
Prognostic and Therapeutic Implications of Immune Classification by CD8+ Tumor-Infiltrating Lymphocytes and PD-L1 Expression in Sinonasal Squamous Cell Carcinoma

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Clinical Features and Follow-Up
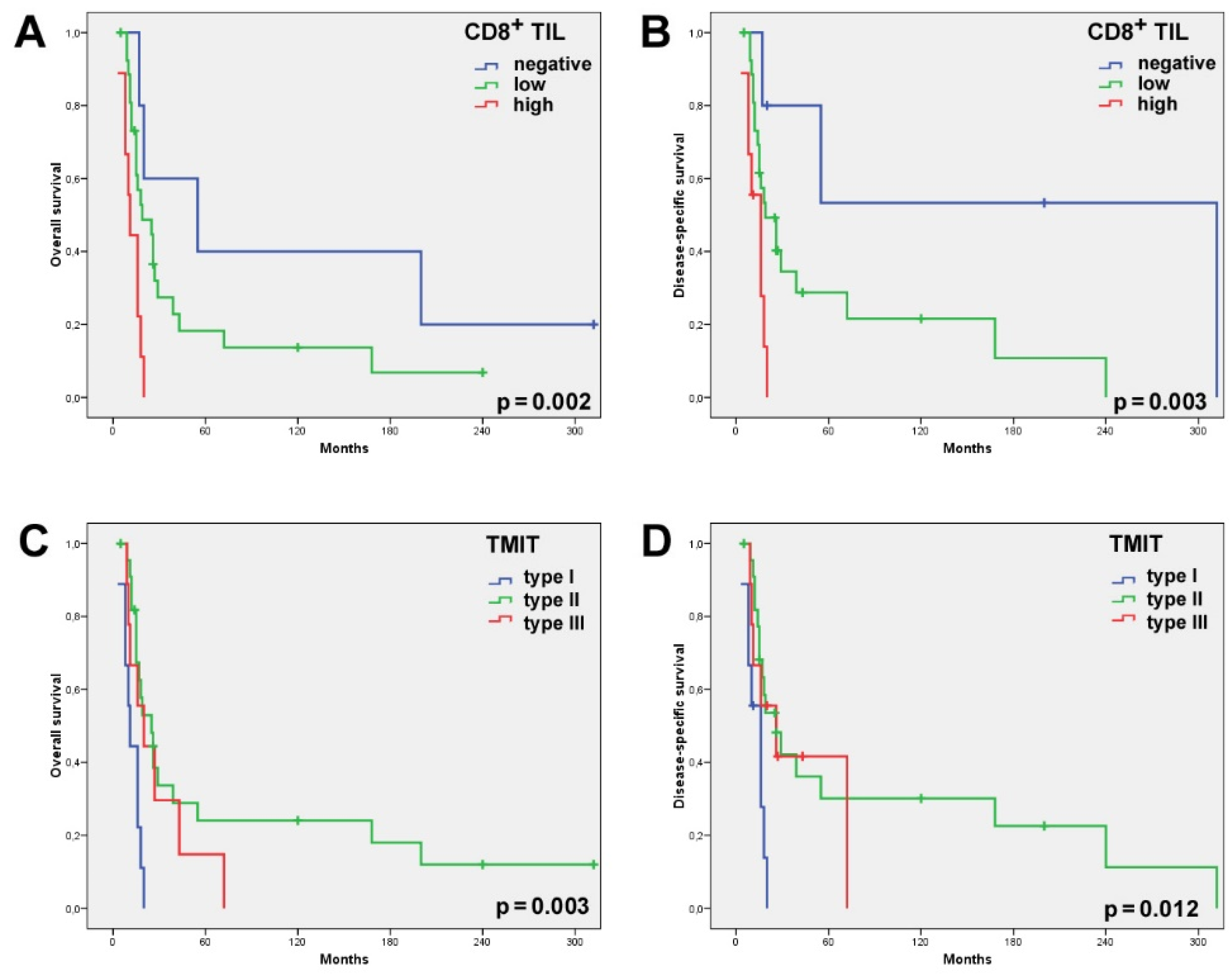
2.2. CD8+ TILs and Correlation with the Clinical and Survival Data
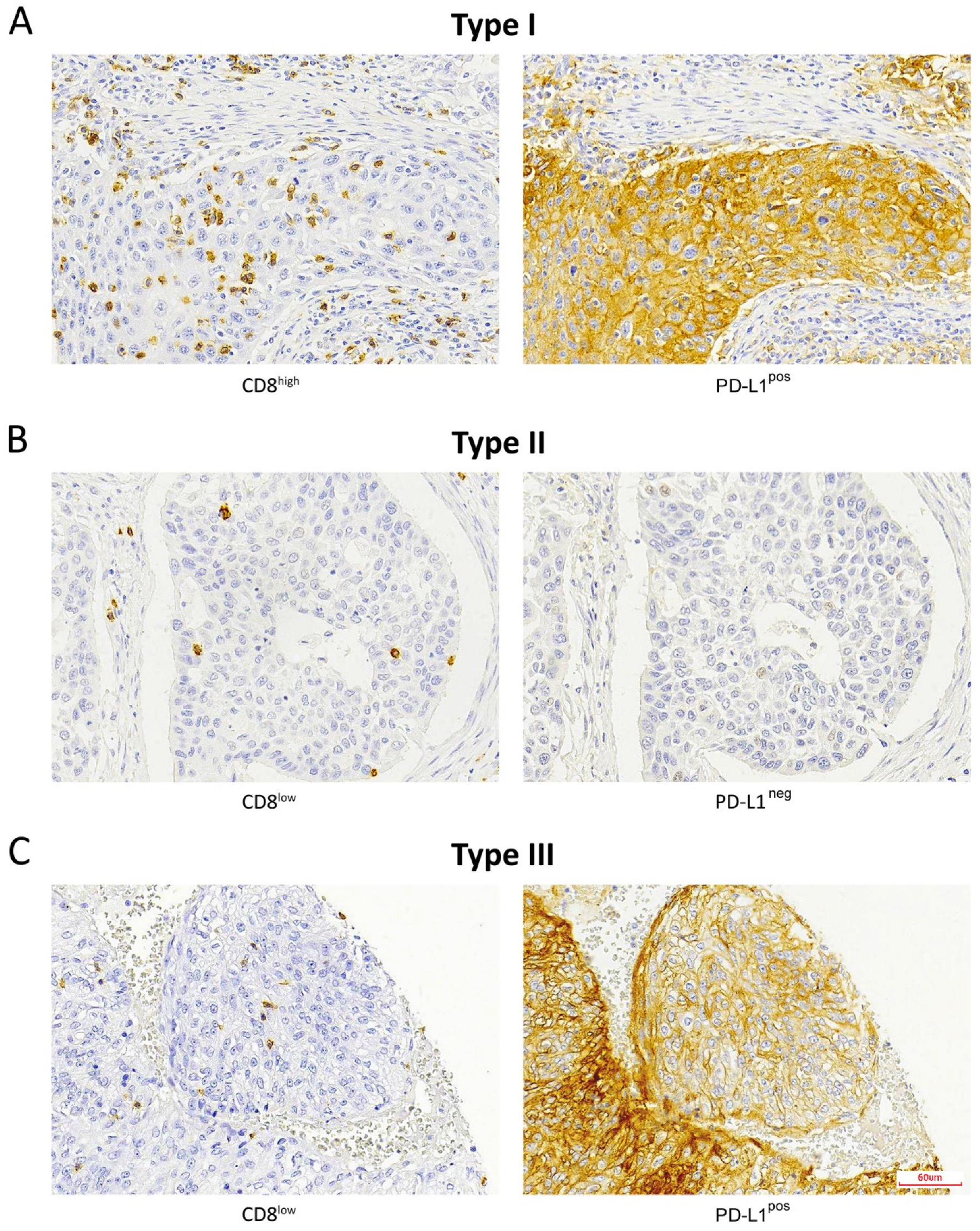
2.3. TMIT and Correlation with the Clinical and Survival Data
2.4. CD8+ TILs Co-Occurs with Tumoral PD-L1-Positive Expression
3. Discussion
4. Materials and Methods
4.1. Patients and Specimens
4.2. Immunohistochemistry
4.3. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koeller, K.K. Radiologic Features of Sinonasal Tumors. Head Neck Pathol. 2016, 10, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youlden, D.R.; Cramb, S.M.; Peters, S.; Porceddu, S.V.; Møller, H.; Fritschi, L.; Baade, P.D. International comparisons of the incidence and mortality of sinonasal cancer. Cancer Epidemiol. 2013, 37, 770–779. [Google Scholar] [CrossRef] [Green Version]
- Turner, J.H.; Reh, D.D. Incidence and survival in patients with sinonasal cancer: A historical analysis of population-based data. Head Neck 2012, 34, 877–885. [Google Scholar] [CrossRef]
- Bossi, P.; Saba, N.F.; Vermorken, J.B.; Strojan, P.; Pala, L.; de Bree, R.; Rodrigo, J.P.; Lopez, F.; Hanna, E.Y.; Haigentz, M.; et al. The role of systemic therapy in the management of sinonasal cancer: A critical review. Cancer Treat. Rev. 2015, 41, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Llorente, J.L.; López, F.; Suárez, C.; Hermsen, M.A. Sinonasal carcinoma: Clinical, pathological, genetic and therapeutic advances. Nat. Rev. Clin. Oncol. 2014, 11, 460–472. [Google Scholar] [CrossRef] [PubMed]
- Constantinidou, A.; Alifieris, C.; Trafalis, D.T. Targeting Programmed Cell Death -1 (PD-1) and Ligand (PD-L1): A new era in cancer active immunotherapy. Pharmacol. Ther. 2019, 194, 84–106. [Google Scholar] [CrossRef]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Al-Saleh, K.; El-Aziz, N.A.; Ali, A.; Abozeed, W.; El-Warith, A.A.; Ibraheem, A.; Ansari, J.; Al-Rikabi, A.; Husain, S.; Nabholtz, J.M. Predictive and prognostic significance of CD8+ tumor-infiltrating lymphocytes in patients with luminal B/HER 2 negative breast cancer treated with neoadjuvant chemotherapy. Oncol. Lett. 2017, 14, 337–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, L.Q.; Haddad, R.; Gupta, S.; Mahipal, A.; Mehra, R.; Tahara, M.; Berger, R.; Eder, J.P.; Burtness, B.; Lee, S.-H.; et al. Antitumor Activity of Pembrolizumab in Biomarker-Unselected Patients with Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma: Results from the Phase Ib KEYNOTE-012 Expansion Cohort. J. Clin. Oncol. 2016, 34, 3838–3845. [Google Scholar] [CrossRef]
