
The Emerging Role of Presepsin (P-SEP) in the Diagnosis of Sepsis in the Critically Ill Infant: A Literature Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
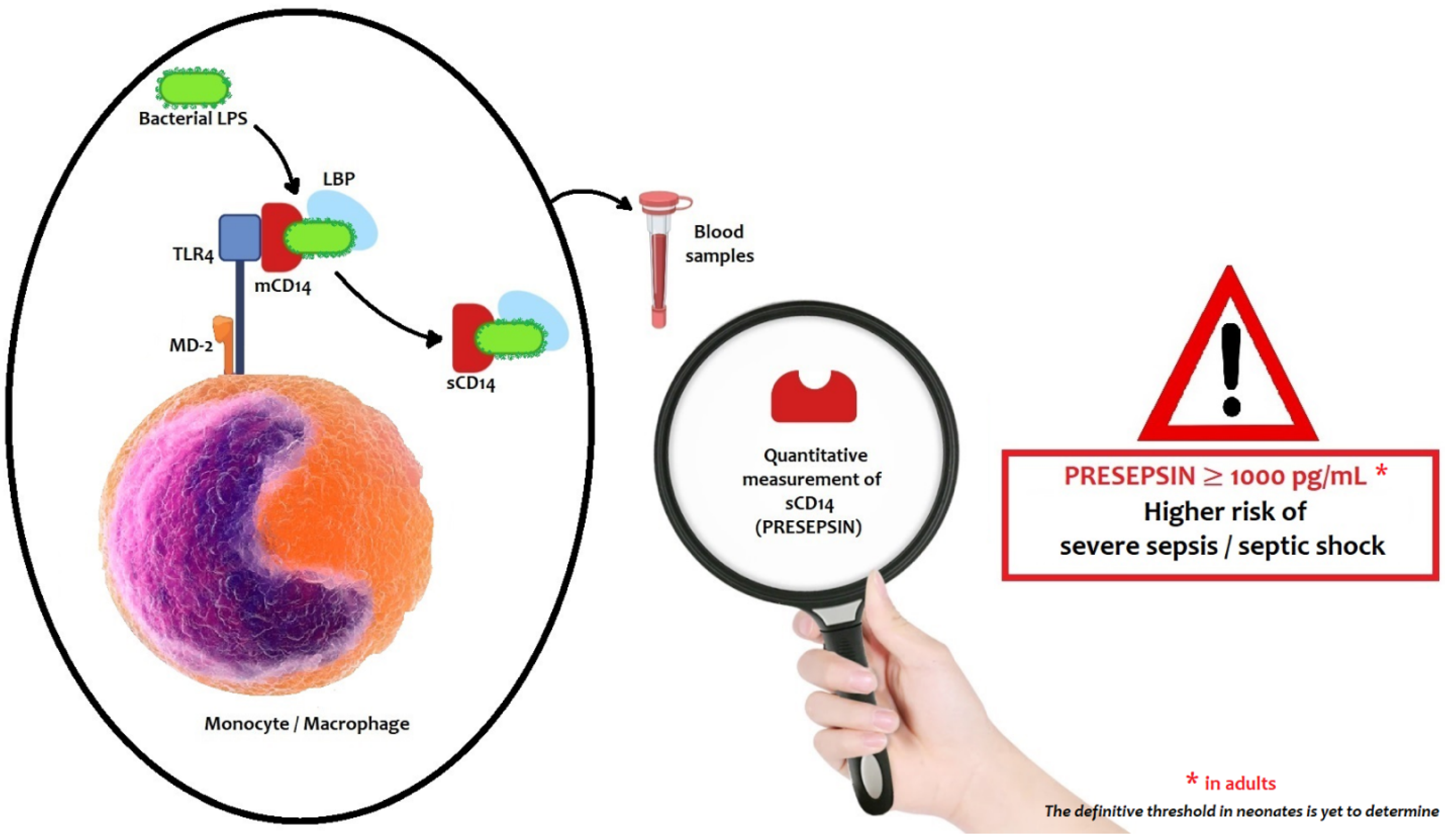
4. Biological Characteristics of Presepsin
5. Presepsin Plasmatic Levels and Renal Function
6. Methods to Measure Presepsin Plasma Levels
7. Accuracy of Presepsin in Detecting Sepsis in Adults and Children
- −
- Presepsin < 200 pg/mL—sepsis excluded;
- −
- Presepsin < 300 pg/mL—systemic infection improbable;
- −
- Presepsin < 500 pg/mL—sepsis probable;
- −
- Presepsin < 1000 pg/mL—significant risk of severe sepsis;
- −
- Presepsin ≥ 1000 pg/mL—high risk of severe sepsis/septic shock equivalent to a SOFA score ≥ 8.
