
Dopamine Transporter Imaging, Current Status of a Potential Biomarker: A Comprehensive Review

 ,
,
Abstract
1. Introduction
2. Targets of Dopaminergic Imaging
3. Confounding Factors on the Interpretation of DAT
4. DAT Imaging and Its Relationship to the Pathological Degeneration of the Nigrostriatal Pathway
5. DAT Imaging as Diagnostic Biomarker
6. DAT Imaging as Preclinical Biomarker
7. DAT Imaging as Predictive Biomarker: Motor Measures
8. DAT Imaging as Predictive Biomarker: Motor Complications
9. DAT Imaging as Predictive Biomarker: Non-Motor Measures
10. Beyond DAT: Correlation with Other Potential Nigrostriatal Biomarkers in PD
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Langston, J.W. The Parkinson’s complex: Parkinsonism is just the tip of the Iceberg. Ann. Neurol. 2006, 59, 591–596. [Google Scholar] [CrossRef]
- Rosa-Grilo, M.; Qamar, M.A.; Taddei, R.N.; Pagonabarraga, J.; Kulisevsky, J.; Sauerbier, A.; Chaudhuri, K.R. Rotigotine transdermal patch and sleep in Parkinson’s disease: Where are we now? NPJ Park. Dis. 2017, 3, 28. [Google Scholar] [CrossRef]
- Adler, C.H.; Beach, T.G.; Hentz, J.G.; Shill, H.A.; Caviness, J.N.; Driver-Dunckley, E.; Sabbagh, M.N.; Sue, L.I.; Jacobson, S.A.; Belden, C.M.; et al. Low clinical diagnostic accuracy of early vs. advanced Parkinson disease: Clinicopathologic study. Neurology 2014, 83, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Copetti, M.; Arcuti, S.; Martino, D.; Fontana, A.; Logroscino, G. Accuracy of clinical diagnosis of Parkinson disease. Neurology 2016, 86, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Ray Dorsey, E.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.Y.J.; Collado-Mateo, D.; et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I.G.; Boeve, B.F.; Dickson, D.W.; Halliday, G.; Taylor, J.P.; Weintraub, D.; Aarsland, D.; Galvin, J.; Attems, J.; Ballard, C.G.; et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology 2017, 89, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Rispoli, V.; Schreglmann, S.R.; Bhatia, K.P. Neuroimaging advances in Parkinson’s disease. Curr. Opin. Neurol. 2018, 31, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Uhl, G.R. Dopamine transporter: Basic science and human variation of a key molecule for dopaminergic function, locomotion, and parkinsonism. Mov. Disord. 2003, 18, 10578. [Google Scholar] [CrossRef]
- Sulzer, D.; Cragg, S.J.; Rice, M.E. Striatal Dopamine Neurotransmission: Regulation of Release and Uptake; Elsevier: Amsterdam, The Netherlands, 2016; Volume 6, ISBN 4418652825. [Google Scholar]
- Benamer, H.T.S.; Patterson, J.; Wyper, D.J.; Hadley, D.M.; Macphee, G.J.A.; Grosset, D.G. Correlation of Parkinson’s disease severity and duration with 123I-FP-CIT SPECT striatal uptake. Mov. Disord. 2000, 15, 692–698. [Google Scholar] [CrossRef]
- Booij, J.; Tissingh, G.; Boer, G.J.; Speelman, J.D.; Stoof, J.C.; Janssen, A.G.M.; Wolters, E.C.; Van Royen, E.A. [123I]FP-CIT SPECT shows a pronounced decline of striatal dopamine transporter labelling in early and advanced Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1997, 62, 133–140. [Google Scholar] [CrossRef]
- Mozley, P.D.; Schneider, J.S.; Acton, P.D.; Plössl, K.; Stern, M.B.; Siderowf, A.; Leopold, N.A.; Li, P.Y.; Alavi, A.; Kung, H.F. Binding of [99mTc]TRODAT-1 to dopamine transporters in patients with Parkinson’s disease and in healthy volunteers. J. Nucl. Med. 2000, 41, 584–589. [Google Scholar]
- Marek, K.; Innis, R.; Van Dyck, C.; Fussell, B.; Early, M.; Eberly, S.; Oakes, D.; Seibyl, J. [123I]β-CIT SPECT imaging assessment of the rate of Parkinson’s disease progression. Neurology 2001, 57, 2089–2094. [Google Scholar] [CrossRef]
- Kim, H.J.; Im, J.H.; Yang, S.O.; Moon, D.H.; Ryu, J.S.; Bong, J.K.; Nam, K.P.; Cheon, J.H.; Lee, M.C.; Lee, H.K. Imaging and quantitation of dopamine transporters with iodine-123-IPT in normal and Parkinson’s disease subjects. J. Nucl. Med. 1997, 38, 1703–1711. [Google Scholar]
- Bohnen, N.I.; Djang, D.S.W.; Herholz, K.; Anzai, Y.; Minoshima, S. Effectiveness and safety of 18F-FDG PET in the evaluation of dementia: A review of the recent literature. J. Nucl. Med. 2012, 53, 59–71. [Google Scholar] [CrossRef]
- Djang, D.S.W.; Janssen, M.J.R.; Bohnen, N.; Booij, J.; Henderson, T.A.; Herholz, K.; Minoshima, S.; Rowe, C.C.; Sabri, O.; Seibyl, J.; et al. SNM practice guideline for dopamine transporter imaging with 123I-ioflupane SPECT 1.0. J. Nucl. Med. 2012, 53, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Marcus, C.; Sheikhbahaei, S.; Solnes, L.B.; Leal, J.P.; Du, Y.; Rowe, S.P.; Higuchi, T.; Buck, A.K.; Lapa, C.; et al. Visual and semiquantitative accuracy in clinical baseline 123I-Ioflupane SPECT/CT imaging. Clin. Nucl. Med. 2019, 44, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Nicastro, N.; Garibotto, V.; Burkhard, P.R. Extrastriatal 123I-FP-CIT SPECT impairment in Parkinson’s disease-the PPMI cohort. BMC Neurol. 2020, 20, 192. [Google Scholar] [CrossRef]
- Kaasinen, V.; Joutsa, J.; Noponen, T.; Johansson, J.; Seppänen, M. Effects of aging and gender on striatal and extrastriatal [123I]FP-CIT binding in Parkinson’s disease. Neurobiol. Aging 2015, 36, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Meoni, S.; Macerollo, A.; Moro, E. Sex differences in movement disorders. Nat. Rev. Neurol. 2020, 16, 84–96. [Google Scholar] [CrossRef]
- Van Dyck, C.H.; Seibyl, J.P.; Malison, R.T.; Laruelle, M.; Zoghbi, S.S.; Baldwin, R.M.; Innis, R.B. Age-related decline in dopamine transporters: Analysis of striatal subregions, nonlinear effects, and hemispheric asymmetries. Am. J. Geriatr. Psychiatry 2002, 10, 36–43. [Google Scholar] [CrossRef]
- Varrone, A.; Dickson, J.C.; Tossici-Bolt, L.; Sera, T.; Asenbaum, S.; Booij, J.; Kapucu, O.L.; Kluge, A.; Knudsen, G.M.; Koulibaly, P.M.; et al. European multicentre database of healthy controls for [123I]FP-CIT SPECT (ENC-DAT): Age-related effects, gender differences and evaluation of different methods of analysis. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 213–227. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, M.F.; Apparsundaram, S.; Gerhardt, G.A. Decreased plasma membrane expression of striatal dopamine transporter in aging. Neurobiol. Aging 2003, 24, 1147–1154. [Google Scholar] [CrossRef]
- Cruz-Muros, I.; Afonso-Oramas, D.; Abreu, P.; Pérez-Delgado, M.M.; Rodríguez, M.; González-Hernández, T. Aging effects on the dopamine transporter expression and compensatory mechanisms. Neurobiol. Aging 2009, 30, 973–986. [Google Scholar] [CrossRef] [PubMed]
- Troiano, A.R.; Schulzer, M.; De La Fuente-Fernandez, R.; Mak, E.; Mckenzie, J.; Sossi, V.; Mccormick, S.; Ruth, T.J.; Stoessl, A.J. Dopamine transporter PET in normal aging: Dopamine transporter decline and its possible role in preservation of motor function. Synapse 2010, 64, 146–151. [Google Scholar] [CrossRef]
- Tissingh, G.; Bergmans, P.; Booij, J.; Winogrodzka, A.; Stoof, J.C.; Wolters, E.C.; Van Royen, E.A. [123I]β-CIT single-photon emission tomography in Parkinson’s disease reveals a smaller decline in dopamine transporters with age than in controls. Eur. J. Nucl. Med. 1997, 24, 1171–1174. [Google Scholar] [CrossRef] [PubMed]
- Tissingh, G.; Booij, J.; Bergmans, P.; Winogrodzka, A.; Janssen, A.G.M.; Van Royen, E.A.; Stoof, J.C.; Wolters, E.C. Iodine-123-N-ω-fluoropropyl-2/β-carbomethoxy3β-(4-iodophenyl)tropane SPECT in healthy controls and early-stage, drug-naive Parkinson’s disease. J. Nucl. Med. 1998, 39, 1143–1148. [Google Scholar] [PubMed]
- Lee, C.S.; Kim, S.J.; Oh, S.J.; Kim, H.O.; Yun, S.C.; Doudet, D.; Kim, J.S. Uneven age effects of [18F]FP-CIT binding in the striatum of Parkinson’s disease. Ann. Nucl. Med. 2014, 28, 874–879. [Google Scholar] [CrossRef]
- Lavalaye, J.; Knol, R.J.J.; De Bruin, K.; Reneman, L.; Janssen, A.G.M.; Booij, J. [123I]FP-CIT binding in rat brain after acute and sub-chronic administration of dopaminergic medication. Eur. J. Nucl. Med. 2000, 27, 346–349. [Google Scholar] [CrossRef]
- Harper Mozley, L.; Gur, R.C.; Mozley, R.D.; Gur, R.E. Striatal dopamine transporters and cognitive functioning in healthy men and women. Am. J. Psychiatry 2001, 158, 1492–1499. [Google Scholar] [CrossRef]
- Staley, J.K.; Krishnan-Sarin, S.; Zoghbi, S.; Tamagnan, G.; Fujita, M.; Seibyl, J.P.; Maciejewski, P.K.; O’Malley, S.; Innis, R.B. Sex differences in [123I]β-CIT SPECT measures of dopamine and serotonin transporter availability in healthy smokers and nonsmokers. Synapse 2001, 41, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Ham, J.H.; Lee, P.H.; Sohn, Y.H. Gender Differences in Age-Related Striatal Dopamine Depletion in Parkinson’s Disease. J. Mov. Disord. 2015, 8, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Ryding, E.; Lindström, M.; Brådvik, B.; Grabowski, M.; Bosson, P.; Träskman-Bendz, L.; Rosén, I. A new model for separation between brain dopamine and serotonin transporters in 123I-β-CIT SPECT measurements: Normal values and sex and age dependence. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1114–1118. [Google Scholar] [CrossRef] [PubMed]
- Best, S.E.; Sarrel, P.M.; Malison, R.T.; Laruelle, M.; Zoghbi, S.S.; Baldwin, R.M.; Seibyl, J.P.; Innis, R.B.; Van Dyck, C.H. Striatal dopamine transporter availability with [123I]β-CIT SPECT is unrelated to gender or menstrual cycle. Psychopharmacology (Berl). 2005, 183, 181–189. [Google Scholar] [CrossRef]
- Munro, C.A.; McCaul, M.E.; Wong, D.F.; Oswald, L.M.; Zhou, Y.; Brasic, J.; Kuwabara, H.; Kumar, A.; Alexander, M.; Ye, W.; et al. Sex Differences in Striatal Dopamine Release in Healthy Adults. Biol. Psychiatry 2006, 59, 966–974. [Google Scholar] [CrossRef]
- Wong, K.K.; Müller, M.L.T.M.; Kuwabara, H.; Studenski, S.A.; Bohnen, N.I. Gender differences in nigrostriatal dopaminergic innervation are present at young-to-middle but not at older age in normal adults. J. Clin. Neurosci. 2012, 19, 183–184. [Google Scholar] [CrossRef] [PubMed]
- Haaxma, C.A.; Bloem, B.R.; Borm, G.F.; Oyen, W.J.G.; Leenders, K.L.; Eshuis, S.; Booij, J.; Dluzen, D.E.; Horstink, M.W.I.M. Gender differences in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2007, 78, 819–824. [Google Scholar] [CrossRef]
- Innis, R.B.; Marek, K.L.; Sheff, K.; Zoghbi, S.; Castronuovo, J.; Feigin, A.; Seibyl, J.P. Effect of treatment with L-dopa/carbidopa or L-selegiline on striatal dopamine transporter SPECT imaging with [123I]β-CIT. Mov. Disord. 1999, 14, 436–442. [Google Scholar] [CrossRef]
- Nurmi, E.; Bergman, J.; Eskola, O.; Solin, O.; Hinkka, S.M.; Sonninen, P.; Rinne, J.O. Reproducibility and effect of levodopa on dopamine transporter function measurements: A [18F]CFT PET study. J. Cereb. Blood Flow Metab. 2000, 20, 1604–1609. [Google Scholar] [CrossRef]
- Parkinson Study Group Dopamine Transporter Brain Imaging to Assess the Effects of Pramipexole vs. Levodopa on Parkinson Disease Progression. JAMA 2002, 287, 1653. [CrossRef]
