miR-497-5p Decreased Expression Associated with High-Risk Endometrial Cancer

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Results
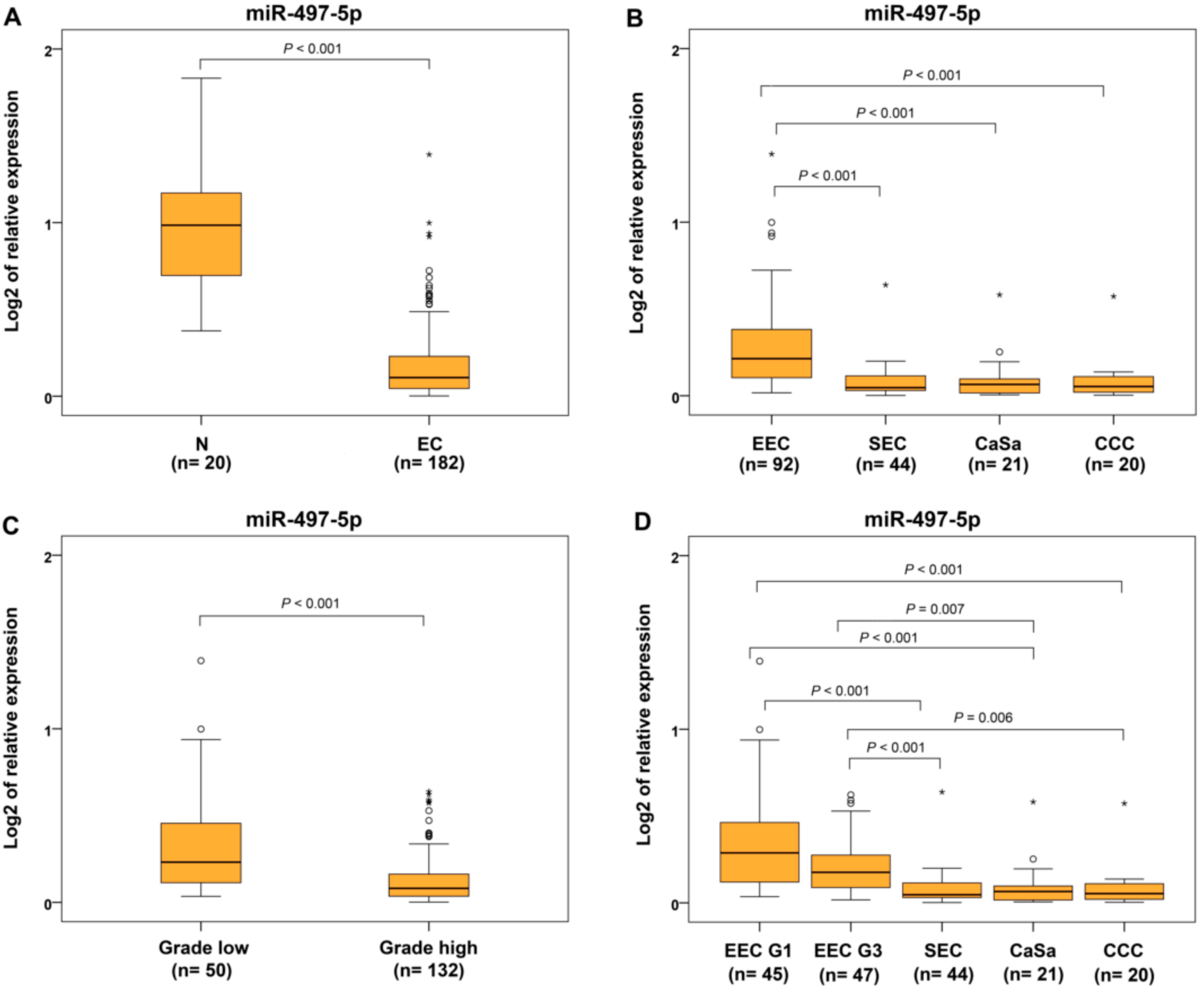
2.1. Verification of Discriminating miRNAs
2.2. miRNA Expression in Rare Subtypes of Endometrial Cancer
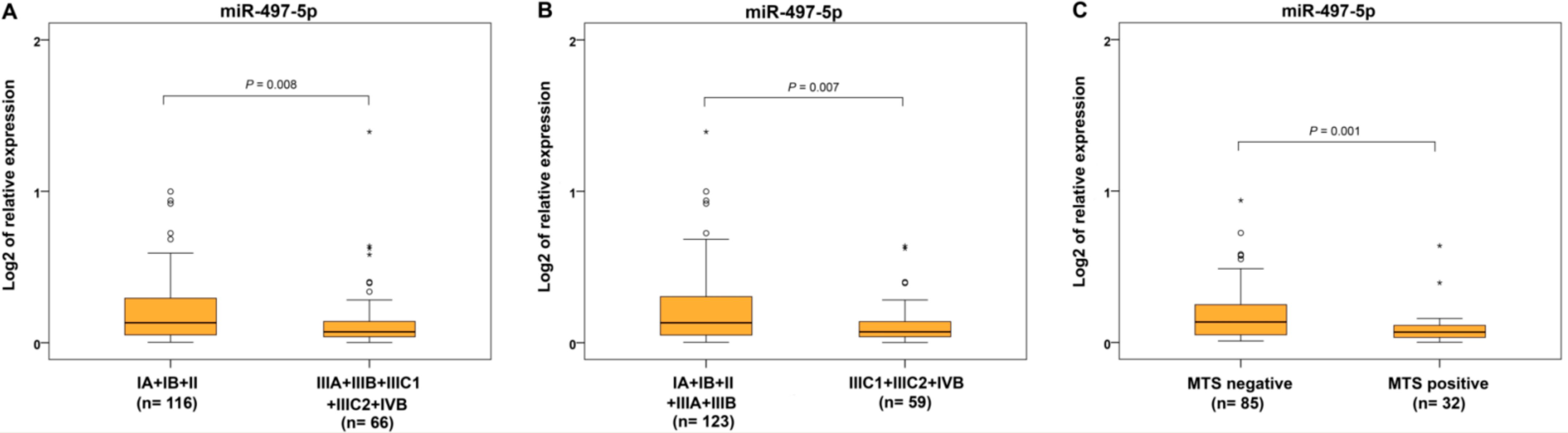
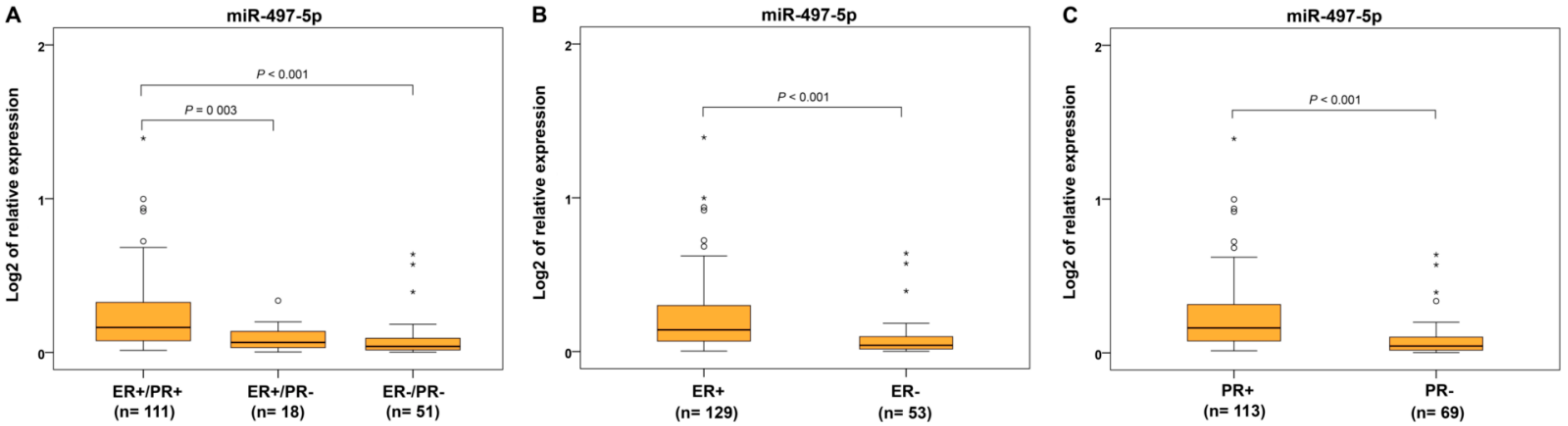
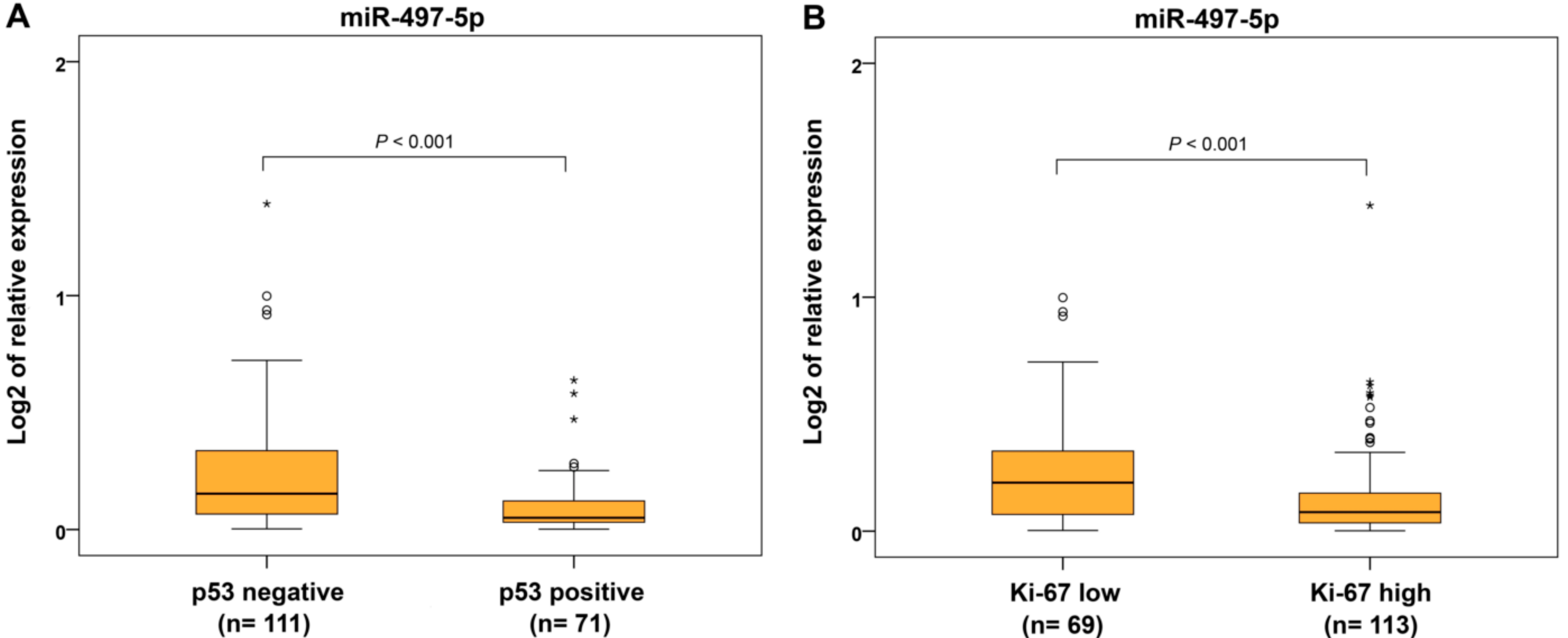
2.3. miR-497-5p Expression and Clinicohistopathological Characteristics
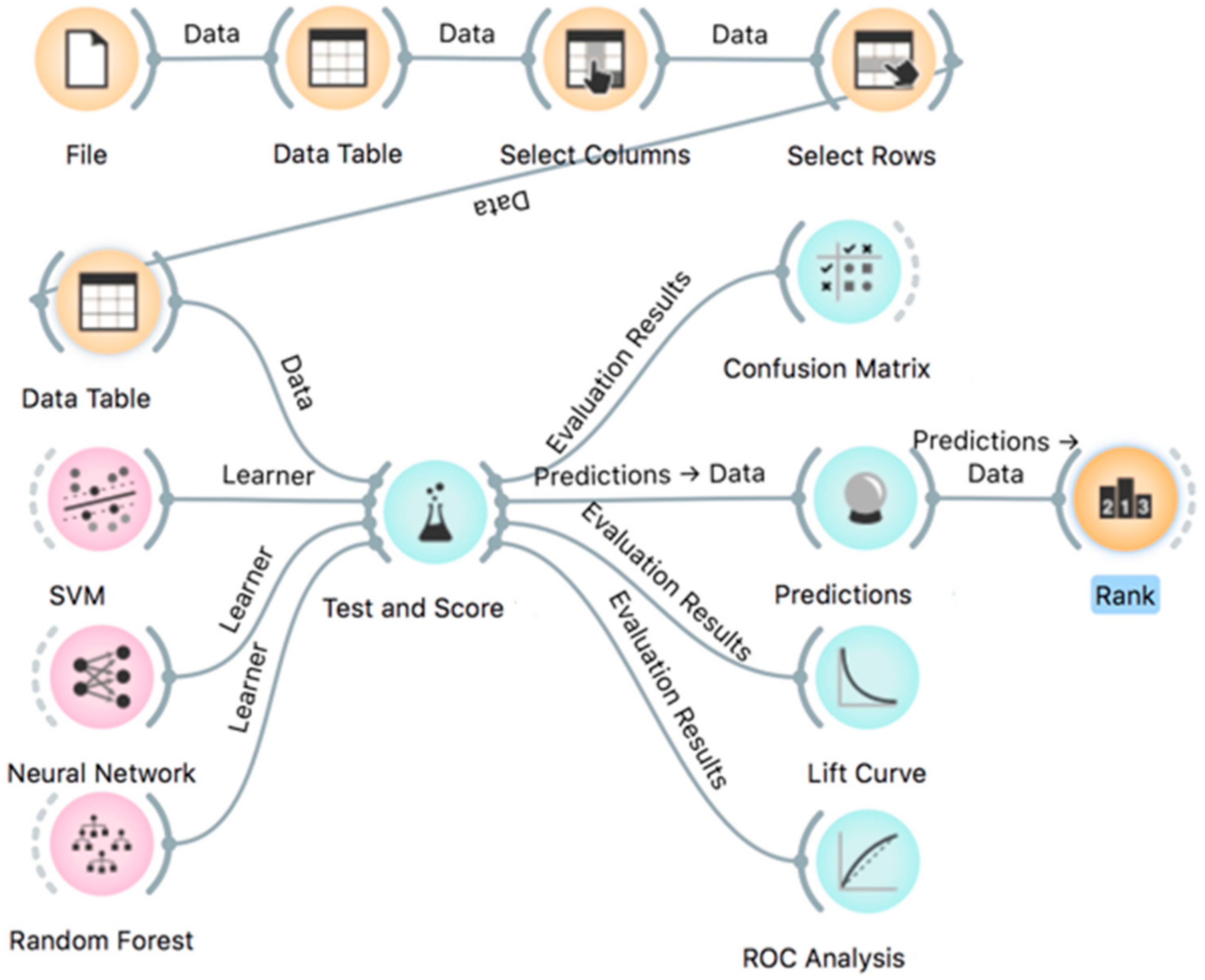
2.4. Machine Learning Analyses
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. miRNA Extraction and Real-Time PCR
4.3. Statistical Analysis
4.4. Machine Learning Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EC | endometrial cancer |
| EEC | endometrioid endometrial cancer |
| G | grade |
| SEC | serous endometrial cancer |
| CCC | clear cell carcinoma |
| CaSa | carcinosarcoma |
| MC | mucinous carcinoma |
| FIGO | International Federation of Gynecology and Obstetrics |
| LN | lymph node |
| LVSI | lymphovascular space invasion |
| IQR | interquartile range |
| N | non-neoplastic endometrium |
| MTS | distant metastases |
| miRNA | microRNAs |
| ML | machine learning |
| SVM | support vector machine |
| CA | classification accuracy |
| AUC | area under ROC curve |
| F1 | F-score |
| PR | progesterone receptor |
| ER | estrogen receptor |
| ERR | estrogen-related receptor |
| GRP30 | G-protein-coupled receptor-30 |
| FFPE | formalin-fixed paraffin embedded |
| MAPK | mitogen-activated protein kinases |
| EMT | epithelial–mesenchymal transition |
| TP | true-positive predictions |
| TNM | Classification of Malignant Tumors |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- McAlpine, J.N.; Temkin, S.M.; Mackay, H.J. Endometrial cancer: Not your grandmother´s cancer. Cancer 2016, 122, 2787–2798. [Google Scholar] [CrossRef] [PubMed]
- Bokhman, J.V. Two pathogenetic types of endometrial carcinoma. Gynecol. Oncol. 1983, 15, 10–17. [Google Scholar] [CrossRef]
- Setiawan, V.W.; Yang, H.P.; Pike, M.C.; McCann, S.E.; Yu, H.; Xiang, Y.B.; Wolk, A.; Wentzensen, N.; Weiss, N.S.; Webb, P.M.; et al. Type I and II endometrial cancers: Have they different risk factors? J. Clin. Oncol 2013, 31, 2607–2618. [Google Scholar] [CrossRef]
- Murali, R.; Soslow, R.A.; Weigelt, B. Classification of endometrial carcinoma: More than two types. Lancet Oncol. 2014, 15, e268–e278. [Google Scholar] [CrossRef]
- Wortman, B.G.; Nout, R.A.; Bosse, T.; Creutzberg, C.L. Selecting Adjuvant Treatment for Endometrial Carcinoma Using Molecular Risk Factors. Curr. Oncol. Rep 2019, 21, 83. [Google Scholar] [CrossRef]
- Vermij, L.; Smit, V.; Nout, R.; Bosse, T. Incorporation of molecular characteristics into endometrial cancer management. Histopathology 2020, 76, 52–63. [Google Scholar] [CrossRef]
