Effect of Peritoneal Dialysis on Serum Fibrosis Biomarkers in Patients with Refractory Congestive Heart Failure

Abstract

1. Introduction
2. Results
2.1. Clinical Characteristics
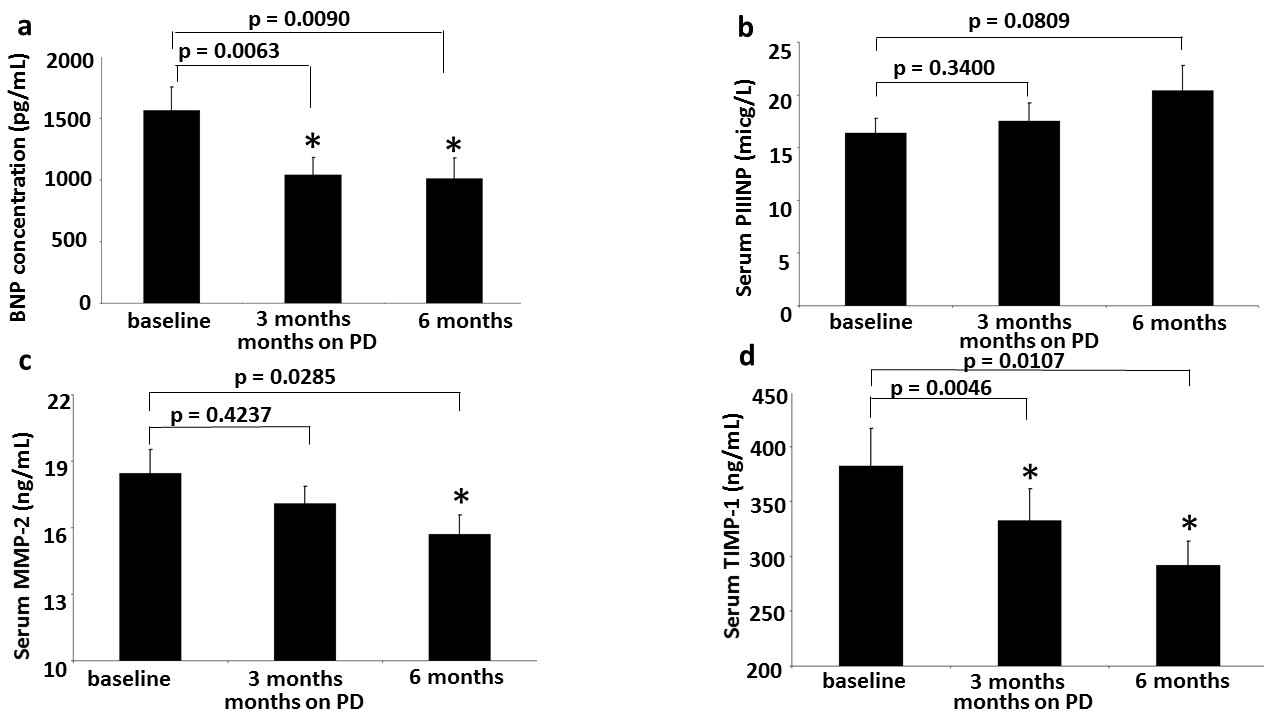
2.2. Circulating BNP Levels
2.3. Circulating PIIINP
2.4. Circulating MMP-2
2.5. Circulating TIMP-1 Levels
2.6. Decrease in All Three Fibrosis Markers Correlates with Survival
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Peritoneal Dialysis Description
4.3. Clinical Evaluation
4.4. BNP Assay
4.5. Matrix Metalloproteinases ELISA Assays
4.6. Procollagen-III-Peptide ELISA Assay
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lopez, B.; Gonzalez, A.; Diez, J. Circulating biomarkers of collagen metabolism in cardiac diseases. Circulation 2010, 121, 1645–1654. [Google Scholar] [CrossRef]
- Clark, I.M.; Swingler, T.E.; Sampieri, C.L.; Edwards, D.R. The regulation of matrix metalloproteinases and their inhibitors. Int. J. Biochem. Cell Biol. 2008, 40, 1362–1378. [Google Scholar] [CrossRef]
- Spinale, F.G. Matrix metalloproteinases: Regulation and dysregulation in the failing heart. Circ. Res. 2002, 90, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Polyakova, V.; Hein, S.; Kostin, S.; Ziegelhoeffer, T.; Schaper, J. Matrix metalloproteinases and their tissue inhibitors in pressure overloaded human myocardium during heart failure progression. J. Am. Coll. Cardiol. 2004, 44, 1609–1618. [Google Scholar]
- Song, Y.H.; Cai, H.; Gu, N.; Qian, C.F.; Cao, S.P.; Zhao, Z.M. Icariin attenuates cardiac remodelling through down-regulating myocardial apoptosis and matrix metalloproteinase activity in rats with congestive heart failure. J. Pharm. Pharmacol. 2011, 63, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Iraqi, W.; Rossignol, P.; Angioi, M.; Fay, R.; Nuée, J.; Ketelslegers, J.M.; Vincent, J.; Pitt, B.; Zannad, F. Extracellular cardiac matrix biomarkers in patients with acute myocardial infarction complicated by left ventricular dysfunction and heart failure: Insights from the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) study. Circulation 2009, 119, 2471–2479. [Google Scholar]
- Kaye, D.M.; Khammy, O.; Mariani, J.; Maeder, M.T. Relationship of circulating matrix biomarkers to myocardial matrix metabolism in advanced heart failure. Eur. J. Heart Fail. 2013, 15, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Klappacher, G.; Franzen, P.; Haab, D.; Mehrabi, M.; Binder, M.; Plesch, K.; Pacher, R.; Grimm, M.; Pribill, I.; Eichler, H.G.; et al. Measuring extracellular matrix turnover in the serum of patients with idiopathic or ischemic dilated cardiomyopathy and impact on diagnosis and prognosis. Am. J. Cardiol. 1995, 75, 913–918. [Google Scholar]
