
Identification of Novel lncRNAs in Ovarian Cancer and Their Impact on Overall Survival

 , ,
, ,
Abstract
1. Introduction
2. Results
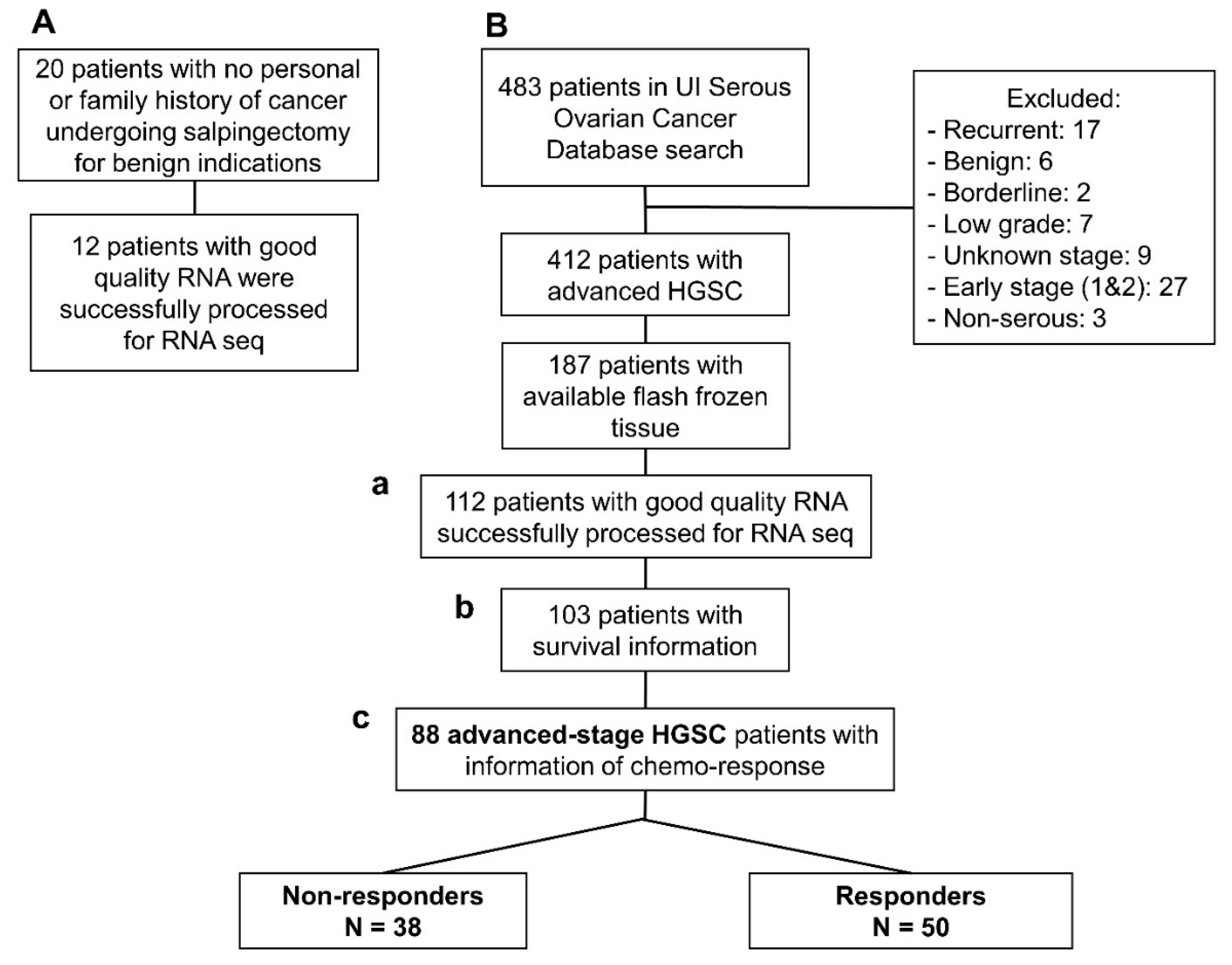
2.1. Association with HGSC
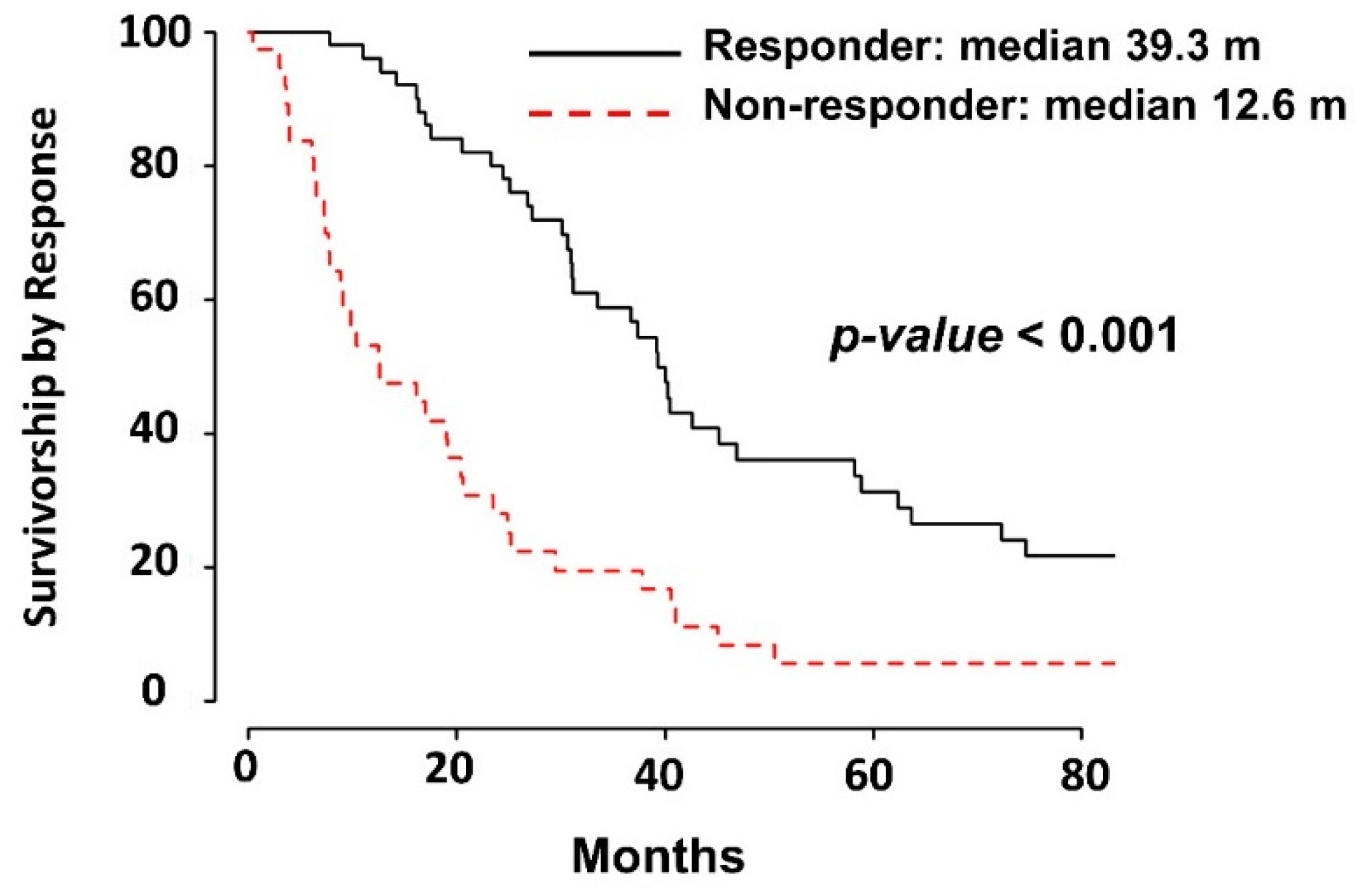
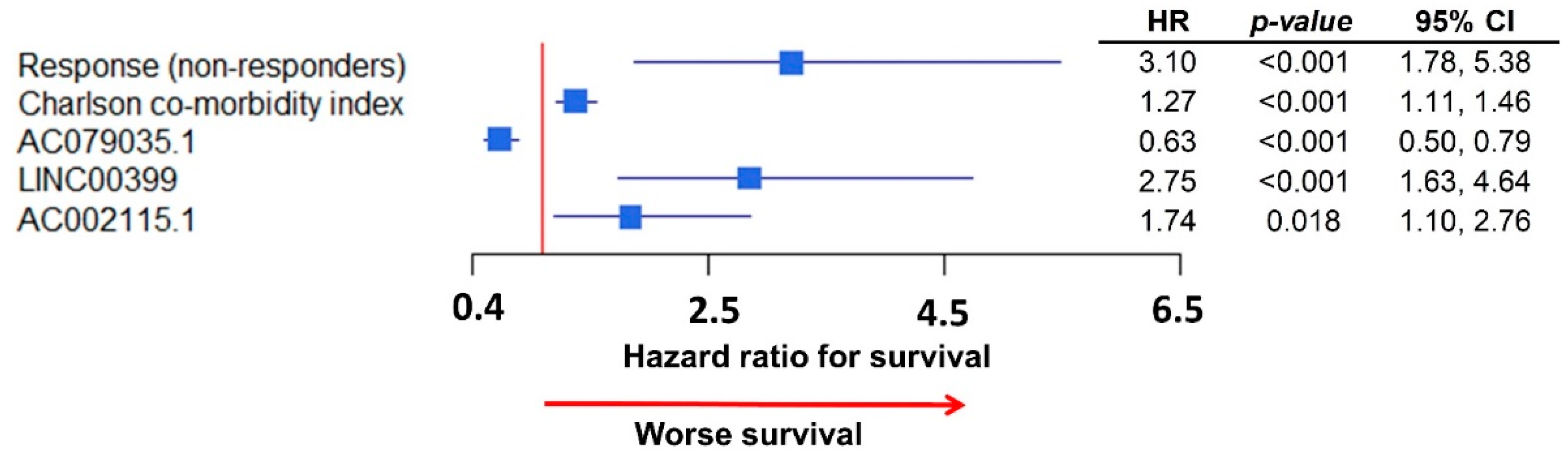
2.2. Association of lncRNAs with Survival
2.3. Association of lncRNAs with Chemo-Response
2.4. Validation of Analyses in the Cancer Genome Atlas (TCGA) HGSC Dataset
3. Discussion
4. Materials and Methods
4.1. Tissue Procurement and Processing
4.2. Clinical Data
4.3. RNA Sequencing
4.4. lncRNA Detection
4.5. Statistical Analysis
4.5.1. Association with HGSC
4.5.2. Association with Survival
4.5.3. Association with Chemo-Response
4.5.4. Validation of Analysis within TCGA Ovarian Cancer Dataset
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Noone, A.M.; Krapcho, M. SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2019. [Google Scholar]
- Reid, B.M.; Permuth, J.B.; Sellers, T.A. Epidemiology of ovarian cancer: A review. Cancer Biol. Med. 2017. [Google Scholar] [CrossRef]
- Kehoe, S.; Hook, J.; Nankivell, M. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015. [Google Scholar] [CrossRef]
- Stark, D.; Nankivell, M.; Pujade-Lauraine, E. Standard chemotherapy with or without bevacizumab in advanced ovarian cancer: Quality-of-life outcomes from the International Collaboration on Ovarian Neoplasms (ICON7) phase 3 randomised trial. Lancet Oncol. 2013. [Google Scholar] [CrossRef]
- Burger, R.A.; Brady, M.F.; Bookman, M.A. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N. Engl. J. Med. 2011. [Google Scholar] [CrossRef]