8. Ranges of Reference Values in Neonates
9. Presepsin Compared to Other Immunologic Biomarkers
10. Presepsin for the Detection of Early-Onset and Late-Onset Sepsis
11. Prognostic Significance of Presepsin
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poggi, C.; Bianconi, T.; Gozzini, E.; Generoso, M.; Dani, C. Presepsin for the detection of late-onset sepsis in preterm newborns. Pediatrics 2015, 135, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Shah, B.A.; Padbury, J.F. Neonatal sepsis an old problem with new insights. Virulence 2014, 5, 170–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, J.Y.; Synnes, A.; Roberts, A.; Deshpandey, A.; Dow, K.; Yoon, E.W.; Lee, K.S.; Dobson, S.; Lee, S.K.; Shah, P.S.; et al. Association between antibiotic use and neonatal mortality and morbidities in very low-birth-weight infants without culture-proven sepsis or necrotizing enterocolitis. JAMA Pediatr. 2016, 170, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Poggi, C.; Vasarri, M.V.; Boni, L.; Pugni, L.; Mosca, F.; Dani, C. Reference ranges of Presepsin in preterm infants in the first 48 h of life: A multicenter observational study. Clin. Chim. Acta 2020, 508, 191–196. [Google Scholar] [CrossRef]
- Chiesa, C.; Natale, F.; Pascone, R.; Osborn, J.F.; Pacifico, L.; Bonci, E.; De Curtis, M.C. Reactive protein and procalcitonin: Refe-rence intervals for preterm and term newborns during the early neonatal period. Clin. Chim. Acta 2011, 412, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- De Rose, D.U.; Perri, A.; Auriti, C.; Gallini, F.; Maggio, L.; Fiori, B.; D’Inzeo, T.; Spanu, T.; Vento, G. Time to positivity of blood cultures could inform decisions on antibiotics administration in neonatal early-onset sepsis. Antibiotics 2021, 10, 123. [Google Scholar] [CrossRef]
- Esaiassen, E.; Fjalstad, J.W.; Juvet, L.K.; van den Anker, J.N.; Klingenberg, C. Antibiotic exposure in neonates and early adverse outcomes: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2017, 72, 1858–1870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, V.N.; Northrup, V.; Bizzarro, M.J. Antibiotic exposure in the newborn intensive care unit and the risk of necrotizing enterocolitis. J. Pediatr. 2011, 159, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, H.; Jia, X.; He, X.; Su, Y.; Zhou, L.; Shen, Y.; Sheng, C.; Liao, A.; Li, C.; Li, Q. Emerging Threat of Multidrug Resistant Pathogens from Neonatal Sepsis. Front. Cell. Infect. Microbiol. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Montaldo, P.; Rosso, R.; Santantonio, A.; Chello, G.; Giliberti, P. Presepsin for the detection of early-onset sepsis in preterm newborns. Pediatr. Res. 2017, 81, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Hincu, M.A.; Zonda, G.I.; Stanciu, G.D.; Nemescu, D.; Paduraru, L. Relevance of Biomarkers Currently in Use or Research for Practical Diagnosis Approach of Neonatal Early-Onset Sepsis. Children 2020, 7, 309. [Google Scholar] [CrossRef] [PubMed]
- Zou, Q.; Wen, W.; Zhang, X.C. Presepsin as a novel sepsis biomarker. World J. Emerg. Med. 2014, 5, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.C.; Lan, H.M.; Han, S.T.; Chaou, C.H.; Yeh, C.F.; Liu, S.H.; Li, C.H.; Blaney, G.N., III; Liu, Z.Y.; Chen, K.F. Comparison of diagnostic accuracy in sepsis between presepsin, procalcitonin, and C-reactive protein: A systematic review and meta-analysis. Ann. Intensive Care 2017, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Pugni, L.; Pietrasanta, C.; Milani, S.; Vener, C.; Ronchi, A.; Falbo, M.; Arghittu, M.; Mosca, F. Presepsin (soluble CD14 subtype): Reference ranges of a new sepsis marker in term and preterm neonates. PLoS ONE 2015, 10, e0146020. [Google Scholar]