- Frantz, S.; Stork, S.; Michels, K.; Eigenthaler, M.; Ertl, G.; Bauersachs, J.; Angermann, C.E. Tissue inhibitor of metalloproteinases levels in patients with chronic heart failure: An independent predictor of mortality. Eur. J. Heart Fail. 2008, 10, 388–395. [Google Scholar] [CrossRef]
- George, J.; Patal, S.; Wexler, D.; Roth, A.; Sheps, D.; Keren, G. Circulating matrix metalloproteinase-2 but not matrix metalloproteinase-3, matrix metalloproteinase-9, or tissue inhibitor of metalloproteinase-1 predicts outcome in patients with congestive heart failure. Am. Heart J. 2005, 150, 484–487. [Google Scholar] [CrossRef]
- Zannad, F.; Alla, F.; Dousset, B.; Perez, A.; Pitt, B. Limitation of excessive extracellular matrix turnover may contribute to survival benefit of spironolactone therapy in patients with congestive heart failure: Insights from the randomized aldactone evaluation study (RALES). Circulation 2000, 102, 2700–2706. [Google Scholar] [CrossRef]
- Yamazaki, T.; Lee, J.D.; Shimizu, H.; Uzui, H.; Ueda, T. Circulating matrix metalloproteinase-2 is elevated in patients with congestive heart failure. Eur. J. Heart Fail. 2004, 6, 41–45. [Google Scholar] [CrossRef]
- Noji, Y.; Shimizu, M.; Ino, H.; Higashikata, T.; Yamaguchi, M.; Nohara, A.; Horita, T.; Shimizu, K.; Ito, Y.; Matsuda, T.; et al. Increased circulating matrix metalloproteinase-2 in patients with hypertrophic cardiomyopathy with systolic dysfunction. Circ. J. 2004, 68, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.H.; Clark, L.L.; Pennington, W.R.; Webb, C.S.; Bonnema, D.D.; Leonardi, A.H.; McClure, C.D.; Spinale, F.G.; Zile, M.R. Matrix metalloproteinases/tissue inhibitors of metalloproteinases: Relationship between changes in proteolytic determinants of matrix composition and structural, functional, and clinical manifestations of hypertensive heart disease. Circulation 2006, 113, 2089–2096. [Google Scholar] [CrossRef] [PubMed]
- Sundstro¨m, J.; Evans, J.C.; Benjamin, E.J.; Levy, D.; Larson, M.G.; Sawyer, D.B.; Siwik, D.A.; Colucci, W.S.; Wilson, P.W.; Vasan, R.S. Relations of plasma total TIMP-1 levels to cardiovascular risk factors and echocardiographic measures: The Framingham heart study. Eur. Heart J. 2004, 25, 1509–1516. [Google Scholar] [CrossRef]
- François, K.; Ronco, C.; Bargman, J.M. Peritoneal Dialysis for Chronic Congestive Heart Failure. Blood Purif. 2015, 40, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Kunin, M.; Carmon, V.; Arad, M.; Levin-Iaina, N.; Freimark, D.; Holtzman, E.J.; Dinour, D. Inflammatory Biomarkers in Refractory Congestive Heart Failure Patients Treated with Peritoneal Dialysis. Biomed. Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Cnossen, T.T.; Kooman, J.P.; Konings, C.J.A.M.; Uszko-Lencer, N.H.M.K.; Leunissen, K.M.L.; van der Sande, F.M. Peritoneal dialysis in patients with primary cardiac failure complicated by renal failure. Blood Purif. 2010, 30, 146–152. [Google Scholar] [CrossRef]
