Differences in Interleukin-8 Plasma Levels between Diabetic Patients and Healthy Individuals Independently on Their Periodontal Status

 , ,
, , 
Abstract
1. Introduction
2. Results
2.1. Study Population
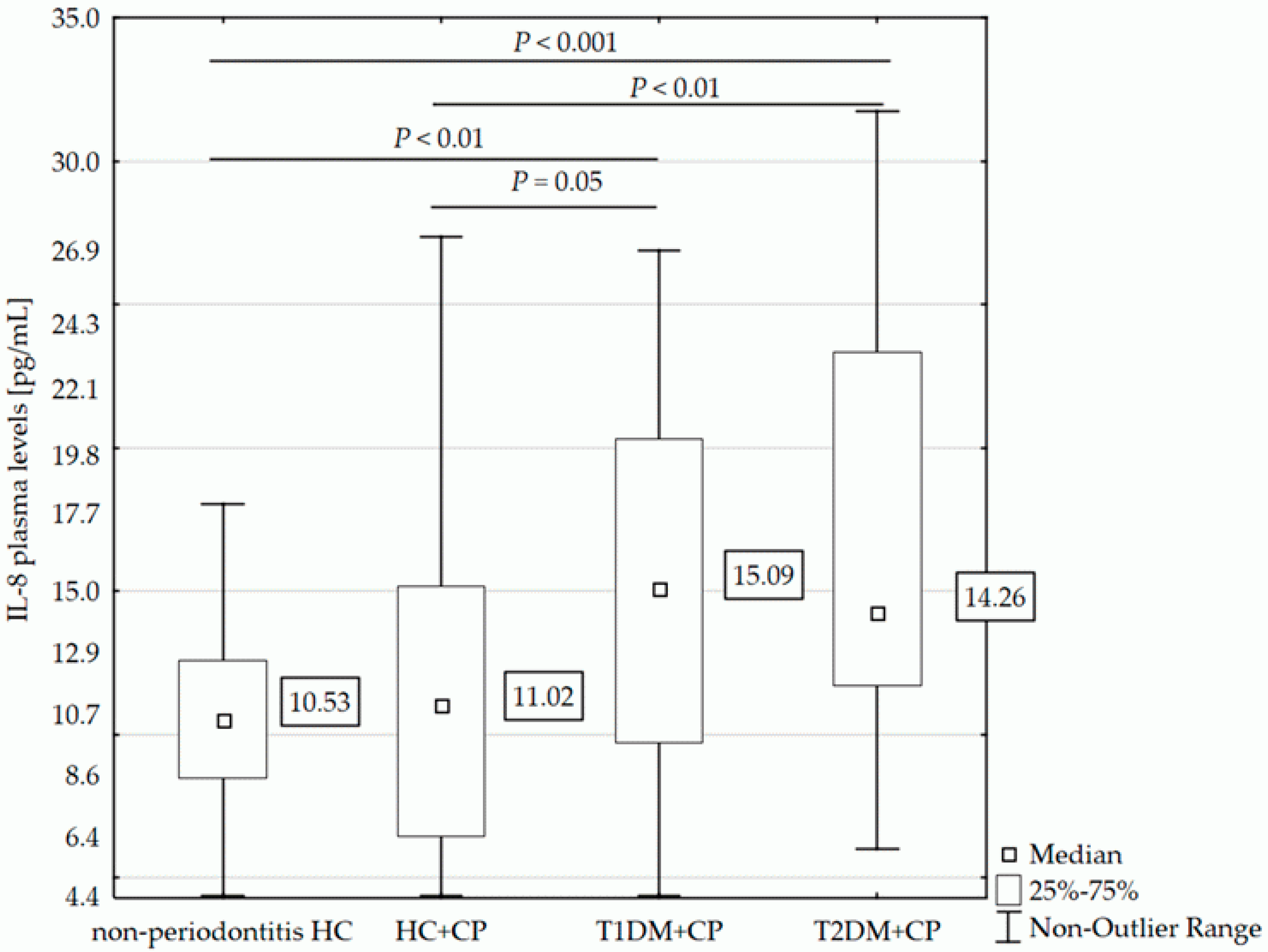
2.2. IL-8 Plasma Levels and Clinical Parameters
2.3. IL-8 Plasma Levels and Gene Variability
2.4. IL-8 Plasma Levels and Periodontal Bacteria
3. Discussion
4. Materials and Methods
4.1. Study Population and Clinical Examinations
4.2. Sample Collection and Plasma Levels Analysis
4.3. Genetic Analysis
4.4. Periodontal Bacteria Analysis
4.5. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| A. a. | Aggregatibacter actinomycetemcomitans |
| AL | Attachment loss |
| ANOVA | One-way analysis of variance |
| BMI | Body mass index |
| CXCR2 | C-X-C motif chemokine receptor 2 (receptor for IL-8) |
| CP | Chronic periodontitis |
| DM | Diabetes mellitus |
| DN | Diabetic nephropathy |
| DPN | Diabetic neuropathy |
| DR | Diabetic retinopathy |
| ELISA | Enzyme-linked immunosorbent assay |
| F. n. | Fusobacterium nucleatum |
| GCF | Gingival crevicular fluid |
| GI | Gingival index |
| HbA1c | Glycated hemoglobin |
| HC | Systemically healthy controls without periodontitis |
| HC+CP | Systemically healthy individuals with chronic periodontitis |
| HDL | High density lipoprotein |
| HWE | Hardy-Weinberg equilibrium |
| IL-8 | Interleukin-8 |
| IQR | Interquartile range |
| LDL | Low density lipoprotein |
| LPS | lipopolysaccharide |
| N | Number |
| Neg | Negative |
| PD | Pocket depth |
| P. g. | Porphyromonas gingivalis |
| P. i. | Prevotella intermedia |
| P. m. | Parvimonas micra |
| Pos | Positive |
| qPCR | Quantitative polymerase chain reaction |
| SD | Standard deviation |
| T1DM | Type 1 diabetes mellitus |
| T2DM | Type 2 diabetes mellitus |
| T. d. | Treponema denticola |
| T. f. | Tanarella forsythia |
| P. i. | Prevotella intermedia |
References
- Harris, S.B.; Tompkins, J.W.; TeHiwi, B. Call to action: A new path for improving diabetes care for Indigenous peoples, a global review. Diabetes Res. Clin. Pract. 2017, 123, 120–133. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of diabetes and diabetes-related complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [PubMed]
- Chawla, D.; Bansal, S.; Banerjee, B.D.; Madhu, S.V.; Kalra, O.P.; Tripathi, A.K. Role of advanced glycation end product (AGE)-induced receptor (RAGE) expression in diabetic vascular complications. Microvasc. Res. 2014, 95, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Papatheodorou, K.; Banach, M.; Edmonds, M.; Papanas, N.; Papazoglou, D. Complications of diabetes. J. Diabetes Res. 2015, 2015, 189525. [Google Scholar] [CrossRef] [PubMed]
- Löe, H. Periodontal disease. The sixth complication of diabetes mellitus. Diabetes Care 1993, 16, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.B.; Thakur, S.; Muddapur, M.V.; Kulkarni, R.D. Systemic cytokines in type 2 diabetes mellitus and chronic periodontitis. Curr. Diabetes Rev. 2018, 14, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J. Consensus report. Periodontal diseases: Pathogenesis and microbial factors. Ann. Periodontol. 1996, 1, 926–932. [Google Scholar] [CrossRef]