- Ishii, M.; Hoshina, T.; Ichikawa, S.; Shimizu, D.; Araki, S.; Kinjo, T.; Shibata, E.; Hachisuga, T.; Kusuhara, K. The physiological variation in plasma presepsin levels during the early neonatal period. Tohoku J. Exp. Med. 2018, 246, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Motalib, T.A.; Khalaf, F.A.; El Hendawy, G.; Kotb, S.E.; Ali, A.M.; Sharnoby, A.E. Soluble CD 14-subtype (Presepsin) and Hepcidin as Diagnostic and Prognostic markers in Early Onset Neonatal Sepsis. EJMM 2015, 24, 45–52. [Google Scholar] [CrossRef]
- Ozdemir, A.A.; Elgormus, Y. Diagnostic Value of Presepsin in Detection of Early-Onset Neonatal Sepsis. Am. J. Perinatol. 2017, 34, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Seliem, W.; Sultan, A.M. Presepsin as a predictor of early onset neonatal sepsis in the umbilical cord blood of premature infants with premature rupture of membranes. Pediatr. Int. 2018, 60, 428–432. [Google Scholar] [CrossRef]
- Sabry, J.H.; Elfeky, O.A.; Elsadek, A.E. Presepsin as an early reliable diagnostic and prognostic marker of neonatal sepsis. Int. J. Adv. Res. 2016, 4, 1538–1549. [Google Scholar] [CrossRef] [Green Version]
- Topcuoglu, S.; Arslanbuga, C.; Gursoy, T.; Aktas, A.; Karatekin, G.; Uluhan, R.; Ovali, F. Role of presepsin in the diagnosis of late-onset neonatal sepsis in preterm infants. J. Matern Neonatal. Med. 2016, 29, 1834–1839. [Google Scholar] [CrossRef]
- Astrawinata, D.A.W.; Kerina Kaban, R.; Dewi Roeslani, R.; Parmawati, E. The Role of Presepsin, C-Reactive Protein and Procalcitonin as a Marker of Therapy Response and Prognosis for Late Onset Neonatal Sepsis in Preterm Neonates. J. Med. Sci. Clin. Res. 2017, 5, 26681–26690. [Google Scholar] [CrossRef]
- Mussap, M.; Puxeddu, E.; Puddu, M.; Ottonello, G.; Coghe, F.; Comite, P.; Cibecchini, F.; Fanos, V. Soluble CD14 subtype (sCD14-ST) presepsin in premature and full term critically ill newborns with sepsis and SIRS. Clin. Chim. Acta 2015, 451, 65–70. [Google Scholar] [CrossRef]
- Saied Osman, A.; Goudah Awadallah, M.; Tabl Hael, M. Presepsin as a novel diagnostic marker in neonatal septicemia. Egypt. J. Med. Microbiol. 2015, 24, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, R.; Khoulouss, S.; Nea, M. Detection of presepsin and surface CD-14 as a biomarker for early diagnosis of neonatal sepsis. J. Am. Sci. 2015, 1111, 104–116. [Google Scholar]
- Tabl, H.A.M.; Abed, N.T. Diagnostic Value of Presepsin in Neonatal Sepsis. Egypt. J. Immunol. 2016, 23, 29–37. [Google Scholar]
- Xiao, T.; Chen, L.P.; Liu, H.; Xie, S.; Luo, Y.; Wu, D.C. The Analysis of Etiology and Risk Factors for 192 Cases of Neonatal Sepsis. BioMed Res. Int. 2017, 2017, 8617076. [Google Scholar] [CrossRef] [Green Version]
- Miyosawa, Y.; Akazawa, Y.; Kamiya, M.; Nakamura, C.; Takeuchi, Y.; Kusakari, M.; Nakamura, T. Presepsin as a predictor of positive blood culture in suspected neonatal sepsis. Pediatr. Int. 2018, 60, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Kumar, J.; Singh, A. A Comparative Evaluation of Presepsin with Procalcitonin and CRP in Diagnosing Neonatal Sepsis: Correspondence. Indian J. Pediatr. 2019, 86, 313–314. [Google Scholar] [CrossRef]
- Iskandar, A.; Arthamin, M.Z.; Indriana, K.; Anshory, M.; Hur, M.; Di Somma, S.; GREAT Network. Comparison between presepsin and procalcitonin in early diagnosis of neonatal sepsis. J. Matern. Neonatal Med. 2019, 32, 3903–3908. [Google Scholar] [CrossRef]