- Whone, A.L.; Watts, R.L.; Stoessl, A.J.; Davis, M.; Reske, S.; Nahmias, C.; Lang, A.E.; Rascol, O.; Ribeiro, M.J.; Remy, P.; et al. Slower progression of Parkinson’s disease with ropinirole versus levodopa: The REAL-PET study. Ann. Neurol. 2003, 54, 93–101. [Google Scholar] [CrossRef]
- Ravina, B.; Marek, K.; Eberly, S.; Oakes, D.; Kurlan, R.; Ascherio, A.; Beal, F.; Beck, J.; Flagg, E.; Galpern, W.R.; et al. Dopamine transporter imaging is associated with long-term outcomes in Parkinson’s disease. Mov. Disord. 2012, 27, 1392–1397. [Google Scholar] [CrossRef]
- Ahlskog, J.E.; Uitti, R.J.; O’Connor, M.K.; Maraganore, D.M.; Matsumoto, J.Y.; Stark, K.F.; Turk, M.F.; Burnett, O.L. The effect of dopamine agonist therapy on dopamine transporter imaging in Parkinson’s disease. Mov. Disord. 1999, 14, 940–946. [Google Scholar] [CrossRef]
- Roussakis, A.A.; Politis, M.; Towey, D.; Piccini, P. Serotonin-to-dopamine transporter ratios in Parkinson disease. Neurology 2016, 86, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Rossi, C.; Genovesi, D.; Marzullo, P.; Giorgetti, A.; Filidei, E.; Corsini, G.U.; Bonuccelli, U.; Ceravolo, R. Striatal dopamine transporter modulation after rotigotine: Results from a pilot single-photon emission computed tomography study in a group of early stage Parkinson disease patients. Clin. Neuropharmacol. 2017, 40, 34–36. [Google Scholar] [CrossRef]
- Guttman, M.; Stewart, D.; Hussey, D.; Wilson, A.; Houle, S.; Kish, S. Influence of L-dopa and pramipexole on striatal dopamine transporter in early PD. Neurology 2001, 56, 1559–1564. [Google Scholar] [CrossRef] [PubMed]
- Booij, J.; De Jong, J.; De Bruin, K.; Knol, R.; De Win, M.M.L.; Van Eck-Smit, B.L.F. Quantification of striatal dopamine transporters with123I-FP-CIT SPECT is influenced by the selective serotonin reuptake inhibitor paroxetine: A double-blind, placebo-controlled, crossover study in healthy control subjects. J. Nucl. Med. 2007, 48, 359–366. [Google Scholar]
- Ikeda, K.; Ebina, J.; Kawabe, K.; Iwasaki, Y. Dopamine transporter imaging in parkinson disease: Progressive changes and therapeutic modification after anti-parkinsonian medications. Intern. Med. 2019, 58, 1665–1672. [Google Scholar] [CrossRef]
- Morbelli, S.; Esposito, G.; Arbizu, J.; Barthel, H.; Boellaard, R.; Bohnen, N.I. EANM practice guideline / SNMMI procedure standard for dopaminergic imaging in Parkinsonian syndromes 1.0. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1885–1912. [Google Scholar] [CrossRef]
- Booij, J.; Kemp, P. Dopamine transporter imaging with [123I]FP-CIT SPECT: Potential effects of drugs. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 424–438. [Google Scholar] [CrossRef]
- Tatsch, K.; Poepperl, G. Nigrostriatal dopamine terminal imaging with dopamine transporter SPECT: An update. J. Nucl. Med. 2013, 54, 1331–1338. [Google Scholar] [CrossRef]
- Byas-Smith, M.; Votaw, J.; Hua, J.; Voll, R.; Martarello, L.; Levey, A.I.; Goodman, M. Phenylephrine and norepinephrine increase dopamine transporter ligand binding in striatum. Mol. Imaging Biol. 2003, 5, 217–226. [Google Scholar] [CrossRef]
- Ikeda, K.; Yanagihashi, M.; Miura, K.; Ishikawa, Y.; Hirayama, T.; Takazawa, T.; Kano, O.; Kawabe, K.; Mizumura, N.; Iwasaki, Y. Zonisamide cotreatment delays striatal dopamine transporter reduction in Parkinson disease: A retrospective, observational cohort study. J. Neurol. Sci. 2018, 391, 5–9. [Google Scholar] [CrossRef]
- Iffland, K.; Grotenhermen, F. An Update on Safety and Side Effects of Cannabidiol: A Review of Clinical Data and Relevant Animal Studies. Cannabis Cannabinoid Res. 2017, 2, 139–154. [Google Scholar] [CrossRef]
- Ashok, A.H.; Mizuno, Y.; Howes, O.D. Tobacco smoking and dopaminergic function in humans: A meta-analysis of molecular imaging studies. Psychopharmacology 2019, 236, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, G.; Knudsen, G.M.; Jensen, P.S.; Ziebell, M.; Holst, K.K.; Asenbaum, S.; Booij, J.; Darcourt, J.; Dickson, J.C.; Kapucu, Ö.L.; et al. No difference in striatal dopamine transporter availability between active smokers, ex-smokers and non-smokers using [123I]FP-CIT (DaTSCAN) and SPECT. EJNMMI Res. 2013, 3, 39. [Google Scholar] [CrossRef]
- Van De Giessen, E.M.; De Win, M.M.L.; Tanck, M.W.T.; Van Den Brink, W.; Baas, F.; Booij, J. Striatal dopamine transporter availability associated with polymorphisms in the dopamine transporter gene SLC6A3. J. Nucl. Med. 2009, 50, 45–52. [Google Scholar] [CrossRef]
- Costa, A.; Riedel, M.; Müller, U.; Möller, H.J.; Ettinger, U. Relationship between SLC6A3 genotype and striatal dopamine transporter availability: A meta-analysis of human single photon emission computed tomography studies. Synapse 2011, 65, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Manni, C.; Pierantozzi, M.; Brusa, L.; Danieli, R.; Stanzione, P.; Schillaci, O. I-fp-cit semi-quantitative spect detects preclinical bilateral dopaminergic deficit in early parkinson’s disease with unilateral symptoms. Nucl. Med. Commun. 2005, 26, 421–426. [Google Scholar] [CrossRef]
- Contrafatto, D.; Mostile, G.; Nicoletti, A.; Raciti, L.; Luca, A.; Dibilio, V.; Lanzafame, S.; Distefano, A.; Drago, F.; Zappia, M. Single photon emission computed tomography striatal asymmetry index may predict dopaminergic responsiveness in Parkinson disease. Clin. Neuropharmacol. 2011, 34, 71–73. [Google Scholar] [CrossRef]
- Scherfler, C.; Seppi, K.; Mair, K.J.; Donnemiller, E.; Virgolini, I.; Wenning, G.K.; Poewe, W. Left hemispheric predominance of nigrostriatal dysfunction in Parkinson’s disease. Brain 2012, 135, 3348–3354. [Google Scholar] [CrossRef]
- Barrett, M.J.; Wylie, S.A.; Harrison, M.B.; Wooten, G.F. Handedness and motor symptom asymmetry in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2011, 82, 1122–1124. [Google Scholar] [CrossRef]
- Kaasinen, V. Ipsilateral deficits of dopaminergic neurotransmission in Parkinson’s disease. Ann. Clin. Transl. Neurol. 2016, 3, 21–26. [Google Scholar] [CrossRef]
- Shigekiyo, T.; Arawaka, S. Laterality of specific binding ratios on DAT-SPECT for differential diagnosis of degenerative parkinsonian syndromes. Sci. Rep. 2020, 10, 15761. [Google Scholar] [CrossRef]
- Nandhagopal, R.; Kuramoto, L.; Schulzer, M.; Mak, E.; Cragg, J.; Lee, C.S.; McKenzie, J.; McCormick, S.; Samii, A.; Troiano, A.; et al. Longitudinal progression of sporadic Parkinson’s disease: A multi-tracer positron emission tomography study. Brain 2009, 132, 2970–2979. [Google Scholar] [CrossRef] [PubMed]
- Surmeier, D.J.; Obeso, J.A.; Halliday, G.M. Selective neuronal vulnerability in Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, T.; Pagano, G.; Niccolini, F.; Politis, M. Predicting cognitive decline with non-clinical markers in Parkinson’s disease (PRECODE-2). J. Neurol. 2019, 266, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Colloby, S.J.; Williams, E.D.; Burn, D.J.; Lloyd, J.J.; McKeith, I.G.; O’Brien, J.T. Progression of dopaminergic degeneration in dementia with Lewy bodies and Parkinson’s disease with and without dementia assessed using 123I-FP-CIT SPECT. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 1176–1185. [Google Scholar] [CrossRef]
- Simuni, T.; Siderowf, A.; Lasch, S.; Coffey, C.S.; Caspell-Garcia, C.; Jennings, D.; Tanner, C.M.; Trojanowski, J.Q.; Shaw, L.M.; Seibyl, J.; et al. Longitudinal Change of Clinical and Biological Measures in Early Parkinson’s Disease: Parkinson’s Progression Markers Initiative Cohort. Mov. Disord. 2018, 33, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Sung, C.; Lee, J.H.; Oh, J.S.; Oh, M.; Lee, S.J.; Oh, S.J.; Chung, S.J.; Lee, C.S.; Kim, J.S. Longitudinal Decline of Striatal Subregional [18F]FP-CIT Uptake in Parkinson’s Disease. Nucl. Med. Mol. Imaging 2017, 51, 304–313. [Google Scholar] [CrossRef]
- Hilker, R.; Schweitzer, K.; Coburger, S.; Ghaemi, M.; Weisenbach, S.; Jacobs, A.H.; Rudolf, J.; Herholz, K.; Heiss, W.D. Nonlinear progression of Parkinson disease as determined by serial positron emission tomographic imaging of striatal fluorodopa F 18 activity. Arch. Neurol. 2005, 62, 378–382. [Google Scholar] [CrossRef]
- Vu, T.C.; Nutt, J.G.; Holford, N.H.G. Progression of motor and nonmotor features of Parkinson’s disease and their response to treatment. Br. J. Clin. Pharmacol. 2012, 74, 267–283. [Google Scholar] [CrossRef]
- Kordower, J.H.; Olanow, C.W.; Dodiya, H.B.; Chu, Y.; Beach, T.G.; Adler, C.H.; Halliday, G.M.; Bartus, R.T. Disease duration and the integrity of the nigrostriatal system in Parkinson’s disease. Brain 2013, 136, 2419–2431. [Google Scholar] [CrossRef]
- Kaasinen, V.; Vahlberg, T. Striatal dopamine in Parkinson disease: A meta-analysis of imaging studies. Ann. Neurol. 2017, 82, 873–882. [Google Scholar] [CrossRef]
- Djaldetti, R.; Lorberboym, M.; Karmon, Y.; Treves, T.A.; Ziv, I.; Melamed, E. Residual striatal dopaminergic nerve terminals in very long-standing Parkinson’s disease: A single photon emission computed tomography imaging study. Mov. Disord. 2011, 26, 327–330. [Google Scholar] [CrossRef]
- Greffard, S.; Verny, M.; Bonnet, A.M.; Beinis, J.Y.; Gallinari, C.; Meaume, S.; Piette, F.; Hauw, J.J.; Duyckaerts, C. Motor score of the unified Parkinson disease rating scale as a good predictor of lewy body-associated neuronal loss in the substantia nigra. Arch. Neurol. 2006, 63, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Samii, A.; Sossi, V.; Ruth, T.J.; Schulzer, M.; Holden, J.E.; Wudel, J.; Pal, P.K.; De La Fuente-Fernandez, R.; Calne, D.B.; et al. In vivo positron emission tomographic evidence for compensatory changes in presynaptic dopaminergic nerve terminals in Parkinson’s disease. Ann. Neurol. 2000, 47, 493–503. [Google Scholar] [CrossRef]
- Jiménez-Sánchez, L.; Blesa, J.; Del Rey, N.L.; Monje, M.H.G.; Obeso, J.A.; Cavada, C. Serotonergic innervation of the striatum in a nonhuman primate model of Parkinson’s disease. Neuropharmacology 2020, 170, 107806. [Google Scholar] [CrossRef] [PubMed]
- Kozina, E.A.; Kim, A.R.; Kurina, A.Y.; Ugrumov, M.V. Cooperative synthesis of dopamine by non-dopaminergic neurons as a compensatory mechanism in the striatum of mice with MPTP-induced Parkinsonism. Neurobiol. Dis. 2017, 98, 108–121. [Google Scholar] [CrossRef]
- Blesa, J.; Trigo-Damas, I.; Dileone, M.; del Rey, N.L.G.; Hernandez, L.F.; Obeso, J.A. Compensatory mechanisms in Parkinson’s disease: Circuits adaptations and role in disease modification. Exp. Neurol. 2017, 298, 148–161. [Google Scholar] [CrossRef]
- Adams, J.R.; Van Netten, H.; Schulzer, M.; Mak, E.; Mckenzie, J.; Strongosky, A.; Sossi, V.; Ruth, T.J.; Lee, C.S.; Farrer, M.; et al. PET in LRRK2 mutations: Comparison to sporadic Parkinson’s disease and evidence for presymptomatic compensation. Brain 2005, 128, 2777–2785. [Google Scholar] [CrossRef]
