
First Insights into Human Fingertip Regeneration by Echo-Doppler Imaging and Wound Microenvironment Assessment


 , ,
, ,
Abstract
:1. Introduction
2. Results
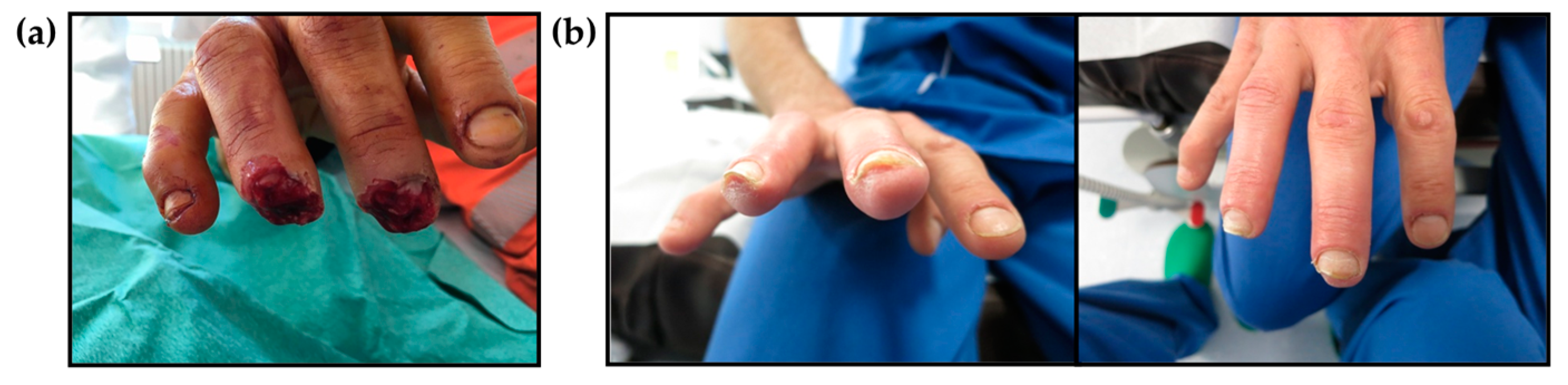
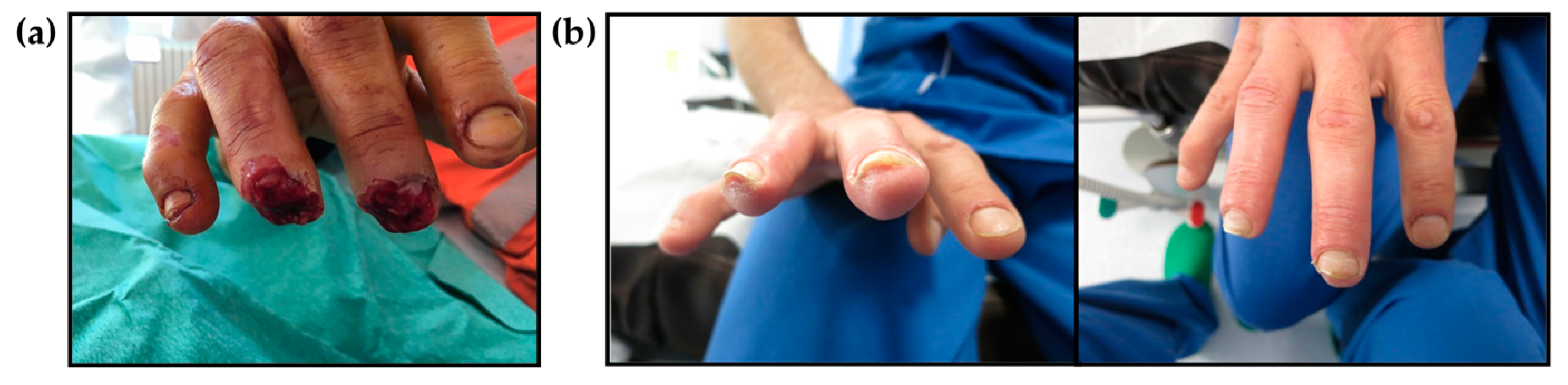
2.1. Clinical Evaluation of Regenerated Fingertips
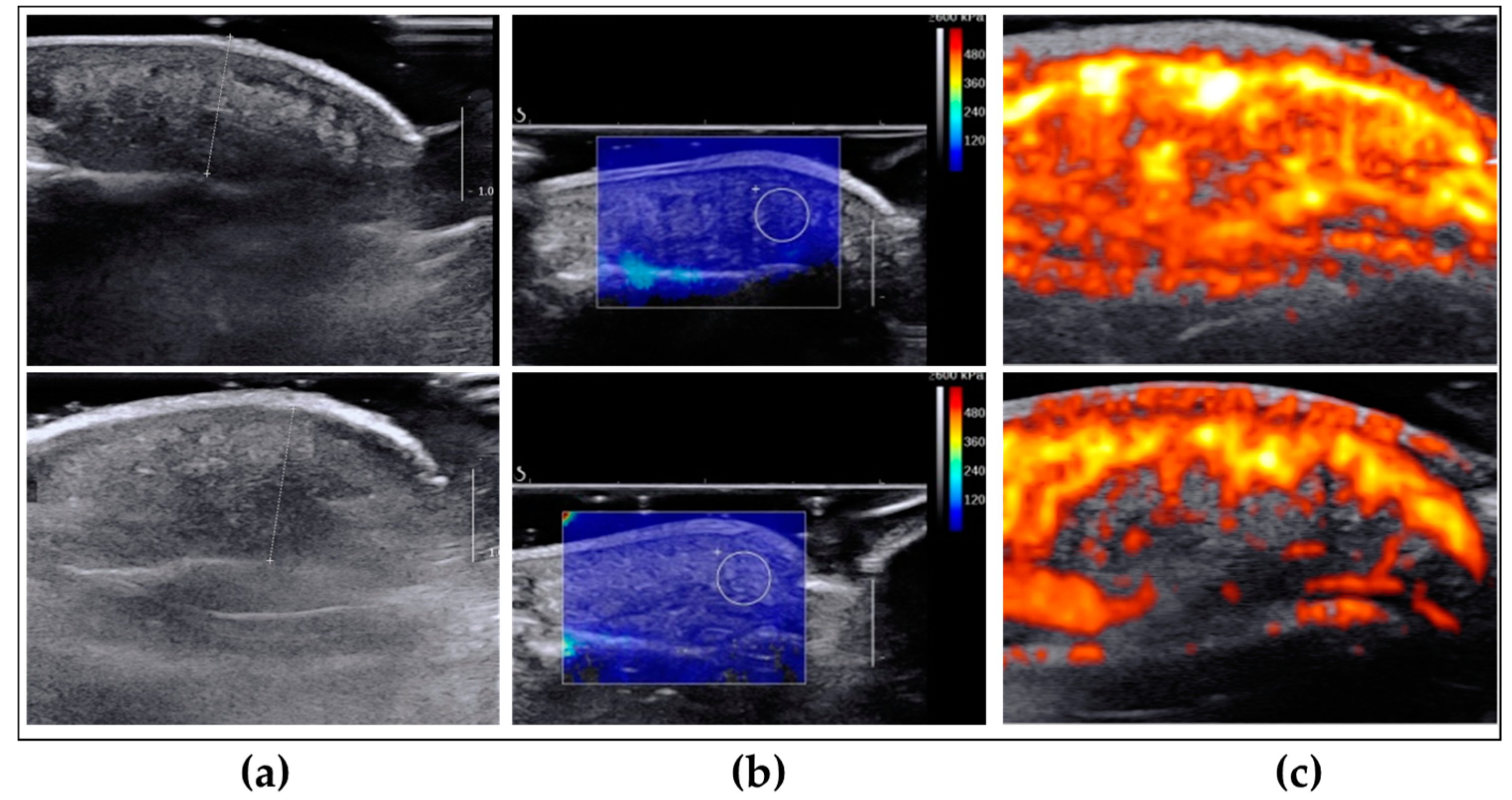
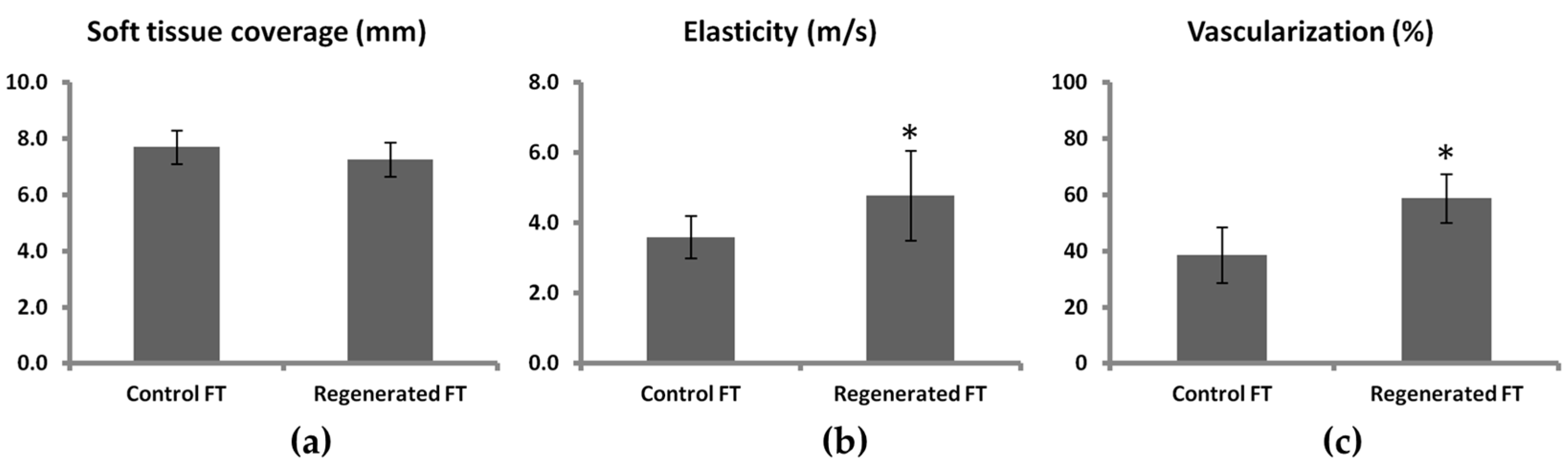
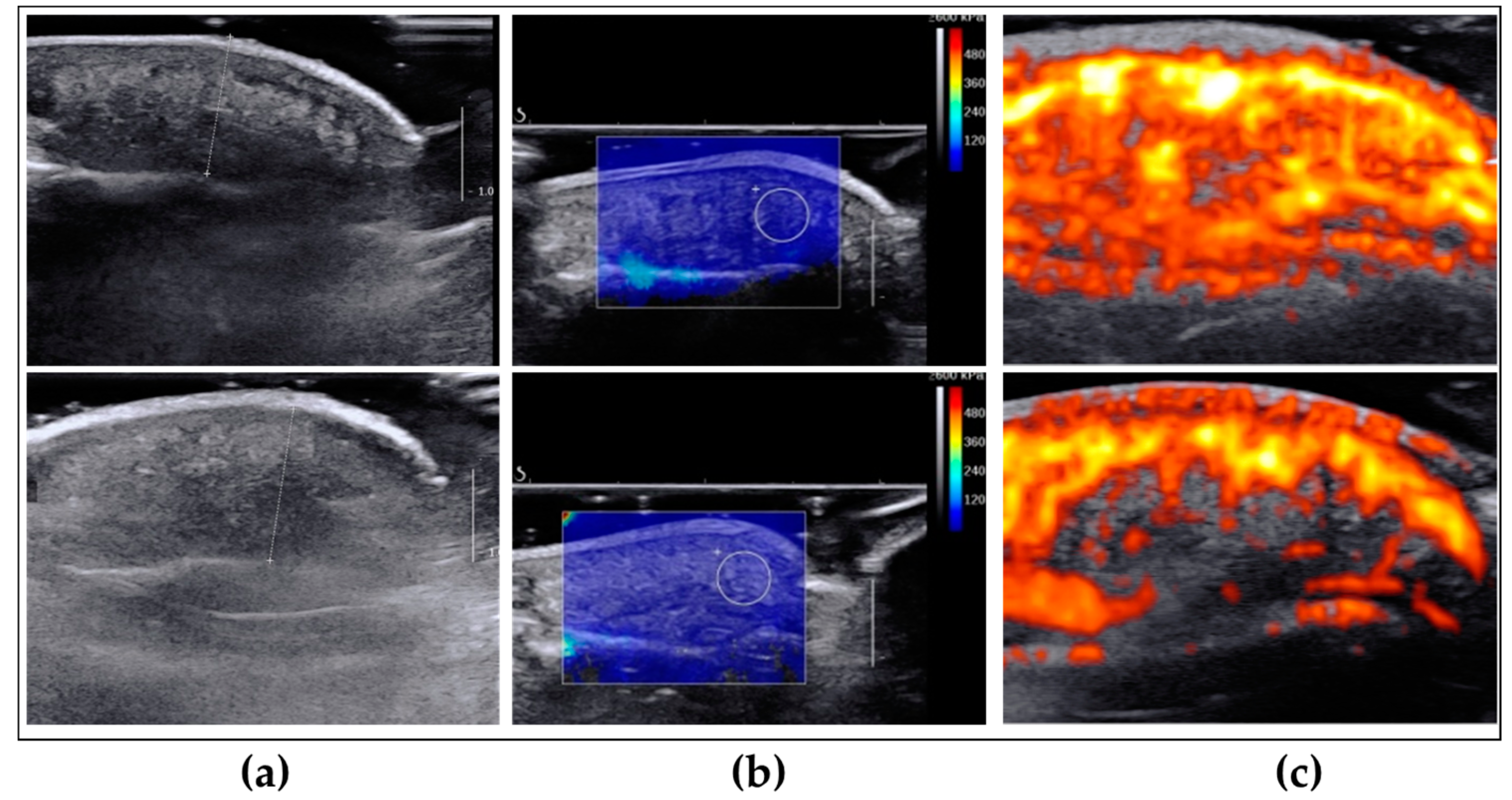
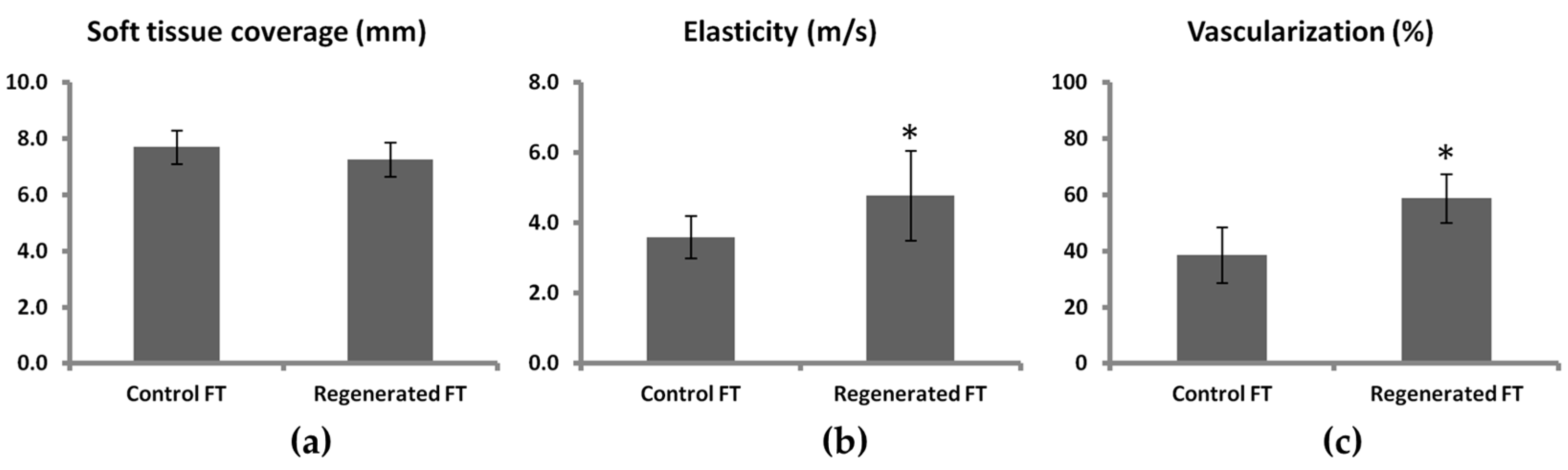
2.2. Evaluation of Morphological, Mechanical and Vascular Properties of Regenerated Fingertips
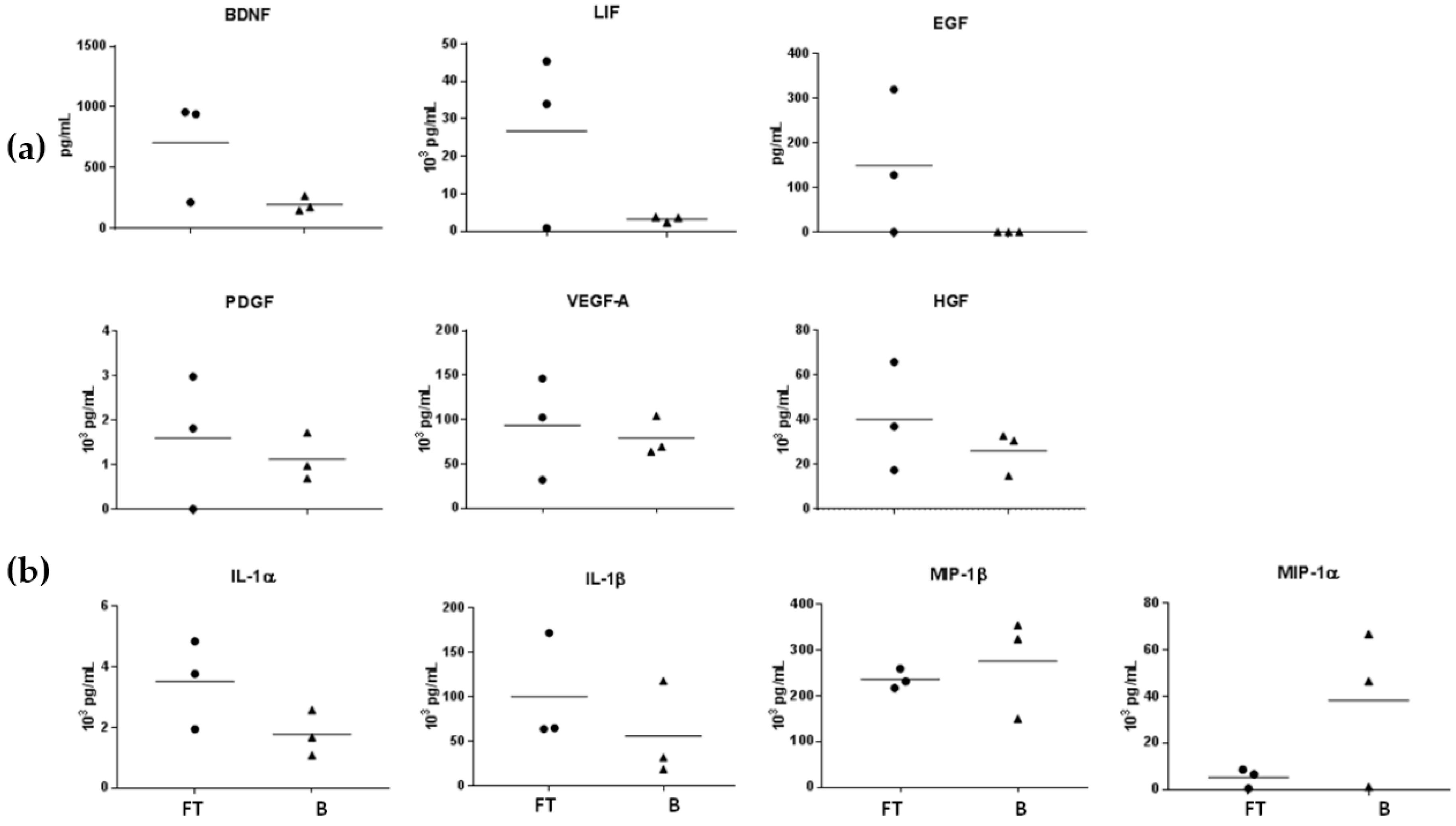
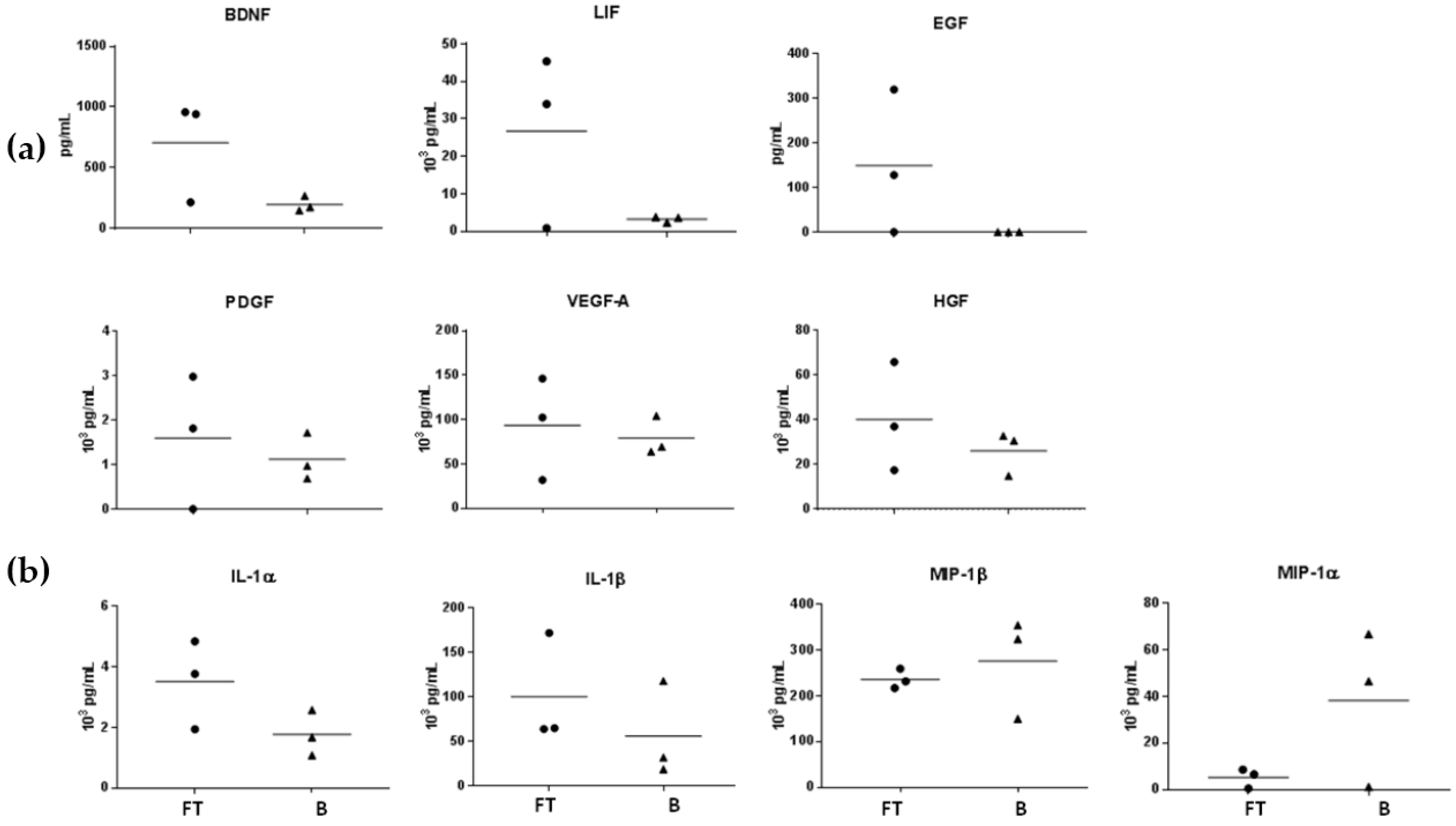
2.3. Regenerative Wound Microenvironment
3. Discussion
4. Materials and Methods
4.1. Ethics
4.2. Fingertip Exudate Collection and Analysis
4.3. Burn Wound Exudate Collection
4.4. Wound Exudate Immunoassay
4.5. Clinical Assessment of the Regenerated Fingertips (Two Point Discrimination, Force and Pain)
4.6. Power-Doppler and Elastography Assessment of Regenerated Fingertips
4.7. Image and Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| FGF-2 | Fibroblast Growth Factor 2 |
| SWE | Sear Wave Elastography |
| BDNF | Brain-derived Neurotrophic factor |
| PDGF | Platelet-Derived Growth Factor |
| VEGF-A | Vascular Endothelial Growth Factor A |
| NGF | Nerve Growth Factor |
| b-FGF | Basic Fibroblast Growth Factor |
| MIP | Macrophage Inflammatory Protein |
| LIF | Leukemia Inhibitory Factor |
| CNTF | Ciliary Neurotrophic Factor |
| HGF | Hepatocyte Growth Factor |
| EGF | Epidermal Growth Factor |
References