- Sanchez, J.E.; Ortega, T.; Rodriguez, C.; Diaz-Molina, B.; Martin, M.; Garcia-Cueto, C.; Vidau, P.; Gago, E.; Ortega, F. Efficacy of peritoneal ultrafiltration in the treatment of refractory congestive heart failure. Nephrol. Dial. Transplant. 2010, 25, 605–610. [Google Scholar] [CrossRef]
- Sotirakopoulos, N.G.; Kalogiannidou, I.M.; Tersi, M.E.; Mavromatidis, K.S. Peritoneal dialysis for patients suffering from severe heart failure. Clin. Nephrol. 2011, 76, 124–129. [Google Scholar] [CrossRef]
- Kunin, M.; Arad, M.; Dinour, D.; Freimark, D.; Holtzman, E.J. Peritoneal Dialysis in Patients with Refractory Congestive Heart Failure: Potential Prognostic Factors. Blood Purif. 2013, 35, 285–294. [Google Scholar] [CrossRef]
- Takawale, A.; Sakamuri, S.S.; Kassiri, Z. Extracellular matrix communication and turnover in cardiac physiology and pathology. Compr. Physiol. 2015, 5, 687–719. [Google Scholar]
- Quilliot, D.; Alla, F.; Bohme, P.; Bruntz, J.-F.; Hammadi, M.; Dousset, B.; Ziegler, O.; Zannad, F. Myocardial collagen turnover in normotensive obese patients: Relation to insulin resistance. Int. J. Obes. (Lond) 2005, 29, 1321–1328. [Google Scholar] [CrossRef]
- Hellawell, J.L.; Margulies, K.B. Myocardial reverse remodeling. Cardiovasc. Ther. 2012, 30, 172–181. [Google Scholar] [CrossRef]
- MacFadyen, R.J.; Barr, C.S.; Struthers, A.D. Aldosterone blockade reduces vascular collagen turnover, improves heart rate variability and reduces early morning rise in heart rate in heart failure patients. Cardiovasc. Res. 1997, 35, 30–34. [Google Scholar] [CrossRef]
- Zannad, F.; Dousset, B.; Alla, F. Treatment of Congestive Heart Failure Interfering the Aldosterone-Cardiac Extracellular Matrix Relationship. Hypertension 2001, 38, 1227–1232. [Google Scholar] [CrossRef][Green Version]
- Kramer, F.; Sandner, P.; Klein, M.; Krahn, T. Plasma concentrations of matrix metalloproteinase-2, tissue inhibitor of metalloproteinase-1 and osteopontin reflect severity of heart failure in DOCA-salt hypertensive rat. Biomarkers 2008, 13, 270–281. [Google Scholar] [CrossRef]
- Dries, D.L.; Sweitzer, N.K.; Drazner, M.H.; Stevenson, L.W.; Gersh, B.J. Prognostic impact of diabetes mellitus in patients with heart failure according to the etiology of left ventricular systolic dysfunction. J. Am. Coll. Cardiol. 2001, 38, 421. [Google Scholar] [CrossRef]
- Gustafsson, I.; Brendorp, B.; Seibaek, M.; Burchardt, H.; Hildebrandt, P.; Køber, L.; Torp-Pedersen, C. Influence of diabetes and diabetes-gender interaction on the risk of death in patients hospitalized with congestive heart failure. Am. Coll. Cardiol. 2004, 43, 771–777. [Google Scholar] [CrossRef]
