


Propranolol versus Other Selected Drugs in the Treatment of Various Types of Anxiety or Stress, with Particular Reference to Stage Fright and Post-Traumatic Stress Disorder



Abstract
1. Introduction
2. Anatomical Therapeutic Chemical (ATC) Classification System
- -
- C07AA—beta blocking agents, non-selective;
- -
- C07AB—beta blocking agents, selective;
- -
- C07AG—alpha and beta blocking agents.
3. Stage Fright
4. Post-Traumatic Stress Disorder (PTSD)
5. The Medical Use of Propranolol
5.1. Cardiovascular
5.2. Psychiatric
5.2.1. Stress
PTSD
5.2.2. Anxiety
Stage Fright
Social Anxiety Disorder (SAD)
Fear of Public Speaking
5.2.3. Phobias
Fear of Dental Extraction
Arachnophobia
5.2.4. Autism Spectrum Disorder (ASD)
5.2.5. Other Psychoses
5.3. Other Uses
6. Mechanism of Action of Propranolol in the Treatment of Stage Fright
7. Mechanism of Action of Propranolol in the Treatment of PTSD
8. Therapeutic Effects of Stage Fright Treatment with Propranolol in Comparison with Selected Drugs for This Indication

{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Participants | Reconsolidation Procedure | Outcome Measures | Results |
|---|---|---|---|---|---|
| Brantigan et al., 1982 [48] | Double blind, crossover study, placebo controlled | 29 subjects, no information provided about age or sex | Propranolol and placebo given 1.5 h before recitals on 2 successive days | Continuous telemetric monitoring of the electrocardiogram (EKG). BP was recorded at the time of initial physical examination, before and after each performance. Subjects were observed during the performance for outward signs of stage fright | Propranolol eliminates the physical impediments to performance caused by stage fright; by eliminating the physical impediments to performance, propranolol can increase the quality of musical performance |
| Brewer, 1972 [90] | Placebo controlled, single blind | Psychology students before examination. According to the researchers, the “objective” stress was kept fairly constant, and the subjects were unusually homogeneous in terms of age, intellectual ability, and social class | Subjects were given increasing doses of propranolol until their resting pulse was slowed to between 55 and 65 beats per minute. The dosage necessary for manifest P-blockade ranged from 10 mg to 80 mg, and each student in the trial took an individually “tailored” dose of propranolol, or placebo, before the examination | Pulse monitoring | The results show clearly that propranolol causes no impairment of examination performance, and they suggest that it may actually improve performance in those who would otherwise be handicapped by severe anxiety, especially if cardiovascular symptoms are prominent |
| Drew et al., 1985 [92] | Randomised, double-blind, placebo controlled | 30 junior doctors aged 23–33 years | Each participant underwent 2 examinations; 4.5 h before each test, candidates were given either 120 mg of propranolol or a matching placebo | Scores from the exams testing powers of mental arithmetic and verbal reasoning | This study has shown that propranolol treatment is associated with a small, but statistically significant, improvement in performance of simple tests of verbal reasoning and mental arithmetic, conducted in an atmosphere of mild stress |
| Faigel, 1991 [49] | Uncontrolled open-label trial | Total 32 students, 11 girls and 21 boys, in their senior year of high school. | A single 40 mg tablet of propranolol one hour before the second exam | Scores from the two consecutive exams, including the Scholastic Aptitude Test (SAT) | The mean improvement in the SAT verbal score was 50 points (95% confidence interval 30 to 60, p < 0.01). The mean increase in the math score was 80 points (95% confidence interval 60 to 90, p < 0.01). Propranolol may be effective in disabling performance anxiety associated with taking the exam test |
| Giddens et al., 2010 [158] | Double-blind, placebo controlled | 12 adults, 6 male and 6 female, between the ages of 20 and 29 years | Each participant was given either 40 mg propranolol or placebo, as dictated by the randomisation schedule, with a glass of water. A delay of 60–75 min to allow for propranolol absorption occurred between treatment administration and the examination. | The intent of this experiment was to examine the effects of stress and beta-blockade on the voice. The parameters of F0, voice onset time (VOT), speaking rate, jitter, shimmer, maximum airflow declination rate, and subglottal pressure were measured under laboratory-induced sympathetic activation and beta-adrenergic blockade | Blockade of the increase in speaking rate in the propranolol treatment group may have indicated a reduction in cold pressor-induced anxiety; vocal jitter was observed to increase during beta-adrenergic blockade and stress |
| Stone et al., 1973 [91] | Double-blind, placebo controlled | 24 college men ages 21 to 28 | 60 mg of propranolol hydrochloride in 6 divided doses (each of them 10 mg) given orally during the 12 h preceding experimental procedures | Plasma free fatty acid (FFA) concentration, anxiety measured from the verbal samples using the method of Gottschalk and Gleser | The correlation between anxiety scored from the initial speech sample and FFA level was positive and significant for the placebo subjects and negative for the propranolol group. Propranolol administered orally may have value as an antianxiety agent and, in addition, is seen as providing an avenue for the exploration of psychobiological relationships |
| Elman et al., 1998 [166] | Randomised, double-blinded, crossover study | 5 3rd year ophthalmology residents, male, under age 30. 73 surgical cases were performed by the residents; the surgeons (residents) were administered propranolol for 40 cases and placebo for 33 | Participants ingested a capsule containing either propranolol, 40 mg, or placebo 1 h prior to performing ophthalmic microsurgery | At the conclusion of each case, both the resident and attending surgeon observer independently completed a form by grading on a sliding scale: (1) amount of overall tremor, (2) amount of tremor during placement of the first 3 sutures after delivery of the lens or lens nucleus (in accordance with the prevailing surgical technique at the time the study was performed), (3) anticipated difficulty of case, (4) actual difficulty of case, and (5) anxiety (surgeon only) | There was a highly significant effect of propranolol in decreasing anxiety (p = 0.0058), reducing surgical tremor overall (p < 0.0001), and reducing tremor while placing the first 3 sutures following lens extraction (p < 0.0001). Propranolol, 40 mg, administered 1 h prior to surgery, significantly decreases tremor and anxiety in the surgeon without untoward effects to the surgeon and the patient |
