Levels of Circulating Fibroblast Growth Factor 23 (FGF23) and Prognosis in Cancer Patients with Bone Metastases

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
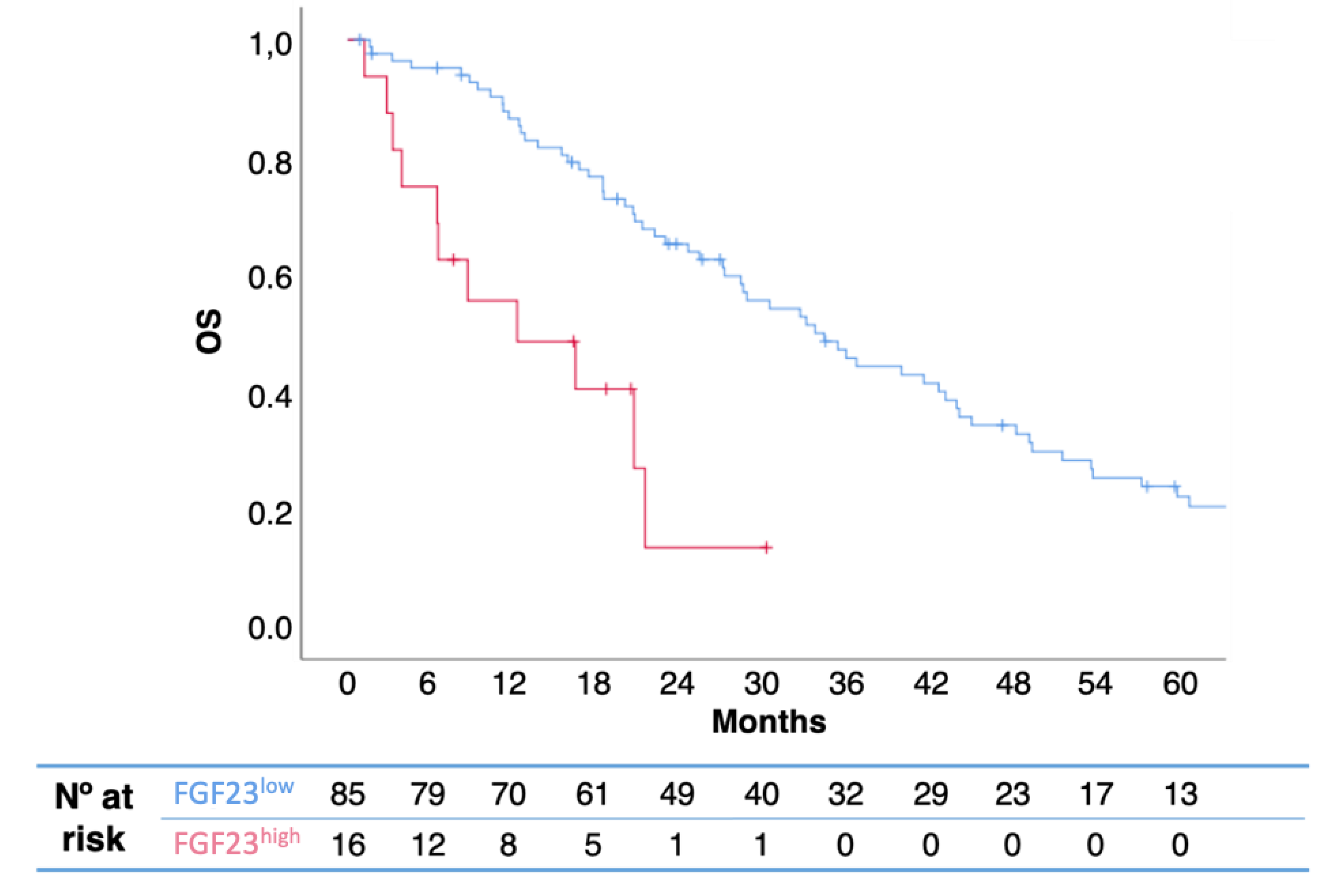
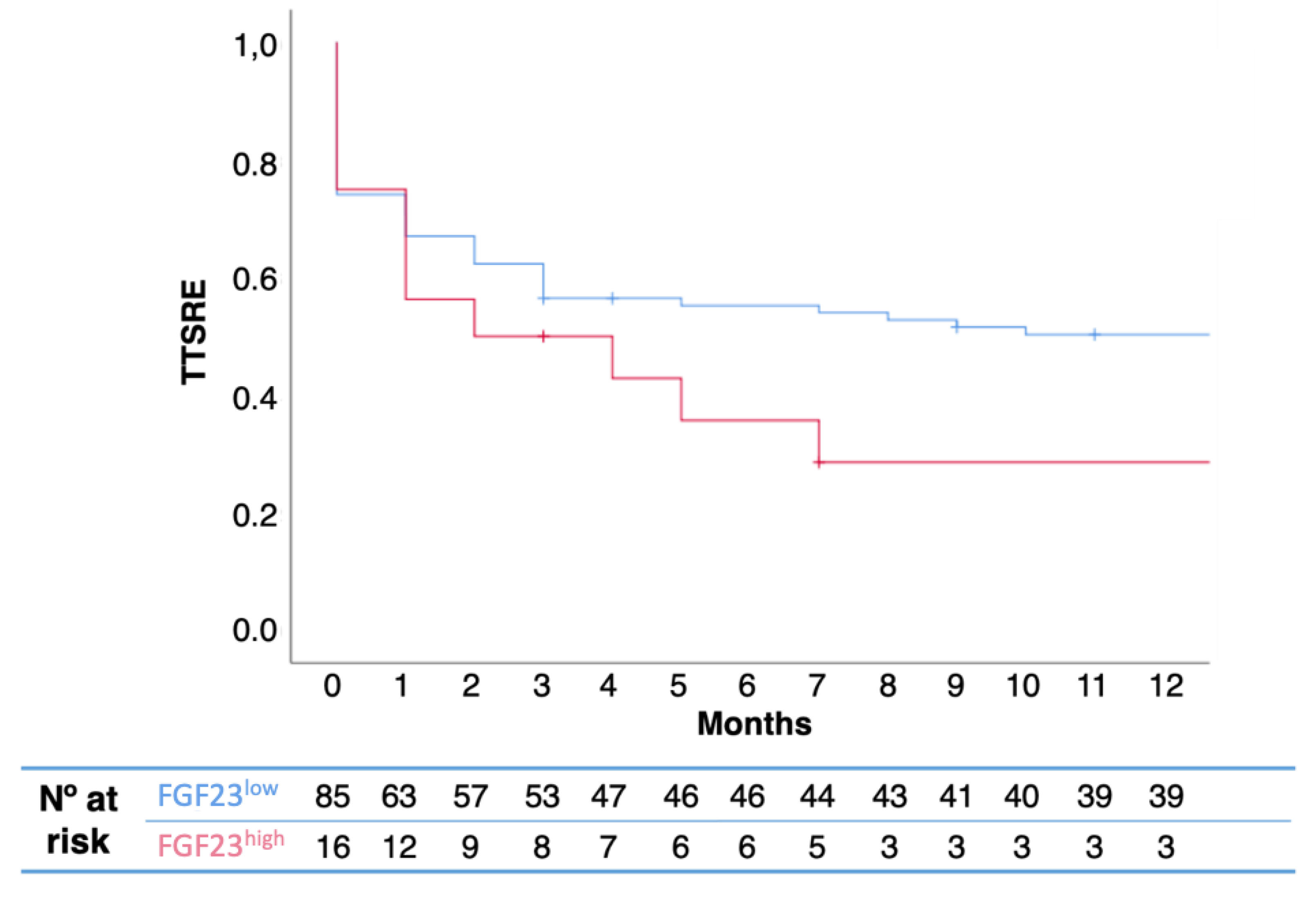
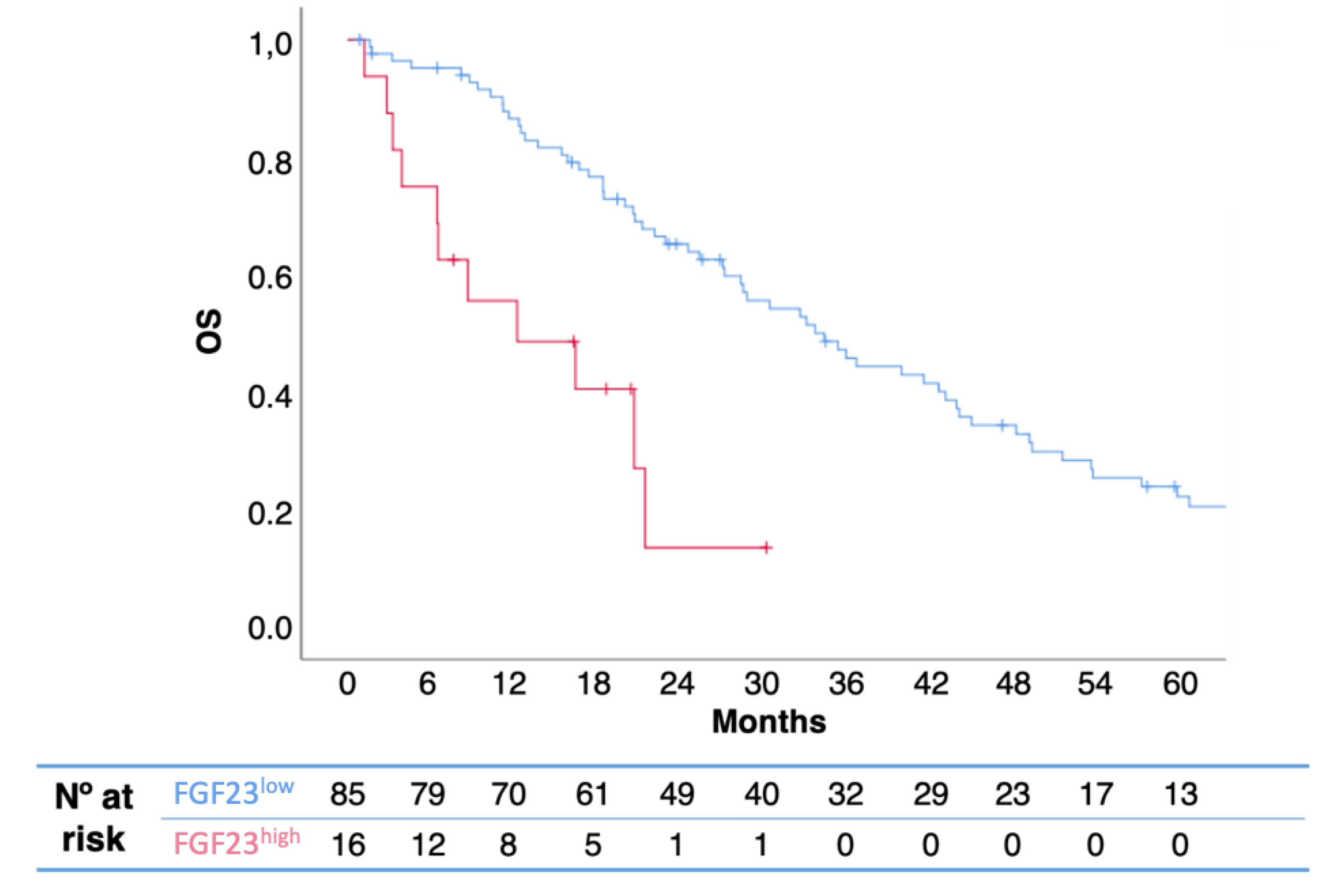
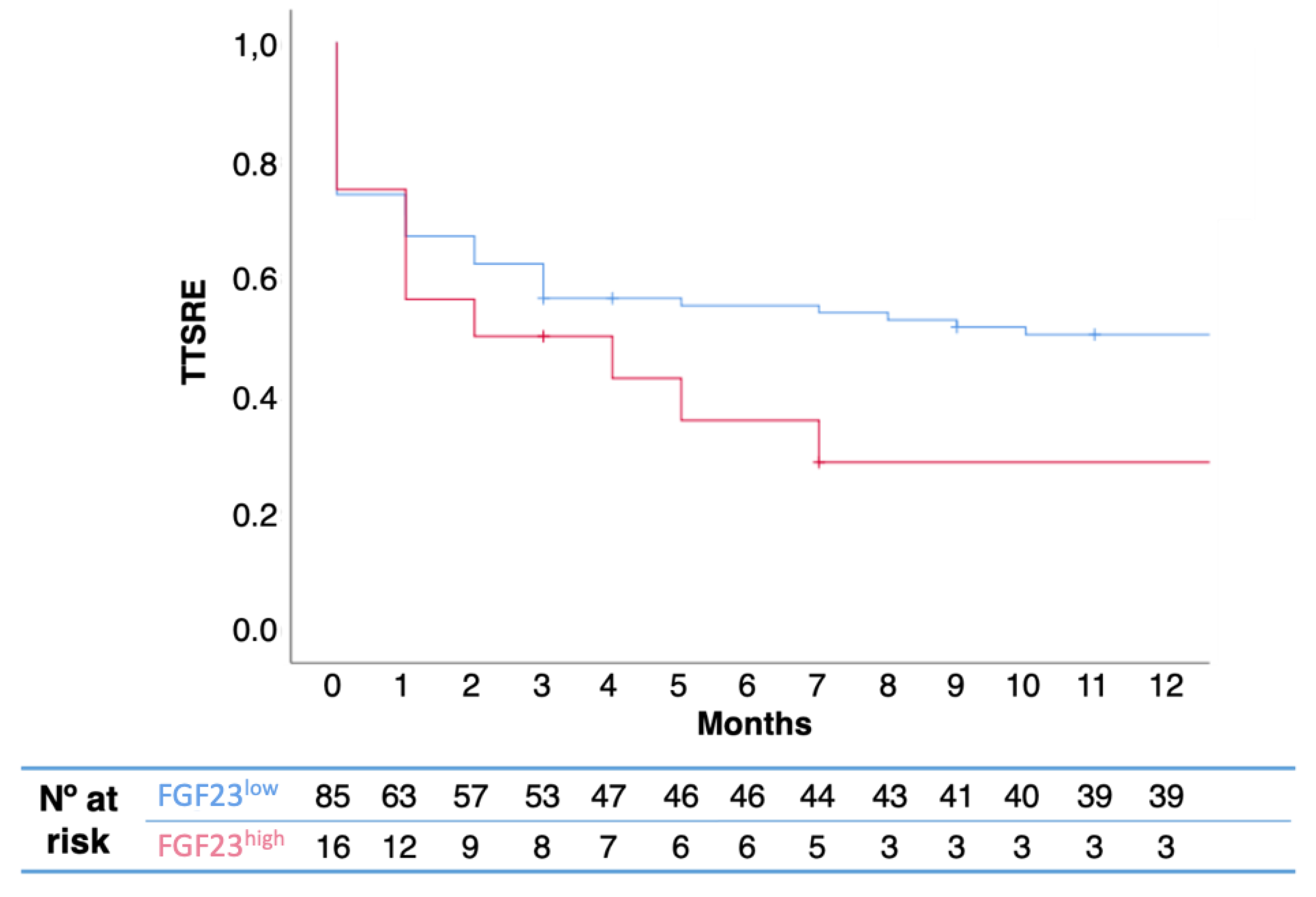
2.2. Survival Analysis
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. uNTX and FGF23 Determination
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ALP | alkaline phosphatase |
| BCE | bone collagen equivalent |
| BTA | bone-targeted agents |
| ELISA | enzyme-linked immunosorbent assay |
| FGF | fibroblast growth factor |
| FGF | fibroblast growth factor receptor |
| HR | hazard ratio |
| IQR | interquartile range |
| OS | overall survival |
| PTH | parathyroid hormone |
| SRE | skeletal-related event |
| TIO | tumor-induced osteomalacia |
| TTSRE | time to skeletal-related events |
| uNTX | urinary N-terminal telopeptide |
References
- Itoh, N.; Ornitz, D.M. Evolution of the FGF and FGFR gene families. Trends Genet. 2004, 20, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Yoshioka, M.; Itoh, N. Identification of a novel fibroblast growth factor, FGF-23, preferentially expressed in the ventrolateral thalamic nucleus of the brain. Biochem. Biophys. Res. Commun. 