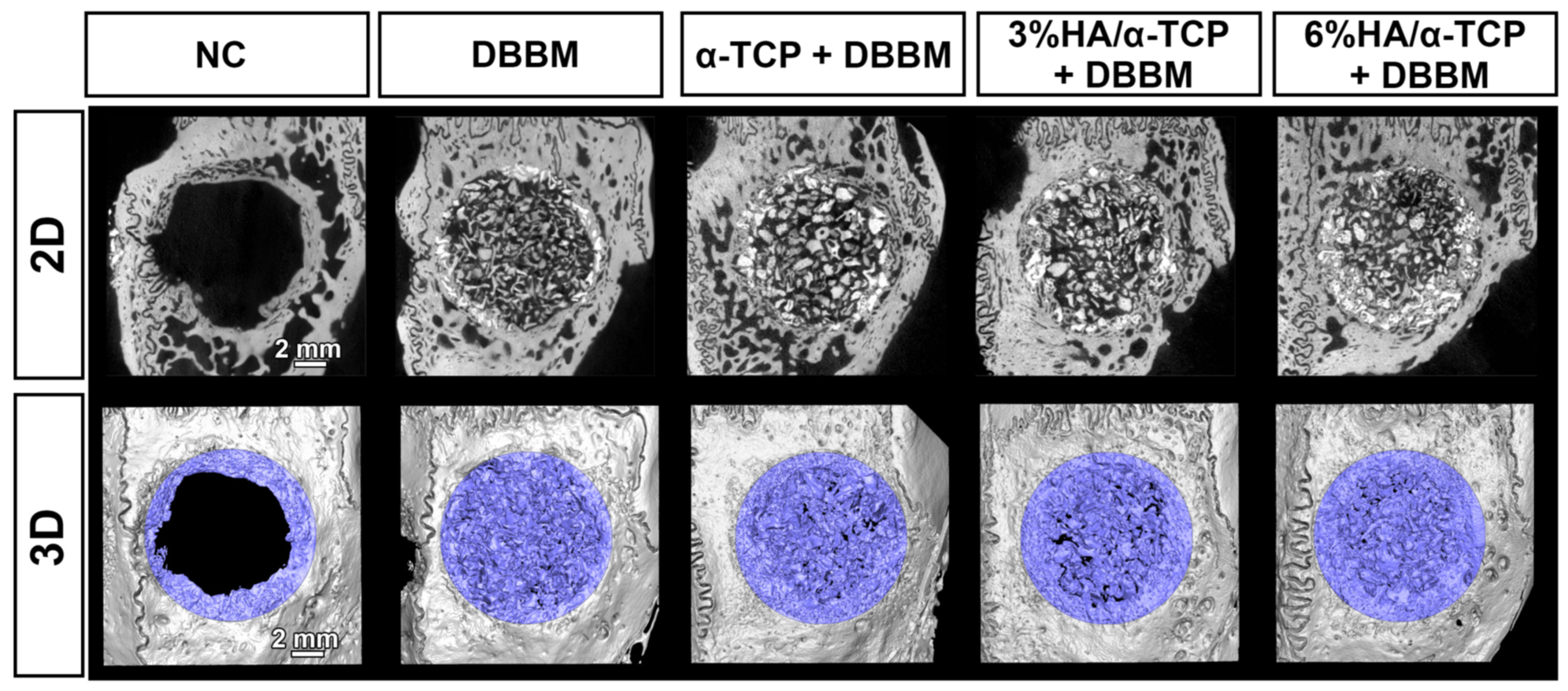
2.1. Micro-CT Analysis in Whole Defects
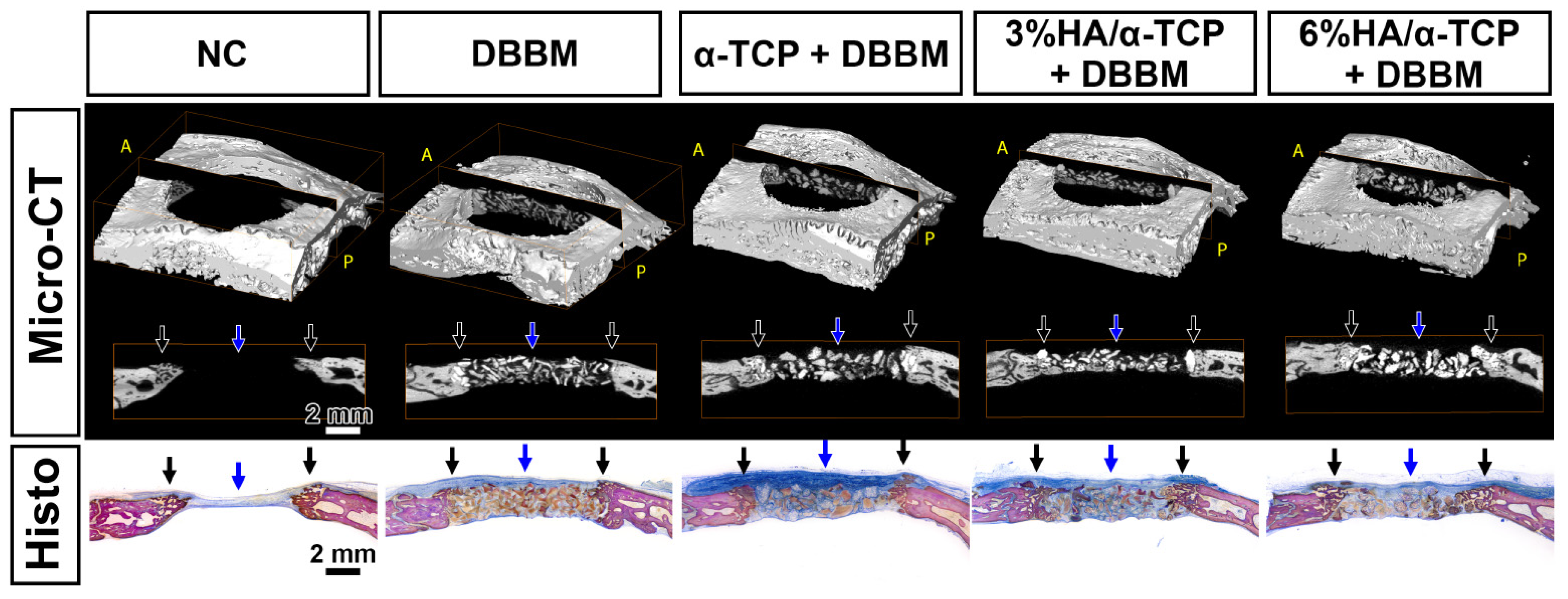
2.2. Histological Analysis
2.3. Material Resorption Assay by Micro-CT Analysis in the Central Area of the Defects
3. Discussion
4. Materials & Methods
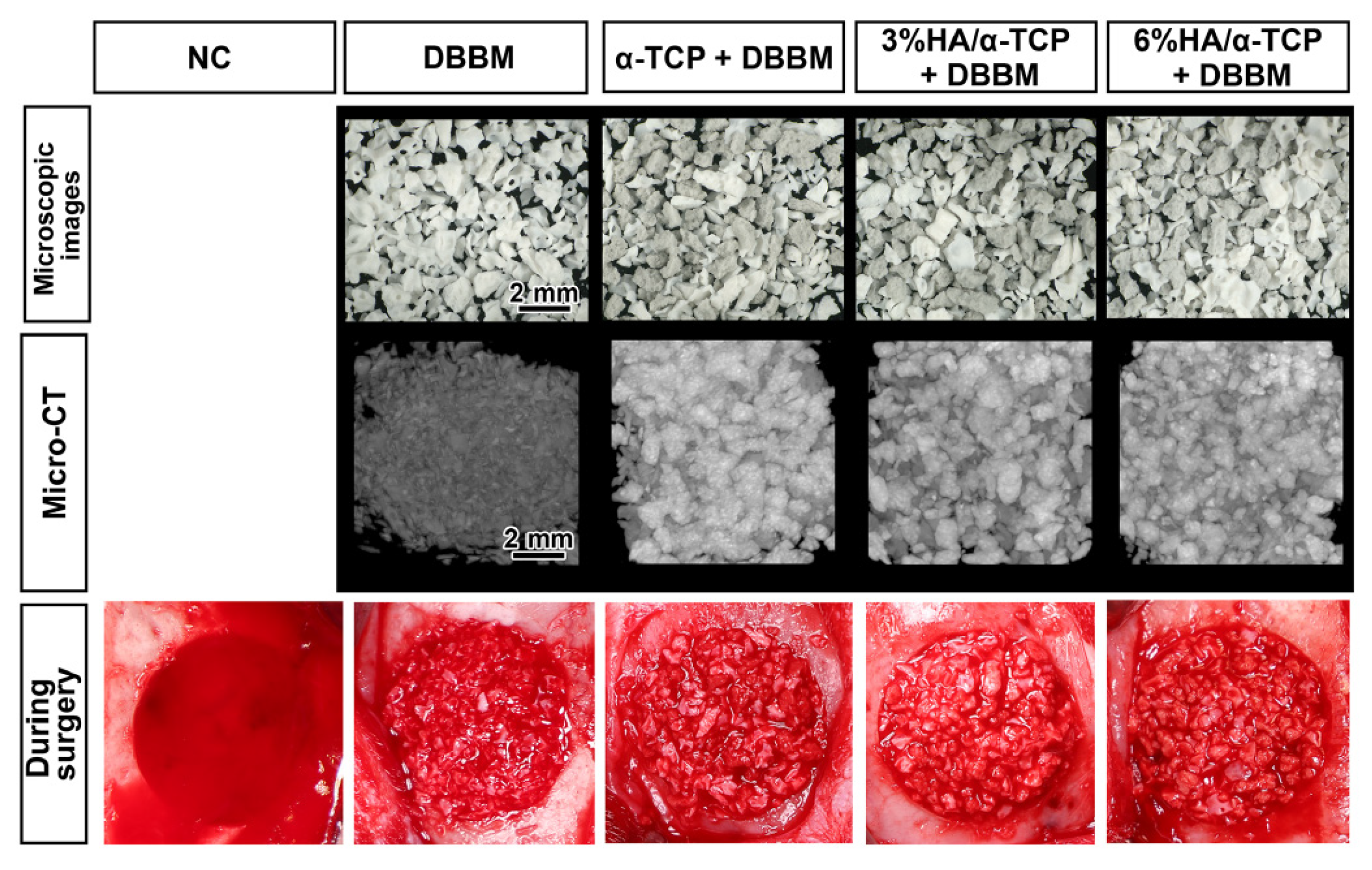
4.1. Materials
4.2. Animals
4.3. Anesthesia
4.4. Surgical Procedures
4.5. Postoperative Procedures
4.6. Micro-CT Analysis
4.7. Histological Processing and Histomorphometric Analysis
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bornstein, M.M.; Halbritter, S.; Harnisch, H.; Weber, H.P.; Buser, D. A retrospective analysis of patients referred for implant placement to a specialty clinic: Indications, surgical procedures, and early failures. Int. J. Oral Maxillofac. Implant. 2008, 23, 1109–1116. [Google Scholar]
- Lang, N.P.; Hämmerle, C.H.; Brägger, U.; Lehmann, B.; Nyman, S.R. Guided tissue regeneration in jawbone defects prior to implant placement. Clin. Oral Implant. Res. 1994, 5, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Chappuis, V.; Kuchler, U.; Bornstein, M.M.; Wittneben, J.G.; Buser, R.; Cavusoglu, Y.; Belser, U.C. Long-term stability of early implant placement with contour augmentation. J. Dent. Res. 2013, 92 (Suppl. 12), 176s–182s. [Google Scholar] [CrossRef] [PubMed]
- Moy, P.; Palacci, P. Minor bone augmentation procedures. In Esthetic Implant Dentistry Soft and Hard Tissue Management; Quintessence: Chicago, IL, USA, 2001; pp. 137–158. [Google Scholar]
- Nkenke, E.; Stelzle, F. Clinical outcomes of sinus floor augmentation for implant placement using autogenous bone or bone substitutes: A systematic review. Clin. Oral Implant. Res. 2009, 20, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Fenner, N.; Hämmerle, C.H.; Zitzmann, N.U. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12–14 years. Clin. Oral Implant. Res. 2013, 24, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Chappuis, V.; Bornstein, M.M.; Wittneben, J.G.; Frei, M.; Belser, U.C. Long-term stability of contour augmentation with early implant placement following single tooth extraction in the esthetic zone: A prospective, cross-sectional study in 41 patients with a 5- to 9-year follow-up. J. Periodontol. 2013, 84, 1517–1527. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, M.; Henriques, J.; Martins, G.; Guerra, F.; Judas, F.; Figueiredo, H. Physicochemical characterization of biomaterials commonly used in dentistry as bone substitutes—Comparison with human bone. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 92, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Titsinides, S.; Agrogiannis, G.; Karatzas, T. Bone grafting materials in dentoalveolar reconstruction: A comprehensive review. Jpn. Dent. Sci. Rev. 2019, 55, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Testori, T.; Weinstein, T.; Scutellà, F.; Wang, H.L.; Zucchelli, G. Implant placement in the esthetic area: Criteria for positioning single and multiple implants. Periodontology 2018, 77, 176–196. [Google Scholar] [CrossRef] [PubMed]
- Broggini, N.; Bosshardt, D.D.; Jensen, S.S.; Bornstein, M.M.; Wang, C.C.; Buser, D. Bone healing around nanocrystalline hydroxyapatite, deproteinized bovine bone mineral, biphasic calcium phosphate, and autogenous bone in mandibular bone defects. J. Biomed. Mater. Res. Part B Appl. Biomater. 2015, 103, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Passi, D.; Singh, P.; Bhuibhar, A. Ceramic and non-ceramic hydroxyapatite as a bone graft material: A brief review. Ir. J. Med. Sci. 2015, 184, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Saulacic, N.; Fujioka-Kobayashi, M.; Kimura, Y.; Bracher, A.I.; Zihlmann, C.; Lang, N.P. The effect of synthetic bone graft substitutes on bone formation in rabbit calvarial defects. J. Mater. Sci. Mater. Med. 2021, 32, 14. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Naef, R.; Schärer, P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration. Int. J. Oral Maxillofac. Implant. 1997, 12, 220–238. [Google Scholar]
