Relationship between Serum BDNF Levels and Depressive Mood in Subacute Stroke Patients: A Preliminary Study



Abstract
1. Introduction
2. Results
2.1. Demographic Data and Clinical Variables
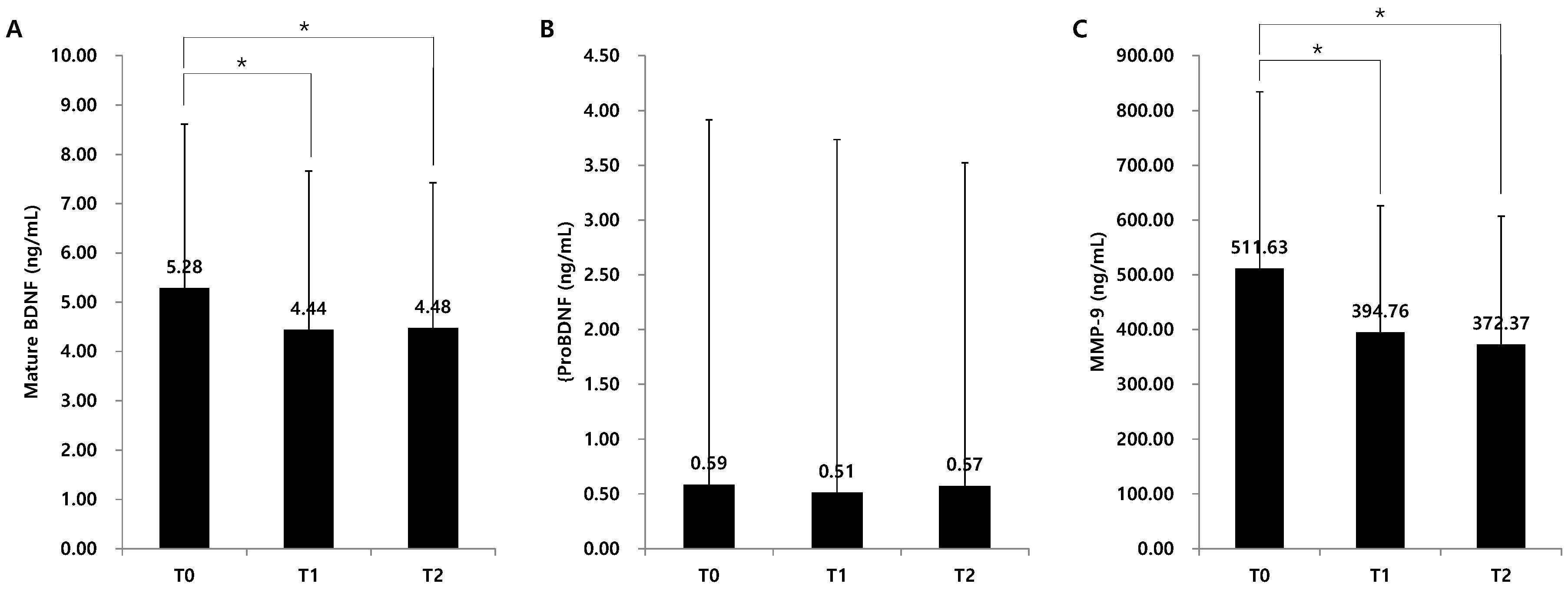
2.2. Serum Levels of Mature BDNF, ProBDNF, and Metalloproteinase-9 (MMP-9)
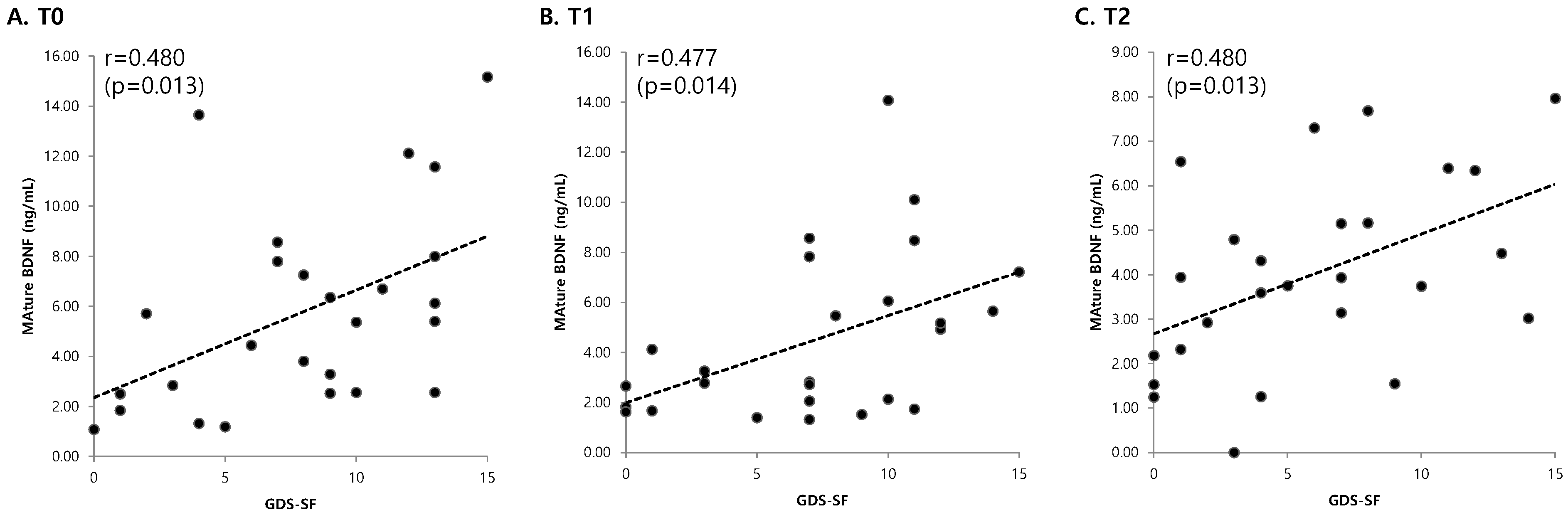
2.3. Correlations with Clinical Variables
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Experimental Design
4.3. Measurement of Mature BDNF, ProBDNF, and MMP-9 Serum Levels
4.4. BDNF Genotyping Technique
4.5. Assessment of Clinical Variables
4.6. Data Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Mukherjee, D.; Patil, C.G. Epidemiology and the global burden of stroke. World Neurosurg. 2011, 76, S85–S90. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Langhorne, P.; Sandercock, P.; Prasad, K. Evidence-based practice for stroke. Lancet Neurol. 2009, 8, 308–309. [Google Scholar] [CrossRef]
- Villa, R.F.; Ferrari, F.; Moretti, A. Post-stroke depression: Mechanisms and pharmacological treatment. Pharmacol. Ther. 2018, 184, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Werheid, K. A Two-Phase Pathogenetic Model of Depression after Stroke. Gerontology 2015, 62, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Levada, O.A.; Troyan, A.S. Poststroke Depression Biomarkers: A Narrative Review. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Gittler, M.; Davis, A.M. Guidelines for Adult Stroke Rehabilitation and Recovery. JAMA 2018, 319, 820–821. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Woo, N.H.; Teng, H.K.; Siao, C.J.; Chiaruttini, C.; Pang, P.T.; Milner, T.A.; Hempstead, B.L.; Lu, B. Activation of p75NTR by proBDNF facilitates hippocampal long-term depression. Nat. Neurosci. 2005, 8, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Lopes, M.; Fregni, F. A systematic review and meta-analysis of clinical studies on major depression and BDNF levels: Implications for the role of neuroplasticity in depression. Int. J. Neuropsychopharmacol. 2008, 11, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhao, Y.D.; Zeng, J.W.; Chen, X.Y.; Wang, R.D.; Cheng, S.Y. Serum Brain-derived neurotrophic factor levels in post-stroke depression. J. Affect. Disord. 