
Combined Analysis of HLA Class II Eplet Mismatch and Tacrolimus Levels for the Prediction of De Novo Donor Specific Antibody Development in Kidney Transplant Recipients

 , , , and
, , , and 
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
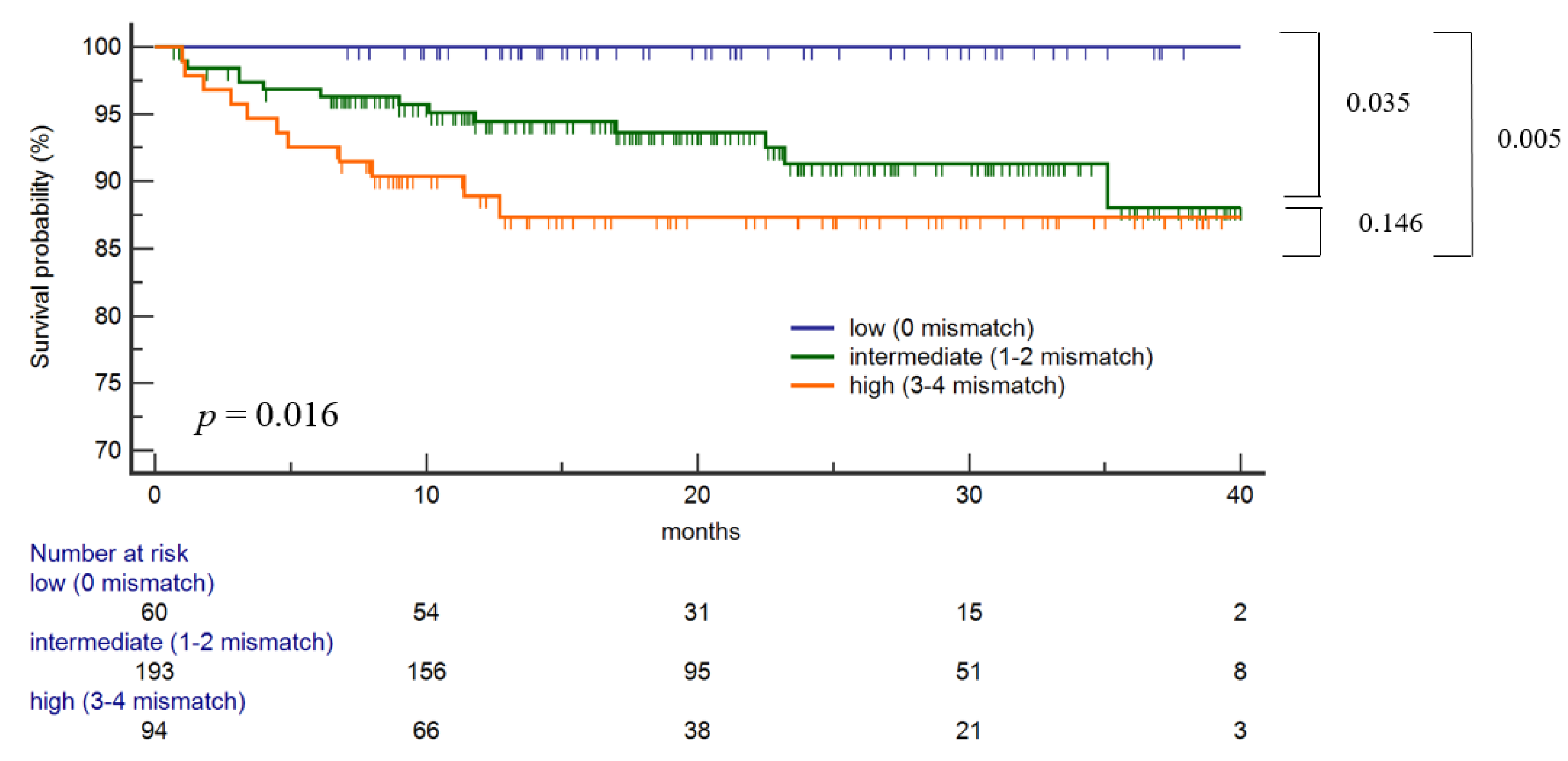
2.2. Traditional HLA DR/DQ Antigen Mismatch and the Risk of Class II dnDSA Development
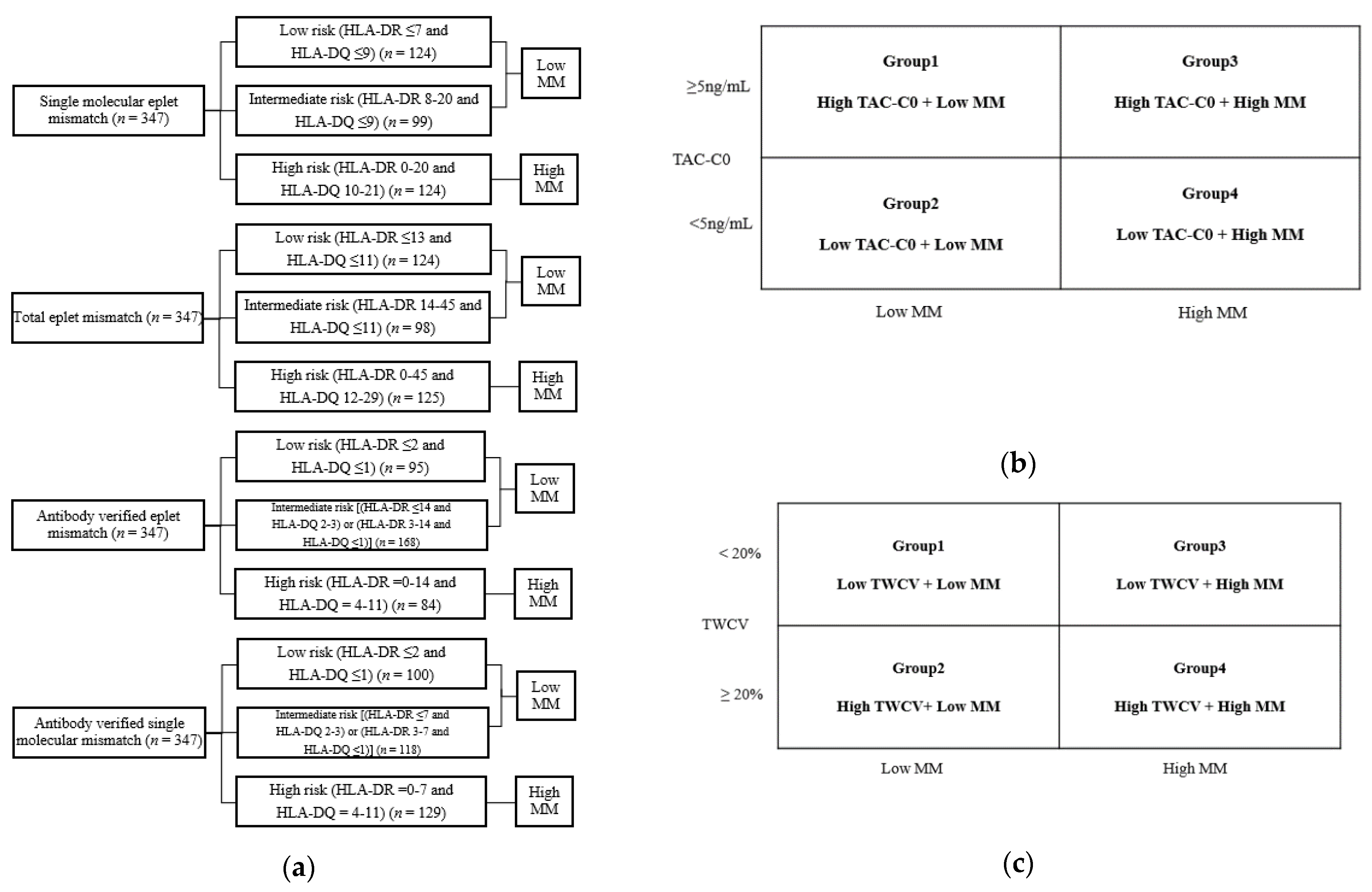
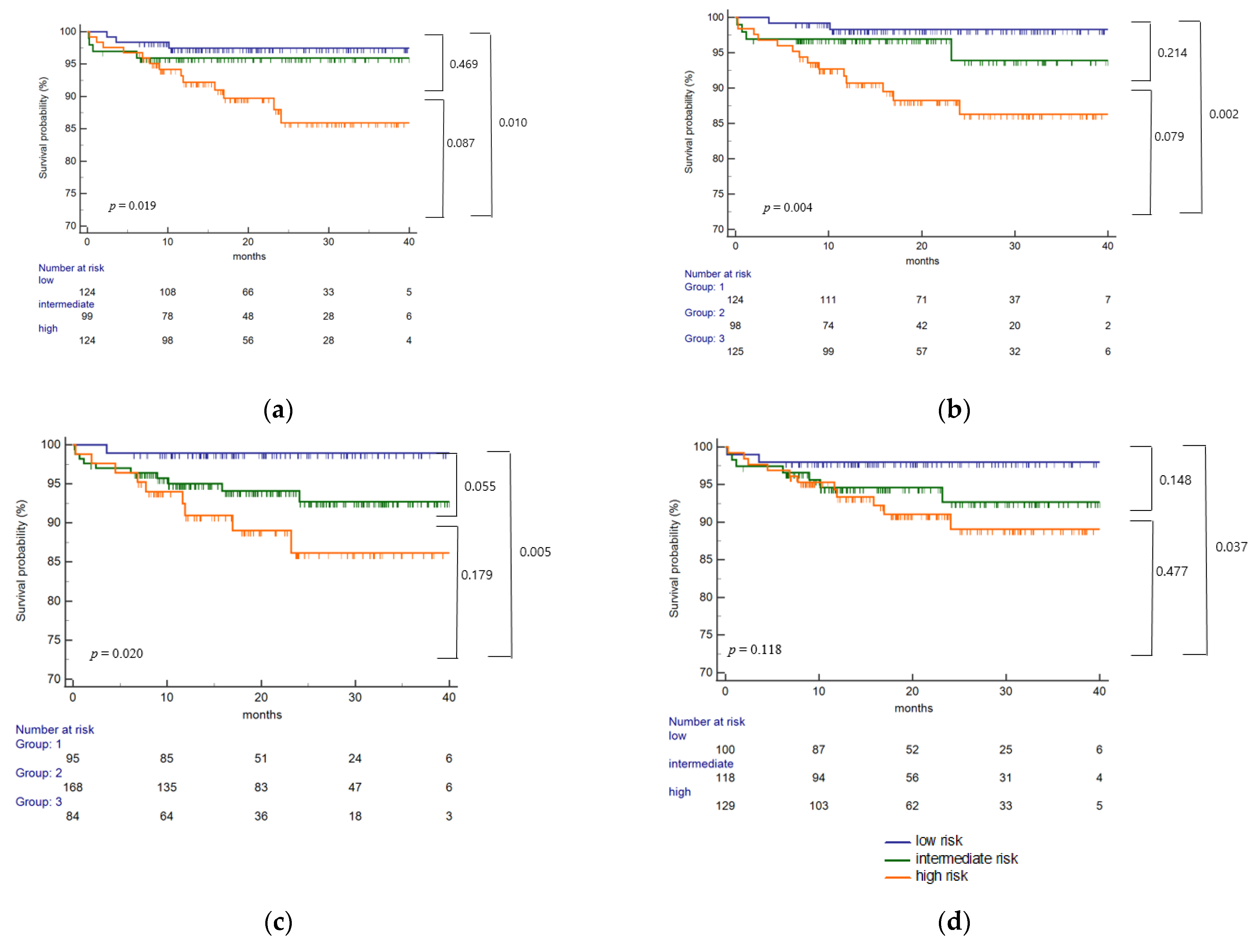
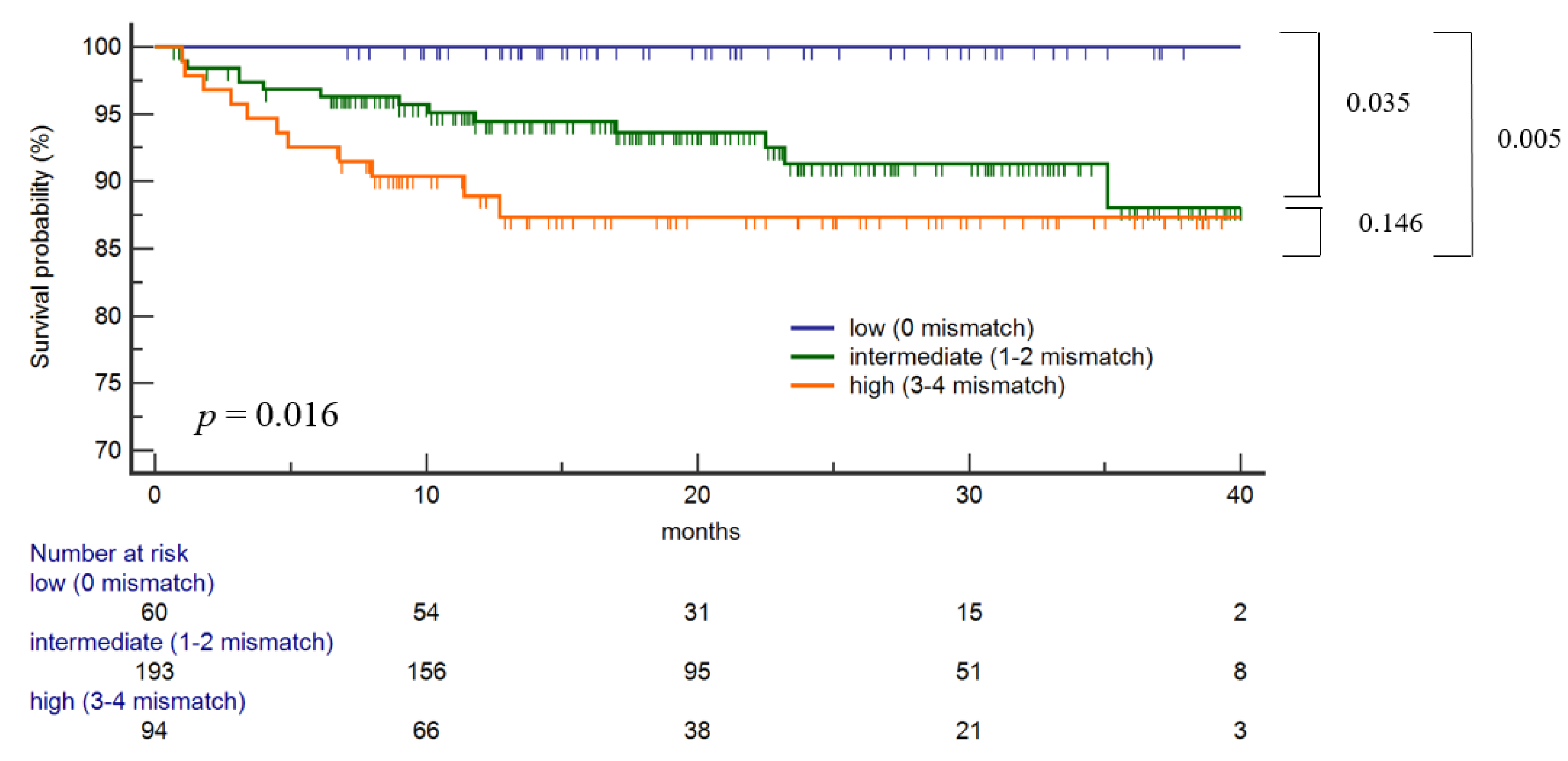
2.3. Defining the Eplet Mismatch Risk Groups
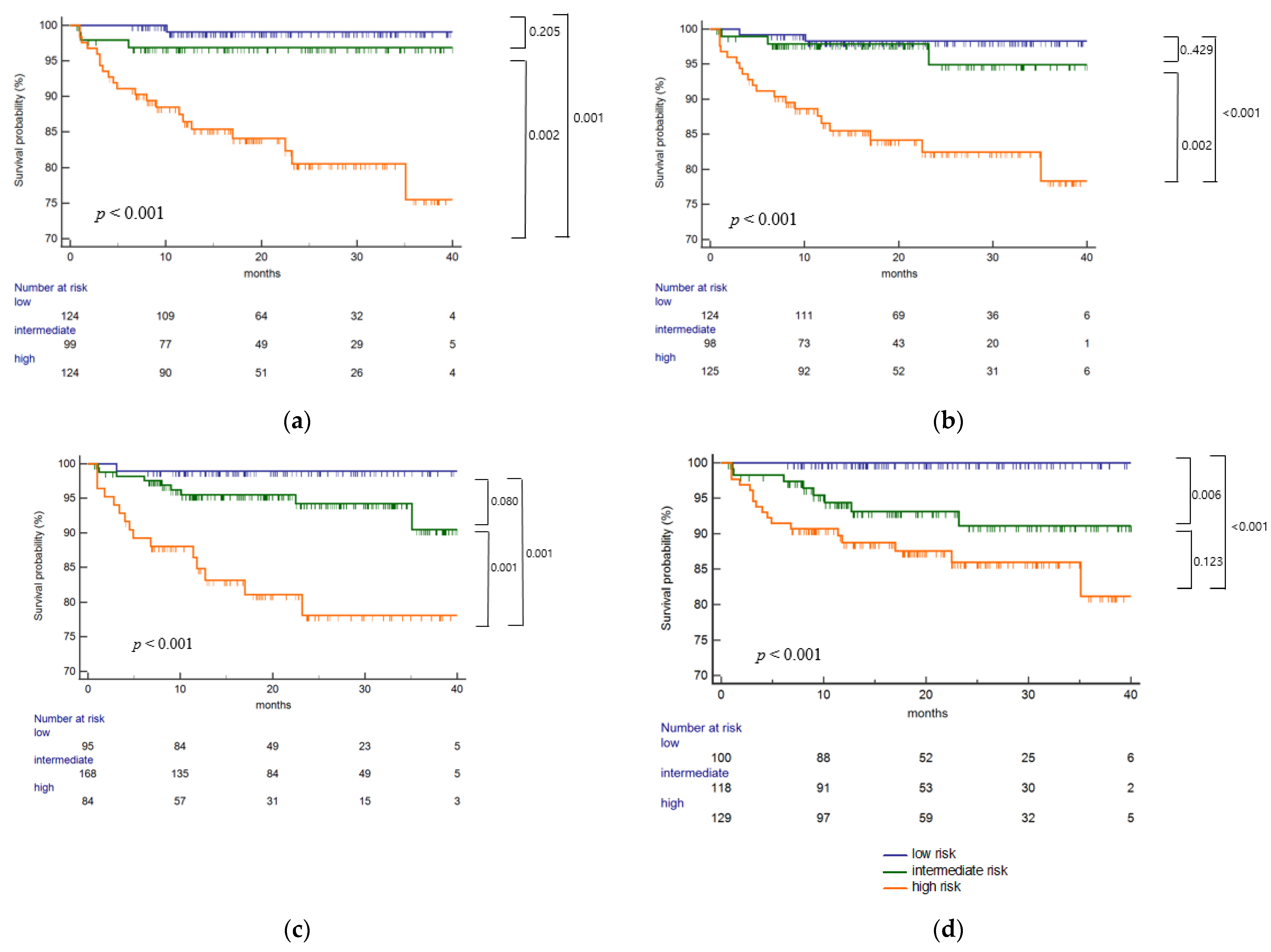
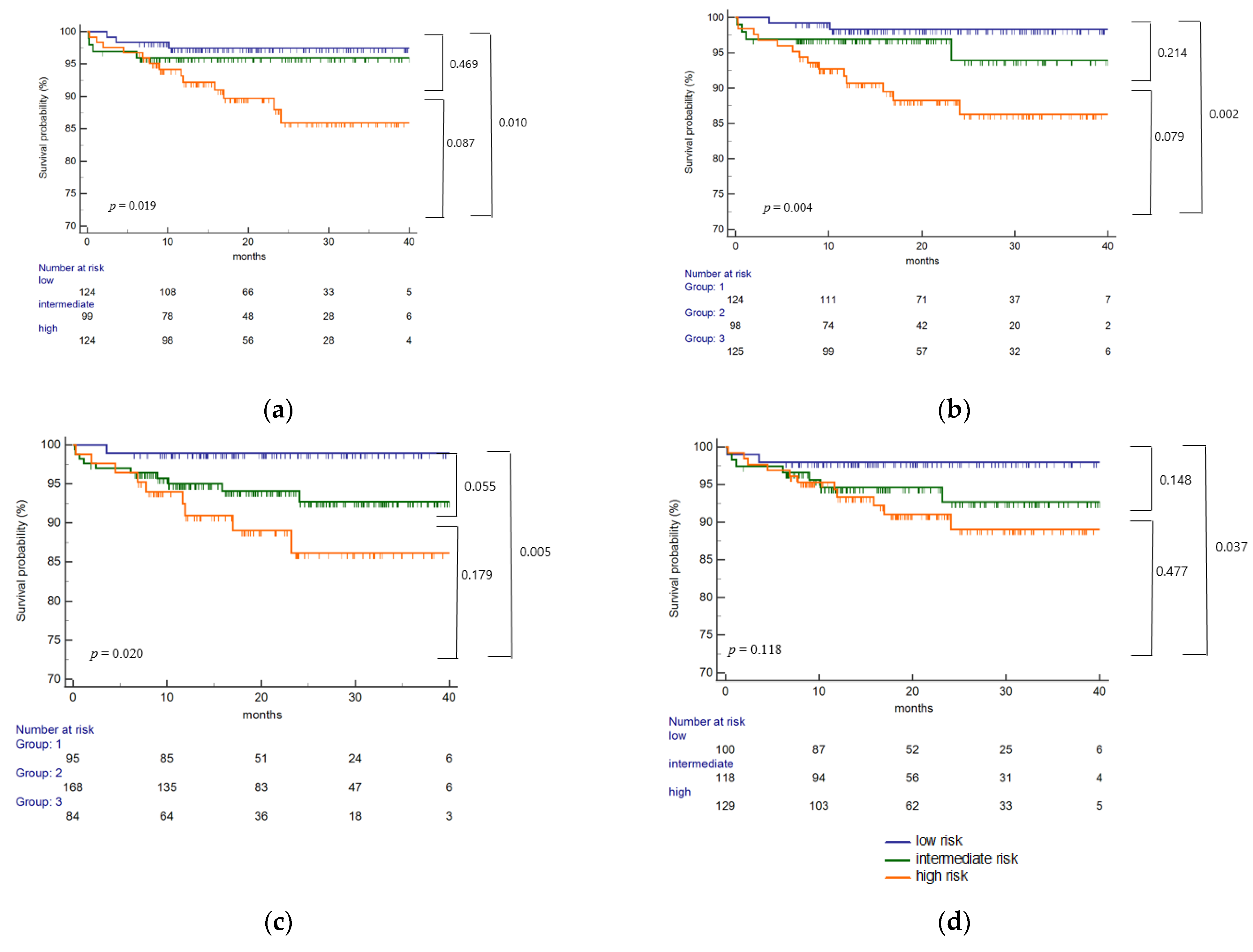
2.4. Eplet Mismatch and Risk of HLA Class II dnDSA
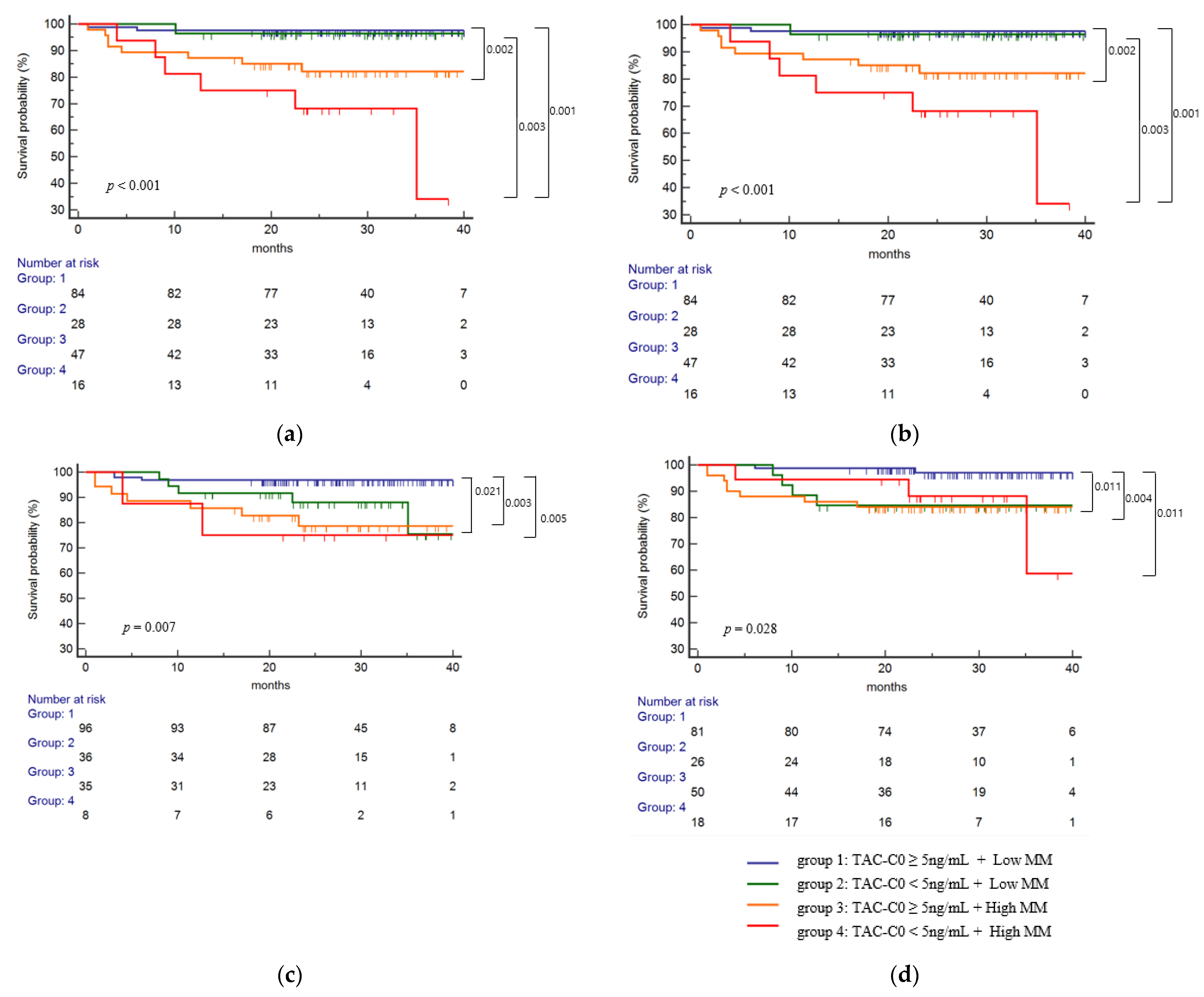
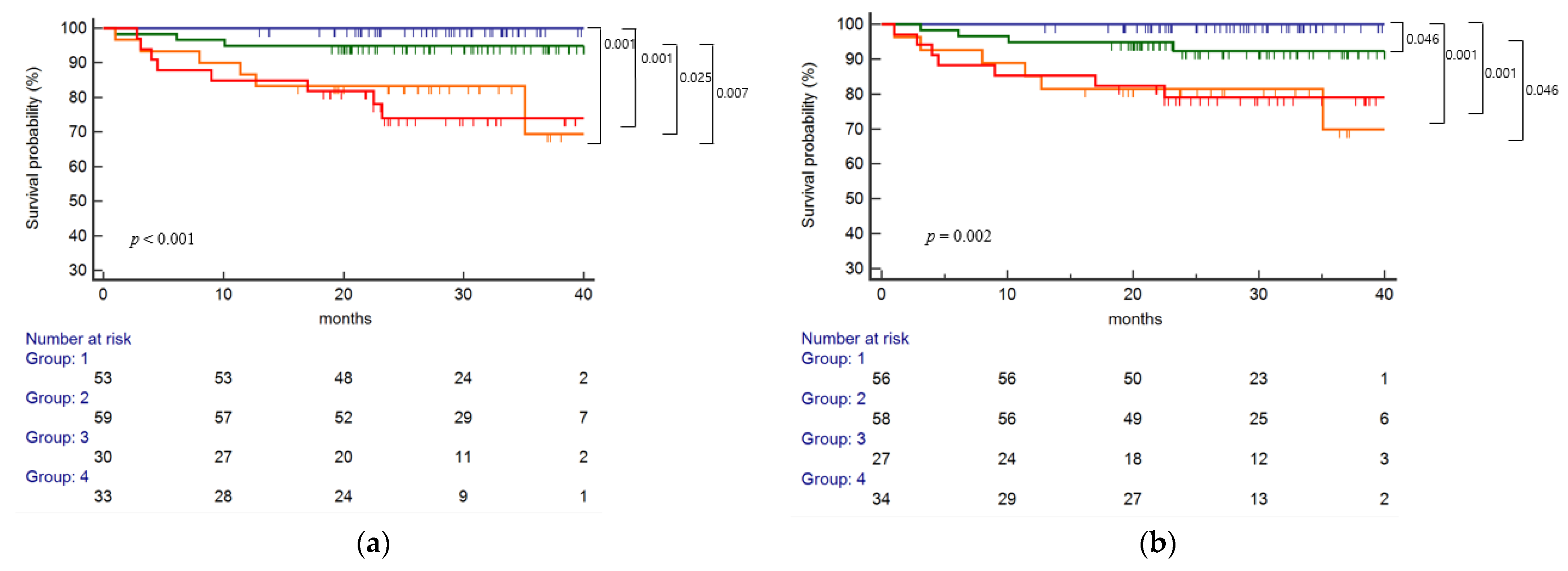
2.5. Eplet Mismatch and TAC-C0 on the Risk of HLA Class II dnDSA
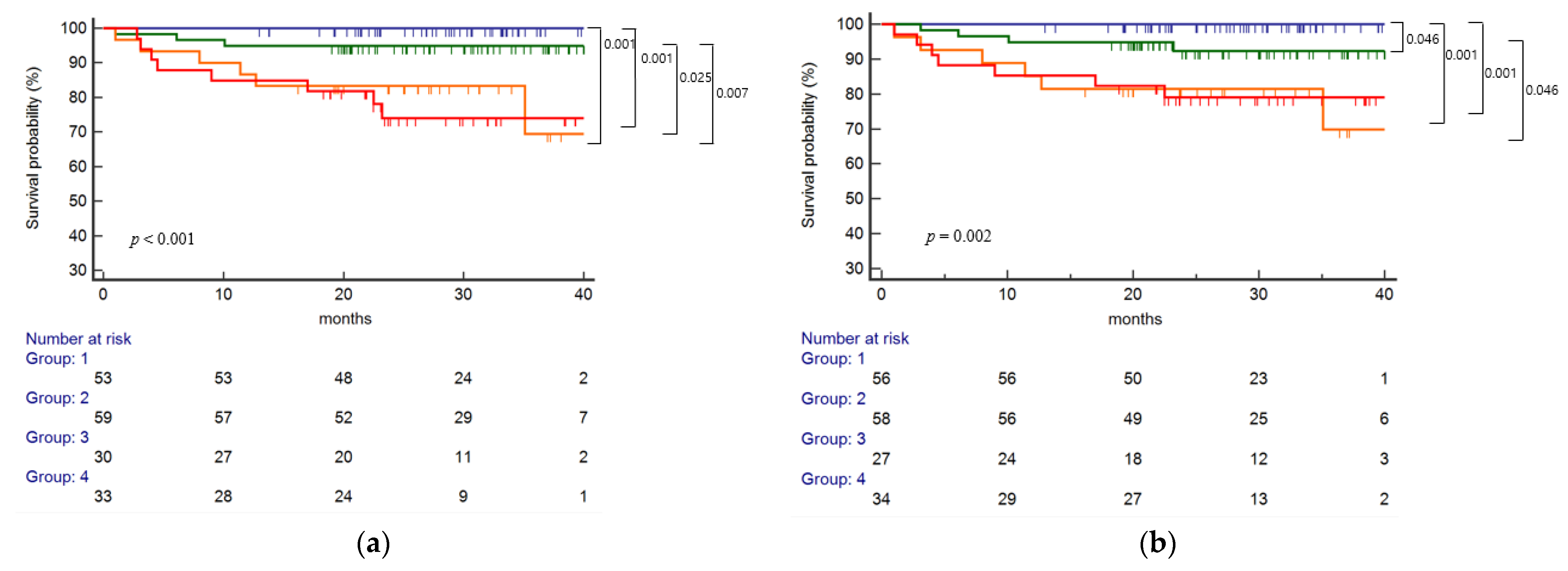
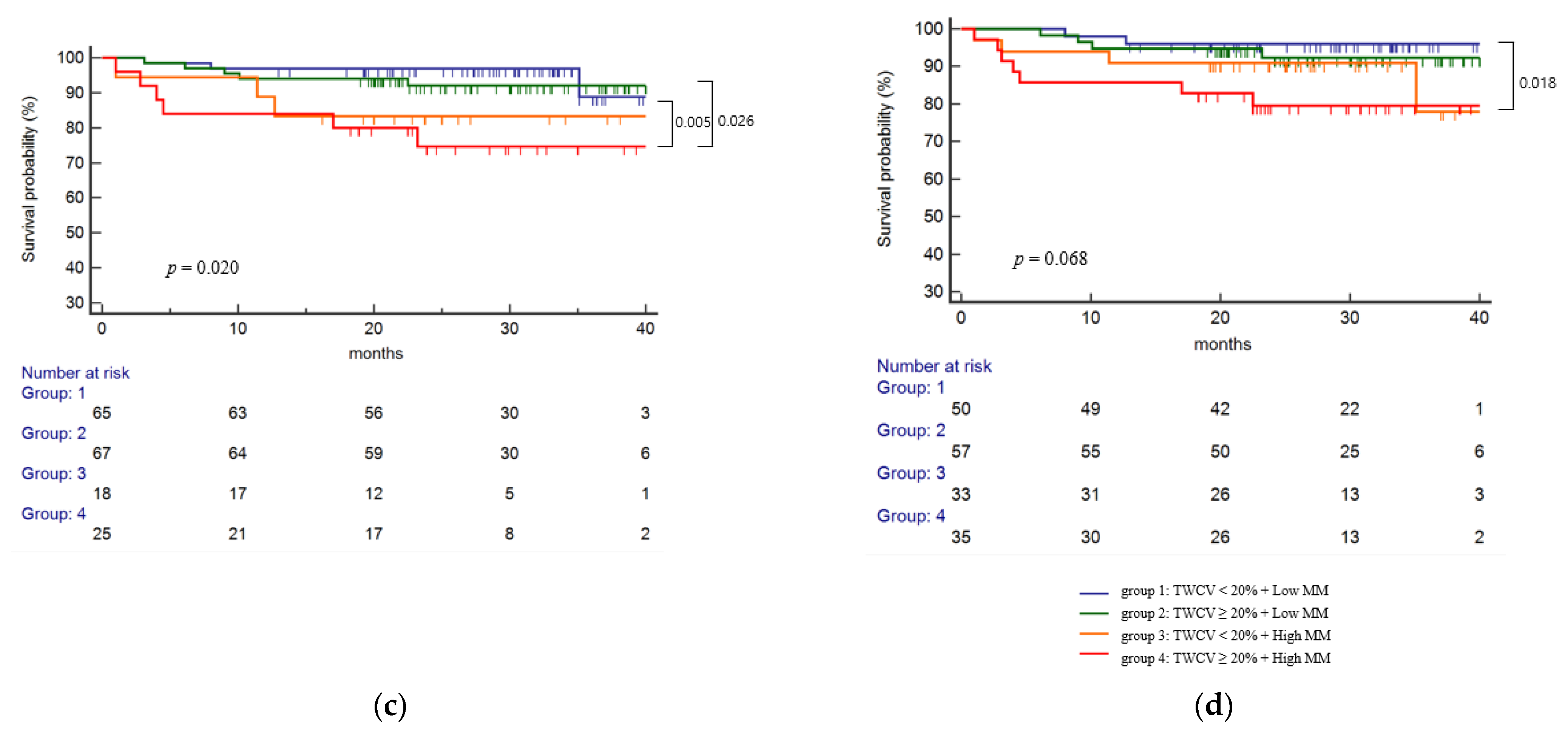
2.6. Eplet Mismatch and TWCV on the Risk of HLA Class II dnDSA
2.7. Multivariable Analysis for the Risk of HLA Class II dnDSA
2.8. Subgroup Analysis for the Risk of HLA-DQ dnDSA
2.9. Eplet Mismatch and Antibody Mediated Rejection Development
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. HLA Typing, Antibody Screening and Eplet Analysis
4.3. Immunosuppression Regimen
4.4. Tacrolimus Variability
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coemans, M.; Susal, C.; Dohler, B.; Anglicheau, D.; Giral, M.; Bestard, O.; Legendre, C.; Emonds, M.P.; Kuypers, D.; Molenberghs, G.; et al. Analyses of the short- and long-term graft survival after kidney transplantation in Europe between 1986 and 2015. Kidney Int. 2018, 94, 964–973. [Google Scholar] [CrossRef]
- Bestard, O.; Meneghini, M.; Crespo, E.; Bemelman, F.; Koch, M.; Volk, H.D.; Viklicky, O.; Giral, M.; Banas, B.; Ruiz, J.C.; et al. Preformed T-cell alloimmunity and HLA eplet mismatch to guide immunosuppression minimization with Tacrolimus monotherapy in Kidney Transplantation. Results of the CELLIMIN trial. Am. J. Transplant. 2021, 21, 2833–2845. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Gibson, I.W.; Blydt-Hansen, T.D.; Karpinski, M.; Ho, J.; Storsley, L.J.; Goldberg, A.; Birk, P.E.; Rush, D.N.; Nickerson, P.W. Evolution and clinical pathologic correlations of de novo donor-specific HLA antibody post kidney transplant. Am. J. Transplant. 2012, 12, 1157–1167. [Google Scholar] [CrossRef]
