Identification of Apolipoprotein C-I as a Potential Wilms’ Tumor Marker after Excluding Inflammatory Factors

Abstract
:
1. Introduction
2. Results
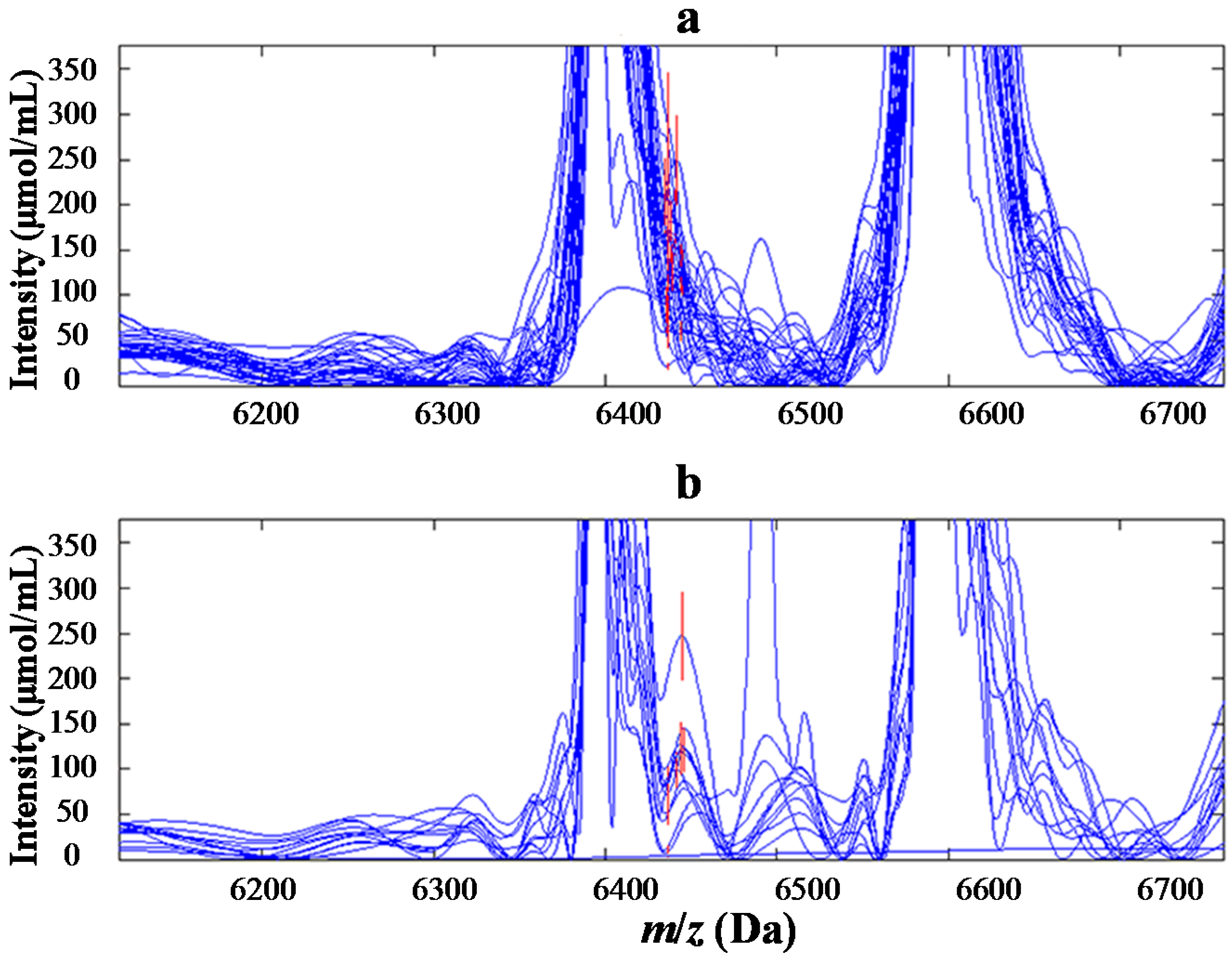
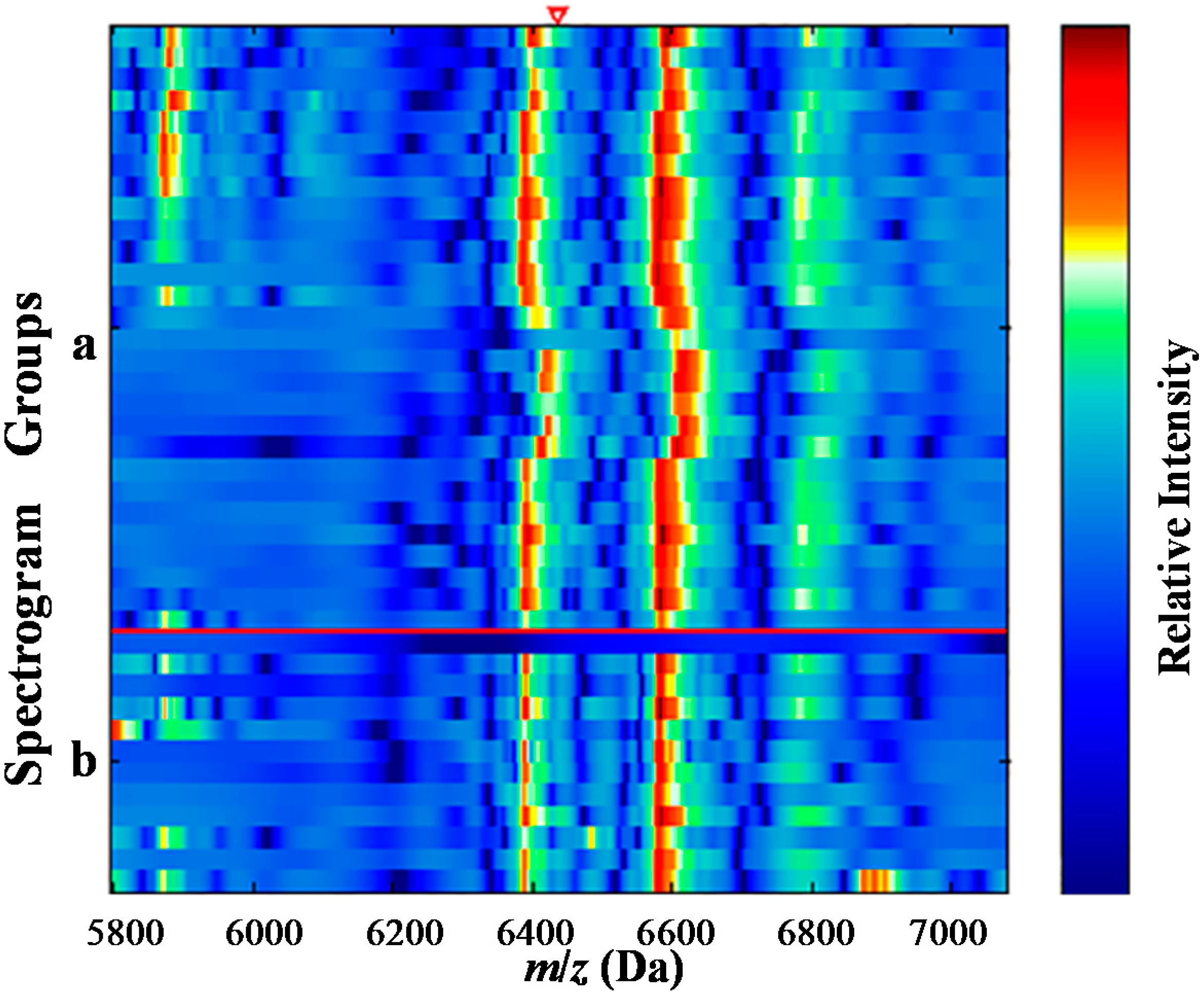
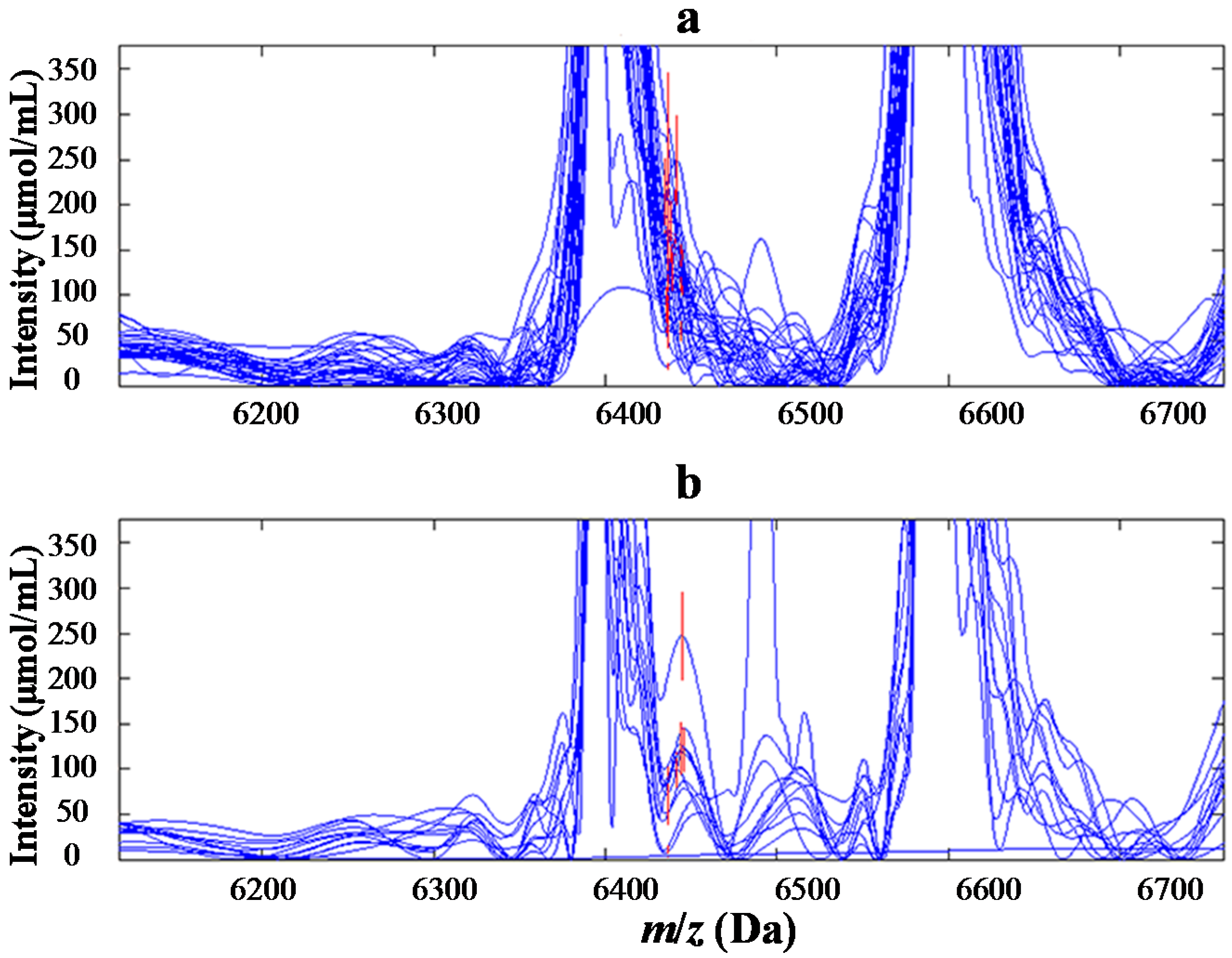
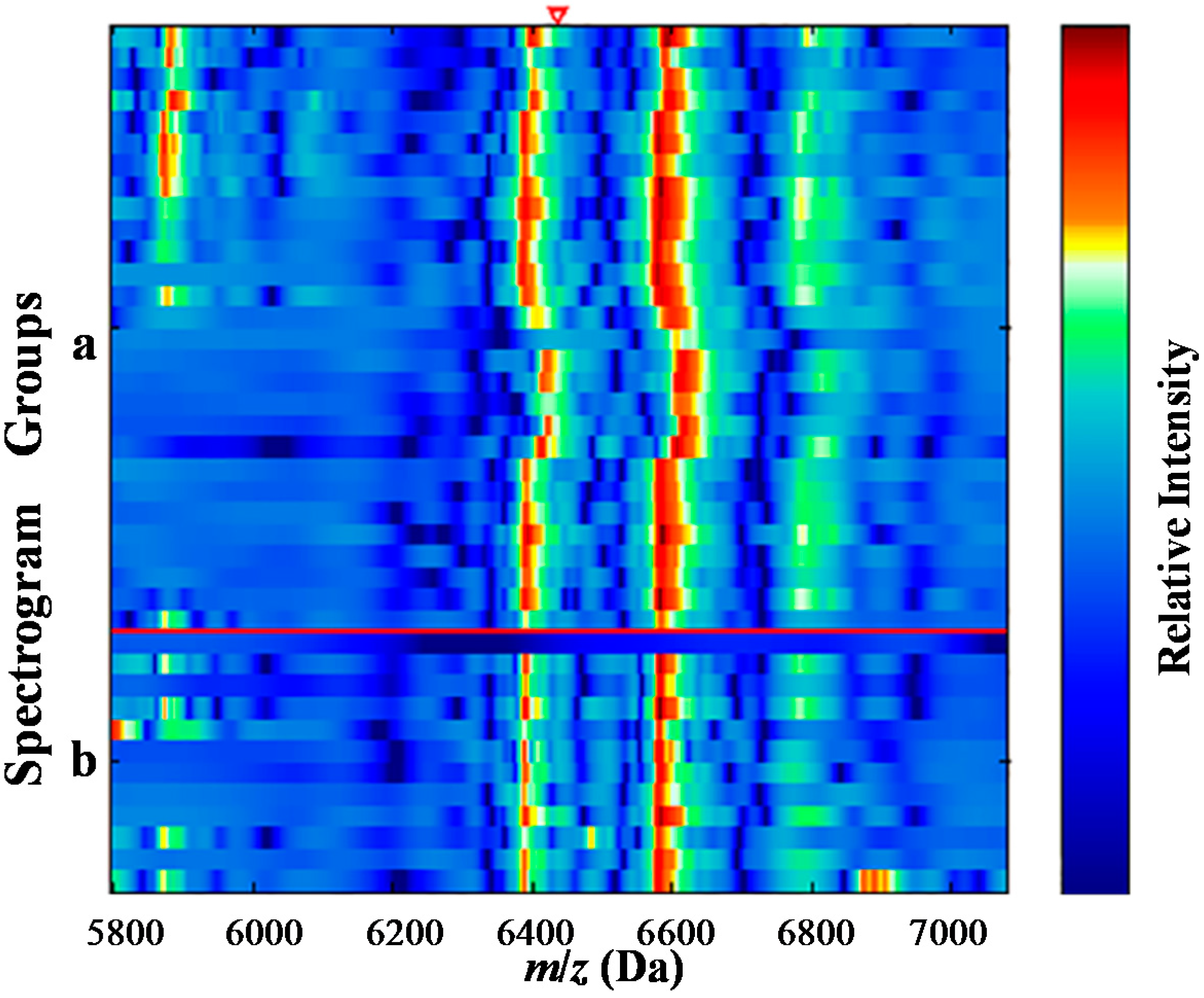
2.1. Determination of the Target Proteins

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| m/z (Da) | Serum of Cases (mean ± SD) | Serum of Controls (mean ± SD) | p |
|---|---|---|---|
| 6438 | 83.3129 ± 68.6291 | 142.928 ± 66.7952 | 0.008254 |
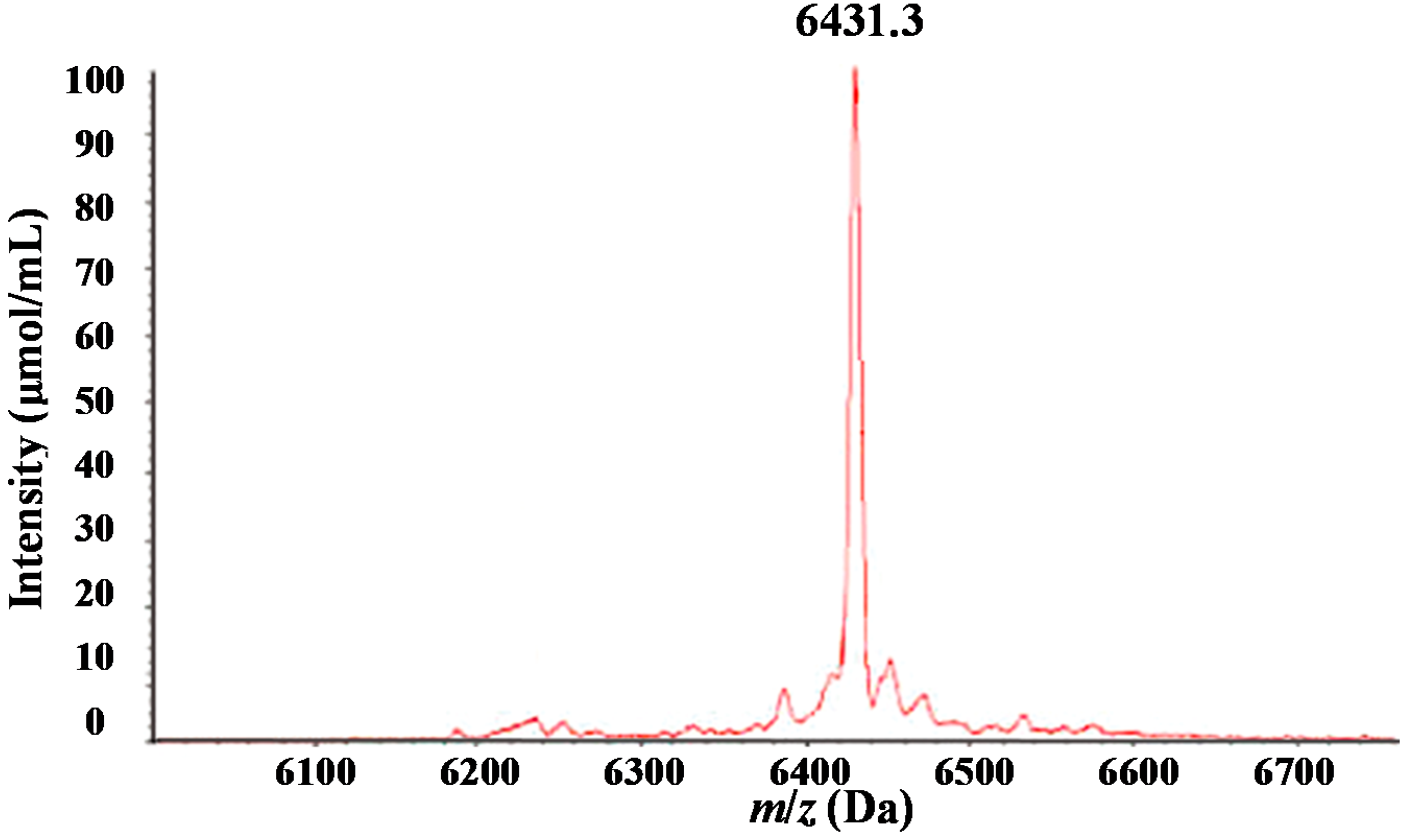
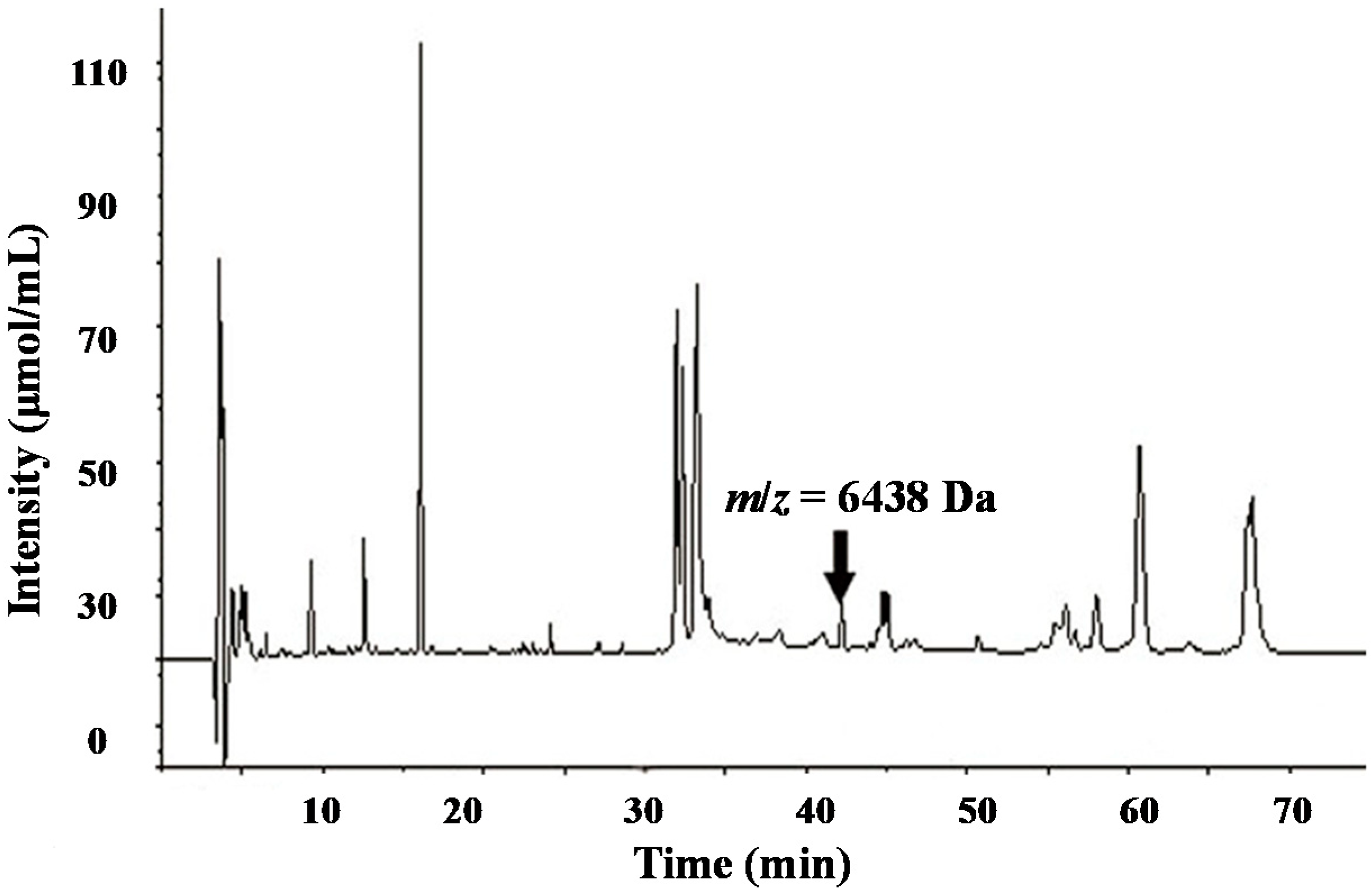
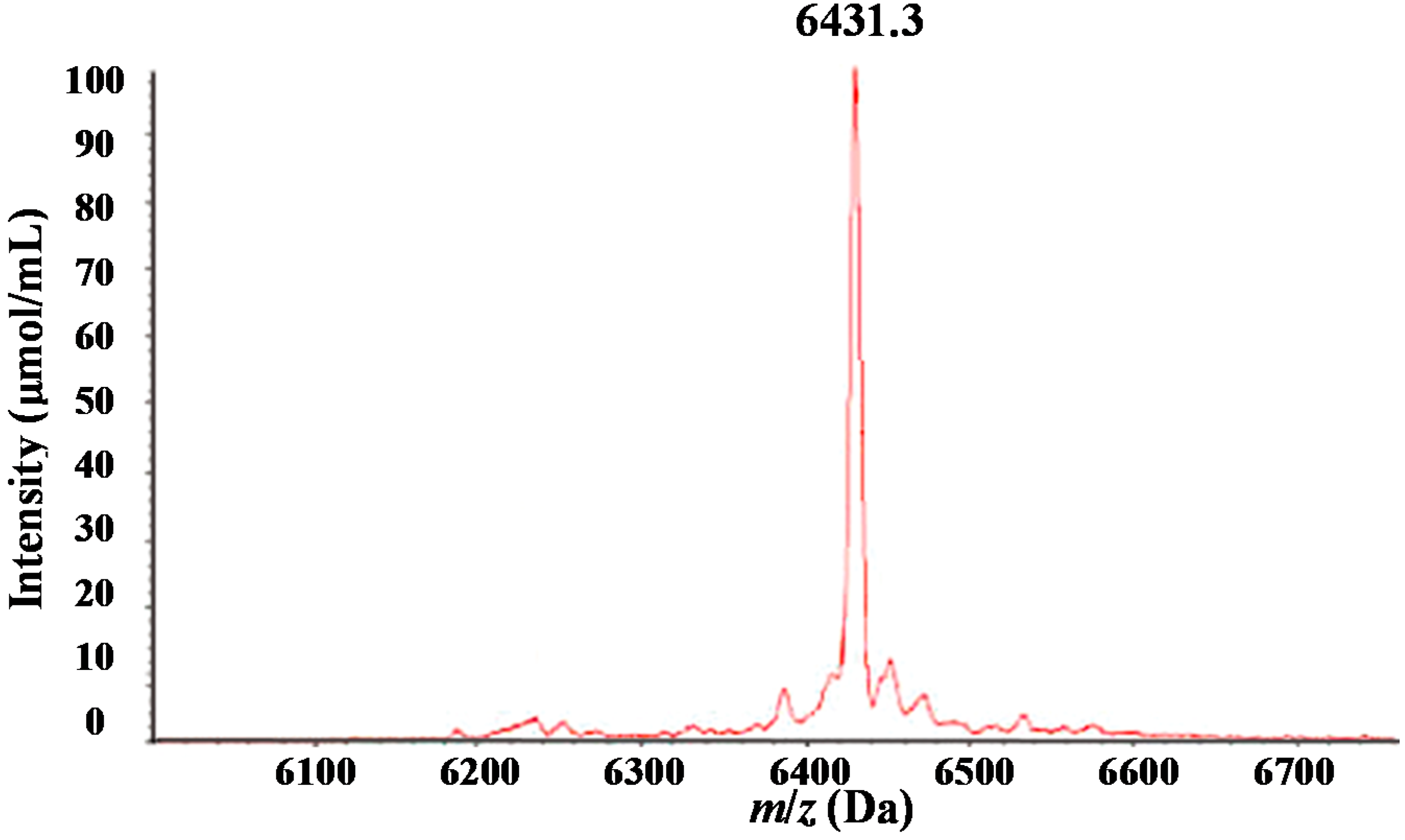
2.2. Purification of the Target Serum Protein Using High-Pressure Liquid Chromatography and Matrix-Assisted Laser Desorption Ionization/Time-of-Flight Mass Spectrometry
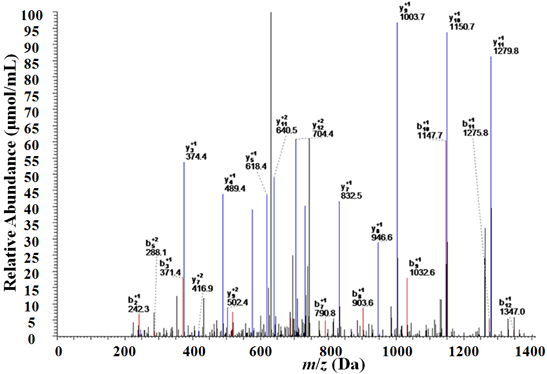
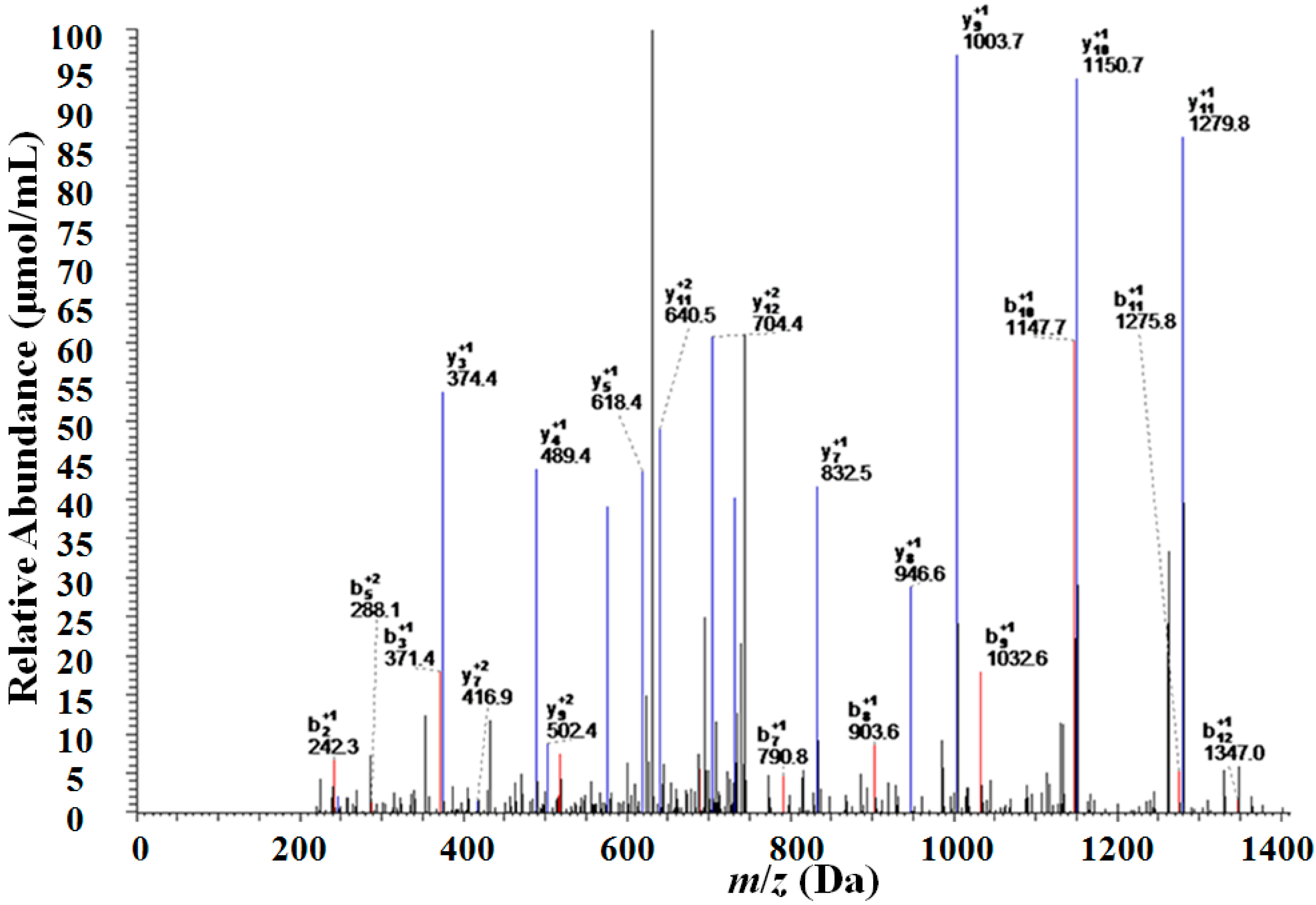
2.3. Identification of the Target Serum Protein with Two-Dimensional Liquid Chromatography-Linearion Trap Mass Spectrometry (2D-LC–LTQ–MS)
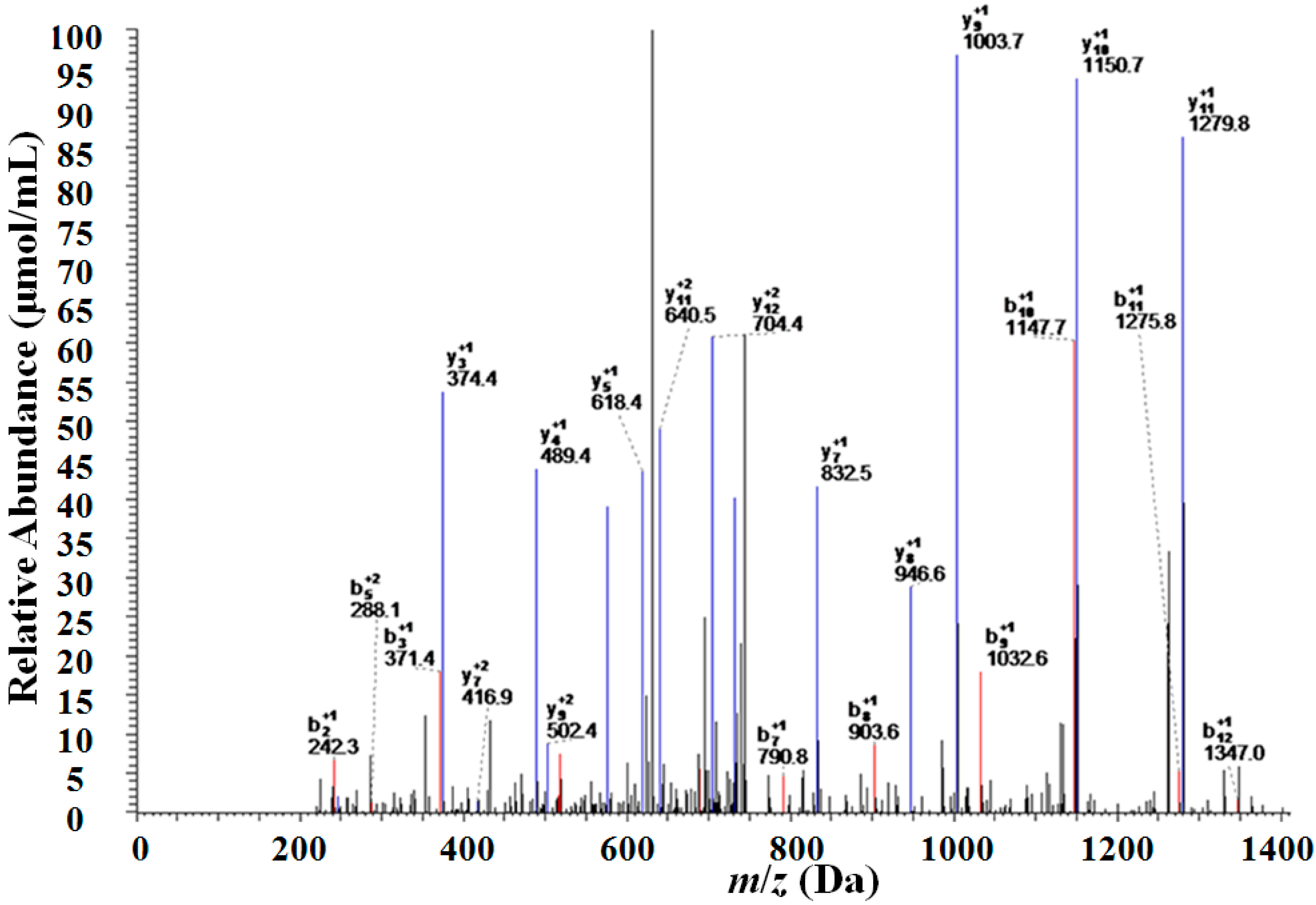
| m/z (Da) | Protein Name | Peptides Identified | Sequence |