- Ceravolo, R.; Antonini, A.; Frosini, D.; De Iuliis, A.; Weis, L.; Cecchin, D.; Tosetti, M.; Bonuccelli, U.; Cosottini, M. Nigral anatomy and striatal denervation in genetic Parkinsonism: A family report. Mov. Disord. 2015, 30, 1148–1149. [Google Scholar] [CrossRef]
- De La Fuente-Fernández, R.; Schulzer, M.; Kuramoto, L.; Cragg, J.; Ramachandiran, N.; Au, W.L.; Mak, E.; McKenzie, J.; McCormick, S.; Sossi, V.; et al. Age-specific progression of nigrostriatal dysfunction in Parkinson’s disease. Ann. Neurol. 2011, 69, 803–810. [Google Scholar] [CrossRef]
- Sossi, V.; De La Fuente-Fernández, R.; Schulzer, M.; Adams, J.; Stoessl, J. Age-related differences in levodopa dynamics in Parkinson’s: Implications for motor complications. Brain 2006, 129, 1050–1058. [Google Scholar] [CrossRef]
- Sossi, V.; De La Fuente-Fernández, R.; Schulzer, M.; Troiano, A.R.; Ruth, T.J.; Stoessl, A.J. Dopamine transporter relation to dopamine turnover in Parkinson’s disease: A positron emission tomography study. Ann. Neurol. 2007, 62, 468–474. [Google Scholar] [CrossRef]
- Hong, J.Y.; Oh, J.S.; Lee, I.; Sunwoo, M.K.; Ham, J.H.; Lee, J.E.; Sohn, Y.H.; Kim, J.S.; Lee, P.H. Presynaptic dopamine depletion predicts levodopa-induced dyskinesia in de novo Parkinson disease. Neurology 2014, 82, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Palermo, G.; Giannoni, S.; Frosini, D.; Morganti, R.; Volterrani, D.; Bonuccelli, U.; Pavese, N.; Ceravolo, R. Dopamine Transporter, Age, and Motor Complications in Parkinson’s Disease: A Clinical and Single-Photon Emission Computed Tomography Study. Mov. Disord. 2020, 35, 1028–1036. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Schulzer, M.; De La Fuente-Fernandez, R.; Mak, E.; Kuramoto, L.; Sossi, V.; Ruth, T.J.; Calne, D.B.; Stoessl, A.J. Lack of regional selectivity during the progression of Parkinson disease: Implications for pathogenesis. Arch. Neurol. 2004, 61, 1920–1925. [Google Scholar] [CrossRef] [PubMed]
- Brooks, D.J. Molecular imaging of dopamine transporters. Ageing Res. Rev. 2016, 30, 114–121. [Google Scholar] [CrossRef]
- Palermo, G.; Ceravolo, R. Molecular Imaging of the Dopamine Transporter. Cells 2019, 8, 872. [Google Scholar] [CrossRef] [PubMed]
- Colloby, S.J.; McParland, S.; O’Brien, J.T.; Attems, J. Neuropathological correlates of dopaminergic imaging in Alzheimer’s disease and Lewy body dementias. Brain 2012, 135, 2798–2808. [Google Scholar] [CrossRef]
- Kraemmer, J.; Kovacs, G.G.; Perju-Dumbrava, L.; Pirker, S.; Traub-Weidinger, T.; Pirker, W. Correlation of striatal dopamine transporter imaging with post mortem substantia nigra cell counts. Mov. Disord. 2014, 29, 1767–1773. [Google Scholar] [CrossRef]
- Karimi, M.; Tian, L.; Brown, C.A.; Flores, H.P.; Loftin, S.K.; Videen, T.O.; Moerlein, S.M.; Perlmutter, J.S. Validation of nigrostriatal positron emission tomography measures: Critical limits. Ann. Neurol. 2013, 73, 390–396. [Google Scholar] [CrossRef]
- Brown, C.A.; Karimi, M.K.; Tian, L.; Flores, H.; Su, Y.; Tabbal, S.D.; Loftin, S.K.; Moerlein, S.M.; Perlmutter, J.S. Validation of midbrain positron emission tomography measures for nigrostriatal neurons in macaques. Ann. Neurol. 2013, 74, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Saari, L.; Kivinen, K.; Gardberg, M.; Joutsa, J.; Noponen, T.; Kaasinen, V. Dopamine transporter imaging does not predict the number of nigral neurons in Parkinson disease. Neurology 2017, 88, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Honkanen, E.A.; Saari, L.; Orte, K.; Gardberg, M.; Noponen, T.; Joutsa, J.; Kaasinen, V. No link between striatal dopaminergic axons and dopamine transporter imaging in Parkinson’s disease. Mov. Disord. 2019, 34, 1562–1566. [Google Scholar] [CrossRef] [PubMed]
- Perlmutter, J.S.; Stoessl, A.J. Striatal DAT SPECT: Caveat Emptor! Mov. Disord. 2019, 34, 1430–1432. [Google Scholar] [CrossRef]
- Pifl, C. The time delay between in vivo imaging and postmortem data poses a caveat on “no link” findings. Mov. Disord. 2019, 34, 1579–1580. [Google Scholar] [CrossRef]
- Frosini, D.; Cosottini, M.; Volterrani, D.; Ceravolo, R. Neuroimaging in Parkinson’s disease: Focus on substantia nigra and nigro-striatal projection. Curr. Opin. Neurol. 2017, 30, 416–426. [Google Scholar] [CrossRef]
- Fabbri, M.; Reimão, S.; Carvalho, M.; Nunes, R.G.; Abreu, D.; Guedes, L.C.; Bouça, R.; Lobo, P.P.; Godinho, C.; Coelho, M.; et al. Substantia Nigra Neuromelanin as an Imaging Biomarker of Disease Progression in Parkinson’s Disease. J. Park. Dis. 2017, 7, 491–501. [Google Scholar] [CrossRef]
- Isaias, I.U.; Trujillo, P.; Summers, P.; Marotta, G.; Mainardi, L.; Pezzoli, G.; Zecca, L.; Costa, A. Neuromelanin imaging and dopaminergic loss in parkinson’s disease. Front. Aging Neurosci. 2016, 8, 196. [Google Scholar] [CrossRef]
- Kuya, K.; Shinohara, Y.; Miyoshi, F.; Fujii, S.; Tanabe, Y.; Ogawa, T. Correlation between neuromelanin-sensitive MR imaging and 123I-FP-CIT SPECT in patients with parkinsonism. Neuroradiology 2016, 58, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Martín-Bastida, A.; Lao-Kaim, N.P.; Roussakis, A.A.; Searle, G.E.; Xing, Y.; Gunn, R.N.; Schwarz, S.T.; Barker, R.A.; Auer, D.P.; Piccini, P. Relationship between neuromelanin and dopamine terminals within the Parkinson’s nigrostriatal system. Brain 2019, 142, 2023–2036. [Google Scholar] [CrossRef] [PubMed]
- Okuzumi, A.; Hatano, T.; Kamagata, K.; Hori, M.; Mori, A.; Oji, Y.; Taniguchi, D.; Daida, K.; Shimo, Y.; Yanagisawa, N.; et al. Neuromelanin or DaT-SPECT: Which is the better marker for discriminating advanced Parkinson’s disease? Eur. J. Neurol. 2019, 26, 1408–1416. [Google Scholar] [CrossRef]
- Tabbal, S.D.; Tian, L.L.; Karimi, M.; Brown, C.A.; Loftin, S.K.; Perlmutter, J.S. Low nigrostriatal reserve for motor parkinsonism in nonhuman primates. Exp. Neurol. 2012, 237, 355–362. [Google Scholar] [CrossRef]
- Fazio, P.; Svenningsson, P.; Cselényi, Z.; Halldin, C.; Farde, L.; Varrone, A. Nigrostriatal dopamine transporter availability in early Parkinson’s disease. Mov. Disord. 2018, 33, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, S.P.; Presotto, L.; Baroncini, D.; Garibotto, V.; Moresco, R.M.; Gianolli, L.; Volonté, M.A.; Antonini, A.; Perani, D. Axonal damage and loss of connectivity in nigrostriatal and mesolimbic dopamine pathways in early Parkinson’s disease. NeuroImage Clin. 2017, 14, 734–740. [Google Scholar] [CrossRef]
- Hsiao, I.T.; Weng, Y.H.; Hsieh, C.J.; Lin, W.Y.; Wey, S.P.; Kung, M.P.; Yen, T.C.; Lu, C.S.; Lin, K.J. Correlation of parkinson disease severity and 18F-DTBZ positron emission tomography. JAMA Neurol. 2014, 71, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Fazio, P.; Svenningsson, P.; Forsberg, A.; Jönsson, E.G.; Amini, N.; Nakao, R.; Nag, S.; Halldin, C.; Farde, L.; Varrone, A. Quantitative analysis of 18F-(E)-N-(3-iodoprop-2-enyl)-2β-carbofluoroethoxy-3β-(4′-methyl-phenyl) nortropane binding to the dopamine transporter in Parkinson disease. J. Nucl. Med. 2015, 56, 714–720. [Google Scholar] [CrossRef]
- Tagliaferro, P.; Burke, R.E. Retrograde Axonal Degeneration in Parkinson Disease. J. Park. Dis. 2016, 6, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.C.; Luk, K.; Purtell, K.; Burke Nanni, S.; Stoessl, A.J.; Trudeau, L.E.; Yue, Z.; Krainc, D.; Oertel, W.; Obeso, J.A.; et al. Neuronal vulnerability in Parkinson disease: Should the focus be on axons and synaptic terminals? Mov. Disord. 2019, 34, 1406–1422. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, N.; Hauser, R.A.; Grachev, I.D. Clinical utility of dopamine transporter single photon emission CT (DaT-SPECT) with (123I) ioflupane in diagnosis of parkinsonian syndromes. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1288–1295. [Google Scholar] [CrossRef]
- Catafau, A.M.; Tolosa, E.; Laloux, P.; Vander Borght, T.; Van Zandijcke, M.; De Geeter, F.; Destee, A.; Steinling, M.; Lacomblez, L.; Habert, M.O.; et al. Impact of dopamine transporter SPECT using 123I-Ioflupane on diagnosis and management of patients with clinically uncertain parkinsonian syndromes. Mov. Disord. 2004, 19, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Bega, D.; Kuo, P.H.; Chalkidou, A.; Grzeda, M.T.; Macmillan, T.; Brand, C.; Sheikh, Z.H.; Antonini, A. Clinical utility of DaTscan in patients with suspected Parkinsonian syndrome: A systematic review and meta-analysis. NPJ Park. Dis. 2021, 7. [Google Scholar] [CrossRef]
- Tolosa, E.; Garrido, A.; Scholz, S.W.; Poewe, W. Challenges in the diagnosis of Parkinson’s disease. Lancet Neurol. 2021, 20, 385–397. [Google Scholar] [CrossRef]
- Ceravolo, R.; Antonini, A.; Volterrani, D.; Rossi, C.; Kiferle, L.; Frosini, D.; Lucetti, C.; Isaias, I.U.; Benti, R.; Murri, L.; et al. Predictive value of nigrostriatal dysfunction in isolated tremor: A clinical and SPECT study. Mov. Disord. 2008, 23, 2049–2054. [Google Scholar] [CrossRef]
- Isaias, I.U.; Canesi, M.; Benti, R.; Gerundini, P.; Cilia, R.; Pezzoli, G.; Antonini, A. Striatal dopamine transporter abnormalities in patients with essential tremor. Nucl. Med. Commun. 2008, 29, 349–353. [Google Scholar] [CrossRef]
- Benamer, H.T.S.; Patterson, J.; Grosset, D.G.; Booij, J.; De Bruin, K.; Van Royen, E.; Speelman, J.D.; Horstink, M.H.I.M.; Sips, H.J.W.A.; Dierckx, R.A.; et al. Accurate differentiation of parkinsonism and essential tremor using visual assessment of [123I]-FP-CIT SPECT imaging: The [123I]-FP-CIT study group. Mov. Disord. 2000, 15, 503–510. [Google Scholar] [CrossRef]
- Antonini, A.; Berto, P.; Lopatriello, S.; Tamma, F.; Annemans, L.; Chambers, M. Cost-effectiveness of 123I-FP-CIT SPECT in the differential diagnosis of essential tremor and Parkinson’s disease in Italy. Mov. Disord. 2008, 23, 2202–2209. [Google Scholar] [CrossRef]
- Thobois, S.; Prange, S.; Scheiber, C.; Broussolle, E. What a neurologist should know about PET and SPECT functional imaging for parkinsonism: A practical perspective. Park. Relat. Disord. 2019, 59, 93–100. [Google Scholar] [CrossRef]
- Benítez-Rivero, S.; Marín-Oyaga, V.A.; García-Solís, D.; Huertas-Fernández, I.; García-Gomez, F.J.; Jesus, S.; Caceres, M.T.; Carrillo, F.; Ortiz, A.M.; Carballo, M.; et al. Clinical features and 123I-FP-CIT SPECT imaging in vascular parkinsonism and Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2013, 84, 122–129. [Google Scholar] [CrossRef]
- Ma, K.K.Y.; Lin, S.; Mok, V.C.T. Neuroimaging in Vascular Parkinsonism. Curr. Neurol. Neurosci. Rep. 2019, 19. [Google Scholar] [CrossRef]