- Jessup, M.; Brozena, S. Heart failure. N. Engl. J. Med. 2003, 348, 2007–2018. [Google Scholar] [CrossRef]
- Morine, K.J.; Paruchuri, V.; Qiao, X.; Mohammad, N.; Mcgraw, A.; Yunis, A.; Jaffe, I.; Kapur, N.K. Circulating multimarker profile of patients with symptomatic heart failure supports enhanced fibrotic degradation and decreased angiogenesis. Biomarkers 2016, 21, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Woessner, J.F., Jr. Matrix metalloproteinases and their inhibitors in connective tissue remodeling. FASEB J. 1991, 131, 2145–2154. [Google Scholar] [CrossRef]
- Denhardt, D.T.; Feng, B.; Edwards, D.R.; Cocuzzi, E.T.; Malyankar, U.M. Tissue inhibitor of metalloproteinases (TIMP aka EPA): Structure, control of expression and biological functions. Pharmacol. Ther. 1993, 59, 329–341. [Google Scholar] [CrossRef]
- Takawale, A.; Zhang, P.; Patel, V.B.; Wang, X.; Oudit, G.; Kassiri, Z. Tissue Inhibitor of Matrix Metalloproteinase-1 Promotes Myocardial Fibrosis by Mediating CD63–Integrin β1 Interaction. Hypertension 2017, 69, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Funck, R.C.; Wilke, A.; Rupp, H.; Brilla, C.G. Regulation and role of myocardial collagen matrix remodeling in hypertensive heart disease. Adv. Exp. Med. Biol. 1997, 432, 35–44. [Google Scholar]
- Chua, C.C.; Hamdy, R.C.; Cha, B.H. Angiotensin II induces TIMP-1 production in rat heart endothelial cells. Biochim. Biophys. Acta 1996, 1311, 175–180. [Google Scholar] [CrossRef][Green Version]
- Varo, N.; Iraburu, M.J.; Varela, M.; Lopez, B.; Etayo, J.C.; Diez, J. Chronic AT1 blockade stimulates extracellular collagen type I degradation and reverses myocardial fibrosis in spontaneously hypertensive rats. Hypertension 2000, 35, 1197–11202. [Google Scholar] [CrossRef] [PubMed]
- Murtha, L.A.; Schullga, M.J.; Mabotuwana, N.S.; Hardy, S.A.; Waters, D.W.; Burgess, J.K.; Knight, D.A.; Boyle, A.J. The Processes and Mechanisms of Cardiac and Pulmonary Fibrosis. Front. Physiol. 2017, 8, 777. [Google Scholar] [CrossRef]
- Wanner, C.; Amann, K.; Shoji, T. The heart and vascular system in dialysis. Lancet 2016, 388, 276–284. [Google Scholar] [CrossRef]
- Cooper, L.T.; Baughman, K.L.; Feldman, A.M.; Frustaci, A.; Jessup, M.; Kuhl, U.; Levine, G.N.; Narula, J.; Starling, R.C.; Towbin, J.; et al. The role of endomyocardial biopsy in the management of cardiovascular disease: A scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007, 116, 2216. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Variables | Mean | |
|---|---|---|
| Age (years) | 66.4 ± 1.79 | |
| Females | 4 (16%) | |
| Ischemic cardiomyopathy | 16 (64%) | |