9. Therapeutic Effects of PTSD Treatment with Propranolol in Comparison with Selected Drugs for this Indication
Animal Clinical Trials
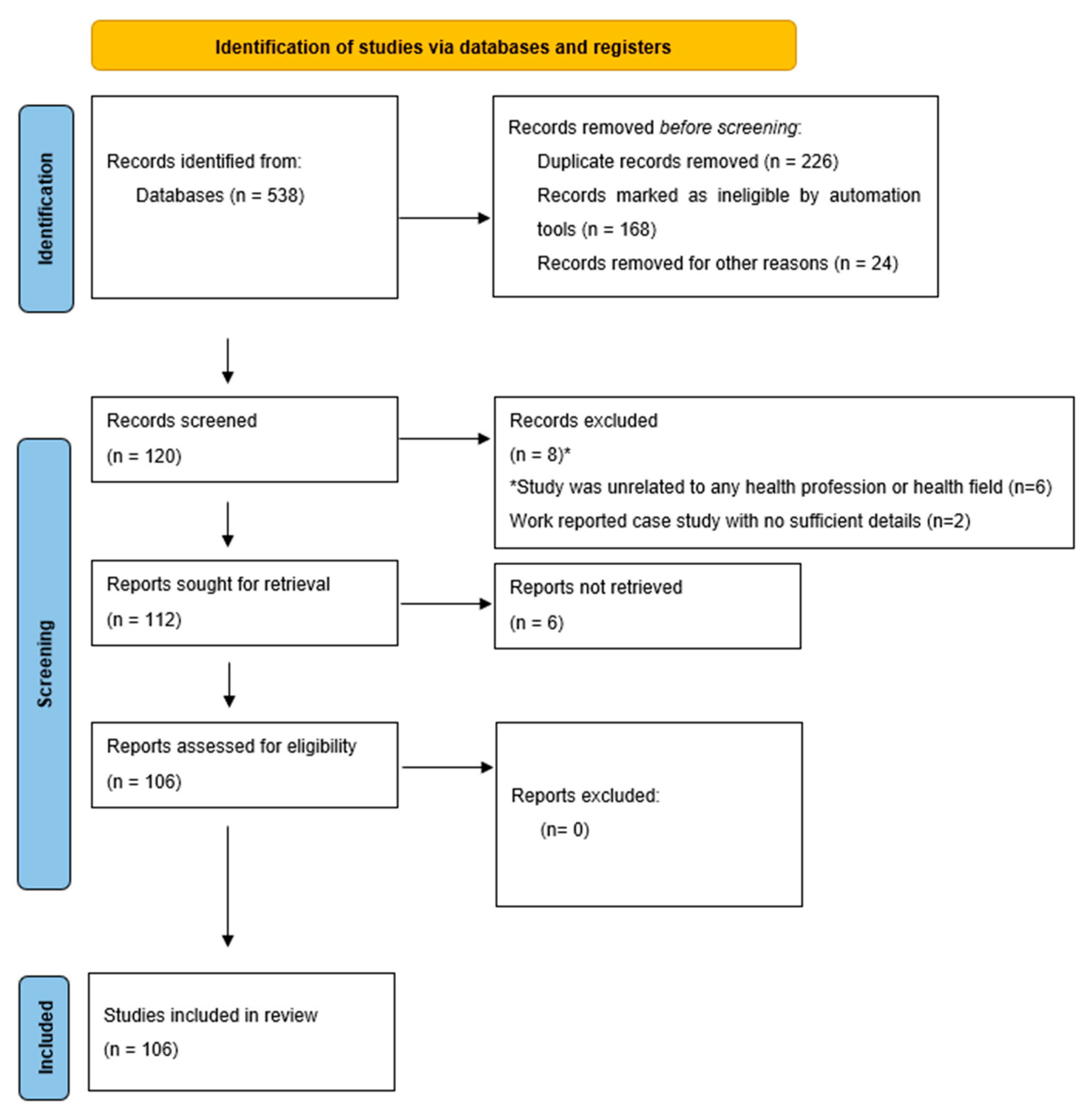
10. Materials and Methods
10.1. Protocol and Registration
10.2. Research Question and Data Extraction
10.3. Study Design and Search Strategy
10.4. Study Selection and Criteria
11. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACA | anterior cingulate area |
| AMG | amygdala |
| AMPAR | α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptor |
| API | Active Pharmaceutical Ingredient |
| ASD | Autism Spectrum Disorder |
| ATC | Anatomical Therapeutic Chemical Classification System |
| β-AR | beta-adrenergic receptor |
| BDI-II | Beck Depression Inventory-II |
| BLA | basolateral amygdala |
| BP | blood pressure |
| cAMP | cyclic adenosine monophosphate |
| CNS | central nervous system |
| CR | conditioned response |
| CREB | cAMP response element-binding protein |
| CS | conditioned stimulus |
| CSF | cerebrospinal fluid |
| dCA3 | dorsal cornu ammonis 3 |
| dDG | dorsal dentate gyrus |
| dHPC | dorsal hippocampus |
| dmPFC | dorsal medial prefrontal cortex |
| DPAG | dorsal periaqueductal grey |
| EBAD | emotional, behavioural, and autonomic dysregulation |
| EKG | electrocardiogram |
| FDA | Food and Drug Administration |
| FFA | free fatty acid |
| HPC | hippocampus |
| HR | heart rate |
| ILA | infralimbic area |
| LA | lateral amygdala |
| NE | noradrenaline, norepinephrine |
| OSF | Open Science Framework |
| PCL-S | PTSD Check List |
| PFC | prefrontal cortex |
| PKA | protein kinase A |
| PO | Perceptual Organisation |
| PRISMA | Preferred Reporting Items for Systematic Reviews |
| PS | Processing Speed |
| PTSD | post-traumatic stress disorder |
| SAD | social anxiety disorder |
| SAT | Scholastic Aptitude Test |
| SD | social defeat |
| SIB | self-injurious behaviour |
| SVTs | supraventricular tachyarrhythmias |
| US | unconditioned stimulus |
| vCA3 | ventral cornu ammonis 3 |
| vHPC | ventral hippocampus |
| VOT | voice onset time |
| WM | Working Memory |
References
- Srinivasan, A.V. Propranolol: A 50-Year Historical Perspective. Ann. Ind. Acad. Neurol. 2019, 22, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Steenen, S.A.; van Wijk, A.J.; van der Heijden, G.J.M.G.; van Westrhenen, R.; de Lange, J.; de Jongh, A. Propranolol for the treatment of anxiety disorders: Systematic review and meta-analysis. J. Psychopharmacol. 2016, 30, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Young, R.; Glennon, R.A. S(-)Propranolol as a discriminative stimulus and its comparison to the stimulus effects of cocaine in rats. Psychopharmacology 2009, 203, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.; Granville-Grossman, K.L. Effect of adrenergic receptor blockade of the tachycardia of thyrotoxicosis and anxiety state. Lancet 1965, 2, 1316–1318. [Google Scholar] [CrossRef]
- WHO Collaborating Center for Drug Statistics Methodology at the Norwegian Institute of Public Health. Available online: http://www.whocc.no (accessed on 17 July 2022).
- Barlow, D.H. Anxiety and Its Disorders: The Nature and Treatment of Anxiety and Panic, 2nd ed.; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Rowland, D.L.; van Lankveld, J.J.D.M. Anxiety and performance in sex, sport, and stage: Identifying common ground. Front. Psychol. 2019, 16, 1615. [Google Scholar] [CrossRef] [PubMed]
- Biasutti, M.; Concina, E. The role of coping strategy and experience in predicting music performance anxiety. Musicae Sci. 2014, 18, 189–202. [Google Scholar] [CrossRef]
- Marchant-Haycox, S.E.; Wilson, G.D. Personality and stress in performing artists. Personal. Individ. Differ. 1992, 13, 1061–1068. [Google Scholar] [CrossRef]
- Van Kemenade, J.F.; van Son, M.J.; van Heesch, N.C. Performance anxiety among professional musicians in symphonic orchestras: A self-report study. Psychol. Rep. 1995, 77, 555–562. [Google Scholar] [CrossRef]
- Yin, Q.; Sun, Z.; Liu, T.; Ni, X.; Deng, X.; Jia, Y.; Shang, Z.; Zhou, Y.; Liu, W. Posttraumatic stress symptoms of health care workers during the corona virus disease 2019. Clin. Psychol. Psychother. 2020, 27, 384–395. [Google Scholar] [CrossRef]
- Ehlers, A.; Hackmann, A.; Steil, R.; Clohessy, S.; Wenninger, K.; Winter, H. The nature of intrusive memories after trauma: The warning signal hypothesis. Behav. Res. Ther. 2002, 40, 995–1002. [Google Scholar] [CrossRef]
- Ehlers, A.; Hackmann, A.; Michael, T. Intrusive re-experiencing in post-traumatic stress disorder: Phenomenology, theory, and therapy. Memory 2004, 12, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.; Brewin, C.R. Intrusive memories in depression and posttraumatic stress disorder. Behav. Res. Ther. 1999, 37, 201–215. [Google Scholar] [CrossRef]
- Nemeroff, C.B.; Bremner, J.D.; Foa, E.B.; Mayberg, H.S.; North, C.S.; Stein, M.B. Posttraumatic stress disorder: A state-of-the-science review. J. Psychiatr. Res. 2006, 40, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Pitman, R.K.; Rasmusson, A.M.; Koenen, K.C.; Shin, L.M.; Orr, S.P.; Gilbertson, M.W.; Milad, M.R.; Liberzon, I. Biological studies of post-traumatic stress disorder. Nat. Rev. Neurosci. 2012, 13, 769–787. [Google Scholar] [CrossRef] [PubMed]
- Zoladz, P.R.; Diamond, D.M. Current status on behavioral and biological markers of PTSD: A search for clarity in a conflicting literature. Neurosci. Biobehav. Rev. 2013, 37, 860–895. [Google Scholar] [CrossRef]
- Brandes, D.; Ben-Schachar, G.; Gilboa, A.; Bonne, O.; Freedman, S.; Shalev, A.Y. PTSD symptoms and cognitive performance in recent trauma survivors. Psychiatry Res. 2002, 110, 231–238. [Google Scholar] [CrossRef]
- Geuze, E.; Vermetten, E.; de Kloet, C.S.; Hijman, R.; Westenberg, H.G.M. Neuropsychological performance is related to current social and occupational functioning in veterans with posttraumatic stress disorder. Depress. Anxiety 2009, 26, 7–15. [Google Scholar] [CrossRef]
- Gardner, J.J.; Griffiths, J. Propranolol, post-traumatic stress disorder, and intensive care: Incorporating new advances in psychiatry into the ICU. Crit. Care 2014, 18, 198. [Google Scholar] [CrossRef]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic Stress Disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef]