- Tafulo, S.; Malheiro, J.; Santos, S.; Dias, L.; Almeida, M.; Martins, S.; Pedroso, S.; Mendes, C.; Lobato, L.; Castro-Henriques, A. HLA class II eplet mismatch load improves prediction of dnDSA development after living donor kidney transplantation. Int. J. Immunogenet. 2021, 48, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tambur, A.R.; Claas, F.H. HLA epitopes as viewed by antibodies: What is it all about? Am. J. Transplant. 2015, 15, 1148–1154. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S.; Iwasaki, K.; Tomosugi, T.; Niemann, M.; Spierings, E.; Miwa, Y.; Horimi, K.; Takeda, A.; Goto, N.; Narumi, S.; et al. Analysis of T and B Cell Epitopes to Predict the Risk of de novo Donor-Specific Antibody (DSA) Production After Kidney Transplantation: A Two-Center Retrospective Cohort Study. Front Immunol. 2020, 11, 2000. [Google Scholar] [CrossRef] [PubMed]
- Duquesnoy, R.J.; Marrari, M.; da M. Sousa, L.C.; de M Barroso, J.R.B.; de S. U. Aita, K.M.; da Silva, A.S.; do Monte, S.J. 16th IHIW: A website for antibody-defined HLA epitope Registry. Int. J. Immunogenet. 2013, 40, 54–59. [Google Scholar] [CrossRef]
- Duquesnoy, R.J. Human leukocyte antigen epitope antigenicity and immunogenicity. Curr. Opin. Organ. Transplant. 2014, 19, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Sapir-Pichhadze, R.; Tinckam, K.; Quach, K.; Logan, A.G.; Laupacis, A.; John, R.; Beyene, J.; Kim, S.J. HLA-DR and -DQ eplet mismatches and transplant glomerulopathy: A nested case-control study. Am. J. Transplant. 2015, 15, 137–148. [Google Scholar] [CrossRef] [Green Version]
- Wiebe, C.; Nevins, T.E.; Robiner, W.N.; Thomas, W.; Matas, A.J.; Nickerson, P.W. The Synergistic Effect of Class II HLA Epitope-Mismatch and Nonadherence on Acute Rejection and Graft Survival. Am. J. Transplant. 2015, 15, 2197–2202. [Google Scholar] [CrossRef] [Green Version]
- Wiebe, C.; Pochinco, D.; Blydt-Hansen, T.D.; Ho, J.; Birk, P.E.; Karpinski, M.; Goldberg, A.; Storsley, L.J.; Gibson, I.W.; Rush, D.N.; et al. Class II HLA epitope matching-A strategy to minimize de novo donor-specific antibody development and improve outcomes. Am. J. Transplant. 2013, 13, 3114–3122. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Nickerson, P.W. Human leukocyte antigen molecular mismatch to risk stratify kidney transplant recipients. Curr. Opin. Organ. Transplant. 2020, 25, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Kosmoliaptsis, V.; Pochinco, D.; Gibson, I.W.; Ho, J.; Birk, P.E.; Goldberg, A.; Karpinski, M.; Shaw, J.; Rush, D.N.; et al. HLA-DR/DQ molecular mismatch: A prognostic biomarker for primary alloimmunity. Am. J. Transplant. 