
Systemic and Renal Dynamics of Free Sulfhydryl Groups during Living Donor Kidney Transplantation
 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
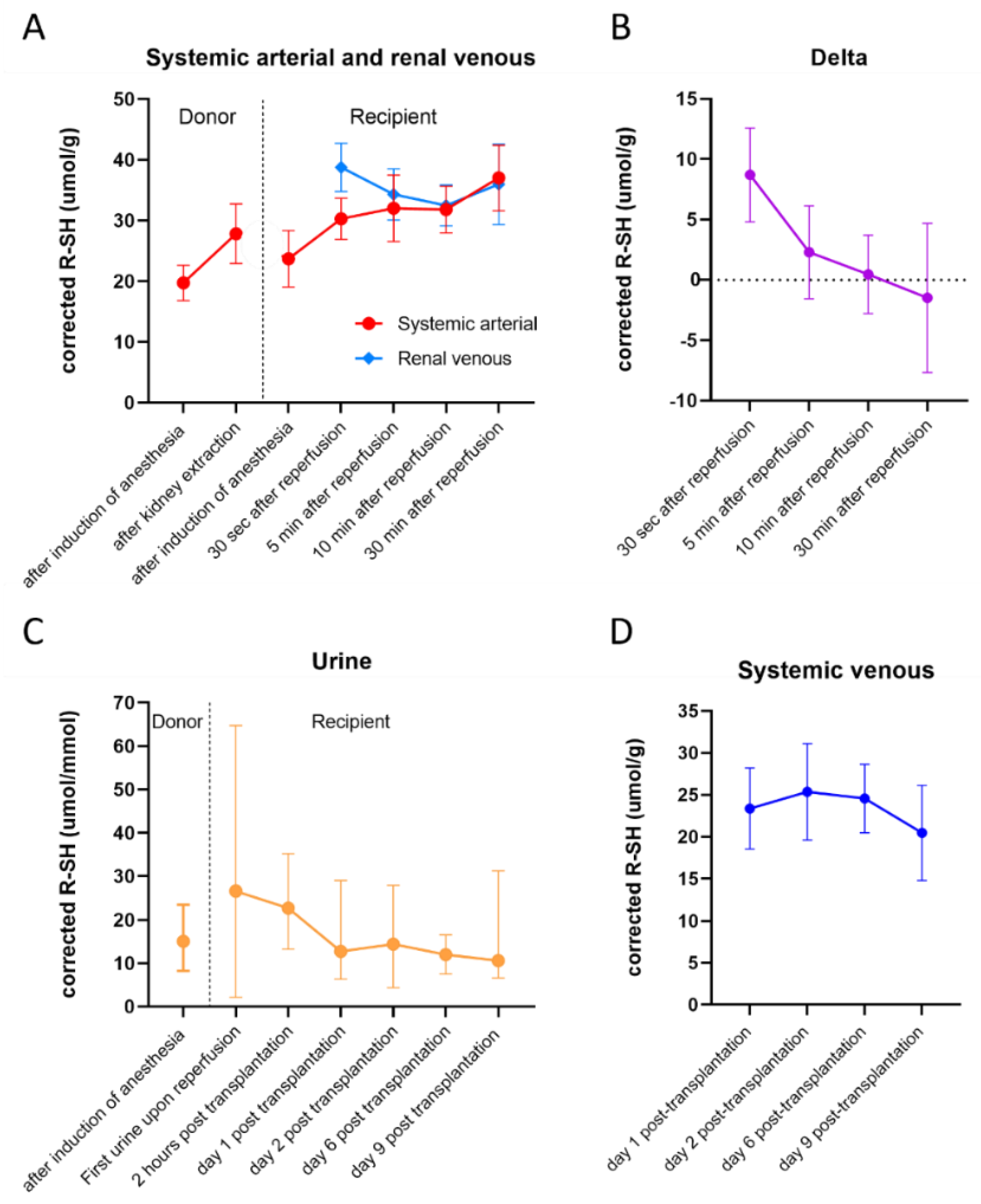
2.2. Plasma R-SH in Different Sample Types
3. Discussion
4. Materials and Methods
4.1. The Study Design and Population
4.2. Clinical Parameters
4.3. Sample Points and Sample Measurements
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Irish, W.D.; Ilsley, J.N.; Schnitzler, M.A.; Feng, S.; Brennan, D.C. A Risk Prediction Model for Delayed Graft Function in the Current Era of Deceased Donor Renal Transplantation. Am. J. Transplant. 2010, 10, 2279–2286. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.S.; Schaubel, D.E.; Guidinger, M.K.; Andreoni, K.A.; Wolfe, R.A.; Merion, R.M.; Port, F.K.; Sung, R.S. A Comprehensive Risk Quantification Score for Deceased Donor Kidneys: The Kidney Donor Risk Index. Transplantation 2009, 88, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Salvadori, M.; Rosso, G.; Bertoni, E. Update on ischemia-reperfusion injury in kidney transplantation: Pathogenesis and treatment. World J. Transplant. 2015, 5, 52–67. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C. Ischaemia-reperfusion injury: A major protagonist in kidney transplantation. Nephrol. Dial. Transpl. 2013, 29, 1134–1140. [Google Scholar] [CrossRef]
- Nieuwenhuijs-Moeke, G.J.; Pischke, S.E.; Berger, S.P.; Sanders, J.S.F.; Pol, R.A.; Struys, M.M.R.F.; Ploeg, R.J.; Leuvenink, H.G.D. Ischemia and Reperfusion Injury in Kidney Transplantation: Relevant Mechanisms in Injury and Repair. J. Clin. Med. 2020, 9, 253. [Google Scholar] [CrossRef]
- Cooper, J.E.; Wiseman, A.C. Acute kidney injury in kidney transplantation. Curr. Opin. Nephrol. Hypertens. 2013, 22, 698–703. [Google Scholar] [CrossRef]
- Cosio, F.G.; Grande, J.P.; Larson, T.S.; Gloor, J.M.; Velosa, J.A.; Textor, S.C.; Griffin, M.D.; Stegall, M.D. Kidney allograft fibrosis and atrophy early after living donor transplantation. Am. J. Transplant 2005, 5, 1130–1136. [Google Scholar] [CrossRef]
- Chouchani, E.T.; Pell, V.R.; Gaude, E.; Aksentijević, D.; Sundier, S.Y.; Robb, E.L.; Logan, A.; Nadtochiy, S.M.; Ord, E.N.J.; Smith, A.C.; et al. Ischaemic accumulation of succinate controls reperfusion injury through mitochondrial ROS. Nature 2014, 515, 431–435. [Google Scholar] [CrossRef]
