
Effect of Acupuncture on Diabetic Neuropathy: A Narrative Review


Abstract
:1. Introduction
2. Results
2.1. Studies Conducted in Rodents
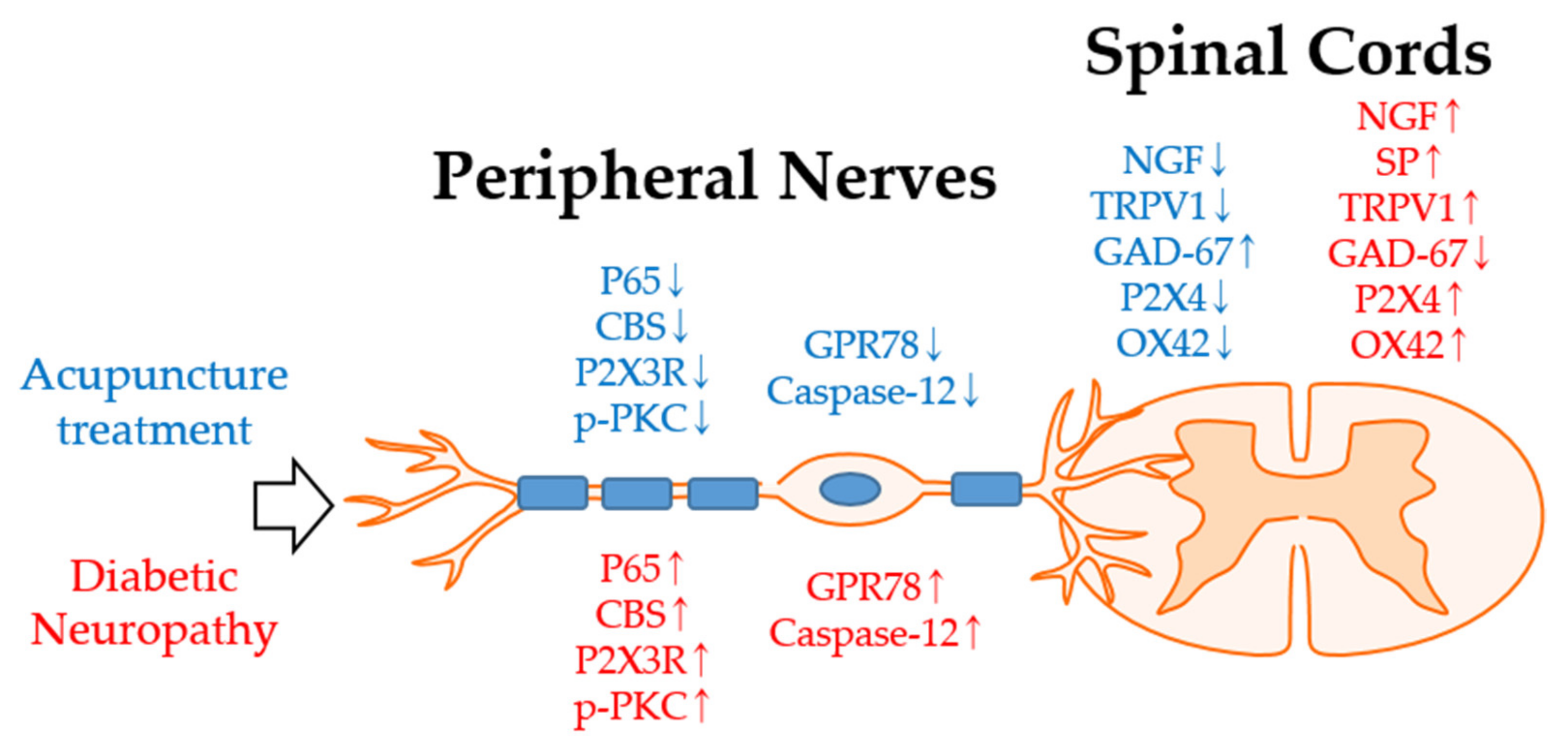
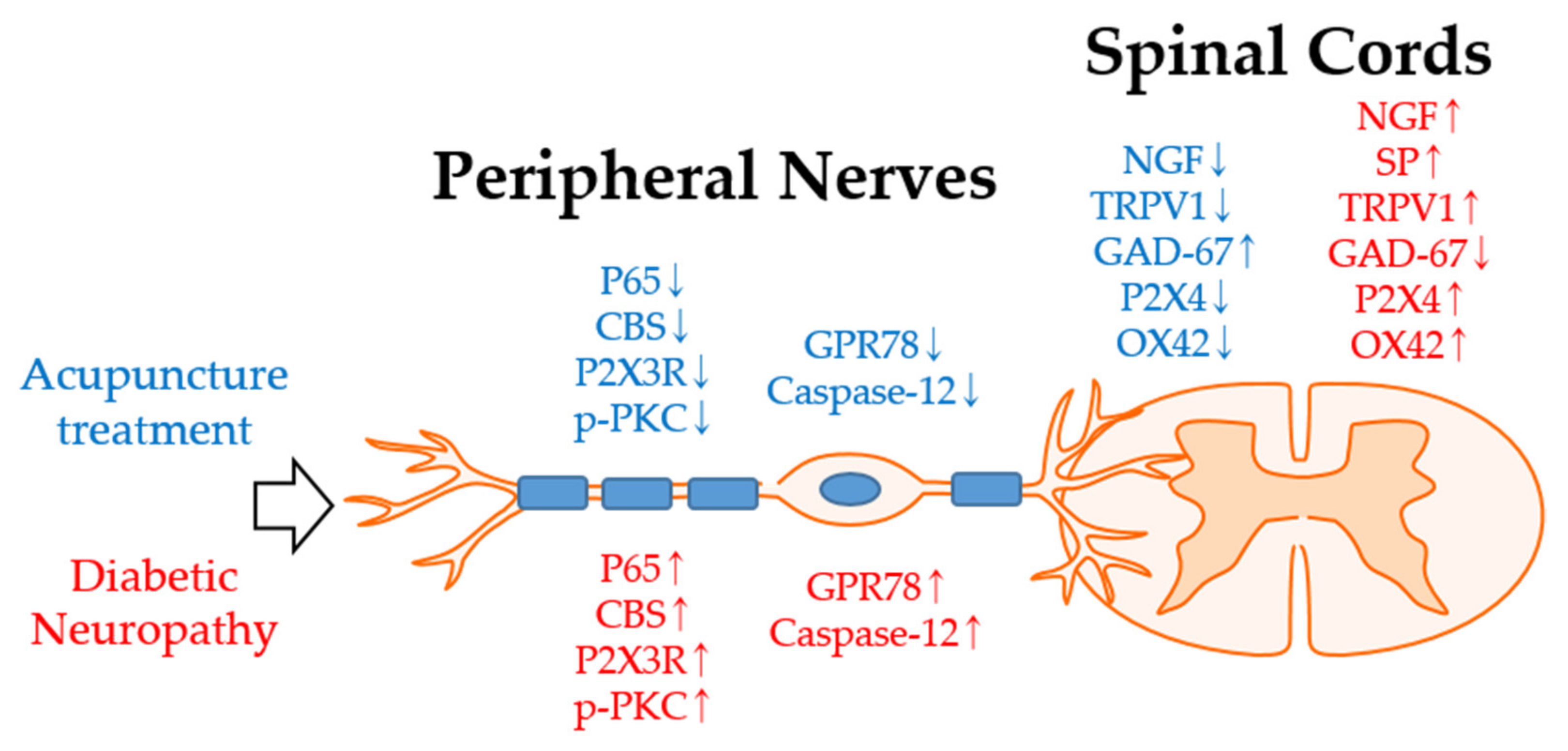
2.1.1. Effect of Acupuncture in the Dorsal Root Ganglion (DRG) in Diabetic Neuropathy Alleviation
2.1.2. Effect of Acupuncture in the Spinal Cord in Diabetic Neuropathy Alleviation

{kind=link}
| Authors | Type of Animal | Diabetic Neuropathy | Acupuncture Treatment ① Acupuncture Types ② Acupoints ③ Retention Time ④ Treatment Duration (Sessions) ⑤ Frequency ⑥ Intensity ⑦ Control to Acupuncture | Findings | |
|---|---|---|---|---|---|
| Manni et al., 2011 [51] | SD Rats Female | Single STZ, 65 mg/kg, i.p., >16.65 mM | ① | EA | STZ decreased latency of response to heat stimuli one to four weeks after administration (p < 0.05 vs. naive). EA at ST36 significantly increased the heat latency time at 4 weeks (p < 0.05 vs. control). STZ increased NGF levels both in the skin and in the spinal cord. EA only lowered that of the spinal cord (p < 0.05 vs. control). STZ increased SP levels in the skin but decreased in the spinal cord. EA only lowered that of the skin (p < 0.05 vs. control). STZ increased TrkA and pTyr496-TrkA levels in the skin. EA significantly decreased both (p < 0.05 vs. control). STZ significantly increased TRPV1 levels in the skin and the spinal cord. EA increased the TRPV1 level in the skin (p < 0.05 vs. control), whereas it decreased in the spinal cord (p < 0.05 vs. control). STZ decreased GAD-67 protein content in the spinal cord and EA significantly restored it (p < 0.05 vs. control). |
| ② | ST36 | ||||
| ③ | 30 min | ||||
| ④ | 3 weeks (6) | ||||
| ⑤ | 2 Hz | ||||
| ⑥ | 1.0–1.5 mA | ||||
| ⑦ | STZ alone | ||||
| Shi et al., 2013 [35] | SD Rats Female | Single STZ, 65 mg/kg, i.p., >16.7 mM | ① | EA | Single STZ injection-induced mechanical allodynia from week 2 to 6 (p < 0.01 vs. naive). Single EA treatment at ST36 significantly increased the mechanical allodynia from 2 h to 4 h compared to control (p < 0.05). EA on BL43 showed no significant effect compared to sham. Multiple EA treatment significantly increased the PWTs starting from 30 min to D5 (p < 0.05 vs. control). Multiple EA on BL43 did not show significant differences. Multiple EA treatment suppresses p65 and CBS expression in L4-6 DRG (p < 0.05 vs. control). |
| ② | ST36, BL43 | ||||
| ③ | 30 min | ||||
| ④ | One week (7) | ||||
| ⑤ | 2/100 Hz | ||||
| ⑥ | 1 mA | ||||
| ⑦ | EA at ST36 without electrical stimulation | ||||