2019, 19, 1708–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duquesnoy, R.J.; Marrari, M.; Tambur, A.R.; Mulder, A.; Sousa, L.C.; da Silva, A.S.; do Monte, S.J. First report on the antibody verification of HLA-DR, HLA-DQ and HLA-DP epitopes recorded in the HLA Epitope Registry. Hum. Immunol. 2014, 75, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Ekberg, H.; Tedesco-Silva, H.; Demirbas, A.; Vítko, S.; Nashan, B.; Gürkan, A.; Margreiter, R.; Hugo, C.; Grinyó, J.M.; Frei, U.; et al. Reduced exposure to calcineurin inhibitors in renal transplantation. N. Engl. J. Med. 2007, 357, 2562–2575. [Google Scholar] [CrossRef] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9 (Suppl. 3), S1–S155. [Google Scholar] [CrossRef]
- Jouve, T.; Fonrose, X.; Noble, J.; Janbon, B.; Fiard, G.; Malvezzi, P.; Stanke-Labesque, F.; Rostaing, L. The TOMATO Study (Tacrolimus Metabolization in Kidney Transplantation): Impact of the Concentration-Dose Ratio on Death-censored Graft Survival. Transplantation 2020, 104, 1263–1271. [Google Scholar] [CrossRef]
- Wiebe, C.; Rush, D.N.; Nevins, T.E.; Birk, P.E.; Blydt-Hansen, T.; Gibson, I.W.; Goldberg, A.; Ho, J.; Karpinski, M.; Pochinco, D.; et al. Class II Eplet Mismatch Modulates Tacrolimus Trough Levels Required to Prevent Donor-Specific Antibody Development. J. Am. Soc. Nephrol. 2017, 28, 3353–3362. [Google Scholar] [CrossRef] [Green Version]
- Beland, M.A.; Lapointe, I.; Noel, R.; Cote, I.; Wagner, E.; Riopel, J.; Latulippe, E.; Desy, O.; Beland, S.; Magee, C.N.; et al. Higher calcineurin inhibitor levels predict better kidney graft survival in patients with de novo donor-specific anti-HLA antibodies: A cohort study. Transpl. Int. 2017, 30, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Davis, S.; Gralla, J.; Klem, P.; Tong, S.; Wedermyer, G.; Freed, B.; Wiseman, A.; Cooper, J.E. Lower tacrolimus exposure and time in therapeutic range increase the risk of de novo donor-specific antibodies in the first year of kidney transplantation. Am. J. Transplant. 2018, 18, 907–915. [Google Scholar] [CrossRef] [Green Version]
- Wen, J.; Basu, A.; Bentall, A.; Henderson, N.; Dukek, B.; Gandhi, M.; Schinstock, C. Is the level of HLA eplet mismatch a risk factor for graft loss among kidney transplant recipients who have already formed de novo donor specific antibody? Hum. Immunol. 2021, 82, 240–246. [Google Scholar] [CrossRef]