- Cramer, J.D.; Burtness, B.; Ferris, R.L. Immunotherapy for head and neck cancer: Recent advances and future directions. Oral Oncol. 2019, 99, 104460. [Google Scholar] [CrossRef]
- Pai, S.I.; Faivre, S.; Licitra, L.; Machiels, J.P.; Vermorken, J.B.; Bruzzi, P.; Gruenwald, V.; Giglio, R.E.; Leemans, C.R.; Seiwert, T.Y.; et al. Comparative analysis of the phase III clinical trials of anti-PD1 monotherapy in head and neck squamous cell carcinoma patients (CheckMate 141 and KEYNOTE 040). J. Immunother. Cancer 2019, 7, 96. [Google Scholar] [CrossRef]
- Herbst, R.S.; Soria, J.C.; Kowanetz, M.; Fine, G.D.; Hamid, O.; Gordon, M.S.; Sosman, J.A.; McDermott, D.F.; Powderly, J.D.; Gettinger, S.N.; et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 2014, 515, 563–567. [Google Scholar] [CrossRef] [Green Version]
- Zou, W.; Wolchok, J.D.; Chen, L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 2016, 8, 328rv4. [Google Scholar] [CrossRef] [Green Version]
- Riobello, C.; Vivanco, B.; Reda, S.; López-Hernández, A.; García-Inclán, C.; Potes-Ares, S.; Cabal, V.N.; López, F.; Llorente, J.L.; Hermsen, M.A. Programmed death ligand-1 expression as immunotherapeutic target in sinonasal cancer. Head Neck 2018, 40, 818–827. [Google Scholar] [CrossRef]
- Quan, H.; Yan, L.; Wang, S.; Wang, S. Clinical relevance and significance of programmed death-ligand 1 expression, tumor-infiltrating lymphocytes, and p16 status in sinonasal squamous cell carcinoma. Cancer Manag. Res. 2019, 11, 4335–4345. [Google Scholar] [CrossRef] [Green Version]
- Balermpas, P.; Michel, Y.; Wagenblast, J.; Seitz, O.; Weiss, C.; Rödel, F.; Rödel, C.; Fokas, E. Tumour-infiltrating lymphocytes predict response to definitive chemoradiotherapy in head and neck cancer. Br. J. Cancer 2013, 110, 501–509. [Google Scholar] [CrossRef]
- Ward, M.J.; Thirdborough, S.M.; Mellows, T.; Riley, C.; Harris, S.; Suchak, K.; Webb, A.; Hampton, C.; Patel, N.N.; Randall, C.J.; et al. Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer. Br. J. Cancer 2014, 110, 489–500. [Google Scholar] [CrossRef] [Green Version]