| NYHA class III/IV | 8/17 | |
| Diabetes mellitus | 17 (68%) | |
| History of hypertension | 17 (68%) | |
| Primary kidney disease | 11 (44%) | |
| Body weight (kg) | 86.11 ± 3.26 | |
| MAP (mm Hg) | 84.46 ± 2.44 | |
| eGFR (mL/min/1.73 m²) | 32.5 ± 3.5 | |
| LVEF (%) | 31.7 ± 4 | |
| Preserved LV function | 8 (32%) | |
| RV dysfunction | 14 (56%) | |
| Estimated SPAP (mm Hg) | 60.13 ± 3.77 | |
| CHF day care treatment | 11 (44%) | |
| Medications | Loop diuretic | 25 (100%) |
| Thiazide and thiazide-like diuretics, metolazone | 6 (24%) | |
| Spironolactone | 9 (36%) | |
| Beta-blockers | 24 (96%) | |
| Digoxin | 10 (40%) | |
| ACEI or ARB | 8 (32%) | |
| Variables | Baseline | 3 Months | p-value |
|---|---|---|---|
| Body weight (kg) | 86.12 ± 3.26 | 77.21 ± 3.08 | <0.0001 |
| NYHA class IV (%) | 17 (68%) | 6 (24%) | 0.0041 |
| Hospitalization (day/month) | 17.3 ± 4.2 | 8.8 ± 3.9 | 0.0012 |
| Residual renal volume (L) | 1.25 ± 0.14 | 1.24 ± 0.13 | 0.8921 |
| Serum creatinine (mg/dL) | 2.53 ± 0.22 | 2.42 ± 0.25 | 0.4556 |
| eGFR (mL/min/1.73 m²) | 32.5 ± 3.5 | 35.64 ± 3.61 | 0.1471 |
| Serum urea (mg/dL) | 174.68 ± 12.66 | 119.96 ± 6.5 | <0.0001 |
| Serum sodium (mEq/L) | 135.56 ± 0.77 | 134.88 ± 0.83 | 0.3749 |
| Serum uric acid (mg/dL) | 10.6 ± 0.55 | 8.8 ± 0.42 | 0.0063 |
| Serum albumin (g/dL) | 3.4 ± 0.08 | 3.02 ± 0.09 | 0.0007 |
| Serum hematocrit (%) | 32.83 ± 1.15 | 35.99 ± 1.12 | 0.0011 |
| Serum WBC (1000/μL) | 6.5 ± 0.43 | 7.45 ± 0.42 | 0.0285 |
| Serum CRP (mg/L) | 29.97 ± 5.9 | 12.08 ± 2.26 | 0.0008 |
| Serum BNP (pg/mL) | 1564.44 ± 190.37 | 1042.96 ± 139.64 | 0.0063 |
| Serum PIIINP (micg/L) | 16.4 ± 1.37 | 17.5 ± 1.72 | 0.3400 |
| Serum MMP-2 (ng/mL) | 18.33 ± 0.92 | 17.37 ± 0.84 | 0.4237 |
| Serum TIMP-1 (ng/mL) | 382.38 ± 33.81 | 332.63 ± 29.0 | 0.0046 |
| Variables | Baseline | 6 Months | p value |
|---|---|---|---|
| Body weight (kg) | 89.65 ± 3.69 | 79.67 ± 3.39 | <0.0001 |
| NYHA class IV (%) | 12 (60%) | 4 (20%) | 0.0225 |
| Hospitalization (day/month) | 26.4 ± 8.0 | 16.8 ± 5.5 | 0.0754 |
| Residual renal volume (L) | 1.29 ± 0.14 | 1.15 ± 0.12 | 0.4663 |
| Serum creatinine (mg/dL) | 2.53 ± 0.22 | 2.81 ± 0.4 | 0.2977 |
| eGFR (mL/min/1.73 m²) | 32.5 ± 3.5 | 34.12 ± 4.66 | 0.6571 |
| Serum urea (mg/dL) | 159.45 ± 13.08 | 121.75 ± 8.15 | 0.0031 |
| Serum sodium (mEq/L) | 135.9 ± 0.83 | 136.4 ± 0.7 | 0.6089 |
| Serum uric acid (mg/dL) | 10.65 ± 0.57 | 8.78 ± 0.4 | 0.0217 |
| Serum albumin (g/dL) | 3.4 ± 0.09 | 3.25 ± 0.08 | 0.1465 |
| Serum hematocrit (%) | 32.29 ± 1.39 | 34.62 ± 1.0 | 0.0071 |
| Serum WBC (1000/μL) | 6.66 ± 0.48 | 7.54 ± 0.39 | 0.0940 |
| Serum CRP (mg/L) | 29.67 ± 6.94 | 12.42 ± 3.46 | 0.0020 |
| Serum BNP (pg/mL) | 1500.35 ± 185.67 | 1052.55 ± 164.13 | 0.0110 |