- Kalra, S.; Grosset, D.G.; Benamer, H.T.S. Differentiating vascular parkinsonism from idiopathic Parkinson’s disease: A systematic review. Mov. Disord. 2010, 25, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Funke, E.; Kupsch, A.; Buchert, R.; Brenner, W.; Plotkin, M. Impact of subcortical white matter lesions on dopamine transporter SPECT. J. Neural Transm. 2013, 120, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Antonini, A.; Vitale, C.; Barone, P.; Cilia, R.; Righini, A.; Bonuccelli, U.; Abbruzzese, G.; Ramat, S.; Petrone, A.; Quatrale, R.; et al. The relationship between cerebral vascular disease and parkinsonism: The VADO study. Park. Relat. Disord. 2012, 18, 775–780. [Google Scholar] [CrossRef]
- Factor, S.A.; Burkhard, P.R.; Caroff, S.; Friedman, J.H.; Marras, C.; Tinazzi, M.; Comella, C.L. Recent developments in drug-induced movement disorders: A mixed picture. Lancet Neurol. 2019, 18, 880–890. [Google Scholar] [CrossRef]
- Tinazzi, M.; Cipriani, A.; Matinella, A.; Cannas, A.; Solla, P.; Nicoletti, A.; Zappia, M.; Morgante, L.; Morgante, F.; Pacchetti, C.; et al. [123I]FP-CIT single photon emission computed tomography findings in drug-induced Parkinsonism. Schizophr. Res. 2012, 139, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Tinazzi, M.; Morgante, F.; Matinella, A.; Bovi, T.; Cannas, A.; Solla, P.; Marrosu, F.; Nicoletti, A.; Zappia, M.; Luca, A.; et al. Imaging of the dopamine transporter predicts pattern of disease progression and response to levodopa in patients with schizophrenia and parkinsonism: A 2-year follow-up multicenter study. Schizophr. Res. 2014, 152, 344–349. [Google Scholar] [CrossRef]
- Brigo, F.; Erro, R.; Marangi, A.; Bhatia, K.; Tinazzi, M. Differentiating drug-induced parkinsonism from Parkinson’s disease: An update on non-motor symptoms and investigations. Park. Relat. Disord. 2014, 20, 808–814. [Google Scholar] [CrossRef]
- Erro, R.; Bhatia, K.P.; Tinazzi, M. Parkinsonism following neuroleptic exposure: A double-hit hypothesis? Mov. Disord. 2015, 30, 780–785. [Google Scholar] [CrossRef]
- Shuaib, U.A.; Rajput, A.H.; Robinson, C.A.; Rajput, A. Neuroleptic-induced Parkinsonism: Clinicopathological study. Mov. Disord. 2016, 31, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.Y.; Sunwoo, M.K.; Oh, J.S.; Kim, J.S.; Sohn, Y.H.; Lee, P.H. Persistent drug-induced parkinsonism in patients with normal dopamine transporter imaging. PLoS ONE 2016, 11, e157410. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.J.; Yoo, H.S.; Moon, H.; Oh, J.S.; Kim, J.S.; Park, Y.H.; Hong, J.Y.; Ye, B.S.; Sohn, Y.H.; Lee, P.H. Early-onset drug-induced parkinsonism after exposure to offenders implies nigrostriatal dopaminergic dysfunction. J. Neurol. Neurosurg. Psychiatry 2018, 89, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Cho, H.; Kim, Y.J.; Ma, H.I.; Jang, S. Drug-induced Parkinsonism: A strong predictor of idiopathic Parkinson’s disease. PLoS ONE 2021, 16, e247354. [Google Scholar] [CrossRef]
- O’Brien, J.T.; McKeith, I.G.; Walker, Z.; Tatsch, K.; Booij, J.; Darcourt, J.; Marquardt, M.; Reininger, C. Diagnostic accuracy of 123I-FP-CIT SPECT in possible dementia with Lewy bodies. Br. J. Psychiatry 2009, 194, 34–39. [Google Scholar] [CrossRef]
- Oliveira, F.P.M.; Walker, Z.; Walker, R.W.H.; Attems, J.; Castanheira, J.C.; Silva, Â.; Oliveira, C.; Vaz, S.; Silva, M.; Costa, D.C. 123I-FP-CIT SPECT in dementia with Lewy bodies, Parkinson’s disease and Alzheimer’s disease: A new quantitative analysis of autopsy confirmed cases. J. Neurol. Neurosurg. Psychiatry 2021, 92, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Mccleery, J.; Morgan, S.; Hyde, C.; Bradley, K.; Ansorge, O. Dopamine transporter imaging for the diagnosis of dementia with Lewy bodies. Cochrane Database Syst. Rev. 2015, 1, CD010633. [Google Scholar] [CrossRef]
- Saeed, U.; Compagnone, J.; Aviv, R.I.; Strafella, A.P.; Black, S.E.; Lang, A.E.; Masellis, M. Imaging biomarkers in Parkinson’s disease and Parkinsonian syndromes: Current and emerging concepts. Transl. Neurodegener. 2017, 6, 8. [Google Scholar] [CrossRef]
- Morgan, S.; Kemp, P.; Booij, J.; Costa, D.C.; Padayachee, S.; Lee, L.; Barber, C.; Carter, J.; Walker, Z. Differentiation of frontotemporal dementia from dementia with Lewy bodies using FP-CIT SPECT. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1063–1070. [Google Scholar] [CrossRef]
- Sestini, S.; Alongi, P.; Berti, V.; Calcagni, M.L.; Cecchin, D.; Chiaravalloti, A.; Chincarini, A.; Cistaro, A.; Guerra, U.P.; Pappatà, S.; et al. Correction to: The role of molecular imaging in the frame of the revised dementia with Lewy body criteria (Clinical and Translational Imaging, (2019), 7, 2, (83-98), 10.1007/s40336-019-00321-8). Clin. Transl. Imaging 2019, 7, 231. [Google Scholar] [CrossRef]
- van der Zande, J.J.; Booij, J.; Scheltens, P.; Raijmakers, P.G.H.M.; Lemstra, A.W. [123]FP-CIT SPECT scans initially rated as normal became abnormal over time in patients with probable dementia with Lewy bodies. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1060–1066. [Google Scholar] [CrossRef]
- Cilia, R.; Rossi, C.; Frosini, D.; Volterrani, D.; Siri, C.; Pagni, C.; Benti, R.; Pezzoli, G.; Bonuccelli, U.; Antonini, A.; et al. Dopamine transporter spect imaging in corticobasal syndrome. PLoS ONE 2011, 6, e018301. [Google Scholar] [CrossRef] [PubMed]
- Ceravolo, R.; Rossi, C.; Cilia, R.; Tognoni, G.; Antonini, A.; Volterrani, D.; Bonuccelli, U. Evidence of delayed nigrostriatal dysfunction in corticobasal syndrome: A SPECT follow-up study. Park. Relat. Disord. 2013, 19, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Pirker, S.; Perju-Dumbrava, L.; Kovacs, G.G.; Traub-Weidinger, T.; Pirker, W. Progressive dopamine transporter binding loss in autopsy-confirmed Corticobasal Degeneration. J. Park. Dis. 2015, 5, 907–912. [Google Scholar] [CrossRef]
- Rodriguez-Porcel, F.; Jamali, S.; Duker, A.P.; Espay, A.J. Dopamine transporter scanning in the evaluation of patients with suspected Parkinsonism: A case-based user’s guide. Expert Rev. Neurother. 2016, 16, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Isaacson, S.H.; Fisher, S.; Gupta, F.; Hermanowicz, N.; Kremens, D.E.; Lew, M.F.; Marek, K.; Pahwa, R.; Russell, D.S.; Seibyl, J. Clinical utility of DaTscanTM imaging in the evaluation of patients with parkinsonism: A US perspective. Expert Rev. Neurother. 2017, 17, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Ba, F.; Martin, W.R.W. Dopamine transporter imaging as a diagnostic tool for parkinsonism and related disorders in clinical practice. Park. Relat. Disord. 2015, 21, 87–94. [Google Scholar] [CrossRef]
- Isaacson, J.R.; Brillman, S.; Chhabria, N.; Isaacson, S.H. Impact of DaTscan Imaging on Clinical Decision Making in Clinically Uncertain Parkinson’s Disease. J. Park. Dis. 2021, 11, 885–889. [Google Scholar] [CrossRef]
- Jaakkola, E.; Joutsa, J.; Kaasinen, V. Predictors of normal and abnormal outcome in clinical brain dopamine transporter imaging. J. Neural Transm. 2016, 123, 205–209. [Google Scholar] [CrossRef]
- Perlmutter, J.S.; Norris, S.A. Neuroimaging biomarkers for Parkinson disease: Facts and fantasy. Ann. Neurol. 2014, 76, 769–783. [Google Scholar] [CrossRef]
- Marek, K.L.; Seibyl, J.P.; Zoghbi, S.S.; Zea-Ponce, Y.; Baldwin, R.M.; Fussell, B.; Charney, D.S.; Van Dyck, C.; Hoffer, P.B.; Innis, R.B. [123I]β-CIT/SPECT imaging demonstrates bilateral loss of dopamine transporters in hemi-Parkinson’s disease. Neurology 1996, 46, 231–237. [Google Scholar] [CrossRef]
- Oakes, D.; Shoulson, I.; Kieburtz, K.; Rudolph, A.; Lang, A.; Olanow, C.W.; Tanner, C.; Marek, K.; Parkinson Study Group. F.S. Levodopa and the progression of Parkinson’s disease. N. Engl. J. Med. 2004, 9, 2498–2508. [Google Scholar] [CrossRef]
- Marshall, V.L.; Patterson, J.; Hadley, D.M.; Grosset, K.A.; Grosset, D.G. Two-year follow-up in 150 consecutive cases with normal dopamine transporter imaging. Nucl. Med. Commun. 2006, 27, 933–937. [Google Scholar] [CrossRef]
- Schneider, S.A.; Edwards, M.J.; Mir, P.; Cordivari, C.; Hooker, J.; Dickson, J.; Quinn, N.; Bhatia, K.P. Patients with adult-onset dystonic tremor resembling Parkinsonian tremor have scans without evidence of dopaminergic deficit (SWEDDs). Mov. Disord. 2007, 22, 2210–2215. [Google Scholar] [CrossRef] [PubMed]
- Marek, K.; Seibyl, J.; Eberly, S.; Oakes, D.; Shoulson, I.; Lang, A.E.; Hyson, C.; Jennings, D. Longitudinal follow-up of SWEDD subjects in the PRECEPT Study. Neurology 2014, 82, 1791–1797. [Google Scholar] [CrossRef]
- Nicastro, N.; Garibotto, V.; Badoud, S.; Burkhard, P.R. Scan without evidence of dopaminergic deficit: A 10-year retrospective study. Park. Relat. Disord. 2016, 31, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Suwijn, S.R.; Verschuur, C.V.M.; Slim, M.A.; Booij, J.; de Bie, R.M.A. Reliability of visual assessment by non-expert nuclear medicine physicians and appropriateness of indications of [123I]FP-CIT SPECT imaging by neurologists in patients with early drug-naive Parkinson’s disease. EJNMMI Res. 2019, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Sixel-Döring, F.; Liepe, K.; Mollenhauer, B.; Trautmann, E.; Trenkwalder, C. The role of 123I-FP-CIT-SPECT in the differential diagnosis of Parkinson and tremor syndromes: A critical assessment of 125 cases. J. Neurol. 2011, 258, 2147–2154. [Google Scholar] [CrossRef]
- Batla, A.; Erro, R.; Stamelou, M.; Schneider, S.A.; Schwingenschuh, P.; Ganos, C.; Bhatia, K.P. Patients with scans without evidence of dopaminergic deficit: A long-term follow-up study. Mov. Disord. 2014, 29, 1820–1825. [Google Scholar] [CrossRef]
- Menéndez-González, M.; Tavares, F.; Zeidan, N.; Salas-Pacheco, J.M.; Arias-Carrión, O. Diagnoses behind patients with hard-to-classify tremor and normal DaT-SPECT: A clinical follow up study. Front. Aging Neurosci. 2014, 6, 56. [Google Scholar] [CrossRef]
- Erro, R.; Schneider, S.A.; Stamelou, M.; Quinn, N.P.; Bhatia, K.P. What do patients with scans without evidence of dopaminergic deficit (SWEDD) have? New evidence and continuing controversies. J. Neurol. Neurosurg. Psychiatry 2016, 87, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Wile, D.J.; Agarwal, P.A.; Schulzer, M.; Mak, E.; Dinelle, K.; Shahinfard, E.; Vafai, N.; Hasegawa, K.; Zhang, J.; McKenzie, J.; et al. Serotonin and dopamine transporter PET changes in the premotor phase of LRRK2 parkinsonism: Cross-sectional studies. Lancet Neurol. 2017, 16, 351–359. [Google Scholar] [CrossRef]
- Erro, R.; Bhatia, K.P. Novel movement disorder society-Parkinson’s disease criteria: What about SWEDD and genetic forms? Mov. Disord. 2016, 31, 431. [Google Scholar] [CrossRef] [PubMed]
- Sprenger, F.S.; Seppi, K.; Djamshidian, A.; Reiter, E.; Nocker, M.; Mair, K.; Göbel, G.; Poewe, W. Nonmotor Symptoms in Subjects Without Evidence of Dopaminergic Deficits. Mov. Disord. 2015, 30, 976–981. [Google Scholar] [CrossRef]
- Taylor, S.; Gafton, J.; Shah, B.; Pagano, G.; Chaudhuri, K.R.; Brooks, D.J.; Pavese, N. Progression of nonmotor symptoms in subgroups of patients with non-dopamine-deficient Parkinsonism. Mov. Disord. 2016, 31, 344–351. [Google Scholar] [CrossRef]