| Zhou et al., 2018 [37] | SD Rats Male | Single STZ, 35 mg/kg, i.p., ≥11.1 mM | ① | EA | Single STZ injection induced mechanical allodynia 7 weeks after its injection (p < 0.01 vs. naive). EA treatment for 7 consecutive days on week 7 significantly attenuated mechanical allodynia (p < 0.01 vs. control). EA failed to improve myelin disruption and dissolute axoplasm of sciatic nerve induced by STZ. EA suppressed STZ induced upregulation of blood membrane protein levels of P2X3 receptor and p-PKC expressions in L4-6 DRG (p < 0.01 vs. control) Intraperitoneal injection of αβ-meATP or PMA inhibited the anti-allodynic effect of EA. PMA injection reversed downregulation of the plasma membrane protein levels of P2X3 receptors in the DRG. |
| ② | ST36, BL60 | ||||
| ③ | 30 min | ||||
| ④ | One week (7) | ||||
| ⑤ | 2 Hz | ||||
| ⑥ | 1–2 mA | ||||
| ⑦ | STZ alone | ||||
| Pan et al., 2019 [45] | SD Rats Male | Single STZ, 50 mg/kg, i.p., ≥16.7 mM | ① | EA | EA significantly increased the decreased heat sensitivity on week 14 (vs. control). EA significantly increased downregulated MCV and SCV (vs. control). MCV of naive group; 50.67 ± 10.71 m/s to 50.86 ± 11.04 m/s, control group; 45.00 ± 9.44 m/s to 20.63 ± 10.27 m/s, EA group; 43.84 ± 9.14 m/s to 30.26 ± 8.96 m/s. SCV of naive group; 51.26 ± 8.93 m/s to 48.32 ± 12.01 m/s; control group; 46.28 ± 11.65 m/s to 21.43 ± 11.51 m/s, EA group; 45.13 ± 9.49 m/s to 29.54 ± 9.39 m/s. EA ameliorated loose with irregular membranous masses myelin sheaths and damaged myelinated nerve fibers induced by STZ injection. EA decreased the upregulated proportion of apoptotic cells (vs. control). EA lowered mean level of GPR78 and Caspase-12. GRP78 of naive group; 0.21 ± 0.05, control; 0.48 ± 0.18, EA group; 0.29 ± 0.07. Caspase-12 of naive group; 0.22 ± 0.07, control; 0.48 ± 0.28, EA group; 0.26 ± 0.04. |
| ② | BL13, BL20, BL23, LI4, LR3, ST36, SP6 | ||||
| ③ | 20 min | ||||
| ④ | 12 weeks (72) | ||||
| ⑤ | 3 Hz | ||||
| ⑥ | - | ||||
| ⑦ | STZ alone | ||||
| Tang et al., 2020 [60] | SD Rats Male | Single STZ, 35 mg/kg, i.p., ≥11.1 mM | ① | Manual acupuncture | Acupuncture treatment increased STZ-induced lowered MWT and TWL at D14 (p < 0.001) and D7-D14 (p < 0.05 (D7) and p < 0.001 (D10, D14)), respectively. Acupuncture lowered the serum levels of CXCR3, IL-1β, IL-6 and TNF-α significantly increased after STZ injection (p < 0.001 vs. control) at D14. Acupuncture lowered the serum level of GSP, TG, TC, LDL-C, and elevated the level of HDL-C altered due to STZ injection (p < 0.001 vs. control) at D14. Acupuncture reduced the increased expression of spinal P2X4 and OX42 expression (p < 0.001 vs. control). |
| ② | BL13, BL20, V23 | ||||
| ③ | 20 min | ||||
| ④ | 2 weeks (14) | ||||
| ⑤ | - | ||||
| ⑥ | - | ||||
| ⑦ | STZ alone | ||||
2.2. Effects of Acupuncture in Studies Conducted in Humans
2.3. Outcomes in Clinical Studies
2.3.1. Patients-Related Outcomes
2.3.2. Neuropathy Disability Score (NDS)
2.3.3. Vibration Perception Threshold (VPT)
2.3.4. Nerve Conduction Velocity
2.3.5. Side Effects
2.3.6. Most Used Acupoints
3. Discussion
4. Methods
Author Contributions
Funding
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2020; pp. 12–15.
