TGFBI Protein Is Increased in the Urine of Patients with High-Grade Urothelial Carcinomas, and Promotes Cell Proliferation and Migration

 and
and
Abstract
1. Introduction
2. Results
2.1. Antibody Array Analyses Identify TGFBI and PF4 as Biomarker Candidates in Urine
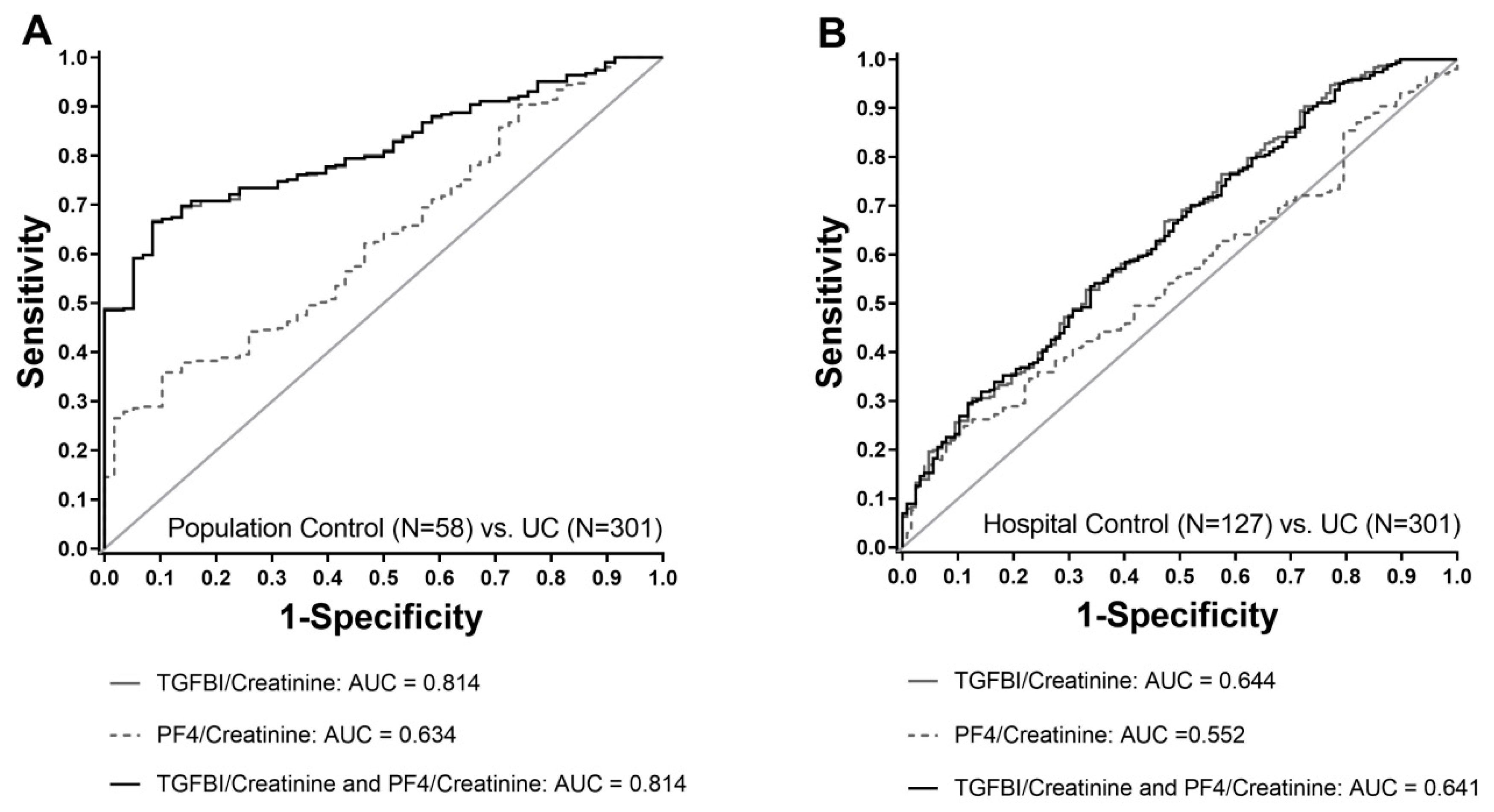
2.2. Verification by ELISA Shows Better Performance of TGFBI Compared to PF4
2.3. TGFBI Predominantly Identifies Muscle Invasive and High-Grade UC
2.4. Clinically Relevant Sample Characteristics Influence TGFBI Concentrations in Urine
2.5. TGFBI Is Required for Bladder Cancer Cell Proliferation
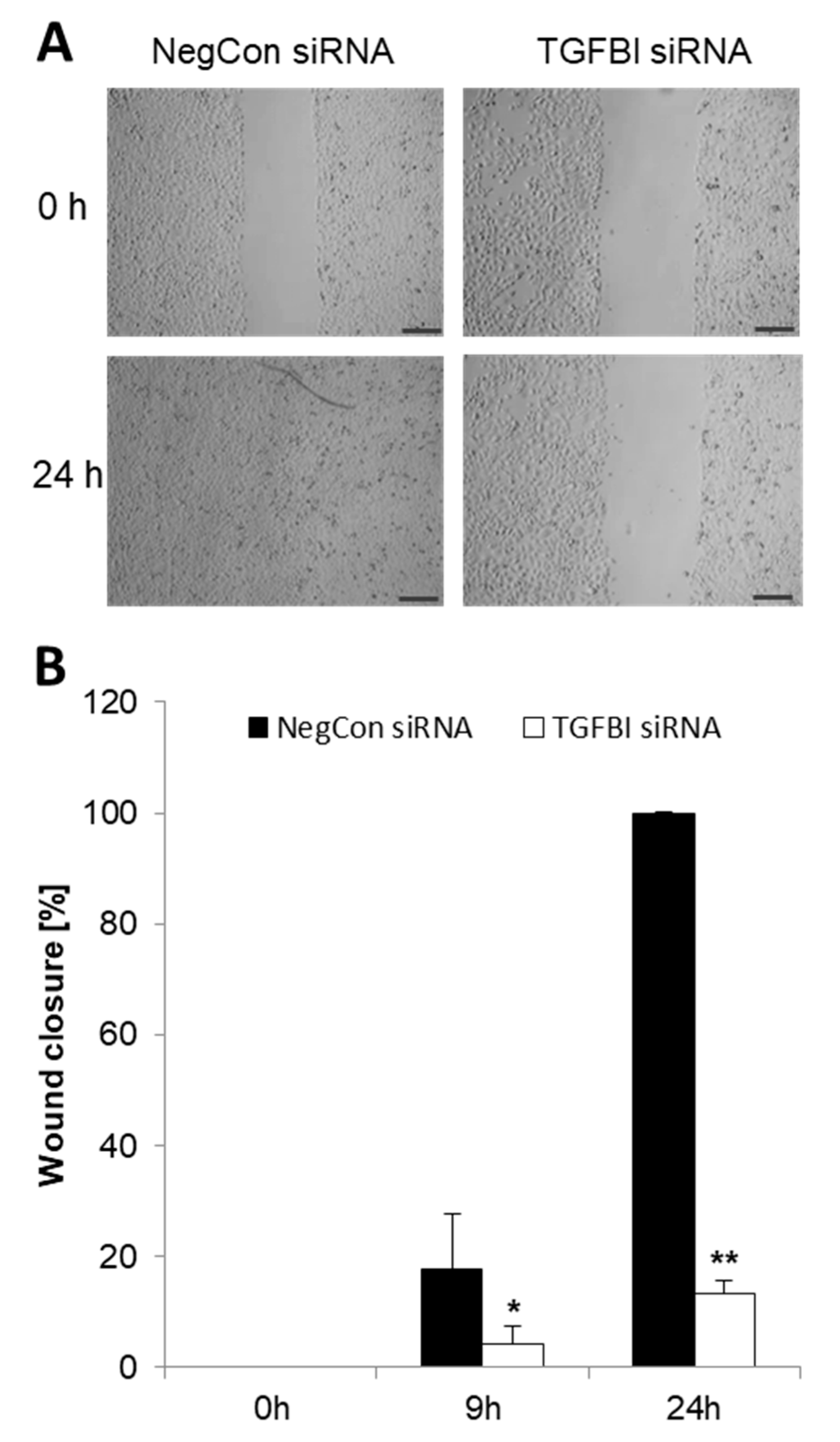
2.6. Elevated TGFBI Secretion in Bladder Cancer Cells Is Associated with Increased Cell Migration
2.7. TGFBI Secretion Is Partially Induced via TGFβ Receptor 1 (TGFβR1)
3. Discussion
4. Materials and Methods
4.1. Subjects and Urine Collection
4.2. Sample Preparation
4.3. Antibody Arrays
4.4. Cell Culture
4.5. Enzyme-Linked Immunosorbent Assay
4.6. siRNA Mediated Gene Silencing
4.7. Protein Isolation and Immunoblotting
4.8. Wound Closure Assay
4.9. BrdU Cell Cycle Assays
4.10. Statistics
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AUC | area under curve |
| CI | confidence interval |
| FDA | Food and Drug Administration |
| H | Hour |
| HRP | horseradish-peroxidase |