- Friedlander, M.; Stockler, M. Clinical trials of palliative chemotherapy in platinum-resistant or -refractory ovarian cancer: Time to think differently? J. Clin. Oncol. 2013. [Google Scholar] [CrossRef]
- Coleman, R.L. Ovarian cancer in 2015: Insights into strategies for optimizing ovarian cancer care. Nat. Rev. Clin. Oncol. 2016. [Google Scholar] [CrossRef]
- Li, Z.Y.; Wang, X.L. Long non-coding RNA UCA1 promotes the progression of paclitaxel resistance in ovarian cancer by regulating the miR-654-5p/SIK2 axis. Eur. Rev. Med. Pharmacol. Sci. 2020. [Google Scholar] [CrossRef]
- Lund, R.J.; Huhtinen, K.; Salmi, J. DNA methylation and Transcriptome Changes Associated with Cisplatin Resistance in Ovarian Cancer. Sci. Rep. 2017. [Google Scholar] [CrossRef]
- Pokhriyal, R.; Hariprasad, R.; Kumar, L.; Hariprasad, G. Chemotherapy Resistance in Advanced Ovarian Cancer Patients. Biomark. Cancer 2019. [Google Scholar] [CrossRef]
- Rupaimoole, R.; Slack, F.J. MicroRNA therapeutics: Towards a new era for the management of cancer and other diseases. Nat. Rev. Drug Discov. 2017. [Google Scholar] [CrossRef]
- Sullenger, B.A.; Nair, S. From the RNA world to the clinic. Science 2016. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.C.; Chang, H.Y. Molecular Mechanisms of Long Noncoding RNAs. Mol. Cell 2011. [Google Scholar] [CrossRef] [PubMed]
- Atianand, M.K.; Fitzgerald, K.A. Long non-coding rnas and control of gene expression in the immune system. Trends Mol. Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Wambecke, A.; Ahmad, M.; Lambert, B. The influence of long non-coding RNAs on the response to chemotherapy in ovarian cancer. Gynecol. Oncol. 2020. [Google Scholar] [CrossRef]
