
The in Vitro Antimicrobial Efficacy of PDT against Periodontopathogenic Bacteria



Abstract
:
1. Introduction
2. Results and Discussion
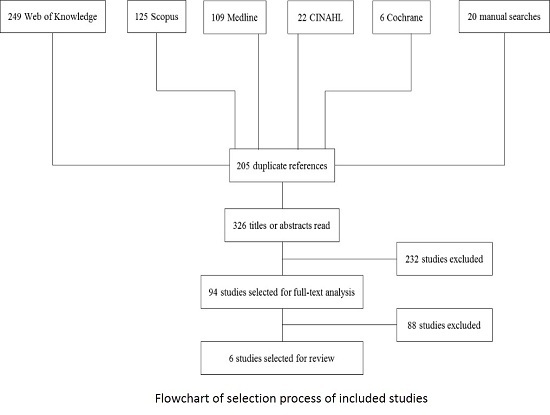
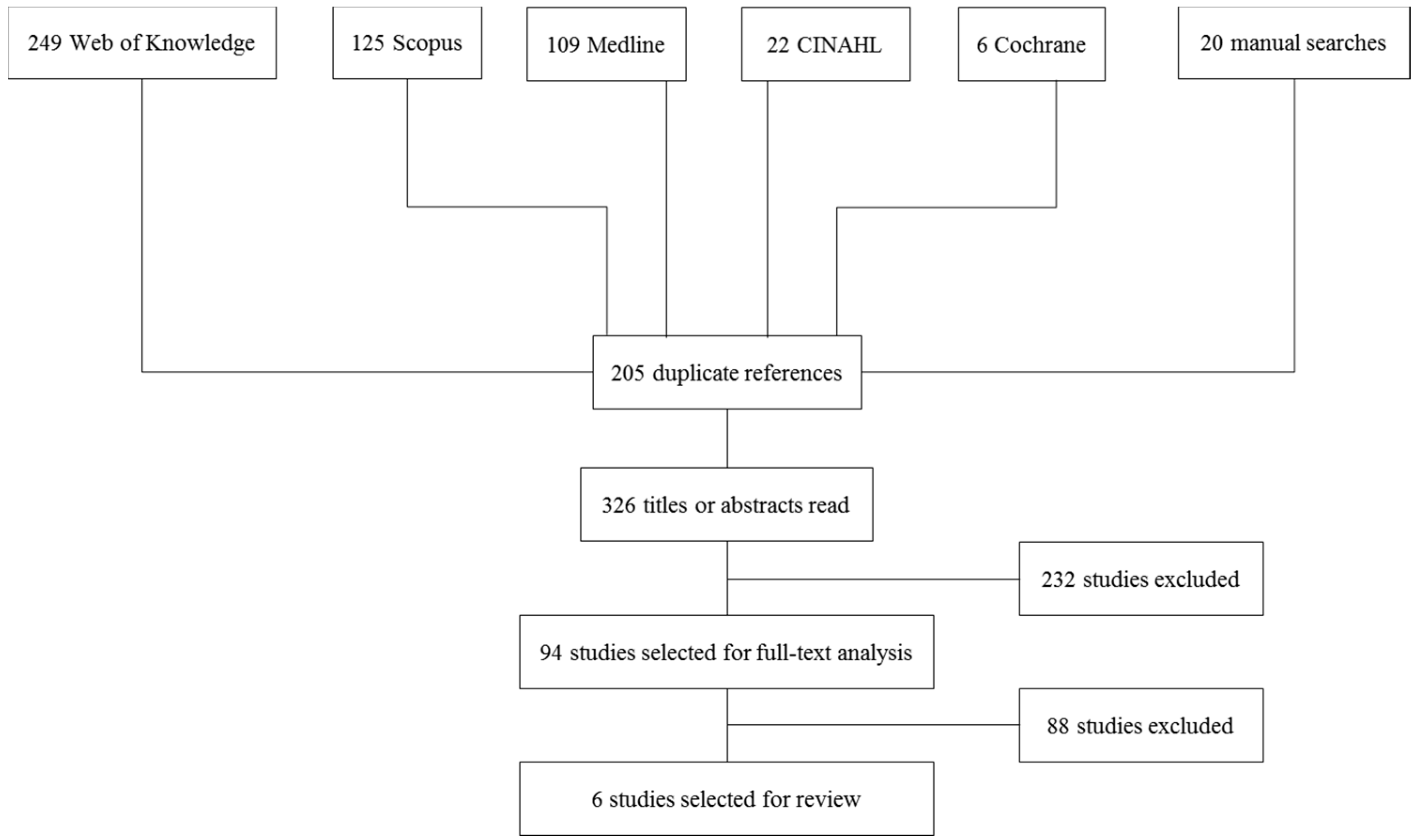
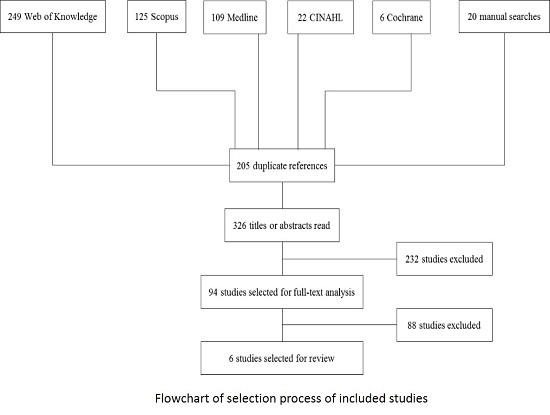
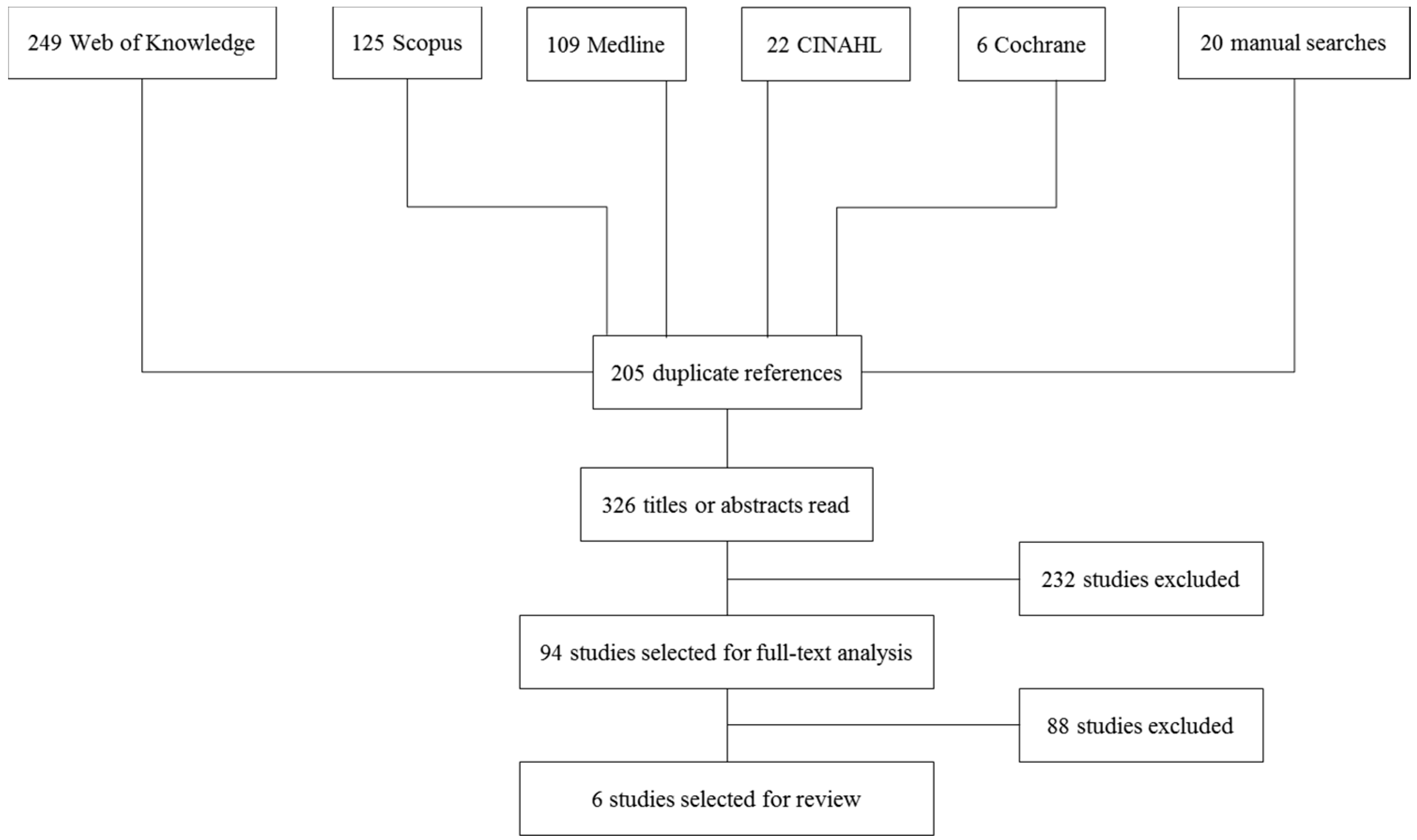
2.1. Search and Screening
2.2. Description of Studies
2.3. Antimicrobial Effects of Photodynamic Therapy (PDT) on Porphyromonas Gingivalis
2.4. Antimicrobial Effects of Photodynamic Therapy (PDT) on Aggregatibacter Actinomycetemcomitans
2.5. Antimicrobial Effects of Photodynamic Therapy (PDT) on Fusobacterium Nucleatum

{kind=link}
{kind=link}
| Reference | Photo-Sensitizer | PDT | Control 1 | Control 2 | Control 3 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Light Source | Bacterial Strain | Mean | Conditions | Mean | Conditions | Mean | Conditions | Mean | ||
| Braham et al. [8] | MB 0.01% at dilution 0.03 | Diode laser λ: 670 nm P: 150 mW | ATCC 33277 | log10 reduction 3.8 ± 1.3 * | N/A | N/A | N/A | N/A | photosensitizer only | no effect |
| Chan and Lai [9] | MB 0.01% | He–Ne laser λ: 632.8 nm P: 30 mW He: 6.4 J/cm2 | ATCC 33277 | Viable count CFU 16 ± 5 | negative control no photosensitizer no light exposure | Viable count CFU 129 ± 7 | light only | Viable count CFU 132 ± 8 | photosensitizer only | Viable count CFU 108 ± 12 |
| Diode laser λ: 665 nm P: 100 mW He: 21.2 J/cm2 | Viable count CFU 1 ± 0.3 | Viable count CFU 117 ± 8 | Viable count CFU 67 ± 8 | Viable count CFU 111 ± 13 | ||||||
| Diode laser λ: 830 nm P: 100 mW He: 21.2 J/cm2 | Viable count CFU 58 ± 6 | Viable count CFU 138 ± 8 | Viable count CFU 81 ± 6 | Viable count CFU 126 ± 4 | ||||||
| Eick et al. [13] | TB 0.1 mg/mL | LED lamp λ: 625–635 nm E: 2 W/cm2 | ATCC 33277 | Viable count CFU (8.17 ± 1.01) log10 | negative control no photosensitizer no light exposure | Viable count CFU (9.73 ± 0.46) log10 | light only | Viable count CFU (9.59 ± 0.64) log10 | photosensitizer only | Viable count CFU (9.08 ± 0.25) log10 |
| M5-1-2 | Viable count CFU (2.73 ± 3.16) log10 | Viable count CFU (9.73 ± 0.65) log10 | Viable count CFU (9.71 ± 0.48) log10 | Viable count CFU (5.22 ± 4.03) log10 | ||||||