2000, 277, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Shimada, T.; Mizutani, S.; Muto, T.; Yoneya, T.; Hino, R.; Takeda, S.; Takeuchi, Y.; Fujita, T.; Fukumoto, S.; Yamashita, T. Cloning and characterization of FGF23 as a causative factor of tumor-induced osteomalacia. Proc. Natl. Acad. Sci. USA 2001, 98, 6500–6505. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Guo, R.; Simpson, L.G.; Xiao, Z.S.; Burnham, C.E.; Quarles, L.D. Regulation of fibroblastic growth factor 23 expression but not degradation by PHEX. J. Biol. Chem. 2003, 278, 37419–37426. [Google Scholar] [CrossRef] [PubMed]
- Larsson, T.; Marsell, R.; Schipani, E.; Ohlsson, C.; Ljunggren, O.; Tenenhouse, H.S.; Jüppner, H.; Jonsson, K.B. Transgenic mice expressing fibroblast growth factor 23 under the control of the alpha1(I) collagen promoter exhibit growth retardation, osteomalacia, and disturbed phosphate homeostasis. Endocrinology 2004, 145, 3087–3094. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Miao, D.; Li, J.; Goltzman, D.; Karaplis, A.C. Transgenic mice overexpressing human fibroblast growth factor 23 (R176Q) delineate a putative role for parathyroid hormone in renal phosphate wasting disorders. Endocrinology 2004, 145, 5269–5279. [Google Scholar] [CrossRef] [PubMed]
- Razzaque, M.S. The FGF23-Klotho axis: Endocrine regulation of phosphate homeostasis. Nat. Rev. Endocrinol. 