- Sun, Z.; Nair, A.; Chen, X.; Prodduturi, N.; Wang, J.; Kocher, J.P. UClncR: Ultrafast and comprehensive long non-coding RNA detection from RNA-seq. Sci. Rep. 2017. [Google Scholar] [CrossRef]
- Lawo, S.; Bashkurov, M.; Mullin, M. HAUS, the 8-Subunit Human Augmin Complex, Regulates Centrosome and Spindle Integrity. Curr. Biol. 2009. [Google Scholar] [CrossRef]
- Yates, A.D.; Achuthan, P.; Akanni, W. Ensembl 2020. Nucleic Acids Res. 2020. [Google Scholar] [CrossRef]
- Taniguchi-Ponciano, K.; Huerta-Padilla, V.; Baeza-Xochihua, V. Revisiting the Genomic and Transcriptomic Landscapes from Female Malignancies Could Provide Molecular Markers and Targets for Precision Medicine. Arch. Med. Res. 2019. [Google Scholar] [CrossRef]
- Wang, S.; Xu, M.; Sun, Z.; Yu, X.; Deng, Y.; Chang, H. LINC01018 confers a novel tumor suppressor role in hepatocellular carcinoma through sponging microRNA-182-5p. Am. J. Physiol. Gastrointest. Liver Physiol. 2019. [Google Scholar] [CrossRef]
- Miao, Y.; Sui, J.; Xu, S.Y.; Liang, G.Y.; Pu, Y.P.; Yin, L.H. Comprehensive analysis of a novel four-lncRNA signature as a prognostic biomarker for human gastric cancer. Oncotarget 2017. [Google Scholar] [CrossRef]
- Zibo, W.; Jibin, L.; Hongyan, Z. Expression and significance of long chain non-coding RNA LINC01018 in non-small cell lung cancer. J. Mod. Oncol. 2017. [Google Scholar] [CrossRef]
- Teschendorff, A.E.; Lee, S.H.; Jones, A. HOTAIR and its surrogate DNA methylation signature indicate carboplatin resistance in ovarian cancer. Genome Med. 2015. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ye, C.; Liu, J.; Hu, Y. UCA1 confers paclitaxel resistance to ovarian cancer through miR-129/ABCB1 axis. Biochem. Biophys. Res. Commun. 2018. [Google Scholar] [CrossRef] [PubMed]