- Vassilakopoulou, M.; Avgeris, M.; Velcheti, V.; Kotoula, V.; Rampias, T.; Chatzopoulos, K.; Perisanidis, C.; Kontos, C.K.; Giotakis, A.I.; Scorilas, A.; et al. Evaluation of PD-L1 Expression and Associated Tumor-Infiltrating Lymphocytes in Laryngeal Squamous Cell Carcinoma. Clin. Cancer Res. 2016, 22, 704–713. [Google Scholar] [CrossRef] [Green Version]
- Fang, J.; Li, X.; Ma, D.; Liu, X.; Chen, Y.; Wang, Y.; Lui, V.W.Y.; Xia, J.; Cheng, B.; Wang, Z. Prognostic significance of tumor infiltrating immune cells in oral squamous cell carcinoma. BMC Cancer 2017, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Quan, H.; Shan, Z.; Liu, Z.; Liu, S.; Yang, L.; Fang, X.; Li, K.; Wang, B.; Deng, Z.; Hu, Y.; et al. The repertoire of tumor-infiltrating lymphocytes within the microenvironment of oral squamous cell carcinoma reveals immune dysfunction. Cancer Immunol. Immunother. 2020, 69, 465–476. [Google Scholar] [CrossRef]
- Takahashi, Y.; Amit, M.; Gleber-Netto, F.O.; Silverman, D.; Bell, D.; Xie, T.X.; Roberts, D.; Myers, J.N.; Hanna, E.Y. Evaluation of the Immune Microenvironment in Sinonasal Squamous Cell Carcinoma and Its Association with Patients’ Survival. J. Neurol. Surg. Part B Skull Base 2021, 82, S022. [Google Scholar] [CrossRef]
- Classe, M.; Burgess, A.; El Zein, S.; Wassef, M.; Herman, P.; Mortuaire, G.; Leroy, X.; Malouf, G.G.; Verillaud, B. Evaluating the prognostic potential of the Ki67 proliferation index and tumour-infiltrating lymphocytes in olfactory neuroblastoma. Histopathology 2019, 75, 853–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Marín, R.; Reda, S.; Riobello, C.; Cabal, V.N.; Suárez-Fernández, L.; Vivanco, B.; López, F.; Llorente, J.L.; Hermsen, M.A. CD8+ Tumour-Infiltrating Lymphocytes and Tumour Microenvironment Immune Types as Biomarkers for Immunotherapy in Sinonasal Intestinal-Type Adenocarcinoma. Vaccines 2020, 8, 202. [Google Scholar] [CrossRef]
- Taube, J.M.; Anders, R.A.; Young, G.D.; Xu, H.; Sharma, R.; McMiller, T.L.; Chen, S.; Klein, A.P.; Pardoll, D.M.; Topalian, S.L.; et al. Colocalization of Inflammatory Response with B7-H1 Expression in Human Melanocytic Lesions Supports an Adaptive Resistance Mechanism of Immune Escape. Sci. Transl. Med. 2012, 4, 127ra37. [Google Scholar] [CrossRef] [Green Version]
- Ock, C.Y.; Keam, B.; Kim, S.; Lee, J.S.; Kim, M.; Kim, T.M.; Jeon, Y.K.; Kim, D.W.; Chung, D.H.; Heo, D.S. Pan-Cancer Immunogenomic Perspective on the Tumor Microenvironment Based on PD-L1 and CD8 T-Cell Infiltration. Clin. Cancer Res. 2016, 22, 2261–2270. [Google Scholar] [CrossRef] [Green Version]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.M.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef]