- Armitage, G.C. Comparison of the microbiological features of chronic and aggressive periodontitis. Periodontol. 2000 2010, 53, 70–88. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Henderson, B.; Sadiq, S.T.; Donos, N. Genetic dysbiosis: The role of microbial insults in chronic inflammatory diseases. J. Oral Microbiol. 2014, 6, 22962. [Google Scholar] [CrossRef] [PubMed]
- Festa, A.; D’Agostino, R., Jr.; Howard, G.; Mykkänen, L.; Tracy, R.P.; Haffner, S.M. Chronic subclinical inflammation as part of the insulin resistance syndrome: The Insulin Resistance Atherosclerosis Study (IRAS). Circulation 2000, 102, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Moutsopoulos, N.M.; Madianos, P.N. Low-grade inflammation in chronic infectious diseases: Paradigm of periodontal infections. Ann. N. Y. Acad. Sci. 2006, 1088, 251–264. [Google Scholar] [CrossRef] [PubMed]
- Manouchehr-Pour, M.; Spagnuolo, P.J.; Rodman, H.M.; Bissada, N.F. Comparison of neutrophil chemotactic response in diabetic patients with mild and severe periodontal disease. J. Periodontol. 1981, 52, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Wuyts, A.; Proost, P.; Lenaerts, J.P.; Ben-Baruch, A.; Van Damme, J.; Wang, J.M. Differential usage of the CXC chemokine receptors 1 and 2 by interleukin-8, granulocyte chemotactic protein-2 and epithelial-cell-derived neutrophil attractant-78. Eur. J. Biochem. 1998, 255, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Harada, A.; Sekido, N.; Akahoshi, T.; Wada, T.; Mukaida, N.; Matsushima, K. Essential involvement of interleukin-8 (IL-8) in acute inflammation. J. Leukoc. Biol. 1994, 56, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, Z.; Arababadi, M.K.; Hassanshahi, G. CXCL10 activities, biological structure, and source along with its significant role played in pathophysiology of type I diabetes mellitus. Inflammation 2013, 36, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Ismail, N.A.; Abd El Baky, A.N.; Ragab, S.; Hamed, M.; Hashish, M.A.; Shehata, A. Monocyte chemoattractant protein 1 and macrophage migration inhibitory factor in children with type 1 diabetes. J. Pediatr. Endocrinol. Metab. 2016, 29, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Harsunen, M.H.; Puff, R.; D’Orlando, O.; Giannopoulou, E.; Lachmann, L.; Beyerlein, A.; von Meyer, A.; Ziegler, A.G. Reduced blood leukocyte and neutrophil numbers in the pathogenesis of type 1 diabetes. Horm. Metab. Res. 2013, 45, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Valle, A.; Giamporcaro, G.M.; Scavini, M.; Stabilini, A.; Grogan, P.; Bianconi, E.; Sebastiani, G.; Masini, M.; Maugeri, N.; Porretti, L.; et al. Reduction of circulating neutrophils precedes and accompanies type 1 diabetes. Diabetes 2013, 62, 2072–2077. [Google Scholar] [CrossRef] [PubMed]