2014, 168, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Castren, E.; Rantamaki, T. Role of brain-derived neurotrophic factor in the aetiology of depression: Implications for pharmacological treatment. CNS Drugs 2010, 24, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Duman, R.; Sanacora, G. Serum brain-derived neurotrophic factor, depression, and antidepressant medications: Meta-analyses and implications. Biol. Psychiatry 2008, 64, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Kishi, T.; Yoshimura, R.; Ikuta, T.; Iwata, N. Brain-Derived Neurotrophic Factor and Major Depressive Disorder: Evidence from Meta-Analyses. Front. Psychiatry 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Stewart, R.; Kang, H.J.; Kim, S.Y.; Kim, S.W.; Shin, I.S.; Park, M.S.; Kim, H.R.; Shin, M.G.; Cho, K.H.; et al. A longitudinal study of BDNF promoter methylation and genotype with poststroke depression. J. Affect. Disord. 2013, 149, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.B.; Xu, Y.H.; He, Y.; Xue, F.; Wei, J.; Zhang, H.; Wu, J. Decreased Serum Brain-Derived Neurotrophic Factor May Indicate the Development of Poststroke Depression in Patients with Acute Ischemic Stroke: A Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2018, 27, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Ploughman, M.; Windle, V.; MacLellan, C.L.; White, N.; Dore, J.J.; Corbett, D. Brain-derived neurotrophic factor contributes to recovery of skilled reaching after focal ischemia in rats. Stroke 2009, 40, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Alcantara, C.C.; Garcia-Salazar, L.F.; Silva-Couto, M.A.; Santos, G.L.; Reisman, D.S.; Russo, T.L. Post-stroke BDNF Concentration Changes Following Physical Exercise: A. Systematic Review. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Mang, C.S.; Campbell, K.L.; Ross, C.J.; Boyd, L.A. Promoting neuroplasticity for motor rehabilitation after stroke: Considering the effects of aerobic exercise and genetic variation on brain-derived neurotrophic factor. Phys. Ther. 2013, 93, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Stanne, T.M.; Aberg, N.D.; Nilsson, S.; Jood, K.; Blomstrand, C.; Andreasson, U.; Blennow, K.; Zetterberg, H.; Isgaard, J.; Svensson, J.; et al. Low Circulating Acute Brain-Derived Neurotrophic Factor Levels Are Associated With Poor Long-Term Functional Outcome After Ischemic Stroke. Stroke 2016, 47, 1943–1945. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Ishikawa, M.; Niitsu, T.; Nakazato, M.; Watanabe, H.; Shiraishi, T.; Shiina, A.; Hashimoto, T.; Kanahara, N.; Hasegawa, T.; et al. Decreased serum levels of mature brain-derived neurotrophic factor (BDNF), but not its precursor proBDNF, in patients with major depressive disorder. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.M.; Kim, Y.H.; Yoon, K.J.; Uhm, K.E.; Chang, W.H. Different responses to facilitatory rTMS according to BDNF genotype. Clin. Neurophysiol. 2015, 126, 1348–1353. [Google Scholar] [CrossRef] [PubMed]
- Lesher, E.L.; Berryhill, J.S. Validation of the Geriatric Depression Scale--Short Form among inpatients. J. Clin. Psychol. 1994, 50, 256–260. [Google Scholar] [CrossRef]
- Sivrioglu, E.Y.; Sivrioglu, K.; Ertan, T.; Ertan, F.S.; Cankurtaran, E.; Aki, O.; Uluduz, D.; Ince, B.; Kirli, S. Reliability and validity of the Geriatric Depression Scale in detection of poststroke minor depression. J. Clin. Exp. Neuropsychol. 2009, 31, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Na, D.L.; Hahn, S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]



{kind=link}
{kind=link}
| Parameters | Total Patients (n = 38) | Patients Who Performed GDS-SF (n = 26) |
|---|---|---|
| Sex (male:female) | 23:15 | 19:7 |
| Age | 62.9 ± 14.6 (28–86) | 59.9 ± 13.2 (33–86) |
| Stroke type (infarct:hemorrhage) | 27:11 | 17:9 |
| Supratentorial:Intratentorial | 35:3 | 23:3 |
| Lesion side (right:left) | 18:20 | 17:9 |
| Duration of stroke (T0, days) | 15.8 ± 6.0 (6–28) | 16.0 ± 5.7 (6–28) |
| NIHSS at T0 | 7.5 ± 5.4 (0–22) | 5.8 ± 4.3 (0–14) |
| BDNF genotype (Val/Val:Val/Met:Met/Met) | 10:13:15 | 6:10:10 |
| Parameters | T0 | T1 | T2 |
|---|---|---|---|
| GDS-SF (n = 26) | 7.9 ± 4.4 | 7.2 ± 4.5 | 6.0 ± 4.6 * |
| NIHSS (n = 38) | 7.5 ± 5.4 | 6.8 ± 4.7 | 6.6 ± 4.8 * |
| K-MMSE (n = 38) | 16.9 ± 12.3 | 18.0 ± 12.7 | 18.7 ± 12.6 * |