- Douglas, B.S. Conservative management of guillotine amputation of the finger in children. Aust. Paediatr. J. 1972, 8, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Illingworth, C.M. Trapped fingers and amputated finger tips in children. J. Pediatr. Surg. 1974, 9, 853–858. [Google Scholar] [CrossRef]
- Takeo, M.; Chou, W.C.; Sun, Q.; Lee, W.; Rabbani, P.; Loomis, C.; Taketo, M.M.; Ito, M. Wnt activation in nail epithelium couples nail growth to digit regeneration. Nature 2013, 499, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, H.; Ogino, H.; Stoick-Cooper, C.L.; Grainger, R.M.; Moon, R.T. Wnt/β-catenin signaling has an essential role in the initiation of limb regeneration. Dev. Biol. 2007, 306, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Yokoyama, S.; Fukuda, N.; Kidoya, H.; Huang, X.Y.; Naitoh, H.; Satoh, N.; Takakura, N. A novel approach for myocardial regeneration with educated cord blood cells cocultured with cells from brown adipose tissue. Biochem. Biophys. Res. Commun. 2007, 353, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Mullen, L.M.; Bryant, S.V.; Torok, M.A.; Blumberg, B.; Gardiner, D.M. Nerve dependency of regeneration: The role of distal-less and fgf signaling in amphibian limb regeneration. Development 1996, 122, 3487–3497. [Google Scholar] [PubMed]
- Poss, K.D. Advances in understanding tissue regenerative capacity and mechanisms in animals. Nat. Rev. Genet. 2010, 11, 710–722. [Google Scholar] [CrossRef] [PubMed]
- Vidal, P.; Dickson, M.G. Regeneration of the distal phalanx. A case report. J. Hand Surg. 1993, 18, 230–233. [Google Scholar] [CrossRef]
