
Multi-Layer Electrospun Membrane Mimicking Tendon Sheath for Prevention of Tendon Adhesions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
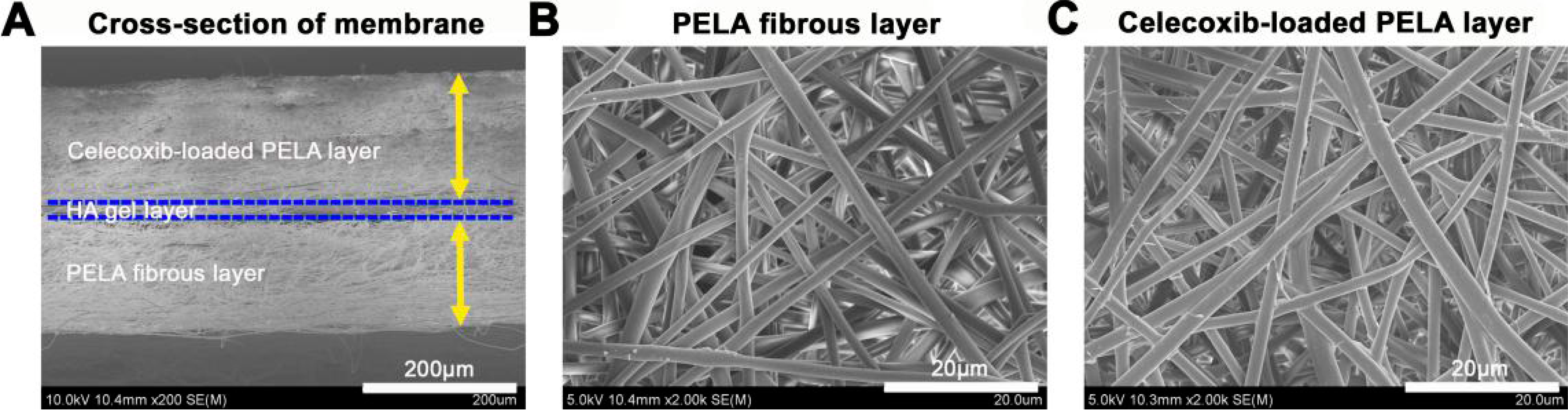
2.1. Characterization of Multi-Layer Electrospun Fibrous Membrane
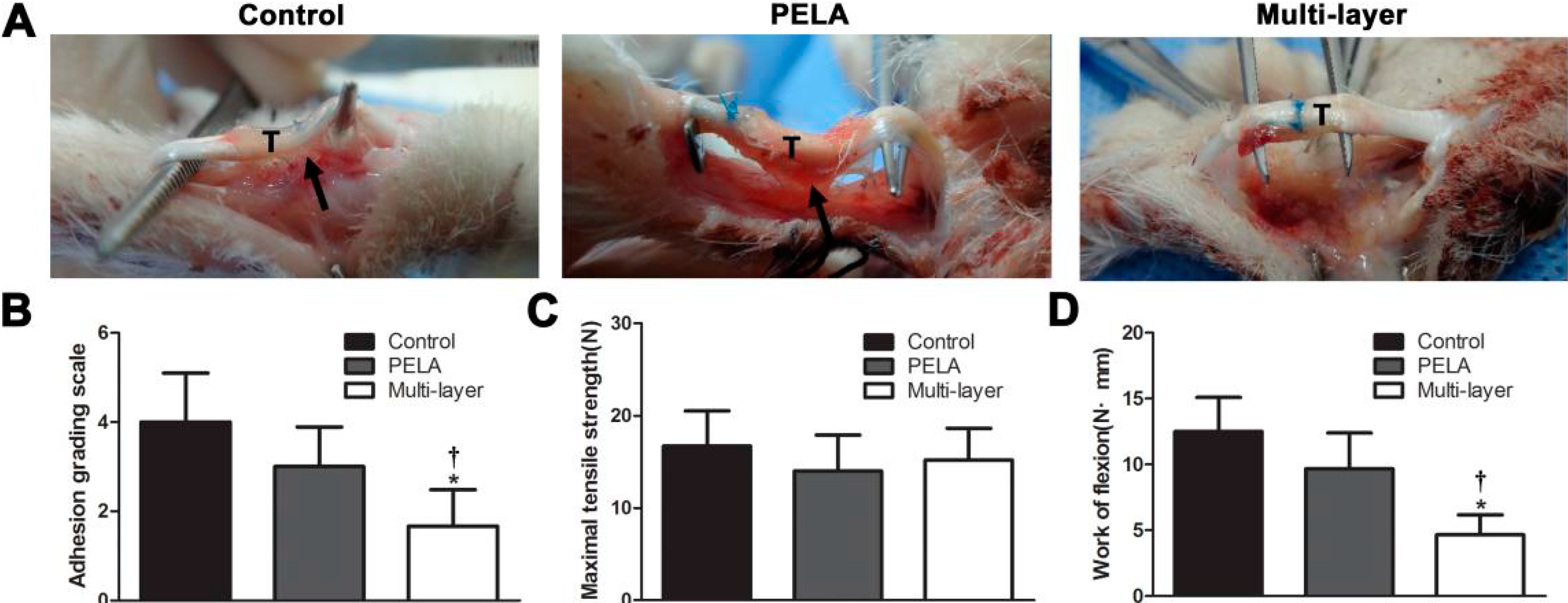
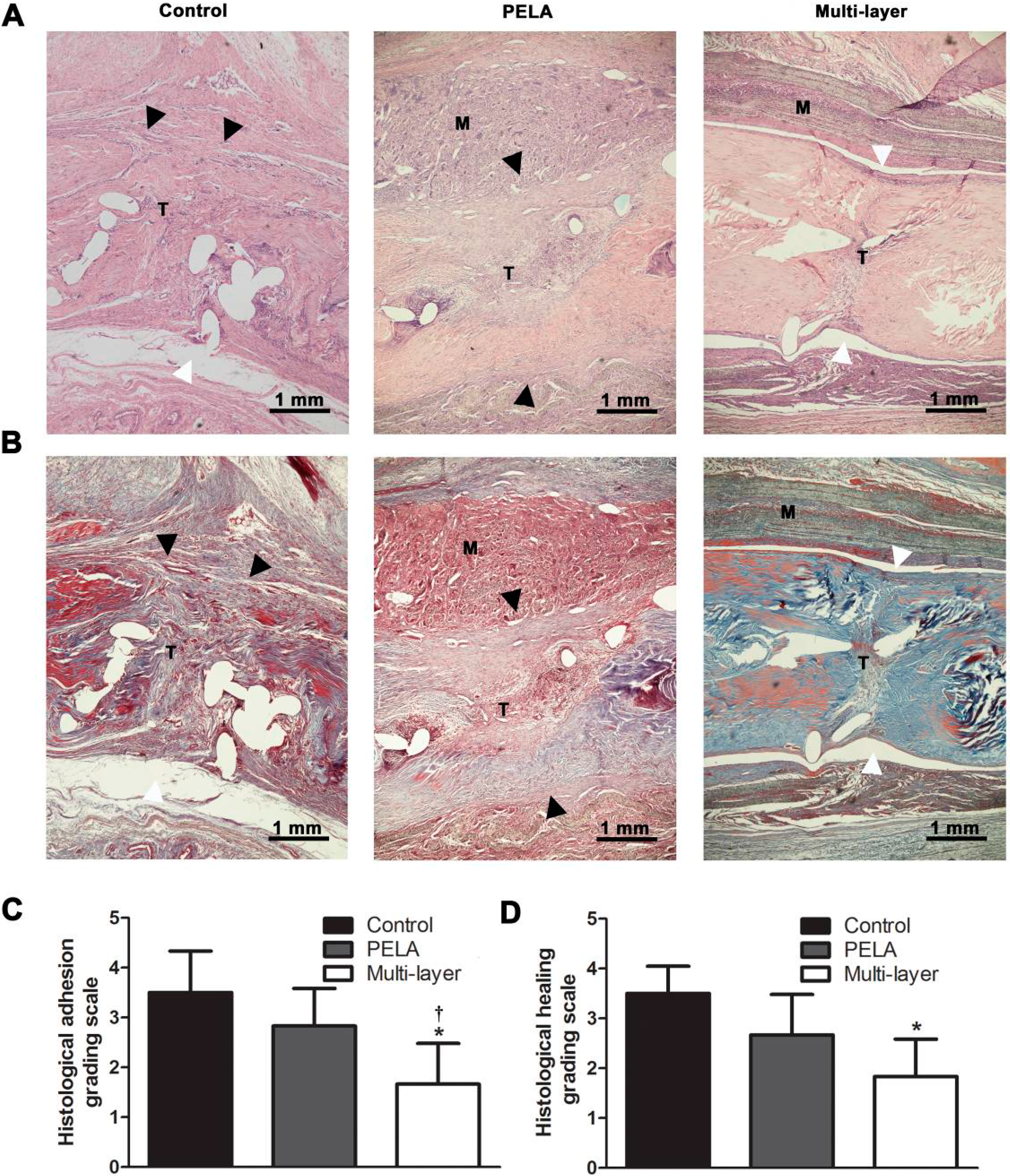
2.2. In Vivo Animal Study

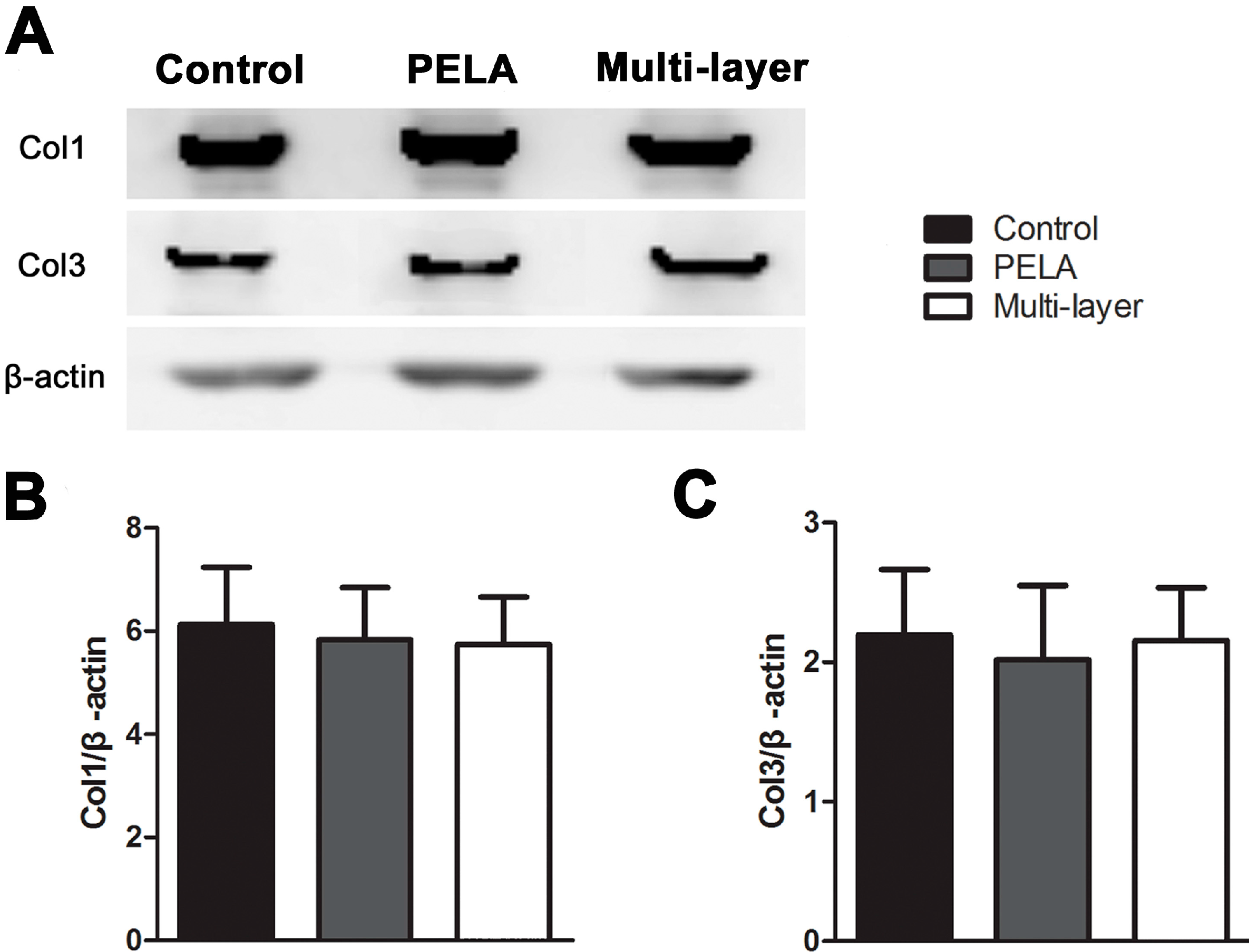
2.3. Collagen Expression in Repair Site
2.4. Discussions

3. Experimental Section
3.1. Materials
3.2. Electrospinning of Nanofibrous Membranes
3.3. Preliminary Animal Study
3.4. Macroscopic Evaluation
3.5. Histological Evaluation
3.6. Biomechanical Evaluation
3.7. Western Blot Analysis
3.8. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kannus, P. Structure of the tendon connective tissue. Scand. J. Med. Sci. Sports 2000, 10, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Maffulli, N. Biology of tendon injury: Healing, modeling and remodeling. J. Musculoskelet. Neuronal Interact. 2006, 6, 181–190. [Google Scholar] [PubMed]
- Peterson, W.W.; Manske, P.R.; Dunlap, J.; Horwitz, D.S.; Kahn, B. Effect of various methods of restoring flexor sheath integrity on the formation of adhesions after tendon injury. J. Hand Surg. 1990, 15, 48–56. [Google Scholar] [CrossRef]
- Isik, S.; Ozturk, S.; Gurses, S.; Yetmez, M.; Guler, M.M.; Selmanpakoglu, N.; Gunhan, O. Prevention of restrictive adhesions in primary tendon repair by ha-membrane: Experimental research in chickens. Br. J. Plast. Surg. 1999, 52, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Akasaka, T.; Nishida, J.; Araki, S.; Shimamura, T.; Amadio, P.C.; An, K.N. Hyaluronic acid diminishes the resistance to excursion after flexor tendon repair: An in vitro biomechanical study. J. Biomech. 