
The Novel Association of Early Apoptotic Circulating Tumor Cells with Treatment Outcomes in Breast Cancer Patients

 , , ,
, , ,
Abstract
:1. Background
2. Results
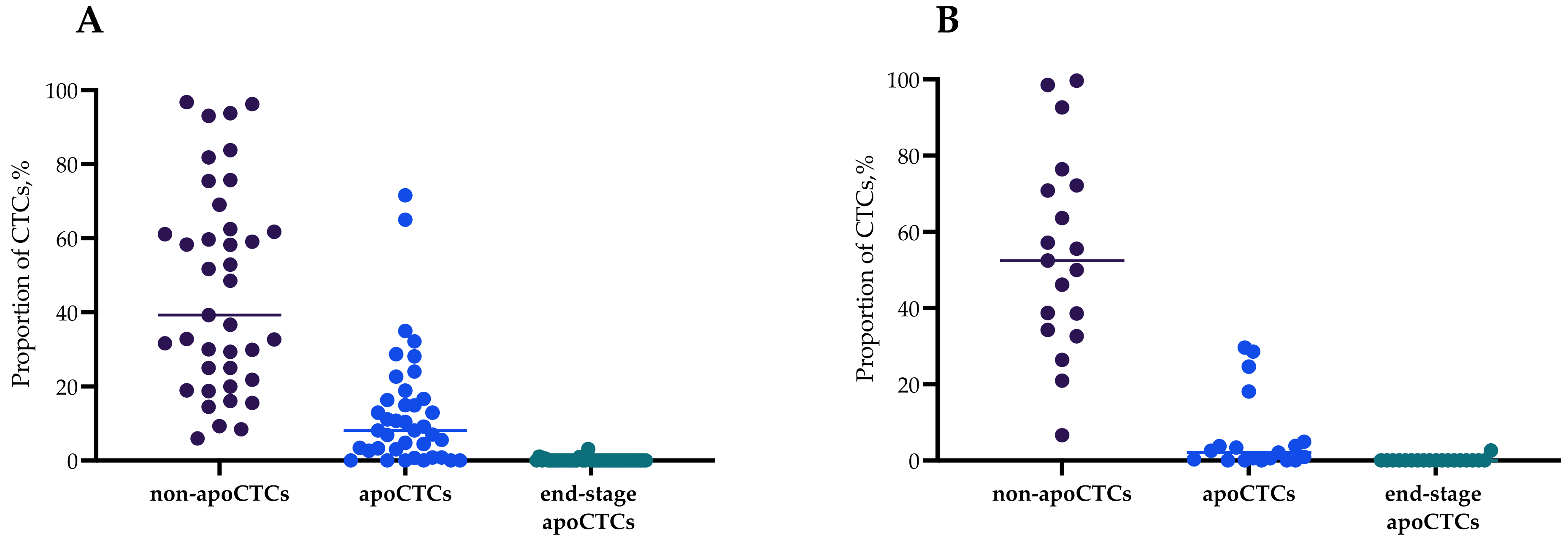
2.1. apoCTCs, Non-apoCTCs and End-Stage apoCTCs in Peripheral Blood of BC Patients
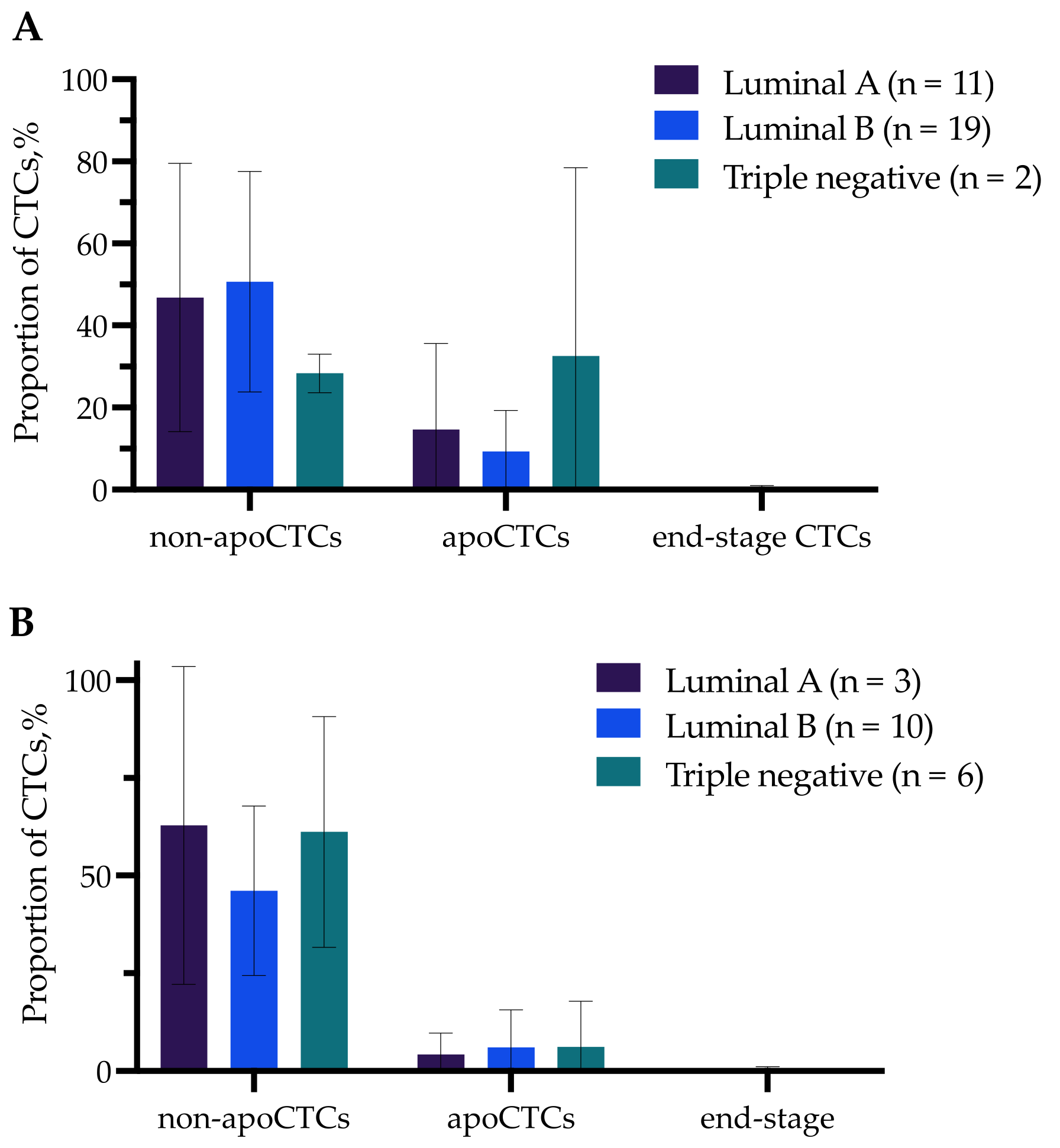
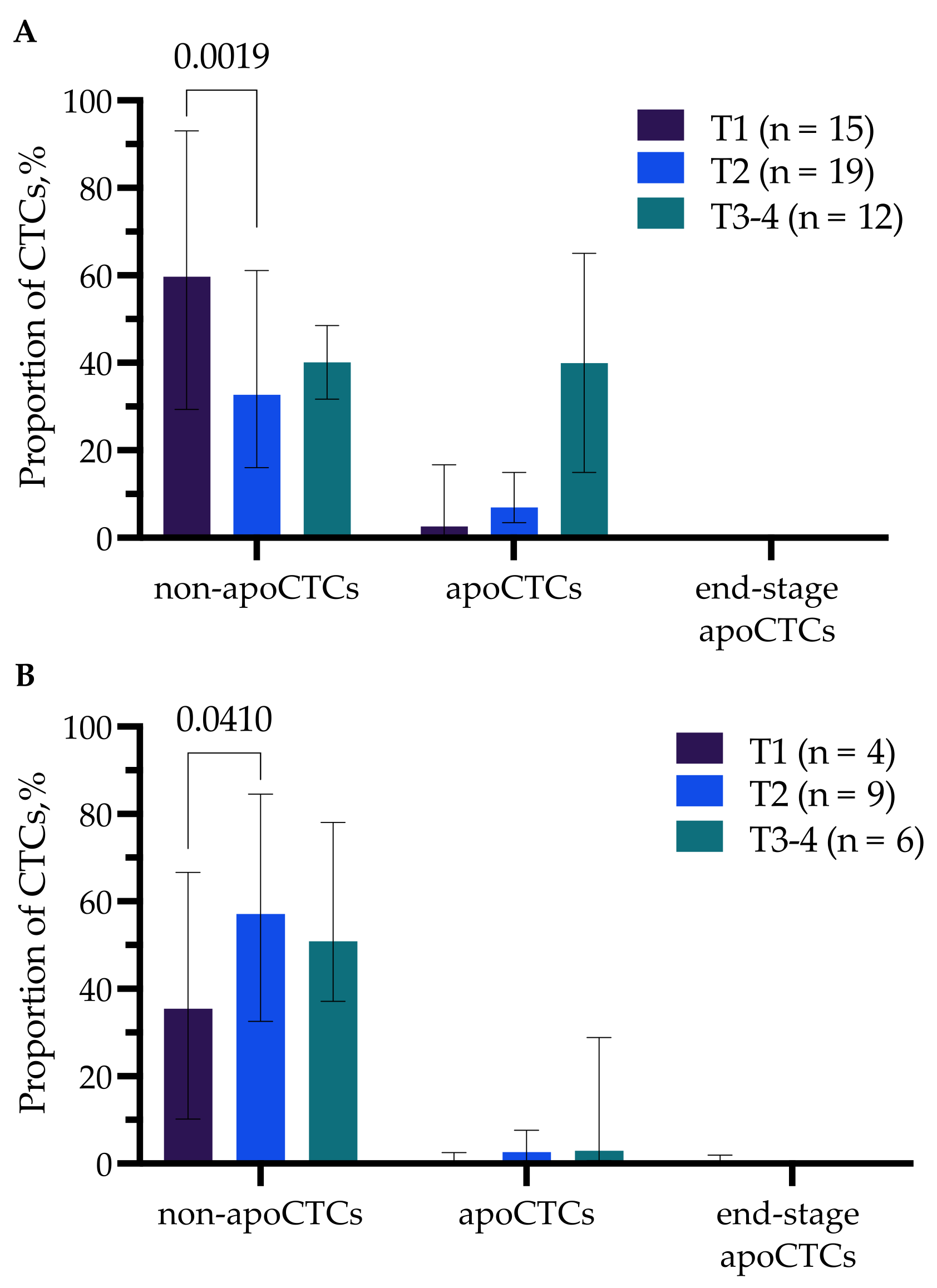
2.2. apoCTCs, Non-apoCTCs and End-Stage apoCTCs in Breast Cancer Patients in Relation to Clinicopathological Characteristics
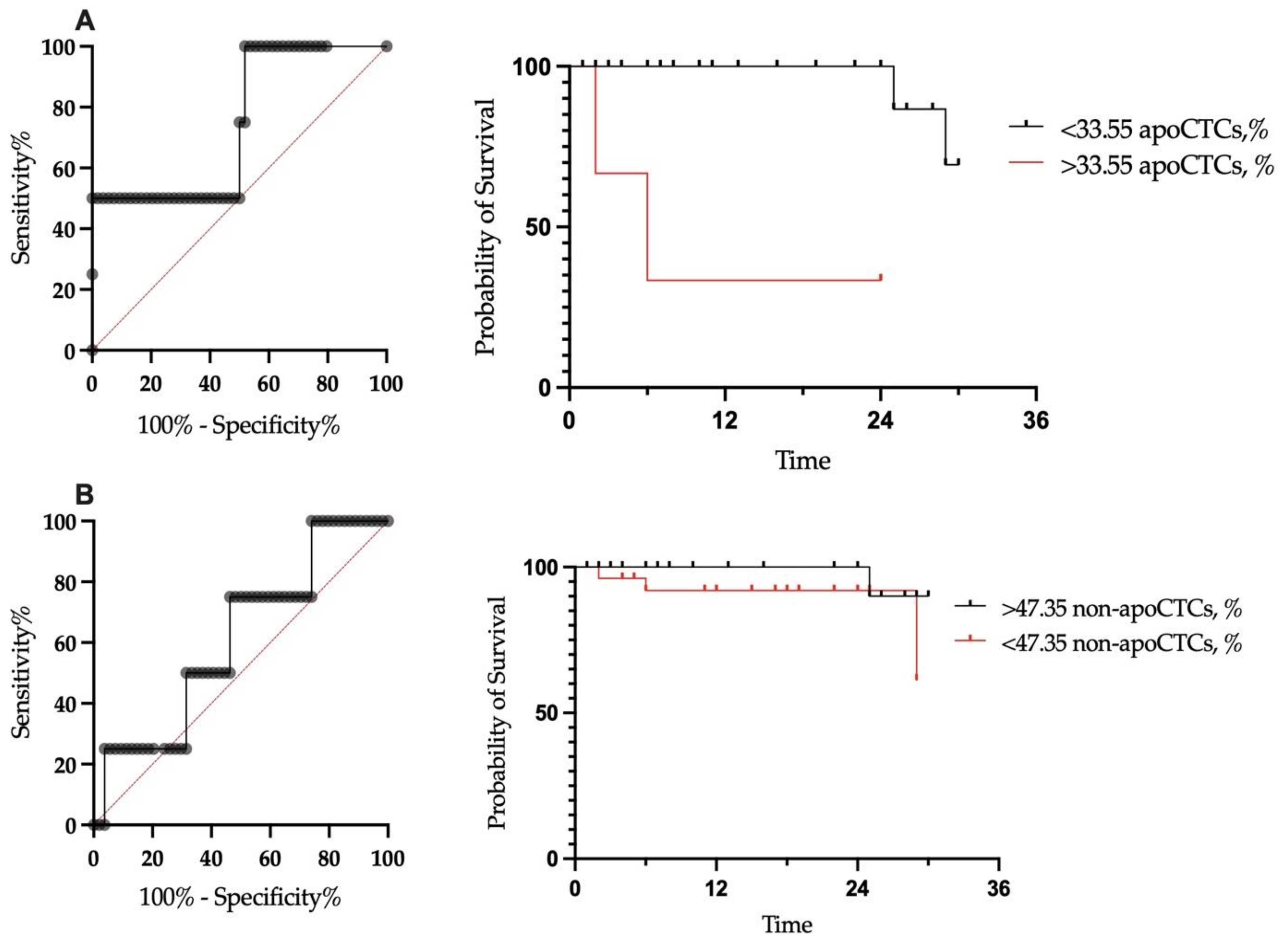
2.3. Prognostic Significance of apoCTCs and Non-apoCTCs for Metastasis-Free Survival
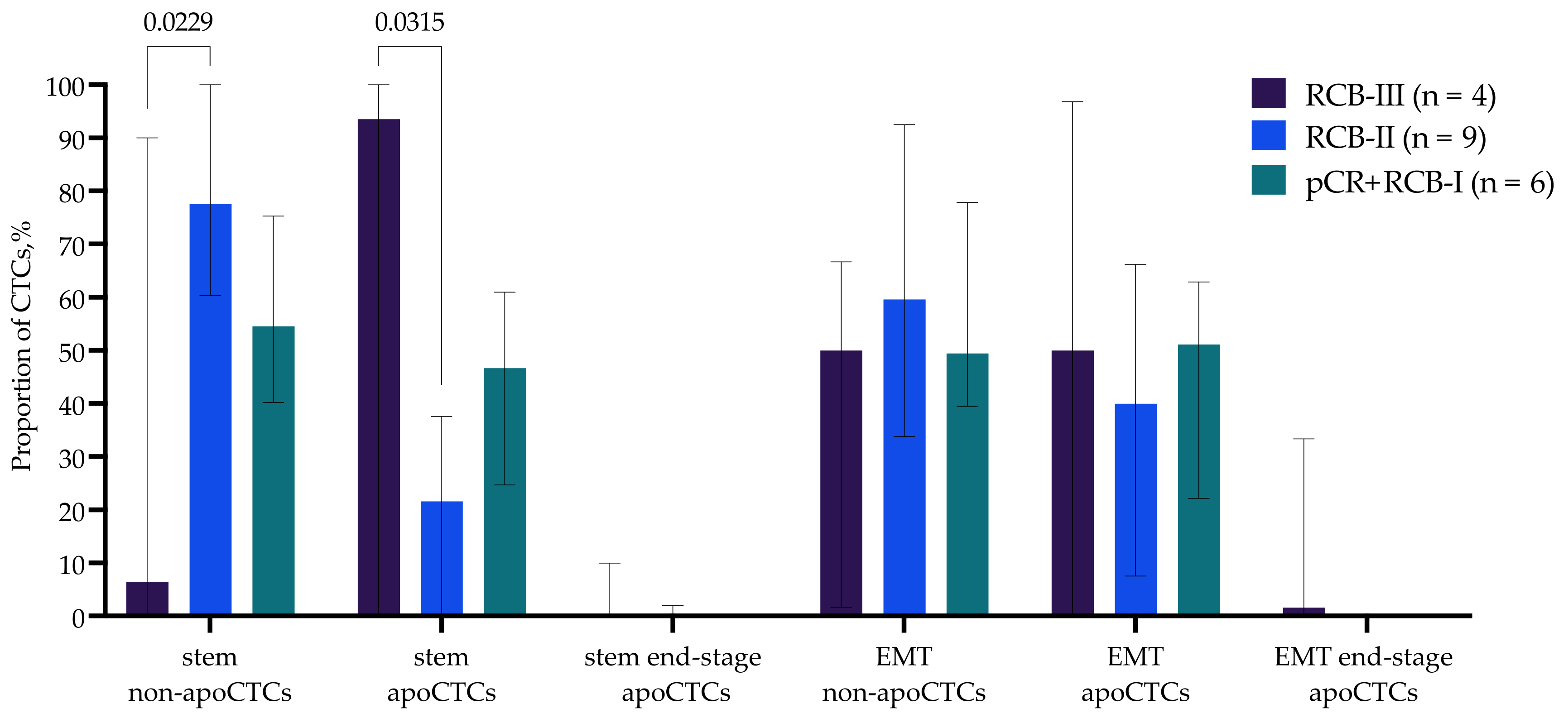
2.4. Association of apoCTCs Proportion with NAC Response
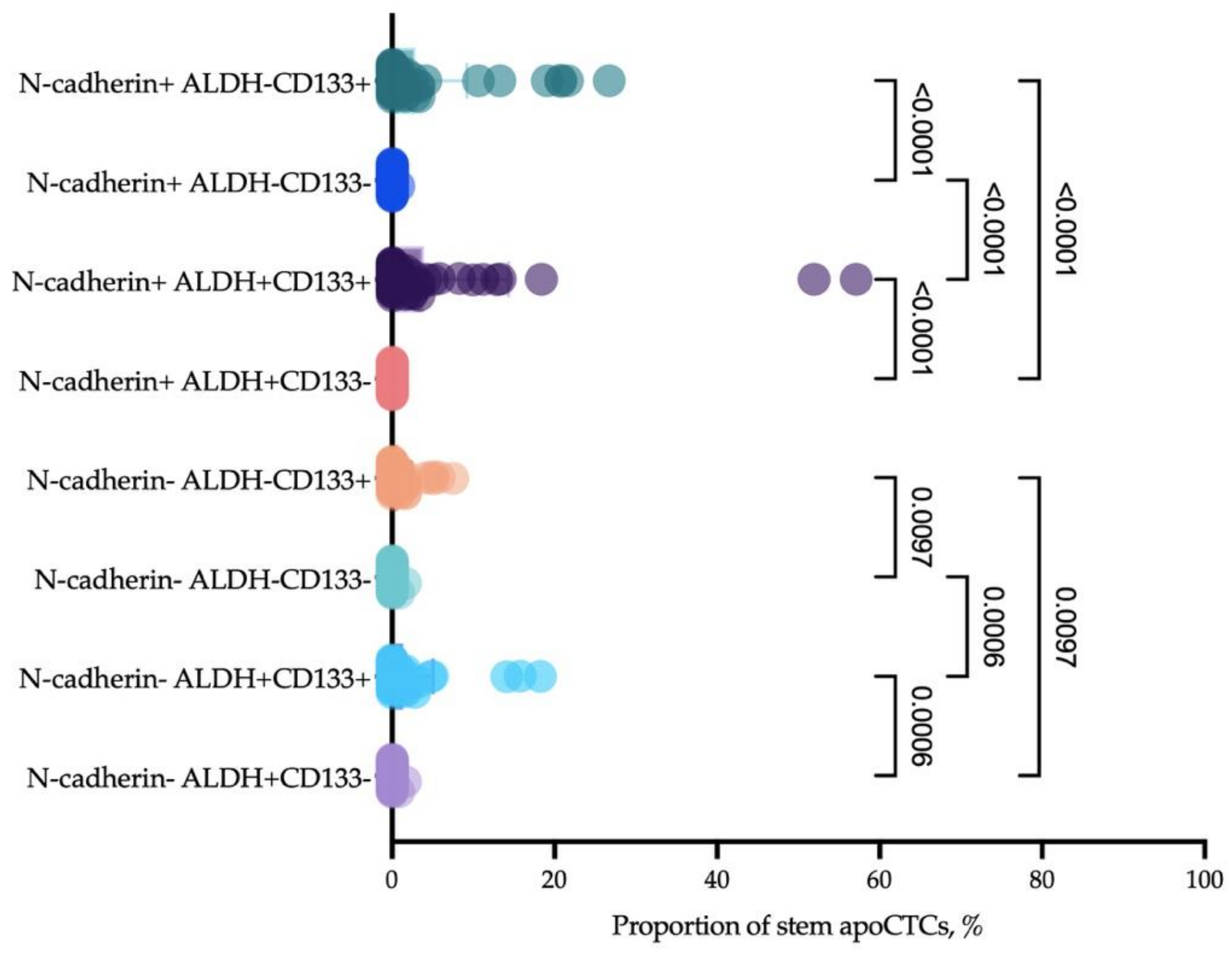
2.5. Phenotypic Characteristics of Cells Associated with Response Neoadjuvant Chemotherapy
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Blood Specimen Collection and Processing for CTCs Immunophenotyping
4.3. Flow Cytometry
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Primeaux, M.; Gowrikumar, S.; Dhawan, P. Role of CD44 isoforms in epithelial-mesenchymal plasticity and metastasis. Clin. Exp. Metastasis 2022, 39, 391–406. [Google Scholar] [CrossRef]
- Jolly, M.K.; Tripathi, S.C.; Jia, D.; Mooney, S.M.; Celiktas, M.; Hanash, S.M.; Mani, S.A.; Pienta, K.J.; Ben-Jacob, E.; Levine, H. Stability of the hybrid epithelial/mesenchymal phenotype. Oncotarget 2016, 7, 27067–27084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, D.; Jolly, M.K.; Tripathi, S.C.; Hollander, P.D.; Huang, B.; Lu, M.; Celiktas, M.; Ramirez-Peña, E.; Ben-Jacob, E.; Onuchic, J.N.; et al. Distinguishing mechanisms underlying EMT tristability. Cancer Converg. 2017, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Antin, P.; Berx, G.; Blanpain, C.; Brabletz, T.; Bronner, M.; Campbell, K.; Cano, A.; Casanova, J.; Christofori, G.; et al. Guidelines and definitions for research on epithelial–Mesenchymal transition. Nat. Rev. Mol. Cell Biol. 2020, 21, 341–352. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Li, Y.; Zhang, X. Stemness-Related Markers in Cancer. Cancer Transl. Med. 2017, 3, 87–95. [Google Scholar]
- Ning, Y.; Zhang, W.; Hanna, D.L.; Yang, D.; Okazaki, S.; Berger, M.D.; Miyamoto, Y.; Suenaga, M.; Schirripa, M.; El-Khoueiry, A.; et al. Clinical relevance of EMT and stem-like gene expression in circulating tumor cells of metastatic colorectal cancer patients. Pharm. J. 2018, 18, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Bode, A.M.; Dong, Z. Circulating tumor cells: Moving biological insights into detection. Theranostics 2017, 7, 2606. [Google Scholar] [CrossRef] [PubMed]
- Gkountela, S.; Szczerba, B.; Donato, C.; Aceto, N. Recent advances in the biology of human circulating tumour cells and metastasis. ESMO Open 2016, 1, e000078. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Wang, C.; Xie, M.; Zhu, C.; Shu, Y.; Tang, J.; Guan, X. Heterogeneity of CTC contributes to the organotropism of breast cancer. Biomed. Pharmacother. 2021, 137, 111314. [Google Scholar] [CrossRef] [PubMed]
- Lucci, A.; Hall, C.S.; Lodhi, A.K.; Bhattacharyya, A.; Anderson, A.E.; Xiao, L.; Bedrosian, I.; Kuerer, H.M.; Krishnamurthy, S. Circulating tumour cells in non-metastatic breast cancer: A prospective study. Lancet Oncol. 2012, 13, 688–695. [Google Scholar] [CrossRef]
- Massague, J.; Obenauf, A.C. Metastatic colonization by circulating tumour cells. Nature 2016, 529, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Kallergi, G.; Konstantinidis, G.; Markomanolaki, H.; Papadaki, M.A.; Mavroudis, D.; Stournaras, C.; Georgoulias, V.; Agelaki, S. Apoptotic Circulating Tumor Cells in Early and Metastatic Breast Cancer. Patients. Mol. Cancer Ther. 2013, 12, 1886–1895. [Google Scholar] [CrossRef] [Green Version]