- Lee, L.P.; Lau, P.Y.; Chan, C.W. A simple and efficient treatment for fingertip injuries. J. Hand Surg. 1995, 20, 63–71. [Google Scholar] [CrossRef]
- Shieh, S.J.; Cheng, T.C. Regeneration and repair of human digits and limbs: Fact and fiction. Regeneration 2015, 2, 149–168. [Google Scholar] [CrossRef] [PubMed]
- Muneoka, K.; Allan, C.H.; Yang, X.; Lee, J.; Han, M. Mammalian regeneration and regenerative medicine. Birth Defects Res. C: Embryo Today 2008, 84, 265–280. [Google Scholar] [CrossRef] [PubMed]
- Werner, S.; Grose, R. Regulation of wound healing by growth factors and cytokines. Physiol. Rev. 2003, 83, 835–870. [Google Scholar] [PubMed]
- Heldin, C.H.; Westermark, B. Mechanism of action and in vivo role of platelet-derived growth factor. Physiol. Rev. 1999, 79, 1283–1316. [Google Scholar] [PubMed]
- Broadley, K.N.; Aquino, A.M.; Woodward, S.C.; Buckley-Sturrock, A.; Sato, Y.; Rifkin, D.B.; Davidson, J.M. Monospecific antibodies implicate basic fibroblast growth factor in normal wound repair. Lab. Investig. 1989, 61, 571–575. [Google Scholar] [PubMed]
- Xin, X.; Yang, S.; Ingle, G.; Zlot, C.; Rangell, L.; Kowalski, J.; Schwall, R.; Ferrara, N.; Gerritsen, M.E. Hepatocyte growth factor enhances vascular endothelial growth factor-induced angiogenesis in vitro and in vivo. Am. J. Pathol. 2001, 158, 1111–1120. [Google Scholar] [CrossRef]