- Reyes, H.D.; Devor, E.J.; Warrier, A. Differential DNA methylation in high-grade serous ovarian cancer (HGSOC) is associated with tumor behavior. Sci. Rep. 2019. [Google Scholar] [CrossRef]
- Newtson, A.M.; Devor, E.J.; Gonzalez Bosquet, J. Prediction of Epithelial Ovarian Cancer Outcomes with Integration of Genomic Data. Clin. Obstet. Gynecol. 2020. [Google Scholar] [CrossRef]
- Schroeder, A.; Mueller, O.; Stocker, S. The RIN: An RNA integrity number for assigning integrity values to RNA measurements. BMC Mol. Biol. 2006. [Google Scholar] [CrossRef]
- Kim, D.; Langmead, B.; Salzberg, S.L. HISAT: A fast spliced aligner with low memory requirements. Nat. Methods 2015. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HGSC Patients | p-Value | |||
|---|---|---|---|---|
| N = 103 | ||||
| Age | (Mean) | 59.8 | 0.002 * | |
| Charlson Comorbidity Index | 1–3 | 18 | 0.004 * | |
| 4–6 | 64 | |||
| >6 | 16 | |||
| FIGO Stage | 2 | 3 | 0.995 | |
| 3 | 68 | |||
| 4 | 25 | |||
| Disease in Upper abdomen (Other than Omentum) by Imaging | Yes | Large Bowel (N = 4) | 63 | 0.089 |
| Porta—Hepatis (N = 5) | ||||
| Mesenteric Mets (N = 4) | ||||
| Other (N = 26) | ||||
| No | 40 | |||
| Disease in the Chest by Imaging | Yes | Chest (N = 5) | 7 | 0.936 |
| Pleural effusion (N = 5) | ||||
| No | 96 | |||
| Grade | 2 | 21 | 0.555 | |
| 3 | 67 | |||
| Residual disease after surgery | Microscopic | 20 | 0.008 * | |
| Macroscopic | 82 | |||
| Optimal (<1 cm) | 64 | 0.105 | ||
| Suboptimal (>1 cm) | 36 | |||
| Removal of Pelvic LN | Yes | 17 | 0.089 | |
| No | 86 | |||
| Removal of Para-Aortic LN | Yes | 10 | 0.144 | |
| No | 93 | |||