- Kosmoliaptsis, V.; Mallon, D.H.; Chen, Y.; Bolton, E.M.; Bradley, J.A.; Taylor, C.J. Alloantibody Responses After Renal Transplant Failure Can Be Better Predicted by Donor-Recipient HLA Amino Acid Sequence and Physicochemical Disparities Than Conventional HLA Matching. Am. J. Transplant. 2016, 16, 2139–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallon, D.H.; Kling, C.; Robb, M.; Ellinghaus, E.; Bradley, J.A.; Taylor, C.J.; Kabelitz, D.; Kosmoliaptsis, V. Predicting Humoral Alloimmunity from Differences in Donor and Recipient HLA Surface Electrostatic Potential. J. Immunol. 2018, 201, 3780–3792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, C.S.M.; Koster, J.; Haasnoot, G.W.; Roelen, D.L.; Claas, F.H.J.; Heidt, S. HLA-EMMA: A user-friendly tool to analyse HLA class I and class II compatibility on the amino acid level. HLA 2020, 96, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Geneugelijk, K.; Spierings, E. PIRCHE-II: An algorithm to predict indirectly recognizable HLA epitopes in solid organ transplantation. Immunogenetics 2020, 72, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Wiebe, C.; Kosmoliaptsis, V.; Pochinco, D.; Taylor, C.J.; Nickerson, P. A comparison of HLA Molecular Mismatch Methods to Determine HLA Immunogenicity. Transplantation 2018, 102, 1338–1343. [Google Scholar] [CrossRef] [Green Version]
- In, J.W.; Roh, E.Y.; Oh, S.; Shin, S.; Park, K.U.; Song, E.Y. Allele and Haplotype Frequencies of Human Leukocyte Antigen-A,-B,-C,-DRB1, and -DQB1 from Sequence-Based DNA Typing Data in Koreans. Ann. Lab. Med. 2015, 35, 429–435. [Google Scholar] [CrossRef]
- Sharma, A.; Taverniti, A.; Graf, N.; Teixeira-Pinto, A.; Lewis, J.R.; Lim, W.H.; Alexander, S.I.; Durkan, A.; Craig, J.C.; Wong, G. The association between human leukocyte antigen eplet mismatches, de novo donor-specific antibodies, and the risk of acute rejection in pediatric kidney transplant recipients. Pediatr. Nephrol. 2020, 35, 1061–1068. [Google Scholar] [CrossRef]
- Lemieux, W.; Mohammadhassanzadeh, H.; Klement, W.; Daniel, C.; Sapir-Pichhadze, R. Matchmaker, matchmaker make me a match: Opportunities and challenges in optimizing compatibility of HLA eplets in transplantation. Int. J. Immunogenet. 2021, 48, 135–144. [Google Scholar] [CrossRef]
- D’Souza, Y.; Ferradji, A.; Saw, C.; Oualkacha, K.; Richard, L.; Popradi, G.; Sapir-Pichhadze, R. Inaccuracies in epitope repertoire estimations when using Multi-Locus Allele-Level hla genotype imputation tools. HLA 2018, 92, 33–39. [Google Scholar] [CrossRef]