- Peng, T.-I.; Jou, M.-J. Oxidative stress caused by mitochondrial calcium overload. Ann. N. Y. Acad. Sci. 2010, 1201, 183–188. [Google Scholar] [CrossRef]
- Granger, D.N.; Kvietys, P.R. Reperfusion injury and reactive oxygen species: The evolution of a concept. Redox Biol. 2015, 6, 524–551. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.L.; Gruszyck, A.V.; Beach, T.E.; Murphy, M.P.; Saeb-Parsy, K. Mitochondrial mechanisms and therapeutics in ischaemia reperfusion injury. Pediatr. Nephrol. 2019, 34, 1167–1174. [Google Scholar] [CrossRef]
- Mills, E.L.; Kelly, B.; O’Neill, L.A.J. Mitochondria are the powerhouses of immunity. Nat. Immunol. 2017, 18, 488–498. [Google Scholar] [CrossRef]
- Tirichen, H.; Yaigoub, H.; Xu, W.; Wu, C.; Li, R.; Li, Y. Mitochondrial Reactive Oxygen Species and Their Contribution in Chronic Kidney Disease Progression Through Oxidative Stress. Front. Physiol. 2021, 12, 627837. [Google Scholar] [CrossRef]
- Jones, D.P.; Sies, H. The Redox Code. Antioxid. Redox Signal. 2015, 23, 734–746. [Google Scholar] [CrossRef]
- Cooper, C.; Patel, R.P.; Brookes, P.S.; Darley-Usmar, V.M. Nanotransducers in cellular redox signaling: Modification of thiols by reactive oxygen and nitrogen species. Trends Biochem. Sci. 2002, 27, 489–492. [Google Scholar] [CrossRef]
- Himmelfarb, J.; McMonagle, E.; Freedman, S.; Klenzak, J.; McMenamin, E.; Ellen, M.; Pupim, L.B.; Ikizler, T. The PICARD Group Oxidative Stress Is Increased in Critically Ill Patients with Acute Renal Failure. J. Am. Soc. Nephrol. 2004, 15, 2449–2456. [Google Scholar] [CrossRef]
- Cortese-Krott, M.M.; Koning, A.; Kuhnle, G.G.C.; Nagy, P.; Bianco, C.L.; Pasch, A.; Wink, D.A.; Fukuto, J.M.; Jackson, A.A.; Van Goor, H.; et al. The Reactive Species Interactome: Evolutionary Emergence, Biological Significance, and Opportunities for Redox Metabolomics and Personalized Medicine. Antioxid. Redox Signal. 2017, 27, 684–712. [Google Scholar] [CrossRef]
- Turell, L.; Radi, R.; Alvarez, B. The thiol pool in human plasma: The central contribution of albumin to redox processes. Free Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef]
- Banne, A.F.; Amiri, A.; Pero, R.W. Reduced Level of Serum Thiols in Patients with a Diagnosis of Active Disease. J. Anti-Aging Med. 2003, 6, 327–334. [Google Scholar] [CrossRef]
