
Vaccine for Diabetes—Where Do We Stand?

 , ,
, ,  , , , , and
, , , , and 
Abstract
1. Introduction
2. Vaccination
2.1. Early Diabetes Prevention
2.2. Rationale behind Vaccine Adjuvant Action
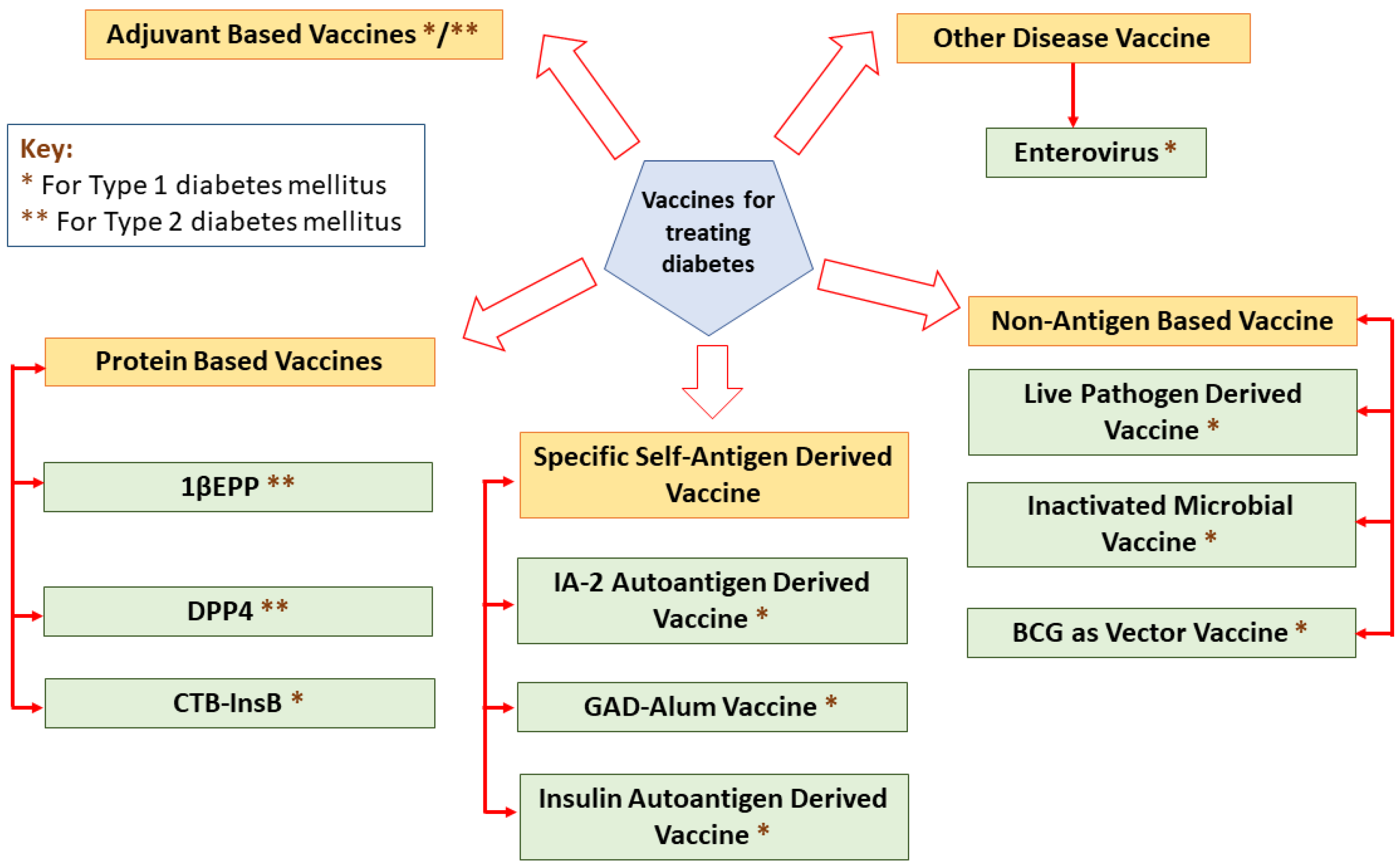
3. Newly Designed Vaccine Products
3.1. Protein-Based Approach in Vaccine Production
3.1.1. IL-1-Targeted Epitope Peptide (1EPP) as a New Vaccine Product for T2DM
3.1.2. Dipeptidyl Peptidase-4 Inhibitor (DPP4) as Novel Vaccine Product for T2DM
3.1.3. CTB-InsB Vaccination Product to Treat T1DM
3.2. Specific Self-Antigens Approach in Vaccine Production
3.2.1. IA-2 as New Vaccine Product for T1DM
3.2.2. Glutamic Acid Decarboxylase 65-kD (GAD65): A New Vaccine Product for T1DM
3.2.3. Insulin as a Target in New Vaccine Product for T1DM
3.3. Non-Antigen Specific Approach in Vaccine Production
3.3.1. Live Pathogen Salmonella as Vector Vaccine
3.3.2. Inactivated Microbial Vaccines
3.3.3. BCG as Vector Vaccine in Clinical Trial Studies
4. Potential of Other Disease-Vaccines in Treating Diabetes
Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 1EPP | IL-1-targeted epitope peptide vaccine adjuvant with polylactic acid microparticles |
| ADA | American Diabetes Association |
| Alum | Aluminum |
| APC | Antigen presenting cells |
| BCG | Bacillus Calmette–Guerin |
| CFA | Complete Freund’s adjuvant |
| CTB | Cholera toxin B subunit |
| DC | Dendritic cell |
| DM | Diabetes mellitus |
| DNA | Deoxyribonucleic acid |
| DPP4 | Dipeptidyl-peptidase-4-inhibitor |
| EV | Enteroviruses |
| FDA | Food and Drug Administration |
| GAD65 | Glutamic acid decarboxylase 65-kD antibody |
| GFAP | Glial fibrillary acidic protein |
| GLP | Glucagon-like-peptide |
| IA-2 | Insulinoma-associated protein 2 |
| IDF | International Diabetes Federation |
| IFA | Incomplete Freund’s adjuvant |
| INSB | B chain of insulin |
| IL-1 | Interleukin-1 cytokine |
| IL-10 | Interleukin-10 |
| MHC | Major histocompatibility complexes |
| MP | Microparticle |
| NOD | Non-obese diabetic |
| PRR | Pattern recognition receptors |
| T1DM | Type 1 diabetes mellitus |
| T2DM | Type 2 diabetes mellitus |
| Th0 | Naive helper T cell |
| Th1 | Cytotoxic helper T cell |
| Th2 | Humoral helper T cell |
| TLR | Toll-like receptor |
| TNF | Tumor necrosis factor |
| Treg cells | Regulatory T cells |
| WHO | World Health Organization |
| ZnT8 | Zinc transporter isoform 8 |
References
- Nair, M. Diabetes mellitus, part 1: Physiology and complications. Br. J. Nurs. 2007, 16, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Rewers, M.; Gottlieb, P. Immunotherapy for the Prevention and Treatment of Type 1 Diabetes: Human trials and a look into the future. Diabetes Care 2009, 32, 1769–1782. [Google Scholar] [CrossRef]
- Alwan, A. Raising the priority accorded to diabetes in global health and development: A promising response. Int. J. Diabetes Mellit. 2010, 3, 139–140. [Google Scholar] [CrossRef][Green Version]
- Slim, I.B.H.S. Cardiovascular risk in type 1 diabetes mellitus. Indian J. Endocrinol. Metab. 2013, 17 (Suppl. 1), S7–S13. [Google Scholar] [CrossRef]
- Diabetes. Available online: http://www.who.int/health-topics/diabetes#tab=tab_1 (accessed on 1 June 2022).
- Hanson, M.A.; Gluckman, P.D.; Ma, R.C.; Matzen, P.; Biesma, R.G. Early life opportunities for prevention of diabetes in low and middle income countries. BMC Public Health 2012, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kaveeshwar, S.A.; Cornwall, J. The current state of diabetes mellitus in India. Australas Med. J. 2014, 7, 45–48. [Google Scholar] [CrossRef]
- Maffi, P.; Secchi, A. The Burden of Diabetes: Emerging Data. Dev. Ophthalmol. 2017, 60, 1–5. [Google Scholar]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of diabetes and diabetes-related complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef]
- Bagchi, D.; Das, A.; Roy, S. Wound Healing, Tissue Repair, and Regeneration in Diabetes; Academic Press: London, UK, 2020; p. 609. [Google Scholar]
- Rother, K.I. Diabetes treatment–bridging the divide. N. Engl. J. Med. 2007, 356, 1499–1501. [Google Scholar] [CrossRef]
- Piero, M.N.; Nzaro, G.M.; Njagi, J.M. Diabetes mellitus-a devastating metabolic disorder. Asian J. Biomed. Pharm. Sci. 2015, 5, 1. [Google Scholar]
- Staeva, T.P.; Chatenoud, L.; Insel, R.; Atkinson, M.A. Recent lessons learned from prevention and recent-onset type 1 diabetes immunotherapy trials. Diabetes 2013, 62, 9–17. [Google Scholar] [CrossRef] [PubMed][Green Version]