- Citro, A.; Valle, A.; Cantarelli, E.; Mercalli, A.; Pellegrini, S.; Liberati, D.; Daffonchio, L.; Kastsiuchenka, O.; Ruffini, P.A.; Battaglia, M.; et al. CXCR1/2 inhibition blocks and reverses type 1 diabetes in mice. Diabetes 2015, 64, 1329–1340. [Google Scholar] [CrossRef] [PubMed]
- Haurogné, K.; Pavlovic, M.; Rogniaux, H.; Bach, J.M.; Lieubeau, B. Type 1 diabetes prone NOD mice have diminished Cxcr1 mRNA expression in polymorphonuclear neutrophils and CD4+ T lymphocytes. PLoS ONE 2015, 10, e0134365. [Google Scholar] [CrossRef] [PubMed]
- Lappin, D.F.; Robertson, D.; Hodge, P.; Treagus, D.; Awang, R.A.; Ramage, G.; Nile, C.J. The influence of glycated hemoglobin on the cross susceptibility between type 1 diabetes mellitus and periodontal disease. J. Periodontol. 2015, 86, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, Y.; Takedachi, M.; Mori, K.; Kubota, M.; Yamada, S.; Kitamura, M.; Murakami, S. High glucose-induced oxidative stress increases IL-8 production in human gingival epithelial cells. Oral Dis. 2016, 22, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Engebretson, S.P.; Vossughi, F.; Hey-Hadavi, J.; Emingil, G.; Grbic, J.T. The influence of diabetes on gingival crevicular fluid beta-glucuronidase and interleukin-8. J. Clin. Periodontol. 2006, 33, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Longo, P.L.; Artese, H.P.; Horliana, A.C.; Gomes, G.H.; Romito, G.A.; Dib, S.A.; Mayer, M.P. Inflammatory markers in gingival crevicular fluid of periodontitis patients with type 2 diabetes mellitus according to glycemic control: A pilot study. Dent. Res. J. (Isfahan) 2015, 12, 449–455. [Google Scholar] [CrossRef]
- Mohamed, H.G.; Idris, S.B.; Ahmed, M.F.; Åstrøm, A.N.; Mustafa, K.; Ibrahim, S.O.; Mustafa, M. Influence of type 2 diabetes on local production of inflammatory molecules in adults with and without chronic periodontitis: A cross-sectional study. BMC Oral Health 2015, 15, 86. [Google Scholar] [CrossRef] [PubMed]
- Purohit, S.; Sharma, A.; Hopkins, D.; Steed, L.; Bode, B.; Anderson, S.W.; Reed, J.C.; Steed, R.D.; Yang, T.; She, J.X. Large-scale discovery and validation studies demonstrate significant reductions in circulating levels of IL8, IL-1Ra, MCP-1, and MIP-1β in patients with type 1 diabetes. J. Clin. Endocrinol. Metab. 2015, 100, E1179–E1187. [Google Scholar] [CrossRef] [PubMed]
- Hull, J.; Thomson, A.; Kwiatkowski, D. Association of respiratory syncytial virus bronchiolitis with the interleukin 8 gene region in UK families. Thorax 2000, 55, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Hu, N.; Westra, J.; Rutgers, A.; Doornbos-Van der Meer, B.; Huitema, M.G.; Stegeman, C.A.; Abdulahad, W.H.; Satchell, S.C.; Mathieson, P.W.; Heeringa, P.; et al. Decreased CXCR1 and CXCR2 expression on neutrophils in anti-neutrophil cytoplasmic autoantibody-associated vasculitides potentially increases neutrophil adhesion and impairs migration. Arthritis Res. Ther. 2011, 13, R201. [Google Scholar] [CrossRef] [PubMed]
