
Proteomic Studies of Blood and Vascular Wall in Atherosclerosis


.JPG)

Abstract
:1. Introduction
2. Results of Proteomic Blood Tests in Population Groups of Individuals and Non-Complicated Coronary Heart Disease
3. Results of Proteomic Blood Tests in Acute Coronary Syndrome and Myocardial Infarction
4. Results of Proteomic Blood Tests for Carotid Artery Atherosclerosis and Stroke
5. Results of Proteomic Studies of Atherosclerotic Plaques
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lebedev, A.T.; Artemenko, K.A.S.T. Fundamentals of Mass Spectrommetry of Proteins and Peptides; Tehnosfera: Moscow, Russia, 2012; ISBN 978-5-94836-334-9. (In Russian) [Google Scholar]
- Jayathirtha, M.; Dupree, E.J.; Manzoor, Z.; Larose, B.; Sechrist, Z.; Neagu, A.-N.; Petre, B.A.; Darie, C.C. Mass Spectrometric (MS) Analysis of Proteins and Peptides. Curr. Protein Pept. Sci. 2021, 22, 92–120. [Google Scholar] [CrossRef] [PubMed]
- Addona, T.A.; Abbatiello, S.E.; Schilling, B.; Skates, S.J.; Mani, D.R.; Bunk, D.M.; Spiegelman, C.H.; Zimmerman, L.J.; Ham, A.J.L.; Keshishian, H.; et al. Multi-site assessment of the precision and reproducibility of multiple reaction monitoring-based measurements of proteins in plasma. Nat. Biotechnol. 2009, 27, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Xia, J.Q.; Sedransk, N.; Feng, X. Variance component analysis of a multi-site study for the reproducibility of multiple reaction monitoring measurements of peptides in human plasma. PLoS ONE 2011, 6, e14590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [Green Version]
- Tereshchenko, S.N.; Galyavich, A.S.; Uskach, T.M.; Ageev, F.T.; Arutyunov, G.P.; Begrambekova, Y.L.; Belenkov, Y.N.; Boytsov, S.A.; Vasyuk, Y.A.; Garganeeva, A.A.; et al. 2020 Clinical practice guidelines for Chronic heart failure. Russ. J. Cardiol. 2020, 25, 311–374. [Google Scholar] [CrossRef]
- Magnussen, C.; Blankenberg, S. Biomarkers for heart failure: Small molecules with high clinical relevance. J. Intern. Med. 2018, 283, 530–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thul, P.J.; Akesson, L.; Wiking, M.; Mahdessian, D.; Geladaki, A.; Ait Blal, H.; Alm, T.; Asplund, A.; Björk, L.; Breckels, L.M.; et al. A subcellular map of the human proteome. Science 2017, 356, eeal3321. [Google Scholar] [CrossRef] [PubMed]
- Corbacho-Alonso, N.; Baldán-Martín, M.; López, J.A.; Rodríguez Sánchez, E.; Martínez, P.J.; Mourino-Alvarez, L.; Martin-Rojas, T.; Sastre-Oliva, T.; Madruga, F.; Vázquez, J.; et al. Novel molecular plasma signatures on cardiovascular disease can stratify patients throughout life. J. Proteomics 2020, 222, 103816. [Google Scholar] [CrossRef]
- Corlin, L.; Lin, H.; Leone, D.; Yang, Q.; Ngo, D.; Levy, D.; Adrienne Cupples, L.; Gerszten, R.E.; Larson, M.G.; Vasan, R.S. Proteomic signatures of lifestyle risk factors for cardiovascular disease: A cross-sectional analysis of the plasma proteome in the framingham heart study. J. Am. Heart Assoc. 2021, 10, e018020. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.; Heidecker, B.; Hveem, K.; Jonasson, C.; Kato, S.; Segal, M.R.; Sterling, D.G.; Williams, S.A. Development and validation of a protein-based risk score for cardiovascular outcomes among patients with stable coronary heart disease. JAMA 2016, 315, 2532–2541. [Google Scholar] [CrossRef] [PubMed]