- Teng, M.W.L.; Ngiow, S.F.; Ribas, A.; Smyth, M.J. Classifying Cancers Based on T-cell Infiltration and PD-L1. Cancer Res. 2015, 75, 2139–2145. [Google Scholar] [CrossRef] [Green Version]
- Blank, C.U.; Haanen, J.B.; Ribas, A.; Schumacher, T.N. The “cancer immunogram”. Science 2016, 352, 658–660. [Google Scholar] [CrossRef]
- London, N.R.; Rooper, L.M.; Bishop, J.A.; Xu, H.; Bernhardt, L.J.; Ishii, M.; Hann, C.L.; Taube, J.M.; Izumchenko, E.; Gaykalova, D.A.; et al. Expression of Programmed Cell Death Ligand 1 and Associated Lymphocyte Infiltration in Olfactory Neuroblastoma. World Neurosurg. 2020, 135, e187–e193. [Google Scholar] [CrossRef]
- Sato, E.; Olson, S.H.; Ahn, J.; Bundy, B.; Nishikawa, H.; Qian, F.; Jungbluth, A.A.; Frosina, D.; Gnjatic, S.; Ambrosone, C.; et al. Intraepithelial CD8+ tumor-infiltrating lymphocytes and a high CD8+/regulatory T cell ratio are associated with favorable prognosis in ovarian cancer. Proc. Natl. Acad. Sci. USA 2005, 102, 18538–18543. [Google Scholar] [CrossRef] [Green Version]
- Nakano, O.; Sato, M.; Naito, Y.; Suzuki, K.; Orikasa, S.; Aizawa, M.; Suzuki, Y.; Shintaku, I.; Nagura, H.; Ohtani, H. Proliferative activity of intratumoural CD8(+) T-lymphocytes as a prognostic factor in human renal cell carcinoma: Clinicopathologic demonstration of antitumour immunity. Cancer Res. 2001, 61, 5132–5136. [Google Scholar]
- Kawai, O.; Ishii, G.; Kubota, K.; Murata, Y.; Naito, Y.; Mizuno, T.; Aokage, K.; Saijo, N.; Nishiwaki, Y.; Gemma, A.; et al. Predominant infiltration of macrophages and CD8+T Cells in cancer nests is a significant predictor of survival in stage IV nonsmall cell lung cancer. Cancer 2008, 113, 1387–1395. [Google Scholar] [CrossRef]
- Fukunaga, A.; Miyamoto, M.; Cho, Y.; Murakami, S.; Kawarada, Y.; Oshikiri, T.; Kato, K.; Kurokawa, T.; Suzuoki, M.; Nakakubo, Y.; et al. CD8+ Tumor-Infiltrating Lymphocytes Together with CD4+ Tumor-Infiltrating Lymphocytes and Dendritic Cells Improve the Prognosis of Patients with Pancreatic Adenocarcinoma. Pancreas 2004, 28, e26–e31. [Google Scholar] [CrossRef]
- Wakabayashi, O.; Yamazaki, K.; Oizumi, S.; Hommura, F.; Kinoshita, I.; Ogura, S.; Dosaka-Akita, H.; Nishimura, M. CD4+ T cells in cancer stroma, not CD8+ T cells in cancer cell nests, are associated with favorable prognosis in human non-small cell lung cancers. Cancer Sci. 2003, 94, 1003–1009. [Google Scholar] [CrossRef]