- Ryan, B.M.; Robles, A.I.; McClary, A.C.; Haznadar, M.; Bowman, E.D.; Pine, S.R.; Brown, D.; Khan, M.; Shiraishi, K.; Kohno, T.; et al. Identification of a functional SNP in the 3’UTR of CXCR2 that is associated with reduced risk of lung cancer. Cancer Res. 2015, 75, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Borilova Linhartova, P.; Vokurka, J.; Poskerova, H.; Fassmann, A.; Izakovicova Holla, L. Haplotype analysis of interleukin-8 gene polymorphisms in chronic and aggressive periodontitis. Mediat. Inflamm. 2013, 2013, 342351. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.; Genco, R.; Working Group 2 of the Joint EFP/AAP Workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef] [PubMed]
- Borgnakke, W.S.; Ylöstalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes: Systematic review of epidemiologic observational evidence. J. Periodontol. 2013, 84, S135–S152. [Google Scholar] [CrossRef] [PubMed]
- Iacopino, A.M. Periodontitis and diabetes interrelationships: Role of inflammation. Ann. Periodontol. 2001, 6, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Van Sickle, B.J.; Simmons, J.; Hall, R.; Raines, M.; Ness, K.; Spagnoli, A. Increased circulating IL-8 is associated with reduced IGF-1 and related to poor metabolic control in adolescents with type 1 diabetes mellitus. Cytokine 2009, 48, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Costa, K.L.; Taboza, Z.A.; Angelino, G.B.; Silveira, V.R.; Montenegro, R., Jr.; Haas, A.N.; Rego, R.O. Influence of periodontal disease on changes of glycated hemoglobin levels in type 2 diabetics: A retrospective cohort study. J. Periodontol. 2017, 88, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Polak, D.; Shapira, L. An update on the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J. Clin. Periodontol. 2018, 45, 150–166. [Google Scholar] [CrossRef] [PubMed]
- Podkówka, R.; Wiśniewska, J.; Korybalska, K.; Wieczorowska-Tobis, K.; Knapowski, J. Plasma level of interleukin-6 and interleukin-8 in the elderly. Prz. Lek. 2002, 59, 230–233. [Google Scholar] [PubMed]
- Kim, C.S.; Park, H.S.; Kawada, T.; Kim, J.H.; Lim, D.; Hubbard, N.E.; Kwon, B.S.; Erickson, K.L.; Yu, R. Circulating levels of MCP-1 and IL-8 are elevated in human obese subjects and associated with obesity-related parameters. Int. J. Obes. (Lond.) 2006, 30, 347–1355. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Yue, Y.; Tian, Y.; Li, J.L.; Wang, M.; Liang, H.; Liao, P.; Loo, W.T.; Cheung, M.N.; Chow, L.W. Association of matrix metalloproteinase (MMP)-1, 3, 9, interleukin (IL)-2, 8 and cyclooxygenase (COX)-2 gene polymorphisms with chronic periodontitis in a Chinese population. Cytokine 2012, 60, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Fredriksson, M.I. Effect of priming in subpopulations of peripheral neutrophils from patients with chronic periodontitis. J. Periodontol. 2012, 83, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Perlman, A.S.; Chevalier, J.M.; Wilkinson, P.; Liu, H.; Parker, T.; Levine, D.M.; Sloan, B.J.; Gong, A.; Sherman, R.; Farrell, F.X. Serum inflammatory and immune mediators are elevated in early stage diabetic nephropathy. Ann. Clin. Lab. Sci. 2015, 45, 256–263. [Google Scholar] [PubMed]