- Engen, R.M.; Jedraszko, A.M.; Conciatori, M.A.; Tambur, A.R. Substituting imputation of HLA antigens for high-resolution HLA typing: Evaluation of a multiethnic population and implications for clinical decision making in transplantation. Am. J. Transplant. 2021, 21, 344–352. [Google Scholar] [CrossRef]
- Senev, A.; Coemans, M.; Lerut, E.; Van Sandt, V.; Kerkhofs, J.; Daniels, L.; Driessche, M.V.; Compernolle, V.; Sprangers, B.; Van Loon, E.; et al. Eplet Mismatch Load and de novo Occurrence of Donor-Specific Anti-HLA Antibodies, Rejection, and Graft Failure after Kidney Transplantation: An Observational Cohort Study. J. Am. Soc. Nephrol. 2020, 31, 2193–2204. [Google Scholar] [CrossRef] [PubMed]
- Bezstarosti, S.; Kramer, C.S.M.; Claas, F.H.J.; de Fijter, J.W.; Reinders, M.E.J.; Heidt, S. Implementation of molecular matching in transplantation requires further characterization of both immunogenicity and antigenicity of individual HLA epitopes. Hum. Immunol. 2021, 23, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Sapir-Pichhadze, R.; Zhang, X.; Ferradji, A.; Madbouly, A.; Tinckam, K.J.; Gebel, H.M.; Blum, D.; Marrari, M.; Kim, S.J.; Fingerson, S.; et al. Epitopes as characterized by antibody-verified eplet mismatches determine risk of kidney transplant loss. Kidney Int. 2020, 97, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guiral, S.; Segundo, D.S.; Irure, J.; Casafont, F.; Fortea, J.I.; Puente, A.; Lopez-Hoyos, M.; Crespo, J.; Fabrega, E. Number of Antibody-verified Eplet in HLA-C Locus as an Independent Factor of T-cell-Mediated Rejection After Liver Transplantation. Transplantation 2020, 104, 562–567. [Google Scholar] [CrossRef]
- Snanoudj, R.; Kamar, N.; Cassuto, E.; Caillard, S.; Metzger, M.; Merville, P.; Thierry, A.; Jollet, I.; Grimbert, P.; Anglicheau, D.; et al. Epitope load identifies kidney transplant recipients at risk of allosensitization following minimization of immunosuppression. Kidney Int. 2019, 95, 1471–1485. [Google Scholar] [CrossRef]
- Tambur, A.R.; Kosmoliaptsis, V.; Claas, F.H.J.; Mannon, R.B.; Nickerson, P.; Naesens, M. Significance of HLA-DQ in kidney transplantation: Time to reevaluate human leukocyte antigen-matching priorities to improve transplant outcomes? An expert review and recommendations. Kidney Int. 2021, 100, 1012–1022. [Google Scholar] [CrossRef]
- Iwami, D.; Hotta, K.; Sasaki, H.; Hirose, T.; Higuchi, H.; Takada, Y.; Shinohara, N. Highly Immunogenic DQB1 Mismatch Eplets Are Associated with Development of Chronic Active Antibody-Mediated Rejection: A First Report from Japan. Transplant. Proc. 2017, 49, 84–87. [Google Scholar] [CrossRef]
