
Early-Stage Pancreatic Cancer Diagnosis: Serum Biomarkers and the Potential for Aptamer-Based Biosensors


Abstract
1. Introduction
2. Serum Biomarkers for Pancreatic Cancer
2.1. Proteins and Glycans
2.1.1. CA19-9
2.1.2. CEA
2.1.3. MUCINs (Mucin 1/CA15-3, Mucin 5AC, Mucin 16/CA125)
2.1.4. Osteopontin
2.2. Extracellular Vehicles (EVs) and Circulating Tumor Cells (CTCs)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker Names | Disease Stage | AUC | SN | SP | Detection Method | Ref. |
|---|---|---|---|---|---|---|
| Glycans and proteins | ||||||
| sCD163 | Early-stage PC vs. health | 0.93 | - | - | ELISA | [113] |
| PHA-E-positive Cp | PDAC vs. health | 0.97 | - | - | MS and Lectin blotting | [114] |
| fibrinogen alpha chain | PDAC vs. health | - | 67.4% | 83.6% | MS | [115] |
| serum N-glycome | PDAC vs. health | 0.81 | 75% | 72% | MS | [116] |
| TNF-α, IL-2R, IL-6, and IL-8 | malignant IPMNs vs. benign IPMN | 0.87 | 88.7% | 73.1% | CLIA | [117] |
| CA19-9 + GLRX3 | PDAC vs. health | - | 98.3% | 100% | ELISA | [118] |
| CA19-9 + bilirubin | Early-stage PDAC vs. BPD | 0.89 | - | - | Immunoassay, diazo method, Luminescence, | [119] |
| CA19-9 < 37 U/mL patient: | 0.84 | - | - | [119] | ||
| CA199 + PIVKA-II | PDAC vs. PB | 0.95 | 83.3% | 94.4% | CLIA | [120] |
| CA19-9 + LTB4 | PDAC vs. health | 0.97 | - | - | ELISA | [121] |
| CA19-9 + sCD40 | Early-stage PC vs. health | 0.95 | - | - | ELISA | [122] |
| CA19-9 + MMP-7 + SDC1 | PDAC vs. health | 1.00 | 100% | 33% | Immunoassay | [123] |
| CA19-9 + MMP-7 | PDAC vs. health | 0.99 | 99% | 65% | Immunoassay | [123] |
| CA19-9 + sAXL | PDAC vs. CP | - | 89.9% | 100% | ELISA | [124] |
| PDAC vs. controls | 0.91 | 100% | - | [124] | ||
| CA19-9 + CA19-9/bilirubin ratio +bilirubin | PDAC vs. PB | 0.91 | 90% | 80% | Immunoassay, diazo method, Luminescence | [125] |
| PDAC vs. dCCA | 0.83 | 64.6% | 90.9% | [125] | ||
| CA19-9 + Asprosin | early stage PDAC vs. diabetics patient | 0.93 | - | - | ELISA | [126] |
| CA19-9 + MMP2 | PC stage I vs. health | - | 85% | 96% | PAC-MANN assay, ELISA | [127] |
| EphA2-NF + CA 19-9 | Early-stage PC vs. health | 0.94 | - | - | CLIA | [128] |
| Circulating Tumor Cells | ||||||
| CA19-9 + CD86, CA14, CD33, CD4, CD11b, CD183, CD25, CD152 and 11 cell subsets | Early-stage PC vs. health | 0.95 | - | - | MS | [129] |
| PDAC vs. health | 0.98 | 92.4% | 91.2% | [129] | ||
| Extracellular Vesicles (detection marker) | ||||||
| CD63 | PDAC vs. Health | 0.85 | 82.1% | 84.6% | ELISA | [130] |
| GPRC5C + EPS8 | Early-stage PC vs. health | 0.92–0.95 | - | - | Ultracentrifugation, MS | [98] |
| hsa_circ_0006220 + hsa_circ_0001666 | PDAC vs. Health | 0.88 | 74.2% | 87.1% | qRT-PCR | [131] |
| GPC-1 | stage I PDAC vs. CP | 0.97 | - | - | flow cytometry | [103] |
| miR-45 Ia | PC vs. health | 0.90 | 80.1% | 86.7% | qRT-PCR | [106] |
| PC vs. PB | 0.86 | 71.2% | 89.5% | [106] | ||
| MUC5AC | invasive high-grade IPMN vs low-grade-IPMN | 0.96 | 82% | 100% | flow cytometry | [90] |
| LRG1 + GPC-1 | Early-stage PC vs. health | 0.95 | 90.0% | 86.7% | Immunoassay | [104] |