| IQR | interquartile range |
| NMP22 | nuclear matrix protein 22 |
| PF4 | platelet factor 4 |
| PURE | Protein Research Unit Ruhr within Europe |
| RT | room temperature |
| ROC | receiver operating characteristic curves |
| SOP | standard operating procedure |
| TGFBI | transforming growth factor beta-induced |
| UC | urothelial carcinoma |
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Black, P.C.; Brown, G.A.; Dinney, C.P. Molecular markers of urothelial cancer and their use in the monitoring of superficial urothelial cancer. J. Clin. Oncol. 2006, 24, 5528–5535. [Google Scholar] [CrossRef]
- Kamat, A.M.; Hahn, N.M.; Efstathiou, J.A.; Lerner, S.P.; Malmström, P.; Choi, W.; Guo, C.C.; Lotan, Y.; Kassouf, W. Bladder Cancer. Lancet 2016, 388, 2796–2810. [Google Scholar] [CrossRef]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumors of the Urinary System and Male Genital Organs-Part B: Prostate and Bladder Tumors. Eur. Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Millan-Rodriguez, F.; Chechile-Toniolo, G.; Salvador-Bayarri, J.; Palou, J.; Vicente-Rodriguez, J. Multivariate analysis of the prognostic factors of primary superficial bladder cancer. J. Urol. 2000, 163, 73–78. [Google Scholar] [CrossRef]