- Vanhove, T.; Vermeulen, T.; Annaert, P.; Lerut, E.; Kuypers, D.R.J. High Intrapatient Variability of Tacrolimus Concentrations Predicts Accelerated Progression of Chronic Histologic Lesions in Renal Recipients. Am. J. Transplant. 2016, 16, 2954–2963. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, E.; Segundo, D.S.; Fernandez-Fresnedo, G.; Lopez-Hoyos, M.; Benito, A.; Ruiz, J.C.; de Cos, M.A.; Arias, M. Within-Patient Variability in Tacrolimus Blood Levels Predicts Kidney Graft Loss and Donor-Specific Antibody Development. Transplantation 2016, 100, 2479–2485. [Google Scholar] [CrossRef]
- Park, S.; Kim, Y.S.; Lee, J.; Huh, W.; Yang, C.W.; Kim, Y.L.; Kim, Y.H.; Kim, J.K.; Oh, C.K.; Park, S.K. Reduced Tacrolimus Trough Level Is Reflected by Estimated Glomerular Filtration Rate (eGFR) Changes in Stable Renal Transplantation Recipients: Results of the OPTIMUM Phase 3 Randomized Controlled Study. Ann. Transplant. 2018, 23, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Lee, H.; Eum, S.H.; Kim, H.D.; Ko, E.J.; Yang, C.W.; Chung, B.H. Intrapatient Variability in Tacrolimus Trough Levels over 2 Years Affects Long-Term Allograft Outcomes of Kidney Transplantation. Front. Immunol. 2021, 12, 746013. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Lee, Y.J.; Jang, S.B.; Lee, J.E.; Kim, K.H.; Park, K. Influence of the CYP3A5 and MDR1 genetic polymorphisms on the pharmacokinetics of tacrolimus in healthy Korean subjects. Br. J. Clin. Pharmacol. 2007, 64, 185–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Han, E.; Choi, A.R.; Ban, T.H.; Chung, B.H.; Yang, C.W.; Choi, Y.J.; Oh, E.J. Clinical impact of complement (C1q, C3d) binding De Novo donor-specific HLA antibody in kidney transplant recipients. PLoS ONE 2018, 13, e0207434. [Google Scholar] [CrossRef]
- Kang, H.; Yoo, J.; Lee, S.Y.; Oh, E.J. Causes of Positive Pretransplant Crossmatches in the Absence of Donor-Specific Anti-Human Leukocyte Antigen Antibodies: A Single-Center Experience. Ann. Lab. Med. 2021, 41, 429–435. [Google Scholar] [CrossRef]
- Chung, B.H.; Kim, K.W.; Kim, B.M.; Piao, S.G.; Lim, S.W.; Choi, B.S.; Park, C.W.; Kim, Y.S.; Cho, M.L.; Yang, C.W. Dysregulation of Th17 cells during the early post-transplant period in patients under calcineurin inhibitor based immunosuppression. PLoS ONE 2012, 7, e42011. [Google Scholar] [CrossRef] [Green Version]