- Boulton, A.J.; Malik, R.A. Diabetic neuropathy. Med. Clin. N. Am. 1998, 82, 909–929. [Google Scholar] [CrossRef]
- Callaghan, B.C.; Price, R.S.; Chen, K.S.; Feldman, E.L. The importance of rare subtypes in diagnosis and treatment of peripheral neuropathy: A review. JAMA Neurol. 2015, 72, 1510–1518. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.L.; Albers, J.W.; Pop-Busui, R. Neuropathy and related findings in the diabetes control and complications trial/epidemiology of diabetes interventions and complications study. Diabetes Care 2014, 37, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Malik, R.; Newrick, P.; Sharma, A.; Jennings, A.; Ah-See, A.; Mayhew, T.; Jakubowski, J.; Boulton, A.; Ward, J. Microangiopathy in human diabetic neuropathy: Relationship between capillary abnormalities and the severity of neuropathy. Diabetologia 1989, 32, 92–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bommer, C.; Heesemann, E.; Sagalova, V.; Manne-Goehler, J.; Atun, R.; Bärnighausen, T.; Vollmer, S. The global economic burden of diabetes in adults aged 20–79 years: A cost-of-illness study. Lancet Diabetes Endocrinol. 2017, 5, 423–430. [Google Scholar] [CrossRef]
- Boyle, J.P.; Thompson, T.J.; Gregg, E.W.; Barker, L.E.; Williamson, D.F. Projection of the year 2050 burden of diabetes in the us adult population: Dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul. Health Metr. 2010, 8, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltier, A.; Goutman, S.A.; Callaghan, B.C. Painful diabetic neuropathy. BMJ Clin. Res. Ed. 2014, 348, g1799. [Google Scholar] [CrossRef] [Green Version]
- Alleman, C.J.; Westerhout, K.Y.; Hensen, M.; Chambers, C.; Stoker, M.; Long, S.; van Nooten, F.E. Humanistic and economic burden of painful diabetic peripheral neuropathy in europe: A review of the literature. Diabetes Res. Clin. Pract. 2015, 109, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Garcia, M.K.; Chang, D.Z.; Chiang, J.; Lu, J.; Yi, Q.; Romaguera, J.; Delasalle, K.; Guo, Y.; Forman, A.; et al. Multiple myeloma, painful neuropathy, acupuncture? Am. J. Clin. Oncol. 2009, 32, 319–325. [Google Scholar] [CrossRef]
- Benbow, S.; Wallymahmed, M.; MacFarlane, I. Diabetic peripheral neuropathy and quality of life. QJM Mon. J. Assoc. Physicians 1998, 91, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Ang, L.; Cowdin, N.; Mizokami-Stout, K.; Pop-Busui, R. Update on the management of diabetic neuropathy. Diabetes Spectr. 2018, 31, 224–233. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, D.; Low, P.A.; Litchy, W.J.; Boulton, A.J.; Vinik, A.I.; Freeman, R.; Samigullin, R.; Tritschler, H.; Munzel, U.; Maus, J.; et al. Efficacy and safety of antioxidant treatment with α-lipoic acid over 4 years in diabetic polyneuropathy: The nathan 1 trial. Diabetes Care 2011, 34, 2054–2060. [Google Scholar] [CrossRef] [Green Version]
- Fraser, D.A.; Diep, L.M.; Hovden, I.A.; Nilsen, K.B.; Sveen, K.A.; Seljeflot, I.; Hanssen, K.F. The effects of long-term oral benfotiamine supplementation on peripheral nerve function and inflammatory markers in patients with type 1 diabetes: A 24-month, double-blind, randomized, placebo-controlled trial. Diabetes Care 2012, 35, 1095–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attal, N.; Cruccu, G.; Baron, R.; Haanpää, M.; Hansson, P.; Jensen, T.S.; Nurmikko, T. Efns guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur. J. Neurol. 2010, 17, 1113-e88. [Google Scholar] [CrossRef] [PubMed]
- Bril, V.; England, J.; Franklin, G.M.; Backonja, M.; Cohen, J.; Del Toro, D.; Feldman, E.; Iverson, D.J.; Perkins, B.; Russell, J.W.; et al. Evidence-based guideline: Treatment of painful diabetic neuropathy: Report of the american academy of neurology, the american association of neuromuscular and electrodiagnostic medicine, and the american academy of physical medicine and rehabilitation. Neurology 2011, 76, 1758–1765. [Google Scholar] [CrossRef] [Green Version]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Griebeler, M.L.; Morey-Vargas, O.L.; Brito, J.P.; Tsapas, A.; Wang, Z.; Carranza Leon, B.G.; Phung, O.J.; Montori, V.M.; Murad, M.H. Pharmacologic interventions for painful diabetic neuropathy: An umbrella systematic review and comparative effectiveness network meta-analysis. Ann. Intern. Med. 2014, 161, 639–649. [Google Scholar] [CrossRef]
- Waldfogel, J.M.; Nesbit, S.A.; Dy, S.M.; Sharma, R.; Zhang, A.; Wilson, L.M.; Bennett, W.L.; Yeh, H.C.; Chelladurai, Y.; Feldman, D.; et al. Pharmacotherapy for diabetic peripheral neuropathy pain and quality of life: A systematic review. Neurology 2017, 88, 1958–1967. [Google Scholar] [CrossRef]
- Hu, J. Clinical observation on 25 cases of hormone dependent bronchial asthma treated by acupuncture. J. Tradit. Chin. Med. Chung I Tsa Chih Ying Wen Pan 1998, 18, 27–30. [Google Scholar]
- Biernacki, W.; Peake, M.D. Acupuncture in treatment of stable asthma. Respir. Med. 1998, 92, 1143–1145. [Google Scholar] [CrossRef] [Green Version]
- Molsberger, A.; Hille, E. The analgesic effect of acupuncture in chronic tennis elbow pain. Br. J. Rheumatol. 1994, 33, 1162–1165. [Google Scholar] [CrossRef]
