Endothelial Dysfunction in Chronic Heart Failure: Assessment, Findings, Significance, and Potential Therapeutic Targets


Abstract
1. Introduction
2. Assessment of Endothelial Function
3. Findings
4. Significance
4.1. Predictive Value of ED in Population-Based Studies
4.2. Predictive Value of ED in the CHF Population
5. Potential Therapeutic Targets for ED in the CHF Population
5.1. Role of Exercise Training on ED in HFrEF
| Adrenergic System, Physical Exercise, and ED in HFrEF Patients |
| The sympathetic nervous system’s (SNS) over activity in heart failure is a well-established mechanism that has a transitional contribution to the pathophysiology, is supportive of cardiac function initially, and is a burden on it ultimately [52]. Research has revealed molecular alterations occurring in SNS in different models, myocardial cells, peripheral lymphocytes, and endothelial cells. Interpretation of these changes should take into consideration genetic polymorphism in human adrenergic receptors (ARs) and NOS enzymes, which adds to the complexity of the pathophysiological interactions of these phenomena in heart failure. |
| In the myocardium, the most abundant AR are βAR subtypes. Their density changes from a predominant β1AR (77%): β2AR (23%) in a non-failing heart to 60%: 38% with improper signaling mechanisms in a failing heart [53,54]. βAR desensitization has also been reported in the myocardium of heart failure patients [55,56], a property that has also been associated with receptor phosphorylation by adrenergic receptor kinase-2 [57]. Peripheral blood lymphocytes served as another model to study changes in βAR in heart failure patients. This is because they exist in high numbers in Tsuppressor/cytotoxic cells, B cells, natural killer cells, and monocytes [58]. These numbers have been found to correlate with βAR density in human myocardial cells [59]. In heart failure patients, the density of βAR on peripheral lymphocytes and isoproterenol-stimulated adenylate cyclase activity were reduced [60]. |
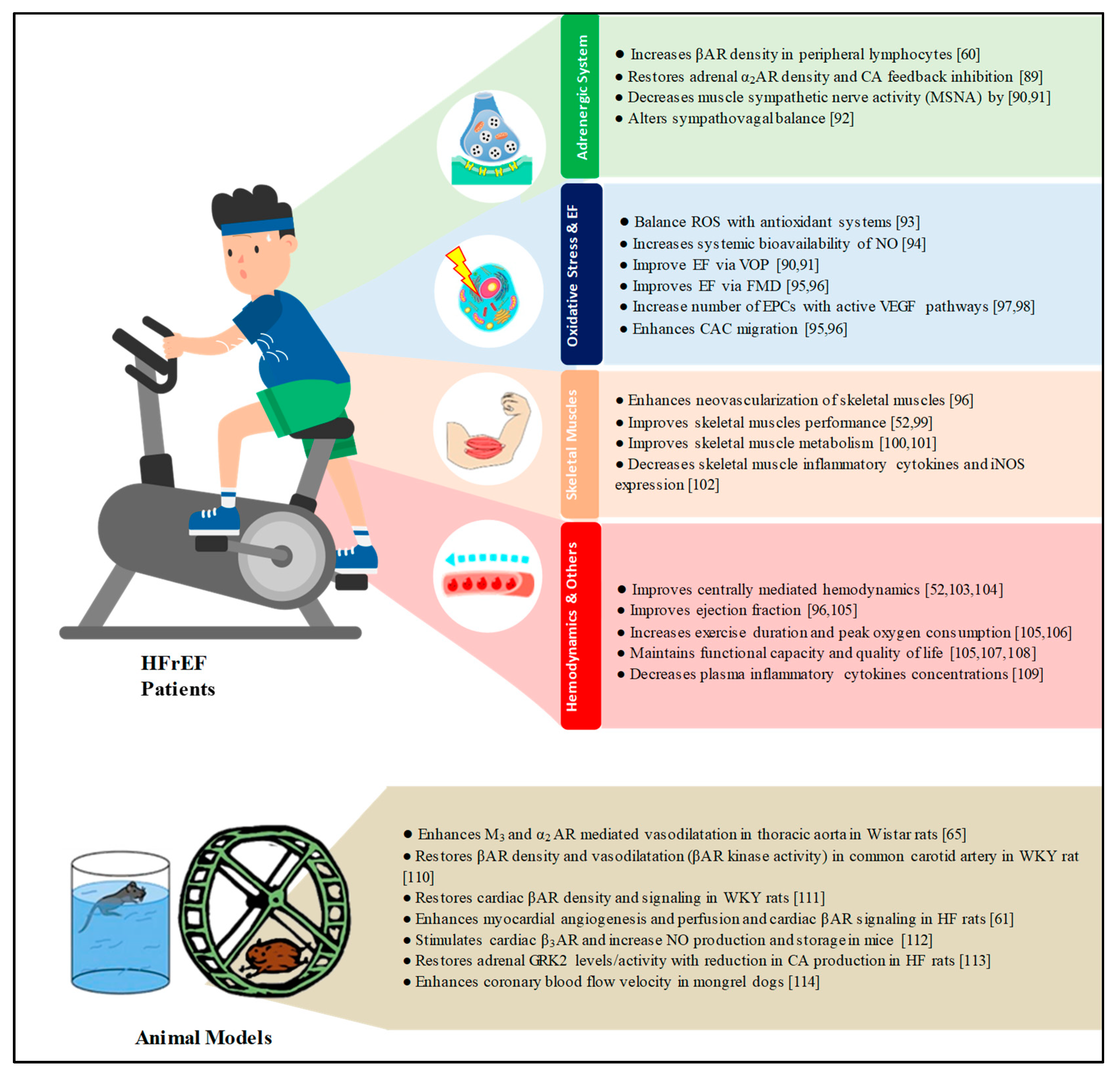
| The benefits of physical exercise in heart failure were studied on myocardial cells and peripheral lymphocytes. In animal models, physical exercise increased myocardial βAR density and reduced G-protein-coupled receptor kinase-2 over-expression, with the resultant improvement of cardiac inotropic activity in response to adrenergic stimulation [61]. In patients with heart failure, physical exercise has increased the density of βAR in peripheral lymphocytes [60]. The third studied model are endothelial cells (ECs), where all AR subtypes exist (with β2AR sub-type predominance) and directly or via NOS stimulation induce NO-dependent vasodilatation [62,63]. α2AR are also expressed and involved in the activation of NOS and NO-dependent vasodilatation [64]. |
| The benefits of physical exercise in heart failure were studied on myocardial cells and peripheral lymphocytes. In animal models, physical exercise increased myocardial βAR density and reduced G-protein-coupled receptor kinase-2 over-expression, with the resultant improvement of cardiac inotropic activity in response to adrenergic stimulation [61]. In patients with heart failure, physical exercise has increased the density of βAR in peripheral lymphocytes [60]. The third studied model are endothelial cells (ECs), where all AR subtypes exist (with β2AR sub-type predominance) and directly or via NOS stimulation induce NO-dependent vasodilatation [62,63]. α2AR are also expressed and involved in the activation of NOS and NO-dependent vasodilatation [64]. |
| Considering the current findings, we could anticipate that physical exercise in heart failure might modify the molecular changes to the adrenergic system at the EC level and improve endothelial function, as it does enhance autonomic receptor-mediated endothelium-dependent vasodilatation in animal models [65]. Such a benefit might be in addition to its ability to recruit EPCs from the bone marrow to repair endothelial function. Therefore, future studies should establish which exercise regimens should be emphasized and to which heart failure patients. In addition, more research is needed to establish the effect of physical exercise on prognosis if continued or terminated. |
5.2. Role of Exercise Training on ED in HFpEF
5.3. Role of Pharmacological Agents on ED in HFrEF
5.4. Role of Pharmacological Agents on ED in HFpEF
6. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Endemann, D.H.; Schiffrin, E.L. Endothelial dysfunction. J. Am. Soc. Nephrol. 2004, 15, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.R.; Kuvin, J.T.; Pandian, N.G.; Smith, J.J.; Udelson, J.E.; Mendelsohn, M.E.; Konstam, M.A.; Karas, R.H. Heart failure etiology affects peripheral vascular endothelial function after cardiac transplantation. J. Am. Coll. Cardiol. 2001, 37, 195–200. [Google Scholar] [CrossRef]
- Kovacic, S.; Plazonic, Z.; Batinac, T.; Miletic, D.; Ruzic, A. Endothelial dysfunction as assessed with magnetic resonance imaging—A major determinant in chronic heart failure. Med. Hypotheses 2016, 90, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I.B.; Webb, D.J. Venous occlusion plethysmography in cardiovascular research: Methodology and clinical applications. Br. J. Clin. Pharmacol. 2001, 52, 631–646. [Google Scholar] [CrossRef] [PubMed]