- Jorge, I.; Burillo, E.; Mesa, R.; Baila-Rueda, L.; Moreno, M.; Trevisan-Herraz, M.; Silla-Castro, J.C.; Camafeita, E.; Ortega-Muñoz, M.; Bonzon-Kulichenko, E.; et al. The human HDL proteome displays high inter-individual variability and is altered dynamically in response to angioplasty-induced atheroma plaque rupture. J. Proteomics 2014, 106, 61–73. [Google Scholar] [CrossRef]
- Wang, G.; Mathew, A.V.; Yu, H.; Li, L.; He, L.; Gao, W.; Liu, X.; Guo, Y.; Byun, J.; Zhang, J.; et al. Myeloperoxidase mediated HDL oxidation and HDL proteome changes do not contribute to dysfunctional HDL in Chinese subjects with coronary artery disease. PLoS ONE 2018, 13, e0193782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexandar, V.; Nayar, P.G.; Murugesan, R.; Shajahan, S.; Krishnan, J.; Ahmed, S.S.S.J. A systems biology and proteomics-based approach identifies: SRC and VEGFA as biomarkers in risk factor mediated coronary heart disease. Mol. Biosyst. 2016, 12, 2594–2604. [Google Scholar] [CrossRef]
- Krishnan, S.; Huang, J.; Lee, H.; Guerrero, A.; Berglund, L.; Anuurad, E.; Lebrilla, C.B.; Zivkovic, A.M. Combined High-Density Lipoprotein Proteomic and Glycomic Profiles in Patients at Risk for Coronary Artery Disease. J. Proteome Res. 2015, 14, 5109–5118. [Google Scholar] [CrossRef] [PubMed]
- Cao, D.J.; Hill, J.A. Copper futures: Ceruloplasmin and heart failure. Circ. Res. 2014, 114, 1678–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabassi, A.; Binno, S.M.; Tedeschi, S.; Ruzicka, V.; Dancelli, S.; Rocco, R.; Vicini, V.; Coghi, P.; Regolisti, G.; Montanari, A.; et al. Low serum ferroxidase i activity is associated with mortality in heart failure and related to both peroxynitrite-induced cysteine oxidation and tyrosine nitration of ceruloplasmin. Circ. Res. 2014, 114, 1723–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stakhneva, E.M.; Meshcheryakova, I.A.; Demidov, E.A.; Starostin, K.V.; Peltek, S.E.; Voevoda, M.I.; Ragino, Y.I. Changes in the proteomic profile of blood serum in coronary atherosclerosis. J. Med. Biochem. 2019, 39, 208. [Google Scholar] [CrossRef]
- Dadu, R.T.; Dodge, R.; Nambi, V.; Virani, S.S.; Hoogeveen, R.C.; Smith, N.L.; Chen, F.; Pankow, J.S.; Guild, C.; Tang, W.H.W.; et al. Ceruloplasmin and heart failure in the atherosclerosis risk in communities study. Circ. Heart Fail. 2013, 6, 936–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arenas de Larriva, A.P.; Norby, F.L.; Chen, L.Y.; Soliman, E.Z.; Hoogeveen, R.C.; Arking, D.E.; Loehr, L.R.; Alonso, A. Circulating ceruloplasmin, ceruloplasmin-associated genes, and the incidence of atrial fibrillation in the atherosclerosis risk in communities study. Int. J. Cardiol. 2017, 241, 223–228. [Google Scholar] [CrossRef]
- YuN, O.; Perelmuter, V.M. Biological functions of complement. Bull. Sib. Med. 2007, 26, 72–82. (In Russian) [Google Scholar] [CrossRef]
- Patzelt, J.; Verschoor, A.; Langer, H.F. Platelets and the complement cascade in atherosclerosis. Front. Physiol. 2015, 6, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, A.M. Complement Activation: An Emerging Player in the Pathogenesis of Cardiovascular Disease. Scientifica 2012, 2012, 402783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasojima, K.; Schwab, C.; McGeer, E.G.; McGeer, P.L. Generation of C-reactive protein and complement components in atherosclerotic plaques. Am. J. Pathol. 2001, 158, 1039–1051. [Google Scholar] [CrossRef] [Green Version]