- Jansson, S.; Bendahl, P.-O.; Larsson, A.-M.; Aaltonen, K.E.; Rydén, L. Prognostic impact of circulating tumor cell apoptosis and clusters in serial blood samples from patients with metastatic breast cancer in a prospective observational cohort. BMC Cancer 2016, 16, 433. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Sipkins, D.A.; Pitsillides, C.M.; Novak, J.; Georgakoudi, I.; Lin, C.P. Real-time Detection of Circulating Apoptotic Cells by in vivo flow cytometry. Mol. Imaging 2005, 4, 415–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, S.; Tripathy, D.; Frenkel, E.P.; Shete, S.; Naftalis, E.Z.; Huth, J.F.; Beitsch, P.D.; Leitch, M.; Hoover, S.; Euhus, D.; et al. Circulating tumor cells in patients with breast cancer dormancy. Clin. Cancer Res. 2004, 10, 8152–8162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, W.; Wang, X.; Liu, G.; Eden, H.; Chen, X. Molecular imaging of apoptosis: From micro to macro. Theranostics 2015, 5, 559–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zembruski, N.C.; Stache, V.; Haefeli, W.E.; Weiss, J. 7-Aminoactinomycin D for apoptosis staining in flow cytometry. Anal. Biochem 2012, 429, 79–81. [Google Scholar] [CrossRef]
- Lee, K.L.; Gibson, F.M. Early Apoptotic Cells Detected by 7-Aminoactinomycin and Annexin V Are Positive for Fluorescence Tagged Activated Caspase-9 Inhibitor (Red-LEHD-FMK). Blood 2008, 112, 4728. [Google Scholar] [CrossRef]
- De Toro, J.; Herschlik, L.; Waldner, C. Emerging Roles of Exosomes in Normal and Pathological Conditions: New Insights for Diagnosis and Therapeutic Applications. Front. Immunol. 2015, 6, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hench, I.B.; Hench, J.; Tolnay, M. Liquid biopsy in clinical management of breast, lung, and colorectal cancer. Front. Med. 2018, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Fei, F.; Du, Y.; Di, G.; Wu, J.; Shao, Z. Are changes in circulating tumor cell (CTC) count associated with the response to neoadjuvant chemotherapy in local advanced breast cancer? A meta-analysis. Oncol. Res. Treat. 