
Nebulized Non-Immunogenic Staphylokinase in the Mice Acute Lung Injury Model

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Effect of Inhaled nSta on Coagulation Parameters
2.2. Mice ALI Model and Morphological Examination
2.3. Histological Examination
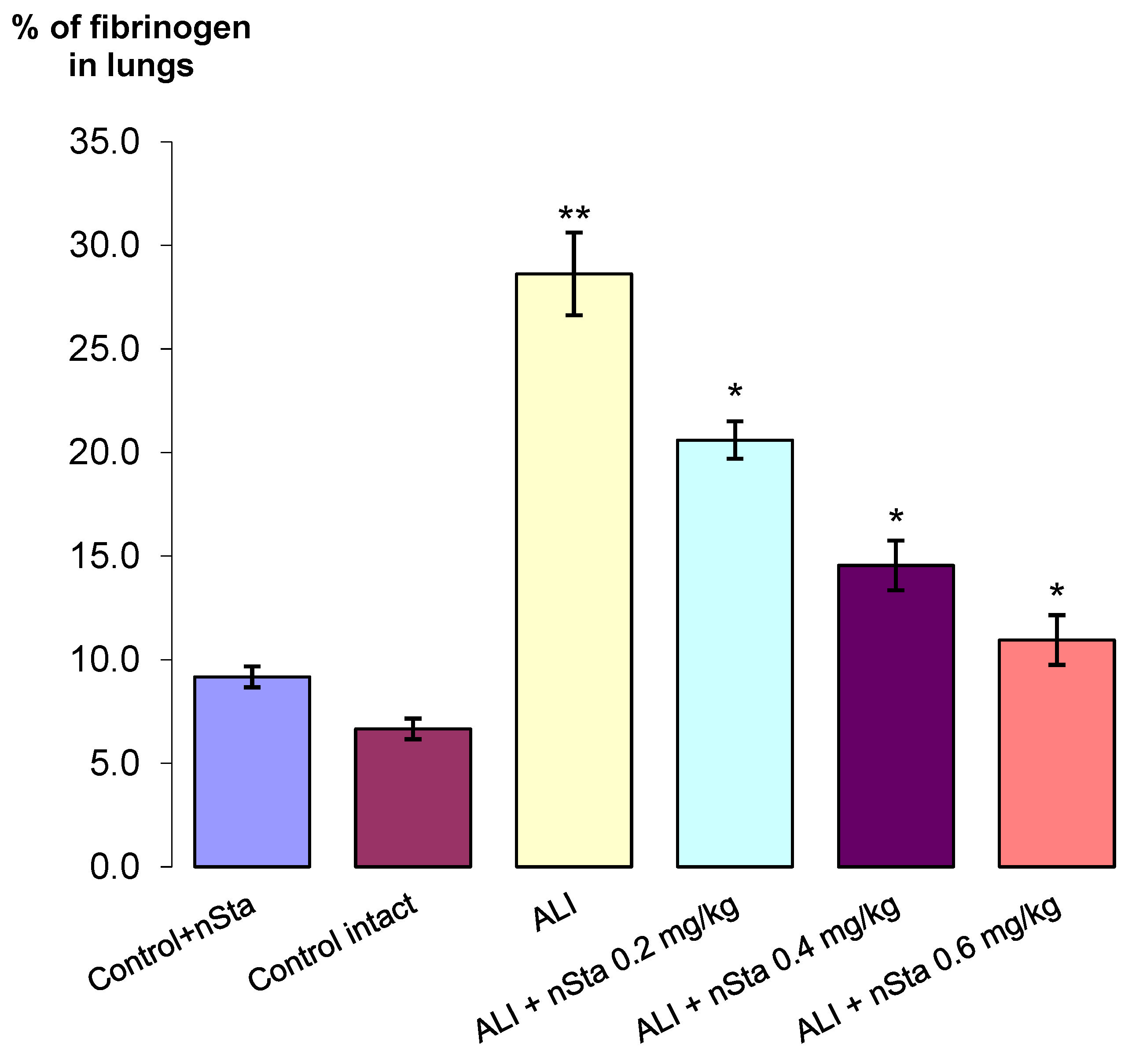