- Lee, W.P.; Tai, D.I.; Lan, K.H.; Li, A.F.; Hsu, H.C.; Lin, E.J.; Lin, Y.P.; Sheu, M.L.; Li, C.P.; Chang, F.Y.; et al. The -251T allele of the interleukin-8 promoter is associated with increased risk of gastric carcinoma featuring diffuse-type histopathology in Chinese population. Clin. Cancer Res. 2005, 11, 6431–6441. [Google Scholar] [CrossRef] [PubMed]
- Benakanakere, M.R.; Finoti, L.S.; Tanaka, U.; Grant, G.R.; Scarel-Caminaga, R.M.; Kinane, D.F. Investigation of the functional role of human Interleukin-8 gene haplotypes by CRISPR/Cas9 mediated genome editing. Sci. Rep. 2016, 6, 31180. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Di Iorio, A.; Onabolu, O.; Lin, G.H. Periodontal infectogenomics: Systematic review of associations between host genetic variants and subgingival microbial detection. J. Clin. Periodontol. 2016, 43, 889–900. [Google Scholar] [CrossRef] [PubMed]
- Mesia, R.; Gholami, F.; Huang, H.; Clare-Salzler, M.; Aukhil, I.; Wallet, S.M.; Shaddox, L.M. Systemic inflammatory responses in patients with type 2 diabetes with chronic periodontitis. BMJ Open Diabetes Res. Care 2016, 4, e000260. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Kim, Y.; Min, B.M.; Han, S.H.; Choi, Y. Innate immune responses of gingival epithelial cells to nonperiodontopathic and periodontopathic bacteria. J. Periodontal. Res. 2007, 42, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Kurgan, Ş.; Kansal, S.; Nguyen, D.; Stephens, D.; Koroneos, Y.; Hasturk, H.; Van Dyke, T.E.; Kantarci, A. Strain-specific impact of Fusobacterium nucleatum on neutrophil function. J. Periodontol. 2017, 88, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Bartova, J.; Borilova Linhartova, P.; Podzimek, S.; Janatova, T.; Svobodova, K.; Fassmann, A.; Duskova, J.; Belacek, J.; Izakovicova Holla, L. The effect of IL-4 gene polymorphisms on cytokine production in patients with chronic periodontitis and in healthy controls. Mediat. Inflamm. 2014, 2014, 85757. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Borilova Linhartova, P.; Bartova, J.; Poskerova, H.; Machal, J.; Vokurka, J.; Fassmann, A.; Izakovicova Holla, L. Apolipoprotein E gene polymorphisms in relation to chronic periodontitis, periodontopathic bacteria, and lipid levels. Arch. Oral Biol. 2015, 60, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Löe, H. The gingival index, the plaque index and the retention index systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of Medical Care in Diabetes—2016. Classification and Diagnosis of Diabetes. Diabetes Care 2016, 39, S11–S22. [Google Scholar] [CrossRef]
- Czech Diabetes Association. Diabetic Treatment. Glycated Hemoglobin and Diabetic Control. Available online: http://www.diabetickaasociace.cz/radi/co-na-vas-prozradi-glykovany-hemoglobin-o-kompenzaci-diabetu/ (accessed on 22 July 2017). (In Czech).