- Burger, M.; van der Aa, M.N.; van Oers, J.M.; Brinkmann, A.; van der Kwast, T.H.; Steyerberg, E.C.; Stoehr, R.; Kirkels, W.J.; Denzinger, S.; Wild, P.J.; et al. Prediction of progression of non-muscle invasive bladder cancer by WHO 1973 and 2004 grading and by FGFR3 mutation status: A prospective study. Eur. Urol. 2008, 54, 835–843. [Google Scholar] [CrossRef]
- Chen, Z.; Ding, W.; Xu, K.; Tan, J.; Sun, C.; Gou, Y.; Tong, S.; Xia, G.; Fang, Z.; Ding, Q. The 1973 WHO Classification is more suitable than the 2004 WHO Classification for predicting prognosis in non-muscle invasive bladder cancer. PLoS ONE 2012, 7, e47199. [Google Scholar] [CrossRef]
- Eble, J.N.; Sauter, G.; Epstein, J.; Sesterhenn, I. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs, WHO Classification of Tumours, 3rd ed.; World Health Organization: Geneva, Switzerland, 2004; Volume 7, Available online: http://publications.iarc.fr/Book-And-Report-Series/Who-Iarc-Classification-Of-Tumours (accessed on 10 September 2019).
- Moch, H.; Humphrey, P.A.; Ulbright, T.M.; Reuter, V.E. WHO Classification of Tumours of the Urinary System and Male Genital Organs, WHO Classification of Tumours, 4th ed.; World Health Organization: Geneva, Switzerland, 2016; Volume 8, Available online: http://publications.iarc.fr/Book-And-Report-Series/Who-Iarc-Classification-Of-Tumours (accessed on 10 September 2019).