| CA19-9 + GPC-1 + CD82 | PDAC vs. CP | 0.96 | - | - | flow cytometry | [132] |
| PDAC vs. health | 0.94 | - | - | [132] | ||
| microRNAs and tsRNAs | ||||||
| miR-320b | PDAC vs. CP | 1 | 100% | 100% | qRT-PCR | [133] |
| miR-122-5p | PDAC vs. health | 0.99 | 98% | 96% | qRT-PCR | [133] |
| hsa-miR-1246+hsa-miR-205-5p+ hsa-miR-191-5p | PDAC vs. CP | 0.92 | 94.5% | 80% | machine learning | [134] |
| CA19-9 + miR-34a-5p + miR-130a-3p + miR-222-3p | PDAC stage II vs. controls | 0.92–0.94 | - | - | miRNA profiling platform | [135] |
| CA19-9 + miR-1290 | PDAC vs. health | 0.963 | 80.4% | 90% | miRNA sequencing | [136] |
| CA19-9 + 100 highly expressed miRNAs | asymptomatic early-stage PC vs health | 0.97 | 67% | 98% | miRNA sequencing, machine learning | [137] |
| PC vs. health | 0.99 | 90% | 98% | |||
| tRF-Pro-AGG-004 + tRF-Leu-CAG-002 | PDAC vs. health | - | 85% | 96.4% | RNA sequencing | [138] |
| Early-stage PC vs. health | 0.84 | 75% | 83.0% | [138] | ||
| ctDNAs and cfDNAs | ||||||
| hypermethylation of BMP3, RASSF1A, BNC1, MESTv2, TFPI2, APC, SFRP1 and SFRP2 | PDAC all stages vs. CP | 0.85–0.93 | - | - | PCR + CLIA. | [139] |
| 5hmC densities in cfDNAs | PDAC vs. health | 0.92–0.94 | - | - | NGS | [140] |
| six DNA methylations of PRKCB | PDAC vs. CP | 1 | - | - | Bisulfite qPCR | [141] |
| cfDNA-derived 5-hydroxymethylcytosine (5hmC) | Early-stage PC vs. high-risk populations | - | 68.3% | 96.9% | NGS + machine learning | [142] |
| CA19-9 + FUT3 test | PDAC (localized) vs. controls | - | 66.4% | 99.3% | ELISA + gene sequencing | [143] |
| CA19-9 + thirteen methylated DNA markers (AK055957, GRIN2D, CD1D, ZNF781, FER1L4, RYR2, CLEC11A, LRRC4, GH05J042948, HOXA1, PRKCB, SHISA9, NTRK3) | Early-stage PC vs. health | 0.9 | 81% | 97.5% | ELISA + TELQAS | [144] |
| PDAC vs. health | - | 92% | 92% | [144] | ||
| CA19-9 + 56-marker classifier | Early-stage PC vs. health | 0.92 | 88% | 89% | bisulfite sequencing | [145] |
| PDAC vs. health | 0.94 | 86% | 89% | [145] | ||
| CA19-9 + DUPAN-2 + FUT test | PC vs. health | - | 80.7% | 97.7% | ELISA + gene sequencing | [146] |
| Early-stage PC vs. health | - | 60.4% | 97.7% | [146] | ||
| Lipids and metabolites | ||||||
| Proline, creatine, and palmitic acid | early-stage PDAC vs. BP | 0.852 | - | - | MS | [147] |
| CA19-9 + Proline, creatine, and palmitic acid | early-stage PDAC vs. BP | 0.91 | - | - | MS | [147] |
| CA19-9 + four metabolites | Early-stage PC vs. health | 0.76–0.85 | 39.7–81.6% | 88.7–94.1% | MS + machine learning | [148] |
| Mixed panels | ||||||
| Five proteins (EEF1A1, RPH3AL, NCOR1, L1CAM, TMEM161A) and three miRNAs (miR-146a-5p, miR-155–5p, miR-375) | high-risk IPMN vs. low-risk IPMN | 0.97 | - | - | qPCR + microarrays | [149] |
| SNP-stratified [CPA activity + CA19-9] | PDAC all stages vs. health | 0.94 | 68% | 98.2% | enzymatic assays, ELISA, TaqMan Assay | [150] |
| PDAC stage I vs. health | 0.90 | 51.9% | 98.2% | [150] | ||
| CA19-9 + EV-CK18 mRNA + EV-CD63 mRNA + EV-miR.409 + cfDNA concentration | PDAC vs. health | 0.95 | 88% | 95% | PCR+ ECLIA + machine learning | [151] |