- Hashem, H.E.; Abdel Halim, R.M.; El Masry, S.A.; Mokhtar, A.M.; Abdelaal, N.M. The Utility of Neutrophil CD64 and Presepsin as Diagnostic, Prognostic, and Monitoring Biomarkers in Neonatal Sepsis. Int. J. Microbiol. 2020, 2020, 8814892. [Google Scholar] [CrossRef]
- Pietrasanta, C.; Ronchi, A.; Vener, C.; Poggi, C.; Ballerini, C.; Testa, L.; Colombo, R.M.; Spada, E.; Dani, C.; Mosca, F.; et al. Presepsin (Soluble cd14 subtype) as an early marker of neonatal sepsis and septic shock: A prospective diagnostic trial. Antibiotics 2021, 10, 580. [Google Scholar] [CrossRef]
- Bellos, I.; Fitrou, G.; Pergialiotis, V.; Thomakos, N.; Perrea, D.N.; Daskalakis, G. The diagnostic accuracy of presepsin in neonatal sepsis: A meta-analysis. Eur. J. Pediatr. 2018, 177, 625–632. [Google Scholar] [CrossRef]
- Ruan, L.; Chen, G.Y.; Liu, Z.; Zhao, Y.; Xu, G.Y.; Li, S.F.; Li, C.N.; Chen, L.S.; Tao, Z. The combination of procalcitonin and C-reactive protein or presepsin alone improves the accuracy of diagnosis of neonatal sepsis: A meta-analysis and systematic review. Crit. Care 2018, 22, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Van Maldeghem, I.; Nusman, C.M.; Visser, D.H. Soluble CD14 subtype (sCD14-ST) as biomarker in neonatal early-onset sepsis and late-onset sepsis: A systematic review and meta-analysis. BMC Immunol. 2019, 20, 1–11. [Google Scholar] [CrossRef]
- Parri, N.; Trippella, G.; Lisi, C.; De Martino, M.; Galli, L.; Chiappini, E. Accuracy of presepsin in neonatal sepsis: Systematic review and meta-analysis. Expert Rev. Anti. Infect. Ther. 2019, 20, 17. [Google Scholar] [CrossRef]
- Ng, P.C.; Cheng, S.H.; Chui, K.M.; Fok, T.F.; Wong, M.Y.; Wong, W.; Wong, R.P.; Cheung, K.L. Diagnosis of late onset neonatal sepsis with cytokines, adhesion molecule, and C-reactive protein in preterm very low birthweight infants. Arch. Dis. Child. Fetal Neonatal Ed. 1997, 77, 6–9. [Google Scholar] [CrossRef] [Green Version]
- Memar, M.Y.; Baghi, H.B. Presepsin: A promising biomarker for the detection of bacterial infections. Biomed. Pharmacother. 2019, 111, 649–656. [Google Scholar] [CrossRef]
- Bamba, Y.; Moro, H.; Aoki, N.; Koizumi, T.; Ohshima, Y.; Watanabe, S.; Sakagami, T.; Koya, T.; Takada, T.; Kikuchi, T. Increased presepsin levels are associated with the severity of fungal bloodstream infections. PLoS ONE 2018, 13, e0206089. [Google Scholar] [CrossRef]
- Miyoshi, M.; Inoue, Y.; Nishioka, M.; Ikegame, A.; Nakao, T.; Takayama, T.; Nagai, K. Usefulness of presepsin/creatinine ratio as a new index that corrects for renal function. J. Med. Investig. 2021, 68, 105–111. [Google Scholar] [CrossRef]
- Okamura, Y.; Yokoi, H. Development of a point-of-care assay system for measurement of presepsin (sCD14-ST). Clin. Chim. Acta 2011, 412, 2157–2161. [Google Scholar] [CrossRef]
- Galliera, E.; Massaccesi, L.; de Vecchi, E.; Banfi, G.; Romanelli, M. Clinical application of presepsin as diagnostic biomarker of infection: Overview and updates. Clin. Chem. Lab. Med. 2019, 44, 21–27. [Google Scholar] [CrossRef]
- Nagata, T.; Yasuda, Y.; Ando, M.; Abe, T.; Katsuno, T.; Kato, S.; Tsuboi, N.; Matsuo, S.; Maruyama, S. Clinical impact of kidney function on presepsin levels. PLoS ONE 2015, 10, e0129159. [Google Scholar] [CrossRef] [Green Version]
- Handke, J.; Piazza, O.; Larmann, J.; Tesoro, S.; De Robertis, E. Presepsin as a biomarker in perioperative medicine. Minerva Anestesiol. 2020, 86, 768–776. [Google Scholar] [CrossRef]