- Chung, B.H.; Joo, Y.Y.; Lee, J.; Kim, H.D.; Kim, J.I.; Moon, I.S.; Choi, B.S.; Oh, E.J.; Park, C.W.; Kim, Y.S.; et al. Impact of ABO Incompatibility on the Development of Acute Antibody-Mediated Rejection in Kidney Transplant Recipients Presensitized to HLA. PLoS ONE 2015, 10, e0123638. [Google Scholar]
- Shuker, N.; van Gelder, T.; Hesselink, D.A. Intra-patient variability in tacrolimus exposure: Causes, consequences for clinical management. Transplant. Rev. 2015, 29, 78–84. [Google Scholar] [CrossRef]
- Rozen-Zvi, B.; Schneider, S.; Lichtenberg, S.; Green, H.; Cohen, O.; Gafter, U.; Chagnac, A.; Mor, E.; Rahamimov, R. Association of the combination of time-weighted variability of tacrolimus blood level and exposure to low drug levels with graft survival after kidney transplantation. Nephrol. Dial. Transplant. 2017, 32, 393–399. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 347) | dn Class II DSA (+) (n = 25) | dn Class II DSA (−) (n = 322) | p Value | |
|---|---|---|---|---|
| Age (years) mean ± SD | 50.0 ± 12.3 | 47.4 ± 11.6 | 50.3 ± 12.4 | 0.249 |
| Male recipient, n (%) | 223 (64.3) | 16 (64.0) | 207 (64.0) | 0.998 |
| Deceased donor, n (%) | 22 (6.3) | 1 (4.0) | 21 (6.5) | 0.619 |
| Retransplantation, n (%) | 29 (8.4) | 1 (4.0) | 28 (8.7) | 0.703 |
| ABO incompatible, n (%) | 95 (27.4) | 7 (28.0) | 88 (27.3) | 0.942 |
| High PRA (>50%), n (%) | 64 (17.1) | 3 (12.0) | 61 (18.9) | 0.389 |
| Preexisting renal disease | 0.701 | |||
| DM, n (%) | 98 (28.2) | 8 (32) | 90 (27.9) | |
| HTN, n (%) | 47 (13.5) | 3 (12.0) | 44 (13.7) | |
| Chronic GN, n (%) | 119 (34.3) | 8 (32.0) | 111 (34.5) | |
| PCKD, n (%) | 15 (4.3) | 0 | 15 (4.7) | |
| SLE, n (%) | 12 (3.5) | 2 (8.0) | 10 (3.1) | |
| Others, n (%) | 56 (16.1) | 4 (16.0) | 52 (16.1) | |
| Preemptive KT, n (%) | 125 (56.1) | 10 (40.0) | 115 (35.7) | |
| Follow-up (months), mean ± SD | 21.5 ± 10.6 | 21.5 ± 10.6 | 21.5 ± 10.6 | 0.975 |
| HLA class I Ag MM, mean ± SD | 3.1 ± 1.7 | 3.4 ± 1.6 | 3.1 ± 1.7 | 0.348 |
| HLA class II Ag MM, mean ± SD | 2.0 ± 1.2 | 2.4 ± 0.9 | 1.9 ± 1.2 | 0.018 |
| Induction, n (%) | 0.801 | |||
| Basiliximab | 285 (82.1) | 21 (84.0) | 264 (82.0) | |
| ATG | 62 (17.9) | 4 (16.0) | 58 (18.0) | |
| Maintenance immunosuppression, n (%) | 0.821 | |||
| Tacrolimus | 342 (98.6) | 25 (100) | 317 (98.4) | |
| Cyclosporine | 3 (0.9) | 0 | 3 (0.9) | |
| Sirolimus | 2 (0.6) | 0 | 2 (0.6) |
| Single Molecular Eplet | Total Eplet | Antibody-Verified Eplet | Antibody-Verified Single Molecular | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Eplet MM & TAC-T0 | ||||||||