2.4. Assessment of Fibrin/Fibrinogen Deposition in the Lungs
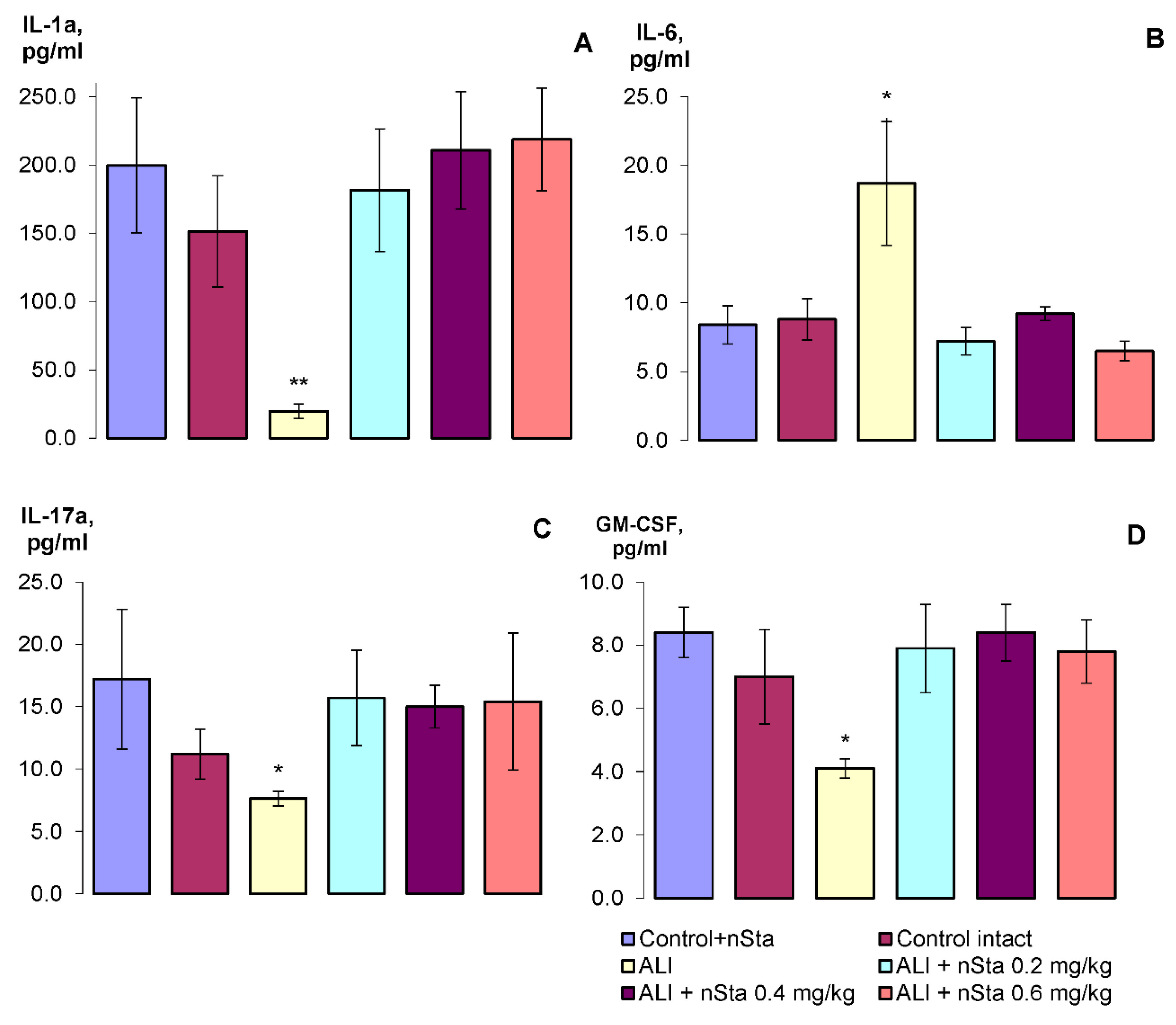
2.5. Evaluation of the Cytokine Profile by Flow Cytometry
3. Discussion
4. Material and Methods
4.1. Animals
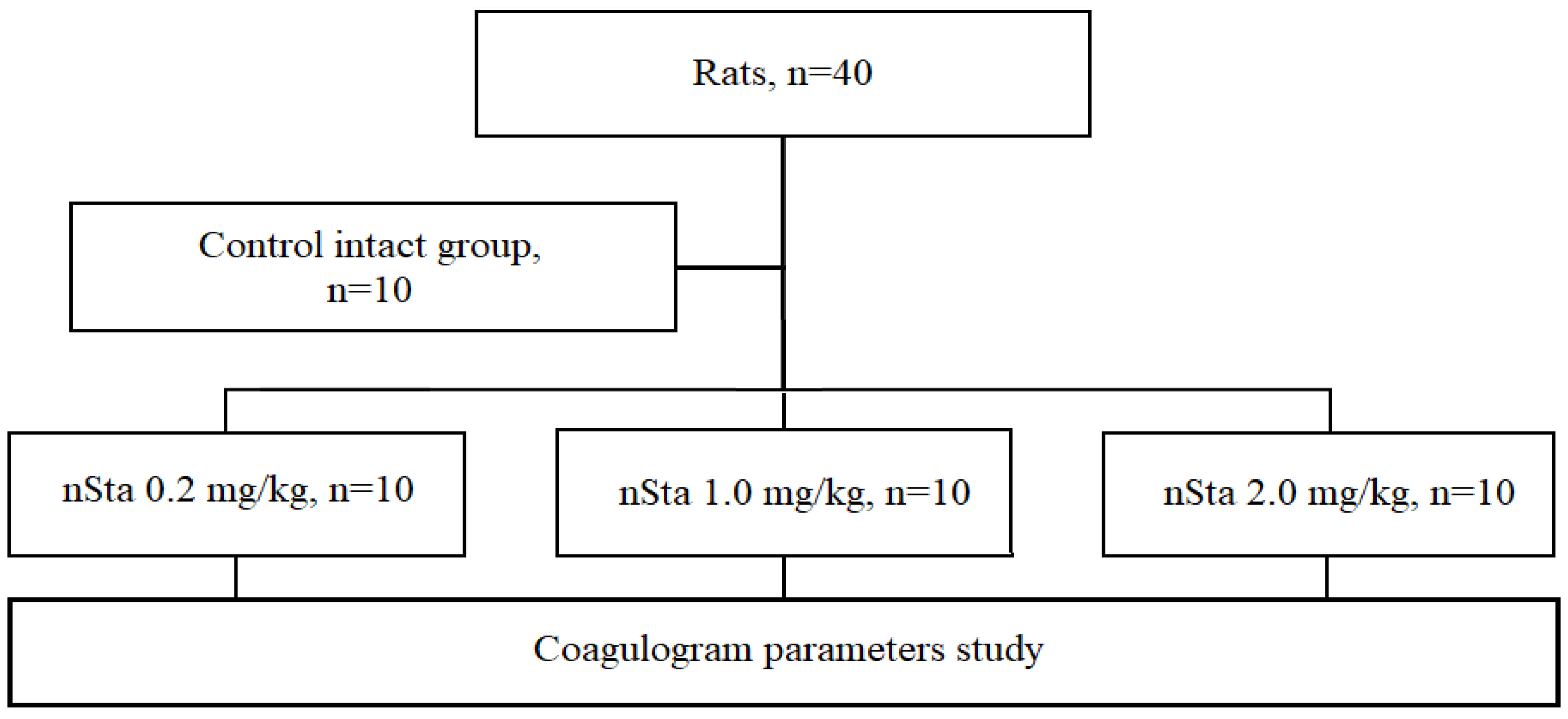
4.2. Evaluation of Coagulation Parameters in Healthy Rats
- Control intact (n = 10): saline nebulization;
- nSta 0.2 mg/kg (n = 10): nSta nebulization at a dose of 0.2 mg/kg;
- nSta 1.0 mg/kg (n = 10): nSta nebulization at a dose of 1.0 mg/kg;
- nSta 2.0 mg/kg (n = 10): nSta nebulization at a dose of 2.0 mg/kg.
