
Long-Term Efficacy of Intranasal Esketamine in Treatment-Resistant Major Depression: A Systematic Review

 ,
,  ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Results and Discussion
2.1. Esketamine Treatment Continuation after the 4-Week Induction Phase
2.2. Follow-Up Phase after the 4-Week Induction Phase
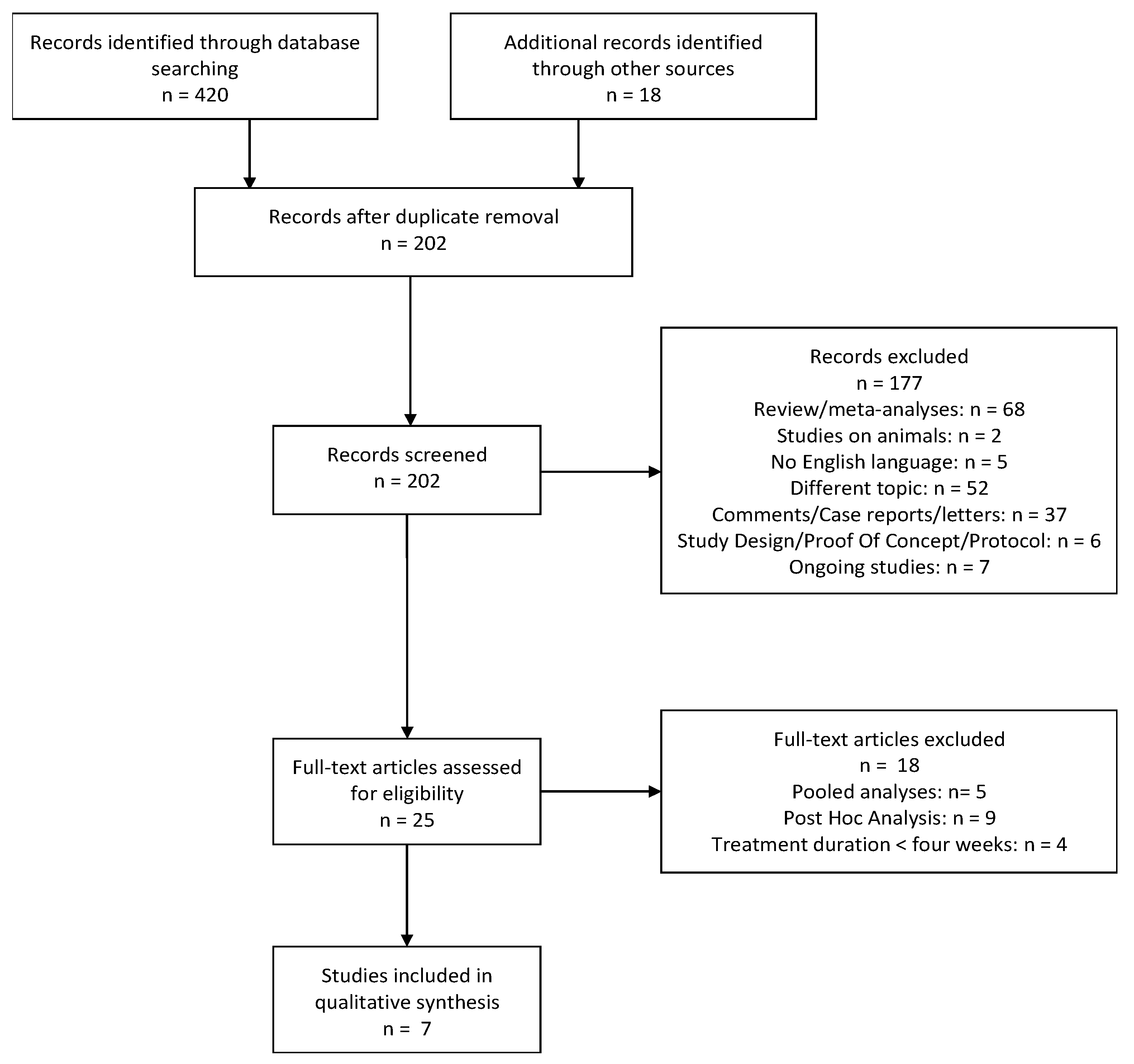
3. Methods
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Trivedi, M.H.; Fava, M.; Wisniewski, S.R.; Thase, M.E.; Quitkin, F.; Warden, D.; Ritz, L.; Nierenberg, A.A.; Lebowitz, B.D.; Biggs, M.M.; et al. STAR*D Study Team. Medication augmentation after the failure of SSRIs for depression. N. Engl. J. Med. 2006, 354, 1243–1252. [Google Scholar] [CrossRef]
- Altamura, A.C.; Dell’Osso, B.; Buoli, M.; Zanoni, S.; Mundo, E. Intravenous augmentative citalopram versus clomipramine in partial/nonresponder depressed patients: A short-term, low dose, randomized, placebo-controlled study. J. Clin. Psychopharmacol. 2008, 28, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.O.; Veronese, N.; Sanches, M.; Stubbs, B.; Koyanagi, A.; Thompson, T.; Tzoulaki, I.; Solmi, M.; Vancampfort, D.; Schuch, F.B.; et al. The association of depression and all-cause and cause-specific mortality: An umbrella review of systematic reviews and meta-analyses. BMC Med. 2018, 16, 112. [Google Scholar] [CrossRef] [PubMed]
- Capuzzi, E.; Caldiroli, A.; Capellazzi, M.; Tagliabue, I.; Buoli, M.; Clerici, M. Biomarkers of suicidal behaviors: A comprehensive critical review. Adv. Clin. Chem. 2020, 96, 179–216. [Google Scholar] [CrossRef]
- Li, X.; Frye, M.A.; Shelton, R.C. Review of pharmacological treatment in mood disorders and future directions for drug development. Neuropsychopharmacology 2012, 37, 77–101. [Google Scholar] [CrossRef]
- Krishnan, V.; Nestler, E.J. The molecular neurobiology of depression. Nature 2008, 455, 894–902. [Google Scholar] [CrossRef]
- Manji, H.K.; Quiroz, J.A.; Sporn, J.; Payne, J.L.; Denicoff, K.; Gray, N.A.; Zarate, C.A., Jr.; Charney, D.S. Enhancing neuronal plasticity and cellular resilience to develop novel, improved therapeutics for difficult-to-treat depression. Biol. Psychiatry 2003, 53, 707–742. [Google Scholar] [CrossRef] [Green Version]
- Skolnick, P.; Popik, P.; Trullas, R. Glutamate-based antidepressants: 20 years on. Trends Pharm. Sci. 2009, 30, 563–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaso, B.A.; Niciu, M.J.; Iadarola, N.D.; Lally, N.; Richards, E.M.; Park, M.; Ballard, E.D.; Nugent, A.C.; Machado-Vieira, R.; Zarate, C.A. Therapeutic Modulation of Glutamate Receptors in Major Depressive Disorder. Curr. Neuropharmacol. 2017, 15, 57–70. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, K. Rapid-acting antidepressant ketamine, its metabolites and other candidates: A historical overview and future perspective. Psychiatry Clin. Neurosci. 2019, 73, 613–627. [Google Scholar] [CrossRef] [PubMed]