- Chou, P.-C.; Chu, H.-Y. Clinical efficacy of acupuncture on rheumatoid arthritis and associated mechanisms: A systemic review. Evid. Based Complement. Altern. Med. 2018, 2018, 8596918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haker, E.; Lundeberg, T. Laser treatment applied to acupuncture points in lateral humeral epicondylalgia. A double-blind study. Pain 1990, 43, 243–247. [Google Scholar] [CrossRef]
- Wong, C.W.-Y.; Ng, E.Y.-L.; Fung, P.-W.; Mok, K.-M.; Yung, P.S.-H.; Chan, K.-M. Comparison of treatment effects on lateral epicondylitis between acupuncture and extracorporeal shockwave therapy. Asia Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2017, 7, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Zijlstra, F.J.; van den Berg-de Lange, I.; Huygen, F.J.P.M.; Klein, J. Anti-inflammatory actions of acupuncture. Mediat. Inflamm. 2003, 12, 807126. [Google Scholar] [CrossRef]
- Korpan, M.I.; Dezu, Y.; Schneider, B.; Leitha, T.; Fialka-Moser, V. Acupuncture in the treatment of posttraumatic pain syndrome. Acta Orthop. Belg. 1999, 65, 197–201. [Google Scholar] [PubMed]
- Danqing, X. Acupuncture for parkinson’s disease: A review of clinical, animal, and functional magnetic resonance imaging studies. J. Tradit. Chin. Med. 2015, 35, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Cao, L.; Li, X.; Li, M.; Yao, L.; Hou, L.; Zhang, W.; Wang, Y.; Niu, J.; Yang, K. The effectiveness of acupuncture for parkinson’s disease: An overview of systematic reviews. Complement. Ther. Med. 2020, 50, 102383. [Google Scholar] [CrossRef]
- Yuan, J.; Purepong, N.; Kerr, D.P.; Park, J.; Bradbury, I.; McDonough, S. Effectiveness of acupuncture for low back pain: A systematic review. Spine 2008, 33, E887–E900. [Google Scholar] [CrossRef]
- Linde, K.; Allais, G.; Brinkhaus, B.; Manheimer, E.; Vickers, A.; White, A.R. Acupuncture for tension-type headache. Cochrane Database Syst. Rev. 2009, 1, CD007587. [Google Scholar]
- Pandey, A.; Tripathi, P.; Pandey, R.; Srivatava, R.; Goswami, S. Alternative therapies useful in the management of diabetes: A systematic review. J. Pharm. Bioallied Sci. 2011, 3, 504. [Google Scholar] [PubMed]
- Liang, F.; Koya, D. Acupuncture: Is it effective for treatment of insulin resistance? Diabetes Obes. Metab. 2010, 12, 555–569. [Google Scholar] [CrossRef]
- Shi, L.; Zhang, H.H.; Xiao, Y.; Hu, J.; Xu, G.Y. Electroacupuncture suppresses mechanical allodynia and nuclear factor κ b signaling in streptozotocin-induced diabetic rats. CNS Neurosci. Ther. 2013, 19, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Bisby, M.A. Increased activation of nuclear factor kappa b in rat lumbar dorsal root ganglion neurons following partial sciatic nerve injuries. Brain Res. 1998, 797, 243–254. [Google Scholar] [CrossRef]
- Zhou, Y.F.; Ying, X.M.; He, X.F.; Shou, S.Y.; Wei, J.J.; Tai, Z.X.; Shao, X.M.; Liang, Y.; Fang, F.; Fang, J.Q.; et al. Suppressing pkc-dependent membrane p2x3 receptor upregulation in dorsal root ganglia mediated electroacupuncture analgesia in rat painful diabetic neuropathy. Purinergic Signal. 2018, 14, 359–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Y.; Xu, C.; Liang, S.; Zhang, A.; Mu, S.; Wang, Y.; Wan, F. Effect of tetramethylpyrazine on primary afferent transmission mediated by p2x3 receptor in neuropathic pain states. Brain Res. Bull. 2008, 77, 27–32. [Google Scholar] [CrossRef]
- Liang, S.; Xu, C.; Li, G.; Gao, Y. P2x receptors and modulation of pain transmission: Focus on effects of drugs and compounds used in traditional chinese medicine. Neurochem. Int. 2010, 57, 705–712. [Google Scholar] [CrossRef]
- Novakovic, S.D.; Kassotakis, L.C.; Oglesby, I.B.; Smith, J.A.; Eglen, R.M.; Ford, A.P.; Hunter, J.C. Immunocytochemical localization of p2x3 purinoceptors in sensory neurons in naive rats and following neuropathic injury. Pain 1999, 80, 273–282. [Google Scholar] [CrossRef]
- Velázquez, K.T.; Mohammad, H.; Sweitzer, S.M. Protein kinase c in pain: Involvement of multiple isoforms. Pharmacol. Res. 2007, 55, 578–589. [Google Scholar] [CrossRef] [Green Version]
- Ahlgren, S.C.; Levine, J.D. Protein kinase c inhibitors decrease hyperalgesia and c-fiber hyperexcitability in the streptozotocin-diabetic rat. J. Neurophysiol. 1994, 72, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-C.; Akopian, A.N.; Sivilottit, L.; Colquhoun, D.; Burnstock, G.; Wood, J.N. A p2x purinoceptor expressed by a subset of sensory neurons. Nature 1995, 377, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Besson, A.; Davy, A.; Robbins, S.M.; Yong, V.W. Differential activation of erks to focal adhesions by pkc ε is required for pma-induced adhesion and migration of human glioma cells. Oncogene 2001, 20, 7398–7407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, H.; Huang, H.; Zhang, L.; Ma, S.; Yang, H.; Wang, H. “Adjusting internal organs and dredging channel” electroacupuncture treatment prevents the development of diabetic peripheral neuropathy by downregulating glucose-related protein 78 (grp78) and caspase-12 in streptozotocin-diabetic rats. J. Diabetes 2019, 11, 928–937. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Zhao, J.; Zhang, J.; Mei, J.; Shao, M.; Pan, Y.; Yang, W.; Jiang, Y.; Liu, F.; Jia, W. Heparan sulfate inhibits inflammation and improves wound healing by downregulating the nlr family pyrin domain containing 3 (nlrp3) inflammasome in diabetic rats. J. Diabetes 2018, 10, 556–563. [Google Scholar] [CrossRef] [Green Version]