- Lepedda, A.J.; Lobina, O.; Rocchiccioli, S.; Nieddu, G.; Ucciferri, N.; De Muro, P.; Idini, M.; Nguyen, H.Q.T.; Guarino, A.; Spirito, R.; et al. Identification of differentially expressed plasma proteins in atherosclerotic patients with type 2 diabetes. J. Diabetes Complicat. 2016, 30, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Shan, L.X.; Pang, L.; Zhang, R.; Murgolo, N.J.; Lan, H.; Hedrick, J.A. PCSK9 binds to multiple receptors and can be functionally inhibited by an EGF-A peptide. Biochem. Biophys. Res. Commun. 2008, 375, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, J.; Janiec, M.; Bergdahl, I.A.; Holmgren, A.; Hultdin, J.; Johansson, B.; Näslund, U.; Siegbahn, A.; Fall, T.; Söderberg, S. Proteomic biomarkers for incident aortic stenosis requiring valvular replacement. Circulation 2018, 138, 590–599. [Google Scholar] [CrossRef]
- Langley, S.R.; Willeit, K.; Didangelos, A.; Matic, L.P.; Skroblin, P.; Barallobre-Barreiro, J.; Lengquist, M.; Rungger, G.; Kapustin, A.; Kedenko, L.; et al. Extracellular matrix proteomics identifies molecular signature of symptomatic carotid plaques. J. Clin. Investig. 2017, 127, 1546–1560. [Google Scholar] [CrossRef]
- Lind, L.; Ärnlöv, J.; Lindahl, B.; Siegbahn, A.; Sundström, J.; Ingelsson, E. Use of a proximity extension assay proteomics chip to discover new biomarkers for human atherosclerosis. Atherosclerosis 2015, 242, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Poss, A.M.; Maschek, J.A.; Cox, J.E.; Hauner, B.J.; Hopkins, P.N.; Hunt, S.C.; Holland, W.L.; Summers, S.A.; Playdon, M.C. Machine learning reveals serum sphingolipids as cholesterol-independent biomarkers of coronary artery disease. J. Clin. Investig. 2020, 130, 1363–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrannini, G.; Manca, M.L.; Magnoni, M.; Andreotti, F.; Andreini, D.; Latini, R.; Maseri, A.; Maggioni, A.P.; Ostroff, R.M.; Williams, S.A.; et al. Coronary artery disease and type 2 diabetes: A proteomic study. Diabetes Care 2020, 43, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Kharb, R.; Sharma, A.; Chaddar, M.K.; Yadav, R.; Agnihotri, P.; Kar, A.; Biswas, S. Plasma proteome profiling of coronary artery disease patients: Downregulation of transthyretin—An important event. Mediat. Inflamm. 2020, 2020, 3429541. [Google Scholar] [CrossRef]
- Ku, E.J.; Cho, K.C.; Lim, C.; Kang, J.W.; Oh, J.W.; Choi, Y.R.; Park, J.M.; Han, N.Y.; Oh, J.J.; Oh, T.J.; et al. Discovery of plasma biomarkers for predicting the severity of coronary artery atherosclerosis by quantitative proteomics. BMJ Open Diabetes Res. Care 2020, 8, e001152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nukala, S.B.; Regazzoni, L.; Aldini, G.; Zodda, E.; Tura-Ceide, O.; Mills, N.L.; Cascante, M.; Carini, M.; D’Amato, A. Differentially Expressed Proteins in Primary Endothelial Cells Derived from Patients with Acute Myocardial Infarction. Hypertension 2019, 74, 947–956. [Google Scholar] [CrossRef] [PubMed]