- Zanos, P.; Gould, T.D. Mechanisms of ketamine action as an antidepressant. Mol. Psychiatry 2018, 23, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Coyle, C.M.; Laws, K.R. The use of ketamine as an antidepressant: A systematic review and meta-analysis. Hum. Psychopharmacol. 2015, 30, 152–163. [Google Scholar] [CrossRef] [Green Version]
- Serafini, G.; Howland, R.H.; Rovedi, F.; Girardi, P.; Amore, M. The role of ketamine in treatment-resistant depression: A systematic review. Curr. Neuropharmacol. 2014, 12, 444–461. [Google Scholar] [CrossRef] [Green Version]
- Bartoli, F.; Riboldi, I.; Crocamo, C.; Di Brita, C.; Clerici, M.; Carrà, G. Ketamine as a rapid-acting agent for suicidal ideation: A meta-analysis. Neurosci. Biobehav. Rev. 2017, 77, 232–236. [Google Scholar] [CrossRef] [PubMed]
- McShane, R.; Baldwin, D.S.; McAllister-Williams, R.H.; Stone, J.M.; Taylor, D.; Winstock, A.R.; Young, A.H. Esketamine and the Need for a New Type of Registry for Drugs With Abuse Potential. Am. J. Psychiatry 2019, 176, 966. [Google Scholar] [CrossRef] [PubMed]
- Zanos, P.; Moaddel, R.; Morris, P.J.; Riggs, L.M.; Highland, J.N.; Georgiou, P.; Pereira, E.; Albuquerque, E.X.; Thomas, C.J.; Zarate, C.A., Jr.; et al. Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms. Pharm. Rev. 2018, 70, 621–660. [Google Scholar] [CrossRef] [Green Version]
- Smith-Apeldoorn, S.Y.; Veraart, J.; Kamphuis, J.; van Asselt, A.; Touw, D.J.; Aan Het Rot, M.; Schoevers, R.A. Correction to: Oral esketamine for treatment-resistant depression: Rationale and design of a randomized controlled trial. BMC Psychiatry 2020, 20, 9. [Google Scholar] [CrossRef] [Green Version]
- Swainson, J.; Thomas, R.K.; Archer, S.; Chrenek, C.; MacKay, M.A.; Baker, G.; Dursun, S.; Klassen, L.J.; Chokka, P.; Demas, M.L. Esketamine for treatment resistant depression. Expert Rev. Neurother. 2019, 19, 899–911. [Google Scholar] [CrossRef]
- Kim, J.; Farchione, T.; Potter, A.; Chen, Q.; Temple, R. Esketamine for Treatment-Resistant Depression—First FDA-Approved Antidepressant in a New Class. N. Engl. J. Med. 2019, 381, 1–4. [Google Scholar] [CrossRef]
- Papakostas, G.I.; Salloum, N.C.; Hock, R.S.; Jha, M.K.; Murrough, J.W.; Mathew, S.J.; Iosifescu, D.V.; Fava, M. Efficacy of Esketamine Augmentation in Major Depressive Disorder: A Meta-Analysis. J. Clin. Psychiatry 2020, 81, 19r12889. [Google Scholar] [CrossRef]