| Serum PIIINP (micg/L) | 17.13 ± 2.05 | 20.40 ± 2.35 | 0.0809 |
| Serum MMP-2 (ng/mL) | 18.94 ± 1.06 | 16.07 ± 0.8 | 0.0285 |
| Serum TIMP-1 (ng/mL) | 360.45 ± 25.35 | 291.71 ± 21.9 | 0.0107 |
| Variables | Decreased (n = 10) | Increased or Unchanged (n = 11) | p-Value |
|---|---|---|---|
| Age (years) | 66.4 ± 2.76 | 63.55 ± 2.58 | 0.4590 |
| Sex (f/m) | 2/8 | 2/9 | 1.0000 |
| CMP (ischemic/nonischemic) | 7/3 | 7/4 | 1.0000 |
| NYHA class III/IV | 2/8 | 4/7 | 0.6351 |
| Diabetes mellitus | 5 (50%) | 10 (91%) | 0.0635 |
| History of hypertension | 8 (80%) | 7 (64%) | 0.6351 |
| Primary kidney disease | 2 (20%) | 7 (64%) | 0.0805 |
| MAP (mm Hg) | 80.29 ± 3.43 | 91.28 ± 3.71 | 0.0438 |
| LVEF (%) | 28.7 ± 7.5 | 30.9 ± 5.3 | 0.8086 |
| Preserved LV function | 3 (30%) | 3 (27%) | 1.0000 |
| RV dysfunction | 6 (60%) | 8 (73%) | 0.6594 |
| LVH | 2 (20%) | 2 (18%) | 1.0000 |
| Estimated SPAP (mm Hg) | 60.6 ± 5.29 | 59 ± 5.25 | 0.8326 |
| LV diastolic dimention (cm) | 5.89 ± 0.6 | 5.67 ± 0.4 | 0.7585 |
| LV systolic dimention (cm) | 4.7 ± 0.64 | 4.65 ± 0.48 | 0.9543 |
| Estimated LV mass index (g/m2) | 131.44 ± 22.11 | 136.64 ± 18.74 | 0.8589 |
| LA diameter (cm) | 5.02 ± 0.27 | 4.74 ± 0.21 | 0.4015 |
| Serum creatinine (mg/dL) | 2.41 ± 0.43 | 2.67 ± 0.28 | 0.6085 |
| Serum albumin (g/dL) | 3.15 ± 0.07 | 3.49 ± 0.11 | 0.0171 |
| Serum sodium (meq/L) | 134.5 ± 1.62 | 136.18 ± 0.84 | 0.3557 |
| Serum CRP (mg/L) | 45.39 ± 11.07 | 12.17 ± 1.64 | 0.0057 |
| Serum BNP (pg/mL) | 1700.9 ± 329.91 | 1767.01 ± 267.51 | 0.8768 |
| Survival (m) | 18.3 ± 4.43 | 17.55 ± 3.37 | 0.8923 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunin, M.; Carmon, V.; Beckerman, P.; Dinour, D. Effect of Peritoneal Dialysis on Serum Fibrosis Biomarkers in Patients with Refractory Congestive Heart Failure. Int. J. Mol. Sci. 2019, 20, 2610. https://doi.org/10.3390/ijms20112610
Kunin M, Carmon V, Beckerman P, Dinour D. Effect of Peritoneal Dialysis on Serum Fibrosis Biomarkers in Patients with Refractory Congestive Heart Failure. International Journal of Molecular Sciences. 2019; 20(11):2610. https://doi.org/10.3390/ijms20112610
Chicago/Turabian StyleKunin, Margarita, Vered Carmon, Pazit Beckerman, and Dganit Dinour. 2019. "Effect of Peritoneal Dialysis on Serum Fibrosis Biomarkers in Patients with Refractory Congestive Heart Failure" International Journal of Molecular Sciences 20, no. 11: 2610. https://doi.org/10.3390/ijms20112610
APA StyleKunin, M., Carmon, V., Beckerman, P., & Dinour, D. (2019). Effect of Peritoneal Dialysis on Serum Fibrosis Biomarkers in Patients with Refractory Congestive Heart Failure. International Journal of Molecular Sciences, 20(11), 2610. https://doi.org/10.3390/ijms20112610