- Sambrook, J.; Fritsch, E.F.; Maniatis, T. Molecular Cloning: A Laboratory Manual, 2nd ed.; Cold Spring Harbor Laboratory Press: Cold Spring, NY, USA, 1989; pp. 9–17. ISBN 0-87969-309-6. [Google Scholar]


{kind=link}
| Characteristics (mean ± SD) | Non-Periodontitis HC N = 32 | HC+CP N = 41 | T1DM+CP N = 36 | T2DM+CP N = 44 |
|---|---|---|---|---|
| Age (years) | 45.5 ± 9.6 | 59.5 ± 9.3 * | 49.7 ± 10.4 | 66.8 ± 8.5 * |
| Duration of DM (years) | 0.0 ± 0.0 | 0.0 ± 0.0 | 25.1 ± 11.8 | 10.2 ± 7.7 |
| DM control (well/satisfactorily/unsatisfactorily controlled) % | − | − | 0.0/8.3/91.7 | 7.7/28.2/64.1 |
| Sex (males) % | 31.3 | 26.8 | 44.4 | 40.9 |
| Smoking (yes) % | 5.3 | 19.4 | 25.0 * | 7.1 ‡,§ |
| DN (yes) % | 0.0 | 0.0 | 27.6 | 16.7 |
| DR (yes) % | 0.0 | 0.0 | 63.3 ‖ | 0.0 |
| DPN (yes) % | 0.0 | 0.0 | 50.0 ‖ | 9.3 |
| BMI | 23.8 ± 4.2 | 26.8 ± 3.9 | 25.1 ± 3.1 | 29.9 ± 7.7 *,§ |
| GI | 0.3 ± 0.2 | 0.9 ± 0.3 † | 1 ± 0.3 † | 1.1 ± 0.3 † |
| PD (mm) | 0.6 ± 0.2 | 3.3 ± 0.9 * | 3.6 ± 0.9 † | 3.8 ± 1.0 † |
| AL (mm) | 0.8 ± 0.2 | 4.1 ± 1.1 † | 4.4 ± 1.5 † | 4.7 ± 1.2 † |
| N of sites with PD ≥ 5 mm | 0 | 18 ± 17 * | 20 ± 19 * | 20 ± 16 * |
| N of teeth with PD ≥ 5 mm | 0 | 10 ± 7 * | 11 ± 7 * | 11 ± 6 * |
| N of sites with AL ≥ 5 mm | 0 | 32 ± 21 * | 38 ± 28 * | 38 ± 19 * |
| N of teeth with AL ≥ 5 mm | 0 | 15 ± 7 * | 15 ± 7 * | 15 ± 6 * |
| HbA1c (mmol/mol) | - | - | 69.6 ± 12.0 | 57.7 ± 14.5 § |
| Blood glucose (mmol/L) | 5.4 ± 0.5 | 5.7 ± 0.3 | 7.5 ± 2.3 | 7.7 ± 2.4 |
| Total cholesterol (mmol/L) | - | - | 4.7 ± 0.7 | 4.7 ± 1.0 |
| Triglycerides (mmol/L) | - | - | 1.0 ± 0.6 | 2.0 ± 1.2 |
| LDL (mmol/L) | - | - | 2.7 ± 0.6 | 2.7 ± 0.9 |
| HDL (mmol/L) | - | - | 1.6 ± 0.4 | 1.3 ± 0.3 |
| IL-8 Levels, Median [IQR] in pg/mL | ||
|---|---|---|
| Well Controlled N = 4 | Satisfactorily Controlled N = 14 | Unsatisfactorily Controlled N = 57 |
| 12.68 [10.52–40.56] | 14.45 [12.15–23.13] | 14.04 [10.05–19.67] |
| IL-8 Levels, Median [IQR] in pg/mL | ||
|---|---|---|
| Normal Weight BMI ≤ 25.0 kg/m2 N = 9 | Overweight 25 kg/m2 < BMI ≤ 30 kg/m2 N = 14 | Obese BMI > 30 kg/m2 N = 21 |
| 12.68 [9.16–16.54] | 13.75 [12.00–23.13] | 14.04 [12.50–16.24] |
| SNPs Genotypes | IL-8 Levels, Median [IQR] in pg/mL | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Periodontitis HC N = 32 (%) | HC+CP N = 41 (%) | T1DM+CP N = 36 (%) | T2DM+CP N = 43 (%) | T2DM+CP Subgroups | |||||||||
| Well/Satisfactorily Controlled N = 16 (%) | Unsatisfactorily Controlled N = 27 (%) | ||||||||||||
| IL-8 (−251A/T, rs4073) | TT | 10 (31.3) | 9.20 [8.61–11.86] | 10 (24.4) | 10.36 [6.47–13.60] | 11 (30.6) | 13.16 [10.43–19.67] | 16 (37.2) | 13.75 [10.73–25.39] | 5 (31.3) | 12.87 [12.29–24.63] | 11 (40.7) | 14.33 [9.16–26.14] |