- Delangle, R.; De Foucher, T.; Larsen, A.K.; Sabbah, M.; Azaïs, H.; Bendifallah, S.; Daraï, E.; Ballester, M.; Mehats, C.; Uzan, C.; et al. The Use of microRNAs in the Management of Endometrial Cancer: A Meta-Analysis. Cancers 2019, 11, 832. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniak, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen., R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Srivastava, S.K.; Ahmad, A.; Zubair, H.; Miree, O.; Singh, S.; Rocconi, R.P.; Scalici, J.; Singh, A.P. MicroRNAs in gynecological cancers: Small molecules with big implications. Cancer Lett. 2017, 407, 123–138. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Torres, K.; Pesci, A.; Ceccaroni, M.; Paszkowski, T.; Cassandrini, P.; Zamboni, G.; Maciejewski, R. Diagnostic and prognostic significance of miRNA signatures in tissue and plasma of endometroid endometrial carcinoma patients. Int. J. Cancer 2013, 132, 1633–1645. [Google Scholar] [CrossRef] [PubMed]
- Canlorbe, G.; Castela, M.; Bendifallah, S.; Wang, Z.; Lefevre, M.; Chabbert-Buffet, N.; Aractingi, S.; Daraï, E.; Méhats, C.; Ballester, M. Micro-RNA signature of lymphovascular space involvement in type 1 endometrial cancer. Histol. Histopathol. 2017, 32, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine learning applications in cancer prognosis and prediction. Comput. Struct Biotechnol. J. 2014, 13, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Ngiam, K.Y.; Khor, I.W. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Kalinkova, L.; Kajo, K.; Karhanek, M.; Wachsmannova, L.; Suran, P.; Zmetakova, I.; Fridrichova, I. Discriminating miRNA Profiles between Endometrioid Well- and Poorly-Differentiated Tumours and Endometrioid and Serous Subtypes of Endometrial Cancers. Int. J. Mol. Sci. 2020, 21, E6071. [Google Scholar] [CrossRef]
- Tao, L.; Zhang, C.Y.; Guo, L.; Li, X.; Han, N.N.; Zhou, Q.; Liu, Z.L. MicroRNA-497 accelerates apoptosis while inhibiting proliferation, migration, and invasion through negative regulation of the MAPK/ERK signaling pathway via RAF-1. J. Cell Physiol. 2018, 233, 6578–6588. [Google Scholar] [CrossRef]
- Pengcheng, S.; Ziqi, W.; Luyao, Y.; Xiangwei, Z.; Liang, L.; Yuwei, L.; Lechen, L.; Wanhai, X. MicroRNA-497 suppresses renal cell carcinoma by targeting VEGFR-2 in ACHN cells. Biosci. Rep. 2017, 37, BSR20170270. [Google Scholar] [CrossRef]
- Xia, Y.; Hu, C.; Lian, L.; Hui, K.; Wang, L.; Qiao, Y.; Liu, L.; Liang, L.; Jiang, X. miR-497 suppresses malignant phenotype in non-small cell lung cancer via targeting KDR. Oncol. Rep. 2019, 42, 443–452. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, H.; Singh, A.; Shou, F. Expression and function of microRNA-497 in human osteosarcoma. Mol. Med. Rep. 2016, 14, 439–445. [Google Scholar] [CrossRef]