|---|---|---|---|
| 6438 | apolipoprotein C-I | R.IKQSELSAK.M | DVSSALDKLKEFGNTLEDKARELISRIKQSELSAKMREWFSETFQKVKEKLKIDS |
| R.IKQSELSAKMR.E | |||
| K.LKEFGNTLEDKAR.E | |||
| K. LKEFGNTLEDK.A | |||
| R.ELISRIKQSELSAK.M | |||
| R.EWFSETFQKVKEK.L | |||
| K.MREWFSETFQKVK.E |
| m/z (Da) | Protein Name | Sequence Identified | Sequence Coverage (%) | Score |
|---|---|---|---|---|
| 6438 | apolipoprotein C-I | LKEFGNTLEDKARELISRIKQSELSAKMREWFSETFQKVKEK | 54.23 | 90.22 |
3. Discussion
4. Materials and Methods
4.1. Patients and Serum Samples
4.2. Reagents and Instruments
4.3. Serum Protein Profiling by SELDI–TOF–MS
4.4. Purification of Candidate Protein Markers by HPLC and MALDI–TOF–MS
4.5. Identification of Candidate Wilms’ Tumor Biomarkers
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Davidoff, A.M. Wilms tumor. Curr. Opin. Pediatr. 2009, 21, 357–364. [Google Scholar] [CrossRef]
- Liou, P.; Bader, L.; Wang, A.; Yamashiro, D.; Kandel, J.J. Correlation of tumor-associated macrophages and clinicopathological factors in Wilms tumor. Vasc. Cell 2013. [Google Scholar] [CrossRef]