- Wyman-Chick, K.A.; Martin, P.K.; Minár, M.; Schroeder, R.W. Cognition in Patients with a Clinical Diagnosis of Parkinson Disease and Scans Without Evidence of Dopaminergic Deficit (SWEDD): 2-Year Follow-Up. Cogn. Behav. Neurol. 2016, 29, 190–196. [Google Scholar] [CrossRef]
- Jackson, L.; Turcano, P.; Stitt, D.; Coon, E.; Savica, R. Autonomic Testing Profiles in Scans without Evidence of Dopaminergic Deficit (SWEDD). J. Park. Dis. 2020, 10, 945–949. [Google Scholar] [CrossRef]
- Lee, J.W.; Song, Y.S.; Kim, H.; Ku, B.D.; Lee, W.W. Patients with scans without evidence of dopaminergic deficit (SWEDD) do not have early Parkinson’s disease: Analysis of the PPMI data. PLoS ONE 2021, 16, e246881. [Google Scholar] [CrossRef]
- Oh, Y.S.; Choi, J.H.; Kwon, D.Y. Classification of Scans Without Evidence of Dopamine Deficit (SWEDD) According to the Olfactory Function. J. Park. Dis. 2016, 6, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Silveira-Moriyama, L.; Birchall, J.; Bain, P.; Lees, A.J.; Bajaj, N.P.S. Hyposmia in SWEDD. Mov. Disord. 2015, 30, 1436–1437. [Google Scholar] [CrossRef]
- Conrado, D.J.; Nicholas, T.; Tsai, K.; Macha, S.; Sinha, V.; Stone, J.; Corrigan, B.; Bani, M.; Muglia, P.; Watson, I.A.; et al. Dopamine Transporter Neuroimaging as an Enrichment Biomarker in Early Parkinson’s Disease Clinical Trials: A Disease Progression Modeling Analysis. Clin. Transl. Sci. 2018, 11, 63–70. [Google Scholar] [CrossRef]
- Massa, J.; Chahine, L.M. Revision of Diagnosis in Early Parkinsonism with Abnormal Dopamine Transporter Imaging. J. Park. Dis. 2019, 9, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Romero, K.; Conrado, D.; Burton, J.; Nicholas, T.; Sinha, V.; Macha, S.; Ahamadi, M.; Cedarbaum, J.; Seibyl, J.; Marek, K.; et al. Molecular Neuroimaging of the Dopamine Transporter as a Patient Enrichment Biomarker for Clinical Trials for Early Parkinson’s Disease. Clin. Transl. Sci. 2019, 12, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Fearnley, J.M.; Lees, A.J. Ageing and parkinson’s disease: Substantia nigra regional selectivity. Brain 1991, 114, 2283–2301. [Google Scholar] [CrossRef] [PubMed]
- Stiasny-Kolster, K.; Doerr, Y.; Möller, J.C.; Höffken, H.; Behr, T.M.; Oertel, W.H.; Mayer, G. Combination of “idiopathic” REM sleep behaviour disorder and olfactory dysfunction as possible indicator for α-synucleinopathy demonstrated by dopamine transporter FP-CIT-SPECT. Brain 2005, 128, 126–137. [Google Scholar] [CrossRef]
- Bonifati, V. Genetics of Parkinson’s disease—State of the art, 2013. Park. Relat. Disord. 2014, 20, S23–S28. [Google Scholar] [CrossRef]
- Stoessl, A.J. Positron emission tomography in premotor Parkinson’s disease. Park. Relat. Disord. 2007, 13, 421–424. [Google Scholar] [CrossRef]
- Iranzo, A.; Tolosa, E.; Gelpi, E.; Molinuevo, J.L.; Valldeoriola, F.; Serradell, M.; Sanchez-Valle, R.; Vilaseca, I.; Lomeña, F.; Vilas, D.; et al. Neurodegenerative disease status and post-mortem pathology in idiopathic rapid-eye-movement sleep behaviour disorder: An observational cohort study. Lancet Neurol. 2013, 12, 443–453. [Google Scholar] [CrossRef]
- Bauckneht, M.; Chincarini, A.; De Carli, F.; Terzaghi, M.; Morbelli, S.; Nobili, F.; Arnaldi, D. Presynaptic dopaminergic neuroimaging in REM sleep behavior disorder: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 41, 266–274. [Google Scholar] [CrossRef]
- Iranzo, A.; Lomeña, F.; Stockner, H.; Valldeoriola, F.; Vilaseca, I.; Salamero, M.; Molinuevo, J.L.; Serradell, M.; Duch, J.; Pavía, J.; et al. Decreased striatal dopamine transporter uptake and substantia nigra hyperechogenicity as risk markers of synucleinopathy in patients with idiopathic rapid-eye-movement sleep behaviour disorder: A prospective study. Lancet Neurol. 2010, 9, 1070–1077. [Google Scholar] [CrossRef]
- Iranzo, A.; Valldeoriola, F.; Lomeña, F.; Molinuevo, J.L.; Serradell, M.; Salamero, M.; Cot, A.; Ros, D.; Pavía, J.; Santamaria, J.; et al. Serial dopamine transporter imaging of nigrostriatal function in patients with idiopathic rapid-eye-movement sleep behaviour disorder: A prospective study. Lancet Neurol. 2011, 10, 797–805. [Google Scholar] [CrossRef]
- Iranzo, A.; Santamaría, J.; Valldeoriola, F.; Serradell, M.; Salamero, M.; Gaig, C.; Niñerola-Baizán, A.; Sánchez-Valle, R.; Lladó, A.; De Marzi, R.; et al. Dopamine transporter imaging deficit predicts early transition to synucleinopathy in idiopathic rapid eye movement sleep behavior disorder. Ann. Neurol. 2017, 82, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Lao-Kaim, N.P.; Roussakis, A.A.; Martín-Bastida, A.; Valle-Guzman, N.; Paul, G.; Loane, C.; Widner, H.; Politis, M.; Foltynie, T.; et al. 11 C-PE2I and 18 F-Dopa PET for assessing progression rate in Parkinson’s: A longitudinal study. Mov. Disord. 2018, 33, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Iranzo, A.; Hu, M.; Högl, B.; Boeve, B.F.; Manni, R.; Oertel, W.H.; Arnulf, I.; Ferini-Strambi, L.; Puligheddu, M.; et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: A multicentre study. Brain 2019, 142, 744–759. [Google Scholar] [CrossRef] [PubMed]
- Chahine, L.M.; Brumm, M.C.; Caspell-Garcia, C.; Oertel, W.; Mollenhauer, B.; Amara, A.; Fernandez-Arcos, A.; Tolosa, E.; Simonet, C.; Hogl, B.; et al. Dopamine transporter imaging predicts clinically-defined α-synucleinopathy in REM sleep behavior disorder. Ann. Clin. Transl. Neurol. 2021, 8, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Arnaldi, D.; Chincarini, A.; Hu, M.T.; Sonka, K.; Boeve, B.; Miyamoto, T.; Puligheddu, M.; De Cock, V.C.; Terzaghi, M.; Plazzi, G.; et al. Dopaminergic imaging and clinical predictors for phenoconversion of REM sleep behaviour disorder. Brain 2021, 144, 278–287. [Google Scholar] [CrossRef]
- Berendse, H.W.; Booij, J.; Francot, C.M.J.E.; Bergmans, P.L.M.; Hijman, R.; Stoof, J.C.; Wolters, E.C. Subclinical dopaminergic dysfunction in asymptomatic Parkinson’s disease patients’ relatives with a decreased sense of smell. Ann. Neurol. 2001, 50, 34–41. [Google Scholar] [CrossRef]
- Ponsen, M.M.; Stoffers, D.; Booij, J.; Van Eck-Smit, B.L.F.; Wolters, E.C.; Berendse, H.W. Idiopathic hyposmia as a preclinical sign of Parkinson’s disease. Ann. Neurol. 2004, 56, 173–181. [Google Scholar] [CrossRef]
- Jennings, D.; Siderowf, A.; Stern, M.; Seibyl, J.; Eberly, S.; Oakes, D.; Marek, K. Imaging prodromal Parkinson disease: The Parkinson associated risk syndrome study. Neurology 2014, 83, 1739–1746. [Google Scholar] [CrossRef]
- Jennings, D.; Siderowf, A.; Stern, M.; Seibyl, J.; Eberly, S.; Oakes, D.; Marek, K. Conversion to Parkinson disease in the PARS hyposmic and dopamine transporter-deficit prodromal cohort. JAMA Neurol. 2017, 74, 933–940. [Google Scholar] [CrossRef]
- Siderowf, A.; Jennings, D.; Stern, M.; Seibyl, J.; Eberly, S.; Oakes, D.; Marek, K.; Jennings, D.; Marek, K.; Seibyl, J.; et al. Clinical and Imaging Progression in the PARS Cohort: Long-Term Follow-up. Mov. Disord. 2020, 35, 1550–1557. [Google Scholar] [CrossRef]
- Noyce, A.J.; Dickson, J.; Rees, R.N.; Bestwick, J.P.; Isaias, I.U.; Politis, M.; Giovannoni, G.; Warner, T.T.; Lees, A.J.; Schrag, A. Dopamine reuptake transporter–single-photon emission computed tomography and transcranial sonography as imaging markers of prediagnostic Parkinson’s disease. Mov. Disord. 2018, 33, 478–482. [Google Scholar] [CrossRef]
- Chung, S.J.; Yoo, H.S.; Lee, Y.H.; Sohn, Y.H.; Ye, B.S.; Cha, J.; Lee, P.H. Minimal parkinsonism in the elderly is associated with striatal dopamine loss and pontine structural damage. Park. Relat. Disord. 2020, 81, 140–143. [Google Scholar] [CrossRef]
- Piccini, P.; Burn, D.J.; Ceravolo, R.; Maraganore, D.; Brooks, D.J. The role of inheritance in sporadic Parkinson’s disease: Evidence from a longitudinal study of dopaminergic function in twins. Ann. Neurol. 1999, 45, 577–582. [Google Scholar] [CrossRef]
- Varrone, A.; Pellecchia, M.T. SPECT Molecular Imaging in Familial Parkinson’s Disease, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2018; Volume 142, ISBN 9780128151419. [Google Scholar]
- Ricciardi, L.; Petrucci, S.; Di Giuda, D.; Serra, L.; Spanò, B.; Sensi, M.; Ginevrino, M.; Cocciolillo, F.; Bozzali, M.; Valente, E.M.; et al. The Contursi Family 20 Years Later: Intrafamilial Phenotypic Variability of the SNCA p.A53T Mutation. Mov. Disord. 2016, 31, 257–258. [Google Scholar] [CrossRef]
- Sierra, M.; Sánchez-Juan, P.; Martínez-Rodríguez, M.I.; González-Aramburu, I.; García-Gorostiaga, I.; Quirce, M.R.; Infante, J.C. Olfaction and imaging biomarkers in premotor LRRK2 G2019S-associated Parkinson disease. Neurology 2013, 80, 621–626. [Google Scholar] [CrossRef]
- Vilas, D.; Ispierto, L.; Álvarez, R.; Pont-Sunyer, C.; Martí, M.J.; Valldeoriola, F.; Compta, Y.; de Fabregues, O.; Hernández-Vara, J.; Puente, V.; et al. Clinical and imaging markers in premotor LRRK2 G2019S mutation carriers. Park. Relat. Disord. 2015, 21, 1170–1176. [Google Scholar] [CrossRef]
- Artzi, M.; Even-Sapir, E.; Shacham, H.L.; Thaler, A.; Urterger, A.O.; Bressman, S.; Marder, K.; Hendler, T.; Giladi, N.; Bashat, D.B.; et al. DaT-SPECT assessment depicts Dopamine depletion among asymptomatic G2019S LRRK2 mutation carriers. PLoS ONE 2017, 12, e175424. [Google Scholar] [CrossRef] [PubMed]
- Bergareche, A.; Rodríguez-Oroz, M.C.; Estanga, A.; Gorostidi, A.; López de Munain, A.; Castillo-Triviño, T.; Ruiz-Martínez, J.; Mondragón, E.; Gaig, C.; Lomeña, F.; et al. DAT imaging and clinical biomarkers in relatives at genetic risk for LRRK2R1441G Parkinson’s disease. Mov. Disord. 2016, 31, 335–343. [Google Scholar] [CrossRef]
- Sierra, M.; González-Aramburu, I.; Sánchez-Juan, P.; Sánchez-Quintana, C.; Polo, J.M.; Berciano, J.; Combarros, O.; Infante, J. High frequency and reduced penetrance of lRRK2 g2019S mutation among Parkinson’s disease patients in Cantabria (Spain). Mov. Disord. 2011, 26, 2343–2346. [Google Scholar] [CrossRef] [PubMed]
- Sierra, M.; Martínez-Rodríguez, I.; Sánchez-Juan, P.; González-Aramburu, I.; Jiménez-Alonso, M.; Sánchez-Rodríguez, A.; Berciano, J.; Banzo, I.; Infante, J. Prospective clinical and DaT-SPECT imaging in premotor LRRK2 G2019S-Associated Parkinson disease. Neurology 2017, 89, 439–444. [Google Scholar] [CrossRef]
- Simuni, T.; Uribe, L.; Cho, H.R.; Caspell-Garcia, C.; Coffey, C.S.; Siderowf, A.; Trojanowski, J.Q.; Shaw, L.M.; Seibyl, J.; Singleton, A.; et al. Clinical and dopamine transporter imaging characteristics of non-manifest LRRK2 and GBA mutation carriers in the Parkinson’s Progression Markers Initiative (PPMI): A cross-sectional study. Lancet Neurol. 2020, 19, 71–80. [Google Scholar] [CrossRef]