- Zheng, W.; Cai, D.B.; Xiang, Y.Q.; Zheng, W.; Jiang, W.L.; Sim, K.; Ungvari, G.S.; Huang, X.; Huang, X.X.; Ning, Y.P.; et al. Adjunctive intranasal esketamine for major depressive disorder: A systematic review of randomized double-blind controlled-placebo studies. J. Affect Disord. 2020, 265, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Chen-Li, D.; Rosenblat, J.D.; Rodrigues, N.B.; Carvalho, I.; Lui, L.; Gill, H.; Narsi, F.; Mansur, R.B.; et al. The acute antisuicidal effects of single-dose intravenous ketamine and intranasal esketamine in individuals with major depression and bipolar disorders: A systematic review and meta-analysis. J. Psychiatr. Res. 2021, 134, 57–68. [Google Scholar] [CrossRef]
- Fedgchin, M.; Trivedi, M.; Daly, E.J.; Melkote, R.; Lane, R.; Lim, P.; Vitagliano, D.; Blier, P.; Fava, M.; Liebowitz, M.; et al. Efficacy and Safety of Fixed-Dose Esketamine Nasal Spray Combined With a New Oral Antidepressant in Treatment-Resistant Depression: Results of a Randomized, Double-Blind, Active-Controlled Study (TRANSFORM-1). Int. J. Neuropsychopharmacol. 2019, 22, 616–630. [Google Scholar] [CrossRef]
- Ochs-Ross, R.; Daly, E.J.; Zhang, Y.; Lane, R.; Lim, P.; Morrison, R.L.; Hough, D.; Manji, H.; Drevets, W.C.; Sanacora, G.; et al. Efficacy and Safety of Esketamine Nasal Spray Plus an Oral Antidepressant in Elderly Patients With Treatment-Resistant Depression-TRANSFORM-3. Am. J. Geriatr. Psychiatry 2020, 28, 121–141. [Google Scholar] [CrossRef]
- Popova, V.; Daly, E.J.; Trivedi, M.; Cooper, K.; Lane, R.; Lim, P.; Mazzucco, C.; Hough, D.; Thase, M.E.; Shelton, R.C.; et al. Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study. Am. J. Psychiatry 2019, 176, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Daly, E.J.; Singh, J.B.; Fedgchin, M.; Cooper, K.; Lim, P.; Shelton, R.C.; Thase, M.E.; Winokur, A.; Van Nueten, L.; Manji, H.; et al. Efficacy and Safety of Intranasal Esketamine Adjunctive to Oral Antidepressant Therapy in Treatment-Resistant Depression: A Randomized Clinical Trial. JAMA Psychiatry 2018, 75, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Daly, E.J.; Trivedi, M.H.; Janik, A.; Li, H.; Zhang, Y.; Li, X.; Lane, R.; Lim, P.; Duca, A.; Hough, R.; et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with Treatment-Resistant Depression: A randomized clinical trial. JAMA Psychiatry 2019, 76, 893–903. [Google Scholar] [CrossRef]
- Wajs, E.; Aluisio, L.; Holder, R.; Daly, E.J.; Lane, R.; Lim, P.; George, J.E.; Morrison, R.L.; Sanacora, G.; Young, A.H.; et al. Esketamine Nasal Spray Plus Oral Antidepressant in Patients With Treatment-Resistant Depression: Assessment of Long-Term Safety in a Phase 3, Open-Label Study (SUSTAIN-2). J. Clin. Psychiatry 2020, 81, 19m12891. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. A Study to Evaluate the Efficacy, Safety and Tolerability of Fixed doses of Intranasal Esketamine in Japanese Participants with Treatment Resistant Depression. ClinicalTrials.gov Identifier: NCT02918318. Available online: https://clinicaltrials.gov/ct2/show/NCT02918318 (accessed on 20 August 2021).