- Maurya, P.; Meleady, P.; Dowling, P.; Clynes, M. Proteomic approaches for serum biomarker discovery in cancer. Anticancer Res. 2007, 27, 1247–1255. [Google Scholar]
- Chechlinska, M.; Kowalewska, M.; Nowak, R. Systemic inflammation as a confounding factor in cancer biomarker discovery and validation. Nat. Rev. Cancer 2010, 10, 2–3. [Google Scholar] [CrossRef]
- Kelly-Spratt, K.S.; Pitteri, S.J.; Gurley, K.E.; Liggitt, D.; Chin, A.; Kennedy, J.; Wong, C.H.; Zhang, Q.; Buson, T.B.; Wang, H.; et al. Plasma proteome profiles associated with inflammation, angiogenesis, and cancer. PLoS One 2011, 6, e19721. [Google Scholar]
- Wang, J.; Wang, L.; Zhang, D.; Fan, Y.; Jia, Z.; Qin, P.; Yu, J.; Zheng, S.; Yang, F. Identification of potential serum biomarkers for Wilms tumor after excluding confounding effects of common systemic inflammatory factors. Mol. Biol. Rep. 2012, 39, 5095–5104. [Google Scholar] [CrossRef]
- Wong, H.R.; Cvijanovich, N.; Allen, G.L.; Lin, R.; Anas, N.; Meyer, K.; Freishtat, R.J.; Monaco, M.; Odoms, K.; Sakthivel, B.; et al. Genomics of Pediatric SIRS/Septic Shock Investigators: Genomic expression profiling across the pediatric systemic inflammatory response syndrome, sepsis, and septic shock spectrum. Crit. Care Med. 2009, 37, 1558–1566. [Google Scholar] [CrossRef]