| Street et al. [10] | MB 0.01% | Diode laser λ: 670 nm He: 9.4 J/cm2 | planktonic ATCC 33277 | log10 reduction 6.8 ± 0.7 | N/A | N/A | N/A | N/A | N/A | N/A |
| MB 0.01% | Diode laser λ: 670 nm He: 6 J/cm2 | biofilm ATCC 33277 | log10 reduction 4.5 ± 1.2 | N/A | N/A | N/A | N/A | N/A | N/A | |
| Reference | Photo-Sensitizer | Light Source | Bacterial Strain | PDT | Control 1 | Control 2 | Control 3 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Conditions | Mean | Conditions | Mean | Conditions | Mean | ||||
| Chan and Lai [9] | MB 0.01% | He-Ne laser λ: 632.8 nm P: 30 mW He: 6.4 J/cm2 | ATCC 29522 | Viable count CFU 17 ± 6 | negative control no photosensitizer no light exposure | Viable count CFU 136 ± 12 | light only | Viable count CFU 116 ± 5 | photosensitizer only | Viable count CFU 141 ± 10 |
| Diode laser λ: 665nm P: 100 mW He: 21.2 J/cm2 | Viable count CFU 6 ± 3 | Viable count CFU 132 ± 12 | Viable count CFU 88 ± 5 | Viable count CFU 137 ± 11 | ||||||
| Diode laser λ: 830 nm P: 100 mW He: 21.2 J/cm2 | Viable count CFU 76 ± 5 | Viable count CFU 125 ± 11 | Viable count CFU 65 ± 10 | Viable count CFU 128 ± 8 | ||||||
| Eick et al. [13] | TB 0.1 g/mL | LED lamp λ: 625–635 nm E: 2 W/cm2 | Y4 | Viable count CFU 7.47 ± 1.24 log10 | negative control no photosensitizer no light exposure | Viable count CFU 9.27 ± 0.14 log10 | light only | Viable count CFU 9.36 ± 0.08 log10 | photosensitizer only | Viable count CFU 8.7 ± 0.41 log10 |
| J7 | Viable count CFU 4.11 ± 2.77 log10 | Viable count CFU 6.77 ± 0.78 log10 | Viable count CFU 6.86 ± 0.8 log10 | Viable count CFU 5.73 ± 0.21 log10 | ||||||
| Goulart et al. [11] | MB 0.5 µmol/L | Dental photo-polymerizer λ: 400–500 nm E: 350–500 mW/cm2 He: 0.65 J/cm2 | planktonic JP2 | 30 min incubation 15% cell death | N/A | N/A | N/A | N/A | photosensitizer only ≤0.1 µmol/L 10 min incubation 30 min incubation | 0% reduction |
| MB 1 µmol/L | Dental photo-polymerizer λ: 400–500 nm E: 350–500 mW/cm2 He: 0.65 J/cm2 | planktonic JP2 | 30 min incubation 25% cell death | N/A | N/A | N/A | N/A | photosensitizer only 10 min incubation 30 min incubation | 19% reduction * 25% reduction * | |
| MB 10 µmol/L | N/A | planktonic JP2 | N/A | N/A | N/A | N/A | N/A | photosensitizer only 10 min incubation 30 min incubation | 23% reduction * 31% reduction * | |