- Raitakari, O.T.; Celermajer, D.S. Flow-mediated dilatation. Br. J. Clin. Pharmacol. 2000, 50, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Panza, J.A.; Quyyumi, A.A.; Brush, J.E., Jr.; Epstein, S.E. Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension. N. Engl. J. Med. 1990, 323, 22–27. [Google Scholar] [CrossRef]
- Dharmashankar, K.; Widlansky, M.E. Vascular endothelial function and hypertension: Insights and directions. Curr. Hypertens. Rep. 2010, 12, 448–455. [Google Scholar] [CrossRef]
- Avogaro, A.; Albiero, M.; Menegazzo, L.; de Kreutzenberg, S.; Fadini, G.P. Endothelial dysfunction in diabetes: the role of reparatory mechanisms. Diabetes Care 2011, 34, S285–S290. [Google Scholar] [CrossRef]
- Severino, P.; D’Amato, A.; Netti, L.; Pucci, M.; De, M.M.; Palmirotta, R.; Volterrani, M.; Mancone, M.; Fedele, F. Diabetes Mellitus and Ischemic Heart Disease: The Role of Ion Channels. Int. J. Mol. Sci. 2018, 19, 802. [Google Scholar] [CrossRef]
- Severino, P.; D’Amato, A.; Netti, L.; Pucci, M.; Infusino, F.; Maestrini, V.; Mancone, M.; Fedele, F. Myocardial Ischemia and Diabetes Mellitus: Role of Oxidative Stress in the Connection between Cardiac Metabolism and Coronary Blood Flow. J. Diabetes Res. 2019, 2019, 9489826. [Google Scholar] [CrossRef] [PubMed]
- Kubo, S.H.; Rector, T.S.; Bank, A.J.; Williams, R.E.; Heifetz, S.M. Endothelium-dependent vasodilation is attenuated in patients with heart failure. Circulation 1991, 84, 1589–1596. [Google Scholar] [CrossRef]
- Drexler, H.; Hayoz, D.; Munzel, T.; Hornig, B.; Just, H.; Brunner, H.R.; Zelis, R. Endothelial function in chronic congestive heart failure. Am. J. Cardiol. 1992, 69, 1596–1601. [Google Scholar] [CrossRef]
- Ramsey, M.W.; Goodfellow, J.; Jones, C.J.; Luddington, L.A.; Lewis, M.J.; Henderson, A.H. Endothelial control of arterial distensibility is impaired in chronic heart failure. Circulation 1995, 92, 3212–3219. [Google Scholar] [CrossRef]
- Landmesser, U.; Spiekermann, S.; Dikalov, S.; Tatge, H.; Wilke, R.; Kohler, C.; Harrison, D.G.; Hornig, B.; Drexler, H. Vascular oxidative stress and endothelial dysfunction in patients with chronic heart failure: role of xanthine-oxidase and extracellular superoxide dismutase. Circulation 2002, 106, 3073–3078. [Google Scholar] [CrossRef]
- Farrero, M.; Blanco, I.; Batlle, M.; Santiago, E.; Cardona, M.; Vidal, B.; Castel, M.A.; Sitges, M.; Barbera, J.A.; Perez-Villa, F. Pulmonary hypertension is related to peripheral endothelial dysfunction in heart failure with preserved ejection fraction. Circ. Heart Fail. 2014, 7, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Marechaux, S.; Samson, R.; van Belle, E.; Breyne, J.; de Monte, J.; Dedrie, C.; Chebai, N.; Menet, A.; Banfi, C.; Bouabdallaoui, N.; et al. Vascular and Microvascular Endothelial Function in Heart Failure With Preserved Ejection Fraction. J. Card Fail. 2016, 22, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.F.; Barrett-O’Keefe, Z.; Garten, R.S.; Nelson, A.D.; Ryan, J.J.; Nativi, J.N.; Richardson, R.S.; Wray, D.W. Evidence of microvascular dysfunction in heart failure with preserved ejection fraction. Heart 2016, 102, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, S.; Kajikawa, M.; Maruhashi, T.; Iwamoto, Y.; Matsumoto, T.; Iwamoto, A.; Oda, N.; Matsui, S.; Hidaka, T.; Kihara, Y.; et al. Endothelial dysfunction and abnormal vascular structure are simultaneously present in patients with heart failure with preserved ejection fraction. Int. J. Cardiol. 2017, 231, 181–187. [Google Scholar] [CrossRef]
- Katz, S.D.; Khan, T.; Zeballos, G.A.; Mathew, L.; Potharlanka, P.; Knecht, M.; Whelan, J. Decreased activity of the L-arginine-nitric oxide metabolic pathway in patients with congestive heart failure. Circulation 1999, 99, 2113–2117. [Google Scholar] [CrossRef]
- Fedele, F.; Mancone, M.; Chilian, W.M.; Severino, P.; Canali, E.; Logan, S.; De Marchis, M.L.; Volterrani, M.; Palmirotta, R.; Guadagni, F. Role of genetic polymorphisms of ion channels in the pathophysiology of coronary microvascular dysfunction and ischemic heart disease. Basic Res. Cardiol. 2013, 108, 387. [Google Scholar] [CrossRef] [PubMed]
- Lopez, F.A.; Casado, S. Heart failure, redox alterations, and endothelial dysfunction. Hypertension 2001, 38, 1400–1405. [Google Scholar]
- Usui, M.; Matsuoka, H.; Miyazaki, H.; Ueda, S.; Okuda, S.; Imaizumi, T. Increased endogenous nitric oxide synthase inhibitor in patients with congestive heart failure. Life Sci. 1998, 62, 2425–2430. [Google Scholar] [CrossRef]
- Tsutsui, T.; Tsutamoto, T.; Wada, A.; Maeda, K.; Mabuchi, N.; Hayashi, M.; Ohnishi, M.; Kinoshita, M. Plasma oxidized low-density lipoprotein as a prognostic predictor in patients with chronic congestive heart failure. J. Am. Coll. Cardiol. 2002, 39, 957–962. [Google Scholar] [CrossRef]
- Polidori, M.C.; Pratico, D.; Savino, K.; Rokach, J.; Stahl, W.; Mecocci, P. Increased F2 isoprostane plasma levels in patients with congestive heart failure are correlated with antioxidant status and disease severity. J. Card Fail. 2004, 10, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Santulli, G. MicroRNAs and Endothelial (Dys) Function. J. Cell Physiol. 2016, 231, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Wronska, A.; Kurkowska-Jastrzebska, I.; Santulli, G. Application of microRNAs in diagnosis and treatment of cardiovascular disease. Acta Physiol. 2015, 213, 60–83. [Google Scholar] [CrossRef]