- Kylänpää, M.L.; Repo, H.; Puolakkainen, P.A. Inflammation and immunosuppression in severe acute pancreatitis. World J. Gastroenterol. 2010, 16, 2867–2872. [Google Scholar]
- De Winter, B.Y.; de Man, J.G. Interplay between inflammation, immune system and neuronal pathways: Effect on gastrointestinal motility. World J. Gastroenterol. 2010, 16, 5523–5535. [Google Scholar]
- Wynn, J.; Cornell, T.T.; Wong, H.R.; Shanley, T.P.; Wheeler, D.S. The host response to sepsis and developmental impact. Pediatrics 2010, 125, 1031–1041. [Google Scholar] [CrossRef]
- Bone, R.C. Toward a theory regarding the pathogenesis of the systemic inflammatory response syndrome: What we do and do not know about cytokine regulation. Crit. Care Med. 1996, 24, 163–172. [Google Scholar] [CrossRef]
- Montravers, P.; Chollet-Martin, S.; Marmuse, J.P.; Gougerot-Pocidalo, M.A.; Desmonts, J.M. Lymphatic release of cytokines during acute lung injury complicating severe pancreatitis. Am. J. Respir. Crit. Care Med. 1995, 152, 1527–1533. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, J.; Dong, R.; Yang, S.; Zheng, S. Identification of novel serum biomarkers in child nephroblastoma using proteomics technology. Mol. Biol. Rep. 2011, 38, 631–638. [Google Scholar]
- Puppione, D.L.; Ryan, C.M.; Bassilian, S.; Souda, P.; Xiao, X.; Ryder, O.A.; Whitelegge, J.P. Detection of two distinct forms of APO C-I in great apes. Comp. Biochem. Physiol. Part D Genomics Proteomics 2010, 5, 73–79. [Google Scholar] [CrossRef]
- Engwegen, J.Y.; Helgason, H.H.; Cats, A.; Harris, N.; Bonfrer, J.M.; Schellens, J.H.; Beijnen, J.H. Identification of serum proteins discriminating colorectal cancer patients and healthy controls using surface-enhanced laser desorption ionisation-time of flight mass spectrometry. World J. Gastroenterol. 2006, 12, 1536–1544. [Google Scholar]
- Gobel, T.; Vorderwulbecke, S.; Hauck, K.; Fey, H.; Häussinger, D.; Erhardt, A. New multi protein patterns differentiate liver fibrosis stages and hepatocellular carcinoma in chronic hepatitis C serum samples. World J. Gastroenterol. 2006, 12, 7604–7612. [Google Scholar]