- Cameron, N.E. Role of endoplasmic reticulum stress in diabetic neuropathy. Diabetes 2013, 62, 696–697. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.R.; Nguyen, L.X.; Sargent, K.E.; Lipson, K.L.; Hackett, A.; Urano, F. Higher stress in beta-cells stimulates intracellular degradation of misfolded insulin. Biochem. Biophys. Res. Commun. 2004, 324, 166–170. [Google Scholar] [CrossRef]
- Kaufman, R.J. Stress signaling from the lumen of the endoplasmic reticulum: Coordination of gene transcriptional and translational controls. Genes Dev. 1999, 13, 1211–1233. [Google Scholar] [CrossRef] [Green Version]
- Omura, T.; Kaneko, M.; Okuma, Y.; Matsubara, K.; Nomura, Y. Endoplasmic reticulum stress and parkinson’s disease: The role of hrd1 in averting apoptosis in neurodegenerative disease. Oxid. Med. Cell. Longev. 2013, 2013, 239854. [Google Scholar] [CrossRef]
- Manni, L.; Florenzano, F.; Aloe, L. Electroacupuncture counteracts the development of thermal hyperalgesia and the alteration of nerve growth factor and sensory neuromodulators induced by streptozotocin in adult rats. Diabetologia 2011, 54, 1900–1908. [Google Scholar] [CrossRef] [Green Version]
- Xing, G.G.; Liu, F.Y.; Qu, X.X.; Han, J.S.; Wan, Y. Long-term synaptic plasticity in the spinal dorsal horn and its modulation by electroacupuncture in rats with neuropathic pain. Exp. Neurol. 2007, 208, 323–332. [Google Scholar] [CrossRef]
- Han, J.S. Acupuncture and endorphins. Neurosci. Lett. 2004, 361, 258–261. [Google Scholar] [CrossRef]
- Bennett, D.L. Neurotrophic factors: Important regulators of nociceptive function. Neuroscientist 2001, 7, 13–17. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, J.; McNaughton, P.A. Ngf rapidly increases membrane expression of trpv1 heat-gated ion channels. EMBO J. 2005, 24, 4211–4223. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, D.R.; Fernyhough, P.; Diemel, L.T. Neurotrophins and peripheral neuropathy. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 1996, 351, 455–462. [Google Scholar]
- Park, J.H.; Han, J.B.; Kim, S.K.; Park, J.H.; Go, D.H.; Sun, B.; Min, B.I. Spinal gaba receptors mediate the suppressive effect of electroacupuncture on cold allodynia in rats. Brain Res. 2010, 1322, 24–29. [Google Scholar] [CrossRef]
- Jolivalt, C.G.; Lee, C.A.; Ramos, K.M.; Calcutt, N.A. Allodynia and hyperalgesia in diabetic rats are mediated by gaba and depletion of spinal potassium-chloride co-transporters. Pain 2008, 140, 48–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heese, K.; Otten, U.; Mathivet, P.; Raiteri, M.; Marescaux, C.; Bernasconi, R. Gaba(b) receptor antagonists elevate both mrna and protein levels of the neurotrophins nerve growth factor (ngf) and brain-derived neurotrophic factor (bdnf) but not neurotrophin-3 (nt-3) in brain and spinal cord of rats. Neuropharmacology 2000, 39, 449–462. [Google Scholar] [CrossRef]
- Tang, H.Y.; Wang, F.J.; Ma, J.L.; Wang, H.; Shen, G.M.; Jiang, A.J. Acupuncture attenuates the development of diabetic peripheral neuralgia by regulating p2x4 expression and inflammation in rat spinal microglia. J. Physiol. Sci. 2020, 70, 45. [Google Scholar] [CrossRef]
- DeLeo, J.A.; Tanga, F.Y.; Tawfik, V.L. Neuroimmune activation and neuroinflammation in chronic pain and opioid tolerance/hyperalgesia. Neuroscientist 2004, 10, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Du, J.Y.; Qiu, Y.J.; Fang, J.F.; Liu, J.; Fang, J.Q. Electroacupuncture attenuates spinal nerve ligation-induced microglial activation mediated by p38 mitogen-activated protein kinase. Chin. J. Integr. Med. 2016, 22, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Hamme, G.; Friedemann, T.; Greten, H.J.; Plaetke, R.; Gerloff, C.; Schroeder, S. Acudin–acupuncture and laser acupuncture for treatment of diabetic peripheral neuropathy: A randomized, placebo-controlled, partially double-blinded trial. BMC Neurol. 2018, 18, 40. [Google Scholar] [CrossRef] [Green Version]
- Rajchgot, T.; Thomas, S.C.; Wang, J.-C.; Ahmadi, M.; Balood, M.; Crosson, T.; Dias, J.P.; Couture, R.; Claing, A.; Talbot, S. Neurons and microglia; a sickly-sweet duo in diabetic pain neuropathy. Front. Neurosci. 2019, 13, 25. [Google Scholar] [CrossRef]
- Beggs, S.; Trang, T.; Salter, M.W. P2x4r+ microglia drive neuropathic pain. Nat. Neurosci. 2012, 15, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.M.; Xu, J.; Song, J.G.; Zheng, B.J.; Wang, X.R. Electroacupuncture inhibits excessive interferon-γ evoked up-regulation of p2x4 receptor in spinal microglia in a cci rat model for neuropathic pain. Br. J. Anaesth. 2015, 114, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abuaisha, B.B.; Costanzi, J.B.; Boulton, A.J. Acupuncture for the treatment of chronic painful peripheral diabetic neuropathy: A long-term study. Diabetes Res. Clin. Pract. 1998, 39, 115–121. [Google Scholar] [CrossRef]