- de Hoog, V.C.; Timmers, L.; Schoneveld, A.H.; Wang, J.W.; Van de Weg, S.M.; Sze, S.K.; Van Keulen, J.K.; Hoes, A.W.; Den Ruijter, H.M.; de Kleijn, D.P.; et al. Serum extracellular vesicle protein levels are associated with acute coronary syndrome. Eur. Heart J. Acute Cardiovasc. Care 2013, 2, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Yin, X.; Subramanian, S.; Hwang, S.J.; O’Donnell, C.J.; Fox, C.S.; Courchesne, P.; Muntendam, P.; Gordon, N.; Adourian, A.; Juhasz, P.; et al. Protein biomarkers of new-onset cardiovascular disease: Prospective study from the systems approach to biomarker research in cardiovascular disease initiative. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 939–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, B.; Serchi, T.; Wagner, D.R.; Gilson, G.; Planchon, S.; Renaut, J.; Hoffmann, L.; Bohn, T.; Devaux, Y. Proteomic analysis of plasma samples from patients with acute myocardial infarction identifies haptoglobin as a potential prognostic biomarker. J. Proteomics 2011, 75, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Bakrim, N.; Mohd Shah, A.N.S.; Talib, N.A.; Ab Rahman, J.; Abdullah, A. Identification of haptoglobin as a potential biomarker in young adults with acute myocardial infarction by proteomic analysis. Malays. J. Med. Sci. 2020, 27, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Raizada, A.; Bhandari, S.; Khan, M.A.; Singh, H.V.; Thomas, S.; Sarabhai, V.; Singh, N.; Trehan, N. Brain type natriuretic peptide (BNP)—A marker of new millennium in diagnosis of congestive heart failure. Indian J. Clin. Biochem. 2007, 22, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Li, Z.; Gao, W. Growth differentiation factor 15 in cardiovascular diseases: From bench to bedside. Biomarkers 2011, 16, 466–475. [Google Scholar] [CrossRef]
- Chan, M.Y.; Efthymios, M.; Tan, S.H.; Pickering, J.W.; Troughton, R.; Pemberton, C.; Ho, H.H.; Prabath, J.F.; Drum, C.L.; Ling, L.H.; et al. Prioritizing Candidates of Post-Myocardial Infarction Heart Failure Using Plasma Proteomics and Single-Cell Transcriptomics. Circulation 2020, 142, 1408–1421. [Google Scholar] [CrossRef] [PubMed]
- Schiopu, A.; Cotoi, O.S. S100A8 and S100A9: DAMPs at the crossroads between innate immunity, traditional risk factors, and cardiovascular disease. Mediat. Inflamm. 2013, 2013, 828354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navas-Carrillo, D.; Marín, F.; Valdés, M.; Orenes-Piñero, E. Deciphering acute coronary syndrome biomarkers: High-resolution proteomics in platelets, thrombi and microparticles. Crit. Rev. Clin. Lab. Sci. 2017, 54, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Basak, T.; Varshney, S.; Akhtar, S.; Sengupta, S. Understanding different facets of cardiovascular diseases based on model systems to human studies: A proteomic and metabolomic perspective. J. Proteomics 2015, 127, 50–60. [Google Scholar] [CrossRef]
- Vélez, P.; Ocaranza-Sánchez, R.; López-Otero, D.; Grigorian-Shamagian, L.; Rosa, I.; Bravo, S.B.; González-Juanatey, J.R.; García, Á. 2D-DIGE-based proteomic analysis of intracoronary versus peripheral arterial blood platelets from acute myocardial infarction patients: Upregulation of platelet activation biomarkers at the culprit site. Proteomics–Clin. Appl. 2016, 10, 851–858. [Google Scholar] [CrossRef]
- Maguire, P.B.; Parsons, M.E.; Szklanna, P.B.; Zdanyte, M.; Münzer, P.; Chatterjee, M.; Wynne, K.; Rath, D.; Comer, S.P.; Hayden, M.; et al. Comparative Platelet Releasate Proteomic Profiling of Acute Coronary Syndrome versus Stable Coronary Artery Disease. Front. Cardiovasc. Med. 2020, 7, 101. [Google Scholar] [CrossRef]