- Yeboah, J.; Folsom, A.R.; Burke, G.L.; Johnson, C.; Polak, J.F.; Post, W.; Lima, J.A.; Crouse, J.R.; Herrington, D.M. Predictive value of brachial flow-mediated dilation for incident cardiovascular events in a population-based study: the multi-ethnic study of atherosclerosis. Circulation 2009, 120, 502–509. [Google Scholar] [CrossRef]
- Lind, L.; Berglund, L.; Larsson, A.; Sundstrom, J. Endothelial function in resistance and conduit arteries and 5-year risk of cardiovascular disease. Circulation 2011, 123, 1545–1551. [Google Scholar] [CrossRef]
- Shechter, M.; Issachar, A.; Marai, I.; Koren-Morag, N.; Freinark, D.; Shahar, Y.; Shechter, A.; Feinberg, M.S. Long-term association of brachial artery flow-mediated vasodilation and cardiovascular events in middle-aged subjects with no apparent heart disease. Int. J. Cardiol. 2009, 134, 52–58. [Google Scholar] [CrossRef]
- Fathi, R.; Haluska, B.; Isbel, N.; Short, L.; Marwick, T.H. The relative importance of vascular structure and function in predicting cardiovascular events. J. Am. Coll. Cardiol. 2004, 43, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Frick, M.; Suessenbacher, A.; Alber, H.F.; Dichtl, W.; Ulmer, H.; Pachinger, O.; Weidinger, F. Prognostic value of brachial artery endothelial function and wall thickness. J. Am. Coll. Cardiol. 2005, 46, 1006–1010. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Meyer, B.; Mortl, D.; Strecker, K.; Hulsmann, M.; Kulemann, V.; Neunteufl, T.; Pacher, R.; Berger, R. Flow-mediated vasodilation predicts outcome in patients with chronic heart failure: Comparison with B-type natriuretic peptide. J. Am. Coll. Cardiol. 2005, 46, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, T.; Baldus, S.; von Kodolitsch, Y.; Rudolph, V.; Meinertz, T. Systemic endothelial dysfunction as an early predictor of adverse outcome in heart failure. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1174–1179. [Google Scholar] [CrossRef] [PubMed]
- Fischer, D.; Rossa, S.; Landmesser, U.; Spiekermann, S.; Engberding, N.; Hornig, B.; Drexler, H. Endothelial dysfunction in patients with chronic heart failure is independently associated with increased incidence of hospitalization, cardiac transplantation, or death. Eur. Heart J. 2005, 26, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.D.; Hryniewicz, K.; Hriljac, I.; Balidemaj, K.; Dimayuga, C.; Hudaihed, A.; Yasskiy, A. Vascular endothelial dysfunction and mortality risk in patients with chronic heart failure. Circulation 2005, 111, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Shechter, M.; Matetzky, S.; Arad, M.; Feinberg, M.S.; Freimark, D. Vascular endothelial function predicts mortality risk in patients with advanced ischaemic chronic heart failure. Eur. J. Heart Fail. 2009, 11, 588–593. [Google Scholar] [CrossRef] [PubMed]
- De Berrazueta, J.R.; Guerra-Ruiz, A.; Garcia-Unzueta, M.T.; Toca, G.M.; Laso, R.S.; de Adana, M.S.; Martin, M.A.; Cobo, M.; Llorca, J. Endothelial dysfunction, measured by reactive hyperaemia using strain-gauge plethysmography, is an independent predictor of adverse outcome in heart failure. Eur. J. Heart Fail. 2010, 12, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Fujisue, K.; Sugiyama, S.; Matsuzawa, Y.; Akiyama, E.; Sugamura, K.; Matsubara, J.; Kurokawa, H.; Maeda, H.; Hirata, Y.; Kusaka, H.; et al. Prognostic Significance of Peripheral Microvascular Endothelial Dysfunction in Heart Failure with Reduced Left Ventricular Ejection Fraction. Circ. J. 2015, 79, 2623–2631. [Google Scholar] [CrossRef] [PubMed]
- Kubrich, M.; Petrakopoulou, P.; Kofler, S.; Nickel, T.; Kaczmarek, I.; Meiser, B.M.; Reichart, B.; von Scheidt, W.; Weis, M. Impact of coronary endothelial dysfunction on adverse long-term outcome after heart transplantation. Transplantation 2008, 85, 1580–1587. [Google Scholar] [CrossRef]
- Yufu, K.; Shinohara, T.; Ebata, Y.; Ayabe, R.; Fukui, A.; Okada, N.; Nakagawa, M.; Takahashi, N. Endothelial Function Predicts New Hospitalization due to Heart Failure Following Cardiac Resynchronization Therapy. Pacing Clin. Electrophysiol. 2015, 38, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Grontved, A.; Koivula, R.W.; Johansson, I.; Wennberg, P.; Ostergaard, L.; Hallmans, G.; Renstrom, F.; Franks, P.W. Bicycling to Work and Primordial Prevention of Cardiovascular Risk: A Cohort Study Among Swedish Men and Women. J. Am. Heart Assoc. 2016, 5, e004413. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Conraads, V.M.; Van Craenenbroeck, E.M.; De Maeyer, C.; Van Berendoncks, A.M.; Beckers, P.J.; Vrints, C.J. Unraveling new mechanisms of exercise intolerance in chronic heart failure: role of exercise training. Heart Fail. Rev. 2013, 18, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Pearson, M.J.; Smart, N.A. Effect of exercise training on endothelial function in heart failure patients: A systematic review meta-analysis. Int. J. Cardiol. 2017, 231, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Ennis, S.; McGregor, G.; Shave, R.; McDonnell, B.; Thompson, A.; Banerjee, P.; Jones, H. Low frequency electrical muscle stimulation and endothelial function in advanced heart failure patients. ESC Heart Fail. 2018, 5, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Maiorana, A.; O’Driscoll, G.; Taylor, R. Effect of exercise training on endothelium-derived nitric oxide function in humans. J. Physiol 2004, 561, 1–25. [Google Scholar] [CrossRef]