2005, 38, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Momose, T.; Amadio, P.C.; Sun, Y.L.; Zhao, C.; Zobitz, M.E.; Harrington, J.R.; An, K.N. Surface modification of extrasynovial tendon by chemically modified hyaluronic acid coating. J. Biomed. Mater. Res. 2002, 59, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Sungur, N.; Uysal, A.; Kocer, U.; Karaaslan, O.; Gumus, M.; Sokmensuer, L.K.; Sokmensuer, C. Prevention of tendon adhesions by the reconstruction of the tendon sheath with solvent dehydrated bovine pericard: An experimental study. J. Trauma 2006, 61, 1467–1472. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Toguchida, J.; Oka, M. Development of polyvinyl alcohol-hydrogel (PVA-H) shields with a high water content for tendon injury repair. J. Hand Surg. Br. 2001, 26, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Zhao, J.; Dong, S.; Huangfu, X.; Li, B.; Yang, H.; Cui, W. Biological augmentation of rotator cuff repair using bFGF-loaded electrospun poly(lactide-co-glycolide) fibrous membranes. Int. J. Nanomed. 2014, 9, 2373–2385. [Google Scholar] [CrossRef]
- Liu, S.; Zhao, J.; Ruan, H.; Tang, T.; Liu, G.; Yu, D.; Cui, W.; Fan, C. Biomimetic sheath membrane via electrospinning for antiadhesion of repaired tendon. Biomacromolecules 2012, 13, 3611–3619. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Hu, C.; Li, F.; Li, X.J.; Cui, W.; Fan, C. Prevention of peritendinous adhesions with electrospun ibuprofen-loaded poly(l-lactic acid)-polyethylene glycol fibrous membranes. Tissue Eng. A 2013, 19, 529–537. [Google Scholar] [CrossRef]