2014, 37, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Michiels, S.; Riethdorf, S.; Mueller, V.; Esserman, L.J.; Lucci, A.; Naume, B.; Horiguchi, J.; Gisbert-Criado, R.; Sleijfer, S.; et al. Circulating Tumor Cells in Breast Cancer Patients Treated by Neoadjuvant Chemotherapy: A Meta-analysis. J. Natl. Cancer Inst. 2018, 110, 560–567. [Google Scholar] [CrossRef]
- Chaffer, C.L.; Weinberg, R.A. A perspective on cancer cell metastasis. Science 2011, 331, 1559–1564. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.A.; Gores, G.J. Physiology and pathophysiology of apoptosis in epithelial cells of the liver, pancreas, and intestine. Am. J. Physiol 1997, 273, G1174–G1188. [Google Scholar] [CrossRef] [PubMed]
- Altoe, M.L.; Kalinsky, K.; Marone, A.; Kim, H.K.; Guo, H.; Hibshoosh, H.; Tejada, M.; Crew, K.D.; Accordino, M.K.; Trivedi, M.S.; et al. Effects of neoadjuvant chemotherapy on the contralateral non-tumor-bearing breast assessed by diffuse optical tomography. Breast Cancer Res. 2021, 23, 16. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Choi, Y.; Yoon, D.S.; Lee, J.W.; Yoon, G.S.; Choi, W.J.; Han, S.H. Comparison of Efficiency of Self-renewal and Differentiation Potential in Tendon-derived Mesenchymal Stem Cells Isolated by Magnetic-activated Cell Sorting Method or Colony Picking Method. J. Korean Foot Ankle Soc. 2014, 18, 100–107. [Google Scholar] [CrossRef]
- Kallergi, G.; Papadaki, M.A.; Politaki, E.; Mavroudis, D.; Georgoulias, V.; Agelaki, S. Epithelial to mesenchymal transition markers expressed in circulating tumour cells of early and metastatic breast cancer patients. Breast Cancer Res. 2011, 13, R59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strilic, B.; Offermanns, S. Intravascular Survival and Extravasation of Tumor Cells. Cancer Cell 2017, 32, 282–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hariharan, C.; Tao, Y.; Jiang, L.; Wen, X.; Liao, J. Assay Technologies for Apoptosis and Autophagy. Med. Drug Discov. 