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.I.; et al. Type 2 diabetes mellitus. Nat. Rev. Dis. Prim. 2015, 1, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Orban, T.; Kent, S.C.; Malik, P.; Milner, J.D.; Schuster, K.; Jackson, R.A.; Hafler, D.A. Heterophile antibodies indicate progression of autoimmunity in human type 1 diabetes mellitus before clinical onset. Autoimmunity 2001, 34, 247–264. [Google Scholar] [CrossRef] [PubMed]
- Orban, T.; Kis, J.T. Prevention of type 1 diabetes mellitus using a novel vaccine. Ther. Adv. Endocrinol. Metab. 2011, 2, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. International Diabetes Federation: A consensus on Type 2 diabetes prevention. Diabet. Med. 2007, 24, 451–463. [Google Scholar] [CrossRef]
- Li, G.; Zhang, P.; Wang, J.; Gregg, E.W.; Yang, W.; Gong, Q.; Li, H.; Li, H.; Jiang, Y.; An, Y.; et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: A 20-year follow-up study. Lancet 2008, 371, 1783–1789. [Google Scholar] [CrossRef]
- Van Belle, T.L.; Coppieters, K.T.; Von Herrath, M.G. Type 1 diabetes: Etiology, immunology, and therapeutic strategies. Physiol. Rev. 2011, 91, 79–118. [Google Scholar] [CrossRef]
- Lernmark, Å.; Larsson, H.E. Immune therapy in type 1 diabetes mellitus. Nat. Rev. Endocrinol. 2013, 9, 92–103. [Google Scholar] [CrossRef]
- Gelber, C.; Paborsky, L.; Singer, S.; McAteer, D.; Tisch, R.; Jolicoeur, C.; Buelow, R.; McDevitt, H.; Fathman, C.G. Isolation of nonobese diabetic mouse T-cells that recognize novel autoantigens involved in the early events of diabetes. Diabetes 1994, 43, 33–39. [Google Scholar] [CrossRef]
- Maclaren, N.; Lan, M.; Coutant, R.; Schatz, D.; Silverstein, J.; Muir, A.; Clare-Salzer, M.; She, J.X.; Malone, J.; Crockett, S.; et al. Only multiple autoantibodies to islet cells (ICA), insulin, GAD65, IA-2 and IA-2β predict immune-mediated (type 1) diabetes in relatives. J. Autoimmun. 1999, 12, 279–287. [Google Scholar] [CrossRef]
- Sabbah, E.; Savola, K.; Kulmala, P.; Veijola, R.; Vahasalo, P.; Karjalainen, J.; Akerblom, H.K.; Knip, M. Childhood Diabetes in Finland Study Group. Diabetes-associated autoantibodies in relation to clinical characteristics and natural course in children with newly diagnosed type 1 diabetes. J. Clin. Endocrinol. Metab. 2011, 84, 1534–1539. [Google Scholar]
- Montgomery, S.M.; Ehlin, A.G.C.; Ekbom, A.; Wakefield, A.J. Pertussis infection in childhood and subsequent type 1 diabetes mellitus. Diabet. Med. 2002, 19, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Blom, L.; Nystrom, L.; Dahlquist, G. The Swedish childhood diabetes study. Vaccinations and infections as risk determinants for diabetes in childhood. Diabetologia 1991, 34, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Petrovsky, N.; Silva, D.; Schatz, D.A. Vaccine therapies for the prevention of type 1 diabetes mellitus. Paediatr Drugs 2003, 5, 575–582. [Google Scholar] [CrossRef]
- Fonseca, V.A. Early identification and treatment of insulin resistance: Impact on subsequent prediabetes and type 2 diabetes. Clin. Cornerstone 2007, 8, S7–S18. [Google Scholar] [CrossRef]
- Weickert, M.O.; Pfeiffer, A.F. Metabolic effects of dietary fiber consumption and prevention of diabetes. J. Nutr. 2008, 138, 439–442. [Google Scholar] [CrossRef]
- Zipitis, C.S.; Akobeng, A.K. Vitamin D supplementation in early childhood and risk of type 1 diabetes: A systematic review and meta-analysis. Arch. Dis. Child 2008, 93, 512–517. [Google Scholar] [CrossRef]
- Narayan, K.M.V.; Williamson, D.F. Prevention of Type 2 Diabetes: Risk Status, Clinic, and Community. J. Gen. Intern. Med. 2010, 25, 154–157. [Google Scholar] [CrossRef]
- Saaristo, T.; Moilanen, L.; Korpi-Hyovalti, E.; Vanhala, M.; Saltevo, J.; Niskanen, L.; Jokelainen, J.; Peltonen, M.; Oksa, H.; Tuomilehto, J.; et al. Lifestyle intervention for prevention of type 2 diabetes in primary health care: One-year follow-up of the Finnish National Diabetes Prevention Program (FIN-D2D). Diabetes Care 2010, 33, 2146–2151. [Google Scholar] [CrossRef]
- Nicholls, E.F.; Madera, L.; Hancock, R.E. Immunomodulators as adjuvants for vaccines and antimicrobial therapy. Ann. N. Y. Acad. Sci. 2010, 1213, 46–61. [Google Scholar] [CrossRef]