- Yang, D.J.; Chen, F.; Xiong, Z.C.; Xiong, C.D.; Wang, Y.Z. Tissue anti-adhesion potential of biodegradable PELA electrospun membranes. Acta Biomater. 2009, 5, 2467–2474. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Liu, S.; Ouyang, Y.; Fan, C.; Wang, T.; Zhang, C.; Zeng, B.; Chai, Y.; Wang, X. Effect of celecoxib on proliferation, collagen expression, ERK1/2 and SMAD2/3 phosphorylation in NIH/3T3 fibroblasts. Eur. J. Pharmacol. 2012, 678, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Zhao, X.; Chen, S.; Pan, G.; Song, J.; He, N.; Li, F.; Cui, W.; Fan, C. Down-regulating ERK1/2 and SMAD2/3 phosphorylation by physical barrier of celecoxib-loaded electrospun fibrous membranes prevents tendon adhesions. Biomaterials 2014, 35, 9920–9929. [Google Scholar] [CrossRef] [PubMed]
- Ishiyama, N.; Moro, T.; Ohe, T.; Miura, T.; Ishihara, K.; Konno, T.; Ohyama, T.; Kimura, M.; Kyomoto, M.; Saito, T.; et al. Reduction of peritendinous adhesions by hydrogel containing biocompatible phospholipid polymer mpc for tendon repair. J. Bone Jt. Surg. Am. 2011, 93, 142–149. [Google Scholar]
- Liu, Y.; Skardal, A.; Shu, X.Z.; Prestwich, G.D. Prevention of peritendinous adhesions using a hyaluronan-derived hydrogel film following partial-thickness flexor tendon injury. J. Orthop. Res. 2008, 26, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Ozboluk, S.; Ozkan, Y.; Ozturk, A.; Gul, N.; Ozdemir, R.M.; Yanik, K. The effects of human amniotic membrane and periosteal autograft on tendon healing: Experimental study in rabbits. J. Hand Surg. Eur. 2010, 35, 262–268. [Google Scholar] [CrossRef]