- Ding, W.-Z.; Ni, Q.-F.; Lu, Y.-T.; Kong, L.-L.; Yu, J.-J.; Tan, L.-W.; Kong, L.-B. MicroRNA-497 regulates cell proliferation in hepatocellular carcinoma. Oncol. Lett. 2016, 11, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Chen, J.; Gao, C.; Zhu, D.; Xu, X.; Wu, C.; Jiang, J. MicroRNA-497 inhibits tumor growth through targeting insulin receptor substrate 1 in colorectal cancer. Oncol. Lett. 2017, 14, 6379–6386. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chen, Y.; Du, J.; Wang, Y.; Shi, H.; Jiang, Q.; Wang, Y.; Zhang, H.; Wei, Y.; Xue, W.; Pu, Z.; et al. MicroRNA-497-5p Induces Cell Cycle Arrest of Cervical Cancer Cells in S Phase by Targeting CBX4. Oncol. Targets Ther. 2019, 12, 10535–10545. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, A.; Barzilai, A.; Gur-Wahnon, D.; Ben-Dov, I.Z.; Glassberg, S.; Meningher, T.; Elharar, E.; Masalha, M.; Jacob-Hirsch, J.; Tabibian-Keissar, H.; et al. Alterations of microRNAs throughout the malignant evolution of cutaneous squamous cell carcinoma: The role of miR-497 in epithelial to mesenchymal transition of keratinocytes. Oncogene 2018, 37, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Bai, Z.; Yin, J.; Zhang, Z. Global transcriptomic analysis identifies SERPINE1 as a prognostic biomarker associated with epithelial-to-mesenchymal transition in gastric cancer. PeerJ 2019, 7, e7091. [Google Scholar] [CrossRef]
- Wu, Z.; Li, X.; Cai, X.; Huang, C.; Zheng, M. miR-497 inhibits epithelial mesenchymal transition in breast carcinoma by targeting Slug. Tumour Biol. 2016, 37, 7939–7950. [Google Scholar] [CrossRef]
- Qu, F.; Ye, J.; Pan, X.; Wang, J.; Gan, S.; Chu, C.; Chu, J.; Zhang, X.; Liu, M.; He, H. MicroRNA-497-5p down-regulation increases PD-L1 expression in clear cell renal cell carcinoma. J. Drug Target. 2019, 27, 67–74. [Google Scholar] [CrossRef]
- Han, L.; Liu, B.; Jiang, L.; Liu, J.; Han, S. MicroRNA-497 downregulation contributes to cell proliferation, migration, and invasion of estrogen receptor alpha negative breast cancer by targeting estrogen-related receptor alpha. Tumour Biol. 2016, 37, 13205–13214. [Google Scholar] [CrossRef]
- Feng, J.; Gu, X.; Liu, L.; Lu, M.; Ma, X.; Cao, Y.; Jiang, R.; Wang, B.; Zhao, Q. Prognostic Role of MicroRNA-497 In Cancer Patients: A Meta-analysis. J. Cancer 2018, 9, 3334–3342. [Google Scholar] [CrossRef]
- Hiroki, E.; Akahira, J.-I.; Suzuki, F.; Nagase, S.; Ito, K.; Suzuki, T.; Sasano, H.; Yaegashi, N. Changes in microRNA expression levels correlate with clinicopathological features and prognoses in endometrial serous adenocarcinomas. Cancer Sci. 2010, 101, 241–249. [Google Scholar] [CrossRef]