- Canuso, C.M.; Singh, J.B.; Fedgchin, M.; Alphs, L.; Lane, R.; Lim, P.; Pinter, C.; Hough, D.; Sanacora, G.; Manji, H.; et al. Efficacy and Safety of Intranasal Esketamine for the Rapid Reduction of Symptoms of Depression and Suicidality in Patients at Imminent Risk for Suicide: Results of a Double-Blind, Randomized, Placebo-Controlled Study. Am. J. Psychiatry 2018, 175, 620–630. [Google Scholar] [CrossRef]
- Fu, D.J.; Ionescu, D.F.; Li, X.; Lane, R.; Lim, P.; Sanacora, G.; Hough, D.; Manji, H.; Drevets, W.C.; Canuso, C.M. Esketamine Nasal Spray for Rapid Reduction of Major Depressive Disorder Symptoms in Patients Who Have Active Suicidal Ideation With Intent: Double-Blind, Randomized Study (ASPIRE I). J. Clin. Psychiatry 2020, 81, 19m13191. [Google Scholar] [CrossRef]
- Ionescu, D.F.; Fu, D.J.; Qiu, X.; Lane, R.; Lim, P.; Kasper, S.; Hough, D.; Drevets, W.C.; Manji, H.; Canuso, C.M. Esketamine Nasal Spray for Rapid Reduction of Depressive Symptoms in Patients With Major Depressive Disorder Who Have Active Suicide Ideation With Intent: Results of a Phase 3, Double-Blind, Randomized Study (ASPIRE II). Int. J. Neuropsychopharmacol. 2021, 24, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strong, C.E.; Kabbaj, M. On the safety of repeated ketamine infusions for the treatment of depression: Effects of sex and developmental periods. Neurobiol. Stress 2018, 9, 166–175. [Google Scholar] [CrossRef]
- Gass, N.; Becker, R.; Reinwald, J.; Cosa-Linan, A.; Sack, M.; Weber-Fahr, W.; Vollmayr, B.; Sartorius, A. The influence of ketamine’s repeated treatment on brain topology does not suggest an antidepressant efficacy. Transl. Psychiatry 2020, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Olié, E.; Nobile, B.; Courtet, P. The Antisuicidal Effect of Esketamine Should Be Further Investigated. J. Clin. Psychiatry 2020, 81, 20l13482. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.S.; Palanca, B.; Ances, B.M.; Kharasch, E.D.; Schweiger, J.A.; Yingling, M.D.; Snyder, A.Z.; Nicol, G.E.; Lenze, E.J.; Farber, N.B. Prolonged ketamine infusion modulates limbic connectivity and induces sustained remission of treatment-resistant depression. Psychopharmacology 2021, 238, 1157–1169. [Google Scholar]
- Witt, K.; Potts, J.; Hubers, A.; Grunebaum, M.F.; Murrough, J.W.; Loo, C.; Cipriani, A.; Hawton, K. Ketamine for suicidal ideation in adults with psychiatric disorders: A systematic review and meta-analysis of treatment trials. Aust. N. Z. J. Psychiatry 2020, 54, 29–45, Correction in Aust. N. Z. J. Psychiatry 2020, 54, 766. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and metaanalyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 26 May 2021).