- Combadiere, B.; Mahe, B. Particle-based vaccines for transcutaneous vaccination. Comp. Immunol. Microbiol. Infect. Dis. 2008, 31, 293–315. [Google Scholar] [CrossRef] [PubMed]
- De Gregorio, E.; Caproni, E.; Ulmer, J.B. Vaccine adjuvants: Mode of action. Front. Immunol. 2013, 4, 214. [Google Scholar] [CrossRef] [PubMed]
- Foged, C. Subunit vaccines of the future: The need for safe, customized and optimized particulate delivery systems. Ther. Deliv. 2011, 2, 1057–1077. [Google Scholar] [CrossRef]
- Schijns, V.E.; Lavelle, E.C. Trends in vaccine adjuvants. Expert Rev. Vaccines 2011, 10, 539–550. [Google Scholar] [CrossRef]
- Wu, T.Y.H.; Singh, M.; Miller, A.T.; De Gregorio, E.; Doro, F.; D’Oro, U.; Skibinski, D.A.; Mbow, M.L.; Bufali, S.; Herman, A.E.; et al. Rational design of small molecules as vaccine adjuvants. Sci. Transl. Med. 2014, 6, 263ra160. [Google Scholar] [CrossRef]
- O’Hagan, D.T.; Fox, C.B. New generation adjuvants–from empiricism to rational design. Vaccine 2015, 33, B14–B20. [Google Scholar] [CrossRef]
- Aguilar, J.C.; Rodriguez, E.G. Vaccine adjuvants revisited. Vaccine 2007, 25, 3752–3762. [Google Scholar] [CrossRef]
- Coffman, R.L.; Sher, A.; Seder, R.A. Vaccine adjuvants: Putting innate immunity to work. Immunity 2010, 33, 492–503. [Google Scholar] [CrossRef]
- Reed, S.G.; Orr, M.T.; Fox, C.B. Key roles of adjuvants in modern vaccines. Nat. Med. 2013, 19, 1597–1608. [Google Scholar] [CrossRef]
- Lambrecht, B.N.; Kool, M.; Willart, M.A.; Hammad, H. Mechanism of action of clinically approved adjuvants. Curr. Opin. Immunol. 2009, 21, 23–29. [Google Scholar] [CrossRef]
- Oleszycka, E.; Lavelle, E.C. Immunomodulatory properties of the vaccine adjuvant alum. Curr. Opin. Immunol. 2014, 28, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.M.; Faulenbach, M.; Vaag, A.; Vølund, A.; Ehses, J.A.; Seifert, B.; Mandrup-Poulsen, T.; Donath, M.Y. Interleukin-1–receptor antagonist in type 2 diabetes mellitus. N. Engl. J. Med. 2007, 356, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Ren, K.; Torres, R. Role of interleukin-1beta during pain and inflammation. Brain Res. Rev. 2009, 60, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Castejon, G.; Brough, D. Understanding the mechanism of IL-1β secretion. Cytokine Growth Factor Rev. 2011, 22, 189–195. [Google Scholar] [CrossRef]
- Banerjee, M. Saxena, M. Interleukin-1 (IL-1) family of cytokines: Role in type 2 diabetes. Clin. Chim. Acta 2012, 413, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Handa, M.; Vanegas, S.; Maddux, B.A.; Mendoza, N.; Zhu, S.; Goldfine, I.D.; Mirza, A.M. XOMA 052, an anti-IL-1β monoclonal antibody, prevents IL-1β-mediated insulin resistance in 3T3-L1 adipocytes. Obesity 2013, 21, 306–309. [Google Scholar] [CrossRef] [PubMed]
- Zha, J.; Chi, X.W.; Yu, X.L.; Liu, X.M.; Liu, D.Q.; Zhu, J.; Ji, H.; Liu, R.T. Interleukin-1β-targeted vaccine improves glucose control and β-cell function in a diabetic KK-Ay mouse model. PLoS ONE 2016, 11, e0154298. [Google Scholar] [CrossRef]
- Spohn, G.; Schori, C.; Keller, I.; Sladko, K.; Sina, C.; Guler, R.; Schwarz, K.; Johansen, P.; Jennings, G.T.; Bachmann, M.F. Preclinical efficacy and safety of an anti-IL-1β vaccine for the treatment of type 2 diabetes. Mol.-Ther. Clin. Dev. 2014, 1, 14048. [Google Scholar] [CrossRef]
- Pagni, P.P.; Bresson, D.; Rodriguez-Calvo, T.; Bel Hani, A.; Manenkova, Y.; Amirian, N.; Blaszczak, A.; Faton, S.; Sachithanantham, S.; von Herrath, M.G. Combination therapy with an anti–IL-1β antibody and GAD65 DNA vaccine can reverse recent-onset diabetes in the RIP-GP mouse model. Diabetes 2014, 63, 2015–2025. [Google Scholar] [CrossRef]
- Cavelti-Weder, C.; Timper, K.; Seelig, E.; Keller, C.; Osranek, M.; Lassing, U.; Spohn, G.; Maurer, P.; Muller, P.; Jennings, G.T.; et al. Development of an interleukin-1β vaccine in patients with type 2 diabetes. Mol. Ther. 2016, 24, 1003–1012. [Google Scholar] [CrossRef]
- Kim, W.; Egan, J.M. The Role of Incretins in Glucose Homeostasis and Diabetes Treatment. Pharmacol. Rev. 2008, 60, 470–512. [Google Scholar] [CrossRef] [PubMed]
- Vella, A. Mechanism of action of DPP-4 inhibitors-new insights. J. Clin. Endocrinol. Metab. 2012, 97, 2626–2628. [Google Scholar] [CrossRef] [PubMed]
- Langley, A.K.; Suffoletta, T.J.; Jennings, H.R. Dipeptidyl peptidase IV inhibitors and the incretin system in type 2 diabetes mellitus. Pharmacotherapy 2007, 27, 1163–1180. [Google Scholar] [CrossRef] [PubMed]