| Surgical complexity score | Low | 52 | 0.789 | |
| Intermediate | 47 | |||
| High | 4 | |||
| Neoadjuvant Chemotherapy | Yes | 13 | <0.001 * | |
| No | 88 | |||
| Number of Cycles delivered | <6 | 1 | 0.194 | |
| ≥6 | 42 | |||
| Dose Dense Chemotherapy | Yes | 3 | 0.354 | |
| Response to Chemotherapy | Yes | 50 | <0.001 * | |
| No | 38 | |||
| HR | p-Value | 95% CI | |
|---|---|---|---|
| Multivariate model with clinical data | |||
| Charlson Index | 1.19 | 0.009 | 1.04, 1.36 |
| Response (non-responders) | 4.17 | <0.001 | 2.50, 6.96 |
| Multivariate model with lncRNA | |||
| AC079035.1 | 0.63 | <0.001 | 0.50, 0.79 |
| LINC00399 | 2.42 | <0.001 | 1.49, 3.94 |
| AL139021.1 | 1.49 | 0.020 | 1.06, 2.08 |
| AC002115.1 | 2.91 | <0.001 | 1.89, 4.49 |
| Responders | Non-Responders | p-Value | |||
|---|---|---|---|---|---|
| N = 50 | N = 38 | ||||
| Age | 56 | 64 | 0.009 * | ||
| Charlson Comorbidity Index | 1–3 | 9 | 4 | 0.068 * | |
| 4–6 | 35 | 21 | |||
| >6 | 1 | 6 | |||
| FIGO Stage | 3 | 39 | 25 | 0.069 | |
| 4 | 7 | 12 | |||
| Disease in Upper abdomen (Other than Omentum) by Imaging | Yes | Large Bowel (N = 4) | 28 | 29 | 0.051 |
| Porta—Hepatis (N = 4) | |||||
| Mesenteric Mets (N = 3) | |||||
| Other (N = 22) | |||||
| No | 22 | 9 | |||
| Disease in the Chest by Imaging | Yes | Chest (N = 4) | 6 | 0 | 0.992 |
| Pleural effusion (N = 5) | |||||
| No | 44 | 38 | |||
| Grade | 2 | 8 | 11 | 0.875 | |
| 3 | 35 | 23 | |||
| Residual disease after surgery | Microscopic | 12 | 3 | 0.053 | |
| Macroscopic | 37 | 35 | |||
| Optimal (<1 cm) | 37 | 20 | 0.039 * | ||
| Suboptimal (>1 cm) | 13 | 18 | |||
| Removal of Pelvic LN | Yes | 9 | 4 | 0.333 | |
| No | 41 | 34 | |||