2009, 5, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Shimada, T.; Hasegawa, H.; Yamazaki, Y.; Muto, T.; Hino, R.; Takeuchi, Y.; Fujita, T.; Nakahara, K.; Fukumoto, S.; Yamashita, T. FGF-23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J. Bone Miner. Res. 2004, 19, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Winer, K.; Econs, M.J.; Marx, S.J.; Collins, M.T. FGF-23 is elevated by chronic hyperphosphatemia. J. Clin. Endocrinol. Metab. 2004, 89, 4489–4492. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Wang, J.; Zhang, Y.; Creighton, C.J.; Ittmann, M. FGF23 promotes prostate cancer progression. Oncotarget 2015, 6, 17291–17301. [Google Scholar] [CrossRef] [PubMed]
- Lipton, A.; Smith, M.R.; Fizazi, K.; Stopeck, A.T.; Henry, D.; Brown, J.E.; Shore, N.D.; Saad, F.; Spencer, A.; Zhu, L.; et al. Changes in Bone Turnover Marker Levels and Clinical Outcomes in Patients with Advanced Cancer and Bone Metastases Treated with Bone Antiresorptive Agents. Clin. Cancer Res. 2016, 22, 5713–5721. [Google Scholar] [CrossRef] [PubMed]
- Bluemn, E.G.; Coleman, I.M.; Lucas, J.M.; Coleman, R.T.; Hernandez-Lopez, S.; Tharakan, R.; Bianchi-Frias, D.; Dumpit, R.F.; Kaipainen, A.; Corella, A.N.; et al. Androgen Receptor Pathway-Independent Prostate Cancer Is Sustained through FGF Signaling. Cancer Cell 2017, 32, 474–489.e6. [Google Scholar] [CrossRef] [PubMed]