- Madsbad, S.; Krarup, T.; Deacon, C.F.; Holst, J.J. Glucagon-like peptide receptor agonists and dipeptidyl peptidase-4 inhibitors in the treatment of diabetes: A review of clinical trials. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Pacini, F. Thyroid nodules and cancer. Preface. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, vii. [Google Scholar] [CrossRef]
- Davidson, J.A. Advances in therapy for type 2 diabetes: GLP-1 receptor agonists and DPP-4 inhibitors. Cleve Clin. J. Med. 2009, 76, S28–S38. [Google Scholar]
- Dicker, D. DPP-4 inhibitors: Impact on glycemic control and cardiovascular risk factors. Diabetes Care 2011, 34, S276–S278. [Google Scholar] [CrossRef]
- Donnelly, D. The structure and function of the glucagon-like peptide-1 receptor and its ligands. Br. J. Pharmacol. 2012, 166, 27–41. [Google Scholar] [CrossRef]
- Li, Y.; Xiao, J.; Tian, H.; Pei, Y.; Lu, Y.; Han, X.; Liu, Y.; Zhong, W.; Sun, B.; Fang, F.; et al. The DPP-4 inhibitor MK0626 and exercise protect islet function in early pre-diabetic kkay mice. Peptides 2013, 49, 91–99. [Google Scholar] [CrossRef]
- Pratley, R.E.; Nauck, M.; Bailey, T.; Montanya, E.; Cuddihy, R.; Filetti, S.; Thomsen, A.B.; Sondergaard, R.E.; Davies, M.; 1860-LIRA-DPP-4 Study Group. Liraglutide versus sitagliptin for patients with type 2 diabetes who did not have adequate glycaemic control with metformin: A 26-week, randomised, parallel-group, open-label trial. The Lancet 2010, 375, 1447–1456. [Google Scholar] [CrossRef]
- Pang, Z.; Nakagami, H.; Osako, M.K.; Koriyama, H.; Nakagami, F.; Tomioka, H.; Shimamura, M.; Kurinami, H.; Takami, Y.; Morishita, R.; et al. Therapeutic vaccine against DPP4 improves glucose metabolism in mice. Proc. Natl. Acad. Sci. USA 2014, 111, E1256–E1263. [Google Scholar] [CrossRef] [PubMed]
- Bresson, D.; Fradkin, M.; Manenkova, Y.; Rottembourg, D.; Von Herrath, M. Genetic-induced variations in the GAD65 T-cell repertoire governs efficacy of anti-CD3/GAD65 combination therapy in new-onset type 1 diabetes. Mol. Ther. 2010, 18, 307–316. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Li, Z.; Fang, J.; Jiao, R.; Wei, X.; Ma, Y.; Liu, X.; Cheng, P.; Li, T. A novel multi-epitope vaccine based on Dipeptidyl Peptidase 4 prevents streptozotocin-induced diabetes by producing anti-DPP4 antibody and immunomodulatory effect in C57BL/6J mice. Biomed. Pharmacother. 2017, 89, 1467–1475. [Google Scholar] [CrossRef] [PubMed]
- Mondal, M.; Trivedy, K.; Nirmal Kumar, S. The silk proteins, sericin and fibroin in silkworm, Bombyx Mori Linn.- A review. Casp. J. Environ. Sci. 2007, 5, 63–76. [Google Scholar]
- Kato, T.; Kajikawa, M.; Maenaka, K.; Park, E.Y. Silkworm expression system as a platform technology in life science. Appl. Microbiol. Biotechnol. 2010, 85, 459–470. [Google Scholar] [CrossRef]
- Dong, Z.; Zhao, P.; Zhang, Y.; Song, Q.; Zhang, X.; Guo, P.; Wang, D.; Xia, Q. Analysis of proteome dynamics inside the silk gland lumen of Bombyx mori. Sci. Rep. 2016, 6, 21158. [Google Scholar] [CrossRef]
- Park, E.Y.; Abe, T.; Kato, T. Improved expression of fusion protein using a cysteine-protease-and chitinase-deficient Bombyx mori (silkworm) multiple nucleopolyhedrovirus bacmid in silkworm larvae. Biotechnol. Appl. Biochem. 2008, 49, 135–140. [Google Scholar] [CrossRef]
- Baldauf, K.J.; Royal, J.M.; Hamorsky, K.T.; Matoba, N. Cholera toxin B: One subunit with many pharmaceutical applications. Toxins 2015, 7, 974–996. [Google Scholar] [CrossRef]
- Gong, Z.; Jin, Y.; Zhang, Y. Suppression of diabetes in non-obese diabetic (NOD) mice by oral administration of a cholera toxin B subunit–insulin B chain fusion protein vaccine produced in silkworm. Vaccine 2007, 25, 1444–1451. [Google Scholar] [CrossRef]
- Langridge, W.; Denes, B.; Fodor, I. Cholera toxin B subunit modulation of mucosal vaccines for infectious and autoimmune diseases. Curr. Opin. Investig. Drugs 2010, 11, 919–928. [Google Scholar]
- Meng, Q.; Wang, W.; Shi, X.; Jin, Y.; Zhang, Y. Protection against autoimmune diabetes by silkworm-produced GFP-tagged CTB-insulin fusion protein. Clin. Dev. Immunol. 2011, 2011, 831704. [Google Scholar] [CrossRef] [PubMed]
- Mbongue, J.C.; Nicholas, D.A.; Zhang, K.; Kim, N.S.; Hamilton, B.N.; Larios, M.; Zhang, G.; Umezawa, K.; Firek, A.F.; Langridge, W.H. Induction of indoleamine 2, 3-dioxygenase in human dendritic cells by a cholera toxin B subunit—Proinsulin vaccine. PLoS ONE 2015, 10, e0118562. [Google Scholar] [CrossRef]