- Tsou, R.; Fathke, C.; Wilson, L.; Wallace, K.; Gibran, N.; Isik, F. Retroviral delivery of dominant-negative vascular endothelial growth factor receptor type 2 to murine wounds inhibits wound angiogenesis. Wound Repair Regen. 2002, 10, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Howdieshell, T.R.; Callaway, D.; Webb, W.L.; Gaines, M.D.; Procter, C.D., Jr.; Sathyanarayana; Pollock, J.S.; Brock, T.L.; McNeil, P.L. Antibody neutralization of vascular endothelial growth factor inhibits wound granulation tissue formation. J. Surg. Res. 2001, 96, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Harsum, S.; Clarke, J.D.; Martin, P. A reciprocal relationship between cutaneous nerves and repairing skin wounds in the developing chick embryo. Dev. Biol. 2001, 238, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Apfel, S.C.; Arezzo, J.C.; Brownlee, M.; Federoff, H.; Kessler, J.A. Nerve growth factor administration protects against experimental diabetic sensory neuropathy. Brain Res. 1994, 634, 7–12. [Google Scholar] [CrossRef]
- DiPietro, L.A.; Burdick, M.; Low, Q.E.; Kunkel, S.L.; Strieter, R.M. Mip-1alpha as a critical macrophage chemoattractant in murine wound repair. J. Clin. Investig. 1998, 101, 1693–1698. [Google Scholar] [CrossRef] [PubMed]
- Gillitzer, R.; Goebeler, M. Chemokines in cutaneous wound healing. J. Leukoc. Biol. 2001, 69, 513–521. [Google Scholar] [PubMed]
- Hubner, G.; Brauchle, M.; Smola, H.; Madlener, M.; Fassler, R.; Werner, S. Differential regulation of pro-inflammatory cytokines during wound healing in normal and glucocorticoid-treated mice. Cytokine 1996, 8, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Johnston, A.P.; Yuzwa, S.A.; Carr, M.J.; Mahmud, N.; Storer, M.A.; Krause, M.P.; Jones, K.; Paul, S.; Kaplan, D.R.; Miller, F.D. Dedifferentiated schwann cell precursors secreting paracrine factors are required for regeneration of the mammalian digit tip. Cell Stem Cell 2016, 19, 433–448. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Yan, M.; Simkin, J.; Ketcham, P.D.; Leininger, E.; Han, M.; Muneoka, K. Angiogenesis is inhibitory for mammalian digit regeneration. Regeneration 2014, 1, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Godwin, J.W.; Pinto, A.R.; Rosenthal, N.A. Macrophages are required for adult salamander limb regeneration. Proc. Natl. Acad. Sci. USA 2013, 110, 9415–9420. [Google Scholar] [CrossRef] [PubMed]
- Rowan, M.P.; Cancio, L.C.; Elster, E.A.; Burmeister, D.M.; Rose, L.F.; Natesan, S.; Chan, R.K.; Christy, R.J.; Chung, K.K. Burn wound healing and treatment: Review and advancements. Crit. Care 2015, 19, 243. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Han, M.; Yan, M.; Lee, E.C.; Lee, J.; Muneoka, K. Bmp signaling induces digit regeneration in neonatal mice. Development 2010, 137, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Goss, R.J. Regeneration versus repair. In Wound Healing: Biochemical and Clinical Aspects; Cohen, I.K., Diegelman, R.F., Lindblad, W.J., Eds.; W.B. Saunders Co.: Philadelphia, PA, USA, 1992; pp. 20–39. [Google Scholar]
- Simkin, J.; Sammarco, M.C.; Dawson, L.A.; Schanes, P.P.; Yu, L.; Muneoka, K. The mammalian blastema: Regeneration at our fingertips. Regeneration 2015, 2, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, A.; Piatkowski, M.; Chen, M.; Kan, L.; Meng, Q.; Fan, H.; Osman, A.H.; Liu, Z.; Ledford, B.; He, J.Q. Superior angiogenesis facilitates digit regrowth in mrl/mpj mice compared to c57bl/6 mice. Biochem. Biophys. Res. Commun. 