2021, 11, 100100. [Google Scholar] [CrossRef]
- Wlodkowic, D.; Skommer, J.; Pelkonen, J. Towards an understanding of apoptosis detection by SYTO dyes. Cytom. A 2007, 71, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Cevatemre, B.; Ulukaya, E.; Sarimahmut, M.; Oral, A.Y.; Frame, F.M. The M30 assay does not detect apoptosis in epithelial-derived cancer cells expressing low levels of cytokeratin 18. Tumour Biol. 2015, 36, 6857–6865. [Google Scholar] [CrossRef]
- Eroglu, Z.; Fielder, O.; Somlo, G. Analysis of circulating tumor cells in breast cancer. J. Natl. Compr. Cancer Netw. 2013, 11, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, T.M.; Riethdorf, S.; Nees, J.; Hartkopf, A.D.; Schönfisch, B.; Domschke, C.; Sprick, M.R.; Schütz, F.; Brucker, S.Y.; Stefanovic, S.; et al. Impact of apoptotic circulating tumor cells (aCTC) in metastatic breast cancer. Breast Cancer Res. Treat. 2016, 160, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Zhao, W.; Zhang, J.; Chen, W.; Xie, T.; Wang, L.; Fan, W.; Xie, S.; Shen, J.; Zheng, H.; et al. Evaluation of the diagnostic value of circulating tumor cells with CytoSorter CTC capture system in patients with breast cancer. Cancer Med. 2020, 9, 1638–1647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, J.; Zou, K.; Yang, C.; Leng, X.; Xu, Y. Clinicopathological and prognostic significance of circulating tumor cells in patients with esophageal cancer: A meta-analysis. Onco Targets Ther. 2018, 11, 8053–8061. [Google Scholar] [CrossRef] [Green Version]