- Compérat, E.M.; Burger, M.; Gontero, P.; Mostafid, A.H.; Palou, J.; Rouprêt, M.; van Rhijn, B.W.G.; Shariat, S.F.; Sylvester, R.J.; Zigeuner, R.; et al. Grading of urothelial carcinoma and the new “World Health Organisation Classification of Tumors of the Urinary System and Male Genital Organs 2016”. Eur. Urol. Focus 2019, 5, 457–466. [Google Scholar] [CrossRef]
- Jordan, B.; Meeks, J.J. T1 bladder cancer: current considerations for diagnosis and management. Nat. Rev. Urol. 2019, 16, 23–34. [Google Scholar] [CrossRef]
- Tomasini, J.M.; Konety, B.R. Urinary markers/cytology: what and when should a urologist use. Urol. Clin. North Am. 2013, 40, 165–173. [Google Scholar] [CrossRef]
- Glas, A.S.; Roos, D.; Deutekom, M.; Zwinderman, A.H.; Bossuyt, P.M.; Kurth, K.H. Tumor markers in the diagnosis of primary bladder cancer. A systematic review. J. Urol. 2003, 169, 1975–1982. [Google Scholar] [CrossRef] [PubMed]
- Van Rhijn, B.W.; van der Poel, H.G.; van der Kwast, T.H. Urine markers for bladder cancer surveillance: a systematic review. Eur. Urol. 2005, 47, 736–748. [Google Scholar] [CrossRef] [PubMed]
- Smith, Z.L.; Guzzo, T.J. Urinary markers for bladder cancer. F1000Prime Reports 2013, 5, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Ecke, T.H.; Weiß, S.; Stephan, C.; Hallmann, S.; Arndt, C.; Barski, D.; Otto, T.; Gerullis, H. UBC® Rapid Test—An Urinary Point-of-Care (POC) Assay for Diagnosis of Bladder Cancer with a focus on Non-Muscle Invasive High-grade Tumors: Results of a Multicenter-Study. Int. J. Mol. Sci. 2018, 19, 3841. [Google Scholar] [CrossRef] [PubMed]
- Goebell, P.J.; Groshen, S.G.; Schmitz-Dräger, B.J. International Study-Initiative on Bladder Cancer (ISBC). p53 immunohistochemistry in bladder cancer–a new approach to an old question. Urol. Oncol. 2010, 28, 377–388. [Google Scholar] [CrossRef]
- Witzke, K.E.; Großerüschekamp, F.; Jütte, H.; Horn, M.; Roghmann, F.; von Landenberg, N.; Bracht, T.; Kallenbach-Thieltges, A.; Käfferlein, H.; Brüning, T.; et al. Integrated Fourier transform infrared imaging and proteomics for identification of a candidate histochemical biomarker in bladder cancer. Am. J. Pathol. 2019, 189, 619–631. [Google Scholar] [CrossRef]
- Lang, K.; Bonberg, N.; Robens, S.; Behrens, T.; Hovanec, J.; Deix, T.; Braun, K.; Roghmann, F.; Noldus, J.; Harth, V.; et al. Soluble chemokine (C-X-C motif) ligand 16 (CXCL16) in urine as novel biomarker candidate to identify high-grade and muscle invasive urothelial carcinomas. Oncotarget 2017, 62, 104946–104959. [Google Scholar] [CrossRef]
- Thapa, N.; Lee, B.H.; Kim, I.S. TGFBIp/βig-h3 protein: a versatile matrix molecule induced by TGF-β. Int. Biochem. Cell Biol. 2007, 39, 2183–2194. [Google Scholar] [CrossRef]
- Holmberg, C.; Quante, M.; Steele, I.; Kumar, J.D.; Balabanova, S.; Duval, C.; Czepan, M.; Rakonczay, Z., Jr.; Tiszlavicz, L.; Nemeth, I.; et al. Release of TGFβig-h3 by gastric myofibroblasts slows tumor growth and is decreased with cancer progression. Carcinogenesis 2012, 33, 1553–1562. [Google Scholar] [CrossRef]
- Zhang, Y.; Wen, G.; Shao, G.; Wang, C.; Lin, C.; Fang, H.; Balajee, A.S.; Bhagat, G.; Hei, T.K.; Zhao, Y. TGFBI deficiency predisposes mice to spontaneous tumor development. Cancer Res. 2009, 69, 37–44. [Google Scholar] [CrossRef]