- De Foucher, T.; Sbeih, M.; Uzan, J.; Bendifallah, S.; Lefevre, M.; Chabbert-Buffet, N.; Aractini, S.; Uzan, C.; Alsalam, I.A.; Mitri, R.; et al. Identification of micro-RNA expression profile related to recurrence in women with ESMO low-risk endometrial cancer. J. Transl. Med. 2018, 16, 131. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Liu, T.; Wang, Y.; Fu, J.; Yang, Q.; Wu, J.; Zhou, H. miRNA-mRNA Associated With Survival in Endometrial Cancer. Front. Genet. 10, 743. [CrossRef] [PubMed]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, 16–41. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.R.; Cooper, K.; Croce, S.; Djordevic, B.; Herrington, S.; Howitt, B.; Hui, P.; Ip, P.; Koebel, M.; Lax, S.; et al. International Society of Gynecological Pathologists (ISGyP) Endometrial Cancer Project: Guidelines From the Special Techniques and Ancillary Studies Group. Int. J. Gynecol. Pathol. 2019, 38 (Suppl. 1), S114–S122. [Google Scholar] [CrossRef]
- Swasti. Estrogen and Progesterone Receptors in Endometrial Cancer and Their Prognostic Relevance. Gynecol. Obstet. 2018, 8, e127. [Google Scholar] [CrossRef]
- Rodriguez, A.C.; Blanchard, Z.; Maurer, K.A.; Gertz, J. Estrogen Signaling in Endometrial Cancer: A Key Oncogenic Pathway with Several Open Questions. Horm. Cancer 2019, 10, 51–63. [Google Scholar] [CrossRef]
- Leslie, K.K.; Thiel, K.W.; Reyes, H.D.; Yang, S.; Zhang, Y.; Carlson, M.J.; Kumar, N.S.; Dai, D.D. The estrogen receptor joins other cancer biomarkers as a predictor of outcome. Obstet. Gynecol. Int. 2013, 2013, 479541. [Google Scholar] [CrossRef]
- Singh, M.; Zaino, R.J.; Filiaci, V.J.; Leslie, K.K. Relationship of estrogen and progesterone receptors to clinical outcome in metastatic endometrial carcinoma: A Gynecologic Oncology Group Study. Gynecol. Oncol. 2007, 106, 325–333. [Google Scholar] [CrossRef]
- Kreizman-Shefer, H.; Pricop, J.; Goldman, S.; Elmalah, I.; Shalev, E. Distribution of estrogen and progesterone receptors isoforms in endometrial cancer. Diagn. Pathol. 2014, 9, 77. [Google Scholar] [CrossRef]
- Stålberg, K.; Bjurberg, M.; Borgfeldt, C.; Carlson, J.; Dahm-Kähler, P.; Flöter-Rådestad, A.; Hellman, K.; Hjerpe, E.; Holmberg, E.; Kjølhede, P.; et al. Lymphovascular space invasion as a predictive factor for lymph node metastases and survival in endometrioid endometrial cancer—A Swedish Gynecologic Cancer Group (SweGCG) study. Acta Oncol. 2019, 58, 1628–1633. [Google Scholar] [CrossRef]