- Simuni, T.; Brumm, M.C.; Uribe, L.; Caspell-Garcia, C.; Coffey, C.S.; Siderowf, A.; Alcalay, R.N.; Trojanowski, J.Q.; Shaw, L.M.; Seibyl, J.; et al. Clinical and Dopamine Transporter Imaging Characteristics of Leucine Rich Repeat Kinase 2 (LRRK2) and Glucosylceramidase Beta (GBA) Parkinson’s Disease Participants in the Parkinson’s Progression Markers Initiative: A Cross-Sectional Study. Mov. Disord. 2020, 35, 833–844. [Google Scholar] [CrossRef] [PubMed]
- Bohnen, N.I.; Albin, R.L. Increased striatal dopamine in carriers of GBA mutations: Compensation or epiphenomenon? Lancet Neurol. 2020, 19, 27–29. [Google Scholar] [CrossRef]
- Liu, Z.Y.; Liu, F.T.; Zuo, C.T.; Koprich, J.B.; Wang, J. Update on Molecular Imaging in Parkinson’s Disease. Neurosci. Bull. 2018, 34, 330–340. [Google Scholar] [CrossRef]
- Nissen, T.; Malek, N.; Grosset, K.A.; Newman, E.J.; Patterson, J.; Hadley, D.; Grosset, D.G. Baseline [123I]FP-CIT SPECT (DaTSCAN) severity correlates with medication use at 3 years in Parkinson’s disease. Acta Neurol. Scand. 2014, 129, 204–208. [Google Scholar] [CrossRef]
- Tissingh, G.; Bergmans, P.; Booij, J.; Winogrodzka, A.; Van Royen, E.A.; Stoof, J.C.; Wolters, E.C. Drug-naive patients with Parkinson’s disease in Hoehn and Yahr stages I and II show a bilateral decrease in striatal dopamine transporters as revealed by [123I]β-CIT SPECT. J. Neurol. 1998, 245, 14–20. [Google Scholar] [CrossRef]
- Wang, J.; Zuo, C.T.; Jiang, Y.P.; Guan, Y.H.; Chen, Z.P.; Xiang, J.D.; Yang, L.Q.; Ding, Z.T.; Wu, J.J.; Su, H.L. 18F-FP-CIT PET imaging and SPM analysis of dopamine transporters in Parkinson’s disease in various Hoehn & Yahr stages. J. Neurol. 2007, 254, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, J.; Hellwig, D.; Samnick, S.; Jost, W.; Möllers, M.O.; Fassbender, K.; Kirsch, C.M.; Dillmann, U. Striatal FP-CIT uptake differs in the subtypes of early Parkinson’s disease. J. Neural Transm. 2007, 114, 331–335. [Google Scholar] [CrossRef]
- Rossi, C.; Frosini, D.; Volterrani, D.; De Feo, P.; Unti, E.; Nicoletti, V.; Kiferle, L.; Bonuccelli, U.; Ceravolo, R. Differences in nigro-striatal impairment in clinical variants of early Parkinson’s disease: Evidence from a FP-CIT SPECT study. Eur. J. Neurol. 2010, 17, 626–630. [Google Scholar] [CrossRef]
- Moccia, M.; Pappatà, S.; Picillo, M.; Erro, R.; Coda, A.R.D.; Longo, K.; Vitale, C.; Amboni, M.; Brunetti, A.; Capo, G.; et al. Dopamine transporter availability in motor subtypes of de novo drug-naïve Parkinson’s disease. J. Neurol. 2014, 261, 2112–2118. [Google Scholar] [CrossRef]
- Jellinger, K.A. Neuropathology of sporadic Parkinson’s disease: Evaluation and changes of concepts. Mov. Disord. 2012, 27, 8–30. [Google Scholar] [CrossRef]
- Eggers, C.; Kahraman, D.; Fink, G.R.; Schmidt, M.; Timmermann, L. Akinetic-rigid and tremor-dominant Parkinson’s disease patients show different patterns of FP-CIT Single photon emission computed tomography. Mov. Disord. 2011, 26, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Helmich, R.C. The cerebral basis of Parkinsonian tremor: A network perspective. Mov. Disord. 2018, 33, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Qamhawi, Z.; Towey, D.; Shah, B.; Pagano, G.; Seibyl, J.; Marek, K.; Borghammer, P.; Brooks, D.J.; Pavese, N. Clinical correlates of raphe serotonergic dysfunction in early Parkinson’s disease. Brain 2015, 138, 2964–2973. [Google Scholar] [CrossRef]
- Bohnen, N.I.; Müller, M.L.T.M.; Koeppe, R.A.; Studenski, S.A.; Kilbourn, M.A.; Frey, K.A.; Albin, R.L. History of falls in Parkinson disease is associated with reduced cholinergic activity. Neurology 2009, 73, 1670–1676. [Google Scholar] [CrossRef]
- Kim, R.; Lee, J.; Kim, Y.; Kim, A.; Jang, M.; Kim, H.J.; Jeon, B.; Kang, U.J.; Fahn, S. Presynaptic striatal dopaminergic depletion predicts the later development of freezing of gait in de novo Parkinson’s disease: An analysis of the PPMI cohort. Park. Relat. Disord. 2018, 51, 49–54. [Google Scholar] [CrossRef]
- Kim, R.; Lee, J.; Kim, H.J.; Kim, A.; Jang, M.; Jeon, B.; Kang, U.J. CSF β-amyloid42 and risk of freezing of gait in early Parkinson disease. Neurology 2019, 92, E40–E47. [Google Scholar] [CrossRef] [PubMed]
- Mäkinen, E.; Joutsa, J.; Jaakkola, E.; Noponen, T.; Johansson, J.; Pitkonen, M.; Levo, R.; Mertsalmi, T.; Scheperjans, F.; Kaasinen, V. Individual parkinsonian motor signs and striatal dopamine transporter deficiency: A study with [I-123]FP-CIT SPECT. J. Neurol. 2019, 266, 826–834. [Google Scholar] [CrossRef]
- Djaldetti, R.; Rigbi, A.; Greenbaum, L.; Reiner, J.; Lorberboym, M. Can early dopamine transporter imaging serve as a predictor of Parkinson’s disease progression and late motor complications? J. Neurol. Sci. 2018, 390, 255–260. [Google Scholar] [CrossRef]
- Latourelle, J.C.; Beste, M.T.; Hadzi, T.C.; Miller, R.E.; Oppenheim, J.N.; Valko, M.P.; Wuest, D.M.; Church, B.W.; Khalil, I.G.; Hayete, B.; et al. Large-scale identification of clinical and genetic predictors of motor progression in patients with newly diagnosed Parkinson’s disease: A longitudinal cohort study and validation. Lancet Neurol. 2017, 16, 908–916. [Google Scholar] [CrossRef]
- Vogt, T.; Kramer, K.; Gartenschlaeger, M.; Schreckenberger, M. Estimation of further disease progression of Parkinson’s disease by dopamin transporter scan vs. clinical rating. Park. Relat. Disord. 2011, 17, 459–463. [Google Scholar] [CrossRef]
- Whone, A.; Luz, M.; Boca, M.; Woolley, M.; Mooney, L.; Dharia, S.; Broadfoot, J.; Cronin, D.; Schroers, C.; Barua, N.U.; et al. Randomized trial of intermittent intraputamenal glial cell line-derived neurotrophic factor in Parkinson’s disease. Brain 2019, 142, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Kordower, J.H.; Goetz, C.G.; Chu, Y.; Halliday, G.M.; Nicholson, D.A.; Musial, T.F.; Marmion, D.J.; Stoessl, A.J.; Sossi, V.; Freeman, T.B.; et al. Robust graft survival and normalized dopaminergic innervation do not obligate recovery in a Parkinson disease patient. Ann. Neurol. 2017, 81, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Rahmim, A.; Salimpour, Y.; Jain, S.; Blinder, S.A.L.; Klyuzhin, I.S.; Smith, G.S.; Mari, Z.; Sossi, V. Application of texture analysis to DAT SPECT imaging: Relationship to clinical assessments. NeuroImage Clin. 2016, 12, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Mäkinen, E.; Joutsa, J.; Vahlberg, T.; Kaasinen, V. Survival in Parkinson’s disease in relation to striatal dopamine transporter binding. Park. Relat. Disord. 2017, 42, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.J.; Grossman, M.; Weintraub, D.; Hurtig, H.I.; Duda, J.E.; Xie, S.X.; Lee, E.B.; Van Deerlin, V.M.; Lopez, O.L.; Kofler, J.K.; et al. Neuropathological and genetic correlates of survival and dementia onset in synucleinopathies: A retrospective analysis. Lancet Neurol. 2017, 16, 55. [Google Scholar] [CrossRef]
- Pagano, G.; Niccolini, F.; Wilson, H.; Yousaf, T.; Khan, N.L.; Martino, D.; Plisson, C.; Gunn, R.N.; Rabiner, E.A.; Piccini, P.; et al. Comparison of phosphodiesterase 10A and dopamine transporter levels as markers of disease burden in early Parkinson’s disease. Mov. Disord. 2019, 34, 1505–1515. [Google Scholar] [CrossRef] [PubMed]
- Betrouni, N.; Moreau, C.; Rolland, A.S.; Carrière, N.; Chupin, M.; Kuchcinski, G.; Lopes, R.; Viard, R.; Defebvre, L.; Devos, D. Texture-based markers from structural imaging correlate with motor handicap in Parkinson’s disease. Sci. Rep. 2021, 11, 2724. [Google Scholar] [CrossRef] [PubMed]
- Rahmim, A.; Huang, P.; Shenkov, N.; Fotouhi, S.; Davoodi-Bojd, E.; Lu, L.; Mari, Z.; Soltanian-Zadeh, H.; Sossi, V. Improved prediction of outcome in Parkinson’s disease using radiomics analysis of longitudinal DAT SPECT images. NeuroImage Clin. 2017, 16, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.S.; Chung, S.J.; Chung, S.J.; Moon, H.; Oh, J.S.; Kim, J.S.; Hong, J.Y.; Ye, B.S.; Sohn, Y.H.; Lee, P.H. Presynaptic dopamine depletion determines the timing of levodopa-induced dyskinesia onset in Parkinson’s disease. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 423–431. [Google Scholar] [CrossRef]
- Jeong, E.H.; Sunwoo, M.K.; Song, Y.S. Serial I-123-FP-CIT SPECT Image Findings of Parkinson’s Disease Patients With Levodopa-Induced Dyskinesia. Front. Neurol. 2018, 9, 1133. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.J.; Lee, Y.; Oh, J.S.; Kim, J.S.; Lee, P.H.; Sohn, Y.H. Putaminal dopamine depletion in de novo Parkinson’s disease predicts future development of wearing-off. Park. Relat. Disord. 2018, 53, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Roussakis, A.-A.; Gennaro, M.; Lao-Kaim, N.P.; Towey, D.; Piccini, P. Dopamine Transporter Density in de novo Parkinson’s Disease Does Not Relate to the Development of Levodopa-Induced Dyskinesias. J. Neuroinflamm. Neurodegener. Dis. 2019, 3, 10000. [Google Scholar] [PubMed]
- Chung, S.J.; Lee, H.S.; Yoo, H.S.; Lee, Y.H.; Lee, P.H.; Sohn, Y.H. Patterns of striatal dopamine depletion in early Parkinson disease: Prognostic relevance. Neurology 2020, 95, E280–E290. [Google Scholar] [CrossRef]
- Pak, K.; Kim, H.; Seok, J.W.; Lee, M.J.; Shin, S.; Kim, K.; Lee, J.M.; Seo, Y.; Kim, B.S.; Jun, S.; et al. Prediction of future weight change with dopamine transporter in patients with Parkinson’s disease. J. Neural Transm. 2019, 126, 723–729. [Google Scholar] [CrossRef]
- La Torre, G.; Herman, A.M.; Jessop, M.; Abdula, N.; Crawshaw, A.; Begley, P.; Wroe, E.; Saha, R.A.; Duka, T.; Dizdarevic, S. 123I-Ioflupane dopamine transporter imaging (DaTSCAN) appearances in relation to emotional responsiveness, impulsivity and olfaction in suspected Parkinsonian syndrome. Nucl. Med. Commun. 2020, 41, 1117–1127. [Google Scholar] [CrossRef]
- Hinkle, J.T.; Perepezko, K.; Mills, K.A.; Mari, Z.; Butala, A.; Dawson, T.M.; Pantelyat, A.; Rosenthal, L.S.; Pontone, G.M.; Program, S.T.; et al. Dopamine transporter availability reflects gastrointestinal dysautonomia in early Parkinson disease. Park. Relat. Disord. 2018, 55, 8–14. [Google Scholar] [CrossRef]
- Jaakkola, E.; Joutsa, J.; Mäkinen, E.; Johansson, J.; Kaasinen, V. Ventral striatal dopaminergic defect is associated with hallucinations in Parkinson’s disease. Eur. J. Neurol. 2017, 24, 1341–1347. [Google Scholar] [CrossRef]
- Arnaldi, D.; De Carli, F.; Famà, F.; Brugnolo, A.; Girtler, N.; Picco, A.; Pardini, M.; Accardo, J.; Proietti, L.; Massa, F.; et al. Prediction of cognitive worsening in de novo Parkinson’s disease: Clinical use of biomarkers. Mov. Disord. 2017, 32, 1738–1747. [Google Scholar] [CrossRef]
- Lohle, M.; Mende, J.; Wolz, M.; Beuthien-Baumann, B.; Oehme, L.; Van Den Hoff, J.; Kotzerke, J.; Reichmann, H.; Storch, A. Putaminal dopamine turnover predicts levodopa-induced motor complications in de novo parkinson’s disease (I3-1A). Neurology 2015, 84, 14. [Google Scholar]
- De La Fuente-Fernández, R.; Sossi, V.; McCormick, S.; Schulzer, M.; Ruth, T.J.; Stoessl, A.J. Visualizing vesicular dopamine dynamics in Parkinson’s disease. Synapse 2009, 63, 713–716. [Google Scholar] [CrossRef]