| MB 20 µmol/L | N/A | N/A | N/A | N/A | N/A | N/A | photosensitizer only incubation time unclear | 50% reduction | ||
| MB 0.5 µmol/L | Dental photo-polymerizer λ: 400–500 nm E: 350–500 mW/cm2 He: 0.65 J/cm2 | biofilm JP2 | 30 min incubation 73% reduction of absorbance * | N/A | N/A | N/A | N/A | photosensitizer only 30 min incubation | 73% reduction of absorbance * | |
| MB 1 µmol/L | biofilm JP2 | 30 min incubation 58% reduction of absorbance * | N/A | N/A | N/A | N/A | photosensitizer only 30 min incubation | 60% reduction of absorbance * | ||
| Street et al. [10] | MB 0.01% | Diode laser λ: 670 nm He: 9.4 J/cm2 | planktonic ATCC 33384 | log10 reduction 1.9 ± 0.6 | N/A | N/A | N/A | N/A | N/A | N/A |
| Diode laser λ: 670 nm He: 6 J/cm2 | biofilm ATCC 43717 | log10 reduction 4.9 ± 1.4 | N/A | N/A | N/A | N/A | N/A | N/A | ||
| Alvarenga et al. [12] | MB 100 µM | L: Diode laser λ: 660 nm P: 100 mW He: 15 J/cm2 | ATCC 29523 | log10 reduction 0.3 | negative control no photosensitizer no light exposure | (cfu/mL) 8.87 ± 0.34 log10 | light only | (cfu/mL) 8.13 ± 0.67 | photosensitizer only | (cfu/mL) 8.47 ± 0.06 |
| Reference | Photosensitizer | Light Source | Bacterial Strain | PDT | Control 1 | Control 2 | Control 3 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Conditions | Mean | Conditions | Mean | Conditions | Mean | ||||
| Chan and Lai [9] | MB 0.01% | He-Ne laser λ: 632.8 nm; P: 30 mW; He: 6.4 J/cm2 | ATCC 23726 | Viable count CFU 19 ± 3 | negative control no photosensitizer no light exposure | Viable count CFU 117 ± 9 | light only no photosensitizer | Viable count CFU 113 ± 6 | photosensitizer only no light | Viable count CFU 112 ± 9 |
| Diode laser λ: 665 nm; P: 100 mW He: 21.2 J/cm2 | Viable count CFU 4 ± 2 | Viable count CFU 106 ± 14 | Viable count CFU 65 ± 9 | Viable count CFU 96 ± 6 | ||||||
| Diode laser λ: 830 nm; P: 100 mW He: 21.2 J/cm2 | Viable count CFU 61 ± 4 | Viable count CFU 121 ± 9 | Viable count CFU 67 ± 11 | Viable count CFU 117 ± 9 | ||||||
| Street et al. [10] | MB 0.01% | Diode laser λ: 670 nm He: 9.4 J/cm2 | planktonic ATCC 25586 | log10 reduction 5.2 ± 0.6 | N/A | N/A | N/A | N/A | N/A | N/A |
| Diode laser λ: 670 nm He: 6 J/cm2 | biofilm ATCC 25586 | log10 reduction 3.4 ± 1.1 | N/A | N/A | N/A | N/A | N/A | N/A | ||