2.3. Nucleic Acids (Circulating RNAs and DNAs)
2.4. Lipids and Metabolites
2.5. Multiplex Biomarker Panels
3. Aptamer-Based Biosensor
3.1. CA19-9 Detection via Aptamer-Based Biosensors
3.1.1. Aptamer-Based Optical Biosensor
Fluorescence-Based Aptamer Biosensor
Surface-Enhanced Raman Spectroscopy-Based Aptamer Biosensor
3.1.2. Electrochemical-Based Aptamer Biosensor
3.2. CEA Detection via Aptamer-Based Biosensors
3.2.1. Aptamer-Based Optical Biosensor
Colorimetric-Based Aptamer Biosensor
Fluorescence-Based Aptamer Biosensor
Switch-On/Off Fluorescence Biosensor
FRET Biosensor
Chemiluminescence-Based Aptamer Biosensor
Electrochemiluminescence-Based Aptamer Biosensor
Surface Plasmon Resonance-Based Aptamer Biosensor
3.2.2. Electrochemical-Based Aptamer Biosensor
Free Aptamers in Solution
Direct Immobilization
Nanomaterial-Assisted Immobilization
DNA Nanostructure-Based Immobilization

3.3. MUC1 Detection via Aptamer-Based Biosensors
3.3.1. Aptamer-Based Optical Biosensor
Colorimetric-Based Aptamer Biosensor
Fluorescence-Based Aptamer Biosensor
3.3.2. Electrochemical-Based Aptamer Biosensor
Voltammetric-Based Electrochemical Aptamer Biosensors
Impedance-Based Electrochemical Aptamer Biosensors

3.4. CA125 Detection via Aptamer-Based Biosensors
3.4.1. Aptamer-Based Optical Biosensor
Colorimetric-Based Aptamer Biosensor
Fluorescence-Based Aptamer Biosensor
Electrochemiluminescence-Based Aptamer Biosensor
Surface Plasmon Resonance-Based Aptamer Biosensor
3.4.2. Electrochemical-Based Aptamer Biosensor
Voltammetric-Based Electrochemical Aptamer Biosensors
Impedance-Based Electrochemical Aptamer Biosensors
3.5. Protein-Related Multiple Biomarker Detection via Aptamer-Based Biosensor

3.6. Exosomes as Biomarkers Detection via Aptamer-Based Biosensors
3.6.1. Single-Biomarker Recognition via Aptamer Biosensor
3.6.2. Multiple-Biomarker Recognition via Aptamer Biosensor
4. Conclusions
5. Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 5hmC | 5-Hydroxymethylcytosine |
| AUC | Area Under the Curve |
| BP | Benign Pancreatic Cystic Neoplasms |
| BPD | Benign Periampullary Disease |
| CA125 | Cancer Antigen 125 |
| CA19-9 | Carbohydrate Antigen 19-9 |
| CEA | Carcinoembryonic Antigen |
| cfDNA | Cell-Free DNA |
| CLIA | Clinical Laboratory Improvement Amendments |
| CLIA | Chemiluminescent Immunoassay |
| CPA | Serum Carboxypeptidase |
| CRISPR | Clustered Regularly Interspaced Short Palindromic Repeats |
| CTCs | Circulating Tumor Cells |
| ctDNA | Circulating Tumor DNA |
| dCCA | Distal Cholangiocarcinoma |
| DPV | Differential Pulse Voltammetry |
| ECL | Electrochemiluminescence |
| ECLIA | Electrochemiluminescence Immunoassay |
| EIS | Electrochemical Impedance Spectroscopy |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| EVs | Extracellular Vesicles |
| FDA | Food and Drug Administration |
| FRET | Fluorescence Resonance Energy Transfer |
| GLRX3 | Glutaredoxin3 |
| GPC-1 | Glypican-1 |
| IL | Interleukin |
| IPMN | Intraductal Papillary Mucinous Neoplasm |
| IVD | In Vitro Diagnostic |
| KRAS | Kirsten Rat Sarcoma Viral Oncogene Homolog |
| LOD | Limit of Detection |