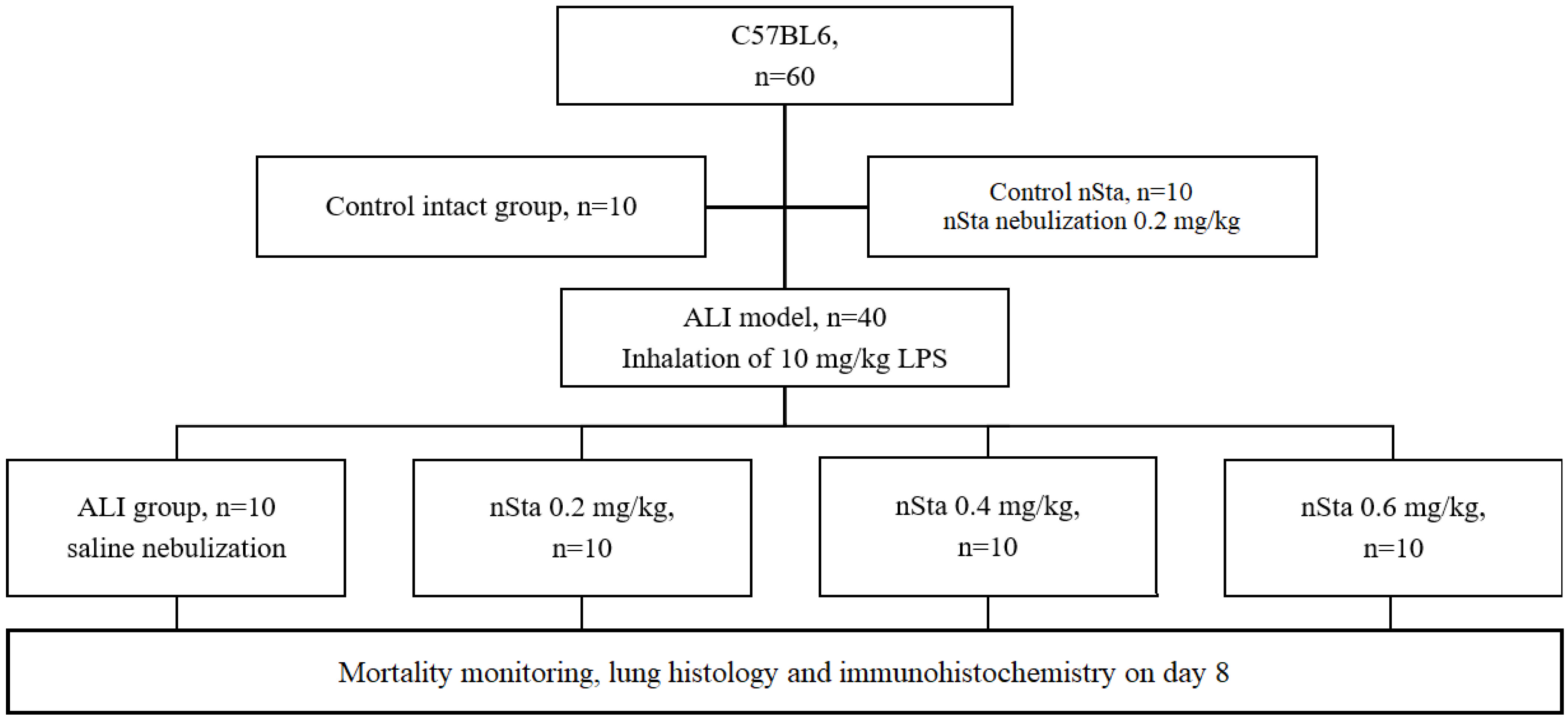
4.3. Acute Lung Injury (ALI) Modeling
4.4. ALI Experimental Groups
- Animals were randomly assigned into 6 experimental groups:
- Control nSta (n = 10): nSta nebulization at a dose of 0.2 mg/kg;
- Control intact (n = 10): saline nebulization;
- ALI (n = 10): saline nebulization;
- nSta (n = 10): nSta nebulization at a dose of 0.2 mg/kg;
- nSta (n = 10): nSta nebulization at a dose of 0.4 mg/kg;
- nSta (n = 10): nSta nebulization at a dose of 0.6 mg/kg.