- Stratmann, T. Cholera Toxin Subunit B as Adjuvant–An Accelerator in Protective Immunity and a Break in Autoimmunity. Vaccines 2015, 3, 579–596. [Google Scholar] [CrossRef] [PubMed]
- Awate, S.; Babiuk, L.A.; Mutwiri, G. Mechanisms of Action of Adjuvants. Front. Immunol. 2013, 4, 114. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, D.; Odumosu, O.; Langridge, W.H. Autoantigen based vaccines for type 1 diabetes. Discov. Med. 2011, 11, 293–301. [Google Scholar] [PubMed]
- Schuch, R.A.; Oliveira, T.L.; Collares, T.F.; Monte, L.G.; Inda, G.R.; Dellagostin, O.A.; Vendruscolo, C.T.; Moreira, A.D.S.; Hartwig, D.D. The use of xanthan gum as vaccine adjuvant: An evaluation of immunostimulatory potential in balb/c mice and cytotoxicity in vitro. BioMed Res. Int. 2017, 2017, 3925024. [Google Scholar] [CrossRef] [PubMed]
- Arvan, P.; Pietropaolo, M.; Ostrov, D.; Rhodes, C.J. Islet autoantigens: Structure, function, localization, and regulation. Cold Spring Harb. Perspect. Med. 2012, 2, a007658. [Google Scholar] [CrossRef]
- Wenzlau, J.M.; Juhl, K.; Yu, L.; Moua, O.; Sarkar, S.A.; Gottlieb, P.; Rewers, M.; Eisenbarth, G.S.; Jensen, J.; Davidson, H.W.; et al. The cation efflux transporter ZnT8 (Slc30A8) is a major autoantigen in human type 1 diabetes. Proc. Natl. Acad. Sci. USA 2007, 104, 17040–17045. [Google Scholar] [CrossRef]
- Guan, Y.; Zhang, M.; Li, Y.; Cao, W.; Ji, M.; Liu, Y. Vaccination with IA-2 autoantigen can prevent late prediabetic nonobese diabetic mice from developing diabetes mellitus. Diabetes Res. Clin. Pract. 2012, 95, 93–97. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, S.; Li, X.; Zheng, P.; Hu, F.; Zhou, Z. Vaccination with a co-expression DNA plasmid containing GAD65 fragment gene and IL-10 gene induces regulatory CD4+ T cells that prevent experimental autoimmune diabetes. Diabetes/Metabolism Res. Rev. 2016, 32, 522–533. [Google Scholar] [CrossRef]
- Shen, L.; Lu, S.; Huang, D.; Li, G.; Liu, K.; Cao, R.; Zong, L.; Jin, L.; Wu, J. A rationally designed peptide IA-2-P2 against type 1 diabetes in streptozotocin-induced diabetic mice. Diabetes Vasc. Dis. Res. 2017, 14, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Li, G.; Liu, K.; Yang, X.; Cao, R.; Zong, L.; Long, J.; Jin, L.; Wu, J. Fusion protein His-Hsp65-6IA2P2 prevents type 1 diabetes through nasal immunization in NOD Mice. Int. Immunopharmacol. 2016, 35, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, E. ZnT8 and type 1 diabetes. Endocr J. 2012, 59, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Yi, B.; Huang, G.; Zhou, Z.G. Current and Future Clinical Applications of Zinc Transporter-8 in Type 1 Diabetes Mellitus. Chin. Med. J. 2015, 128, 2387–2394. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Wang, X.; Gu, Y.; Zhang, X.; Qin, Y.; Chen, H.; Xu, X.; Yang, T.; Zhang, M. Screening and identification of human ZnT8-specific single-chain variable fragment (scFv) from type 1 diabetes phage display library. Sci. China Life Sci. 2016, 59, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Gu, Y.; Bian, L.; Shi, Y.; Cai, Y.; Chen, Y.; Chen, H.; Qian, L.; Wu, X.; Xu, K.; et al. Characterization of immune response to novel HLA-A2-restricted epitopes from zinc transporter 8 in type 1 diabetes. Vaccine 2016, 34, 854–862. [Google Scholar] [CrossRef]
- Hjorth, M.; Axelsson, S.; Ryden, A.; Faresjo, M.; Ludvigsson, J.; Casas, R. GAD-alum treatment induces GAD65-specific CD4+ CD25highFOXP3+ cells in type 1 diabetic patients. Clin. Immunol. 2011, 138, 117–126. [Google Scholar] [CrossRef]
- Morales, A.E.; Thrailkill, K.M. GAD-alum immunotherapy in Type 1 diabetes mellitus. Immunotherapy 2011, 3, 323–332. [Google Scholar] [CrossRef]
- Marrack, P.; McKee, A.S.; Munks, M.W. Towards an understanding of the adjuvant action of aluminium. Nat. Rev. Immunol. 2009, 9, 287–293. [Google Scholar] [CrossRef]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood 2011, 117, 3720–3732. [Google Scholar] [CrossRef]
- Agardh, C.D.; Lynch, K.F.; Palmer, M.; Link, K.; Lernmark, Å. GAD65 vaccination: 5 years of follow-up in a randomised dose-escalating study in adult-onset autoimmune diabetes. Diabetologia 2009, 52, 1363–1368. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J. The role of immunomodulation therapy in autoimmune diabetes. J. Diabetes Sci. Technol. 2009, 3, 320–330. [Google Scholar] [CrossRef]