- Formisano, L.; Stauffer, K.M.; Young, C.D.; Bhola, N.E.; Guerrero-Zotano, A.L.; Jansen, V.M.; Estrada, M.M.; Hutchinson, K.E.; Giltnane, J.M.; Schwarz, L.J.; et al. Association of FGFR1 with ERα Maintains Ligand-Independent ER Transcription and Mediates Resistance to Estrogen Deprivation in ER+ Breast Cancer. Clin. Cancer Res. 2017, 23, 6138–6150. [Google Scholar] [CrossRef] [PubMed]
- Minisola, S.; Peacock, M.; Fukumoto, S.; Cipriani, C.; Pepe, J.; Tella, S.H.; Collins, M.T. Tumour-induced osteomalacia. Nat. Rev. Dis. Primers 2017, 3, 17044. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Shao, L.; Castro, P.; Coleman, I.; Nelson, P.S.; Smith, P.D.; Davies, B.R.; Ittmann, M. Combination treatment of prostate cancer with FGF receptor and AKT kinase inhibitors. Oncotarget 2017, 8, 6179–6192. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; Frezzetti, D.; Gallo, M.; Normanno, N. FGFR-targeted therapeutics for the treatment of breast cancer. Expert Opin. Investig. Drugs 2017, 26, 303–311. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | FGF23low (n = 94) | FGF23high (n = 18) | p |
|---|---|---|---|
| Age, years | |||
| Average ± SD | 57.4 ± 14.1 | 57.9 ± 5.6 | 0.360 |
| Median (IQR) | 57.5 (45.9–68.3) | 58.9 (56.2–61.9) | |
| Tumor type, n (%) | |||
| Breast | 58 (65.2) | 8 (53.3) | 0.096 |
| Prostate | 16 (18.0) | 1 (6.7) | |
| Others (Renal Cell Carcinoma—9; Biliary adenocarcinoma—1; Gastric adenocarcinoma—1; Sarcoma—3; Urothelial—4; Lung adenocarcinoma—1; Neuroendocrine—1; Cervix squamous carcinoma—1) | 15 (16.9) | 6 (40.0) | |
| Extraskeletal metastases, n (%) | |||