4.5. Necropsy
4.6. Histological Examination
4.7. Assessment of Fibrin/Fibrinogen Deposits in the Lungs
4.8. Evaluation of the Cytokine Profile by Flow Cytometry
4.9. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kostopanagiotou, K.; Schuurmans, M.M.; Inci, I.; Hage, R. COVID-19-related end stage lung disease: Two distinct phenotypes. Ann. Med. 2022, 54, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Camprubí-Rimblas, M.; Tantinyà, N.; Guillamat-Prats, R.; Bringué, J.; Puig, F.; Gómez, M.N.; Blanch, L.; Artigas, A. Effects of nebulized antithrombin and heparin on inflammatory and coagulation alterations in an acute lung injury model in rats. J. Thromb. Haemostasis. 2020, 8, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemostasis. 2020, 18, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- Sawdey, M.S.; Loskutoff, D.J. Regulation of murine type 1 plasminogen activator inhibitor gene expression in vivo. Tissue specificity and induction by lipopolysaccharide, tumor necrosis factor-alpha, and transforming growth factor-beta. J. Clin. Investig. 1991, 88, 1346–1353. [Google Scholar] [CrossRef]
- Farsalinos, K.; Niaura, R.; Le Houezec, J.; Barbouni, A.; Tsatsakis, A.; Kouretas, D.; Vantarakis, A.; Poulas, K. Editorial: Nicotine and SARS-CoV-2: COVID-19 may be a disease of the nicotinic cholinergic system. Toxic Rep. 2020, 20, 658–663. [Google Scholar] [CrossRef]
- Tian, S.; Hu, W.; Niu, L.; Liu, H.; Xu, H.; Xiao, S.Y. Pulmonary pathology of earlyphase 2019 novel coronavirus (COVID-19) pneumonia in two patients with lung cancer. J. Thorac. Oncol. 2020, 15, 700–704. [Google Scholar] [CrossRef]
- Camprubí-Rimblas, M.; Tantinyà, N.; Bringué, J.; Guillamat-Prats, R.; Artigas, A. Anticoagulant therapy in acute respiratory distress syndrome. Ann. Transl. Med. 2018, 6, 36. [Google Scholar] [CrossRef]
- Interactions with Key COVID-19 Therapies/Liverpool Drug Interactions Group. 2022. Available online: https://www.covid19-druginteractions.org/checker (accessed on 17 August 2022).