- Xu, N.; Papagiannakopoulos, T.; Pan, G.; Thomson, J.A.; Kosik, K.S. MicroRNA-145 regulates OCT4, SOX2, and KLF4 and represses pluripotency in human embryonic stem cells. Cell 2009, 137, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Liu, S.; Xin, H.; Jiang, J.; Younglai, E.; Sun, S.; Wang, H. Up-regulation of microRNA-145 promotes differentiation by repressing OCT4 in human endometrial adenocarcinoma cells. Cancer 2011, 117, 3989–3998. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Zhang, D.; Shi, H.; Bian, Y.; Guo, R. MiR-143 inhibits endometrial cancer cell proliferation and metastasis by targeting MAPK1. Oncotarget 2017, 8, 84384–84395. [Google Scholar] [CrossRef] [PubMed]
- Shu, S.; Liu, X.; Xu, M.; Gao, X.; Fan, J.; Liu, H.; Li, R. MicroRNA-424 regulates epithelial-mesenchymal transition of endometrial carcinoma by directly targeting insulin-like growth factor 1 receptor. J. Cell Biochem 2018, 120. [Google Scholar] [CrossRef]
- Gupta, S.; Tran, T.; Luo, W.; Phung, D.; Kennedy, R.L.; Broad, A.; Campbell, D.; Kipp, D.; Singh, M.; Khasraw, M.; et al. Machine-learning prediction of cancer survival: A retrospective study using electronic administrative records and a cancer registry. BMJ Open 2014, 4, e004007. [Google Scholar] [CrossRef]
- IJspeert, J.E.G.; Madani, A.; Overbeek, L.I.H.; Dekker, E.; Nagtegaal, I.D. Implementation of an e-learning module improves consistency in the histopathological diagnosis of sessile serrated lesions within a nationwide population screening programme. Histopathology 2017, 70, 929–937. [Google Scholar] [CrossRef]
- Zhu, W.; Xie, L.; Han, J.; Guo, X. The Application of Deep Learning in Cancer Prognosis Prediction. Cancers 2020, 12, 603. [Google Scholar] [CrossRef]
- Bashiri, A.; Ghazisaeedi, M.; Safdari, R.; Shahmoradi, L.; Ehtesham, H. Improving the Prediction of Survival in Cancer Patients by Using Machine Learning Techniques: Experience of Gene Expression Data: A Narrative Review. Iran. J. Public Health 2017, 46, 165–172. [Google Scholar]
- Kurman, R.J.; Carcangiu, M.L.; Herrington, S.; Young, R.H. WHO Classification of Tumours of Female Reproductive Organs; IARC: Lyon, FR, USA, 2014; ISBN 978-92-832-2435-8. [Google Scholar]
- Creasman, W.T.; Odicino, F.; Maisonneuve, P.; Quinn, M.A.; Beller, U.; Benedet, J.L.; Heintz, A.P.M.; Ngan, H.Y.S.; Pecorelli, S. Carcinoma of the corpus uteri. FIGO 26th annual report on the results of treatment in gynecological cancer. Int. J. Gynecol. Pathol. 2006, 95 (Suppl. 1), S105–S143. [Google Scholar] [CrossRef]
- Creasman, W. Revised FIGO staging for carcinoma of the endometrium. Int. J. Gynaecol. Obstet. 2009, 105, 109. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; John Wiley and Sons, Inc.: Oxford, UK; Hoboken, NJ, USA, 2017; ISBN 9781119263579. [Google Scholar]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2[-Delta Delta C[T]] Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Demsar, J.; Curk, T.; Erjavec, A.; Gorup, C.; Hocevar, T.; Milutinovic, M.; Mozina, M.; Polajnar, M.; Toplak, M.; Staric, A.; et al. Orange: Data Mining Toolbox in Python. J. Mach. Learn. Res. 2013, 14, 2349–2353. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0 Contributors. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Downregulated | EEC G1 vs. N | EEC G3 vs. N | EEC G3 vs. G1 | ||||||