- Hambrecht, R.; Adams, V.; Erbs, S.; Linke, A.; Krankel, N.; Shu, Y.; Baither, Y.; Gielen, S.; Thiele, H.; Gummert, J.F.; et al. Regular physical activity improves endothelial function in patients with coronary artery disease by increasing phosphorylation of endothelial nitric oxide synthase. Circulation 2003, 107, 3152–3158. [Google Scholar] [CrossRef]
- Linke, A.; Adams, V.; Schulze, P.C.; Erbs, S.; Gielen, S.; Fiehn, E.; Mobius-Winkler, S.; Schubert, A.; Schuler, G.; Hambrecht, R. Antioxidative effects of exercise training in patients with chronic heart failure: Increase in radical scavenger enzyme activity in skeletal muscle. Circulation 2005, 111, 1763–1770. [Google Scholar] [CrossRef]
- Volaklis, K.A.; Tokmakidis, S.P.; Halle, M. Acute and chronic effects of exercise on circulating endothelial progenitor cells in healthy and diseased patients. Clin. Res. Cardiol. 2013, 102, 249–257. [Google Scholar] [CrossRef]
- Recchioni, R.; Marcheselli, F.; Antonicelli, R.; Lazzarini, R.; Mensa, E.; Testa, R.; Procopio, A.D.; Olivieri, F. Physical activity and progenitor cell-mediated endothelial repair in chronic heart failure: Is there a role for epigenetics? Mech. Ageing Dev. 2016, 159, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Lymperopoulos, A.; Rengo, G.; Koch, W.J. Adrenergic nervous system in heart failure: Pathophysiology and therapy. Circ. Res. 2013, 113, 739–753. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R.; Ginsburg, R.; Minobe, W.; Cubicciotti, R.S.; Sageman, W.S.; Lurie, K.; Billingham, M.E.; Harrison, D.C.; Stinson, E.B. Decreased catecholamine sensitivity and beta-adrenergic-receptor density in failing human hearts. N. Engl. J. Med. 1982, 307, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R.; Ginsburg, R.; Umans, V.; Fowler, M.; Minobe, W.; Rasmussen, R.; Zera, P.; Menlove, R.; Shah, P.; Jamieson, S. Beta 1- and beta 2-adrenergic-receptor subpopulations in nonfailing and failing human ventricular myocardium: Coupling of both receptor subtypes to muscle contraction and selective beta 1-receptor down-regulation in heart failure. Circ. Res. 1986, 59, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Ungerer, M.; Parruti, G.; Bohm, M.; Puzicha, M.; DeBlasi, A.; Erdmann, E.; Lohse, M.J. Expression of beta-arrestins and beta-adrenergic receptor kinases in the failing human heart. Circ. Res. 1994, 74, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.J.; Rockman, H.A. Beta-adrenergic receptor desensitization in cardiac hypertrophy and heart failure. Cell Biochem. Biophys. 1999, 31, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Rengo, G.; Perrone-Filardi, P.; Femminella, G.D.; Liccardo, D.; Zincarelli, C.; De Lucia, C.; Pagano, G.; Marsico, F.; Lymperopoulos, A.; Leosco, D. Targeting the beta-adrenergic receptor system through G-protein-coupled receptor kinase 2: a new paradigm for therapy and prognostic evaluation in heart failure: from bench to bedside. Circ. Heart Fail. 2012, 5, 385–391. [Google Scholar] [CrossRef]
- Maisel, A.S.; Harris, T.; Rearden, C.A.; Michel, M.C. Beta-adrenergic receptors in lymphocyte subsets after exercise. Alterations in normal individuals and patients with congestive heart failure. Circulation 1990, 82, 2003–2010. [Google Scholar] [CrossRef]
- Brodde, O.E.; Kretsch, R.; Ikezono, K.; Zerkowski, H.R.; Reidemeister, J.C. Human beta-adrenoceptors: relation of myocardial and lymphocyte beta-adrenoceptor density. Science 1986, 231, 1584–1585. [Google Scholar] [CrossRef]
- Mancini, D.M.; Frey, M.J.; Fischberg, D.; Molinoff, P.B.; Wilson, J.R. Characterization of lymphocyte beta-adrenergic receptors at rest and during exercise in ambulatory patients with chronic congestive heart failure. Am. J. Cardiol. 1989, 63, 307–312. [Google Scholar] [CrossRef]
- Leosco, D.; Rengo, G.; Iaccarino, G.; Golino, L.; Marchese, M.; Fortunato, F.; Zincarelli, C.; Sanzari, E.; Ciccarelli, M.; Galasso, G.; et al. Exercise promotes angiogenesis and improves beta-adrenergic receptor signalling in the post-ischaemic failing rat heart. Cardiovasc. Res. 2008, 78, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, S.; Moura, D. Vascular adrenoceptors: An update. Pharmacol. Rev. 2001, 53, 319–356. [Google Scholar] [PubMed]
- Iaccarino, G.; Cipolletta, E.; Fiorillo, A.; Annecchiarico, M.; Ciccarelli, M.; Cimini, V.; Koch, W.J.; Trimarco, B. Beta(2)-adrenergic receptor gene delivery to the endothelium corrects impaired adrenergic vasorelaxation in hypertension. Circulation 2002, 106, 349–355. [Google Scholar] [CrossRef]
- Lembo, G.; Iaccarino, G.; Vecchione, C.; Barbato, E.; Morisco, C.; Monti, F.; Parrella, L.; Trimarco, B. Insulin enhances endothelial alpha2-adrenergic vasorelaxation by a pertussis toxin mechanism. Hypertension 1997, 30, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Yang, C.; Hsu, L.; Lin, M.T.; Jen, C.J.; Chen, H. Acute exercise enhances receptor-mediated endothelium-dependent vasodilation by receptor upregulation. J. Biomed. Sci. 1999, 6, 22–27. [Google Scholar] [CrossRef]