| LRG1 | Leucine-Rich Alpha-2-Glycoprotein 1 |
| LTB4 | Leukotriene B4 |
| MFDS | Ministry of Food and Drug Safety |
| miRNAs | MicroRNAs |
| MMP | Matrix Metalloproteinase |
| MUC | Mucin |
| NGS | Next-Generation Sequencing |
| PanIN | Pancreatic Intraepithelial Neoplasia |
| PB | Pancreatic Benign Disease |
| PC | Pancreatic Cancer |
| PDAC | Pancreatic Ductal Adenocarcinoma |
| PHA-E-positive Cp | Phaseolus vulgaris Erythroagglutinin-Positive Ceruloplasmin |
| POCT | Point-of-Care Testing |
| PRKCB | Protein Kinase C Beta Type Gene |
| qRT-PCR | Quantitative Reverse Transcription and Real-Time Polymerase Chain Reaction |
| RUO | Research Use Only |
| sCD40 | Soluble CD40 |
| sCD163 | Soluble CD163 |
| SDC1 | Syndecan-1 |
| SELEX | Systematic Evolution of Ligands by Exponential Enrichment |
| SN | Sensitivity |
| SP | Specificity |
| SPR | Surface Plasmon Resonance |
| SWV | Square Wave Voltammetry |
| TELQAS | Target Enrichment Long-Probe Quantitative Amplified Signal Assay |
| TIMP1 | Tissue Inhibitor of Metalloproteinases 1 |
| TNF-α | Tumor Necrosis Factor Alpha |
| VEGF | Vascular Endothelial Growth Factor |
References
- Danpanichkul, P.; Suparan, K.; Tothanarungroj, P.; Dejvajara, D.; Rakwong, K.; Pang, Y.; Barba, R.; Thongpiya, J.; Fallon, M.B.; Harnois, D.; et al. Epidemiology of gastrointestinal cancers: A systematic analysis from the Global Burden of Disease Study 2021. Gut 2025, 74, 26. [Google Scholar] [CrossRef]
- Zhou, Y.; Song, K.; Chen, Y.; Zhang, Y.; Dai, M.; Wu, D.; Chen, H. Burden of six major types of digestive system cancers globally and in China. Chin. Med. J. 2024, 137, 1957–1964. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, E.M.; Brand, R.E.; Goggins, M. Pancreatic Cancer: Changing Epidemiology and New Approaches to Risk Assessment, Early Detection, and Prevention. Gastroenterology 2023, 164, 752–765. [Google Scholar] [CrossRef] [PubMed]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef]
- Conroy, T.; Pfeiffer, P.; Vilgrain, V.; Lamarca, A.; Seufferlein, T.; O’Reilly, E.M.; Hackert, T.; Golan, T.; Prager, G.; Haustermans, K.; et al. Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 987–1002. [Google Scholar] [CrossRef]
- Klein, E.A.; Richards, D.; Cohn, A.; Tummala, M.; Lapham, R.; Cosgrove, D.; Chung, G.; Clement, J.; Gao, J.; Hunkapiller, N.; et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Ann. Oncol. 2021, 32, 1167–1177. [Google Scholar] [CrossRef]
- Chowdhury, S.; Kesling, M.; Collins, M.; Lopez, V.; Xue, Y.; Oliveira, G.; Friedl, V.; Bergamaschi, A.; Haan, D.; Volkmuth, W.; et al. Analytical Validation of an Early Detection Pancreatic Cancer Test Using 5-Hydroxymethylation Signatures. J. Mol. Diagn. 2024, 26, 888–896. [Google Scholar] [CrossRef]
- Brand, R.E.; Persson, J.; Bratlie, S.O.; Chung, D.C.; Katona, B.W.; Carrato, A.; Castillo, M.; Earl, J.; Kokkola, A.; Lucas, A.L.; et al. Detection of Early-Stage Pancreatic Ductal Adenocarcinoma From Blood Samples: Results of a Multiplex Biomarker Signature Validation Study. Clin. Transl. Gastroenterol. 2022, 13, e00468. [Google Scholar] [CrossRef]