- Pennington, Z.T.; Cai, D.J. Propranolol Inhibits Reactivation of Fear Memory. Biol. Psychiatry 2021, 89, 1111–1112. [Google Scholar] [CrossRef]
- Panagioti, M.; Gooding, P.A.; Tarrier, N. A meta-analysis of the association between posttraumatic stress disorder and suicidality: The role of comorbid depression. Compr. Psychiatry 2012, 53, 915–930. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, R.H.; El-Gabalawy, R.; Tsai, J.; Sareen, J.; Neumeister, A.; Southwick, S.M. Typologies of posttraumatic stress disorder in the U.S. adult population. J. Affect. Disord. 2014, 162, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Saxe, G.; Stoddard, F.; Courtney, D.; Cunningham, K.; Chawla, N.; Sheridan, R.; King, D.; King, L. Relationship between acute morphine and the course of PTSD in children with burns. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Saxe, G.N.; Stoddard, F.; Hall, E.; Chawla, N.; Lopez, C.; Sheridan, R.; King, D.; King, L.; Yehuda, R. Pathways to PTSD, part I: Children with burns. Am. J. Psychiatry 2005, 162, 1299–1304. [Google Scholar] [CrossRef]
- Rosenberg, L.; Rosenberg, M.; Sharp, S.; Thomas, C.R.; Humphries, H.F.; Holzer, C.E.; Herndon, D.N.; Meyer, W.J. Does Acute Propranolol Treatment Prevent Posttraumatic Stress Disorder, Anxiety, and Depression in Children with Burns? J. Child Adolesc. Psychopharmacol. 2018, 28, 117–123. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Chandavarkar, R.; Sangha, S.; Khalil, S. Resolution of flashbacks of PTSD with propranolol: A case report. Prog. Neurol. Psychiatry 2016, 20, 10–13. [Google Scholar] [CrossRef][Green Version]
- Brady, K.; Pearlstein, T.; Asnis, G.M.; Baker, D.; Rothbaum, B.; Sikes, C.R.; Farfel, G.M. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: A randomized controlled trial. J. Am. Med. Assoc. 2000, 283, 1837–1844. [Google Scholar] [CrossRef]
- Marshall, R.D.; Beebe, K.L.; Oldham, M.; Zaninelli, R. Efficacy and safety of paroxetine treatment for chronic PTSD: A fixed-dose, placebo-controlled study. Am. J. Psychiatry 2001, 158, 1982–1988. [Google Scholar] [CrossRef]
- Tolin, D.F.; Foa, E.B. Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychol. Bull. 2006, 132, 959–992. [Google Scholar] [CrossRef]
- Tran, K.; Moulton, K.; Santesso, N.; Rabb, D. Cognitive Processing Therapy for Post-Traumatic Stress Disorder: A Systematic Review and Meta-analysis. In CADTH Health Technology Assessment; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2016; pp. 1–8. [Google Scholar]
- Strawn, J.R.; Geracioti, T.D. Noradrenergic dysfunction and the psychopharmacology of posttraumatic stress disorder. Depress. Anxiety 2008, 25, 260–271. [Google Scholar] [CrossRef]
- Auxéméry, Y. L’état de stress post-traumatique comme conséquence de l’interaction entre une susceptibilité génétique individuelle, un évènement traumatogène et un contexte social. Encephale 2012, 38, 373–380. [Google Scholar] [CrossRef]
- Blanchard, E.B.; Kolb, L.C.; Pallmeyer, T.P.; Gerardi, R.J. A psychophysiological study of posttraumatic stress disorder in Vietnam veterans. Psychiatr. Q. 1982, 54, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Elsesser, K.; Sartory, G.; Tackenberg, A. Attention, Heart Rate, and Startle Response during Exposure to Trauma-Relevant Pictures: A Comparison of Recent Trauma Victims and Patients with Posttraumatic Stress Disorder. J. Abnorm. Psychol. 2004, 113, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Besterman, E.M.M.; Friedlander, D.H. Clinical experiences with propranolol. Postgrad. Med. J. 1965, 41, 526–535. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Prichard, B.N.C.; Gillam, P.M.S. Treatment of Hypertension with Propranolol. Br. Med. J. 1969, 1, 7–16. [Google Scholar] [CrossRef]
- Goldstein, S. Propranolol therapy in patients with acute myocardial infarction: The beta-blocker heart attack trial. Circulation 1983, 67, 153–157. [Google Scholar]
- Morganroth, J.; Lichstein, E.; Byington, R. Beta-blocker heart attack trial: Impact of propranolol therapy on ventricular arrhythmias. Prev. Med. 1985, 14, 346–357. [Google Scholar] [CrossRef]
- Lee, S.H.; Yoon, S.B.; Cho, J.R.; Choi, S.; Jung, J.H.; Lee, N. The effects of different β-blockers on left-ventricular volume and function after primary coronary stenting in acute myocardial infarction. Angiology 2008, 59, 676–681. [Google Scholar] [CrossRef]
- Barton, A.L.; Moffett, B.S.; Valdes, S.O.; Miyake, C.; Kim, J.J. Efficacy and safety of high-dose propranolol for the management of infant supraventricular tachyarrhythmias. J. Pediatr. 2015, 166, 115–118. [Google Scholar] [CrossRef]
- Bonten, T.N.; Plaizier, C.E.I.; Snoep, J.J.; Stijnen, T.; Dekkers, O.M.; van der Bom, J.G. Effect of β-blockers on platelet aggregation: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2014, 78, 940–949. [Google Scholar] [CrossRef]
- Chrysant, S.G.; Chrysant, G.S.; Dimas, B. Current and future status of beta-blockers in the treatment of hypertension. Clin. Cardiol. 2008, 31, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Lonergan, M.H.; Olivera-Figueroa, L.A.; Pitman, R.K.; Brunet, A. Propranolol’s effects on the consolidation and reconsolidation of long-term emotional memory in healthy participants: A meta-analysis. J. Psychiatry Neurosci. 2013, 38, 222–231. [Google Scholar] [CrossRef]
- Grillon, C.; Cordova, J.; Morgan, C.A.; Charney, D.S.; Davis, M. Effects of the beta-blocker propranolol on cued and contextual fear conditioning in humans. Psychopharmacology 2004, 175, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Brantigan, C.O.; Brantigan, T.A.; Joseph, N. Effect of beta blockade and beta stimulation on stage fright. Am. J. Med. 1982, 72, 88–94. [Google Scholar] [CrossRef]
- Faigel, H.C. The Effect of Beta Blockade on Stress-Induced Cognitive Dysfunction in Adolescents. Clin. Pediatr. 1991, 30, 441–445. [Google Scholar] [CrossRef]
- Ananth, J.; Keh-Ming, L. Propranolol in psychiatry. Therapeutic Uses and Side Effects. Neuropsychobiology 1986, 15, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Christ, C.C.; Cahill, M.M.; Aldrich, S.J.; Taylor-Yeremeeva, E. Voluntary exercise or systemic propranolol ameliorates stress-related maladaptive behaviors in female rats. Physiol. Behav. 2019, 198, 120–133. [Google Scholar] [CrossRef]
- Taylor, E.A.; Harrison, J.; Turner, P. Propranolol in experimentally induced stress. Br. J. Psychiatry 1981, 139, 545–549. [Google Scholar] [CrossRef]