- Tong, B.; Xu, Y.; Zhao, J.; Chen, M.; Xing, J.; Zhong, W.; Wang, M. Prognostic significance of circulating tumor cells in non-small cell lung cancer patients undergoing chemotherapy. Oncotarget 2017, 8, 86615–86624. [Google Scholar] [CrossRef] [Green Version]
- Pang, S.; Li, H.; Xu, S.; Feng, L.; Ma, X.; Chu, Y.; Zou, B.; Wang, S.; Zhou, G. Circulating tumour cells at baseline and late phase of treatment provide prognostic value in breast cancer. Sci. Rep. 2021, 11, 13441. [Google Scholar] [CrossRef]
- Xu, Y.; So, C.; Lam, H.-M.; Fung, M.-C.; Tsang, S.-Y. Apoptosis Reversal Promotes Cancer Stem Cell-Like Cell Formation. Neoplasia 2018, 20, 295–303. [Google Scholar] [CrossRef]
- Loh, C.Y.; Chai, J.Y.; Tang, T.F.; Wong, W.F.; Sethi, G.; Shanmugam, M.K.; Chong, P.P.; Looi, C.Y. The E-Cadherin and N-Cadherin Switch in Epithelial-to-Mesenchymal Transition: Signaling, Therapeutic Implications, and Challenges. Cells 2019, 8, 1118. [Google Scholar] [CrossRef] [Green Version]
- Yiding, C.; Zhongyi, H. Differences Between the Quality Aspects of Various Generic and Branded Docetaxel Formulations. Curr. Med. Res. Opin. 2021, 37, 1421–1433. [Google Scholar] [CrossRef]
- Mohsin, S.K.; Weiss, H.L.; Gutierrez, M.C.; Chamness, G.C.; Schiff, R.; DiGiovanna, M.P.; Wang, C.-X.; Hilsenbeck, S.G.; Osborne, C.K.; Allred, D.C.; et al. Neoadjuvant trastuzumab induces apoptosis in primary breast cancers. J. Clin. Oncol. 2005, 23, 2460–2468. [Google Scholar] [CrossRef] [PubMed]
- Nunes, T.; Hamdan, D.; Leboeuf, C.; El Bouchtaoui, M.; Gapihan, G.; Nguyen, T.T.; Meles, S.; Angeli, E.; Ratajczak, P.; Lu, H.; et al. Targeting Cancer Stem Cells to Overcome Chemoresistance. Int. J. Mol. Sci. 2018, 19, 4036. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Examination of Tumor Regression Grading Systems in Breast Cancer Patients Who Received Neoadjuvant Therapy. Pathol. Oncol. Res. 2020, 26, 2747–2754. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Frequency, % (n) | |