- Nakamura, Y.; Ishikura, H.; Nishida, T.; Kawano, Y.; Yuge, R.; Ichiki, R.; Murai, A. Usefulness of presepsin in the diagnosis of sepsis in patients with or without acute kidney injury. BMC Anesthesiol. 2014, 14, 88. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, Y.; Murai, A.; Mizunuma, M.; Ohta, D.; Kawano, Y.; Matsumoto, N.; Nishida, T.; Ishikura, H. Potential use of procalcitonin as biomarker for bacterial sepsis in patients with or without acute kidney injury. J. Infect. Chemother. 2015, 21, 257–263. [Google Scholar] [CrossRef]
- Nakamura, Y.; Hoshino, K.; Kiyomi, F.; Kawano, Y.; Mizunuma, M.; Tanaka, J.; Nishida, T.; Ishikura, H. Comparison of accuracy of presepsin and procalcitonin concentrations in diagnosing sepsis in patients with and without acute kidney injury. Clin. Chim. Acta 2019, 490, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Leonard, N.; Mohora, R.; Cretoiu, D.; Condrat, C.E.; Stoicescu, S.M. Congenital nephrogenic diabetes insipidus in a preterm infant: Case presentation. Acta Endocrinol. 2019, 15, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Shirakawa, K.; Naitou, K.; Hirose, J.; Takahashi, T.; Furusako, S. Presepsin (sCD14-ST): Development and evaluation of one-step ELISA with a new standard that is similar to the form of presepsin in septic patients. Clin. Chem. Lab. Med. 2011, 49, 937–939. [Google Scholar] [CrossRef]
- Sandquist, M.; Wong, H.R. Biomarkers of sepsis and their potential value in diagnosis, prognosis and treatment. Expert Rev. Clin. Immunol. 2014, 10, 1349–1356. [Google Scholar] [CrossRef] [Green Version]
- Taneja, R.; Batra, P. Biomarkers as point of care tests (POCT) in neonatal sepsis: A state of science review. J. Neonatal Perinat. Med. 2021, 14, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Di Serio, F.; Caputo, M.; Zaninotto, M.; Ottomano, C.; Plebani, M. Evaluation of analytical performance of the Pathfast cardiac troponin I. Clin. Chem. Lab. Med. 2009, 47, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Endo, S.; Suzuki, Y.; Takahashi, G.; Shozushima, T.; Ishikura, H.; Murai, A.; Nishida, T.; Irie, Y.; Miura, M.; Iguchi, H.; et al. Usefulness of presepsin in the diagnosis of sepsis in a multicenter prospective study. J. Infect. Chemother. 2012, 18, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Masson, S.; Caironi, P.; Fanizza, C.; Thomae, R.; Bernasconi, R.; Noto, A.; Oggioni, R.; Pasetti, G.S.; Romero, M.; Tognoni, G.; et al. Circulating presepsin (soluble CD14 subtype) as a marker of host response in patients with severe sepsis or septic shock: Data from the multicenter, randomized ALBIOS trial. Intensive Care Med. 2015, 41, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulla, M.; Pizzolato, E.; Lucchiari, M.; Loiacono, M.; Soardo, F.; Forno, D.; Morello, F.; Lupia, E.; Moiraghi, C.; Mengozzi, G.; et al. Diagnostic and prognostic value of presepsin in the management of sepsis in the emergency department: A multicenter prospective study. Crit. Care 2013, 17, R168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chenevier-Gobeaux, C.; Borderie, D.; Weiss, N.; Mallet-Coste, T.; Claessens, Y.E. Presepsin (sCD14-ST), an innate immune response marker in sepsis. Clin. Chim. Acta 2015, 450, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Klouche, K.; Cristol, J.P.; Devin, J.; Gilles, V.; Kuster, N.; Larcher, R.; Amigues, L.; Corne, P.; Jonquet, O.; Dupuy, A.M. Diagnostic and prognostic value of soluble CD14 subtype (Presepsin) for sepsis and community-acquired pneumonia in ICU patients. Ann. Intensive Care 2016, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Sakyi, S.A.; Enimil, A.; Adu, D.K.; Ephraim, R.D.; Danquah, K.O.; Fondjo, L.; Baidoe-Ansah, D.; Adoba, P.; Toboh, E.; Afranie, B.O. Individual and combined bioscore model of presepsin, procalcitonin, and high sensitive C-reactive protein as biomarkers for early diagnosis of paediatric sepsis. Heliyon 2020, 6, e04841. [Google Scholar] [CrossRef]