- Bae, J.S.; Lee, S.H.; Kim, J.E.; Choi, J.Y.; Park, R.W.; Yong Park, J.; Park, H.S.; Sohn, Y.S.; Lee, D.S.; Bae Lee, E.; et al. βig-h3 supports keratinocyte adhesion, migration, and proliferation through α3β1 integrin. Biochem. Biophys. Res. Commun. 2002, 294, 940–948. [Google Scholar] [CrossRef]
- Lauden, L.; Siewiera, J.; Boukouaci, W.; Ramgolam, K.; Mourah, S.; Lebbe, C.; Charron, D.; Aoudjit, F.; Jabrane-Ferrat, N.; Al-Daccak, R. TGF-β-induced (TGFBI) protein in melanoma: A signature of high metastatic potential. J. Invest. Dermatol. 2014, 134, 1675–1685. [Google Scholar] [CrossRef] [PubMed]
- Costanza, B.; Rademaker, G.; Tiamiou, A.; De Tullio, P.; Leenders, J.; Blomme, A.; Bellier, J.; Bianchi, E.; Turtoi, A.; Delvenne, P.; et al. Transforming growth factor beta-induced, an extracellular matrix interacting protein, enhances glycolysis and promotes pancreatic cancer cell migration. Int. J. Cancer 2019, 145, 1570–1584. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Rong, Y.; Radiloff, D.R.; Datto, M.B.; Centeno, B.; Bao, S.; Cheng, A.W.; Lin, F.; Jiang, S.; Yeatman, T.J.; et al. Extracellular matrix protein βig-h3/TGFBI promotes metastasis of colon cancer by enhancing cell extravasation. Genes Dev. 2008, 22, 308–321. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kwon, H.J.; Kim, D.S. Matrix metalloproteinase 9 (MMP-9)-dependent processing of βig-h3 protein regulates cell migration, invasion, and adhesion. J. Biol. Chem. 2012, 287, 38957–38969. [Google Scholar] [CrossRef]
- Ween, M.P.; Oehler, M.K.; Ricciardelli, C. Transforming growth Factor-Beta-Induced protein (TGFBI)/(βig-H3): A matrix protein with dual functions in ovarian cancer. Int. J. Mol. Sci. 2012, 13, 10461–10477. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lim, S.W.; Choi, B.S.; Lee, S.H.; Cha, J.H.; Kim, I.S.; Kim, J.; Yang, C.W. Inhibitory effect of pravastatin on transforming growth factor β1-inducible gene h3 expression in a rat model of chronic cyclosporine nephropathy. Am. J. Nephrol. 2005, 25, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Gratchev, A.; Guillot, P.; Hakiy, N.; Politz, O.; Orfanos, C.E.; Schledzewski, K.; Goerdt, S. Alternatively activated macrophages differentially express fibronectin and its splice variants and the extracellular matrix protein βIG-H3. Scand. J. Immunol. 2001, 53, 386–392. [Google Scholar] [CrossRef]
- O‘Brien, E.R.; Bennett, K.L.; Garvin, M.R.; Zderic, T.W.; Hinohara, T.; Simpson, J.B.; Kimura, T.; Nobuyoshi, M.; Mizgala, H.; Purchio, A.; et al. βig-h3, a transforming growth factor-β-inducible gene, is overexpressed in atherosclerotic and restenotic human vascular lesions. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 576–584. [Google Scholar] [CrossRef]
- Zuiverloon, T.C.M.; de Jong, F.C.; Costello, J.C.; Theodorescu, D. Systematic review: Characteristics and preclinical uses of bladder cancer cell lines. Bladder Cancer 2018, 4, 169–183. [Google Scholar] [CrossRef]