| AT | 15 (46.9) | 11.00 [7.52–12.87] | 21 (51.2) | 7.68 [5.66–15.17] | 16 (44.4) | 17.38 [7.01–20.92] | 17 (39.5) | 14.18 [11.43–16.54] | 6 (37.4) | 15.10 [9.86–20.27] | 11 (40.7) | 13.49 [11.43–16.54] | |
| AA | 7 (21.8) | 10.86 [8.61–12.66] | 10 (24.4) | 12.19 [8.88–16.24] | 9 (25.0) | 13.33 [10.86–22.70] | 10 (23.3) | 15.80 [12.33–23.13] | 5 (31.3) | 16.69 [15.36–23.13] | 5 (18.6) | 14.04 [12.00–16.24] | |
| CXCR2 (+1208C/T, rs1126579) | CC | 9 (28.1) | 11.28 [8.61–12.87] | 14 (34.1) | 12.30 [7.92–15.21] | 9 (25.0) | 17.89 [10.43–20.87] | 17 (39.5) | 15.09 [12.29–23.91] | 7 (43.8) | 15.36 [12.29–24.63] | 10 (37.0) | 14.88 [9.16–23. 91] |
| CT | 17 (53.1) | 9.09 [7.52–11.43] | 18 (43.9) | 11.57 [6.47–15.17] | 20 (55.6) | 14.00 [8.63–23.52] | 21 (48.9) | 13.16 [11.43–16.24] | 7 (43.8) | 14.18 [9.86–30.99] | 14 (51.9) | 13.16 [11.43–16.24] | |
| TT | 6 (18.8) | 11.43 [10.86–12.50] | 9 (22.0) | 6.99 [5.66–11.02] | 7 (19.4) | 12.00 [4.39–18.57] | 5 (11.6) | 16.69 [13.49–20.27] | 2 (12.4) | 18.48 [16.69–20.27] | 3 (11.1) | 13.49 [12.00–31.74] | |
| Bacteria (%) | IL-8 Levels, Median [IQR] in pg/mL | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Periodontitis HC N = 19 | HC+CP N = 41 | T1DM+CP N = 36 | T2DM+CP N = 44 | T2DM+CP Subgroups | ||||||||
| Well/Satisfactorily Controlled N = 17 | Unsatisfactorily Controlled N = 27 | |||||||||||
| F. n. neg | 0.0 | - | 2.4 | 46.40 [46.40–46.40] | 0.0 | - | 2.3 | 30.86 [30.86–30.86] | 0.0 | - | 3.7 | 30.86 [30.86–30.86] |
| F. n. pos | 100.0 | 10.21 [8.61–12.66] | 97.6 | 10.80 [6.43–14.83] | 100.0 | 15.09 [9.73–20.32] | 97.7 | 14.18 [11.43–23.13] | 100.0 | 15.36 [12.29–23.13] | 96.3 | 13.77 [11.43–16.54] |
| A. a. neg | 68.4 | 10.21 [8.61–12.50] | 48.8 | 7.80 [5.99–13.32] | 55.6 | 18.41 [10.38–24.41] | 38.6 | 13.49 [12.33–16.54] | 29.4 | 28.16 [12.87–30.99] | 44.4 | 13.33 [10.58–14.50] |
| A. a. pos | 31.6 | 10.14 [9.09–13.49] | 51.2 | 13.45 [8.75–15.17] | 44.4 | 13.25 [8.63–17.72] | 61.4 | 15.09 [11.18–23.58] | 70.6 | 14.77 [10.52–18.48] | 55.6 | 15.09 [12.00–26.14] |
| P. g. neg | 68.4 | 9.73 [7.24–12.66] | 14.6 | 13.18 [7.99–27.35] | 25.0 | 24.33 [16.86–24.78] | 22.7 | 14.26 [12.33–26.14] | 17.6 | 12.33 [9.09–15.36] | 25.9 | 16.24 [12.50–30.86] |
| P. g. pos | 31.6 | 10.54 [9.41–12.50] | 85.4 | 10.57 [6.02–14.48] | 75.0 | 12.00 [7.24–18.92] * | 77.3 | 14.26 [11.43–23.13] | 82.4 | 16.36 [12.29–24.63] | 74.1 | 13.77 [10.58–15.82] |
| T. f. neg | 36.8 | 8.61 [6.72–9.73] | 2.4 | 46.40 [46.40–46.40] | 8.3 | 24.33 [19.67–40.67] | 0.0 | - | 0.0 | - | 0.0 | - |