- Honda, K.; Kobayashi, M.; Okusaka, T.; Rinaudo, J.A.; Huang, Y.; Marsh, T.; Sanada, M.; Sasajima, Y.; Nakamori, S.; Shimahara, M.; et al. Plasma biomarker for detection of early stage pancreatic cancer and risk factors for pancreatic malignancy using antibodies for apolipoprotein-AII isoforms. Sci. Rep. 2015, 5, 15921. [Google Scholar] [CrossRef]
- Kashiro, A.; Kobayashi, M.; Oh, T.; Miyamoto, M.; Atsumi, J.; Nagashima, K.; Takeuchi, K.; Nara, S.; Hijioka, S.; Morizane, C.; et al. Clinical development of a blood biomarker using apolipoprotein-A2 isoforms for early detection of pancreatic cancer. J. Gastroenterol. 2024, 59, 263–278. [Google Scholar] [CrossRef]
- Röthlisberger, P.; Hollenstein, M. Aptamer chemistry. Adv. Drug Deliv. Rev. 2018, 134, 3–21. [Google Scholar] [CrossRef]
- Yu, H.; Alkhamis, O.; Canoura, J.; Liu, Y.; Xiao, Y. Advances and Challenges in Small-Molecule DNA Aptamer Isolation, Characterization, and Sensor Development. Angew. Chem. Int. Ed. Engl. 2021, 60, 16800–16823. [Google Scholar] [CrossRef] [PubMed]
- Scarà, S.; Bottoni, P.; Scatena, R. CA 19-9: Biochemical and Clinical Aspects. In Advances in Cancer Biomarkers: From Biochemistry to Clinic for a Critical Revision; Scatena, R., Ed.; Springer: Dordrecht, The Netherlands, 2015; pp. 247–260. [Google Scholar]
- Schmiegel, W.H.; Kreiker, C.; Eberl, W.; Arndt, R.; Classen, M.; Greten, H.; Jessen, K.; Kalthoff, H.; Soehendra, N.; Thiele, H.G. Monoclonal antibody defines CA 19-9 in pancreatic juices and sera. Gut 1985, 26, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Koprowski, H.; Steplewski, Z.; Mitchell, K.; Herlyn, M.; Herlyn, D.; Fuhrer, P. Colorectal carcinoma antigens detected by hybridoma antibodies. Somat. Cell Genet. 1979, 5, 957–971. [Google Scholar] [CrossRef] [PubMed]
- Kalthoff, H.; Kreiker, C.; Schmiegel, W.H.; Greten, H.; Thiele, H.G. Characterization of CA 19-9 bearing mucins as physiological exocrine pancreatic secretion products. Cancer Res. 1986, 46, 3605–3607. [Google Scholar]
- Makovitzky, J. The distribution and localization of the monoclonal antibody-defined antigen 19-9 (CA19-9) in chronic pancreatitis and pancreatic carcinoma. Virchows Arch. B 1986, 51, 535–544. [Google Scholar] [CrossRef]
- Engle, D.D.; Tiriac, H.; Rivera, K.D.; Pommier, A.; Whalen, S.; Oni, T.E.; Alagesan, B.; Lee, E.J.; Yao, M.A.; Lucito, M.S.; et al. The glycan CA19-9 promotes pancreatitis and pancreatic cancer in mice. Science 2019, 364, 1156–1162. [Google Scholar] [CrossRef]
- Yue, T.; Maupin, K.A.; Fallon, B.; Li, L.; Partyka, K.; Anderson, M.A.; Brenner, D.E.; Kaul, K.; Zeh, H.; Moser, A.J.; et al. Enhanced Discrimination of Malignant from Benign Pancreatic Disease by Measuring the CA 19-9 Antigen on Specific Protein Carriers. PLoS ONE 2011, 6, e29180. [Google Scholar] [CrossRef]
- Yue, T.; Partyka, K.; Maupin, K.A.; Hurley, M.; Andrews, P.; Kaul, K.; Moser, A.J.; Zeh, H.; Brand, R.E.; Haab, B.B. Identification of blood-protein carriers of the CA 19-9 antigen and characterization of prevalence in pancreatic diseases. Proteomics 2011, 11, 3665–3674. [Google Scholar] [CrossRef]