- Skonier, J.; Neubauer, M.; Madisen, L.; Bennett, K.; Plowman, G.D.; Purchio, A.F. cDNA cloning and sequence analysis of βig-h3, anovel gene induced in a human adenocarcinoma cell line after treatment with transforming growth factor-beta. DNA Cell Biol. 1992, 11, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, S.V.; Ivanova, A.V.; Salnikow, K.; Timofeeva, O.; Subramaniam, M.; Lerman, M.I. Two novel VHL targets, TGFBI (βIGH3) and its transactivator KLF10, are up-regulated in renal clear cell carcinoma and other tumors. Biochem. Biophys. Res. Commun. 2008, 370, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Chen, X.; Liao, Z.; He, C.; Hu, X. TGFBI protein high expression predicts poor prognosis in colorectal cancer patients. Int. J. Clin. Exp. Pathol. 2015, 8, 702–710. [Google Scholar]
- Lebdai, S.; Verhoest, G.; Parikh, H.; Jacquet, S.F.; Bensalah, K.; Chautard, D.; Rioux Leclercq, N.; Azzouzi, A.R.; Bigot, P. Identification and validation of TGFBI as a promising prognosis marker of clear cell renal cell carcinoma. Urol. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Shang, D.; Liu, Y.; Yang, P.; Chen, Y.; Tian, Y. TGFBI-promoted adhesion, migration and invasion of human renal cell carcinoma depends on inactivation of von Hippel-Lindau tumor suppressor. Urology 2012, 79, 966.e1–966.e7. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.B.; Zhang, C.H.; Wang, S.Q.; Ai, P.H.; Chen, K.; Zhu, L.; Sun, Z.L.; Feng, D.F. Transforming growth factor beta induced (TGFBI) is a potential signature gene for mesenchymal subtype high-grade glioma. J. Neurooncol. 2018, 137, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Cai, H.; Chen, Y.; Hu, B.; Luo, H.; Wu, Y.; Wu, J. The role of TGFBI (βig-h3) in gastrointestinal tract tumorigenesis. Mol. Cancer 2015, 14, 64. [Google Scholar] [CrossRef]
- Shang, D.; Song, B.; Liu, Y. Epirubicin suppresses proliferative and metastatic potential by downregulating transforming growth factor-β-induced expression in urothelial carcinoma. Cancer Sci. 2018, 109, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Huang, R.; Li, H.; Wang, B.; Chen, Y.; Chen, S.; Ou, K.; Wang, X. Secreted TGF transforming growth factor-β-induced expression in bladder cancer cells. Cancer Manag. Res. 2019, 11, 6995–7006. [Google Scholar] [CrossRef]
- Bonsnes, R.W.; Taussky, H.H. On the colorimetric determination of creatinine by the Jaffé reaction. J. Biol. Chem. 1945, 158, 581–591. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TGFBI (pg/mg Creatinine) | PF4 (pg/mg Creatinine) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Population Controls (N = 58) | Urological Hospital Controls (N = 128) | Urothelial Carcinoma (N = 303) | Population Controls (N = 58) | Urological Hospital Controls (N = 127) | Urothelial Carcinoma (N = 301) | ||||||||
| n | Median (IQR) | n | Median (IQR) | n | Median (IQR) | n | Median (IQR) | n | Median (IQR) | n | Median (IQR) | ||
| Total | 58 | 475.6 (282.6–600.0) | 128 | 701.3 (292.3–1882.4) | 303 | 1321.0 (565.2–5311.2) | 58 | 9.6 (3.4–26.7) | 127 | 13.6 (5.7–38.7) | 301 | 17.4 (5.2–126.4) | |
| Age (years) | <70 | 33 | 426.0 (287.7–595.6) | 70 | 617.0 (240.5–1631.7) | 118 | 977.2 (495.9–2479.5) | 33 | 9.2 (3.4–20.6) | 70 | 13.4 (5.7–27.4) | 117 | 14.1 (4.8–58.0) |
| ≥70 | 25 | 498.2 (228.4–624.8) | 58 | 919.3 (388.7–2496.3) | 185 | 1608.4 (608.0–6411.4) | 25 | 14.8 (3.9–30.4) | 57 | 15.5 (5.8–72.4) | 184 | 19.8 (5.4–195.4) | |
| Gender | Men | 47 | 426.0 (258.0–595.6) | 92 | 762.5 (299.0–1816.5) | 251 | 1293.1 (565.2–4575.9) | 47 | 9.3 (3.3–21.4) | 91 | 11.0 (5.4–29.7) | 250 | 15.2 (5.0–83.6) |
| Women | 11 | 568.8 (335.2–660.8) | 36 | 603.9 (178.3–2237.9) | 52 | 1892.3 (548.8–6780.0) | 11 | 22.9 (3.4–34.3) | 36 | 18.9 (8.7–77.2) | 51 | 44.7 (6.6–321.3) | |