2016, 473, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Gohel, M.S.; Windhaber, R.A.; Tarlton, J.F.; Whyman, M.R.; Poskitt, K.R. The relationship between cytokine concentrations and wound healing in chronic venous ulceration. J. Vasc. Surg. 2008, 48, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Nissen, N.N.; Polverini, P.J.; Koch, A.E.; Volin, M.V.; Gamelli, R.L.; DiPietro, L.A. Vascular endothelial growth factor mediates angiogenic activity during the proliferative phase of wound healing. Am. J. Pathol. 1998, 152, 1445–1452. [Google Scholar] [PubMed]
- Lehoczky, J.A. Are fingernails are a key to unlocking the puzzle of mammalian limb regeneration? Exp. Dermatol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Mescher, A.L.; Neff, A.W.; King, M.W. Inflammation and immunity in organ regeneration. Dev. Comp. Immunol. 2017, 66, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Grow, M.; Neff, A.W.; Mescher, A.L.; King, M.W. Global analysis of gene expression in xenopus hindlimbs during stage-dependent complete and incomplete regeneration. Dev. Dyn. 2006, 235, 2667–2685. [Google Scholar] [CrossRef] [PubMed]
- King, M.W.; Neff, A.W.; Mescher, A.L. The developing xenopus limb as a model for studies on the balance between inflammation and regeneration. Anat. Rec. (Hoboken) 2012, 295, 1552–1561. [Google Scholar] [CrossRef] [PubMed]