| Group 1 | Reference | Reference | Reference | Reference | ||||
| Group 2 | 1.51 (0.14–16.67) | 0.736 | 1.14 (0.12–10.92) | 0.912 | 4.69 (1.12–19.64) | 0.034 | 1.51 (0.14–16.67) | 0.736 |
| Group 3 | 9.14 (1.97–42.40) | 0.005 | 6.99 (1.81–26.95) | 0.005 | 9.51 (2.48–36.50) | 0.001 | 9.14 (1.97–42.40) | 0.005 |
| Group 4 | 16.10 (3.12–83.23) | 0.001 | 10.13 (2.41–42.45) | 0.002 | 5.04 (0.52–48.61) | 0.162 | 16.10 (3.12–83.23) | 0.001 |
| Eplet MM & TWCV | ||||||||
| Group 1 | Reference | Reference | Reference | Reference | ||||
| Group 2 | 1.78 (0.16–19.59) | 0.640 | 0.92 (0.13–6.56) | 0.935 | 0.97 (0.24–3.88) | 0.964 | 1.78 (0.16–19.59) | 0.640 |
| Group 3 | 13.72 (1.69–111.51) | 0.014 | 7.23 (1.46–35.86) | 0.016 | 4.52 (1.12–18.21) | 0.034 | 13.72 (1.69–111.51) | 0.014 |
| Group 4 | 13.41 (1.65–109.21) | 0.015 | 7.72 (1.57–37.94) | 0.012 | 4.14 (1.10–15.55) | 0.035 | 13.41 (1.65–109.21) | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Min, J.W.; Kang, H.; Lee, H.; Eum, S.H.; Park, Y.; Yang, C.W.; Chung, B.H.; Oh, E.-J. Combined Analysis of HLA Class II Eplet Mismatch and Tacrolimus Levels for the Prediction of De Novo Donor Specific Antibody Development in Kidney Transplant Recipients. Int. J. Mol. Sci. 2022, 23, 7357. https://doi.org/10.3390/ijms23137357
Lee H, Min JW, Kang H, Lee H, Eum SH, Park Y, Yang CW, Chung BH, Oh E-J. Combined Analysis of HLA Class II Eplet Mismatch and Tacrolimus Levels for the Prediction of De Novo Donor Specific Antibody Development in Kidney Transplant Recipients. International Journal of Molecular Sciences. 2022; 23(13):7357. https://doi.org/10.3390/ijms23137357
Chicago/Turabian StyleLee, Hyeyoung, Ji Won Min, Hyunhye Kang, Hanbi Lee, Sang Hun Eum, Yohan Park, Chul Woo Yang, Byung Ha Chung, and Eun-Jee Oh. 2022. "Combined Analysis of HLA Class II Eplet Mismatch and Tacrolimus Levels for the Prediction of De Novo Donor Specific Antibody Development in Kidney Transplant Recipients" International Journal of Molecular Sciences 23, no. 13: 7357. https://doi.org/10.3390/ijms23137357
APA StyleLee, H., Min, J. W., Kang, H., Lee, H., Eum, S. H., Park, Y., Yang, C. W., Chung, B. H., & Oh, E.-J. (2022). Combined Analysis of HLA Class II Eplet Mismatch and Tacrolimus Levels for the Prediction of De Novo Donor Specific Antibody Development in Kidney Transplant Recipients. International Journal of Molecular Sciences, 23(13), 7357. https://doi.org/10.3390/ijms23137357