| Smoking Status | Non smoker | 21 | 482.9 (283.1–660.8) | 26 | 1189.1 (553.1–2639.8) | 54 | 1530.6 (473.7–6244.2) | 21 | 8.7 (3.3–30.8) | 26 | 18.9 (6.4–42.7) | 54 | 25.2 (5.6–131.2) |
| Former smoker | 29 | 426.0 (231.1–581.3) | 59 | 540.4 (221.5–1516.5) | 146 | 1385.7 (582.7–5321.9) | 29 | 9.9 (4.5–22.0) | 59 | 12.1 (3.8–44.2) | 145 | 14.0 (4.8–86.1) | |
| Smoker | 8 | 328.3 (236.3–571.0) | 32 | 662.2 (437.8–2032.7) | 80 | 1267.4 (642.2–3991.8) | 8 | 11.7 (3.3–28.5) | 31 | 11.0 (4.0–23.8) | 79 | 17.8 (6.2–121.0) | |
| Missing | 0 | 11 | 1131.7 (10.6–3190.7) | 23 | 956.2 (480.1–6818.7) | 0 | 11 | 20.6 (7.7–290.5) | 23 | 16.5 (4.5–230.4) | |||
| Leucocytes | Negative | 45 | 426.0 (258.0–595.6) | 64 | 430.5 (184.2–775.9) | 158 | 894.4 (463.0–2142.4) | 45 | 9.3 (3.3–22.0) | 64 | 13.4 (5.8–27.1) | 156 | 11.8 (4.7–33.1) |
| ~25 | 5 | 600.0 (558.3–624.8) | 27 | 954.4 (492.1–2137.9) | 83 | 1369.1 (603.0–5621.6) | 5 | 4.5 (0.0–16.9) | 26 | 14.7 (5.3–25.3) | 83 | 18.2 (4.9–86.1) | |
| ~100 | 5 | 482.9 (289.0–614.3) | 10 | 1545.5 (620.0–2639.8) | 23 | 4413.7 (1608.4–11,104.3) | 5 | 22.9 (21.4–27.8) | 10 | 8.8 (3.4–42.7) | 23 | 131.0 (8.8–1584.0) | |
| ~500 | 1 | 581.3 | 23 | 2317.9 (819.6–6892.0) | 33 | 26,403.6 (1667.0–62,186.3) | 1 | 3.9 | 23 | 29.7 (6.1–126.2) | 33 | 1568.2 (16.5–4228.9) | |
| Missing | 2 | 324.8 (126.6–523.0) | 4 | 837.7 (537.7–1068.2) | 6 | 2291.7 (792.1–6741.3) | 2 | 39.6 (4.7 - 74.5) | 4 | 9.1 (6.4 - 68.8) | 6 | 17.5 (5.0–76.0) | |
| Erythrocytes $ | Negative-~10 | 52 | 482.6 (282.9–616.6) | 78 | 456.1 (190.9–910.5) | 122 | 612.2 (353.9–1136.3) | 52 | 10.1 (3.9–27.0) | 77 | 11.0 (5.5–22.9) | 120 | 9.6 (4.2–20.9) |
| ~25–50 | 2 | 387.9 (335.2–440.7) | 21 | 1159.1 (552.1–2794.7) | 58 | 1176.0 (533.6–2703.4) | 2 | 2.5 (1.6–3.4) | 21 | 20.2 (5.7–36.1) | 58 | 8.6 (4.2–25.9) | |
| ~150–250 | 1 | 0.0 | 26 | 2549.8 (1516.5–6892.0) | 118 | 5612.2 (1569.0–18,846.9) | 1 | 3.3 | 26 | 59.3 (9.4–223.2) | 118 | 207.1 (19.8–1584.0) | |
| Missing | 3 | 523.0 (126.6–595.6) | 3 | 670.6 (404.8–1004.7) | 5 | 1931.9 (792.1–2651.4) | 3 | 20.6 (4.7–74.5) | 3 | 9.2 (3.8–128.3) | 5 | 5.7 (5.0–76.0) | |
| UC History | No | 57 | 468.9 (282.6–600.0) | 55 | 670.6 (435.0–2268.8) | 195 | 1856.7 (789.3–8193.0) | 57 | 9.3 (3.4–26.7) | 54 | 13.7 (5.3–64.5) | 193 | 26.7 (7.8–294.0) |
| Yes | 0 | 72 | 701.3 (267.8–1462.6) | 108 | 658.2 (362.9–1508.7) | 0 | 72 | 13.3 (5.8–27.4) | 108 | 9.2 (4.3–23.0) | |||
| Missing | 1 | 482.9 | 1 | 13,648.1 | 0 | 1 | 22.9 | 1 | 321.0 | 0 | |||
| Tumor Grading | Low grade 1 | 233 | 943.1 (480.1–2244.0) | 231 | 12.8 (4.8–52.4) | ||||||||
| High-grade | 66 | 8190.7 (2142.4–26,933.5) | 66 | 84.9 (15.0–1402.4) | |||||||||
| Missing | 4 | 2429.2 (1331.2–4279.2) | 4 | 18.1 (11–42.5) | |||||||||
| Tumor Staging | pTa 3 | 160 | 680.0 (385.5–1446.5) | 158 | 10.4 (4.3–33.0) | ||||||||
| pT1 2,4 | 102 | 2387.7 (878.8–8193.0) | 102 | 25.9 (6.6–292.4) | |||||||||
| pT2, pT2a, pT2b 2,5 | 39 | 14,411.7 (2479.5–50875.1) | 39 | 201.9 (19.8–1572.5) | |||||||||
| pTis only 6 | 2 | 2249.3 (1503.6–2995.0) | 2 | 12.3 (8.8–15.9) | |||||||||
| Model 1 | Model 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| N (N+) | Exp(β) | 95% CI | N (N+) | Exp(β) | 95% CI | ||||