- Fernando, W.A.; Leininger, E.; Simkin, J.; Li, N.; Malcom, C.A.; Sathyamoorthi, S.; Han, M.; Muneoka, K. Wound healing and blastema formation in regenerating digit tips of adult mice. Dev. Biol. 2011, 350, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Brockes, J.P. Nerve dependence in tissue, organ, and appendage regeneration. Trends Neurosci. 2012, 35, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Rinkevich, Y.; Montoro, D.T.; Muhonen, E.; Walmsley, G.G.; Lo, D.; Hasegawa, M.; Januszyk, M.; Connolly, A.J.; Weissman, I.L.; Longaker, M.T. Clonal analysis reveals nerve-dependent and independent roles on mammalian hind limb tissue maintenance and regeneration. Proc. Natl. Acad. Sci. USA 2014, 111, 9846–9851. [Google Scholar] [CrossRef] [PubMed]
- Rinkevich, Y.; Lindau, P.; Ueno, H.; Longaker, M.T.; Weissman, I.L. Germ-layer and lineage-restricted stem/progenitors regenerate the mouse digit tip. Nature 2011, 476, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Baudoin, J.; Jafari, P.; Meuli, J.; Applegate, L.A.; Raffoul, W. Topical negative pressure on burns: An innovative method for wound exudate collection. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1117. [Google Scholar] [CrossRef] [PubMed]
- Bercoff, J.; Tanter, M.; Fink, M. Supersonic shear imaging: A new technique for soft tissue elasticity mapping. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2004, 51, 396–409. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Amputated Finger/Hand | Two Points Discrimination | Pinch Test | Pain (0–5) |
|---|---|---|---|---|---|
| Patient 1 | 30 | Middle/left | ≤4 mm on both fingers | 2 kg/2 kg | 0/0 |