- Troiano, A.R.; De La Fuente-Fernandez, R.; Sossi, V.; Schulzer, M.; Mak, E.; Ruth, T.J.; Stoessl, A.J. PET demonstrates reduced dopamine transporter expression in PD with dyskinesias. Neurology 2009, 72, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Roussakis, A.; Towey, D.; Gennaro, M.; Lao–Kaim, N.P.; Piccini, P. Parkinson’s Disease Dyskinesias Possibly Relate to Greater Dopamine Transporter Losses in the Putamen Over Time. J. Neurol. Exp. Neurosci. 2019, 5, 6–11. [Google Scholar] [CrossRef]
- Angela Cenci, M. Presynaptic mechanisms of L-DOPA-induced dyskinesia: The findings, the debate, the therapeutic implications. Front. Neurol. 2014, 5, 242. [Google Scholar] [CrossRef]
- Lee, J.Y.; Seo, S.; Lee, J.S.; Kim, H.J.; Kim, Y.K.; Jeon, B.S. Putaminal serotonergic innervation. Neurology 2015, 85, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Brumberg, J.; Küsters, S.; Al-Momani, E.; Marotta, G.; Cosgrove, K.P.; van Dyck, C.H.; Herrmann, K.; Homola, G.A.; Pezzoli, G.; Buck, A.K.; et al. Cholinergic activity and levodopa-induced dyskinesia: A multitracer molecular imaging study. Ann. Clin. Transl. Neurol. 2017, 4, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Pagano, G.; Niccolini, F.; Politis, M. The serotonergic system in Parkinson’s patients with dyskinesia: Evidence from imaging studies. J. Neural Transm. 2018, 125, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; Santangelo, G.; Erro, R.; Cozzolino, A.; Amboni, M.; Vitale, C.; Barone, P.; Pellecchia, M.T. Association between dopaminergic dysfunction and anxiety in de novo Parkinson’s disease. Park. Relat. Disord. 2017, 37, 106–110. [Google Scholar] [CrossRef]
- Hesse, S.; Meyer, P.M.; Strecker, K.; Barthel, H.; Wegner, F.; Oehlwein, C.; Isaias, I.U.; Schwarz, J.; Sabri, O. Monoamine transporter availability in Parkinson’s disease patients with or without depression. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 428–435. [Google Scholar] [CrossRef]
- Vriend, C.; Raijmakers, P.; Veltman, D.J.; Van Dijk, K.D.; Van Der Werf, Y.D.; Foncke, E.M.J.; Smit, J.H.; Berendse, H.W.; Van Den Heuvel, O.A. Depressive symptoms in Parkinson’s disease are related to reduced [123I]FP-CIT binding in the caudate nucleus. J. Neurol. Neurosurg. Psychiatry 2014, 85, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.W.; Oh, Y.S.; Hwang, E.J.; Ryu, D.W.; Lee, K.S.; Lyoo, C.H.; Kim, J.S. “Depressed” caudate and ventral striatum dopamine transporter availability in de novo Depressed Parkinson’s disease. Neurobiol. Dis. 2019, 132, 104563. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; Vitale, C.; Picillo, M.; Cuoco, S.; Moccia, M.; Pezzella, D.; Erro, R.; Longo, K.; Vicidomini, C.; Pellecchia, M.T.; et al. Apathy and striatal dopamine transporter levels in de-novo, untreated Parkinson’s disease patients. Park. Relat. Disord. 2015, 21, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Cilia, R.; Ko, J.H.; Cho, S.S.; van Eimeren, T.; Marotta, G.; Pellecchia, G.; Pezzoli, G.; Antonini, A.; Strafella, A.P. Reduced dopamine transporter density in the ventral striatum of patients with Parkinson’s disease and pathological gambling. Neurobiol. Dis. 2010, 39, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Siderowf, A.; Newberg, A.; Chou, K.L.; Lloyd, M.; Colcher, A.; Hurtig, H.I.; Stern, M.B.; Doty, R.L.; Mozley, P.D.; Wintering, N.; et al. [99mTc]TRODAT-1 SPECT imaging correlates with odor identification in early Parkinson disease. Neurology 2005, 64, 1716–1720. [Google Scholar] [CrossRef] [PubMed]
- Berendse, H.W.; Roos, D.S.; Raijmakers, P.; Doty, R.L. Motor and non-motor correlates of olfactory dysfunction in Parkinson’s disease. J. Neurol. Sci. 2011, 310, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Deeb, J.; Shah, M.; Muhammed, N.; Gunasekera, R.; Gannon, K.; Findley, L.J.; Hawkes, C.H. A basic smell test is as sensitive as a dopamine transporter scan: Comparison of olfaction, taste and DaTSCAN in the diagnosis of Parkinson’s disease. QJM 2010, 103, 941–952. [Google Scholar] [CrossRef]
- Roos, D.S.; Twisk, J.W.R.; Raijmakers, P.G.H.M.; Doty, R.L.; Berendse, H.W. Hyposmia as a marker of (non-)motor disease severity in Parkinson’s disease. J. Neural Transm. 2019, 126, 1471–1478. [Google Scholar] [CrossRef]
- Sakakibara, R.; Shinotoh, H.; Uchiyama, T.; Yoshiyama, M.; Hattori, T.; Yamanishi, T. SPECT imaging of the dopamine transporter with [123I]-β-CIT reveals marked decline of nigrostriatal dopaminergic function in Parkinson’s disease with urinary dysfunction. J. Neurol. Sci. 2001, 187, 55–59. [Google Scholar] [CrossRef]
- Pagano, G.; Niccolini, F.; Yousaf, T.; Wilson, H.; Polychronis, S.; Chaudhuri, K.R.; Politis, M. Urinary dysfunction in early de novo patients with Parkinson’s disease. Mov. Disord. 2017, 32, 939–940. [Google Scholar] [CrossRef]
- van Deursen, D.N.; van den Heuvel, O.A.; Booij, J.; Berendse, H.W.; Vriend, C. Autonomic failure in Parkinson’s disease is associated with striatal dopamine deficiencies. J. Neurol. 2020, 267, 1922–1930. [Google Scholar] [CrossRef] [PubMed]
- Mito, Y.; Yabe, I.; Yaguchi, H.; Takei, T.; Terae, S.; Tajima, Y. Relation of overactive bladder with motor symptoms and dopamine transporter imaging in drug-naïve Parkinson’s disease. Park. Relat. Disord. 2018, 50, 37–41. [Google Scholar] [CrossRef]
- Kim, R.; Jun, J.S. Association of autonomic symptoms with presynaptic striatal dopamine depletion in drug-naive Parkinson’s disease: An analysis of the PPMI data. Auton. Neurosci. Basic Clin. 2019, 216, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cao, R.; Huang, T.; Liu, C.; Fan, Y. Urinary dysfunction is associated with nigrostriatal dopaminergic degeneration in early and untreated patients with Parkinson’s disease. Park. Dis. 2020, 2020, 4981647. [Google Scholar] [CrossRef]
- Yousaf, T.; Pagano, G.; Niccolini, F.; Politis, M. Excessive daytime sleepiness may be associated with caudate denervation in Parkinson disease. J. Neurol. Sci. 2018, 387, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Oh, J.S.; Ham, J.H.; Lee, D.H.; Lee, I.; Sohn, Y.H.; Kim, J.S.; Lee, P.H. Association of body mass index and the depletion of nigrostriatal dopamine in Parkinson’s disease. Neurobiol. Aging 2016, 38, 197–204. [Google Scholar] [CrossRef]
- Qamar, M.A.; Sauerbier, A.; Politis, M.; Carr, H.; Loehrer, P.; Chaudhuri, K.R. Presynaptic dopaminergic terminal imaging & non-motor symptoms assessment of Parkinson’s disease: Evidence for dopaminergic basis? Park. Dis. 2017, 3, 5. [Google Scholar] [CrossRef]
- Liu, R.; Umbach, D.M.; Tröster, A.I.; Huang, X.; Chen, H. Non-motor symptoms and striatal dopamine transporter binding in early Parkinson’s disease. Park. Relat. Disord. 2020, 72, 23–30. [Google Scholar] [CrossRef]
- Chung, S.J.; Lee, S.; Yoo, H.S.; Lee, Y.H.; Lee, H.S.; Choi, Y.; Lee, P.H.; Yun, M.; Sohn, Y.H. Association of the Non-Motor Burden with Patterns of Striatal Dopamine Loss in de novo Parkinson’s Disease. J. Park. Dis. 2020, 10, 1541–1549. [Google Scholar] [CrossRef]
- Schifitto, G.; Friedman, J.H.; Oakes, D.; Shulman, L.; Comella, C.L.; Marek, K.; Fahn, S. Fatigue in levodopa-naïve subjects with Parkinson disease. Neurology 2008, 71, 481–485. [Google Scholar] [CrossRef]
- Moriyama, T.S.; Felicio, A.C.; Chagas, M.H.N.; Tardelli, V.S.; Ferraz, H.B.; Tumas, V.; Amaro-Junior, E.; Andrade, L.A.F.; Crippa, J.A.; Bressan, R.A. Increased dopamine transporter density in Parkinson’s disease patients with social anxiety disorder. J. Neurol. Sci. 2011, 310, 53–57. [Google Scholar] [CrossRef]
- Ceravolo, R.; Frosini, D.; Poletti, M.; Kiferle, L.; Pagni, C.; Mazzucchi, S.; Volterrani, D.; Bonuccelli, U. Mild affective symptoms in de novo Parkinson’s disease patients: Relationship with dopaminergic dysfunction. Eur. J. Neurol. 2013, 20, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.J.; Lee, J.J.; Ham, J.H.; Lee, P.H.; Sohn, Y.H. Apathy and striatal dopamine defects in non-demented patients with Parkinson’s disease. Park. Relat. Disord. 2016, 23, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.J.; Lee, J.J.; Ham, J.H.; Ye, B.S.; Lee, P.H.; Sohn, Y.H. Striatal dopamine depletion patterns and early non-motor burden in Parkinsons disease. PLoS ONE 2016, 11, e161316. [Google Scholar] [CrossRef] [PubMed]
- Moccia, M.; Erro, R.; Picillo, M.; Santangelo, G.; Spina, E.; Allocca, R.; Longo, K.; Amboni, M.; Palladino, R.; Assante, R.; et al. A four-year longitudinal study on restless legs syndrome in Parkinson disease. Sleep 2016, 39, 405–412. [Google Scholar] [CrossRef]
- Jaakkola, E.; Joutsa, J.; Mäkinen, E.; Noponen, T.; Pitkonen, M.; Levo, R.; Mertsalmi, T.; Scheperjans, F.; Kaasinen, V. Burden of non-motor symptoms in unclear parkinsonism and tremor: A study with [123I]FP-CIT SPECT. J. Neurol. Sci. 2019, 404, 124–127. [Google Scholar] [CrossRef]
- Ye, B.S.; Jeon, S.; Yoon, S.; Kang, S.W.; Baik, K.W.; Lee, Y.; Chung, S.J.; Oh, J.S.; Moon, H.; Kim, J.S.; et al. Effects of dopaminergic depletion and brain atrophy on neuropsychiatric symptoms in de novo Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2018, 89, 197–204. [Google Scholar] [CrossRef]
- Nobili, F.; Campus, C.; Arnaldi, D.; De Carli, F.; Cabassi, G.; Brugnolo, A.; Dessi, B.; Morbelli, S.; Sambuceti, G.; Abbruzzese, G.; et al. Cognitive-nigrostriatal relationships in de novo, drug-naïve Parkinson’s disease patients: A [I-123]FP-CIT SPECT Study. Mov. Disord. 2010, 25, 35–43. [Google Scholar] [CrossRef]
- Siepel, F.J.; Brønnick, K.S.; Booij, J.; Ravina, B.M.; Lebedev, A.V.; Pereira, J.B.; Grüner, R.; Aarsland, D. Cognitive executive impairment and dopaminergic deficits in de novo Parkinson’s disease. Mov. Disord. 2014, 29, 1802–1808. [Google Scholar] [CrossRef]
- Pellecchia, M.T.; Picillo, M.; Santangelo, G.; Longo, K.; Moccia, M.; Erro, R.; Amboni, M.; Vitale, C.; Vicidomini, C.; Salvatore, M.; et al. Cognitive performances and DAT imaging in early Parkinson’s disease with mild cognitive impairment: A preliminary study. Acta Neurol. Scand. 2015, 131, 275–281. [Google Scholar] [CrossRef]
- Kübler, D.; Schroll, H.; Buchert, R.; Kühn, A.A. Cognitive performance correlates with the degree of dopaminergic degeneration in the associative part of the striatum in non-demented Parkinson’s patients. J. Neural Transm. 2017, 124, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.J.; Yoo, H.S.; Oh, J.S.; Kim, J.S.; Ye, B.S.; Sohn, Y.H.; Lee, P.H. Effect of striatal dopamine depletion on cognition in de novo Parkinson’s disease. Park. Relat. Disord. 2018, 51, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Oh, M.; Oh, J.S.; Moon, H.; Chung, S.J.; Lee, C.S.; Kim, J.S. Association of striatal dopaminergic neuronal integrity with cognitive dysfunction and cerebral cortical metabolism in Parkinson’s disease with mild cognitive impairment. Nucl. Med. Commun. 2019, 40, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Arnaldi, D.; De Carli, F.; Picco, A.; Ferrara, M.; Accardo, J.; Bossert, I.; Famà, F.; Girtler, N.; Morbelli, S.; Sambuceti, G.; et al. Nigro-caudate dopaminergic deafferentation: A marker of REM sleep behavior disorder? Neurobiol. Aging 2015, 36, 3300–3305. [Google Scholar] [CrossRef] [PubMed]