- Mahabir, M.; Ashbaugh, A.R.; Saumier, D.; Tremblay, J. Propranolol’s impact on cognitive performance in post-traumatic stress disorder. J. Affect. Disord. 2016, 192, 98–103. [Google Scholar] [CrossRef]
- Kindt, M.; Soeter, M.; Vervliet, B. Beyond extinction: Erasing human fear responses and preventing the return of fear. Nat. Neurosci. 2009, 12, 256–258. [Google Scholar] [CrossRef]
- Nader, K.; Schafe, G.E.; Le Doux, J.E. Fear memories require protein synthesis in the amygdala for reconsolidation after retrieval. Nature 2000, 406, 722–726. [Google Scholar] [CrossRef]
- Brunet, A.; Orr, S.P.; Tremblay, J.; Robertson, K.; Nader, K.; Pitman, R.K. Effect of post-retrieval propranolol on psychophysiologic responding during subsequent script-driven traumatic imagery in post-traumatic stress disorder. J. Psychiatr. Res. 2008, 42, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Shi, L.; Yuan, K.; Yao, P.; Chen, S.; Que, J.; Gong, Y.; Bao, Y.; Shi, J.; Han, Y.; et al. Propranolol-induced inhibition of unconditioned stimulus-reactivated fear memory prevents the return of fear in humans. Transl. Psychiatry 2020, 10, 345. [Google Scholar] [CrossRef]
- Cahill, L.; Prinst, B.; Webertt, M.; McGaugh, J.L. β Adrenergic activation and memory for emotional events. Sci. Ment. Health Stress Brain 1994, 9, 702–704. [Google Scholar] [CrossRef] [PubMed]
- Vaiva, G.; Ducrocq, F.; Jezequel, K.; Averland, B.; Lestavel, P.; Brunet, A.; Marmar, C.R. Immediate treatment with propranolol decreases posttraumatic stress disorder two months after trauma. Biol. Psychiatry 2003, 54, 947–949. [Google Scholar] [CrossRef]
- Pitman, R.K.; Sanders, K.M.; Zusman, R.M.; Healy, A.R.; Cheema, F.; Lasko, N.B.; Cahill, L.; Orr, S.P. Pilot study of secondary prevention of posttraumatic stress disorder with propranolol. Biol. Psychiatry 2002, 51, 189–192. [Google Scholar] [CrossRef]
- Walker, M.P.; Brakefield, T.; Hobson, J.A.; Stickgold, R. Dissociable stages of human memory consolidation and reconsolidation. Nature 2003, 425, 616–620. [Google Scholar] [CrossRef]
- Duvarci, S.; Nader, K. Characterization of fear memory reconsolidation. J. Neurosci. 2004, 24, 9269–9275. [Google Scholar] [CrossRef]
- Schiller, D.; Monfils, M.H.; Raio, C.M.; Johnson, D.C.; Ledoux, J.E.; Phelps, E.A. Preventing the return of fear in humans using reconsolidation update mechanisms. Nature 2010, 463, 49–53. [Google Scholar] [CrossRef]
- Hoge, E.A.; Worthington, J.J.; Nagurney, J.T.; Chang, Y.; Kay, E.B.; Feterowski, C.M.; Katzman, A.R.; Goetz, J.M.; Rosasco, M.L.; Lasko, N.B.; et al. Effect of acute posttrauma propranolol on PTSD outcome and physiological responses during script-driven imagery. CNS Neurosci. Ther. 2012, 18, 21–27. [Google Scholar] [CrossRef]
- Brunet, A.; Saumier, D.; Liu, A.; Streiner, D.L.; Tremblay, J.; Pitman, R.K. Reduction of PTSD symptoms with Pre-reactivation propranolol therapy: A randomized controlled trial. Am. J. Psychiatry 2018, 175, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Roullet, P.; Vaiva, G.; Véry, E.; Bourcier, A.; Yrondi, A.; Dupuch, L.; Lamy, P.; Thalamas, C.; Jasse, L.; Hage, W.E.; et al. Traumatic memory reactivation with or without propranolol for PTSD and comorbid MD symptoms: A randomised clinical trial. Neuropsychopharmacology 2021, 46, 1643–1649. [Google Scholar] [CrossRef] [PubMed]
- Brunet, A.; Thomas, É.; Saumier, D.; Ashbaugh, A.R.; Azzoug, A.; Pitman, R.K.; Orr, S.P.; Tremblay, J. Trauma reactivation plus propranolol is associated with durably low physiological responding during subsequent script-driven traumatic imagery. Can. J. Psychiatry 2014, 59, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, L.; Nader, K.; Wolf, O.T.; Beaudry, T.; Pruessner, J.C. Neural signature of reconsolidation impairments by propranolol in humans. Biol. Psychiatry 2012, 71, 380–386. [Google Scholar] [CrossRef]
- Brunet, A.; Poundja, J.; Tremblay, J.; Bui, E.; Thomas, E.; Orr, S.P.; Azzoug, A.; Birmes, P.; Pitman, R.K. Trauma reactivation under the influence of propranolol decreases posttraumatic stress symptoms and disorder: 3 open-label trials. J. Clin. Psychopharmacol. 2011, 31, 547–550. [Google Scholar] [CrossRef]
- Mahabir, M.; Tucholka, A.; Shin, L.M.; Etienne, P.; Brunet, A. Emotional face processing in post-traumatic stress disorder after reconsolidation impairment using propranolol: A pilot fMRI study. J. Anxiety Disord. 2015, 36, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, L.; Nader, K.; Pruessner, J.C. β-Adrenergic blockade during reactivation reduces the subjective feeling of remembering associated with emotional episodic memories. Biol. Psychol. 2013, 92, 227–232. [Google Scholar] [CrossRef]
- Soeter, M.; Kindt, M. Dissociating response systems: Erasing fear from memory. Neurobiol. Learn. Mem. 2010, 94, 30–41. [Google Scholar] [CrossRef]
- Soeter, M.; Kindt, M. Disrupting reconsolidation: Pharmacological and behavioral manipulations. Learn. Mem. 2011, 18, 357–366. [Google Scholar] [CrossRef]
- Soeter, M.; Kindt, M. An Abrupt Transformation of Phobic Behavior after a Post-Retrieval Amnesic Agent. Biol. Psychiatry 2015, 78, 880–886. [Google Scholar] [CrossRef]
- Sevenster, D.; Beckers, T.; Kindt, M. Retrieval per se is not sufficient to trigger reconsolidation of human fear memory. Neurobiol. Learn. Mem. 2012, 97, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Sevenster, D.; Beckers, T.; Kindt, M. Prediction error governs pharmacologically induced amnesia for learned fear. Science 2013, 339, 830–833. [Google Scholar] [CrossRef] [PubMed]
- Sevenster, D.; Beckers, T.; Kindt, M. Prediction error demarcates the transition from retrieval, to reconsolidation, to new learning. Learn. Mem. 2014, 21, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Kindt, M.; Soeter, M. Pharmacologically induced amnesia for learned fear is time and sleep dependent. Nat. Commun. 2018, 9, 1316. [Google Scholar] [CrossRef]
- Kindt, M.; van Emmerik, A. New avenues for treating emotional memory disorders: Towards a reconsolidation intervention for posttraumatic stress disorder. Ther. Adv. Psychopharmacol. 2016, 6, 283–295. [Google Scholar] [CrossRef]
- Thierrée, S.; Richa, S.; Brunet, A.; Egreteau, L.; Roig, Q.; Clarys, D.; El-Hage, W. Trauma reactivation under propranolol among traumatized Syrian refugee children: Preliminary evidence regarding efficacy. Eur. J. Psychotraumatol. 2020, 11, 1733248. [Google Scholar] [CrossRef]
- Famularo, R.; Kinscherff, R.; Fenton, T. Propranolol Treatment for Childhood Posttraumatic Stress Disorder, Acute Type: A Pilot Study. Am. J. Dis. Child. 1988, 142, 1244–1247. [Google Scholar] [CrossRef]