| Removal of Para-Aortic LN | Yes | 5 | 3 | 0.734 | |
| No | 45 | 35 | |||
| Surgical complexity score | Low | 22 | 23 | 0.990 | |
| Intermediate | 28 | 12 | |||
| High | 0 | 3 | |||
| Neoadjuvant Chemotherapy | Yes | 2 | 10 | 0.009 * | |
| No | 47 | 28 | |||
| Number of Cycles delivered | <6 | 2 | 8 | 0.344 | |
| ≥6 | 48 | 30 | |||
| Dose Dense Chemotherapy | Yes | 1 | 1 | 0.844 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardillo, N.; Russo, D.; Newtson, A.; Reyes, H.; Lyons, Y.; Devor, E.; Bender, D.; Goodheart, M.J.; Gonzalez-Bosquet, J. Identification of Novel lncRNAs in Ovarian Cancer and Their Impact on Overall Survival. Int. J. Mol. Sci. 2021, 22, 1079. https://doi.org/10.3390/ijms22031079
Cardillo N, Russo D, Newtson A, Reyes H, Lyons Y, Devor E, Bender D, Goodheart MJ, Gonzalez-Bosquet J. Identification of Novel lncRNAs in Ovarian Cancer and Their Impact on Overall Survival. International Journal of Molecular Sciences. 2021; 22(3):1079. https://doi.org/10.3390/ijms22031079
Chicago/Turabian StyleCardillo, Nicholas, Douglas Russo, Andreea Newtson, Henry Reyes, Yasmin Lyons, Eric Devor, David Bender, Michael J. Goodheart, and Jesus Gonzalez-Bosquet. 2021. "Identification of Novel lncRNAs in Ovarian Cancer and Their Impact on Overall Survival" International Journal of Molecular Sciences 22, no. 3: 1079. https://doi.org/10.3390/ijms22031079
APA StyleCardillo, N., Russo, D., Newtson, A., Reyes, H., Lyons, Y., Devor, E., Bender, D., Goodheart, M. J., & Gonzalez-Bosquet, J. (2021). Identification of Novel lncRNAs in Ovarian Cancer and Their Impact on Overall Survival. International Journal of Molecular Sciences, 22(3), 1079. https://doi.org/10.3390/ijms22031079