- Shin, M.; Park, S.H.; Mun, S.; Lee, J.; Kang, H.G. Biomarker discovery of acute coronary syndrome using proteomic approach. Molecules 2021, 26, 1136. [Google Scholar] [CrossRef] [PubMed]
- Das, A.A.; Choudhury, K.R.; Jagadeeshaprasad, M.G.; Kulkarni, M.J.; Mondal, P.C.; Bandyopadhyay, A. Proteomic analysis detects deregulated reverse cholesterol transport in human subjects with ST-segment elevation myocardial infarction. J. Proteomics 2020, 222, 103796. [Google Scholar] [CrossRef]
- Zou, L.; Wang, X.; Guo, Z.; Sun, H.; Shao, C.; Yang, Y.; Sun, W. Differential urinary proteomics analysis of myocardial infarction using iTRAQ quantification. Mol. Med. Rep. 2019, 49, 3972–3988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nehme, A.; Kobeissy, F.; Zhao, J.; Zhu, R.; Feugier, P.; Mechref, Y.; Zibara, K. Functional pathways associated with human carotid atheroma: A proteomics analysis. Hypertens. Res. 2019, 42, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Sentman, M.L.; Granström, M.; Jakobson, H.; Reaume, A.; Basu, S.; Marklund, S.L. Phenotypes of mice lacking extracellular superoxide dismutase and copper- and zinc-containing superoxide dismutase. J. Biol. Chem. 2006, 281, 6904–6909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, N.M.; Capri, J.; Cohn, W.; Abdaljaleel, M.; Restrepo, L.; Gornbein, J.A.; Yong, W.H.; Liebeskind, D.S.; Whitelegge, J.P. Peptide composition of stroke causing emboli correlate with serum Markers of atherosclerosis and inflammation. Front. Neurol. 2017, 8, 427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lepedda, A.J.; Nieddu, G.; Zinellu, E.; De Muro, P.; Piredda, F.; Guarino, A.; Spirito, R.; Carta, F.; Turrini, F.; Formato, M. Proteomic analysis of plasma-purified VLDL, LDL, and HDL fractions from atherosclerotic patients undergoing carotid endarterectomy: Identification of serum amyloid a as a potential marker. Oxid. Med. Cell. Longev. 2013, 2013, 385214. [Google Scholar] [CrossRef] [PubMed]
- Brea, D.; Rodríguez-González, R.; Sobrino, T.; Rodríguez-Yañez, M.; Blanco, M.; Castillo, J. Proteomic analysis shows differential protein expression in endothelial progenitor cells between healthy subjects and ischemic stroke patients. Neurol. Res. 2011, 33, 1057–1063. [Google Scholar] [CrossRef]
- Qin, C.; Zhao, X.L.; Ma, X.T.; Zhou, L.Q.; Wu, L.J.; Shang, K.; Wang, W.; Tian, D.S. Proteomic profiling of plasma biomarkers in acute ischemic stroke due to large vessel occlusion. J. Transl. Med. 2019, 17, 214. [Google Scholar] [CrossRef] [PubMed]
- Cevik, O.; Baykal, A.T.; Sener, A. Platelets proteomic profiles of acute ischemic stroke patients. PLoS ONE 2016, 11, e0158287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagnato, C.; Thumar, J.; Mayya, V.; Hwang, S.I.; Zebroski, H.; Claffey, K.P.; Haudenschild, C.; Eng, J.K.; Lundgren, D.H.; Han, D.K. Proteomics analysis of human coronary atherosclerotic plaque: A feasibility study of direct tissue proteomics by liquid chromatography and tandem mass spectrometry. Mol. Cell. Proteomics 2007, 6, 1088–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Yuan, J.; Fan, Y.; An, F.; Chen, J.; Zhang, Y.; Jin, J.; Gu, M.; Mao, Z.; Sun, H.; et al. Proteomic landscape of human