- Eid, A.; Wiedermann, C.J.; Kinasewitz, G.T. Early administration of high-dose antithrombin in severe sepsis: Single center results from the KyberSept-trial. Anesth. Analg. 2008, 107, 1633–1638. [Google Scholar] [CrossRef]
- Juschten, J.; Tuinman, P.R.; Juffermans, N.P.; Dixon, B.; Levi, M.; Schultz, M.J. Nebulized anticoagulants in lung injury in critically ill patients-an updated systematic review of preclinical and clinical studies. Ann. Transl. Med. 2017, 5, 444. [Google Scholar] [CrossRef]
- Collen, D. Staphylokinase: A potent, uniquely fibrin-selective thrombolytic agent. Nat. Med. 1998, 4, 279–284. [Google Scholar] [CrossRef]
- Markin, S.S.; Semenov, A.M.; Markov, V.A.; Nizov, A.A.; Ponomarev, E.A.; Lebedev, P.A. Clinical trial of fibrinselective thrombolytic pharmaceutical agent FORTELYZIN (III Phase). Rudn. J. Med. 2012, 1, 105–110. [Google Scholar]
- Gusev, E.I.; Martynov, M.Y.; Nikonov, A.A.; Shamalov, N.A.; Semenov, M.P.; Gerasimets, E.A.; Yarovaya, E.B.; Semenov, A.M.; Archakov, A.I.; Markin, S.S.; et al. Non-immunogenic recombinant staphylokinase versus alteplase for patients with acute ischaemic stroke 4-5 h after symptom onset in Russia (FRIDA): A randomised, open label, multicentre, parallel-group, non-inferiority trial. Lancet Neurol. 2021, 20, 721–728. [Google Scholar] [CrossRef]
- Markov, V.A.; Duplyakov, D.V.; Konstantinov, S.L.; Klein, G.V.; Aksentev, S.B.; Platonov, D.Y.; Vyshlov, E.V.; Ponomarev, E.A.; Rabinovich, R.M.; Makarov, E.L.; et al. Fortelyzin in comparison with Metalyse for ST-elevated myocardial infarction: One-year results and clinical outcomes of a multicenter randomized study FRIDOM 1. Russ. J. Cardiol. 2018, 23, 110–116. [Google Scholar] [CrossRef]
- Chimenti, L.; Camprubí-Rimblas, M.; Guillamat-Prats, R.; Gomez, M.N.; Tijero, J.; Blanch, L.; Artigas, A. Nebulized Heparin Attenuates Pulmonary Coagulopathy and Inflammation through Alveolar Macrophages in a Rat Model of Acute Lung Injury. Thromb. Haemost. 2017, 117, 2125–2134. [Google Scholar] [CrossRef] [PubMed]
- Bai, C.; Wang, X. Multiple-systems dysfunction within the lung: A new angle for understanding pulmonary dysfunction. J. Soc. Motion Pict. Eng. 2006, 2, 2–3. [Google Scholar] [CrossRef]
- Maca, J.; Jor, O.; Holub, M.; Sklienka, P.; Bursa, F.; Burda, M.; Janout, V.; Ševčík, P. Past and present ARDS mortality rates: A systematic review. Respir. Care. 2017, 62, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Dosquet, C.; Weill, D.; Wautier, J.L. Cytokines and thrombosis. J. Cardiovasc. Pharmacol. 1995, 25, S13-9. [Google Scholar] [CrossRef] [PubMed]
- Ware, L.B.; Bastarache, J.A.; Wang, L. Coagulation and fibrinolysis in human acute lung injury—New therapeutic targets? Keio J. Med. 2005, 54, 142–149. [Google Scholar] [CrossRef] [PubMed]