- Beversdorf, D.Q.; White, C.A.D.M.; Chever, D.C.; Hughes, J.D.; Bornstein, R.A. Central beta-adrenergic modulation of cognitive flexibility. NeuroReport 2002, 13, 2505–2507. [Google Scholar] [CrossRef]
- Giustino, T.F.; Fitzgerald, P.J.; Maren, S. Revisiting propranolol and PTSD: Memory erasure or extinction enhancement? Neurobiol. Learn. Mem. 2016, 130, 26–33. [Google Scholar] [CrossRef]
- Kessler, R.C.; Aguilar-Gaxiola, S.; Alonso, J.; Chatterji, S.; Lee, S.; Ormel, J.; Üstün, T.B.; Wang, P.S. The global burden of mental disorders: An update from the WHO World Mental Health (WMH) surveys. Epidemiol. E Psichiatr. Soc. 2009, 18, 23–33. [Google Scholar] [CrossRef]
- Beddington, J.; Cooper, C.L.; Field, J.; Goswami, U.; Huppert, F.A.; Jenkins, R.; Jones, H.S.; Kirkwood, T.B.L.; Sahakian, B.J.; Thomas, S.M. The mental wealth of nations. Nature 2008, 455, 1057–1060. [Google Scholar] [CrossRef] [PubMed]
- Fogari, R.; Zoppi, A. Effect of antihypertensive agents on quality of life in the elderly. Drugs Aging 2004, 21, 377–393. [Google Scholar] [CrossRef] [PubMed]
- Granville-Grossman, K.L.; Turner, P. The effect of propranolol on anxiety. Lancet 1966, 1, 788–790. [Google Scholar] [CrossRef]
- Kathol, R.G.; Noyes, R., Jr.; Slymen, D.J.; Crowe, R.R.; Clancy, J.; Kerber, R.E. Propranolol in Chronic Anxiety Disorders. Arch. Gen. Psychiatry 1980, 37, 1361–1365. [Google Scholar] [CrossRef] [PubMed]
- Chalkia, A.; Weermeijer, J.; van Oudenhove, L.; Beckers, T. Acute but not permanent effects of propranolol on fear memory expression in humans. Front. Hum. Neurosci. 2019, 13, 51. [Google Scholar] [CrossRef]
- Brewer, C. Beneficial effect of beta-adrenergic blockade on “exam. nerves”. Lancet 1972, 2, 435. [Google Scholar] [CrossRef]
- Stone, W.N.; Gleser, G.C.; Gottschalk, L.A. Anxiety and beta-adrenergic blockade. Arch. Gen. Psychiatry 1973, 29, 620–622. [Google Scholar] [CrossRef] [PubMed]
- Drew, J.T.P.; Barnes, N.J.; Evans, J.W.S. The effects of acute B-adrenoceptor blockade on examination performance. Br. J. Psychiatry 1983, 19, 782–786. [Google Scholar] [CrossRef]
- Clark, D.B.; Agras, W.S. The assessment and treatment of performance anxiety in musicians. Am. J. Psychiatry 1991, 148, 598–605. [Google Scholar] [CrossRef]
- Dyck, J.B.; Chung, F. A comparison of propranolol and diazepam for preoperative anxiolysis. Can. J. Anaesth. 1991, 38, 704–709. [Google Scholar] [CrossRef]
- Jakobsson, J.; Rane, K.; Ryberg, G. Oral premedication one hour before minor gynaecological surgery—Does it have any effect? Acta Anaesthesiol. Scand. 1995, 39, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Dommisse, C.S.; Hayes, P.E. Current concepts in clinical therapeutics: Anxiety disorders, Part 2. Clin. Pharm. 1987, 6, 196–215. [Google Scholar]
- Morissette, S.B.; Spiegel, D.A.; Barlow, D.H. Combining exposure and pharmacotherapy in the treatment of social anxiety disorder: A preliminary study of state dependent learning. J. Psychopathol. Behav. Assess. 2008, 30, 211–219. [Google Scholar] [CrossRef]
- Elsey, J.W.B.; Filmer, A.I.; Galvin, H.R.; Kurath, J.D.; Vossoughi, L.; Thomander, L.S.; Zavodnik, M.; Kindt, M. Reconsolidation-based treatment for fear of public speaking: A systematic pilot study using propranolol. Transl. Psychiatry 2020, 10, 179. [Google Scholar] [CrossRef] [PubMed]
- Bodie, G.D. A racing heart, rattling knees, and ruminative thoughts: Defining, explaining, and treating public speaking anxiety. Commun. Educ. 2010, 59, 70–105. [Google Scholar] [CrossRef]
- Soeter, M.; Kindt, M. High trait anxiety: A challenge for disrupting fear memory reconsolidation. PLoS ONE 2013, 8, e75239. [Google Scholar] [CrossRef]
- Liu, H.H.; Milgrom, P.; Fiset, L. Effect of a Beta-adrenergic Blocking Agent on Dental Anxiety. J. Dent. Res. 1991, 70, 1306–1308. [Google Scholar] [CrossRef]
- Steenen, S.A.; van Wijk, A.J.; van Westrhenen, R.; de Lange, J.; de Jongh, A. Effects of propranolol on fear of dental extraction: Study protocol for a randomized controlled trial. Trials 2015, 16, 536. [Google Scholar] [CrossRef]
- De Jongh, A.; Olff, M.; van Hoolwerff, H.; Aartman, I.H.A.; Broekman, B.; Lindauer, R.; Boer, F. Anxiety and post-traumatic stress symptoms following wisdom tooth removal. Behav. Res. Ther. 2008, 46, 1305–1310. [Google Scholar] [CrossRef]
- De Jongh, A.; van Wijk, A.J.; Lindeboom, J.A. Psychological impact of third molar surgery: A 1-month prospective study. J. Oral Maxillofac. Surg. 2011, 69, 59–65. [Google Scholar] [CrossRef]
- Van Houtem, C.M.H.H.; van Wijk, A.J.; de Jongh, A. Presence, Content, and Characteristics of Memories of Individuals with Dental Phobia. Appl. Cogn. Psychol. 2015, 29, 515–523. [Google Scholar] [CrossRef]
- Mineka, S.; Öhman, A. Phobias and preparedness: The selective, automatic, and encapsulated nature of fear. Biol. Psychiatry 2002, 52, 927–937. [Google Scholar] [CrossRef]
- Elsey, J.W.B.; Kindt, M. Placebo and Non-specific Effects in Reconsolidation-Based Treatment for Arachnophobia. Front. Psychiatry 2021, 12, 775770. [Google Scholar] [CrossRef] [PubMed]
- Greendyke, R.M.; Kanter, D.R.; Schuster, D.B.; Verstreate, S.; Wootton, J. Propranolol Treatment of Assaultive Patients with Organic Brain Disease. J. Nerv. Ment. Dis. 1986, 174, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.G.; Dombovy, M.L.; Watkins, K. Treatment of Viral Encephalitis Organic Personality Disorder and Autistic Features with Propranolol: A Case Report. Neurorehabilit. Neural Repair 1995, 9, 41–45. [Google Scholar] [CrossRef]
- Williams, D.T.; Mehl, R.; Yudofsky, S.; Adams, D.; Roseman, B. The Effect of Propranolol on Uncontrolled Rage Outbursts in Children and Adolescents with Organic Brain Dysfunction. J. Am. Acad. Child Psychiatry 1982, 21, 129–135. [Google Scholar] [CrossRef]
- Connor, D.F.; Steingard, R.J. A Clinical Approach to the Pharmacotherapy of Aggression in Children and Adolescents. Ann. N. Y. Acad. Sci. 1996, 794, 290–307. [Google Scholar] [CrossRef]
- Sweeney, D.P.; Forness, S.R.; Levitt, J.G. An Overview of Medications Commonly Used to Treat Behavioral Disorders Associated with Autism, Tourette Syndrome, and Pervasive Developmental Disorders. Focus Autism Other Dev. Disabil. 2015, 13, 144–150. [Google Scholar] [CrossRef]
- Kuperman, S.; Stewart, M.A. Use of propranolol to decrease aggressive outbursts in younger patients. Psychosomatics 1987, 28, 315–319. [Google Scholar] [CrossRef]
- Knabe, R.; Bovier, P. Pharmacological treatment of extreme self-injurious behavior in autism. Eur. Psychiatry 1992, 7, 297–298. [Google Scholar] [CrossRef]