- Ikeda, S.; Funakoshi, N.; Inagaki, M.; Shibata, T. Clinicopathologic Roles of Tumor-Infiltrating Lymphocytes and CD8-Positive Lymphocytes in Lung Cancer Imprint Smears in Squamous Cell Carcinoma and Adenocarcinoma. Acta Cytol. 2006, 50, 423–429. [Google Scholar] [CrossRef]
- Kinoshita, T.; Kudo-Saito, C.; Muramatsu, R.; Fujita, T.; Saito, M.; Nagumo, H.; Sakurai, T.; Noji, S.; Takahata, E.; Yaguchi, T.; et al. Determination of poor prognostic immune features of tumour microenvironment in non-smoking patients with lung adenocarcinoma. Eur. J. Cancer 2017, 86, 15–27. [Google Scholar] [CrossRef]
- Aptsiauri, N.; Ruiz-Cabello, F.; Garrido, F. The transition from HLA-I positive to HLA-I negative primary tumors: The road to escape from T-cell responses. Curr. Opin. Immunol. 2018, 51, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Wickenhauser, C.; Bethmann, D.; Kappler, M.; Eckert, A.W.; Steven, A.; Bukur, J.; Fox, B.A.; Beer, J.; Seliger, B. Tumor Microenvironment, HLA Class I and APM Expression in HPV-Negative Oral Squamous Cell Carcinoma. Cancers 2021, 13, 620. [Google Scholar] [CrossRef] [PubMed]
- Cabal, V.N.; Menendez, M.; Vivanco, B.; Potes-Ares, S.; Riobello, C.; Suarez-Fernandez, L.; Garcia-Marin, R.; Blanco-Lorenzo, V.; Lopez, F.; Alvarez-Marcos, C.; et al. EGFR mutation and HPV infection in sinonasal inverted papilloma and squamous cell carcinoma. Rhinol. J. 2020, 58, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, K.; Syrjänen, S. Detection of human papillomavirus in esophageal papillomas: Systematic review and meta-analysis. APMIS 2013, 121, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Udager, A.M.; McHugh, J.B.; Goudsmit, C.M.; Weigelin, H.C.; Lim, M.S.; Elenitoba-Johnson, K.S.J.; Betz, B.L.; Carey, T.E.; Brown, N.A. Human papillomavirus (HPV) and somatic EGFR mutations are essential, mutually exclusive oncogenic mechanisms for inverted sinonasal papillomas and associated sinonasal squamous cell carcinomas. Ann. Oncol. 