- Fan, Y.; Wang, J.; Yang, Y.; Liu, Q.; Fan, Y.; Yu, J.; Zheng, S.; Li, M.; Wang, J. Detection and identification of potential biomarkers of breast cancer. Cancer Res. Clin. Oncol. 2010, 136, 1243–1254. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, S.; Fan, Y.; Zhao, F.; Liu, Q.; Hu, W.; Liu, D.; Fan, K.; Wang, J.; Wang, J. Detection and identification of potential biomarkers of non-small cell lung cancer. Technol. Cancer Res. Treat. 2009, 8, 455–466. [Google Scholar]
- Fan, Y.; Shi, L.; Liu, Q.; Dong, R.; Zhang, Q.; Yang, S.; Fan, Y.; Yang, H.; Wu, P.; Yu, J.; et al. Discovery and identification of potential biomarkers of papillary thyroid carcinoma. Mol. Cancer 2009, 8, 79. [Google Scholar] [CrossRef]
- Hegmans, J.P.; Veltman, J.D.; Fung, E.T.; Verch, T.; Glover, C.; Zhang, F.; Allard, W.J.; T’Jampens, D.; Hoogsteden, H.C.; Lambrecht, B.N.; et al. Protein profiling of pleural effusions to identify malignant pleural mesothelioma using SELDI–TOF–MS. Technol. Cancer Res. Treat. 2009, 8, 323–332. [Google Scholar]
- Yamamoto-Ishikawa, K.; Suzuki, H.; Nezu, M.; Kamiya, N.; Imamoto, T.; Komiya, A.; Sogawa, K.; Tomonaga, T.; Nomura, F.; Ichikawa, T. The isolation and identification of apolipoprotein C-I in hormonerefractory prostate cancer using surface-enhanced laser desorption/ionization time-of-flight mass spectrometry. Asian J. Androl. 2009, 11, 299–307. [Google Scholar]