- Sagar-Ouriaghli, I.; Lievesley, K.; Santosh, P.J. Propranolol for treating emotional, behavioural, autonomic dysregulation in children and adolescents with autism spectrum disorders. J. Psychopharmacol. 2018, 32, 641–653. [Google Scholar] [CrossRef] [PubMed]
- Santosh, P.J.; Bell, L.; Fiori, F.; Singh, J. Pediatric Antipsychotic Use and Outcomes Monitoring. J. Child Adolesc. Psychopharmacol. 2017, 27, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Beversdorf, D.Q.; Carpenter, A.L.; Miller, R.F.; Cios, J.S.; Hillier, A. Effect of propranolol on verbal problem solving in autism spectrum disorder. Neurocase 2008, 14, 378–383. [Google Scholar] [CrossRef]
- Zamzow, R.M.; Ferguson, B.J.; Ragsdale, A.S.; Lewis, M.L.; Beversdorf, D.Q. Effects of acute beta-adrenergic antagonism on verbal problem solving in autism spectrum disorder and exploration of treatment response markers. J. Clin. Exp. Neuropsychol. 2017, 39, 596–606. [Google Scholar] [CrossRef]
- Beversdorf, D.Q.; Saklayen, S.; Higgins, K.F.; Bodner, K.E.; Kanne, S.M.; Christ, S.E. Effect of propranolol on word fluency in autism. Cogn. Behav. Neurol. 2011, 24, 11–17. [Google Scholar] [CrossRef]
- Bodner, K.E.; Beversdorf, D.Q.; Saklayen, S.S.; Christ, S.E. Noradrenergic moderation of working memory impairments in adults with autism spectrum disorder. J. Int. Neuropsychol. Soc. 2012, 18, 556–564. [Google Scholar] [CrossRef]
- Hegarty, J.P.; Ferguson, B.J.; Zamzow, R.M.; Rohowetz, L.J.; Johnson, J.D.; Christ, S.E.; Beversdorf, D.Q. Beta-adrenergic antagonism modulates functional connectivity in the default mode network of individuals with and without autism spectrum disorder. Brain Imaging Behav. 2017, 11, 1278–1289. [Google Scholar] [CrossRef]
- Narayanan, A.; White, C.A.; Saklayen, S.; Scaduto, M.J.; Carpenter, A.L.; Abduljalil, A.; Schmalbrock, P.; Beversdorf, D.Q. Effect of propranolol on functional connectivity in autism spectrum disorder—A pilot study. Brain Imaging Behav. 2010, 4, 189–197. [Google Scholar] [CrossRef]
- Zamzow, R.M.; Ferguson, B.J.; Stichter, J.P.; Porges, E.C.; Ragsdale, A.S.; Lewis, M.L.; Beversdorf, D.Q. Effects of propranolol on conversational reciprocity in autism spectrum disorder: A pilot, double-blind, single-dose psychopharmacological challenge study. Psychopharmacology 2016, 233, 1171–1178. [Google Scholar] [CrossRef]
- Deepmala; Agrawal, M. Use of Propranolol for Hypersexual Behavior in an Adolescent with Autism. Ann. Pharmacother. 2014, 48, 1385–1388. [Google Scholar] [CrossRef]
- Petrie, W.M.; Ban, T.A. Propranolol in Organic Agitation. Lancet 1981, 317, 324. [Google Scholar] [CrossRef]
- Elliott, F.A. Propranolol for the control of belligerent behavior following acute brain damage. Ann. Neurol. 1977, 1, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Schreier, H.A. Use of propranolol in the treatment of postencephalitic psychosis. Am. J. Psychiatry 1979, 136, 840–841. [Google Scholar] [CrossRef] [PubMed]
- O’Reagan, J.B. The treatment of acute postpartum psychosis. Can. Med. Assoc. J. 1981, 125, 1083. [Google Scholar]
- Chowdhury, D.; Bansal, L.; Duggal, A.; Datta, D.; Mundra, A.; Krishnan, A.; Koul, A.; Gupta, A. TOP-PRO study: A randomized double-blind controlled trial of topiramate versus propranolol for prevention of chronic migraine. Cephalalgia 2022, 42, 396–408. [Google Scholar] [CrossRef]
- Fogelholm, R. Propranolol and cluster headache. Br. Med. J. 1972, 4, 110. [Google Scholar] [CrossRef][Green Version]
- Mihai, R.; Sadler, G.P.; Bridge, H. Adrenergic blockade with phenoxybenzamine and propranolol in a cohort of 60 patients undergoing surgery for phaeochromocytoma. Eur. J. Anaesthesiol. 2008, 25, 508–510. [Google Scholar] [CrossRef]
- Cuesta, A.M.; Gallardo-Vara, E.; Casado-Vela, J.; Recio-Poveda, L.; Botella, L.M.; Albiñana, V. The Role of Propranolol as a Repurposed Drug in Rare Vascular Diseases. Int. J. Mol. Sci. 2022, 23, 4217. [Google Scholar] [CrossRef]
- Kaushik, S.; Kataria, P.; Joshi, G.S.; Singh, R.; Handa, S.; Pandav, S.S.; Ram, J.; Gupta, A. Perioperative Propranolol: A Useful Adjunct for Glaucoma Surgery in Sturge-Weber Syndrome. Ophthalmology. Glaucoma 2019, 2, 267–274. [Google Scholar] [CrossRef]
- Cervantes, J.; Perper, M.; Eber, A.E.; Fertig, R.M.; Tsatalis, J.P.; Nouri, K. Laser treatment of primary axillary hyperhidrosis: A review of the literature. Lasers Med. Sci. 2018, 33, 675–681. [Google Scholar] [CrossRef]
- Lima, D.R.; Turner, P. Propranolol increases reduced beta-receptor function in severely anxious patients. Lancet 1983, 2, 1505. [Google Scholar] [CrossRef]
- Audi, E.A.; de Oliveira, R.M.W.; Graeff, F.G. Microinjection of propranolol into the dorsal periaqueductal gray causes an anxiolytic effect in the elevated plus-maze antagonized by ritanserin. Psychopharmacology 1991, 105, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Kroes, M.C.W.; Tona, K.D.; Den Ouden, H.E.M.; Vogel, S.; van Wingen, G.A.; Fernández, G. How administration of the beta-blocker propranolol before extinction can prevent the return of fear. Neuropsychopharmacology 2016, 41, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Müller, U.; Mottweiler, E.; Bublak, P. Noradrenergic blockade and numeric working memory in humans. J. Psychopharmacol. 2005, 19, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.P.; Cain, C.K.; Ostroff, L.E.; Ledoux, J.E. Molecular mechanisms of fear learning and memory. Cell 2011, 147, 509–524. [Google Scholar] [CrossRef]
- Hao, Y.; Jing, H.; Bi, Q.; Zhang, J.; Qin, L.; Yang, P. Intra-amygdala microinfusion of IL-6 impairs the auditory fear conditioning of rats via JAK/STAT activation. Behav. Brain Res. 2014, 275, 88–95. [Google Scholar] [CrossRef]
- Gavin Norris, J.; Benveniste, E.N. Interleukin-6 production by astrocytes: Induction by the neurotransmitter norepinephrine. J. Neuroimmunol. 1993, 45, 137–145. [Google Scholar] [CrossRef]
- Geracioti, T.D., Jr.; Baker, D.G.; Ekhator, N.N.; West, S.A.; Hill, K.K.; Bruce, A.B.; Schmidt, D.; Rounds-Kugler, B.; Yehuda, R.; Keck, P.E.; et al. CSF Norepinephrine Concentrations in Posttraumatic Stress Disorder. Am. J. Psychiatry 2001, 158, 1227–1230. [Google Scholar] [CrossRef]
- Kosten, T.R.; Mason, J.W.; Giller, E.L.; Ostroff, R.B. Sustained urinary norepinephrine and epinephrine elevation in post-traumatic stress disorder. Psychoneuroendocrinology 1987, 12, 13–20. [Google Scholar] [CrossRef]