| Yes | 51 (60.0) | 12 (80.0) | 0.161 |
| No | 34 (40.0) | 3 (20.0) | |
| Time to BTA, median months | 1.10 | 1.28 | 0.161 |
| uNTX, nmol BCE/mmol creatinine | |||
| Median (IQR) | 118.0 | 824.3 | 0.040 |
| NTXhigh, n (%) | 45 (52.9) | 6 (66.7) | 0.501 |
| NTXlow, n (%) | 40 (47.1) | 3 (33.3) | |
| Calcium, n (%) | |||
| Hypercalcemia | 15 (17.0) | 6 (37.5) | 0.113 |
| Normal range | 66 (75.0) | 10 (62.5) | |
| Hypocalcemia | 7 (8.0) | 0 (0.0) | |
| Median (IQR) | 9.7 (9.4–10.1) | 10.5 (9.9–11.05) | 0.883 |
| Median (95% CI) | Univariate HR (95% CI) | p | Multivariate HR (95% CI) | p | |
|---|---|---|---|---|---|
| FGF23 | |||||
| FGF23low | 34.4 (26.4–42.3) | 0.27 (0.14–0.55) | 0.001 | 0.18 (0.07–0.44) | 0.001 |
| FGF23high | 12.2 (0.0–25.1) | ||||
| Hypercalcemia | |||||
| No | 34.4 (22.8–45.9) | 0.55 (0.32–0.97) | 0.036 | 0.62 (0.34–1.15) | 0.133 |
| Yes | 18.5 (6.9–30.0) | ||||
| Pathologic fractures | |||||
| No | 28.8 (19.3–38.3) | 1.03 (0.60–1.77) | 0.911 | 1.13 (0.63–2.00) | 0.689 |
| Yes | 34.4 (13.8–55.0) | ||||
| Extraskeletal metastases | |||||
| No | 43.9 (35.6–52.2) | 0.63 (0.39–1.02) | 0.058 | 0.62 (0.37–1.04) | 0.070 |
| Yes | 22.9 (17.5–28.3) |
| SRE, n (%) | FGFlow | FGFhigh | p Value |
|---|---|---|---|
| Yes | 54 (57.4) | 6 (33.3) | 0.603 |
| No | 40 (42.6) | 12 (66.7) | |