- Larsson, H.E.; Lernmark, A. Vaccination against type 1 diabetes. J. Intern. Med. 2011, 269, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.; Hjorth, M.; Cheramy, M.; Axelsson, S.; Pihl, M.; Forsander, G.; Nilsson, N.O.; Samuelsson, B.O.; Wood, T.; Aman, J.; et al. Extended evaluation of the safety and efficacy of GAD treatment of children and adolescents with recent-onset type 1 diabetes: A randomised controlled trial. Diabetologia 2011, 54, 634–640. [Google Scholar] [CrossRef]
- Harrison, L.C.; Wentworth, J.M.; Zhang, Y.; Bandala-Sanchez, E.; Bohmer, R.M.; Neale, A.M.; Stone, N.L.; Naselli, G.; Bosco, J.J.; Auyeung, P.; et al. Antigen-based vaccination and prevention of type 1 diabetes. Curr. Diabetes Rep. 2013, 13, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Beam, C.A.; MacCallum, C.; Herold, K.C.; Wherrett, D.K.; Palmer, J.; Ludvigsson, J. GAD vaccine reduces insulin loss in recently diagnosed type 1 diabetes: Findings from a Bayesian meta-analysis. Diabetologia 2017, 60, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Tavira, B.; Cheramy, M.; Axelsson, S.; Åkerman, L.; Ludvigsson, J.; Casas, R. Effect of simultaneous vaccination with H1N1 and GAD-alum on GAD65-induced immune response. Diabetologia 2017, 60, 1276–1283. [Google Scholar] [CrossRef]
- Wherrett, D.K.; Bundy, B.; Becker, D.J.; DiMeglio, L.A.; Gitelman, S.E.; Goland, R.; Gottlieb, P.A.; Greenbaum, C.J.; Herold, K.C.; Marks, J.B.; et al. Antigen-based therapy with glutamic acid decarboxylase (GAD) vaccine in patients with recent-onset type 1 diabetes: A randomised double-blind trial. Lancet 2011, 378, 319–327. [Google Scholar] [CrossRef]
- Ludvigsson, J.; Krisky, D.; Casas, R.; Battelino, T.; Castaño, L.; Greening, J.; Kordonouri, O.; Otonkoski, T.; Pozzilli, P.; Robert, J.J.; et al. GAD65 antigen therapy in recently diagnosed type 1 diabetes mellitus. N. Engl. J. Med. 2012, 366, 433–442. [Google Scholar] [CrossRef]
- Ludvigsson, J.; Cheramy, M.; Axelsson, S.; Pihl, M.; Åkerman, L.; Casas, R.; Clinical GAD-Study Group in Sweden. GAD-treatment of children and adolescents with recent-onset type 1 diabetes preserves residual insulin secretion after 30 months. Diabetes/Metabolism Res. Rev. 2014, 30, 405–414. [Google Scholar] [CrossRef]
- Cook, D.P.; Gysemans, C.; Mathieu, C. Prospects of a type 1 diabetes vaccine. Expert Opin. Biol. Ther. 2017, 17, 403–406. [Google Scholar] [CrossRef]
- Denes, B.; Fodor, I.; Langridge, W.H. Autoantigens plus interleukin-10 suppress diabetes autoimmunity. Diabetes Technol. Ther. 2010, 12, 649–661. [Google Scholar] [CrossRef]
- Tsui, H.; Chan, Y.; Tang, L.; Winer, S.; Cheung, R.K.; Paltser, G.; Selvanantham, T.; Elford, A.R.; Ellis, J.R.; Becker, D.J.; et al. Targeting of pancreatic glia in type 1 diabetes. Diabetes 2008, 57, 918–928. [Google Scholar] [CrossRef] [PubMed]
- Pang, Z.; Kushiyama, A.; Sun, J.; Kikuchi, T.; Yamazaki, H.; Iwamoto, Y.; Koriyama, H.; Yoshida, S.; Shimamura, M.; Higuchi, M.; et al. Glial fibrillary acidic protein (GFAP) is a novel biomarker for the prediction of autoimmune diabetes. FASEB J. 2017, 31, 4053–4063. [Google Scholar] [CrossRef]
- Pang, Z.; Higuchi, M.; Koriyama, H.; Yoshida, S.; Kurinami, H.; Shimamura, M.; Takami, Y.; Rakugi, H.; Morishita, R.; Nakagami, H. Evaluating the potential of the GFAP-KLH immune-tolerizing vaccine for type 1 diabetes in mice. FEBS Lett. 2017, 591, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Dolgova, N.V.; Zhang, Y.; Xia, C.Q.; Wasserfall, C.H.; Atkinson, M.A.; Clare-Salzler, M.J.; Keselowsky, B.G. A combination dual-sized microparticle system modulates dendritic cells and prevents type 1 diabetes in prediabetic NOD mice. Clin. Immunol. 2015, 160, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.M.; Lewis, J.S.; Carstens, M.R.; Campbell-Thompson, M.; Wasserfall, C.H.; Atkinson, M.A.; Keselowsky, B.G. A combination hydrogel microparticle-based vaccine prevents type 1 diabetes in non-obese diabetic mice. Sci. Rep. 2015, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.; Nylander, K.; Harnaha, J.; Machen, J.; Lakomy, R.; Styche, A.; Gillis, K.; Brown, L.; Lafreniere, D.; Gallo, M.; et al. A microsphere-based vaccine prevents and reverses new-onset autoimmune diabetes. Diabetes 2008, 57, 1544–1555. [Google Scholar] [CrossRef] [PubMed]