- Sharma, P.; Maffulli, N. Tendon injury and tendinopathy: Healing and repair. J. Bone Jt. Surg. Am. 2005, 87, 187–202. [Google Scholar] [CrossRef]
- Ni, M.; Rui, Y.F.; Tan, Q.; Liu, Y.; Xu, L.L.; Chan, K.M.; Wang, Y.; Li, G. Engineered scaffold-free tendon tissue produced by tendon-derived stem cells. Biomaterials 2013, 34, 2024–2037. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, A.M.; Yam, A.; Chin, S.I.; Heong, T.S.; Helvacioglu, F.; Tan, A. Synovial cell culture and tissue engineering of a tendon synovial cell biomembrane. J. Biomed. Mater. Res. A 2008, 84, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Baymurat, A.C.; Ozturk, A.M.; Yetkin, H.; Ergun, M.A.; Helvacioglu, F.; Ozkizilcik, A.; Tuzlakoglu, K.; Sener, E.E.; Erdogan, D. Bio-engineered synovial membrane to prevent tendon adhesions in rabbit flexor tendon model. J. Biomed. Mater. Res. A 2015, 103, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Gelberman, R.H.; Vande Berg, J.S.; Lundborg, G.N.; Akeson, W.H. Flexor tendon healing and restoration of the gliding surface. An ultrastructural study in dogs. J. Bone Jt. Surg. Am. 1983, 65, 70–80. [Google Scholar]
- Cashman, J.; Burt, H.M.; Springate, C.; Gleave, J.; Jackson, J.K. Camptothecin-loaded films for the prevention of postsurgical adhesions. Inflamm. Res. 2004, 53, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Ishiyama, N.; Moro, T.; Ishihara, K.; Ohe, T.; Miura, T.; Konno, T.; Ohyama, T.; Kimura, M.; Kyomoto, M.; Nakamura, K.; et al. The prevention of peritendinous adhesions by a phospholipid polymer hydrogel formed in situ by spontaneous intermolecular interactions. Biomaterials 2010, 31, 4009–4016. [Google Scholar]