| Reference | Bacteria Investigated | PDT | P.g. | A.a. | F.n. | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Photosensitizer | Light Source | Reduction in % | Log10 Reduction | Reduction in % | Log10 Reduction | Reduction in % | Log10 Reduction | |||
| Braham et al. [8] | P.g. | MB 0.01% at dilution 0.03 | Diode laser λ: 670 nm; P: 150 mW | 99.98 | 3.8 * | N/A | N/A | N/A | N/A | |
| Chan and Lai [9] | P.g. A.a. F.n. | MB 0.01% | He–Ne laser λ: 632.8 nm; P: 30 mW; He: 6.4 J/cm2 | 90.7 | 1.03 | 87.5 | 0.9 | 83.76 | 0.79 | |
| Diode laser λ: 665 nm; P: 100 mW; He: 21.2 J/cm2 | 99.15 | 2.07 | 95.45 | 1.3 | 96.23 | 1.42 | ||||
| Diode laser λ: 830 nm; P: 100 mW; He: 21.2 J/cm2 | 57.97 | 0.38 | 39.2 | 0.21 | 49.59 | 0.3 | ||||
| Eick et al. [13] | P.g. A.a. | ATCC 33277 Y4 | TB 0.1 mg/mL | LED lamp λ: 625-635 nm; E: 2 W/cm2 | 97.25 | 1.56 | 98.42 | 1.8 | N/A | N/A |
| M5-1-2 J7 | LED lamp λ: 625-635 nm; E: 2 W/cm2 | 99.99 | 7 | 99.78 | 2.66 | N/A | N/A | |||
| Street et al. [10] | P.g. A.a. F.n. | planktonic | MB 0.01% | Diode laser λ: 670 nm; He: 9.4 J/cm2 | 100 | 6.8 | 98.74 | 1.9 | 99.99 | 5.2 |
| P.g. A.a. F.n. | biofilm | Diode laser λ: 670 nm; He: 6 J/cm2 | 100 | 4.5 | 100 | 4.9 | 99.96 | 3.4 | ||
| Alvarenga et al. [12] | A.a. | MB 100 µM | L: Diode laser λ: 660 nm; P: 100 mW; He: 15 J/cm2 | N/A | N/A | 50 | 0.3 | N/A | N/A | |
| Goulart et al. [11] | A.a. | MB 0.5 µmol/L | Dental photopolymerizer λ: 400–500 nm; E: 350–500 mW/cm2 He: 0.65 J/cm2 | N/A | N/A | 15 | 0.07 | N/A | N/A | |
| MB 1 µmol/L | Dental photopolymerizer λ: 400–500 nm; E: 350–500 mW/cm2 He: 0.65 J/cm2 | N/A | N/A | 25 | 0.12 | N/A | N/A | |||
2.6. Discussion
3. Experimental Section
3.1. Search Strategy
3.2. Eligibility Criteria for Studies
3.3. Outcome Measures
3.4. Study Selection
3.5. Analysis of the Results
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Teles, R.P.; Haffajee, A.D.; Socransky, S.S. Microbiological goals of periodontal therapy. Periodontology 2006, 42, 180–218. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, S.A.; Robertson, P.B. Calculus removal by scaling/root planing with and without surgical access. J. Periodontol. 