- American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1.
- Nijs, M.; Wajs, E.; Aluisio, L.; Turkoz, I.; Daly, E.; Janik, A.; Borentain, S.; Singh, J.B.; DiBernardo, A.; Wiegand, F. Managing Esketamine Treatment Frequency Toward Successful Outcomes: Analysis of Phase 3 Data. Int. J. Neuropsychopharmacol. 2020, 23, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, S.A. Long-term treatment of depression. Br. J. Psychiatry Suppl. 1994, 26, 31–36. [Google Scholar] [CrossRef]
- Buoli, M.; Cumerlato Melter, C.; Caldiroli, A.; Altamura, A.C. Are antidepressants equally effective in the long-term treatment of major depressive disorder? Hum. Psychopharmacol. 2015, 30, 21–27. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Phase | Sample | Age Mean (SD), y | Design | Country | Dosage | Duration | Risk of Bias | Long-Term Outcome Measures | Results | Cohen’s d |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Daly et al., 2018 [26] (1) * | II | 57 | 44.7 (10.04) | Multicenter: -screening; -double-blind treatment (days 1–8 and 8–15): PBO/PBO or PBO/ESK or ESK/ESK -optional open-label treatment (days 15–74) -post-treatment follow-up (days 74–130) | United States and Belgium | Flexible dose Range: 28–84 mg, weekly for 3 weeks, then every 2 weeks | 8.5 weeks | High 1 | MADRS | Response rates after post-treatment follow-up a,b: PBO/PBO: 100% PBO/ESK: 50% ESK/ESK: 61% Remission rates after post treatment follow-up a,b: PBO/PBO: 33% PBO/ESK: 40% ESK/ESK: 28% | Responders: d = −0.185 Remitters: d = −0.245 |
| Daly et al., 2019 [27] SUSTAIN I (1) * | III | 297 | 46.3 (11.13) | Multicenter: -screening and prospective observation phase -open-label induction phase (4 weeks) -fixed-dose optimization phase (12 weeks) -Responders and remitters→ flexible-dose randomized maintenance phase (relapsed during maintenance → long-term safety study) -post-treatment follow-up (2 weeks) | United States, Canada, Europe | Responders: 56 mg or 84 mg once weekly Remitters: 56 mg or 84 mg/2 weeks | Median among responders: 19.4 weeks Median among remitters: 17.7 weeks | Low 1 | -Time to relapse (median) -MADRS | Responders c: PBO > ESK (p < 0.001) PBO: 88.0 days ESK: 635.0 days Remitters c: PBO > ESK (p = 0.003) PBO: 273.0 days ESK: NE Relapse rates: -Responders: PBO: 57.6% ESK: 25.8% -Remitters: PBO: 45.3% ESK: 26.7% | Responders: d = −0.288 Remitters: d = −0.171 Responders: d = −0.751 Remitters: d = −0.455 |
| Wajs et al., 2020 [28] SUSTAIN II (2) * | III | 150 | 52.2 (±13.7) | Multicenter, open-label: -screening (4 weeks) -induction phase (4 weeks) -optimization/maintenance phase (48 weeks) -follow-up phase (4 weeks) | United States, United Kingdom, Argentina, Brazil, Europe, Republic of Korea, Malaysia, Mexico, South Africa, Australia, Taiwan, Turkey | Flexible dose range (28-mg, 56-mg, or 84-mg) | 48 weeks | Moderate 2 | -MADRS -PHQ-9 -SDS | MADRS: Responders 76.5% Remitters 58.2% PHQ-9: Responders 74.6% Remitters 47.4% SDS: Responders 63.0% Remitters 39.5% | - |
| Reference | Phase | Sample | Age Mean (SD), y | Design | Country | Duration | Risk of Bias | Long-Term Outcome Measures | Results | Cohen’s d |
|---|---|---|---|---|---|---|---|---|---|---|