- Asad, A.; Hameed, M.A.; Khan, U.A.; Ahmed, N.; Butt, M.U. Reliability of the neurological scores for assessment of sensorimotor neuropathy in type 2 diabetics. JPMA J. Pak. Med. Assoc. 2010, 60, 166–170. [Google Scholar] [PubMed]
- Garrow, A.P.; Boulton, A.J. Vibration perception threshold—A valuable assessment of neural dysfunction in people with diabetes. Diabetes Metab. Res. Rev. 2006, 22, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Shi, K.; Li, X.; Zhou, W.; Cao, Y. Clinical study on the wrist-ankle acupuncture treatment for 30 cases of diabetic peripheral neuritis. J. Tradit. Chin. Med. Chung I Tsa Chih Ying Wen Pan 2006, 26, 8–12. [Google Scholar]
- Zhang, C.; Ma, Y.X.; Yan, Y. Clinical effects of acupuncture for diabetic peripheral neuropathy. J. Tradit. Chin. Med. Chung I Tsa Chih Ying Wen Pan 2010, 30, 13–14. [Google Scholar] [CrossRef]
- Tong, Y.; Guo, H.; Han, B. Fifteen-day acupuncture treatment relieves diabetic peripheral neuropathy. J. Acupunct. Meridian Stud. 2010, 3, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Sathya, G.R.; Krishnamurthy, N.; Veliath, S.; Arulneyam, J.; Venkatachalam, J. F wave index: A diagnostic tool for peripheral neuropathy. Indian J. Med. Res. 2017, 145, 353–357. [Google Scholar] [PubMed]
- Garrow, A.P.; Xing, M.; Vere, J.; Verrall, B.; Wang, L.; Jude, E.B. Role of acupuncture in the management of diabetic painful neuropathy (dpn): A pilot rct. Acupunct. Med. 2014, 32, 242–249. [Google Scholar] [CrossRef]
- Jeon, E.; Kwon, H.; Shin, I.; Kang, S.; Shon, H. Effect of acupuncture on diabetic peripheral neuropathy: An uncontrolled preliminary study from korea. Acupunct. Med. 2014, 32, 350–352. [Google Scholar] [CrossRef]
- Bailey, A.; Wingard, D.; Allison, M.; Summers, P.; Calac, D. Acupuncture treatment of diabetic peripheral neuropathy in an american indian community. J. Acupunct. Meridian Stud. 2017, 10, 90–95. [Google Scholar] [CrossRef]
- Fronek, A.; DiTomasso, D.G.; Allison, M. Noninvasive assessment of endothelial activity in patients with peripheral arterial disease and cardiovascular risk factors. Endothelium 2007, 14, 199–205. [Google Scholar] [CrossRef]
- Shin, K.M.; Lee, S.; Lee, E.Y.; Kim, C.H.; Kang, J.W.; Lee, C.K.; Seo, B.N.; Kim, A.R.; Jung, S.Y.; Kwon, O.; et al. Electroacupuncture for painful diabetic peripheral neuropathy: A multicenter, randomized, assessor-blinded, controlled trial. Diabetes Care 2018, 41, e141–e142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, M.T.; Schillinger, D.; Nguyen, U.; Santana, T.; Liu, R.; Gregorich, S.; Hecht, F.M. A randomized clinical trial of group acupuncture for painful diabetic neuropathy among diverse safety net patients. Pain Med. 2019, 20, 2292–2302. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z. Principles of acupuncture therapeutics. In Essentials of Chinese Medicine; Springer: Berlin/Heidelberg, Germany, 2010; pp. 592–601. [Google Scholar]
- Maciocia, G. The Foundations of Chinese Medicine; Churchill Livingstone: London, UK, 1989. [Google Scholar]
- Choi, W.; Lee, S.; Cho, S.; Park, K. Differential autonomic response to acupuncture at wood and metal of five-shu acupoints. J. Altern. Complement. Med. 2012, 18, 959–964. [Google Scholar] [CrossRef]
- Stux, G.; Berman, B.; Pomeranz, B. Basics of Acupuncture; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2003. [Google Scholar]
- Meyer-Hamme, G.; Friedemann, T.; Greten, J.; Gerloff, C.; Schroeder, S. Electrophysiologically verified effects of acupuncture on diabetic peripheral neuropathy in type 2 diabetes: The randomized, partially double-blinded, controlled acudin trial. J. Diabetes 2020, 13, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Yin, C.S.; Park, H.-J.; Seo, J.-C.; Lim, S.; Koh, H.-G. An evaluation of the cun measurement system of acupuncture point location. Am. J. Chin. Med. 2005, 33, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, A.; Murchison, C.; Oken, B. Acupuncture for the treatment of peripheral neuropathy: A systematic review and meta-analysis. J. Altern. Complement. Med. 2017, 23, 164–179. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-Q.; Chen, Z.; Zhang, K.; Liang, N.; Yang, G.-Y.; Lai, L.; Liu, J.-P. Zusanli (st36) acupoint injection for diabetic peripheral neuropathy: A systematic review of randomized controlled trials. J. Altern. Complement. Med. 2018, 24, 1138–1149. [Google Scholar] [CrossRef]
- Chen, W.; Yang, G.-Y.; Liu, B.; Manheimer, E.; Liu, J.-P. Manual acupuncture for treatment of diabetic peripheral neuropathy: A systematic review of randomized controlled trials. PLoS ONE 2013, 8, e73764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, J.; Armour, M.; Penkala, S. Acupuncture for the treatment of lower limb diabetic peripheral neuropathy: A systematic review. Acupunct. Med. 2019, 37, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Dan, Y. Clinical observation on therapeutic effects of acupuncture treatment for 100 cases of type ii diabetes. J. Acupunct. Tuina Sci. 2004, 2, 34–35. [Google Scholar] [CrossRef]