coronary artery atherosclerosis. Int. J. Mol. Med. 2020, 46, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Mancio, J.; Barros, A.S.; Conceicao, G.; Pessoa-Amorim, G.; Santa, C.; Bartosch, C.; Ferreira, W.; Carvalho, M.; Ferreira, N.; Vouga, L.; et al. Epicardial adipose tissue volume and annexin A2/fetuin-A signalling are linked to coronary calcification in advanced coronary artery disease: Computed tomography and proteomic biomarkers from the EPICHEART study. Atherosclerosis 2020, 292, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xi, D.; Luo, T.; Xiong, H.; Liu, J.; Lu, H.; Li, M.; Hou, Y.; Guo, Z. SAP: Structure, function, and its roles in immune-related diseases. Int. J. Cardiol. 2015, 187, 20–26. [Google Scholar] [CrossRef]
- Xi, D.; Zhao, J.; Guo, K.; Hu, L.; Chen, H.; Fu, W.; Lai, W.; Guo, Z. Serum amyloid P component therapeutically attenuates atherosclerosis in mice via its effects on macrophages. Theranostics 2018, 8, 3214–3223. [Google Scholar] [CrossRef]
- Malaud, E.; Merle, D.; Piquer, D.; Molina, L.; Salvetat, N.; Rubrecht, L.; Dupaty, E.; Galea, P.; Cobo, S.; Blanc, A.; et al. Local carotid atherosclerotic plaque proteins for the identification of circulating biomarkers in coronary patients. Atherosclerosis 2014, 233, 551–558. [Google Scholar] [CrossRef]
- Stöhr, R.; Schurgers, L.; Van Gorp, R.; Jaminon, A.; Marx, N.; Reutelingsperger, C. Annexin A5 reduces early plaque formation in ApoE−/− mice. PLoS ONE 2017, 12, e0190229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, R.; Fischer, R.; Charles, P.D.; Adlam, D.; Valli, A.; Di Gleria, K.; Kharbanda, R.K.; Choudhury, R.P.; Antoniades, C.; Kessler, B.M.; et al. A novel workflow combining plaque imaging, plaque and plasma proteomics identifies biomarkers of human coronary atherosclerotic plaque disruption. Clin. Proteomics 2017, 14, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stakhneva, E.M.; Meshcheryakova, I.A.; Demidov, E.A.; Starostin, K.V.; Sadovski, E.V.; Peltek, S.E.; Voevoda, M.I.; Chernyavskii, A.M.; Volkov, A.M.; Ragino, Y.I. A proteomic study of atherosclerotic plaques in men with coronary atherosclerosis. Diagnostics 2019, 9, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrington, D.M.; Mao, C.; Parker, S.J.; Fu, Z.; Yu, G.; Chen, L.; Venkatraman, V.; Fu, Y.; Wang, Y.; Howard, T.D.; et al. Proteomic Architecture of Human Coronary and Aortic Atherosclerosis. Circulation 2018, 137, 2741–2756. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhao, S.; Gong, Y.; Hou, G.; Li, X.; Li, L. Serum cyclin-dependent kinase 9 is a potential biomarker of atherosclerotic inflammation. Oncotarget 2016, 7, 1854–1862. [Google Scholar] [CrossRef] [PubMed]
- Lepedda, A.J.; Cigliano, A.; Cherchi, G.M.; Spirito, R.; Maggioni, M.; Carta, F.; Turrini, F.; Edelstein, C.; Scanu, A.M.; Formato, M. A proteomic approach to differentiate histologically classified stable and unstable plaques from human carotid arteries. Atherosclerosis 2009, 203, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Olson, F.J.; Sihlbom, C.; Davidsson, P.; Hulthe, J.; Fagerberg, B.; Bergström, G. Consistent differences in protein distribution along the longitudinal axis in symptomatic carotid atherosclerotic plaques. Biochem. Biophys. Res. Commun. 2010, 401, 574–580. [Google Scholar] [CrossRef]