- MacLaren, R.; Stringer, K.A. Emerging role of anticoagulants and fibrinolytics in the treatment of acute respiratory distress syndrome. Pharmacotherapy 2007, 27, 860–873. [Google Scholar] [CrossRef]
- Liu, C.; Ma, Y.; Su, Z.; Zhao, R.; Zhao, X.; Nie, H.G.; Xu, P.; Zhu, L.; Zhang, M.; Li, X.; et al. Meta-Analysis of Preclinical Studies of Fibrinolytic Therapy for Acute Lung Injury. Front. Immunol. 2018, 9, 1898. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Murray, V.; Berge, E.; Zoppo, G.J. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst. Rev. 2014, CD000213. [Google Scholar] [CrossRef] [PubMed]
- McCaul, M.; Lourens, A.; Kredo, T. Pre-hospital versus in-hospital thrombolysis for ST-elevation myocardial infarction. Cochrane Database Syst. Rev. 2014, 9, CD010191. [Google Scholar] [CrossRef]
- Cucherat, M.; Bonnefoy, E.; Tremeau, G. Primary Angioplasty Versus Intravenous Thrombolysis for Acute Myocardial Infarction. Cochrane Database Syst. Rev. 2003, 3, CD001560. [Google Scholar] [CrossRef]
- Abdelaal, A.A.M.; Mahmoud, H.E.; Mahran, M.A.; Khaled, M. Streptokinase Versus Unfractionated Heparin Nebulization in Patients with Severe Acute Respiratory Distress Syndrome (ARDS): A Randomized Controlled Trial With Observational Controls. J. Cardiothorac. Vasc. Anesth. 2020, 34, 436–443. [Google Scholar] [CrossRef]
- Choi, G.; Hofstra, J.J.; Roelofs, J.J.; Rijneveld, A.W.; Bresser, P.; Zee, J.S.; Florquin, S.; Poll, T.; Levi, M.; Schultz, M.J. Antithrombin inhibits bronchoalveolar activation of coagulation and limits lung injury during Streptococcus pneumoniae pneumonia in rats. Crit. Care Med. 2008, 36, 204–210. [Google Scholar] [CrossRef]
- Food and Drug Administration. Estimating the Safe Starting Dose in Clinical Trials for Therapeutics in Adult Healthy Volunteers. Guidance for Industry; Food and Drug Administration: Rockville, MD, USA, 2005. [Google Scholar]
- Khin Hnin, S.M.; Mitaca, C.; Tulafu, M.; Abe, S.; Kitagawa, M.; Ikeda, S.; Eishi, Y.; Kurata, S.; Tomita, M. Inhibition of poly (adenosine diphosphate-ribose) polimerase attenuates lung-kidney crosstalk induced by intratracheal lipopolysaccharide instillation in rats. Respir. Res. 2013, 14, 126. [Google Scholar] [CrossRef] [PubMed]
- Kudinov, V.A.; Artyushev, R.I.; Zurina, I.M.; Zorina, E.S.; Lapshin, R.D.; Snopova, L.B.; Mukhina, I.V.; Saburina, I.N. Inhaled Placental Mesenchymal Stromal Cell Secretome from Two- and Three-Dimensional Cell Cultures Promotes Survival and Regeneration in Acute Lung Injury Model in Mice. Int. J. Mol. Sci. 2022, 23, 3417. [Google Scholar] [CrossRef] [PubMed]
- Crowe, A.; Yue, W. Semi-quantitative Determination of Protein Expression Using Immunohistochemistry Staining and Analysis: An Integrated Protocol. Bio-Protocol 2019, 9, e3465. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Fibrinogen, g/L (M ± SD) | APTT, s (M ± SD) | Prothrombin Time, s (M ± SD) | |||
|---|---|---|---|---|---|---|