1987, 58, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Mongardini, C.; Pauwels, M.; Bollen, C.M.; van Eldere, J.; van Steenberghe, D. One stage full- versus partial-mouth disinfection in the treatment of chronic adult or generalized early-onset periodontitis. Ii. Long-term impact on microbial load. J. Periodontol. 1999, 70, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Soukos, N.S.; Ximenez-Fyvie, L.A.; Hamblin, M.R.; Socransky, S.S.; Hasan, T. Targeted antimicrobial photochemotherapy. Antimicrob. Agents Chemother. 1998, 42, 2595–2601. [Google Scholar] [PubMed]
- Sharman, W.M.; Allen, C.M.; van Lier, J.E. Photodynamic therapeutics: Basic principles and clinical applications. Drug Discov. Today 1999, 4, 507–517. [Google Scholar] [CrossRef]
- Meisel, P.; Kocher, T. Photodynamic therapy for periodontal diseases: State of the art. J. Photochem. Photobiol. B 2005, 79, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Muller, P.; Guggenheim, B.; Schmidlin, P.R. Efficacy of gasiform ozone and photodynamic therapy on a multispecies oral biofilm in vitro. Eur. J. Oral Sci. 2007, 115, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Braham, P.; Herron, C.; Street, C.; Darveau, R. Antimicrobial photodynamic therapy may promote periodontal healing through multiple mechanisms. J. Periodontol. 2009, 80, 1790–1798. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.; Lai, C.H. Bactericidal effects of different laser wavelengths on periodontopathic germs in photodynamic therapy. Lasers Med. Sci. 2003, 18, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Street, C.N.; Pedigo, L.A.; Loebel, N.G. Energy dose parameters affect antimicrobial photodynamic therapy-mediated eradication of periopathogenic biofilm and planktonic cultures. Photomed. Laser Surg. 2010, 28 (Suppl. S1), S61–S66. [Google Scholar] [CrossRef] [PubMed]
- Goulart Rde, C.; Thedei, G., Jr.; Souza, S.L.; Tedesco, A.C.; Ciancaglini, P. Comparative study of methylene blue and erythrosine dyes employed in photodynamic therapy for inactivation of planktonic and biofilm-cultivated aggregatibacter actinomycetemcomitans. Photomed. Laser Surg. 2010, 28 (Suppl. S1), S85–S90. [Google Scholar] [PubMed]