- Mellman, T.A.; Kumar, A.; Kulick-Bell, R.; Kumar, M.; Nolan, B. Nocturnal/daytime urine noradrenergic measures and sleep in combat-related PTSD. Biol. Psychiatry 1995, 38, 174–179. [Google Scholar] [CrossRef]
- Yehuda, R.; Southwick, S.M.; Giller, E.L.; Ma, X.; Mason, J.W. Urinary catecholamine excretion and severity of PTSD symptoms in Vietnam combat veterans. J. Nerv. Ment. Dis. 1992, 180, 321–325. [Google Scholar] [CrossRef]
- Dębiec, J.; Bush, D.E.A.; LeDoux, J.E. Noradrenergic enhancement of reconsolidation in the amygdala impairs extinction of conditioned fear in rats—A possible mechanism for the persistence of traumatic memories in PTSD. Depress. Anxiety 2011, 28, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Krystal, J.H.; Davis, L.L.; Neylan, T.C.; Raskind, M.; Schnurr, P.P.; Stein, M.B.; Vessicchio, J.; Shiner, B.; Gleason, T.; Huang, G.D. It Is Time to Address the Crisis in the Pharmacotherapy of Posttraumatic Stress Disorder: A Consensus Statement of the PTSD Psychopharmacology Working Group. Biol. Psychiatry 2017, 82, e51–e59. [Google Scholar] [CrossRef] [PubMed]
- Przybyslawski, J.; Roullet, P.; Sara, S.J. Attenuation of emotional and nonemotional memories after their reactivation: Role of β adrenergic receptors. J. Neurosci. 1999, 19, 6623–6628. [Google Scholar] [CrossRef]
- Kandel, E.R. The molecular biology of memory: CAMP, PKA, CRE, CREB-1, CREB-2, and CPEB. Mol. Brain 2012, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- Otis, J.M.; Werner, C.T.; Mueller, D. Noradrenergic regulation of fear and drug-associated memory reconsolidation. Neuropsychopharmacology 2015, 40, 793–803. [Google Scholar] [CrossRef]
- Zhou, J.; Luo, Y.; Zhang, J.T.; Li, M.X.; Wang, C.M.; Guan, X.L.; Wu, P.F.; Hu, Z.L.; Jin, Y.; Ni, L.; et al. Propranolol decreases retention of fear memory by modulating the stability of surface glutamate receptor GluA1 subunits in the lateral amygdala. Br. J. Pharmacol. 2015, 172, 5068–5082. [Google Scholar] [CrossRef]
- Pitman, R.K.; Delahanty, D.L. Conceptually driven pharmacologic approaches to acute trauma. CNS Spectr. 2005, 10, 99–106. [Google Scholar] [CrossRef]
- Adamec, R.; Muir, C.; Grimes, M.; Pearcey, K. Involvement of noradrenergic and corticoid receptors in the consolidation of the lasting anxiogenic effects of predator stress. Behav. Brain Res. 2007, 179, 192–207. [Google Scholar] [CrossRef]
- Aykaç, A.; Aydin, B.; Cabadak, H.; Gören, M.Z. The change in muscarinic receptor subtypes in different brain regions of rats treated with fluoxetine or propranolol in a model of post-traumatic stress disorder. Behav. Brain Res. 2012, 232, 124–129. [Google Scholar] [CrossRef]
- Burhans, L.B.; Smith-Bell, C.A.; Schreurs, B.G. Propranolol produces short-term facilitation of extinction in a rabbit model of post-traumatic stress disorder. Neuropharmacology 2018, 135, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Leal Santos, S.; Stackmann, M.; Muñoz Zamora, A.; Mastrodonato, A.; de Landri, A.V.; Vaughan, N.; Chen, B.K.; Lanio, M.; Denny, C.A. Propranolol Decreases Fear Expression by Modulating Fear Memory Traces. Biol. Psychiatry 2021, 89, 1150–1161. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.B.; Moser, E.I.; Forrest, E.; Andersen, P.; Morris, R.G.M. Spatial learning with a minislab in the dorsal hippocampus. Proc. Natl. Acad. Sci. USA 1995, 92, 9697–9701. [Google Scholar] [CrossRef] [PubMed]
- Giddens, C.L.; Barron, K.W.; Clark, K.F.; Warde, W.D. Beta-Adrenergic Blockade and Voice: A Double-Blind, Placebo-Controlled Trial. J. Voice 2010, 24, 477–489. [Google Scholar] [CrossRef]
- Brantigan, C.O.; Brantigan, T.A.; Joseph, N. The effect of beta blockade on stage fright. A controlled study. Rocky Mt. Med. J. 1979, 76, 227–233. [Google Scholar]
- Harris, D.A. Using Beta-blockers to Control Stage Fright: A Dancer’s Dilemma. In Medical Problems of Performing Artists; Science & Medicine, Inc.: Narberth, PA, USA, 2001; Volume 16, pp. 72–76. [Google Scholar] [CrossRef]
- Albus, M.; Zellner, A.; Bondy, B.; Muller-Spahn, F.; Engel, R.; Ackenheil, M. Influence of CGP 361A, propranolol and diazepam on autonomous reactions to different stressors. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 1989, 13, 87–97. [Google Scholar] [CrossRef]
- File, S.; Lister, R. A comparison of the effects of lorazepam with those of propranolol on experimentally-induced anxiety and performance. Br. J. Clin. Pharmacol. 1985, 19, 445–451. [Google Scholar] [CrossRef]
- Hallstrom, C.; Treasaden, I.; Edwards, J.G.; Lader, M. Diazepam, propranolol and their combination in the management of chronic anxiety. Br. J. Psychiatry 1981, 139, 417–421. [Google Scholar] [CrossRef]
- Chaturvedi, S.K. Propranolol versus metoprolol in anxiety disorders. Can. J. Psychiatry 1987, 32, 250–251. [Google Scholar] [CrossRef]
- Ibrahim, A.N.; Atallah, R.Y. Ivabradine versus propranolol given orally in microlaryngoscopic surgeries in attenuating stress response: A comparative prospective double blind randomized study. Egypt. J. Anaesth. 2016, 32, 503–511. [Google Scholar] [CrossRef]
- Elman, M.J.; Sugar, J.; Fiscella, R.; Deutsch, T.A.; Noth, J.; Nyberg, M.; Packo, K.; Anderson, R.J. The effect of propranolol versus placebo on resident surgical performance. Trans. Am. Ophthalmol. Soc. 1998, 96, 283–289. [Google Scholar] [PubMed]
- Vermetten, E.; Vythilingam, M.; Southwick, S.M.; Charney, D.S.; Bremner, J.D. Long-term treatment with paroxetine increases verbal declarative memory and hippocampal volume in posttraumatic stress disorder. Biol. Psychiatry 2003, 54, 693–702. [Google Scholar] [CrossRef]
- Fani, N.; Kitayama, N.; Ashraf, A.; Reed, L.; Afzal, N.; Jawed, F.; Bremner, J.D. Neuropsychological functioning in patients with posttraumatic stress disorder following short-term paroxetine treatment. Psychopharmacol. Bull. 2009, 42, 53–68. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3230323/ (accessed on 5 July 2022). [PubMed]
- Thomas, T.; Dooley, T. Treatment of Anxiety Prior to a Medical Procedure using an Atenolol–Scopolamine Combination Drug. J. Depress. Anxiety 2018, 7, 303. [Google Scholar] [CrossRef]
- Armstrong, C.; Kapolowicz, M.R. A Preliminary Investigation on the Effects of Atenolol for Treating Symptoms of Anxiety. Mil. Med. 2020, 185, E1954–E1960. [Google Scholar] [CrossRef]
- Krauseneck, T.; Padberg, F.; Roozendaal, B.; Grathwohl, M.; Weis, F.; Hauer, D.; Kaufmann, I.; Schmoeckel, M.; Schelling, G. A Β-adrenergic antagonist reduces traumatic memories and PTSD symptoms in female but not in male patients after cardiac surgery. Psychol. Med. 2010, 40, 861–869. [Google Scholar] [CrossRef]