- Rocchiccioli, S.; Pelosi, G.; Rosini, S.; Marconi, M.; Viglione, F.; Citti, L.; Ferrari, M.; Trivella, M.G.; Cecchettini, A. Secreted proteins from carotid endarterectomy: An untargeted approach to disclose molecular clues of plaque progression. J. Transl. Med. 2013, 11, 260. [Google Scholar] [CrossRef] [Green Version]
- Fasehee, H.; Fakhraee, M.; Davoudi, S.; Vali, H.; Faghihi, S. Cancer biomarkers in atherosclerotic plaque: Evidenced from structural and proteomic analyses. Biochem. Biophys. Res. Commun. 2019, 509, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Seki, T.; Saita, E.; Kishimoto, Y.; Ibe, S.; Miyazaki, Y.; Miura, K.; Ohmori, R.; Ikegami, Y.; Kondo, K.; Momiyama, Y. Low levels of plasma osteoglycin in patients with complex coronary lesions. J. Atheroscler. Thromb. 2018, 25, 1149–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.M.; Akkerhuis, K.M.; Meilhac, O.; Oemrawsingh, R.M.; Garcia-Garcia, H.M.; Van Geuns, R.J.; Piquer, D.; Merle, D.; Du Paty, E.; Galéa, P.; et al. Circulating osteoglycin and NGAL/MMP9 complex concentrations predict 1-year major adverse cardiovascular events after coronary angiography. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1078–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chistiakov, D.A.; Orekhov, A.N.; Bobryshev, Y.V. Endothelial barrier and its abnormalities in cardiovascular disease. Front. Physiol. 2015, 6, 365. [Google Scholar] [CrossRef]
- Stintzing, S.; Ocker, M.; Hartner, A.; Amann, K.; Barbera, L.; Neureiter, D. Differentiation patterning of vascular smooth muscle cells (VSMC) in atherosclerosis. Virchows Arch. 2009, 455, 171–185. [Google Scholar] [CrossRef] [PubMed]
- Tu, Z.L.; Yu, B.; Huang, D.Y.; Ojha, R.; Zhou, S.K.; An, H.D.; Liu, R.; Du, C.; Shen, N.; Fu, J.H.; et al. Proteomic analysis and comparison of intra- and extracranial cerebral atherosclerosis responses to hyperlipidemia in rabbits. Mol. Med. Rep. 2017, 16, 2347–2354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matyushenko, A.M.; Koubassova, N.A.; Shchepkin, D.V.; Kopylova, G.V.; Nabiev, S.R.; Nikitina, L.V.; Bershitsky, S.Y.; Levitsky, D.I.; Tsaturyan, A.K. The effects of cardiomyopathy-associated mutations in the head-to-tail overlap junction of α-tropomyosin on its properties and interaction with actin. Int. J. Biol. Macromol. 2019, 125, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Dirajlal-Fargo, S.; Kulkarni, M.; Bowman, E.; Shan, L.; Sattar, A.; Funderburg, N.; McComsey, G.A. Serum albumin is associated with higher inflammation and carotid atherosclerosis in treated human immunodeficiency virus infection. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2018; Volume 5. [Google Scholar] [CrossRef]

{kind=link}
| Proteomic Biomolecules | References | |
|---|---|---|
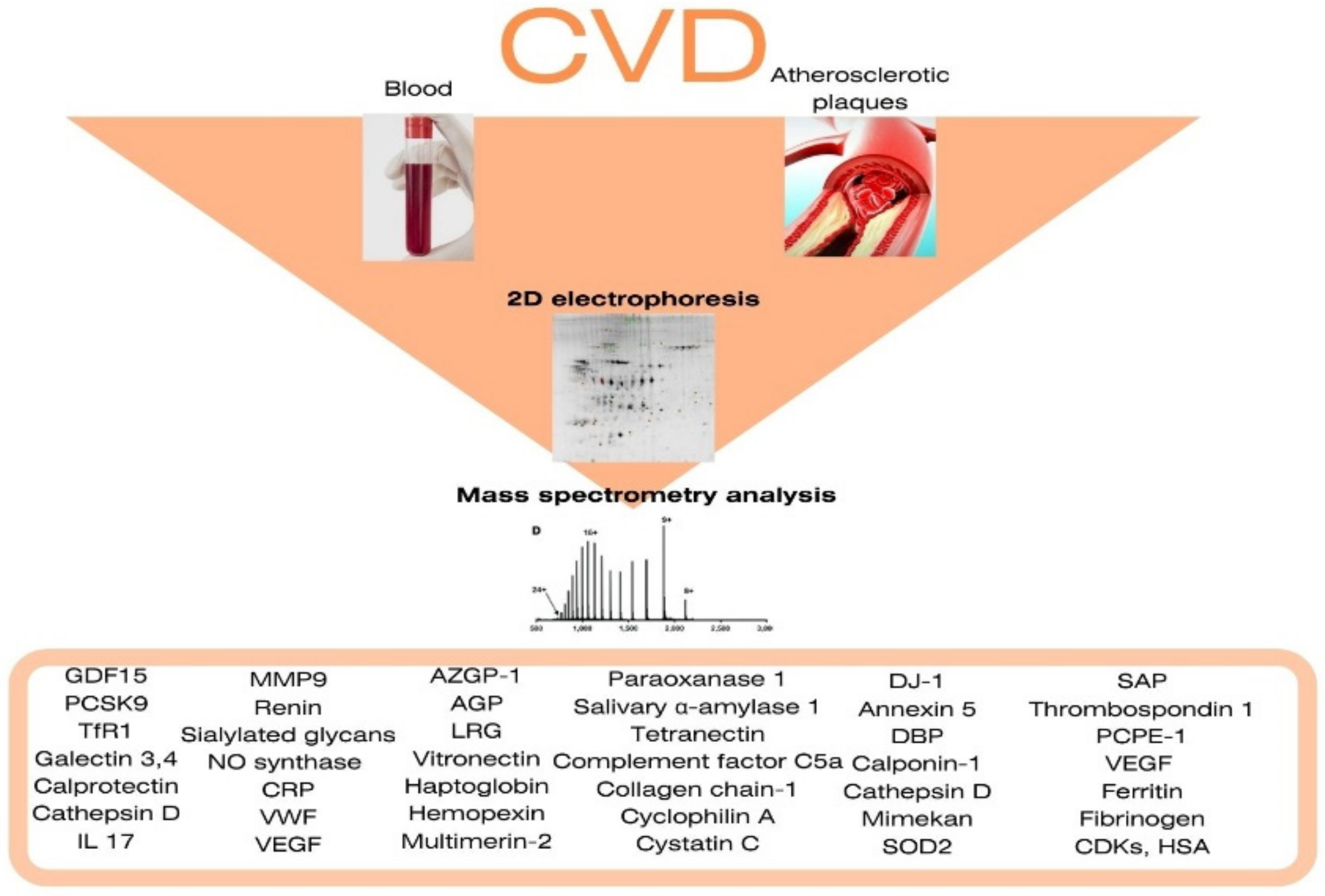
| Elevated blood levels in patients with coronary atherosclerosis and coronary heart disease | Growth differentiation factor 15 Proprotein convertase of subtilisin-kexin type 9 Transferrin receptor protein 1 Galectin-3 Galectin-4 Interleukin 17 Calprotectin Cathepsin D Complement components C3 (Chain B), C4, C9 Matrix metalloproteinase 9 Renin Sialylated glycans NO synthase C-reactive protein the Willebrand factor vascular endothelial growth factor | Alexandar, V. et al. [14] Krishnan, S. et al. [15] Stakhneva, E.M. et al. [18] Ljungberg, J. et al. [27] Langley, S.R. et al. [28] Ferrannini, G. et al. [31] |