| miRNA | FC | p-Value | 95% CI | FC | p-Value | 95% CI | FC | p-Value | 95% CI |
| let-7c-5p | 0.593 | 0.005 | (0.378,0.853) | 0.482 | <0.001 | (0.334,0.665) | 0.812 | 0.359 | (0.525,1.312) |
| miR-125b-5p | 0.199 | <0.001 | (0.101,0.314) | 0.186 | <0.001 | (0.101,0.286) | 0.932 | 0.83 | (0.463,1.966) |
| miR-23b-3p | 0.453 | <0.001 | (0.243,0.693) | 0.351 | <0.001 | (0.154,0.572) | 0.776 | 0.212 | (0.321,1.626) |
| miR-99a-5p | 0.176 | <0.001 | (0.083,0.288) | 0.159 | <0.001 | (0.075,0.259) | 0.901 | 0.777 | (0.390,2.083) |
| miR-145-5p | 0.230 | <0.001 | (0.099,0.390) | 0.262 | <0.001 | (0.034, 0.523) | 1.138 | 0.808 | (0.148,3.143) |
| EEC vs. N | SEC vs. N | SEC vs EEC | |||||||
| FC | p-Value | 95% CI | FC | p-Value | 95% CI | FC | p-Value | 95% CI | |
| let-7g-5p | 1.059 | 0.700 | (0.773,1.397) | 0.518 | <0.001 | (0.371,0.692) | 0.490 | <0.001 | (0.339,0.703) |
| miR-195-5p | 0.423 | <0.001 | (0.333,0.534) | 0.409 | 0.0005 | (0.139,0.699) | 0.966 | 0.917 | (0.335,1.658) |
| miR-34a-5p | 0.658 | 0.003 | (0.515,0.846) | 0.480 | 0.001 | (0.242,0.752) | 0.729 | 0.172 | (0.373,1.126) |
| miR-497-5p | 0.256 | <0.001 | (0.180,0.351) | 0.081 | <0.001 | (0.054,0.115) | 0.318 | <0.001 | (0.204,0.480) |
| miR-143-3p | 0.185 | <0.001 | (0.112,0.287) | 0.089 | <0.001 | (0.040,0.152) | 0.481 | 0.023 | (0.212,0.896) |
| miR-424-5p | 0.263 | <0.001 | (0.109,0.442) | 0.074 | <0.001 | (0.0450,0.110) | 0.281 | 0.018 | (0.148,0.699) |
| EC Subypes | let-7c-5p | miR-125b-5p | miR-23b-3p | miR-99a-5p | miR-145-5p | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| FC | p-Value | FC | p-Value | FC | p-Value | FC | p-Value | FC | p-Value | |
| CaSa vs. N | 0.726 | 0.187 | 0.156 | <0.001 | 0.229 | <0.001 | 0.121 | <0.001 | 0.052 | <0.001 |
| CCC vs. N | 0.386 | <0.001 | 0.160 | <0.001 | 0.301 | <0.001 | 0.104 | <0.001 | 0.136 | <0.001 |
| MC vs. N | 0.635 | 0.232 | 0.087 | <0.001 | 0.353 | <0.001 | 0.076 | <0.001 | 0.112 | <0.001 |
| CaSa vs. EEC G1 | 1.223 | 0.526 | 0.782 | 0.432 | 0.505 | 0.048 | 0.681 | 0.279 | 0.044 | <0.001 |
| CaSa vs. EEC G3 | 1.507 | 0.215 | 0.839 | 0.543 | 0.651 | 0.252 | 0.756 | 0.415 | 0.071 | <0.001 |
| CCC vs. EEC G1 | 0.650 | 0.151 | 0.800 | 0.574 | 0.664 | 0.247 | 0.589 | 0.249 | 0.663 | 0.164 |
| CCC vs. EEC G3 | 0.802 | 0.431 | 0.859 | 0.692 | 0.856 | 0.690 | 0.654 | 0.355 | 1.069 | 0.801 |
| MC vs. EEC G1 | 1.070 | 0.884 | 0.434 | 0.128 | 0.779 | 0.564 | 0.431 | 0.090 | 0.094 | <0.001 |