2018, 29, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Sahnane, N.; Ottini, G.; Turri-Zanoni, M.; Furlan, D.; Battaglia, P.; Karligkiotis, A.; Albeni, C.; Cerutti, R.; Mura, E.; Chiaravalli, A.M.; et al. Comprehensive analysis of HPV infection, EGFR exon 20 mutations and LINE1 hypomethylation as risk factors for malignant transformation of sinonasal-inverted papilloma to squamous cell carcinoma. Int. J. Cancer 2019, 144, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; Heath, K.; McClanahan, T.; Lunceford, J.; Gause, C.; et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): An open-label, multicentre, phase 1b trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | All | CD8+ TILs, Intratumoral | CD8+ TILs, Stromal | TMIT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0% | 1–10% | >10% | p-value | 0% | 1–10% | >10% | p-value | I | II | III | p-value | ||
| All | 57 | 7 | 39 | 11 | 1 | 32 | 24 | 11 | 31 | 15 | |||
| Gender | 0.244 | 0.548 | 0.555 | ||||||||||
| Female | 20 (35) | 4 (57) | 11 (28) | 5 (45) | 0 (0) | 10 (31) | 10 (42) | 5 (45) | 9 (29) | 6 (40) | |||
| Male | 37(65) | 3 (43) | 28 (72) | 6 (55) | 1 (100) | 22 (69) | 14 (58) | 6 (55) | 22 (71) | 9 (60) | |||
| Tumor site | 0.117 | 0.497 | 0.282 | ||||||||||
| Maxillary sinus | 49 (86) | 7 (100) | 31 (80) | 11 (100) | 1 (100) | 26 (81) | 22 (92) | 11 (100) | 25 (81) | 13 (87) | |||
| Ethmoid sinus | 8 (14) | 0 (0) | 8 (20) | 0 (0) | 0 (0) | 6 (19) | 2 (8) | 0 (0) | 6 (19) | 2 (13) | |||
| Disease stage | 0.534 | 0.802 | 0.704 | ||||||||||
| I | 1 (2) | 0 (0) | 1 (3) | 0 (0) | 0 (0) | 1 (3) | 0 (0) | 0 (0) | 1 (3) | 0 (0) | |||
| II | 3 (5) | 0 (0) | 3 (8) | 0 (0) | 0 (0) | 2 (6) | 1 (4) | 0 (0) | 3 (10) | 0 (0) | |||
| III | 17 (30) | 4 (57) | 11 (28) | 2 (18) | 0 (0) | 11 (34) | 6 (25) | 2 (18) | 10 (32) | 5 (33) | |||
| IVa | 25 (44) | 3 (43) | 15 (38) | 7 (64) | 1 (100) | 14 (44) | 10 (42) | 7 (64) | 11 (36) | 7 (47) | |||
| IVb | 11 (19) | 0 (0) | 9 (23) | 2 (18) | 0 | 4 (13) | 7 (29) | 2 (18) | 6 (19) | 3 (20) | |||
| Differentiation | 0.828 | 0.525 | 0.712 | ||||||||||
| Good | 22 (39) | 4 (57) | 14 (36) | 4 (36) | 1 (100) | 10 (31) | 11 (46) | 4 (36) | 14 (45) | 4 (27) | |||
| Moderate | 13 (22) | 1 (14) | 10 (26) | 2 (18) | 0 (0) | 9 (28) | 4 (17) | 2 (18) | 6 (19) | 5 (33) | |||
| Poor | 22 (39) | 2 (29) | 15 (38) | 5 (46) | 0 (0) | 13 (41) | 9 (37) | 5 (46) | 11 (36) | 6 (40) | |||
| Recurrence | 0.084 | 0.564 | 0.087 | ||||||||||
| No | 13 (23) | 1 (14) | 12 (31) | 0 (0) | 0 (0) | 6 (19) | 7 (29) | 0 (0) | 10 (32) | 3 (20) | |||
| Yes | 44 (77) | 6 (86) | 27 (69) | 11 (100) | 1 (100) | 26 (81) | 17 (71) | 11 (100) | 21 (68) | 12 (80) | |||
| Metastasis | 0.372 | 0.931 | 0.569 | ||||||||||
| No | 50 (88) | 5 (71) | 35 (90) | 10 (91) | 1 (100) | 28 (88) | 21 (87) | 10 (91) | 28 (90) | 12 (80) | |||