- Alvarenga, L.H.; Prates, R.A.; Yoshimura, T.M.; Kato, I.T.; Suzuki, L.C.; Ribeiro, M.S.; Ferreira, L.R.; Pereira, S.A.; Martinez, E.F.; Saba-Chujfi, E. Aggregatibacter actinomycetemcomitans biofilm can be inactivated by methylene blue-mediated photodynamic therapy. Photodiagn. Photodyn. Ther. 2015, 12, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.; Markauskaite, G.; Nietzsche, S.; Laugisch, O.; Salvi, G.E.; Sculean, A. Effect of photoactivated disinfection with a light-emitting diode on bacterial species and biofilms associated with periodontitis and peri-implantitis. Photodiagn. Photodyn. Ther. 2013, 10, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Rajesh, S.; Koshi, E.; Philip, K.; Mohan, A. Antimicrobial photodynamic therapy: An overview. J. Indian Soc. Periodontol. 2011, 15, 323–327. [Google Scholar] [PubMed]
- Soukos, N.S.; Goodson, J.M. Photodynamic therapy in the control of oral biofilms. Periodontology 2011, 55, 143–166. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.; Dobson, J.; Harvey, W. Sensitization of oral bacteria to killing by low-power laser radiation. Curr. Microbiol. 1992, 25, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.; Dobson, J. Lethal photosensitization of oral anaerobic bacteria. Clin. Infect. Dis. 1993, 16 (Suppl. S4), S414–S415. [Google Scholar] [CrossRef] [PubMed]
- Usacheva, M.N.; Teichert, M.C.; Biel, M.A. Comparison of the methylene blue and toluidine blue photobactericidal efficacy against gram-positive and gram-negative microorganisms. Lasers Surg. Med. 2001, 29, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Fontana, C.R.; Abernethy, A.D.; Som, S.; Ruggiero, K.; Doucette, S.; Marcantonio, R.C.; Boussios, C.I.; Kent, R.; Goodson, J.M.; Tanner, A.C.; et al. The antibacterial effect of photodynamic therapy in dental plaque-derived biofilms. J. Periodontal Res. 2009, 44, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K. Riddle of biofilm resistance. Antimicrob. Agents Chemother. 2001, 45, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Tegos, G.P.; Hamblin, M.R. Phenothiazinium antimicrobial photosensitizers are substrates of bacterial multidrug resistance pumps. Antimicrob. Agents Chemother. 2006, 50, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.R.; Allison, D.G.; Gilbert, P. Resistance of bacterial biofilms to antibiotics: A growth-rate related effect? J. Antimicrob. Chemother. 1988, 22, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Palmer, R.J., Jr. Supragingival and subgingival plaque: Paradigm of biofilms. Compend. Contin. Educ. Dent. 2010, 31, 104–106. [Google Scholar] [PubMed]