| MC vs. EEC G3 | 1.319 | 0.585 | 0.466 | 0.156 | 1.005 | 0.992 | 0.478 | 0.134 | 0.152 | <0.001 |
| CaSa vs. CCC | 1.880 | 0.109 | 0.977 | 0.950 | 0.761 | 0.432 | 1.155 | 0.738 | 0.385 | 0.168 |
| CaSa vs. MC | 1.143 | 0.777 | 1.801 | 0.265 | 0.648 | 0.421 | 1.581 | 0.305 | 0.467 | 0.402 |
| CCC vs. MC | 0.608 | 0.399 | 1.844 | 0.328 | 0.851 | 0.745 | 1.369 | 0.607 | 1.214 | 0.785 |
| EC Subtypes | let-7g-5p | miR-195-5p | miR-34a-5p | miR-497-5p | miR-143-3p | miR-424-5p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FC | p-Value | FC | p-Value | FC | p-Value | FC | p-Value | FC | p-Value | FC | p-Value | |
| CaSa vs. N | 0.593 | 0.005 | 0.239 | <0.001 | 0.431 | 0.002 | 0.120 | <0.001 | 0.054 | <0.001 | 0.186 | <0.001 |
| CCC vs. N | 0.912 | 0.693 | 0.341 | <0.001 | 0.454 | <0.001 | 0.116 | <0.001 | 0.103 | <0.001 | 0.098 | <0.001 |
| MC vs. N | 2.108 | 0.506 | 0.547 | 0.023 | 0.529 | 0.008 | 0.173 | <0.001 | 0.057 | <0.001 | 0.131 | <0.001 |
| CaSa vs. EEC | 0.560 | 0.008 | 0.565 | 0.0001 | 0.655 | 0.151 | 0.467 | 0.005 | 0.293 | <0.001 | 0.709 | 0.428 |
| CaSa vs. SEC | 1.144 | 0.567 | 0.585 | 0.222 | 0.899 | 0.793 | 1.470 | 0.275 | 0.608 | 0.176 | 2.522 | 0.073 |
| CCC vs. EEC | 0.861 | 0.552 | 0.806 | 0.322 | 0.689 | 0.127 | 0.454 | 0.008 | 0.557 | 0.096 | 0.372 | 0.041 |
| CCC vs. SEC | 1.759 | 0.084 | 0.835 | 0.659 | 0.945 | 0.874 | 1.428 | 0.389 | 1.157 | 0.743 | 1.325 | 0.316 |
| MC vs. EEC | 1.992 | 0.528 | 1.293 | 0.421 | 0.804 | 0.335 | 0.675 | 0.101 | 0.308 | 0.034 | 0.499 | 0.168 |
| MC vs. SEC | 4.067 | 0.354 | 1.339 | 0.479 | 1.103 | 0.763 | 2.123 | 0.048 | 0.639 | 0.517 | 1.777 | 0.348 |
| CaSa vs. CCC | 0.650 | 0.185 | 0.700 | 0.194 | 0.951 | 0.905 | 1.029 | 0.946 | 0.526 | 0.184 | 1.904 | 0.161 |
| CaSa vs. MC | 0.281 | 0.375 | 0.437 | 0.085 | 0.815 | 0.716 | 0.693 | 0.207 | 0.951 | 0.949 | 1.420 | 0.495 |
| CCC vs. MC | 0.432 | 0.477 | 0.623 | 0.225 | 0.857 | 0.648 | 0.673 | 0.278 | 1.810 | 0.407 | 0.746 | 0.580 |
| Variables | N | % | |
|---|---|---|---|
| All patients | 182 | 100 | |
| Histological subtype | EEC | 92 | 50.55 |
| SEC | 44 | 24.18 | |
| CaSa | 21 | 11.54 | |
| CCC | 20 | 10.99 | |
| MC | 5 | 2.75 | |
| Grade | EEC grade 1 | 45 | 48.91 |
| EEC grade 3 | 47 | 51.09 | |
| Low * | 50 | 27.47 | |
| High ** | 132 | 72.53 | |
| FIGO stage | IA | 70 | 38.46 |
| IB | 24 | 13.19 | |
| II | 22 | 12.09 | |
| IIIA | 6 | 3.3 | |
| IIIB | 1 | 0.55 | |
| IIIC1 | 18 | 9.89 | |
| IIIC2 | 9 | 4.95 | |
| IVB | 32 | 17.58 | |
| T (tumor) | T1a | 82 | 45.05 |
| T1b | 33 | 18.13 | |
| T2 | 34 | 18.68 | |
| T3a | 28 | 15.38 | |
| T3b | 5 | 2.75 | |
| LN status | N0 | 98 | 70.5 |
| N1 | 31 | 22.3 | |
| N2 | 10 | 7.19 | |
| Metastatic status | Negative | 85 | 72.65 |
| Positive | 32 | 27.35 | |
| HR status | ER−/PR− | 51 | 28.02 |