| Median (IQR) | 1 (0.0–2.0) | 1 (1.0–1.5) | 0.419 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mansinho, A.; Ferreira, A.R.; Casimiro, S.; Alho, I.; Vendrell, I.; Costa, A.L.; Sousa, R.; Abreu, C.; Pulido, C.; Macedo, D.; et al. Levels of Circulating Fibroblast Growth Factor 23 (FGF23) and Prognosis in Cancer Patients with Bone Metastases. Int. J. Mol. Sci. 2019, 20, 695. https://doi.org/10.3390/ijms20030695
Mansinho A, Ferreira AR, Casimiro S, Alho I, Vendrell I, Costa AL, Sousa R, Abreu C, Pulido C, Macedo D, et al. Levels of Circulating Fibroblast Growth Factor 23 (FGF23) and Prognosis in Cancer Patients with Bone Metastases. International Journal of Molecular Sciences. 2019; 20(3):695. https://doi.org/10.3390/ijms20030695
Chicago/Turabian StyleMansinho, André, Arlindo R. Ferreira, Sandra Casimiro, Irina Alho, Inês Vendrell, Ana Lúcia Costa, Rita Sousa, Catarina Abreu, Catarina Pulido, Daniela Macedo, and et al. 2019. "Levels of Circulating Fibroblast Growth Factor 23 (FGF23) and Prognosis in Cancer Patients with Bone Metastases" International Journal of Molecular Sciences 20, no. 3: 695. https://doi.org/10.3390/ijms20030695
APA StyleMansinho, A., Ferreira, A. R., Casimiro, S., Alho, I., Vendrell, I., Costa, A. L., Sousa, R., Abreu, C., Pulido, C., Macedo, D., Pacheco, T. R., Correia, L., & Costa, L. (2019). Levels of Circulating Fibroblast Growth Factor 23 (FGF23) and Prognosis in Cancer Patients with Bone Metastases. International Journal of Molecular Sciences, 20(3), 695. https://doi.org/10.3390/ijms20030695