- Cohen, M.; Yossef, R.; Erez, T.; Kugel, A.; Welt, M.; Karpasas, M.M.; Bones, J.; Rudd, P.M.; Taieb, J.; Boissin, H.; et al. Serum apolipoproteins C-I and C-III are reduced in stomach cancer patients: Results from MALDI-based peptidome and immuno-based clinical assays. PLoS One 2011, 6, e14540. [Google Scholar] [CrossRef]
- Claerhout, S.; Lim, J.Y.; Choi, W.; Park, Y.Y.; Kim, K.; Kim, S.B.; Lee, J.S.; Mills, G.B.; Cho, J.Y. Gene expression signature analysis identifies vorinostatas a candidate therapy for gastric cancer. PLoS One 2011, 6, e24662. [Google Scholar] [CrossRef]
- Xue, A.; Scarlett, C.J.; Chung, L.; Butturini, G.; Scarpa, A.; Gandy, R.; Wilson, S.R.; Baxter, R.C.; Smith, R.C. Discovery of serum biomarkers for pancreatic adenocarcinoma using proteomic analysis. Br. J. Cancer 2010, 103, 391–400. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zhang, J.; Guo, F.; Wang, L.; Zhao, W.; Zhang, D.; Yang, H.; Yu, J.; Niu, L.; Yang, F.; Zheng, S.; et al. Identification of Apolipoprotein C-I as a Potential Wilms’ Tumor Marker after Excluding Inflammatory Factors. Int. J. Mol. Sci. 2014, 15, 16186-16195. https://doi.org/10.3390/ijms150916186