- Yoon, S.H.; Kim, E.H.; Kim, H.Y.; Ahn, J.G. Presepsin as a diagnostic marker of sepsis in children and adolescents: A systemic review and meta-analysis. BMC Infect. Dis. 2019, 19, 760. [Google Scholar] [CrossRef] [Green Version]
- Levy, O. Innate immunity of the newborn: Basic mechanisms and clinical correlates. Nat. Rev. Immunol. 2007, 7, 379–390. [Google Scholar] [CrossRef]
- Levy, E.; Xanthou, G.; Petrakou, E.; Zacharioudaki, V.; Tsatsanis, C.; Fotopoulos, S.; Xanthou, M. Distinct roles of TLR4 and CD14 in LPS-induced inflammatory responses of neonates. Pediatr. Res. 2009, 66, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Perrone, S.; Lotti, F.; Longini, M.; Rossetti, A.; Bindi, I.; Bazzini, F.; Belvisi, E.; Sarnacchiaro, P.; Scapellato, C.; Buonocore, G.C. Reactive protein in healthy term newborns during the first 48 hours of life. Arch. Dis. Child Fetal. Neonatal Ed. 2018, 103, F163–F166. [Google Scholar] [CrossRef] [PubMed]
- Macallister, K.; Smith-Collins, A.; Gillet, H.; Hamilton, L.; Davis, J. Serial C-Reactive Protein Measurements in Newborn Infants without Evidence of Early-Onset Infection. Neonatology 2019, 116, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Hamade, B.; Huang, D.T. Procalcitonin: Where Are We Now? Crit. Care Clin. 2020, 36, 23–40. [Google Scholar] [CrossRef]
- Mwesigye, P.; Rizwan, F.; Alassaf, N.; Khan, R. The Role and Validity of Diagnostic Biomarkers in Late-Onset Neonatal Sepsis. Cureus 2021, 13, 4–11. [Google Scholar]
- Kuzniewicz, M.W.; Mukhopadhyay, S.; Li, S.; Walsh, E.M.; Puopolo, K.M. Time to Positivity of Neonatal Blood Cultures for Early-onset Sepsis. Pediatr. Infect. Dis. J. 2020, 39, 634–640. [Google Scholar] [CrossRef]
- Yang, H.S.; Hur, M.; Yi, A.; Kim, H.; Lee, S.; Kim, S.N. Prognostic value of presepsin in adult patients with sepsis: Systematic review and meta-analysis. PLoS ONE 2018, 13, e0191486. [Google Scholar] [CrossRef]
- Gad, G.I.; Shinkar, D.M.; Kamel El-Din, M.M.; Nagi, H.M. The Utility of Soluble CD14 Subtype in Early Diagnosis of Culture-Proven Early-Onset Neonatal Sepsis and Prediction of Outcome. Am. J. Perinatol. 2020, 37, 497–502. [Google Scholar] [CrossRef]
- El Gendy, F.M.; El-Mekkawy, M.S.; Saleh, N.Y.; Habib, M.S.E.D.; Younis, F.E. Clinical study of Presepsin and Pentraxin 3 in critically ill children. J. Crit. Care 2018, 47, 36–40. [Google Scholar] [CrossRef]


{kind=link}
| 5th Centile | 25th Centile | 50th Centile | 75th Centile | 95th Centile | |
|---|---|---|---|---|---|
| Term (>37 weeks GA)[n= 484] | 315 | 466 | 604 | 791 | 1178 |
| Preterm (24–36 weeks GA)[n= 195] | 352 | 503 | 620 | 864 | 1370 |
| Type of Study | Authors, Year | Country | Population | Cut-off Value of P-SEP (pg/mL) | AUC | Type of Sample | Assay | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Referenceranges | ||||||||
| Prospective | Pugni et al., 2015 [14] | Italy | 484 healthy term 195 healthy preterm (GA 24–36 w) | 604 (50th centile) 620 (50th centile) | N/A | Whole blood | CLEIA | P-SEP levels are higher in preterm than in at-term neonates |