- Auschill, T.M.; Hellwig, E.; Sculean, A.; Hein, N.; Arweiler, N.B. Impact of the intraoral location on the rate of biofilm growth. Clin. Oral Investig. 2004, 8, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Al-Ahmad, A.; Wunder, A.; Auschill, T.M.; Follo, M.; Braun, G.; Hellwig, E.; Arweiler, N.B. The in vivo dynamics of streptococcus spp., actinomyces naeslundii, fusobacterium nucleatum and veillonella spp. in dental plaque biofilm as analysed by five-colour multiplex fluorescence in situ hybridization. J. Med. Microbiol. 2007, 56, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Graziani, F.; Gatto, R.; Monaco, A. Adjunctive photodynamic therapy to non-surgical treatment of chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2013, 40, 514–526. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A. Photodynamic therapy as an adjunctive treatment for chronic periodontitis: A meta-analysis. Lasers Med. Sci. 2010, 25, 605–613. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haag, P.A.; Steiger-Ronay, V.; Schmidlin, P.R. The in Vitro Antimicrobial Efficacy of PDT against Periodontopathogenic Bacteria. Int. J. Mol. Sci. 2015, 16, 27327-27338. https://doi.org/10.3390/ijms161126027
Haag PA, Steiger-Ronay V, Schmidlin PR. The in Vitro Antimicrobial Efficacy of PDT against Periodontopathogenic Bacteria. International Journal of Molecular Sciences. 2015; 16(11):27327-27338. https://doi.org/10.3390/ijms161126027
Chicago/Turabian StyleHaag, Philippe A., Valerie Steiger-Ronay, and Patrick R. Schmidlin. 2015. "The in Vitro Antimicrobial Efficacy of PDT against Periodontopathogenic Bacteria" International Journal of Molecular Sciences 16, no. 11: 27327-27338. https://doi.org/10.3390/ijms161126027
APA StyleHaag, P. A., Steiger-Ronay, V., & Schmidlin, P. R. (2015). The in Vitro Antimicrobial Efficacy of PDT against Periodontopathogenic Bacteria. International Journal of Molecular Sciences, 16(11), 27327-27338. https://doi.org/10.3390/ijms161126027