- Baldini, N.; De Sanctis, M.; Ferrari, M. Deproteinized bovine bone in periodontal and implant surgery. Dent. Mater. 2011, 27, 61–70. [Google Scholar] [CrossRef] [PubMed]
- De Santis, E.; Lang, N.P.; Ferreira, S.; Rangel Garcia, I., Jr.; Caneva, M.; Botticelli, D. Healing at implants installed concurrently to maxillary sinus floor elevation with Bio-Oss(®) or autologous bone grafts. A histo-morphometric study in rabbits. Clin. Oral Implant. Res. 2017, 28, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.S.; Gruber, R.; Buser, D.; Bosshardt, D.D. Osteoclast-like cells on deproteinized bovine bone mineral and biphasic calcium phosphate: Light and transmission electron microscopical observations. Clin. Oral Implant. Res. 2015, 26, 859–864. [Google Scholar] [CrossRef] [PubMed]
- Kunert-Keil, C.; Scholz, F.; Gedrange, T.; Gredes, T. Comparative study of biphasic calcium phosphate with beta-tricalcium phosphate in rat cranial defects—A molecular-biological and histological study. Ann. Anat. Anat. Anz. 2015, 199, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Titsinides, S.; Karatzas, T.; Perrea, D.; Eleftheriadis, E.; Podaropoulos, L.; Kalyvas, D.; Katopodis, C.; Agrogiannis, G. Osseous healing in surgically prepared bone defects using different grafting materials: An experimental study in pigs. Dent. J. 2020, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- Schmid, J.; Hämmerle, C.; Olah, A.; Lang, N. Membrane permeability is unnecessary for guided generation of new bone. An experimental study in the rabbit. Clin. Oral Implant. Res. 1994, 5, 125–130. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Reference |
|---|---|---|---|---|---|---|