- Pasquini, J.; Durcan, R.; Wiblin, L.; Gersel Stokholm, M.; Rochester, L.; Brooks, D.J.; Burn, D.; Pavese, N. Clinical implications of early caudate dysfunction in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2019, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Sampedro, F.; Marín-Lahoz, J.; Martínez-Horta, S.; Camacho, V.; Lopez-Mora, D.A.; Pagonabarraga, J.; Kulisevsky, J. Extrastriatal SPECT-DAT uptake correlates with clinical and biological features of de novo Parkinson’s disease. Neurobiol. Aging 2021, 97, 120–128. [Google Scholar] [CrossRef]
- Fiorenzato, E.; Antonini, A.; Bisiacchi, P.; Weis, L.; Biundo, R. Asymmetric Dopamine Transporter Loss Affects Cognitive and Motor Progression in Parkinson’s Disease. Mov. Disord. 2021, 2021, 28682. [Google Scholar] [CrossRef]
- Bae, Y.J.; Kim, J.M.; Sohn, C.H.; Choi, J.H.; Choi, B.S.; Song, Y.S.; Nam, Y.; Cho, S.J.; Jeon, B.; Kim, J.H. Imaging the substantia nigra in Parkinson disease and other Parkinsonian syndromes. Radiology 2021, 300, 260–278. [Google Scholar] [CrossRef]
- Mahlknecht, P.; Krismer, F.; Poewe, W.; Seppi, K. Meta-analysis of dorsolateral nigral hyperintensity on magnetic resonance imaging as a marker for Parkinson’s disease. Mov. Disord. 2017, 32, 619–623. [Google Scholar] [CrossRef]
- De Marzi, R.; Seppi, K.; Högl, B.; Müller, C.; Scherfler, C.; Stefani, A.; Iranzo, A.; Tolosa, E.; Santamarìa, J.; Gizewski, E.; et al. Loss of dorsolateral nigral hyperintensity on 3.0 tesla susceptibility-weighted imaging in idiopathic rapid eye movement sleep behavior disorder. Ann. Neurol. 2016, 79, 1026–1030. [Google Scholar] [CrossRef]
- Kim, J.M.; Jeong, H.J.; Bae, Y.J.; Park, S.Y.; Kim, E.; Kang, S.Y.; Oh, E.S.; Kim, K.J.; Jeon, B.; Kim, S.E.; et al. Loss of substantia nigra hyperintensity on 7 Tesla MRI of Parkinson’s disease, multiple system atrophy, and progressive supranuclear palsy. Park. Relat. Disord. 2016, 26, 47–54. [Google Scholar] [CrossRef]
- Bae, Y.J.; Kim, J.M.; Kim, E.; Lee, K.M.; Kang, S.Y.; Park, H.S.; Kim, K.J.; Kim, Y.E.; Oh, E.S.; Yun, J.Y.; et al. Loss of Nigral Hyperintensity on 3 Tesla MRI of Parkinsonism: Comparison with 123I-FP-CIT SPECT. Mov. Disord. 2016, 31, 684–692. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, Y.; Zhu, C.; Li, G.; Kang, J.; Chen, F.; Yang, L. The diagnostic value of SNpc using NM-MRI in Parkinson’s disease: Meta-analysis. Neurol. Sci. 2019, 40, 2479–2489. [Google Scholar] [CrossRef]
- Kuya, K.; Ogawa, T.; Shinohara, Y.; Ishibashi, M.; Fujii, S.; Mukuda, N.; Tanabe, Y. Evaluation of Parkinson’s disease by neuromelanin-sensitive magnetic resonance imaging and 123I-FP-CIT SPECT. Acta Radiol. 2018, 59, 593–598. [Google Scholar] [CrossRef]
- Matsusue, E.; Fujihara, Y.; Tanaka, K.; Aozasa, Y.; Shimoda, M.; Nakayasu, H.; Nakamura, K.; Ogawa, T. The utility of the combined use of 123 I-FP-CIT SPECT and neuromelanin MRI in differentiating Parkinson’s disease from other parkinsonian syndromes. Acta Radiol. 2019, 60, 230–238. [Google Scholar] [CrossRef]
- Gaurav, R.; Yahia-Cherif, L.; Pyatigorskaya, N.; Mangone, G.; Biondetti, E.; Valabrègue, R.; Ewenczyk, C.; Hutchison, R.M.; Cedarbaum, J.M.; Corvol, J.C.; et al. Longitudinal Changes in Neuromelanin MRI Signal in Parkinson’s Disease: A Progression Marker. Mov. Disord. 2021, 36, 1592–1602. [Google Scholar] [CrossRef]
- Takahashi, H.; Watanabe, Y.; Tanaka, H.; Mihara, M.; Mochizuki, H.; Takahashi, K.; Yamamoto, K.; Liu, T.; Wang, Y.; Tomiyama, N. Comprehensive MRI quantification of the substantia nigra pars compacta in Parkinson’s disease. Eur. J. Radiol. 2018, 109, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Heim, B.; Krismer, F.; De Marzi, R.; Seppi, K. Magnetic resonance imaging for the diagnosis of Parkinson’s disease. J. Neural Transm. 2017, 124, 915–964. [Google Scholar] [CrossRef] [PubMed]
- Vaillancourt, D.; Lehéricy, S. Illuminating basal ganglia and beyond in Parkinson’s disease. Mov. Disord. 2018, 33, 1373–1375. [Google Scholar] [CrossRef] [PubMed]


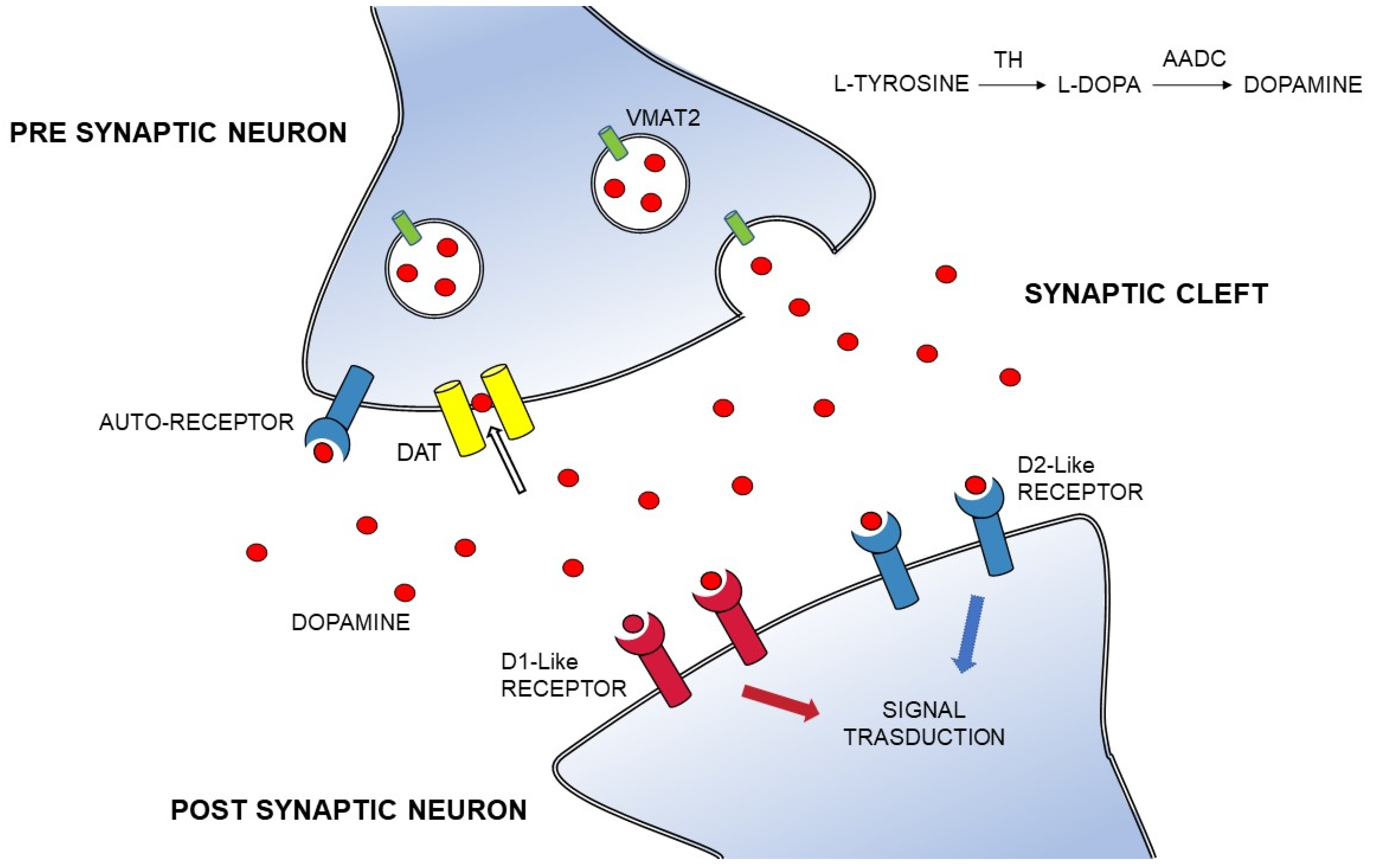{kind=link}
| Outcomes | Authors and Year | Type of Study | Radioligand | Population | Main Results |
|---|---|---|---|---|---|
| Motor Severity | |||||
| UPDRS motor score, Hoen and Yahr scale, Freezing of gait, Falling | Vogt et al., 2011 [224] | Prospective | [123I]-β-CIT SPECT | 44 early-stage PD | Weak correlation between baseline DAT binding ratios and staging parameters (UPDRS II-III and H&Y) at follow-up |
| Ravina et al., 2012 [43] | Prospective | [123I]-β-CIT SPECT | 491 de novo PD | Lower baseline DAT binding is associated with higher risk for motor-related disability, falling and postural instability | |
| Rahmim et al., 2016 [227] | Prospective | [123I]-FP-CIT SPECT | 64 de novo PD | Baseline DAT binding is significantly correlated with UPDRS III and disease duration | |
| Djaldetti et al., 2018 [222] | Retrospective | [123I]-FP-CIT SPECT | 41 early-stage PD | Baseline DAT binding does not predict H&Y or UPDRS motor score progression, but lower DAT uptake at baseline is associated with the development of FOG | |
| Kim et al., 2018 [219] | Retrospective | [123I]-FP-CIT SPECT | 390 de novo PD | Lower baseline DAT binding in the caudate nucleus and putamen significantly predicts the development of FOG | |
| Simuni et al., 2018 [70] | Prospective | [123I]-FP-CIT SPECT | 358 early-stage PD | No correlation between the rate of change of UPDRS-III and change in the striatal DAT uptake | |
| Li et al., 2018 [184] | Prospective | 11C-PE2I PET | 33 mild-moderate stage PD | Negative correlation between baseline DAT binding in the caudate, anterior and posterior putamen, and motor severity (UPDRS-III, bradykinesia-rigidity subscores) | |
| Kim et al., 2019 [219] | Prospective | [123I]-FP-CIT SPECT | 392 early-stage PD | Baseline caudate DAT binding significantly predicts FOG | |
| Pagano et al., 2019 [230] | Prospective | 11C-PE2I PET | 17 de novo PD, 15 early-stage LD-treated PD, 24 moderate-advanced LD-treated PD | Negative correlation between change in motor severity (UPDRS-III and bradykinesia/rigidity subscores) and change in the baseline DAT uptake in the caudate and posterior putamen | |
| Survival | Makinen et al., 2017 [228] | Retrospective | [123I]-FP-CIT SPECT | 162 PD: all stages | Baseline DAT binding does not predict mortality |
| Motor complications | |||||
| Levodopa-induced dyskinesia (LID) Motor fluctuations | Hong et al., 2014 [87] | Prospective | 18F-FP-CIT PET | 127 de novo PD | Baseline putaminal DAT uptake significantly predicts the development of LID |
| Palermo et al. 2020 [88] | Retrospective | [123I]-FP-CIT SPECT | 105 de novo PD | Lower baseline DAT binding in early-onset PD predicts later motor complications | |
| Yoo et al., 2017 [233] | Retrospective | 18F-FP-CIT PET | 65 de novo PD | Lower DAT binding in the posterior putamen at baseline is a major risk factor for earlier onset of LID | |
| Jeong et al., 2018 [234] | Prospective | [123I]-FP-CIT SPECT | 290 de novo PD | Baseline DAT binding is lower in PD patients who will develop LID | |
| Chung et al., 2018 [235] | Retrospective | 18F-FP-CIT PET | 342 de novo PD | Lower baseline DAT binding in the anterior putamen predicts the wearing-off phenomenon | |
| Djaldetti et al., 2018 [222] | Retrospective | [123I]-FP-CIT SPECT | 41 early-stage PD | Baseline DAT binding does not predict motor complications | |
| Roussakis et al., 2019 [236] | Prospective | [123I]-FP-CIT SPECT | 42 de novo PD | Baseline DAT binding does not predict LID | |
| Chung et al., 2020 [237] | Retrospective | 18F-FP-CIT PET | 205 early-stage PD | Baseline DAT binding, particularly in the anterior putamen, predicts the wearing-off phenomenon | |
| Non-motor symptoms | |||||
| Anxiety, Depression, Impulsivity, Constipation, Autonomic symptoms, Visual hallucinations, Body weight gain/loss | Ravina et al., 2012 [43] | Prospective | [123I]-β-CIT SPECT | 491 de novo PD | Lower striatal DAT binding at baseline is associated with depressive symptoms |
| Kyoungjune et al., 2019 [238] | Prospective | [123I]-FP-CIT SPECT | 163 de novo PD | Lower baseline putamen-to-caudate DAT binding ratio is associated with future weight gain in men (but not women) | |
| La Torre et al., 2020 [239] | Prospective | [123I]-FP-CIT SPECT | 20 de novo PD | Higher baseline putamen-to-caudate DAT binding ratios are associated with higher emotional responsiveness and higher non-planning impulsivity | |
| Hinkle et al., 2018 [240] | Prospective | [123I]-FP-CIT SPECT | 397 de novo PD | Constipation is closely associated with lower baseline caudate DAT binding | |
| Jaakkola et al., 2017 [241] | Prospective | [123I]-FP-CIT SPECT | 70 early-stage PD | Baseline low ventral striatal DAT binding is associated with visual hallucinations | |
| Cognitive performances | |||||
| Ravina et al., 2012 [43] | Prospective | [123I]-β-CIT SPECT | 491 de novo PD | Lower striatal DAT binding at baseline is associated with cognitive impairment | |
| Arnaldi et al., 2017 [242] | Prospective | [123I]-FP-CIT SPECT | 54 de novo PD | Caudate DAT binding predicts patients’ cognitive worsening at the follow up | |
| Yousaf et al., 2019 [68] | Prospective | [123I]-FP-CIT SPECT | 262 de novo PD | Lower caudate DAT binding at baseline is associated with higher risk of cognitive impairment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palermo, G.; Giannoni, S.; Bellini, G.; Siciliano, G.; Ceravolo, R. Dopamine Transporter Imaging, Current Status of a Potential Biomarker: A Comprehensive Review. Int. J. Mol. Sci. 2021, 22, 11234. https://doi.org/10.3390/ijms222011234
Palermo G, Giannoni S, Bellini G, Siciliano G, Ceravolo R. Dopamine Transporter Imaging, Current Status of a Potential Biomarker: A Comprehensive Review. International Journal of Molecular Sciences. 2021; 22(20):11234. https://doi.org/10.3390/ijms222011234
Chicago/Turabian StylePalermo, Giovanni, Sara Giannoni, Gabriele Bellini, Gabriele Siciliano, and Roberto Ceravolo. 2021. "Dopamine Transporter Imaging, Current Status of a Potential Biomarker: A Comprehensive Review" International Journal of Molecular Sciences 22, no. 20: 11234. https://doi.org/10.3390/ijms222011234
APA StylePalermo, G., Giannoni, S., Bellini, G., Siciliano, G., & Ceravolo, R. (2021). Dopamine Transporter Imaging, Current Status of a Potential Biomarker: A Comprehensive Review. International Journal of Molecular Sciences, 22(20), 11234. https://doi.org/10.3390/ijms222011234