- Karavidas, A.; Driva, M.; Parissis, J.T.; Farmakis, D.; Mantzaraki, V.; Varounis, C.; Paraskevaidis, I.; Ikonomidis, I.; Pirgakis, V.; Anastasiou-Nana, M.; et al. Functional electrical stimulation of peripheral muscles improves endothelial function and clinical and emotional status in heart failure patients with preserved left ventricular ejection fraction. Am. Heart J. 2013, 166, 760–767. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.H.; Herrington, D.M.; Morgan, T.M.; Stewart, K.P.; Hundley, W.G.; Abdelhamed, A.; Haykowsky, M.J. Effect of endurance exercise training on endothelial function and arterial stiffness in older patients with heart failure and preserved ejection fraction: A randomized, controlled, single-blind trial. J. Am. Coll. Cardiol. 2013, 62, 584–592. [Google Scholar] [CrossRef]
- Shahin, Y.; Khan, J.A.; Samuel, N.; Chetter, I. Angiotensin converting enzyme inhibitors effect on endothelial dysfunction: a meta-analysis of randomised controlled trials. Atherosclerosis 2011, 216, 7–16. [Google Scholar] [CrossRef]
- Koh, K.K.; Quon, M.J.; Lee, Y.; Han, S.H.; Ahn, J.Y.; Chung, W.J.; Kim, J.A.; Shin, E.K. Additive beneficial cardiovascular and metabolic effects of combination therapy with ramipril and candesartan in hypertensive patients. Eur. Heart J. 2007, 28, 1440–1447. [Google Scholar] [CrossRef]
- Souza-Barbosa, L.A.; Ferreira-Melo, S.L.E.; Ubaid-Girioli, S.; Nogueira, E.A.; Yugar-Toledo, J.C.; Moreno, H., Jr. Endothelial Vascular Function in Hypertensive Patients After Renin-Angiotensin System Blockad. J. Clin. Hypertens. 2006, 8, 803–811. [Google Scholar] [CrossRef]
- Farquharson, C.A.; Struthers, A.D. Spironolactone increases nitric oxide bioactivity, improves endothelial vasodilator dysfunction, and suppresses vascular angiotensin I/angiotensin II conversion in patients with chronic heart failure. Circulation 2000, 101, 594–597. [Google Scholar] [CrossRef] [PubMed]
- Abiose, A.K.; Mansoor, G.A.; Barry, M.; Soucier, R.; Nair, C.K.; Hager, D. Effect of spironolactone on endothelial function in patients with congestive heart failure on conventional medical therapy. Am. J. Cardiol. 2004, 93, 1564–1566. [Google Scholar] [CrossRef] [PubMed]
- Erbs, S.; Beck, E.B.; Linke, A.; Adams, V.; Gielen, S.; Krankel, N.; Mobius-Winkler, S.; Hollriegel, R.; Thiele, H.; Hambrecht, R.; et al. High-dose rosuvastatin in chronic heart failure promotes vasculogenesis, corrects endothelial function, and improves cardiac remodeling—Results from a randomized, double-blind, and placebo-controlled study. Int. J. Cardiol. 2011, 146, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Andreou, I.; Tsiatas, M.; Miliou, A.; Tentolouris, C.; Siasos, G.; Papageorgiou, N.; Papadimitriou, C.A.; Dimopoulos, M.A.; Stefanadis, C. Effects of rosuvastatin and allopurinol on circulating endothelial progenitor cells in patients with congestive heart failure: the impact of inflammatory process and oxidative stress. Atherosclerosis 2011, 214, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.; Siasos, G.; Zaromitidou, M.; Hatzis, G.; Mourouzis, K.; Chrysohoou, C.; Zisimos, K.; Mazaris, S.; Tourikis, P.; Athanasiou, D.; et al. Atorvastatin treatment improves endothelial function through endothelial progenitor cells mobilization in ischemic heart failure patients. Atherosclerosis 2015, 238, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Castro, P.F.; Miranda, R.; Verdejo, H.E.; Greig, D.; Gabrielli, L.A.; Alcaino, H.; Chiong, M.; Bustos, C.; Garcia, L.; Mellado, R.; et al. Pleiotropic effects of atorvastatin in heart failure: role in oxidative stress, inflammation, endothelial function, and exercise capacity. J. Heart Lung Transplant. 2008, 27, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Houston, M.; Estevez, A.; Chumley, P.; Aslan, M.; Marklund, S.; Parks, D.A.; Freeman, B.A. Binding of xanthine oxidase to vascular endothelium. Kinetic characterization and oxidative impairment of nitric oxide-dependent signaling. J. Biol. Chem. 1999, 274, 4985–4994. [Google Scholar] [CrossRef]
- Kato, M.; Hisatome, I.; Tomikura, Y.; Kotani, K.; Kinugawa, T.; Ogino, K.; Ishida, K.; Igawa, O.; Shigemasa, C.; Somers, V.K. Status of endothelial dependent vasodilation in patients with hyperuricemia. Am. J. Cardiol. 2005, 96, 1576–1578. [Google Scholar] [CrossRef]
- Alem, M.M. Allopurinol and endothelial function: A systematic review with meta-analysis of randomized controlled trials. Cardiovasc. Ther. 2018, 36, e12432. [Google Scholar] [CrossRef]
- Grossini, E.; Molinari, C.; Caimmi, P.P.; Uberti, F.; Vacca, G. Levosimendan induces NO production through p38 MAPK, ERK and Akt in porcine coronary endothelial cells: role for mitochondrial K(ATP) channel. Br. J. Pharmacol. 2009, 156, 250–261. [Google Scholar] [CrossRef]
- Parissis, J.T.; Karavidas, A.; Bistola, V.; Arapi, S.; Paraskevaidis, I.A.; Farmakis, D.; Korres, D.; Filippatos, G.; Matsakas, E.; Kremastinos, D.T. Effects of levosimendan on flow-mediated vasodilation and soluble adhesion molecules in patients with advanced chronic heart failure. Atherosclerosis 2008, 197, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Swedberg, K.; Komajda, M.; Bohm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. Ivabradine and outcomes in chronic heart failure (SHIFT): A randomised placebo-controlled study. Lancet 2010, 376, 875–885. [Google Scholar] [CrossRef]