- Ulett, G.A.; Han, S.; Han, J.S. Electroacupuncture: Mechanisms and clinical application. Biol. Psychiatry 1998, 44, 129–138. [Google Scholar] [CrossRef]
- Lee, J.H.; Go, D.; Kim, W.; Lee, G.; Bae, H.; Quan, F.S.; Kim, S.K. Involvement of spinal muscarinic and serotonergic receptors in the anti-allodynic effect of electroacupuncture in rats with oxaliplatin-induced neuropathic pain. Korean J. Physiol. Pharmacol. 2016, 20, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Han, J.-S. Acupuncture: Neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003, 26, 17–22. [Google Scholar] [CrossRef]
- Vieira, J.S.; Toreti, J.A.; de Carvalho, R.C.; de Araújo, J.E.; Silva, M.L.; Silva, J.R. Analgesic effects elicited by neuroactive mediators injected into the st 36 acupuncture point on inflammatory and neuropathic pain in mice. J. Acupunct. Meridian Stud. 2018, 11, 280–289. [Google Scholar] [CrossRef]
- Butts, R.; Dunning, J.; Serafino, C. Dry needling strategies for musculoskeletal conditions: Do the number of needles and needle retention time matter? A narrative review of the literature. J. Bodyw. Mov. Ther. 2020, 26, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Khdour, M.R. Treatment of diabetic peripheral neuropathy: A review. J. Pharm. Pharmacol. 2020, 72, 863–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furman, B.L. Streptozotocin-induced diabetic models in mice and rats. Curr. Protoc. Pharmacol. 2015, 70. [Google Scholar] [CrossRef]
- Zuo, L.; Zhang, L. Study on the effect of acupuncture plus methylcobalamin in treating diabetic peripheral neuropathy. J. Acupunct. Tuina Sci. 2010, 8, 249–252. [Google Scholar] [CrossRef]
- Lunn, M.P.; Hughes, R.A.; Wiffen, P.J. Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia. Cochrane Database Syst. Rev. 2014, 1, CD007115. [Google Scholar] [CrossRef]
| Author | Characteristics of Patients | Acupuncture Treatment ① Acupuncture Types ② Acupoints ③ Retention Time ④ Treatment Duration (Sessions) ⑤ Conventional Treatment ⑥ Control to Acupuncture | Outcomes | ||
|---|---|---|---|---|---|
| Patients-Related Outcomes | Nerve-Function Outcomes | ||||
| Abuaisha et al., 1998 [67] | Participants: n = 44 | ① | Manual acupuncture | Improved in primary (74.9 ± 2.4 to 44.5 ± 4.3) and secondary (70.3 ± 2.9 to 43.5 ± 4.2) symptoms: 34/44 (77%) Complete symptoms relief after treatment: 7/34 (21%) No significant change in NDS (7.3 ± 0.5 to 7.2 ± 0.7) | No significant change in VPT (30.4 ± 1.9 to 31.1 ± 2.2 volts) |
| ② | LI3, SP6, SP9, ST36 | ||||
| ③ | 20 min (first week: 5 min) | ||||
| ④ | 10 weeks (6) | ||||
| ⑤ | Analgesics, tricyclic drugs, anticonvulsants (63%) | ||||
| ⑥ | - | ||||
| Jiang et al., 2006 [70] | Participants: n = 90 Wrist-ankle acupuncture: n = 30 Body acupuncture: n = 30 Control: n = 30 | ① | Manual acupuncture | Wrist-ankle acupuncture: 56.67% markedly relieved and 36.67% improved Body acupuncture: 56.67% markedly relieved and 33.33% improved Control: 23.33% markedly relieved and 40.00% improved | Wrist-ankle acupuncture: Improved CV of median (42.12 ± 3.80 → 46.87 ± 5.57 m/s) & common peroneal nerve (41.42 ± 4.47 → 45.45 ± 4.82 m/s) Body acupuncture: Improved CV of median (42.17 ± 4.51 → 45.48 ± 4.92 m/s) & common peroneal nerve (42.12 ± 4.63 → 45.37 ± 4.90 m/s) Control: No change in CV of median (42.22 ± 4.90 → 43.15 ± 5.24 m/s) & common peroneal nerve (42.04 ± 4.53 → 43.91 ± 5.51 m/s) |
| ② | Wrist-ankle acupuncture: upper 2 and lower 2 Body acupuncture: SP6, SP10, KI3, LI11, GB34 Additional acupoints regarding to symptoms applied to both groups | ||||
| ③ | 15–30 min | ||||
| ④ | 25 days (21) | ||||
| ⑤ | - | ||||
| ⑥ | VB1 and VB12, i.m. | ||||
| Zhang et al., 2010 [71] | Participants: n = 65 Acupuncture: n = 32 Control: n = 33 | ① | Manual acupuncture | Acupuncture: 16 markedly relieved, 12 improved, 4 failed Control: 7 markedly relieved, 14 improved, 12 failed | - |
| ② | BL18, BL20, BL23, BL58, ST36, SP6, SP3, CV6, CV4, ST40, GB34, Ex-B3 + acupoints regarding to symptoms | ||||
| ③ | 25 min | ||||
| ④ | 3 months (70) | ||||
| ⑤ | - | ||||
| ⑥ | Inositol, p.o., 2 g/day | ||||
| Tong et al., 2010 [72] | Participants: n = 63 Acupuncture: n = 42 Control: n = 21 | ① | Manual acupuncture | Improved numbness of lower extremities Improved spontaneous pain of lower extremities Improved rigidity in upper extremities Improved alterations in temperature perception in lower extremities | Improved F-wave minimum latency in tibial nerve (52.6 ± 0.5 → 53.0 ± 0.3 m/s) Improved MNCV in tibial nerve (39.5 ± 0.5 → 40.2 ± 3.9 m/s) Improved FCV in median nerve (55.6 ± 0.4 → 56.5 ± 0.5 m/s) Improved SNCV of forearm (47.8 ± 0.5 → 48.3 ± 0.7 m/s) Improved VPT (8.05 ± 3.22 → 8.56 ± 3.43 s) |
| ② | LI4, ST40, LI11, ST36, SP6 | ||||
| ③ | 30 min | ||||
| ④ | 15 days (15) | ||||
| ⑤ | - | ||||
| ⑥ | 0.3 cm (vs. 1.2–2.3 cm) needles insertion without stimulation | ||||