- Keselowsky, B.G.; Xia, C.Q.; Clare-Salzler, M. Multifunctional dendritic cell-targeting polymeric microparticles: Engineering new vaccines for type 1 diabetes. Hum. Vaccines 2011, 7, 37–44. [Google Scholar] [CrossRef][Green Version]
- Miller, S.D.; Turley, D.M.; Podojil, J.R. Antigen-specific tolerance strategies for the prevention and treatment of autoimmune disease. Nat. Rev. Immunol. 2007, 7, 665–677. [Google Scholar] [CrossRef]
- Roep, B.O.; Solvason, N.; Gottlieb, P.A.; Abreu, J.R.; Harrison, L.C.; Eisenbarth, G.S.; Yu, L.; Leviten, M.; Hagopian, W.A.; Buse, J.B.; et al. Plasmid-encoded proinsulin preserves C-peptide while specifically reducing proinsulin-specific CD8+ T cells in type 1 diabetes. Sci. Transl. Med. 2013, 5, 191ra82. [Google Scholar] [CrossRef]
- Ludvigsson, J.; Sumnik, Z.; Pelikanova, T.; Nattero Chavez, L.; Lundberg, E.; Rica, I.; Martínez-Brocca, M.A.; Ruiz de Adana, M.; Wahlberg, J.; Katsarou, A.; et al. Intralymphatic glutamic acid decarboxylase with vitamin D supplementation in recent-onset type 1 diabetes: A double-blind, randomized, placebo-controlled phase IIb trial. Diabetes Care 2021, 44, 1604–1612. [Google Scholar] [CrossRef] [PubMed]
- Geenen, V.; Mottet, M.; Dardenne, O.; Kermani, H.; Martens, H.; Francois, J.M.; Galleni, M.; Hober, D.; Rahmouni, S.; Moutschen, M. Thymic self-antigens for the design of a negative/tolerogenic self-vaccination against type 1 diabetes. Curr. Opin. Pharmacol. 2010, 10, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Harrison, L.C. Vaccination against self to prevent autoimmune disease: The type 1 diabetes model. Immunol. Cell Biol. 2008, 86, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.K. Live-attenuated Salmonella as a prototype vaccine vector for passenger immunogens in humans: Are we there yet? Expert Rev. Vaccines 2007, 6, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Petrovsky, N. Immunomodulation with microbial vaccines to prevent type 1 diabetes mellitus. Nat. Rev. Endocrinol. 2010, 6, 131–138. [Google Scholar] [CrossRef]
- Husseiny, M.I.; Rawson, J.; Kaye, A.; Nair, I.; Todorov, I.; Hensel, M.; Kandeel, F.; Ferreri, K. An oral vaccine for type 1 diabetes based on live attenuated Salmonella. Vaccine 2014, 32, 2300–2307. [Google Scholar] [CrossRef]
- Cheminay, C.; Hensel, M. Rational design of Salmonella recombinant vaccines. Int. J. Med. Microbiol. 2008, 298, 87–98. [Google Scholar] [CrossRef]
- Oikawa, Y.; Shimada, A.; Yamada, Y.; Okubo, Y.; Katsuki, T.; Shigihara, T.; Miyazaki, J.I.; Narumi, S.; Itoh, H. CXC chemokine ligand 10 DNA vaccination plus Complete Freund’s Adjuvant reverses hyperglycemia in non-obese diabetic mice. Rev. Diabet. Stud. RDS 2010, 7, 209. [Google Scholar]
- Denes, B.; Fodor, I.; Langridge, W.H. Persistent suppression of type 1 diabetes by a multicomponent vaccine containing a cholera toxin B subunit-autoantigen fusion protein and complete Freund’s adjuvant. Clin. Dev. Immunol. 2013, 2013, 578786. [Google Scholar] [CrossRef]
- Lin, M.S.; Tse, H.M.; Delmastro, M.M.; Bertera, S.; Wong, C.T.; Lakomy, R.; He, J.; Sklavos, M.M.; Coudriet, G.M.; Pietropaolo, M.; et al. A multivalent vaccine for type 1 diabetes skews T cell subsets to Th2 phenotype in NOD mice. Immunol. Res. 2011, 50, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Lilani, Z.; Ahmed, A.; Tazeem, R.; Naeem, E. BCG vaccine—An innovation for diabetes treatment in Pakistan? J. Ayub Med. Coll. Abbottabad 2017, 29, 1–2. [Google Scholar] [PubMed]
- Faustman, D.L.; Wang, L.; Okubo, Y.; Burger, D.; Ban, L.; Man, G.; Zheng, H.; Schoenfeld, D.; Pompei, R.; Avruch, J.; et al. Proof-of-concept, randomized, controlled clinical trial of Bacillus-Calmette-Guerin for treatment of long-term type 1 diabetes. PLoS ONE 2012, 7, e41756. [Google Scholar] [CrossRef]
- Karaci, M. The protective effect of the BCG vaccine on the development of type 1 diabetes in humans. In The Value of BCG and TNF in Autoimmunity; Academic Press: Cambridge, MA, USA, 2014; pp. 52–62. [Google Scholar]
- Kowalewicz-Kulbat, M.; Locht, C. BCG and protection against inflammatory and auto-immune diseases. Expert Rev. Vaccines 2017, 16, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Bluestone, J.A.; Herold, K.; Eisenbarth, G. Genetics, pathogenesis and clinical interventions in type 1 diabetes. Nature 2010, 464, 1293–1300. [Google Scholar] [CrossRef]