| Day 7 | Day 21 | Day 7 | Day 21 | Day 7 | Day 21 | |
| Control intact (n = 10) | 1.96 ± 0.10 | 1.91 ± 0.13 | 15.26 ± 062 | 15.36 ± 0.63 | 22.44 ± 0.85 | 22.18 ± 0.58 |
| nSta 0.2 mg/kg (n = 10) | 1.91 ± 0.09 | 1.93 ± 0.09 | 15.14 ± 0.65 | 15.40 ± 0.46 | 22.34 ± 0.74 | 22.12 ± 0.45 |
| nSta 1.0 mg/kg (n = 10) | 1.93 ± 0.08 | 1.96 ± 0.09 | 15.24 ± 0.34 | 15.18 ± 0.55 | 22.20 ± 0.83 | 22.16 ± 0.71 |
| nSta 2.0 mg/kg (n = 10) | 1.92 ± 0.10 | 1.94 ± 0.13 | 15.32 ± 0.66 | 15.12 ± 0.56 | 22.20 ± 0.80 | 22.24 ± 0.83 |
| Groups | Weight before ALI Induction, g (M ± SD) | Weight on Day 8, g (M ± SD) |
|---|---|---|
| Control nSta (n = 10) | 19.56 ± 0.14 | 26.31 ± 0.95 |
| Control intact (n = 10) | 18.44 ± 0.75 | 27.12 ± 0.63 |
| ALI (n = 6) | 19.87 ± 0.25 | 21.20 ± 0.75 * |
| ALI + nSta 0.2 mg/kg (n = 10) | 19.26 ± 0.32 | 23.54 ± 0.24 |
| ALI + nSta 0.4 mg/kg (n = 10) | 18.63 ± 0.27 | 25.37 ± 0.59 |
| ALI + nSta 0.6 mg/kg (n = 10) | 18.92 ± 0.31 | 26.63 ± 0.10 |
| Groups | Lungs’ Weight, g (M ± SD) | Exudate Score in Lungs (M ± SD) | Interstitial Edema and Hyaline Membrane Formation Score in Lungs (M ± SD) |
|---|---|---|---|
| Control nSta (n = 10) | 0.165 ± 0.011 | 0 | 1 |
| Control intact (n = 10) | 0.161 ± 0.028 | 0 | 1 |
| ALI (n = 6) | 0.233 ± 0.013 * | 2.33 ±0.51 ** | 3.66 ± 0.51 ** |
| ALI + nSta 0.2 mg/kg (n = 10) | 0.191 ± 0.014 ^ | 1.1 ± 0.73 | 2.2 ± 0.78 |
| ALI + nSta 0.4 mg/kg (n = 10) | 0.187 ± 0.024 ^ | 0.6 ± 0.51 ^^ | 1.4 ± 0.51 ^ |
| ALI + nSta 0.6 mg/kg (n = 10) | 0.161 ± 0.008 ^^ | 0.5 ± 0.52 ^^ | 1 ^^ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markin, S.S.; Lapshin, R.D.; Baskina, O.S.; Korotchenko, S.A.; Mukhina, I.V.; Ivanov, S.V.; Semenov, M.P.; Beregovykh, V.V.; Semenov, A.M. Nebulized Non-Immunogenic Staphylokinase in the Mice Acute Lung Injury Model. Int. J. Mol. Sci. 2022, 23, 9307. https://doi.org/10.3390/ijms23169307
Markin SS, Lapshin RD, Baskina OS, Korotchenko SA, Mukhina IV, Ivanov SV, Semenov MP, Beregovykh VV, Semenov AM. Nebulized Non-Immunogenic Staphylokinase in the Mice Acute Lung Injury Model. International Journal of Molecular Sciences. 2022; 23(16):9307. https://doi.org/10.3390/ijms23169307
Chicago/Turabian StyleMarkin, Sergey S., Roman D. Lapshin, Olga S. Baskina, Svetlana A. Korotchenko, Irina V. Mukhina, Sergei V. Ivanov, Mikhail P. Semenov, Valerii V. Beregovykh, and Andrey M. Semenov. 2022. "Nebulized Non-Immunogenic Staphylokinase in the Mice Acute Lung Injury Model" International Journal of Molecular Sciences 23, no. 16: 9307. https://doi.org/10.3390/ijms23169307
APA StyleMarkin, S. S., Lapshin, R. D., Baskina, O. S., Korotchenko, S. A., Mukhina, I. V., Ivanov, S. V., Semenov, M. P., Beregovykh, V. V., & Semenov, A. M. (2022). Nebulized Non-Immunogenic Staphylokinase in the Mice Acute Lung Injury Model. International Journal of Molecular Sciences, 23(16), 9307. https://doi.org/10.3390/ijms23169307