- Abdulle, A.E.; Van Roon, A.M.; Smit, A.J.; Pasch, A.; Van Meurs, M.; Bootsma, H.; Bakker, S.J.L.; Said, Y.; Fernandez, B.; Feelisch, M.; et al. Rapid free thiol rebound is a physiological response following cold-induced vasoconstriction in healthy humans, primary Raynaud and systemic sclerosis. Physiol. Rep. 2019, 7, e14017. [Google Scholar] [CrossRef]
- Subramani, J.; Kundumani-Sridharan, V.; Hilgers, R.H.P.; Owens, C.; Das, K.C. Thioredoxin Uses a GSH-independent Route to Deglutathionylate Endothelial Nitric-oxide Synthase and Protect against Myocardial Infarction. J. Biol. Chem. 2016, 291, 23374–23389. [Google Scholar] [CrossRef] [PubMed]
- Duni, A.; Liakopoulos, V.; Koutlas, V.; Pappas, C.; Mitsis, M.; Dounousi, E. The Endothelial Glycocalyx as a Target of Ischemia and Reperfusion Injury in Kidney Transplantation—Where Have We Gone So Far? Int. J. Mol. Sci. 2021, 22, 2157. [Google Scholar] [CrossRef] [PubMed]
- Latchana, N. Preservation solutions used during abdominal transplantation: Current status and outcomes. World J. Transplant. 2015, 5, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Aebi, S.; Assereto, R.; Lauterburg, B. High-dose intravenous glutathione in man. Pharmacokinetics and effects on cyst(e)ine in plasma and urine. Eur. J. Clin. Investig. 1991, 21, 103–110. [Google Scholar] [CrossRef]
- Nielsen, M.B.; Jespersen, B.; Birn, H.; Krogstrup, N.V.; Bourgonje, A.R.; Leuvenink, H.G.D.; van Goor, H.; Nørregaard, R. Elevated plasma free thiols are associated with early and one-year graft function in renal transplant recipients. PLoS ONE 2021, 16, e0255930. [Google Scholar] [CrossRef]
- Nieuwenhuijs-Moeke, G.J.; Nieuwenhuijs, V.B.; Seelen, M.A.J.; Berger, S.P.; Heuvel, M.C.V.D.; Burgerhof, J.G.M.; Ottens, P.J.; Ploeg, R.J.; Leuvenink, H.G.D.; Struys, M.M.R.F. Propofol-based anaesthesia versus sevoflurane-based anaesthesia for living donor kidney transplantation: Results of the VAPOR-1 randomized controlled trial. Br. J. Anaesth. 2017, 118, 720–732. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Donor | n = 24 |
| Age [y] | 52.8 (±11.6) |
| Male [n (%)] | 11 (45.8%) |
| BMI [kg/m2] | 27 (± 3.2) |
| Smoking [n (%)] | 9 (37.5%) |
| Cardiovascular risk factors [n (%)] | 8 (33.3%) |
| Pre-donation mGFR [mL/min/1,73 m2] | 112.5 (96.3–128.8) |