|---|---|---|
| Age | <35 | 5.17% (3/58) |
| 35–50 | 32.76% (19/58) | |
| >50 | 62.07% (36/58) | |
| Menstrual function | Premenopausal | 34.48% (20/58) |
| Postmenopausal | 65.52% (38/58) | |
| Tumor size (T) | 1 | 32.76% (19/58) |
| 2 | 53.45% (31/58) | |
| 3 | 5.17% (3/58) | |
| 4 | 8.62% (5/58) | |
| Stage | I | 20.69% (12/58) |
| IIA | 34.48% (20/58) | |
| IIB | 25.86% (15/58) | |
| IIIA | 3.45% (2/58) | |
| IIIB | 12.07% (7/58) | |
| IIIC | 3.45% (2/58) | |
| Molecular subtype | Luminal A | 25.86% (15/58) |
| Luminal B | 56.90% (33/58) | |
| Triple negative | 15.52% (9/58) | |
| HER2 positive | 1.72% (1/58) | |
| Tumor grade | 1 | 17.24% (10/58) |
| 2 | 67.24% (39/58) | |
| 3 | 15.52% (9/58) | |
| Estrogen receptor α | positive | 82.76% (48/58) |
| negative | 17.24% (10/58) | |
| Progesterone receptor | positive | 70.69% (41/58) |
| negative | 29.31% (17/58) | |
| HER2 | positive | 25.86% (15/58) |
| negative | 74.14% (43/58) | |
| Ki67 expression | <20% | 34.48% (20/58) |
| >20% | 65.52% (38/58) | |
| Lymph node metastasis | Yes | 37.93% (22/58) |
| No | 62.07% (36/58) | |
| Distant metastasis | Yes | 6.90% (4/58) |
| No | 87.93% (51/58) | |
| No data | 5.17% (3/58) | |
| Neoadjuvant chemotherapy | Yes | 31.03% (18/58) |
| No | 68,97% (40/58) | |
| Univariate | Multivariate | ||||
|---|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | ||
| apoCTCs | <33.55% | ref | ref | ||
| >33.55% | 27.62 (1.74–338.20) | 0.0001 | 13.73 (1.34–182.33) | 0.0002 | |
| Neoadjuvant chemotherapy | No | ref | ref | ||
| Yes | 0.31 (0.03–3.44) | 0.3446 | 0.48 (0.04–5.93) | 0.4532 | |
| Menopausal | No | ref | ref | ||
| Yes | 1.47 (0.29–23.98) | 0.2830 | 0.33 (0.03–6.19) | 0.4011 | |
| Molecular type | Lum | ref | ref | ||
| TN | 0.32 (0.02–5.28) | 0.4383 | 0.27 (0.02–5.617) | 0.3998 | |
| Ki67 | <20 | ref | ref | ||
| >20 | 0.94 (0.08–10.49) | 0.9651 | 1.04 (0.12–7.13) | 0.7782 | |