- Bonadei, I.; Sciatti, E.; Vizzardi, E.; Fabbricatore, D.; Pagnoni, M.; Rossi, L.; Carubelli, V.; Lombardi, C.M.; Metra, M. Effects of ivabradine on endothelial function, aortic properties and ventricular-arterial coupling in chronic systolic heart failure patients. Cardiovasc. Ther. 2018, 36, e12323. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Lewis, G.D.; McNulty, S.E.; Semigran, M.J.; LeWinter, M.; Chen, H.; Lin, G.; Deswal, A.; Margulies, K.B.; Redfield, M.M. Effects of sildenafil on ventricular and vascular function in heart failure with preserved ejection fraction. Circ. Heart Fail. 2015, 8, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Schwarzl, M.; Hamdani, N.; Seiler, S.; Alogna, A.; Manninger, M.; Reilly, S.; Zirngast, B.; Kirsch, A.; Steendijk, P.; Verderber, J.; et al. A porcine model of hypertensive cardiomyopathy: implications for heart failure with preserved ejection fraction. Am. J. Physiol. Heart Circ. Physiol. 2015, 309, H1407–H1418. [Google Scholar] [CrossRef] [PubMed]
- Fedele, F.; Severino, P.; Calcagno, S.; Mancone, M. Heart failure: TNM-like classification. J. Am. Coll. Cardiol. 2014, 63, 1959–1960. [Google Scholar] [CrossRef]
- Kato, M.; Masuda, T.; Ogano, M.; Hotta, K.; Takagi, H.; Tanaka, S.; Kamada, Y.; Akiyama, A.; Kamekawa, D.; Shimizu, R.; et al. Stretching Exercises Improve Vascular Endothelial Dysfunction Through Attenuation of Oxidative Stress in Chronic Heart Failure Patients With an Implantable Cardioverter Defibrillator. J. Cardiopulm. Rehabil. Prev. 2017, 37, 130–138. [Google Scholar] [CrossRef]
- Tanaka, S.; Sanuki, Y.; Ozumi, K.; Harada, T.; Tasaki, H. Heart failure with preserved vs. reduced ejection fraction following cardiac rehabilitation: impact of endothelial function. Heart Vessels 2018, 33, 886–892. [Google Scholar] [CrossRef]
- Leosco, D.; Parisi, V.; Femminella, G.D.; Formisano, R.; Petraglia, L.; Allocca, E.; Bonaduce, D. Effects of exercise training on cardiovascular adrenergic system. Front. Physiol. 2013, 4, 348. [Google Scholar] [CrossRef]
- Fraga, R.; Franco, F.G.; Roveda, F.; de Matos, L.N.; Braga, A.M.; Rondon, M.U.; Rotta, D.R.; Brum, P.C.; Barretto, A.C.; Middlekauff, H.R.; et al. Exercise training reduces sympathetic nerve activity in heart failure patients treated with carvedilol. Eur. J. Heart Fail. 2007, 9, 630–636. [Google Scholar] [CrossRef]
- Roveda, F.; Middlekauff, H.R.; Rondon, M.U.; Reis, S.F.; Souza, M.; Nastari, L.; Barretto, A.C.; Krieger, E.M.; Negrao, C.E. The effects of exercise training on sympathetic neural activation in advanced heart failure: A randomized controlled trial. J. Am. Coll. Cardiol. 2003, 42, 854–860. [Google Scholar] [CrossRef]
- Coats, A.J.; Adamopoulos, S.; Radaelli, A.; McCance, A.; Meyer, T.E.; Bernardi, L.; Solda, P.L.; Davey, P.; Ormerod, O.; Forfar, C. Controlled trial of physical training in chronic heart failure. Exercise performance, hemodynamics, ventilation, and autonomic function. Circulation 1992, 85, 2119–2131. [Google Scholar] [CrossRef] [PubMed]
- Conti, V.; Russomanno, G.; Corbi, G.; Izzo, V.; Vecchione, C.; Filippelli, A. Adrenoreceptors and nitric oxide in the cardiovascular system. Front. Physiol. 2013, 4, 321. [Google Scholar] [CrossRef] [PubMed]
- Laurent, M.; Daline, T.; Malika, B.; Fawzi, O.; Philippe, V.; Benoit, D.; Catherine, M.; Jacques, R. Training-induced increase in nitric oxide metabolites in chronic heart failure and coronary artery disease: An extra benefit of water-based exercises? Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 215–221. [Google Scholar] [PubMed]
- Van Craenenbroeck, E.M.; Hoymans, V.Y.; Beckers, P.J.; Possemiers, N.M.; Wuyts, K.; Paelinck, B.P.; Vrints, C.J.; Conraads, V.M. Exercise training improves function of circulating angiogenic cells in patients with chronic heart failure. Basic Res. Cardiol. 2010, 105, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Erbs, S.; Hollriegel, R.; Linke, A.; Beck, E.B.; Adams, V.; Gielen, S.; Mobius-Winkler, S.; Sandri, M.; Krankel, N.; Hambrecht, R.; et al. Exercise training in patients with advanced chronic heart failure (NYHA IIIb) promotes restoration of peripheral vasomotor function, induction of endogenous regeneration, and improvement of left ventricular function. Circ. Heart Fail. 2010, 3, 486–494. [Google Scholar] [CrossRef]
- Sarto, P.; Balducci, E.; Balconi, G.; Fiordaliso, F.; Merlo, L.; Tuzzato, G.; Pappagallo, G.L.; Frigato, N.; Zanocco, A.; Forestieri, C.; et al. Effects of exercise training on endothelial progenitor cells in patients with chronic heart failure. J. Card. Fail. 2007, 13, 701–708. [Google Scholar] [CrossRef]
- Mezzani, A.; Grassi, B.; Jones, A.M.; Giordano, A.; Corra, U.; Porcelli, S.; Della, B.S.; Taddeo, A.; Giannuzzi, P. Speeding of pulmonary VO2 on-kinetics by light-to-moderate-intensity aerobic exercise training in chronic heart failure: clinical and pathophysiological correlates. Int. J. Cardiol. 2013, 167, 2189–2195. [Google Scholar] [CrossRef]
- Adams, V.; Doring, C.; Schuler, G. Impact of physical exercise on alterations in the skeletal muscle in patients with chronic heart failure. Front. Biosci. 2008, 13, 302–311. [Google Scholar] [CrossRef][Green Version]