| NC (n = 6) | DBBM (n = 6) | α-TCP + DBBM (n = 6) | 3%HA/ α-TCP + DBBM (n = 6) | 6%HA/ α-TCP + DBBM (n = 5) | Intact Bone (n = 8) | |
| MV (mm3) | 25.43 ± 7.73 | 59.31 ± 11.42 | 68.93 ± 16.17 | 64.30 ± 17.83 | 71.30 ± 9.62 | 71.53 ± 8.59 |
| vs. NC ** | vs. NC # | vs. NC # | vs. NC # | |||
| MV/TV (%) | 11.50 ± 1.71 | 29.06 ± 3.51 | 32.18 ± 6.43 | 29.83 ± 7.57 | 31.28 ± 2.88 | 35.94 ± 7.64 |
| vs. NC # | vs. NC # | vs. NC # | vs. NC # | |||
| MD (mgHA/ccm) | 611.74 ± 18.66 | 689.05 ± 17.95 | 728.08 ± 27.65 | 716.13 ± 22.54 | 724.69 ± 18.26 | 680.37 ± 13.48 |
| vs. NC # | vs. NC # | vs. NC # | vs. NC # | |||
| vs. DBBM * | ||||||
| HDC (%) | 48.40 ± 27.37 | 25.80 ± 9.85 | 33.48 ± 5.83 | 32.33 ± 11.98 | 39.66 ± 7.24 |
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Reference |
|---|---|---|---|---|---|---|
| NC (n = 6) | DBBM (n = 6) | α-TCP + DBBM (n = 6) | 3%HA/ α-TCP + DBBM (n = 6) | 6%HA/ α-TCP + DBBM (n = 5) | Intact Bone (n = 8) | |
| NBA (%) | 18.82 ± 5.36 | 8.94 ± 3.38 | 12.74 ± 4.76 | 13.25 ± 7.77 | 13.62 ± 3.41 | 52.35 ± 6.32 |
| vs. NC * | ||||||
| BMA (%) | 3.99 ± 1.51 | 1.72 ± 1.08 | 2.91 ± 1.77 | 2.37 ± 2.16 | 3.36 ± 0.67 | 38.02 ± 7.64 |
| CTA (%) | 77.19 ± 6.78 | 63.66 ± 3.90 | 60.97 ± 3.63 | 62.33 ± 7.21 | 59.53 ± 3.16 | 9.63 ± 2.59 |
| RMA (%) | 25.68 ± 2.38 | 23.38 ± 3.50 | 22.05 ± 4.58 | 23.49 ± 5.98 | ||
| RMA-D (%) | 25.68 ± 2.38 | 16.15 ± 2.27 | 18.26 ± 4.46 | 18.25 ± 4.55 | ||
| vs. DBBM # | vs. DBBM ** | vs. DBBM * | ||||
| RMA-S (%) | 7.22 ± 2.41 | 3.79 ± 1.71 | 5.24 ± 3.26 | |||
| HDC (%) | 52.66 ± 27.30 | 31.85 ± 13.66 | 51.19 ± 30.99 | 54.14 ± 21.14 | 51.62 ± 20.64 |
| Parameter (Central 5 mm) | Group 2 | Group 3 | Group 4 | Group 5 |
|---|---|---|---|---|
| DBBM (n = 6) | α-TCP + DBBM (n = 6) | 3%HA/ α-TCP + DBBM (n = 6) | 6%HA/ α-TCP + DBBM (n = 5) | |
| MV (mm3) | 9.55 ± 3.25 | 12.77 ± 4.94 | 10.27 ± 3.21 | 11.04 ± 3.08 |
| MV/TV (%) | 18.57 ± 4.47 | 24.03 ± 9.36 | 18.93 ± 5.25 | 19.34 ± 4.99 |
| vs. DBBM # | vs. DBBM # | vs. DBBM # | ||