| ER+/PR+ | 111 | 60.99 | |
| ER+/PR− | 18 | 9.89 | |
| ER−/PR+ | 2 | 1.1 | |
| ER status | Positive | 129 | 70.88 |
| Negative | 53 | 29.12 | |
| PR status | Positive | 113 | 62.09 |
| Negative | 69 | 37.91 | |
| p53 status | Negative | 111 | 60.99 |
| Positive | 71 | 39.01 | |
| Ki-67 proliferative index | Low | 69 | 37.91 |
| High | 113 | 62.09 | |
| Tumor Characteristics | ER, PR, Ki67, P53 | ER, PR, Ki67, P53, T, P53, T, FIGO, Grade | ER%, PR%, Ki67%, Age | ER%, PR%, Ki67%, P53, Age, T, FIGO, Grade | ||||
|---|---|---|---|---|---|---|---|---|
| Prediction | Prediction | Prediction | Prediction | |||||
| % (95% ±ΔCI) | % (95% ±ΔCI) | % (95% ±ΔCI) | % (95% ±ΔCI) | |||||
| miRNA -497-5p | without | with | without | with | without | with | without | with |
| EEC G1 | 86.7 (8.3) | 88.9 (8.0) | 91.1 (6.31) | 93.3 (5.99) | 75.6 (10.2) | 77.8 (10.4) | 88.9 (6.7) | 93.3 (6.0) |
| EEC G3 | 66.0 (11.3) | 72.3 (10.9) | 61.7 (11.8) | 59.6 (12.2) | 46.8 (12.6) | 51.1 (12.1) | 59.6 (12.3) | 61.7 (12.1) |
| SEC | 59.1 (11.9) | 65.9 (11.6) | 59.1 (12.0) | 52.3 (12.7) | 63.6 (12.9) | 63.6 (12.5) | 47.7 (12.6) | 52.3 (12.3) |
| CaSa | 47.6 (14.2) | 28.6 (15.2) | 71.4 (13.1) | 57.1 (13.4) | 42.9 (14.0) | 47.6 (13.6) | 61.9 (12.4) | 61.9 (13.1) |
| CCC | 55.0 (7.1) | 50.0 (7.1) | 50.0 (11.3) | 45.0 (11.7) | 55.0 (10.4) | 45.0 (11.3) | 50.0 (11.7) | 50.0 (11.3) |
| MC | 0.0 (20.0) | 0.0 (20.8) | 0.0 (14.2) | 0.0 (15.0) | 0.0 (14.2) | 0.0 (15.7) | 20.0 (15.7) | 20.0 (14.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fridrichova, I.; Kalinkova, L.; Karhanek, M.; Smolkova, B.; Machalekova, K.; Wachsmannova, L.; Nikolaieva, N.; Kajo, K. miR-497-5p Decreased Expression Associated with High-Risk Endometrial Cancer. Int. J. Mol. Sci. 2021, 22, 127. https://doi.org/10.3390/ijms22010127
Fridrichova I, Kalinkova L, Karhanek M, Smolkova B, Machalekova K, Wachsmannova L, Nikolaieva N, Kajo K. miR-497-5p Decreased Expression Associated with High-Risk Endometrial Cancer. International Journal of Molecular Sciences. 2021; 22(1):127. https://doi.org/10.3390/ijms22010127
Chicago/Turabian StyleFridrichova, Ivana, Lenka Kalinkova, Miloslav Karhanek, Bozena Smolkova, Katarina Machalekova, Lenka Wachsmannova, Nataliia Nikolaieva, and Karol Kajo. 2021. "miR-497-5p Decreased Expression Associated with High-Risk Endometrial Cancer" International Journal of Molecular Sciences 22, no. 1: 127. https://doi.org/10.3390/ijms22010127
APA StyleFridrichova, I., Kalinkova, L., Karhanek, M., Smolkova, B., Machalekova, K., Wachsmannova, L., Nikolaieva, N., & Kajo, K. (2021). miR-497-5p Decreased Expression Associated with High-Risk Endometrial Cancer. International Journal of Molecular Sciences, 22(1), 127. https://doi.org/10.3390/ijms22010127