- Gudemez, E.; Eksioglu, F.; Korkusuz, P.; Asan, E.; Gursel, I.; Hasirci, V. Chondroitin sulfate-coated polyhydroxyethyl methacrylate membrane prevents adhesion in full-thickness tendon tears of rabbits. J. Hand Surg. 2002, 27, 293–306. [Google Scholar] [CrossRef]
- Siddiqi, N.A.; Hamada, Y.; Ide, T.; Akamatsu, N. Effects of hydroxyapatite and alumina sheaths on postoperative peritendinous adhesions in chickens. J. Appl. Biomater. 1995, 6, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.B.; Shi, D.; Zhang, Q.G. Biomechanical and histologic evaluation of tendon sheath management. J. Hand Surg. 1996, 21, 900–908. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, S.; Yan, H.; Fan, D.; Song, J.; Fan, C. Multi-Layer Electrospun Membrane Mimicking Tendon Sheath for Prevention of Tendon Adhesions. Int. J. Mol. Sci. 2015, 16, 6932-6944. https://doi.org/10.3390/ijms16046932
Jiang S, Yan H, Fan D, Song J, Fan C. Multi-Layer Electrospun Membrane Mimicking Tendon Sheath for Prevention of Tendon Adhesions. International Journal of Molecular Sciences. 2015; 16(4):6932-6944. https://doi.org/10.3390/ijms16046932
Chicago/Turabian StyleJiang, Shichao, Hede Yan, Dapeng Fan, Jialin Song, and Cunyi Fan. 2015. "Multi-Layer Electrospun Membrane Mimicking Tendon Sheath for Prevention of Tendon Adhesions" International Journal of Molecular Sciences 16, no. 4: 6932-6944. https://doi.org/10.3390/ijms16046932
APA StyleJiang, S., Yan, H., Fan, D., Song, J., & Fan, C. (2015). Multi-Layer Electrospun Membrane Mimicking Tendon Sheath for Prevention of Tendon Adhesions. International Journal of Molecular Sciences, 16(4), 6932-6944. https://doi.org/10.3390/ijms16046932