| Stage | I–II | ref | ref | ||
| III–IV | 1.11 (0.19–2.42) | 0.9995 | 1.15 (0.20–6.33) | 0.7811 | |
| Grade | 1 | ref | ref | ||
| 2 | 0.18 (0.01–3.15) | 0.1712 | 0.28 (0.01–2.88) | 0.3190 | |
| 3 | 0.83 (0.05–12.50) | 0.5466 | 1.93 (0.06–17.35) | 0.3552 | |
| Lymph node metastasis | No | ref | ref | ||
| Yes | 1.72 (0.23–12.70) | 0.9963 | 2.95 (0.22–31.75) | 0.3320 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigoryeva, E.S.; Tashireva, L.A.; Alifanov, V.V.; Savelieva, O.E.; Vtorushin, S.V.; Zavyalova, M.V.; Cherdyntseva, N.V.; Perelmuter, V.M. The Novel Association of Early Apoptotic Circulating Tumor Cells with Treatment Outcomes in Breast Cancer Patients. Int. J. Mol. Sci. 2022, 23, 9475. https://doi.org/10.3390/ijms23169475
Grigoryeva ES, Tashireva LA, Alifanov VV, Savelieva OE, Vtorushin SV, Zavyalova MV, Cherdyntseva NV, Perelmuter VM. The Novel Association of Early Apoptotic Circulating Tumor Cells with Treatment Outcomes in Breast Cancer Patients. International Journal of Molecular Sciences. 2022; 23(16):9475. https://doi.org/10.3390/ijms23169475
Chicago/Turabian StyleGrigoryeva, Evgeniya S., Liubov A. Tashireva, Vladimir V. Alifanov, Olga E. Savelieva, Sergey V. Vtorushin, Marina V. Zavyalova, Nadezhda V. Cherdyntseva, and Vladimir M. Perelmuter. 2022. "The Novel Association of Early Apoptotic Circulating Tumor Cells with Treatment Outcomes in Breast Cancer Patients" International Journal of Molecular Sciences 23, no. 16: 9475. https://doi.org/10.3390/ijms23169475
APA StyleGrigoryeva, E. S., Tashireva, L. A., Alifanov, V. V., Savelieva, O. E., Vtorushin, S. V., Zavyalova, M. V., Cherdyntseva, N. V., & Perelmuter, V. M. (2022). The Novel Association of Early Apoptotic Circulating Tumor Cells with Treatment Outcomes in Breast Cancer Patients. International Journal of Molecular Sciences, 23(16), 9475. https://doi.org/10.3390/ijms23169475