| Garrow et al., 2014 [74] | Participants: n = 45 Acupuncture: n = 24 Control: n = 21 | ① | Manual acupuncture | Improved LANSS score (14.3 ± 6.4 → 13.6 ± 7.2) Improved VAS pain intensity (73 ± 24 → 58 ± 26) Improved MYMOP score (4.3 ± 1.2 → 3.4 ± 1.3) Improved SF-36 physical component score (40.7 ± 13.2 → 39.2 ± 14.0) No change in SF-36 bodily pain score (37.7 ± 27.4 → 40.2 ± 20.2) | - |
| ② | LR3, KI3, SP6, ST36 | ||||
| ③ | 30 min | ||||
| ④ | 10 weeks (10) | ||||
| ⑤ | - | ||||
| ⑥ | Sham acupuncture (blunt and slides into the handle) | ||||
| Jeon et al., 2015 [75] | Participants: n = 9 | ① | Manual acupuncture | No significant change in TSS score (7.99 ± 3.55 → 4.95 ± 4.41) No significant change in MNSI score (6.33 ± 1.31 → 4.33 ± 3.00) | - |
| ② | Ex-LE10, LR3, GB34, GB39, GB41, ST36, SP6, SP9 | ||||
| ③ | 21–28 min | ||||
| ④ | 4 weeks (12) | ||||
| ⑤ | - | ||||
| ⑥ | - | ||||
| Bailey et al., 2017 [76] | Participants: n = 25 | ① | Manual acupuncture | Improved NTSS-6 scores: aching pain (2.4 ± 0.6 → 1.6 ± 0.5) burning pain (1.7 ± 0.7 → 1.0 ± 0.6) tingling and prickling (2.2 ± 0.5 → 1.2 ± 0.6) numbness (1.7 ± 0.6 → 1.0 ± 0.6) allodynia (1.9 ± 0.6 → 1.2 ± 0.7) No significantly different NTSS-6 scores: lancinating pain (2.0 ± 0.6 → 1.6 ± 0.6) NDS (5.2 ± 3.6 → 4.9 ± 3.4) | - |
| ② | EX-LE10, ST32, ST37, ST42, SP7, SP9, KI1, KI3, KI9, LR4, LR7, GB34, GB37 | ||||
| ③ | 30 min | ||||
| ④ | 10 weeks (10) | ||||
| ⑤ | - | ||||
| ⑥ | - | ||||
| Shin et al., 2018 [78] | Participants: n = 126 Acupuncture: n = 63 Control: n = 63 | ① | EA (2/120 Hz) | Improved PI-NRS scores (−0.67 [95% CI−1.29 to −0.06] vs. control) at week 9 Improved short-form McGill pain questionnaire, sleep interference scores, and the EuroQol-5 dimensions at week 9 | No significant difference in nerve conduction velocity |
| ② | ST36, GB39, SP9, SP6, LR3, GB41 + additional acupoints regarding to symptoms (Ex-LE10) | ||||
| ③ | - | ||||
| ④ | 8 weeks (16) | ||||
| ⑤ | Anti-diabetes and rescue medication allowed (acetaminophen 500 mg, max 3000 mg/day) | ||||
| ⑥ | No EA treatment | ||||
| Chao et al., 2019 [79] | Participants: n = 40 Acupuncture (1/week): n = 14 Acupuncture (2/week): n = 12 Control: n = 14 | ① | Manual acupuncture | Improved NRS score (between-group differences): Average pain intensity (−1.86 (week 6), −2.06 (week 12)) Worst pain intensity (−1.88 (week 6), −2.34 (week 12)) Least pain intensity (−1.24 (week 6), −1.46 (week 12)) | - |
| ② | Jing well and shu stream acupoints + acupoints regarding to symptoms (8–12 acupoints) | ||||
| ③ | 20–40 min. | ||||
| ④ | 12 weeks (12 and 24) | ||||
| ⑤ | Antidepressants, opiates, and anticonvulsants | ||||
| ⑥ | No acupuncture treatment | ||||
| Meyer-Hamme et al., 2020 [84] | Participants n = 120 Acupuncture n = 60 Laser acupuncture n = 60 Control n = 60 | ① | Manual and laser acupuncture | Improved 12/12 items of patient-related outcomes in acupuncture group Improved 11/12 items of patient-related outcomes (exclusion: hyperesthesia) in laser acupuncture group Improved 9/12 of patient-related outcomes (exclusion: hyperesthesia, heat sensation, muscle cramps) in control | Improved sural SNAP (μV) in all three groups Improved sural SNCV (m/s) in the manual and laser acupuncture group Improved tibial MNCV (m/s) in the manual acupuncture group No significant difference in tibial MNAP (mV) in all group |
| ② | Ex-LE10, Ex-LE12, ST34 | ||||
| ③ | 20 min | ||||
| ④ | 10 weeks (10) | ||||
| ⑤ | - | ||||
| ⑥ | Laser acupuncture without laser | ||||
| Acupoints | Anatomical Location | Number of Studies Used | References |
|---|---|---|---|
| Ex-LE10 (Bafeng) | Between each proximal phalanx | 4 | [75,76,78,84] |
| GB34 (Yanglingquan) | On the fibular aspect of the leg, in the depression anterior, and distal to the head of the fibula. | 4 | [70,71,75,76] |
| SP6 (Sanyinjiao) | On the tibial aspect of the leg, posterior to the medial border of the tibia, 3 B-cun [85] superior to the prominence of the medial malleolus. | 7 | [67,70,71,72,74,75,78] |
| SP9 (Yinlingquan) | On the tibial aspect of the leg, in the depression between the inferior border of the medial condyle of the tibia, and the medial border of the tibia. | 4 | [67,75,76,78] |
| ST36 (Zusanli) | On the anterior aspect of the leg, on the line connecting ST35 with ST41, 3 B-cun inferior to ST35 | 6 | [67,71,72,74,75,78] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, E.; Kim, W. Effect of Acupuncture on Diabetic Neuropathy: A Narrative Review. Int. J. Mol. Sci. 2021, 22, 8575. https://doi.org/10.3390/ijms22168575
Cho E, Kim W. Effect of Acupuncture on Diabetic Neuropathy: A Narrative Review. International Journal of Molecular Sciences. 2021; 22(16):8575. https://doi.org/10.3390/ijms22168575
Chicago/Turabian StyleCho, Eunwoo, and Woojin Kim. 2021. "Effect of Acupuncture on Diabetic Neuropathy: A Narrative Review" International Journal of Molecular Sciences 22, no. 16: 8575. https://doi.org/10.3390/ijms22168575
APA StyleCho, E., & Kim, W. (2021). Effect of Acupuncture on Diabetic Neuropathy: A Narrative Review. International Journal of Molecular Sciences, 22(16), 8575. https://doi.org/10.3390/ijms22168575