| Recipient | n = 24 |
| Age [y] | 52.3 (±11.7) |
| Male [n (%)] | 9 (37.5%) |
| BMI [kg/m2] | 25.5 (±4.0) |
| Cardiovascular risk factors [n (%)] | 16 (66.7%) |
| Unrelated donor [n (%)] | 11 (45.8%) |
| Pre-emptive transplantation [n (%)] | 8 (33.3%) |
| Re-transplantation [n (%)] | 3 (12.5%) |
| ≥3 Human leukocytes antigen mismatches [n (%)] | 12 (50%) |
| Positive panel reactive antibodies (≥15%) [n (%)] | 4 (16.7%) |
| WIT1 [min] CIT [min] WIT2 [min] | 4 (3–4) 177 (155–207.5) 42.1 (±6.7) |
| Post-transplantation Outcomes | n = 24 * |
| DGF [n (%)] | 1 (4.2%) |
| eGFR 1 month post-transplantation [mL/min/1,73 m2] | 47.5 (41.3–59.5) |
| eGFR 3 months post-transplantation [mL/min/1,73 m2] | 43.1 (37.4–58.2) |
| eGFR 6 months post-transplantation [mL/min/1,73 m2] | 48.5 (38.9–61.5) |
| eGFR 12 month post-transplantation [mL/min/1,73 m2] | 48.4 (38.5–54.4) |
| eGFR 24 month post-transplantation [mL/min/1,73 m2] | 50.3 (40.2–61.8) |
| Acute rejection 2 years [n (%)] | 4 (16.7%) |
| Graft loss [n (%)] | 0 (0%) |
| Mortality [n (%)] | 1 (4.2%) |
| p-Value | b | SE b | 95% CI | |
|---|---|---|---|---|
| Systemic arterial R-SH | ||||
| Time | <0.001 * | 24.86 | 3.72 | 17.4–32.3 |
| Time2 | <0.001 * | −8.04 | 1.38 | −10.8–−5.3 |
| Time3 | <0.001 * | 0.86 | 0.15 | 0.6–1.2 |
| Renal venous R-SH | ||||
| Time | <0.001 * | −11.1 | 1.56 | −14.3–−7.9 |
| Time2 | <0.001 * | 2.0 | 0.30 | 1.4–2.6 |
| Delta R-SH | ||||
| Time | <0.001 * | −9.2 | 1.6 | −12.6–−5.9 |
| Time2 | <0.001 * | 1.3 | 0.3 | 0.6–1.9 |
| Systemic venous R-SH | ||||
| Time | 0.012 * | 6.6 | 2.6 | 1.5–11.8 |
| Time2 | 0.004 * | −1.5 | 0.5 | −2.5–−0.5 |
| Urinary R-SH | ||||
| Time | 0.156 | -5.3 | 3.7 | −12.6–−2.0 |
| Estimated Means (95% CI) | F-Statistic | p-Value | |
|---|---|---|---|
| Systemic arterial R-SH | 28.9 | <0.001 * | |
| After induction of anesthesia | 23.7 (21.9–25.5) | ||
| 30 sec after reperfusion | 30.2 (28.2–32.1) | ||
| 5 min after reperfusion | 31.8 (29.8–33.9) | ||
| 10 min after reperfusion | 31.8 (29.8–33.9) | ||
| 30 min after reperfusion | 37.0 (34.9–39.0) | ||
| Renal venous R-SH | 12.2 | <0.001 * | |
| 30 sec after reperfusion | 38.8 (36.7–40.8) | ||
| 5 min after reperfusion | 34.0 (31.9–36.1) | ||
| 10 min after reperfusion | 32.3 (30.2–34.5) | ||
| 30 min after reperfusion | 35.6 (33.4–37.8) | ||