- Belkin, M.R.; Schwartz, T.L. Alpha-2 receptor agonists for the treatment of posttraumatic stress disorder. Drugs Context 2015, 4, 2–6. [Google Scholar] [CrossRef]
- Raskind, M.A.; Peskind, E.R.; Kanter, E.D.; Petrie, E.C.; Radant, A.; Thompson, C.E.; Dobie, D.J.; Hoff, D.; Rein, R.J.; Straits-Tröster, K.; et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: A placebo-controlled study. Am. J. Psychiatry 2003, 160, 371–373. [Google Scholar] [CrossRef]
- Tawa, J.; Murphy, S. Psychopharmacological treatment for military posttraumatic stress disorder: An integrative review. J. Am. Assoc. Nurse Pract. 2013, 25, 419–423. [Google Scholar] [CrossRef]
- Taylor, H.R.; Freeman, M.K.; Cates, M.E. Prazosin for treatment of nightmares related to posttraumatic stress disorder. Am. J. Health-Syst. Pharm. 2008, 65, 716–722. [Google Scholar] [CrossRef][Green Version]
- Boehnlein, J.K.; Kinzie, J.D. Pharmacologic reduction of CNS noradrenergic activity in PTSD: The case for clonidine and prazosin. J. Psychiatr. Pract. 2007, 13, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Detweiler, M.B.; Pagadala, B.; Candelario, J.; Boyle, J.S.; Detweiler, J.G.; Lutgens, B.W. Treatment of post-traumatic stress disorder nightmares at a veterans affairs medical center. J. Clin. Med. 2016, 5, 117. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, C.L. Pharmacologic treatment approaches for children and adolescents with posttraumatic stress disorder. Child Adolesc. Psychiatr. Clin. N. Am. 2003, 12, 251–269. [Google Scholar] [CrossRef]
- Zoladz, P.R.; Fleshner, M.; Diamond, D.M. Differential effectiveness of tianeptine, clonidine and amitriptyline in blocking traumatic memory expression, anxiety and hypertension in an animal model of PTSD. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 44, 1–16. [Google Scholar] [CrossRef]
- Shinba, T.; Shinozaki, T.; Mugishima, G. Clonidine immediately after immobilization stress prevents long-lasting locomotion reduction in the rat. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2001, 25, 1629–1640. [Google Scholar] [CrossRef]
- Olson, V.G.; Rockett, H.R.; Reh, R.K.; Redila, V.A.; Tran, P.M.; Venkov, H.A.; DeFino, M.C.; Hague, C.; Peskind, E.R.; Szot, P.; et al. The role of norepinephrine in differential response to stress in an animal model of posttraumatic stress disorder. Biol. Psychiatry 2011, 70, 441–448. [Google Scholar] [CrossRef]
- Gamache, K.; Pitman, R.K.; Nader, K. Preclinical evaluation of reconsolidation blockade by clonidine as a potential novel treatment for posttraumatic stress disorder. Neuropsychopharmacology 2012, 37, 2789–2796. [Google Scholar] [CrossRef]
- Alao, A.; Selvarajah, J.; Razi, S. The use of clonidine in the treatment of nightmares among patients with co-morbid PTSD and traumatic brain injury. Int. J. Psychiatry Med. 2012, 44, 165–169. [Google Scholar] [CrossRef]
- David Kinzie, J.; Leung, P. Clonidine in cambodian patients with posttraumatic stress disorder. J. Nerv. Ment. Dis. 1989, 177, 546–550. [Google Scholar] [CrossRef]
- Pitman, R.K.; Milad, M.R.; Igoe, S.A.; Vangel, M.G.; Orr, S.P.; Tsareva, A.; Gamache, K.; Nader, K. Systemic mifepristone blocks reconsolidation of cue-conditioned fear; Propranolol prevents this effect. Behav. Neurosci. 2011, 125, 632–638. [Google Scholar] [CrossRef]
- Dȩbiec, J.; LeDoux, J.E. Noradrenergic signaling in the amygdala contributes to the reconsolidation of fear memory: Treatment implications for PTSD. Ann. N. Y. Acad. Sci. 2006, 1071, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Romaguera, J.; Sotres-Bayon, F.; Mueller, D.; Quirk, G.J. Systemic Propranolol Acts Centrally to Reduce Conditioned Fear in Rats Without Impairing Extinction. Biol. Psychiatry 2009, 65, 887–892. [Google Scholar] [CrossRef]
- Vetere, G.; Piserchia, V.; Borreca, A.; Novembre, G.; Aceti, M.; Ammassari-Teule, M. Reactivating fear memory under propranolol resets pre-trauma levels of dendritic spines in basolateral amygdala but not dorsal hippocampus neurons. Front. Behav. Neurosci. 2013, 7, 211. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, P.J.; Giustino, T.F.; Seemann, J.R.; Maren, S. Noradrenergic blockade stabilizes prefrontal activity and enables fear extinction under stress. Proc. Natl. Acad. Sci. USA 2015, 112, E3729–E3737. [Google Scholar] [CrossRef] [PubMed]
- Dębiec, J.; Díaz-Mataix, L.; Bush, D.E.A.; Doyère, V.; Ledoux, J.E. The amygdala encodes specific sensory features of an aversive reinforcer. Nat. Neurosci. 2010, 13, 536–537. [Google Scholar] [CrossRef]
- Huang, B.; Zhu, H.; Zhou, Y.; Liu, X.; Ma, L. Unconditioned- and conditioned-stimuli induce differential memory reconsolidation and β-AR-dependent CREB activation. Front. Neural Circuits 2017, 11, 53. [Google Scholar] [CrossRef]
- Zaidi, S.; Atrooz, F.; Valdez, D.; Liu, H.; Kochi, C.; Bond, R.A.; Salim, S. Protective effect of propranolol and nadolol on social defeat-induced behavioral impairments in rats. Neurosci. Lett. 2020, 725, 134892. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 10, 89. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Model List of Essential Medicines: 22nd List. 2021. Available online: https://apps.who.int/iris/handle/10665/345533 (accessed on 19 July 2022).



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szeleszczuk, Ł.; Frączkowski, D. Propranolol versus Other Selected Drugs in the Treatment of Various Types of Anxiety or Stress, with Particular Reference to Stage Fright and Post-Traumatic Stress Disorder. Int. J. Mol. Sci. 2022, 23, 10099. https://doi.org/10.3390/ijms231710099
Szeleszczuk Ł, Frączkowski D. Propranolol versus Other Selected Drugs in the Treatment of Various Types of Anxiety or Stress, with Particular Reference to Stage Fright and Post-Traumatic Stress Disorder. International Journal of Molecular Sciences. 2022; 23(17):10099. https://doi.org/10.3390/ijms231710099
Chicago/Turabian StyleSzeleszczuk, Łukasz, and Dawid Frączkowski. 2022. "Propranolol versus Other Selected Drugs in the Treatment of Various Types of Anxiety or Stress, with Particular Reference to Stage Fright and Post-Traumatic Stress Disorder" International Journal of Molecular Sciences 23, no. 17: 10099. https://doi.org/10.3390/ijms231710099
APA StyleSzeleszczuk, Ł., & Frączkowski, D. (2022). Propranolol versus Other Selected Drugs in the Treatment of Various Types of Anxiety or Stress, with Particular Reference to Stage Fright and Post-Traumatic Stress Disorder. International Journal of Molecular Sciences, 23(17), 10099. https://doi.org/10.3390/ijms231710099