- Kannagi, R. Carbohydrate-mediated cell adhesion involved in hematogenous metastasis of cancer. Glycoconj. J. 1997, 14, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Shibata, C.; Otsuka, M.; Ishigaki, K.; Seimiya, T.; Kishikawa, T.; Fujishiro, M. CA19-9-Positive Extracellular Vesicle Is a Risk Factor for Cancer-Associated Thrombosis in Pancreatic Cancer. Gastro Hep Adv. 2024, 3, 551–561. [Google Scholar] [CrossRef]
- Kannagi, R.; Izawa, M.; Koike, T.; Miyazaki, K.; Kimura, N. Carbohydrate-mediated cell adhesion in cancer metastasis and angiogenesis. Cancer Sci. 2004, 95, 377–384. [Google Scholar] [CrossRef]
- Kannagi, R. Molecular mechanism for cancer-associated induction of sialyl Lewis X and sialyl Lewis A expression—The Warburg effect revisited. Glycoconj. J. 2003, 20, 353–364. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, X.; Wan, Y.; Wang, W.; Ma, J. Antitumor effect of an antibody against gastrointestinal cancer-associated antigen CA19.9. Cancer Biother. Radiopharm. 2007, 22, 597–606. [Google Scholar] [CrossRef]
- Nakisa, A.; Sempere, L.F.; Chen, X.; Qu, L.T.; Woldring, D.; Crawford, H.C.; Huang, X. Tumor-Associated Carbohydrate Antigen 19-9 (CA 19-9), a Promising Target for Antibody-Based Detection, Diagnosis, and Immunotherapy of Cancer. ChemMedChem 2024, 19, e202400491. [Google Scholar] [CrossRef] [PubMed]
- Ballehaninna, U.K.; Chamberlain, R.S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 2012, 3, 105–119. [Google Scholar] [CrossRef]
- Zhao, B.; Zhao, B.; Chen, F. Diagnostic value of serum carbohydrate antigen 19-9 in pancreatic cancer: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2022, 34, 891–904. [Google Scholar] [CrossRef]
- Ciprani, D.; Morales-Oyarvide, V.; Qadan, M.; Hank, T.; Weniger, M.; Harrison, J.M.; Rodrigues, C.; Horick, N.K.; Mino-Kenudson, M.; Ferrone, C.R.; et al. An elevated CA 19-9 is associated with invasive cancer and worse survival in IPMN. Pancreatology 2020, 20, 729–735. [Google Scholar] [CrossRef]
- Zhuge, X.; Guo, C.; Chen, Y.; Feng, L.; Jia, R.; Zhao, Y.; Sun, K.; Wang, Z.; Chen, X. The Levels of Tumor Markers in Pancreatic Neuroendocrine Carcinoma and Their Values in Differentiation Between Pancreatic Neuroendocrine Carcinoma and Pancreatic Ductal Adenocarcinoma. Pancreas 2018, 47, 1290–1295. [Google Scholar] [CrossRef]
- Zeng, P.; Li, H.; Chen, Y.; Pei, H.; Zhang, L. Chapter Fourteen-Serum CA199 levels are significantly increased in patients suffering from liver, lung, and other diseases. In Progress in Molecular Biology and Translational Science; Zhang, L., Ed.; Academic Press: Cambridge, MA, USA, 2019; Volume 162, pp. 253–264. [Google Scholar]
- Bengtsson, A.; Draus, T.; Andersson, R.; Ansari, D. Prediagnostic blood biomarkers for pancreatic cancer: Meta-analysis. BJS open 2024, 8, zrae046. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, D.P.; Sandanayake, N.S.; Jenkinson, C.; Gentry-Maharaj, A.; Apostolidou, S.; Fourkala, E.-O.; Camuzeaux, S.; Blyuss, O.; Gunu, R.; Dawnay, A.; et al. Serum CA19-9 Is Significantly Upregulated up to 2 Years before Diagnosis with Pancreatic Cancer: Implications for Early Disease Detection. Clin. Cancer Res. 2015, 21, 622–631. [Google Scholar] [CrossRef]