| T. f. pos | 63.2 | 11.67 [9.81–13.66] * | 97.6 | 10.80 [6.43–14.83] | 91.7 | 13.33 [9.41–19.43] * | 100.0 | 14.26 [11.72–23.36] | 100.0 | 15.36 [12.29–23.13] | 100.0 | 14.04 [11.43–23.58] |
| T. d. neg | 47.4 | 8.77 [7.24–12.33] | 14.6 | 14.83 [13.45–19.37] | 25.0 | 20.87 [19.43–24.78] | 22.7 | 13.33 [12.50–15.36] | 17.6 | 12.87 [12.33–15.36] | 25.9 | 13.49 [12.50–16.54] |
| T. d. pos | 52.6 | 10.93 [9.41–13.83] | 85.4 | 10.15 [6.39–14.04] | 75.0 | 12.00 [7.24–18.57] * | 77.3 | 14.50 [11.18–23.91] | 82.4 | 16.36 [11.18–24.63] | 74.1 | 14.19 [10.58–23.75] |
| P. m. neg | 31.6 | 9.89 [7.24–12.66] | 2.4 | 46.40 [46.40–46.40] | 0.0 | - | 0.0 | - | 0.0 | - | 0.0 | - |
| P. m. pos | 68.4 | 10.21 [9.09–12.50] | 97.6 | 10.80 [6.43–14.83] | 100.0 | 15.09 [9.73–20.32] | 100.0 | 14.26 [11.72–23.36] | 100.0 | 15.36 [12.29–23.13] | 100.0 | 14.04 [11.43–23.58] |
| P. i. neg | 47.4 | 8.77 [6.72–12.66] | 41.5 | 7.99 [6.02–14.48] | 41.7 | 17.89 [12.15–24.33] | 45.5 | 14.08 [10.14–16.39] | 35.3 | 11.76 [9.09–15.36] | 51.9 | 15.05 [11.43–23.58] |
| P. i. pos | 52.6 | 10.54 [9.41–12.50] | 58.5 | 11.57 [7.60–15.19] | 58.3 | 12.00 [7.84–18.92] | 54.5 | 14.26 [12.40–24.27] | 64.7 | 20.27 [12.87–28.16] * | 48.1 | 13.49 [12.00–14.67] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borilova Linhartova, P.; Kavrikova, D.; Tomandlova, M.; Poskerova, H.; Rehka, V.; Dušek, L.; Izakovicova Holla, L. Differences in Interleukin-8 Plasma Levels between Diabetic Patients and Healthy Individuals Independently on Their Periodontal Status. Int. J. Mol. Sci. 2018, 19, 3214. https://doi.org/10.3390/ijms19103214
Borilova Linhartova P, Kavrikova D, Tomandlova M, Poskerova H, Rehka V, Dušek L, Izakovicova Holla L. Differences in Interleukin-8 Plasma Levels between Diabetic Patients and Healthy Individuals Independently on Their Periodontal Status. International Journal of Molecular Sciences. 2018; 19(10):3214. https://doi.org/10.3390/ijms19103214
Chicago/Turabian StyleBorilova Linhartova, Petra, Denisa Kavrikova, Marie Tomandlova, Hana Poskerova, Vaclav Rehka, Ladislav Dušek, and Lydie Izakovicova Holla. 2018. "Differences in Interleukin-8 Plasma Levels between Diabetic Patients and Healthy Individuals Independently on Their Periodontal Status" International Journal of Molecular Sciences 19, no. 10: 3214. https://doi.org/10.3390/ijms19103214
APA StyleBorilova Linhartova, P., Kavrikova, D., Tomandlova, M., Poskerova, H., Rehka, V., Dušek, L., & Izakovicova Holla, L. (2018). Differences in Interleukin-8 Plasma Levels between Diabetic Patients and Healthy Individuals Independently on Their Periodontal Status. International Journal of Molecular Sciences, 19(10), 3214. https://doi.org/10.3390/ijms19103214