- Nurminen, N.; Oikarinen, S.; Hyoty, H. Virus infections as potential targets of preventive treatments for type 1 diabetes. Rev. Diabet. Stud. RDS 2012, 9, 260. [Google Scholar] [CrossRef]
- Hyoty, H.; Knip, M. Developing a vaccine for type 1 diabetes through targeting enteroviral infections. Expert Rev. Vaccines 2014, 13, 989–999. [Google Scholar] [CrossRef]
- Larsson, P.G.; Lakshmikanth, T.; Laitinen, O.H.; Utorova, R.; Jacobson, S.; Oikarinen, M.; Domsgen, E.; Koivunen, M.R.; Chaux, P.; Devard, N.; et al. A preclinical study on the efficacy and safety of a new vaccine against Coxsackievirus B1 reveals no risk for accelerated diabetes development in mouse models. Diabetologia 2015, 58, 346–354. [Google Scholar] [CrossRef]
- Rodrigues dos Santos, R., Jr.; Sartori, A.; Deperon Bonato, V.L.; Coelho Castelo, A.A.M.; Vilella, C.A.; Zollner, R.L.; Lopes Silva, C. Immune modulation induced by tuberculosis DNA vaccine protects non-obese diabetic mice from diabetes progression. Clin. Exp. Immunol. 2007, 149, 570–578. [Google Scholar] [CrossRef][Green Version]
- Stratton, K.R.; Howe, C.J.; Johnston, R.B. Adverse Effects of Vaccines: Evidence and Causality; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Boettler, T.; Pagni, P.P.; Jaffe, R.; Cheng, Y.; Zerhouni, P.; von Herrath, M. The clinical and immunological significance of GAD-specific autoantibody and T-cell responses in type 1 diabetes. J. Autoimmun. 2013, 44, 40–48. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Type of Vaccine | Vaccine Name | Indication | Mechanism of Action | References |
|---|---|---|---|---|
| Adjuvant-based vaccines | Alum adjuvant-based vaccine | T1DM and T2DM | Activation of immune response; Promoting humoral immunity | [42,43] |
| Protein-based vaccines | IL-1-targeted epitope peptide (1EPP) | T2DM | Alters the level of glucose tolerance and provides a hyperglycaemia shield | [49] |
| Dipeptidyl peptidase-4 inhibitor (DPP4) based vaccine | T2DM | Inhibition of dipeptidyl peptidase-4 inhibitor (DPP4) enzyme | [53,54] | |
| CTB-InsB vaccination product | T1DM | Down-regulation response in the onset of T1DM; Induction of immune tolerance | [71,72,73,74,75] | |
| Specific self-antigen-based approach in vaccine production | IA-2 as a vaccine product | T1DM | Islet autoantigen mechanism; delaying the onset and the late stages of autoimmune diabetes | [81,82] |
| Glutamic Acid Decarboxylase 65-kD (GAD65)-Alum vaccine | T1DM | Suppression of -cell autoreactivity | [104] | |
| Insulin autoantigen-based vaccine | T1DM | Enhancing insulin production | [115] | |
| Non-Antigen-based vaccines | Live pathogen Salmonella-based vector vaccine | T1DM | T-cell autoreactive downregulation response | [119] |
| Inactivated microbial vaccine | T1DM | Positive immunogenic response induction | [121] | |
| BCG as a vector vaccine | T1DM | Restoration of endogenous -cell function | [124] | |
| Other Disease-Based Vaccines | Enteroviruses (EV)-based vaccine | T1DM | Delayed onset response | [129,130] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chellappan, D.K.; Bhandare, R.R.; Shaik, A.B.; Prasad, K.; Suhaimi, N.A.A.; Yap, W.S.; Das, A.; Banerjee, P.; Ghosh, N.; Guith, T.; et al. Vaccine for Diabetes—Where Do We Stand? Int. J. Mol. Sci. 2022, 23, 9470. https://doi.org/10.3390/ijms23169470
Chellappan DK, Bhandare RR, Shaik AB, Prasad K, Suhaimi NAA, Yap WS, Das A, Banerjee P, Ghosh N, Guith T, et al. Vaccine for Diabetes—Where Do We Stand? International Journal of Molecular Sciences. 2022; 23(16):9470. https://doi.org/10.3390/ijms23169470
Chicago/Turabian StyleChellappan, Dinesh Kumar, Richie R. Bhandare, Afzal B. Shaik, Krishna Prasad, Nurfatihah Azlyna Ahmad Suhaimi, Wei Sheng Yap, Arpita Das, Pradipta Banerjee, Nandini Ghosh, Tanner Guith, and et al. 2022. "Vaccine for Diabetes—Where Do We Stand?" International Journal of Molecular Sciences 23, no. 16: 9470. https://doi.org/10.3390/ijms23169470
APA StyleChellappan, D. K., Bhandare, R. R., Shaik, A. B., Prasad, K., Suhaimi, N. A. A., Yap, W. S., Das, A., Banerjee, P., Ghosh, N., Guith, T., Das, A., Balakrishnan, S., Candasamy, M., Mayuren, J., Palaniveloo, K., Gupta, G., Singh, S. K., & Dua, K. (2022). Vaccine for Diabetes—Where Do We Stand? International Journal of Molecular Sciences, 23(16), 9470. https://doi.org/10.3390/ijms23169470