| Prospective | Ishii et al., 2018 [15] | Japan | 30 healthy term (GA > 37 w) | 318.5 (at birth) 180.5 (day 5) | N/A | Whole blood | CLEIA | P-SEP levels show physiological variation during early neonatal period |
| Prospective | Poggi et al., 2020 [4] | Italy | 183 preterm (GA < 32 w) | 583 (0–6 h) 614 (12 h) 604 (24 h) 513 (48 h) 50th centile | N/A | Whole blood | CLEIA | P-SEP levels in preterm <32 weeks GA are affected by GA during first 24 h of life |
| EOS | ||||||||
| Case- control | Motalib et al., 2015 [16] | Egypt | 28 EOS 34 healthy | 672 | 0.95 | Serum | CLEIA | P-SEP is an accurate marker in detecting EOS |
| Prospective | Ozdemir et al., 2016 [17] | Turkey | 29 EOS 40 healthy (term neonates) | 539 | 0.77 | Serum | CLEIA | P-SEP may be used a reliable and accurate marker for both diagnosis and follow-up of EOS |
| Case- control | Montaldo et al., 2017 [10] | Italy | 32 EOS 38 healthy (GA < 34 w) | 788 | 0.97 | Serum | CLEIA | P-SEP is significantly higher in preterm infants with EOS compared with uninfected infants |
| Prospective | Seliem and Sultan, 2018 [18] | Egypt | 76 EOS 212 healthy (GA 24–36 w) | 2231 | N/A | Umbilical cord blood | ELISA | Umbilical cord blood P-SEP is a predictor of EOS in preterm infants born to mothers with premature rupture of membranes |
| LOS | ||||||||
| Prospective | Poggi et al., 2015 [1] | Italy | 19 LOS 21 healthy (GA < 32 w) | 885 | 0.97 | Whole blood | CLEIA | P-SEP is an accurate marker for the diagnosis of LOS in preterm infants |
| Case- control | Sabry et al., 2016 [19] | Egypt | 80 LOS 40 healthy | 722 | 0.99 | Serum | ELISA | P-SEP is an accurate marker for the diagnosis of LOS |
| Prospective | Topcuoglu et al., 2016 [20] | Turkey | 42 LOS (GA < 34 w) | 800.5 | 0.86 | Plasma | CLEIA | P-SEP can used as a reliable biomarker for the diagnosis of and response to treatment in LOS |
| Prospective | Astrawinata et al., 2017 [21] | Indonesia | 40 LOS in preterm 40 healthy | 406 | 0.89 | Whole blood | CLEIA | P-SEP is the earliest and best-performing marker of LOS for the prognosis of preterm neonatal mortality when compared to CRP and PCT |
| EOS/LOS | ||||||||
| Prospective | Mussap et al., 2015 [22] | Italy | 25 sepsis 25 SIRS 25 healthy | 600 | 0.99 | Whole blood | CLEIA | In critically ill neonates, P-SEP could help in diagnosis and follow-up of neonatal sepsis and non-bacterial SIRS |
| Case- control | Saied Osman et al., 2015 [23] | Egypt | 40 sepsis 15 healthy (full-term) | 875 | 0.95 | Plasma | CLEIA | P-SEP is a novel diagnostic marker in neonatal sepsis |
| Prospective | Mostafa et al., 2015 [24] | Egypt | 49 sepsis 29 healthy | 686 | 0.78 | Plasma | CLEIA | P-SEP is useful in neonatal sepsis |
| N/A | Tabl et al., 2016 [25] | Egypt | 22 sepsis 28 non- infectious SIRS 20 healthy (term neonates) | 812 | 0.99 | Plasma | CLEIA | P-SEP can discriminate between infections and non-infectious inflammatory conditions |
| Prospective | Xiao et al., 2016 [26] | China | 140 sepsis 53 healthy | 786 | 0.94 | Whole blood | CLEIA | PSEP is accurate in early identify neonatal hematosepsis; its diagnostic value is superior to other laboratory Biomarkers |
| Prospective | Miyosawa et al., 2018 [27] | Japan | 13 sepsis 18 healthy (preterm) | 795 | 0.86 | Whole blood | CLEIA | P-SEP can discriminate between infections and non-infectious inflammatory conditions |
| Prospective | Kumar, et al., 2018 [28] | India | 41 sepsis | 1800 | 0.90 | Plasma | CLEIA | P-SEP, in comparison with CRP and PCT, offers a better sensitivity and negative predictive value |