| MD (mgHA/ccm) | 666.13 ± 21.76 | 735.48 ± 47.90 | 722.77 ± 26.96 | 748.83 ± 23.59 |
| vs. DBBM ** | vs. DBBM * | vs. DBBM ** |
| Parameter (Peripheral 2.5-mm) | Group 2 | Group 3 | Group 4 | Group 5 |
|---|---|---|---|---|
| DBBM (n = 6) | α-TCP + DBBM (n = 6) | 3%HA/ α-TCP + DBBM (n = 6) | 6%HA/ α-TCP + DBBM (n = 5) | |
| MV (mm3) | 49.76 ± 9.31 | 56.16 ± 13.69 | 54.03 ± 14.98 | 60.26 ± 6.91 |
| MV/TV (%) | 32.56 ± 4.35 | 34.90 ± 7.06 | 33.46 ± 8.59 | 35.26 ± 2.21 |
| MD (mgHA/ccm) | 692.76 ± 18.94 | 724.74 ± 23.15 | 711.32 ± 23.31 | 720.29 ± 17.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujioka-Kobayashi, M.; Katagiri, H.; Lang, N.P.; Imber, J.-C.; Schaller, B.; Saulacic, N. Addition of Synthetic Biomaterials to Deproteinized Bovine Bone Mineral (DBBM) for Bone Augmentation—A Preclinical In Vivo Study. Int. J. Mol. Sci. 2022, 23, 10516. https://doi.org/10.3390/ijms231810516
Fujioka-Kobayashi M, Katagiri H, Lang NP, Imber J-C, Schaller B, Saulacic N. Addition of Synthetic Biomaterials to Deproteinized Bovine Bone Mineral (DBBM) for Bone Augmentation—A Preclinical In Vivo Study. International Journal of Molecular Sciences. 2022; 23(18):10516. https://doi.org/10.3390/ijms231810516
Chicago/Turabian StyleFujioka-Kobayashi, Masako, Hiroki Katagiri, Niklaus P. Lang, Jean-Claude Imber, Benoit Schaller, and Nikola Saulacic. 2022. "Addition of Synthetic Biomaterials to Deproteinized Bovine Bone Mineral (DBBM) for Bone Augmentation—A Preclinical In Vivo Study" International Journal of Molecular Sciences 23, no. 18: 10516. https://doi.org/10.3390/ijms231810516
APA StyleFujioka-Kobayashi, M., Katagiri, H., Lang, N. P., Imber, J.-C., Schaller, B., & Saulacic, N. (2022). Addition of Synthetic Biomaterials to Deproteinized Bovine Bone Mineral (DBBM) for Bone Augmentation—A Preclinical In Vivo Study. International Journal of Molecular Sciences, 23(18), 10516. https://doi.org/10.3390/ijms231810516