| Patient 2 | 45 | Middle/right | ≤4 mm on both fingers | 2.5 kg/2 kg | 0/0 |
| Patient 3 | 76 | Index/right | ≤4 mm on both fingers | Not obtained | 0/0 |
| Patient 4 | 47 | Middle/left | ≤4 mm on both fingers | Not obtained | 0/0 |
| Patient 5 | 52 | Middle/right | ≤4 mm on both fingers | 1.5 kg/2.5 kg | 1/0 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jafari, P.; Muller, C.; Grognuz, A.; Applegate, L.A.; Raffoul, W.; Di Summa, P.G.; Durand, S. First Insights into Human Fingertip Regeneration by Echo-Doppler Imaging and Wound Microenvironment Assessment. Int. J. Mol. Sci. 2017, 18, 1054. https://doi.org/10.3390/ijms18051054
Jafari P, Muller C, Grognuz A, Applegate LA, Raffoul W, Di Summa PG, Durand S. First Insights into Human Fingertip Regeneration by Echo-Doppler Imaging and Wound Microenvironment Assessment. International Journal of Molecular Sciences. 2017; 18(5):1054. https://doi.org/10.3390/ijms18051054
Chicago/Turabian StyleJafari, Paris, Camillo Muller, Anthony Grognuz, Lee Ann Applegate, Wassim Raffoul, Pietro G. Di Summa, and Sébastien Durand. 2017. "First Insights into Human Fingertip Regeneration by Echo-Doppler Imaging and Wound Microenvironment Assessment" International Journal of Molecular Sciences 18, no. 5: 1054. https://doi.org/10.3390/ijms18051054
APA StyleJafari, P., Muller, C., Grognuz, A., Applegate, L. A., Raffoul, W., Di Summa, P. G., & Durand, S. (2017). First Insights into Human Fingertip Regeneration by Echo-Doppler Imaging and Wound Microenvironment Assessment. International Journal of Molecular Sciences, 18(5), 1054. https://doi.org/10.3390/ijms18051054