| Yes | 7 (12) | 2 (29) | 4 (10) | 1 (9) | 0 (0) | 4 (12) | 3 (13) | 1 (9) | 3 (10) | 3 (20) | |||
| Patient status | 0.449 | 0.790 | 0.252 | ||||||||||
| Alive | 8 (14) | 1(14) | 6 (15) | 1 (9) | 0 (0) | 4 (12) | 4 (17) | 1 (9) | 6 (19) | 1 (6) | |||
| Died of the disease | 41 (72) | 4 (57) | 27 (70) | 10 (91) | 1 (100) | 22 (69) | 18 (75) | 10 (91) | 21 (68) | 10 (67) | |||
| Died of other causes | 8 (14) | 2 (29) | 6 (15) | 0 (0) | 0 (0) | 6 (19) | 2 (8) | 0 (0) | 4 (13) | 4 (27) | |||
| Score | PD-L1-Expressing Tumor Cells | |||
|---|---|---|---|---|
| Negative | Positive | p-value | ||
| CD8+ TILs | Negative (0%) | 6 | 1 | |
| Low (1–10%) | 25 | 14 | 0.000 | |
| High (>10%) | 0 | 11 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Marín, R.; Reda, S.; Riobello, C.; Cabal, V.N.; Suárez-Fernández, L.; Vivanco, B.; Álvarez-Marcos, C.; López, F.; Llorente, J.L.; Hermsen, M.A. Prognostic and Therapeutic Implications of Immune Classification by CD8+ Tumor-Infiltrating Lymphocytes and PD-L1 Expression in Sinonasal Squamous Cell Carcinoma. Int. J. Mol. Sci. 2021, 22, 6926. https://doi.org/10.3390/ijms22136926
García-Marín R, Reda S, Riobello C, Cabal VN, Suárez-Fernández L, Vivanco B, Álvarez-Marcos C, López F, Llorente JL, Hermsen MA. Prognostic and Therapeutic Implications of Immune Classification by CD8+ Tumor-Infiltrating Lymphocytes and PD-L1 Expression in Sinonasal Squamous Cell Carcinoma. International Journal of Molecular Sciences. 2021; 22(13):6926. https://doi.org/10.3390/ijms22136926
Chicago/Turabian StyleGarcía-Marín, Rocío, Sara Reda, Cristina Riobello, Virginia N. Cabal, Laura Suárez-Fernández, Blanca Vivanco, César Álvarez-Marcos, Fernando López, José L. Llorente, and Mario A. Hermsen. 2021. "Prognostic and Therapeutic Implications of Immune Classification by CD8+ Tumor-Infiltrating Lymphocytes and PD-L1 Expression in Sinonasal Squamous Cell Carcinoma" International Journal of Molecular Sciences 22, no. 13: 6926. https://doi.org/10.3390/ijms22136926
APA StyleGarcía-Marín, R., Reda, S., Riobello, C., Cabal, V. N., Suárez-Fernández, L., Vivanco, B., Álvarez-Marcos, C., López, F., Llorente, J. L., & Hermsen, M. A. (2021). Prognostic and Therapeutic Implications of Immune Classification by CD8+ Tumor-Infiltrating Lymphocytes and PD-L1 Expression in Sinonasal Squamous Cell Carcinoma. International Journal of Molecular Sciences, 22(13), 6926. https://doi.org/10.3390/ijms22136926