- Adamopoulos, S.; Coats, A.J.; Brunotte, F.; Arnolda, L.; Meyer, T.; Thompson, C.H.; Dunn, J.F.; Stratton, J.; Kemp, G.J.; Radda, G.K. Physical training improves skeletal muscle metabolism in patients with chronic heart failure. J. Am. Coll. Cardiol. 1993, 21, 1101–1106. [Google Scholar] [CrossRef]
- Hambrecht, R.; Niebauer, J.; Fiehn, E.; Kalberer, B.; Offner, B.; Hauer, K.; Riede, U.; Schlierf, G.; Kubler, W.; Schuler, G. Physical training in patients with stable chronic heart failure: Effects on cardiorespiratory fitness and ultrastructural abnormalities of leg muscles. J. Am. Coll. Cardiol. 1995, 25, 1239–1249. [Google Scholar] [CrossRef]
- Gielen, S.; Adams, V.; Mobius-Winkler, S.; Linke, A.; Erbs, S.; Yu, J.; Kempf, W.; Schubert, A.; Schuler, G.; Hambrecht, R. Anti-inflammatory effects of exercise training in the skeletal muscle of patients with chronic heart failure. J. Am. Coll. Cardiol. 2003, 42, 861–868. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Higginbotham, M.B.; Cobb, F.R. Exercise training in patients with severe left ventricular dysfunction. Hemodynamic and metabolic effects. Circulation 1988, 78, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Adamopoulos, S.; Ponikowski, P.; Cerquetani, E.; Piepoli, M.; Rosano, G.; Sleight, P.; Coats, A.J. Circadian pattern of heart rate variability in chronic heart failure patients. Effects of physical training. Eur. Heart J. 1995, 16, 1380–1386. [Google Scholar] [CrossRef] [PubMed]
- Hambrecht, R.; Gielen, S.; Linke, A.; Fiehn, E.; Yu, J.; Walther, C.; Schoene, N.; Schuler, G. Effects of exercise training on left ventricular function and peripheral resistance in patients with chronic heart failure: A randomized trial. JAMA 2000, 283, 3095–3101. [Google Scholar] [CrossRef] [PubMed]
- Coats, A.J.; Adamopoulos, S.; Meyer, T.E.; Conway, J.; Sleight, P. Effects of physical training in chronic heart failure. Lancet 1990, 335, 63–66. [Google Scholar] [CrossRef]
- Belardinelli, R.; Georgiou, D.; Cianci, G.; Purcaro, A. 10-year exercise training in chronic heart failure: A randomized controlled trial. J. Am. Coll. Cardiol. 2012, 60, 1521–1528. [Google Scholar] [CrossRef]
- Flynn, K.E.; Pina, I.L.; Whellan, D.J.; Lin, L.; Blumenthal, J.A.; Ellis, S.J.; Fine, L.J.; Howlett, J.G.; Keteyian, S.J.; Kitzman, D.W.; et al. Effects of exercise training on health status in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA 2009, 301, 1451–1459. [Google Scholar] [CrossRef]
- Adamopoulos, S.; Parissis, J.; Karatzas, D.; Kroupis, C.; Georgiadis, M.; Karavolias, G.; Paraskevaidis, J.; Koniavitou, K.; Coats, A.J.; Kremastinos, D.T. Physical training modulates proinflammatory cytokines and the soluble Fas/soluble Fas ligand system in patients with chronic heart failure. J. Am. Coll. Cardiol. 2002, 39, 653–663. [Google Scholar] [CrossRef]
- Leosco, D.; Iaccarino, G.; Cipolletta, E.; De Santis, D.; Pisani, E.; Trimarco, V.; Ferrara, N.; Abete, P.; Sorriento, D.; Rengo, F.; et al. Exercise restores beta-adrenergic vasorelaxation in aged rat carotid arteries. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H369–H374. [Google Scholar] [CrossRef]
- Leosco, D.; Rengo, G.; Iaccarino, G.; Filippelli, A.; Lymperopoulos, A.; Zincarelli, C.; Fortunato, F.; Golino, L.; Marchese, M.; Esposito, G.; et al. Exercise training and beta-blocker treatment ameliorate age-dependent impairment of beta-adrenergic receptor signaling and enhance cardiac responsiveness to adrenergic stimulation. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H1596–H1603. [Google Scholar] [CrossRef] [PubMed]
- Calvert, J.W.; Condit, M.E.; Aragon, J.P.; Nicholson, C.K.; Moody, B.F.; Hood, R.L.; Sindler, A.L.; Gundewar, S.; Seals, D.R.; Barouch, L.A.; et al. Exercise protects against myocardial ischemia-reperfusion injury via stimulation of beta(3)-adrenergic receptors and increased nitric oxide signaling: role of nitrite and nitrosothiols. Circ. Res. 2011, 108, 1448–1458. [Google Scholar] [CrossRef] [PubMed]
- Rengo, G.; Leosco, D.; Zincarelli, C.; Marchese, M.; Corbi, G.; Liccardo, D.; Filippelli, A.; Ferrara, N.; Lisanti, M.P.; Koch, W.J.; et al. Adrenal GRK2 lowering is an underlying mechanism for the beneficial sympathetic effects of exercise training in heart failure. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H2032–H2038. [Google Scholar] [CrossRef] [PubMed]
- DiCarlo, S.E.; Blair, R.W.; Bishop, V.S.; Stone, H.L. Role of beta 2-adrenergic receptors on coronary resistance during exercise. J. Appl. Physiol. 1988, 64, 2287–2293. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Sample Size and Population | Methodology | Findings |
|---|---|---|---|
| Farrero et al. 2014 [16] | 28 HFpEF | Brachial artery FMD | Patients 1.95 (−0.81–4.92)% (median, IQR) Controls 5.02 (3.90–10.12)% p = 0.002 |
| 42 Hypertensive control subjects | |||
| Maréchaux et al. 2016 [17] | 45 HFpEF | Brachial artery FMD | Patients 3.6 (0.4–7.4)% (median, IQR) Controls 7.2 (3.2–17.2)% p = 0.001 |
| 45 Hypertensive control subjects | Laser Doppler Flowmetry to assess forearm cutaneous peak blood flow | Patients 135 (104–206) PU Controls 177 (139–216) PU p = 0.03 | |
| Lee et al. 2016 [18] | 24 HFpEF | Brachial artery FMD | Patients 3.06 ± 0.68% (mean ± SEM) Controls 5.06 ± 0.53% p = 0.03, with no difference when corrected to shear rate |