| Parameters | GDS-SF (n = 26) | K-MMSE (n = 38) | NIHSS (n = 38) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | ||
| Mature BDNF (ng/mL) | T0 | 0.480 * | - | - | 0.043 | - | - | 0.045 | - | - |
| (0.013) | (0.800) | (0.788) | ||||||||
| T1 | - | 0.477 * | - | - | −0.104 | - | - | 0.186 | - | |
| (0.014) | (0.541) | (0.263) | ||||||||
| T2 | - | - | 0.480 * | - | - | −0.180 | - | - | 0.194 | |
| (0.013) | (0.280) | (0.243) | ||||||||
| ProBDNF (ng/mL) | T0 | 0.006 | - | - | −0.168 | - | - | 0.126 | - | - |
| (0.977) | (0.313) | (0.452) | ||||||||
| T1 | - | 0.141 | - | - | −0.111 | - | 0.117 | - | ||
| (0.492) | (0.513) | (0.483) | ||||||||
| T2 | - | - | 0.373 | - | - | 0.048 | - | - | 0.024 | |
| (0.060) | (0.775) | (0.888) | ||||||||
| MMP-9 (ng/mL) | T0 | 0.079 | - | - | −0.394 * | - | - | 0.495 * | - | - |
| (0.700) | (0.014) | (0.002) | ||||||||
| T1 | - | 0.312 | - | - | −0.191 | - | 0.355 * | - | ||
| (0.120) | (0.256) | (0.029) | ||||||||
| T2 | - | - | 0.093 | - | −0.207 | - | - | 0.147 | ||
| (0.651) | (0.213) | (0.379) | ||||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, W.H.; Shin, M.A.; Lee, A.; Kim, H.; Kim, Y.-H. Relationship between Serum BDNF Levels and Depressive Mood in Subacute Stroke Patients: A Preliminary Study. Int. J. Mol. Sci. 2018, 19, 3131. https://doi.org/10.3390/ijms19103131
Chang WH, Shin MA, Lee A, Kim H, Kim Y-H. Relationship between Serum BDNF Levels and Depressive Mood in Subacute Stroke Patients: A Preliminary Study. International Journal of Molecular Sciences. 2018; 19(10):3131. https://doi.org/10.3390/ijms19103131
Chicago/Turabian StyleChang, Won Hyuk, Min A Shin, Ahee Lee, Heegoo Kim, and Yun-Hee Kim. 2018. "Relationship between Serum BDNF Levels and Depressive Mood in Subacute Stroke Patients: A Preliminary Study" International Journal of Molecular Sciences 19, no. 10: 3131. https://doi.org/10.3390/ijms19103131
APA StyleChang, W. H., Shin, M. A., Lee, A., Kim, H., & Kim, Y.-H. (2018). Relationship between Serum BDNF Levels and Depressive Mood in Subacute Stroke Patients: A Preliminary Study. International Journal of Molecular Sciences, 19(10), 3131. https://doi.org/10.3390/ijms19103131