| Study group | Population control | 54 (2) | 1 | Study group | Population control | 54 (2) | 1 | ||
| Hospital control | 113 (34) | 7.43 | (1.54–35.72) | Hospital control | 113 (34) | 7.83 | (1.62–37.41) | ||
| UC (low-grade) | 213 (81) | 8.22 | (1.79–37.64) | Non-muscle invasive UC | 243 (106) | 10.20 | (2.18–45.23) | ||
| UC (high-grade) | 58 (50) | 42.34 | (7.60–235.94) | Muscle invasive UC | 32 (28) | 33.84 | (5.40–239.08) | ||
| Gender | Male | 349 (132) | 1 | Gender | Male | 353 (135) | 1 | ||
| Female | 89 (35) | 0.54 | (0.25–1.19) | Female | 89 (35) | 0.57 | (0.27–1.21) | ||
| Age (years) | <70 | 200 (60) | 1 | Age (years) | <70 | 201 (60) | 1 | ||
| ≥70 | 238 (107) | 1.37 | (0.79–2.41) | ≥70 | 241 (110) | 1.58 | (0.91–2.71) | ||
| Leucocytes | Negative | 246 (61) | 1 | Leucocytes | Negative | 248 (63) | 1 | ||
| ~25 | 106 (47) | 1.93 | (1.01–3.67) | ~25 | 107 (48) | 1.82 | (0.98–3.41) | ||
| ~100 | 35 (22) | 3.29 | (1.197–9.06) | ~100 | 36 (22) | 2.69 | (1.01–7.14) | ||
| ~500 | 51 (37) | 4.27 | (1.68–10.90) | ~500 | 51 (37) | 3.91 | (1.47–9.44) | ||
| Erythrocytes | Negative - ~10 | 231 (30) | 1 | Erythrocytes | Negative - ~10 | 234 (32) | 1 | ||
| ~25–50 | 76 (30) | 2.54 | (1.30–4.95) | ~25–50 | 77 (31) | 2.56 | (1.36–4.96) | ||
| ~150–250 | 131 (107) | 12.40 | (6.42–23.93) | ~150–250 | 131 (107) | 12.87 | (6.79–24.49) | ||
| Smoking | Never | 98 (39) | 1 | Smoking | Never | 99 (40) | 1 | ||
| Former | 225 (84) | 0.77 | (0.37–1.60) | Former | 226 (85) | 0.81 | (0.40–1.66) | ||
| Current | 115 (44) | 0.57 | (0.25–1.28) | Current | 117 (45) | 0.62 | (0.28–1.36) | ||
| Former UC | No | 276 (123) | 1 | Former UC | No | 280 (126) | 1 | ||
| Yes | 162 (44) | 0.40 | (0.23–0.72) | Yes | 162 (44) | 0.38 | (0.22–0.68) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lang, K.; Kahveci, S.; Bonberg, N.; Wichert, K.; Behrens, T.; Hovanec, J.; Roghmann, F.; Noldus, J.; Tam, Y.C.; Tannapfel, A.; et al. TGFBI Protein Is Increased in the Urine of Patients with High-Grade Urothelial Carcinomas, and Promotes Cell Proliferation and Migration. Int. J. Mol. Sci. 2019, 20, 4483. https://doi.org/10.3390/ijms20184483
Lang K, Kahveci S, Bonberg N, Wichert K, Behrens T, Hovanec J, Roghmann F, Noldus J, Tam YC, Tannapfel A, et al. TGFBI Protein Is Increased in the Urine of Patients with High-Grade Urothelial Carcinomas, and Promotes Cell Proliferation and Migration. International Journal of Molecular Sciences. 2019; 20(18):4483. https://doi.org/10.3390/ijms20184483
Chicago/Turabian StyleLang, Kerstin, Selcan Kahveci, Nadine Bonberg, Katharina Wichert, Thomas Behrens, Jan Hovanec, Florian Roghmann, Joachim Noldus, Yu Chun Tam, Andrea Tannapfel, and et al. 2019. "TGFBI Protein Is Increased in the Urine of Patients with High-Grade Urothelial Carcinomas, and Promotes Cell Proliferation and Migration" International Journal of Molecular Sciences 20, no. 18: 4483. https://doi.org/10.3390/ijms20184483
APA StyleLang, K., Kahveci, S., Bonberg, N., Wichert, K., Behrens, T., Hovanec, J., Roghmann, F., Noldus, J., Tam, Y. C., Tannapfel, A., Käfferlein, H. U., & Brüning, T. (2019). TGFBI Protein Is Increased in the Urine of Patients with High-Grade Urothelial Carcinomas, and Promotes Cell Proliferation and Migration. International Journal of Molecular Sciences, 20(18), 4483. https://doi.org/10.3390/ijms20184483