| 24 healthy controls | Microvascular function via reactive hyperemia (RH) | Patients 454 ± 35 mL/min (mean AUC ± SEM) Controls 659 ± 63 mL/min p = 0.03 | |
| Kishimoto et al. 2017 [19] | 41 HFpEF | Brachial artery FMD | Patients 2.9 ± 2.1% (mean ± SD) Controls 4.6 ± 2.7% p = 0.0002 |
| 165 control subjects with cardiovascular risk factors | Brachial artery IMT | Patients 0.35 ± 0.06 mm Controls 0.31 ± 0.07 mm p = 0.0002 |
| Study | Sample Size and Population | Methodology | Follow-up | Outcome | Findings |
|---|---|---|---|---|---|
| Meyer et al. 2005 [33] | 75 CHF with systolic dysfunction NYHA class I–IV Ischemic and non-ischemic etiology | BA-FMD Response to reactive hyperemia | 3 years | Conversion to United Network of Organ Sharing UNOS status 1 (chronic inotropic support or implantation of ventricular assist device) or death | 27 UNOS-1/death 48 survivors |
| 2 control groups (19 healthy and young subjects, and 14 age- and gender- matched control subjects) | Multivariate stepwise analysis showed that FMD (Chi-square = 11.5, p = 0.0007), log BNP (Chi-square = 8.7, p = 0.003), and mean BP (Chi-square = 3.9, p = 0.047) were independent predictors of the combined endpoint | ||||
| Heitzer et al. 2005 [34] | 287 CHF with mild systolic dysfunction NYHA class I Ischemic and non-ischemic etiology | VOP Response to Ach and SNP | 4.8 years | Death, heart transplant, readmission due to worsening HF | 79 patients had events 208 patients without |
| Cox-proportional hazards model showed that age (HR = 1.07, 95%CI; 1.03–1.11, p = 0.001), renal function (HR = 0.97, 95%CI; 0.94–1.02, p = 0.001), and blunted Ach-induced vasodilatation (HR = 0.96, 95%CI; 0.94–0.98, p = 0.007) were independent predictors of the outcome | |||||
| Fischer et al. 2005 [35] | 67 CHF (30 had systolic dysfunction) NYHA class II–III Ischemic and non-ischemic etiology | FDD Radial artery | 3.8 years | Cardiac death, hospitalization due to worsening HF, or heart transplant | 24 patients had events 43 patients without |
| Cox-regression analysis showed that FDD (HR = 0.665 ± SE 0.182, p < 0.01), DM (HR = 0.055 ± 0.946, p < 0.01), and EF (HR = 0.054 ± 0.894, p < 0.01) were independent predictors of the outcome | |||||
| Katz et al. 2005 [36] | 259 CHF with systolic dysfunction NYHA class II–III Ischemic and non-ischemic etiology | BA-FMD Response to reactive hyperemia in 149 patients | 2.3 years | Death, and urgent transplantation | 17 patients had events 132 patients without |
| Exhaled NO production during submaximal exercise (pulmonary circulation) in 110 patients | 1 year | 19 patients had events 91 patients without Cox- multivariate proportional- hazards model showed that FMD (HR for 1% decrease in FMD = 1.20; 95%CI; 1.03–1.45; p = 0.027), and exhaled NO (HR for 1-ppb/min decrease = 1.31, 95%CI; 1.01–1.69, p = 0.04) were independent predictors of the outcome | |||
| Shechter et al. 2009 [37] | 82 CHF with systolic dysfunction NYHA class IV (advanced) Ischemic etiology | BA-FMD Response to reactive hyperemia | 1.2 years | Death, hospitalization for CHF exacerbation, or MI | 30 patients had events 52 patients without |
| Cox-proportional hazard model showed that FMD (HR for 1% decrease = 1.20; 95%CI; 1.01–1.69; p < 0.03) was an independent predictor of mortality | |||||
| de Berrazueta et al. 2010 [38] | 242 CHF with systolic dysfunction NYHA class I–IV Ischemic and non-ischemic etiology | VOP Response to reactive hyperemia | 5 years | Total events (death, heart attack, angina, stroke, NYHA class IV, or hospitalization for worsening HF) | 737 total events 62 patients died 180 patients survived |
| Cox-regression hazard model showed that FBF post-hyperemia (HR = 0.665 ± SE 0.182, p = 0.01) was an independent predictor of total events | |||||
| Fujisue et al. 2015 [39] | 362 HFrEF NYHA class I–III Ischemic and non-ischemic etiology | RH-PAT Reactive Hyperemia-Peripheral Arterial Tonometry (peripheral microvascular EF; distal finger) | 3 years | HF-related events (composite of cardiovascular death and HF hospitalization) | 82 patients had events 280 patients without |
| Cox-regression hazard model showed that Ln-RH-PAT (per 0.1, HR = 0.84, 95%CI; 0.75–0.95, p = 0.005); Serum sodium (per meq/L, HR = 0.92, 95%CI; 0.87–0.98, p = 0.004); and Ln-BNP (per 1.0, HR = 1.38, 95%CI; 1.12–1.70, p = 0.002) were independent predictors of HF-related events |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alem, M.M. Endothelial Dysfunction in Chronic Heart Failure: Assessment, Findings, Significance, and Potential Therapeutic Targets. Int. J. Mol. Sci. 2019, 20, 3198. https://doi.org/10.3390/ijms20133198
Alem MM. Endothelial Dysfunction in Chronic Heart Failure: Assessment, Findings, Significance, and Potential Therapeutic Targets. International Journal of Molecular Sciences. 2019; 20(13):3198. https://doi.org/10.3390/ijms20133198
Chicago/Turabian StyleAlem, Manal M. 2019. "Endothelial Dysfunction in Chronic Heart Failure: Assessment, Findings, Significance, and Potential Therapeutic Targets" International Journal of Molecular Sciences 20, no. 13: 3198. https://doi.org/10.3390/ijms20133198
APA StyleAlem, M. M. (2019). Endothelial Dysfunction in Chronic Heart Failure: Assessment, Findings, Significance, and Potential Therapeutic Targets. International Journal of Molecular Sciences, 20(13), 3198. https://doi.org/10.3390/ijms20133198