| Prospective | Iskandar et al., 2018 [29] | Indonesia | 51 sepsis | 706.5 | 0.80 | Whole blood | CLEIA | In early diagnosis of neonatal sepsis, compared with procalcitonin, presepsin seems to provide a better diagnostic value |
| Prospective | Hashem et al., 2020 [30] | Egypt | 133 sepsis 102 healthy | 686 | 0.88 | Plasma | CLEIA | Presepsin is a valuable early diagnostic and monitoring sepsis biomarker, with higher specificity compared to neutrophil CD64 (nCD64) |
| Prospective | Pietrasanta et al., 2021 [31] | Italy | 58 infections 77 sepsis 24 septic shock | 987.5 | 0.86 | Whole blood | CLEIA | P-SEP is an early marker of neonatal sepsis severity, but does not support the early identification of neonates with positive blood culture |
| Number of Studies Considered | Authors, Year | Country | Number of Infants Included | Cut-off Value of P-SEP (pg/mL) | AUC | Pooled Sensitivity | Pooled Specificity | Conclusions |
|---|---|---|---|---|---|---|---|---|
| 11 studies | Bellos et al., 2018 [32] | Greece | 783 (391 sepsis vs. 392 controls) | <650 | 0.96 | 91% | 85% | Diagnostic accuracy of P-SEP resulted high in detecting neonatal sepsis |
| 650–850 | 0.99 | 91% | 97% | |||||
| >850 | 0.97 | 90% | 86% | |||||
| 28 studies comparing CRP, PCT, CRP + PCT or P-SEP | Ruan et al., 2018 [33] | China | 2661 (1281 sepsis vs. 1380 controls) | 722 | 0.99 | 94% | 98% | The combination of PCT and CRP or presepsin alone improves the accuracy of diagnosis of neonatal sepsis |
| 10 studies | Van Maldeghem et al., 2019 [34] | Holland | 1369 (89 EOS, 61 LOS, 209 EOS and LOS combined vs. 1010 controls) | 305–672 | 0.94 | 81% | 86% | P-SEP is a promising and rapid-responding diagnostic biomarker for EOS and LOS. The difference in pooled means between EOS and LOS underlines the importance of considering them as two different disease entities |
| 801–855 | N/A | 81% | 100% | |||||
| 9 studies | Parri et al., 2019 [35] | Italy | 3 studies including 268 infants | <600 | 0.81 | 93% | 81% | Even though it cannot be recommended as a single diagnostic test, P-SEP could be a helpful and valuable biomarker in neonates with suspected sepsis |
| 6 studies including 375 infants | >600 | 0.97 | 87% | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maddaloni, C.; De Rose, D.U.; Santisi, A.; Martini, L.; Caoci, S.; Bersani, I.; Ronchetti, M.P.; Auriti, C. The Emerging Role of Presepsin (P-SEP) in the Diagnosis of Sepsis in the Critically Ill Infant: A Literature Review. Int. J. Mol. Sci. 2021, 22, 12154. https://doi.org/10.3390/ijms222212154
Maddaloni C, De Rose DU, Santisi A, Martini L, Caoci S, Bersani I, Ronchetti MP, Auriti C. The Emerging Role of Presepsin (P-SEP) in the Diagnosis of Sepsis in the Critically Ill Infant: A Literature Review. International Journal of Molecular Sciences. 2021; 22(22):12154. https://doi.org/10.3390/ijms222212154
Chicago/Turabian StyleMaddaloni, Chiara, Domenico Umberto De Rose, Alessandra Santisi, Ludovica Martini, Stefano Caoci, Iliana Bersani, Maria Paola Ronchetti, and Cinzia Auriti. 2021. "The Emerging Role of Presepsin (P-SEP) in the Diagnosis of Sepsis in the Critically Ill Infant: A Literature Review" International Journal of Molecular Sciences 22, no. 22: 12154. https://doi.org/10.3390/ijms222212154
APA StyleMaddaloni, C., De Rose, D. U., Santisi, A., Martini, L., Caoci, S., Bersani, I., Ronchetti, M. P., & Auriti, C. (2021). The Emerging Role of Presepsin (P-SEP) in the Diagnosis of Sepsis in the Critically Ill Infant: A Literature Review. International Journal of Molecular Sciences, 22(22), 12154. https://doi.org/10.3390/ijms222212154