| Canuso et al., 2018 [30] (1) * | II | 44 pts at imminent risk for suicide | 35.8 (13.03) | Double-blind RCT: -screening (24–48 h) -double-blind treatment (days 1–25) -post-treatment follow-up (days 26–81) | 11 sites at United States | 8 weeks | High 1 | -MADRS -BECK Scale for Suicide Ideation -BECK Hopelessness Scale -Remission rates a | -ESK = PBO (p = 0.21) -ESK = PBO (p = 0.84) -ESK = PBO (p = 0.35) -PBO = 50% ESK = 59.3% | d = –0.069 d = –0.257 d = 0.030 d = 0.207 |
| Fu et al., 2020 [31] ASPIRE I (1) * | III | 84 from ESK group 80 from PBO group | 39.3 (12.91) | Double-blind RCT: -screening (24–48 h) -double-blind treatment (days 1–25) -post-treatment follow-up (days 26–90) | United States, Europe, Asia, South Africa | 9 weeks | Some concerns 1 | -MADRS | Low MADRS scores ESK = PBO (no statistics available) | - |
| Ionescu et al., 2021 [32] ASPIRE II (1) * | III | 81 from ESK group 85 from PBO group | 40.8 (13.07) | ≈ | United States, Canada, Argentina, Brazil, Europe, Turkey | ≈ | Low 1 | -MADRS -CGI-SS-r | -low MADRS and CGI-SS-r scores ESK = PBO (no statistics available) | - |
| Daly et al., 2018 [26] (1) * | II | 41 | 44.7 (10.04) | Multicenter: -screening -double-blind treatment (days 1–8 and 8–15): PBO/PBO or PBO/ESK or ESK/ESK -optional open-label treatment (days 15–74) -post-treatment follow-up (days 74–130) | United States and Belgium | 8 weeks | High 1 | MADRS | Response rates b: PBO/PBO: 71% PBO/ESK: 25% ESK/ESK: 68% Remission rates b: PBO/PBO: 57% PBO/ESK: 25% ESK/ESK: 46% | Responders: d = 0.596 Remitters: d = 0.197 |
| NCT02918318 [29] (1) * | II | 68 | 43.4 (10.35) | Double-blind induction phase (4 weeks) -Responders—post-treatment phase (relapsed during post-treatment—open-label induction phase with ESK at flexible dose) -Non-responders—DB Follow-up Phase (4 weeks) | Japan | 24 weeks | Low 1 | Time to relapse (median) in participants with response a | ESK28: 32.0 days ESK56: 26.0 days ESK84: 79.5 days PBO: 91.0 days | -- |
| ≈ | II | 37 | ≈ | ≈ | Japan | ≈ | Low 1 | Time to relapse (median) in participants with remission a | ESK28: 34.0 days ESK56: 52.0 days ESK84: 37.0 days PBO: 30.0 days | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capuzzi, E.; Caldiroli, A.; Capellazzi, M.; Tagliabue, I.; Marcatili, M.; Colmegna, F.; Clerici, M.; Buoli, M.; Dakanalis, A. Long-Term Efficacy of Intranasal Esketamine in Treatment-Resistant Major Depression: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 9338. https://doi.org/10.3390/ijms22179338
Capuzzi E, Caldiroli A, Capellazzi M, Tagliabue I, Marcatili M, Colmegna F, Clerici M, Buoli M, Dakanalis A. Long-Term Efficacy of Intranasal Esketamine in Treatment-Resistant Major Depression: A Systematic Review. International Journal of Molecular Sciences. 2021; 22(17):9338. https://doi.org/10.3390/ijms22179338
Chicago/Turabian StyleCapuzzi, Enrico, Alice Caldiroli, Martina Capellazzi, Ilaria Tagliabue, Matteo Marcatili, Fabrizia Colmegna, Massimo Clerici, Massimiliano Buoli, and Antonios Dakanalis. 2021. "Long-Term Efficacy of Intranasal Esketamine in Treatment-Resistant Major Depression: A Systematic Review" International Journal of Molecular Sciences 22, no. 17: 9338. https://doi.org/10.3390/ijms22179338
APA StyleCapuzzi, E., Caldiroli, A., Capellazzi, M., Tagliabue, I., Marcatili, M., Colmegna, F., Clerici, M., Buoli, M., & Dakanalis, A. (2021). Long-Term Efficacy of Intranasal Esketamine in Treatment-Resistant Major Depression: A Systematic Review. International Journal of Molecular Sciences, 22(17), 9338. https://doi.org/10.3390/ijms22179338