| Delta R-SH | 20.9 | <0.001 * | |
| 30 sec after reperfusion | 8.7 (6.8–10.6) | ||
| 5 min after reperfusion | 2.3 (0.3–4.2) | ||
| 10 min after reperfusion | 0.4 ((−1.6)–2.4) | ||
| 30 min after reperfusion | −1.5 ((−3.6)–0.6) | ||
| Systemic venous R-SH | 4.2 | 0.009 * | |
| Day 1 post-transplantation | 23.4 (21.3–25.4) | ||
| Day 2 post-transplantation | 25.4 (23.3–27.4) | ||
| Day 6 post-transplantation | 24.6 (22.5–26.6) | ||
| Day 9 post-transplantation | 20.5 (18.3–22.6) | ||
| Urinary R-SH | 1.34 | 0.252 | |
| First urine upon reperfusion | 55.5 (26.6–84.7) | ||
| 2 h post-transplantation | 26.2 ((−4.3)–56.6) | ||
| Day 1 post-transplantation | 19.0 ((−12.2)–50.2) | ||
| Day 2 post-transplantation | 52.1 (20.8–83.3) | ||
| Day 6 post-transplantation | 16.4 ((−14.8)–47.7) | ||
| Day 9 post-transplantation | 18.8 ((−11.7)–49.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spraakman, N.A.; Coester, A.M.; Bourgonje, A.R.; Nieuwenhuijs, V.B.; Sanders, J.-S.F.; Leuvenink, H.G.D.; van Goor, H.; Nieuwenhuijs-Moeke, G.J. Systemic and Renal Dynamics of Free Sulfhydryl Groups during Living Donor Kidney Transplantation. Int. J. Mol. Sci. 2022, 23, 9789. https://doi.org/10.3390/ijms23179789
Spraakman NA, Coester AM, Bourgonje AR, Nieuwenhuijs VB, Sanders J-SF, Leuvenink HGD, van Goor H, Nieuwenhuijs-Moeke GJ. Systemic and Renal Dynamics of Free Sulfhydryl Groups during Living Donor Kidney Transplantation. International Journal of Molecular Sciences. 2022; 23(17):9789. https://doi.org/10.3390/ijms23179789
Chicago/Turabian StyleSpraakman, Nora A., Annemieke M. Coester, Arno R. Bourgonje, Vincent B. Nieuwenhuijs, Jan-Stephan F. Sanders, Henri G. D. Leuvenink, Harry van Goor, and Gertrude J. Nieuwenhuijs-Moeke. 2022. "Systemic and Renal Dynamics of Free Sulfhydryl Groups during Living Donor Kidney Transplantation" International Journal of Molecular Sciences 23, no. 17: 9789. https://doi.org/10.3390/ijms23179789
APA StyleSpraakman, N. A., Coester, A. M., Bourgonje, A. R., Nieuwenhuijs, V. B., Sanders, J.-S. F., Leuvenink, H. G. D., van Goor, H., & Nieuwenhuijs-Moeke, G. J. (2022). Systemic and Renal Dynamics of Free Sulfhydryl Groups during Living Donor Kidney Transplantation. International Journal of Molecular Sciences, 23(17), 9789. https://doi.org/10.3390/ijms23179789