| Elevated in the blood in patients with in ACS and MI | Zinc-alpha-2-glycoprotein Cluster of differentiation 5 α-1-acid glycoprotein 1 Antigen-like differentiation cluster 5 (CD5) Leucine-rich alpha-2 glycoprotein Vitronectin Haptoglobin Hemopexin Growth differentiation factor 15 Calprotectin Cell-surface glycoprotein mucin cell surface-associated protein 18 Multimerin-2 Paraoxanase 1 Polygenic immunoglobulin receptor Salivary α-amylase 1 Tetranectin Complement factor C5a Collagen chain-1 Cyclophilin A Cystatin C | de Hoog, V.C. et al. [35] Yin, X. et al. [36] Mohamed Bakrim, N. et al. [38] Xu, X. et al. [40] Schiopu, A. et al. [42] Shin M. et al. [47] Das A. A. et al. [48] |
| Elevated in the blood in patients with carotid artery atherosclerosis and stroke | Crk-like protein S100A8/S100A9 Apolipoprotein AI Apolipoprotein H Arachidonate-12-lipoxygenase Vitronectin Galectin-3-binding protein Histidine-rich glycoprotein Glucose-6-phosphate dehydrogenase Growth hormone Growth differentiation factor 15 Insulin-like growth factor 2 Integrin alpha-M Cathepsin D Clusterin Complement component C3 Matrix metalloproteinase 9 Matrix metalloproteinase 12 Myeloperoxidase Mitochondrial superoxide dismutase 2 Pro-platelet basic protein Osteoprotegerin Peroxiredoxin-1 Renin Lymphatic vessel endothelial hyaluronic acid receptor 1 Septin 2 Serum Amyloid A (SAA) T-cell immunoglobulin and mucin domain 1 Thrombospondin 1 Elongation factor-2 Phosphoglycerate kinase 1 member of the tumour necrosis factor superfamily 14 | Langley, S.R. et al. [28] Lind L. et al. [29] Rao, N.M. et al. [52] Lepedda A. J. et al. [53] Brea D.et al. [54] Qin C. et al. [55] Cevik O. et al. [56] |
| Elevated in unstable atherosclerotic plaques | Protein Deglycase DJ-1 Annexin 5 Vitamin D binding protein Calponin-1 Cathepsin D Mimekan Superoxide dismutase 2 Serum Amyloid P-component Thrombospondin 1 Procollagen C-proteinase enhancer-1 Vascular endothelial Growth Factor Ferritin Fibrinogen Cyclin-dependent kinases Human Serum Albumin | Malaud E. et al. [62] Stöhr R. et al. [63] Lee R. et al. [64] Stakhneva E. M. et al. [65] Han Y. et al. [67] Lepedda A. J. et al. [68] Olson F.J. et al. [69] Rocchiccioli S. et al. [70] Fasehee H. et al. [71] Cheng J.M. et al. [73] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stakhneva, E.M.; Striukova, E.V.; Ragino, Y.I. Proteomic Studies of Blood and Vascular Wall in Atherosclerosis. Int. J. Mol. Sci. 2021, 22, 13267. https://doi.org/10.3390/ijms222413267
Stakhneva EM, Striukova EV, Ragino YI. Proteomic Studies of Blood and Vascular Wall in Atherosclerosis. International Journal of Molecular Sciences. 2021; 22(24):13267. https://doi.org/10.3390/ijms222413267
Chicago/Turabian StyleStakhneva, Ekaterina Mikhailovna, Evgeniia Vitalievna Striukova, and Yulia Igorevna Ragino. 2021. "Proteomic Studies of Blood and Vascular Wall in Atherosclerosis" International Journal of Molecular Sciences 22, no. 24: 13267. https://doi.org/10.3390/ijms222413267
APA StyleStakhneva, E. M., Striukova, E. V., & Ragino, Y. I. (2021). Proteomic Studies of Blood and Vascular Wall in Atherosclerosis. International Journal of Molecular Sciences, 22(24), 13267. https://doi.org/10.3390/ijms222413267