Zhang J, Guo F, Wang L, Zhao W, Zhang D, Yang H, Yu J, Niu L, Yang F, Zheng S, et al. Identification of Apolipoprotein C-I as a Potential Wilms’ Tumor Marker after Excluding Inflammatory Factors. International Journal of Molecular Sciences. 2014; 15(9):16186-16195. https://doi.org/10.3390/ijms150916186
Chicago/Turabian StyleZhang, Junjie, Fei Guo, Lei Wang, Wei Zhao, Da Zhang, Heying Yang, Jiekai Yu, Lili Niu, Fuquan Yang, Shu Zheng, and et al. 2014. "Identification of Apolipoprotein C-I as a Potential Wilms’ Tumor Marker after Excluding Inflammatory Factors" International Journal of Molecular Sciences 15, no. 9: 16186-16195. https://doi.org/10.3390/ijms150916186
APA StyleZhang, J., Guo, F., Wang, L., Zhao, W., Zhang, D., Yang, H., Yu, J., Niu, L., Yang, F., Zheng, S., & Wang, J. (2014). Identification of Apolipoprotein C-I as a Potential Wilms’ Tumor Marker after Excluding Inflammatory Factors. International Journal of Molecular Sciences, 15(9), 16186-16195. https://doi.org/10.3390/ijms150916186