- Honda, K.; Katzke, V.A.; Hüsing, A.; Okaya, S.; Shoji, H.; Onidani, K.; Olsen, A.; Tjønneland, A.; Overvad, K.; Weiderpass, E.; et al. CA19-9 and apolipoprotein-A2 isoforms as detection markers for pancreatic cancer: A prospective evaluation. Int. J. Cancer 2019, 144, 1877–1887. [Google Scholar] [CrossRef]
- Fahrmann, J.F.; Schmidt, C.M.; Mao, X.; Irajizad, E.; Loftus, M.; Zhang, J.; Patel, N.; Vykoukal, J.; Dennison, J.B.; Long, J.P.; et al. Lead-Time Trajectory of CA19-9 as an Anchor Marker for Pancreatic Cancer Early Detection. Gastroenterology 2021, 160, 1373–1383.e6. [Google Scholar] [CrossRef]
- Mason, J.; Lundberg, E.; Jonsson, P.; Nyström, H.; Franklin, O.; Lundin, C.; Naredi, P.; Antti, H.; Sund, M.; Öhlund, D. A Cross-Sectional and Longitudinal Analysis of Pre-Diagnostic Blood Plasma Biomarkers for Early Detection of Pancreatic Cancer. Int. J. Mol. Sci. 2022, 23, 12969. [Google Scholar] [CrossRef]
- Fahrmann, J.F.; Yip-Schneider, M.; Vykoukal, J.; Spencer, R.; Dennison, J.B.; Do, K.A.; Long, J.P.; Maitra, A.; Zhang, J.; Schmidt, C.M.; et al. Lead time trajectory of blood-based protein biomarkers for detection of pancreatic cancer based on repeat testing. Cancer Lett. 2025, 612, 217450. [Google Scholar] [CrossRef] [PubMed]
- van Manen, L.; Groen, J.V.; Putter, H.; Pichler, M.; Vahrmeijer, A.L.; Bonsing, B.A.; Mieog, J.S.D. Stage-Specific Value of Carbohydrate Antigen 19-9 and Carcinoembryonic Antigen Serum Levels on Survival and Recurrence in Pancreatic Cancer: A Single Center Study and Meta-Analysis. Cancers 2020, 12, 2970. [Google Scholar] [CrossRef] [PubMed]
- van Oosten, A.F.; Groot, V.P.; Dorland, G.; Burkhart, R.A.; Wolfgang, C.L.; van Santvoort, H.C.; He, J.; Molenaar, I.Q.; Daamen, L.A. Dynamics of Serum CA19-9 in Patients Undergoing Pancreatic Cancer Resection. Ann. Surg. 2024, 279, 493–500. [Google Scholar] [CrossRef]
- Azizian, A.; Rühlmann, F.; Krause, T.; Bernhardt, M.; Jo, P.; König, A.; Kleiß, M.; Leha, A.; Ghadimi, M.; Gaedcke, J. CA19-9 for detecting recurrence of pancreatic cancer. Sci. Rep. 2020, 10, 1332. [Google Scholar] [CrossRef]
- Yi, N.; Zhao, X.; Ji, J.; Xu, M.; Jiao, Y.; Qian, T.; Zhu, S.; Jiang, F.; Chen, J.; Xiao, M. Serum galectin-3 as a biomarker for screening, early diagnosis, prognosis and therapeutic effect evaluation of pancreatic cancer. J. Cell Mol. Med. 2020, 24, 11583–11591. [Google Scholar] [CrossRef]
- Kim, J.E.; Lee, K.T.; Lee, J.K.; Paik, S.W.; Rhee, J.C.; Choi, K.W. Clinical usefulness of carbohydrate antigen 19-9 as a screening test for pancreatic cancer in an asymptomatic population. J. Gastroenterol. Hepatol. 2004, 19, 182–186. [Google Scholar] [CrossRef]
- Hao, C.; Zhang, G.; Zhang, L. Chapter Eleven-Serum CEA levels in 49 different types of cancer and noncancer diseases. In Progress in Molecular Biology and Translational Science; Zhang, L., Ed.; Academic Press: Cambridge, MA, USA, 2019; Volume 162, pp. 213–227. [Google Scholar]
- Beauchemin, N.; Arabzadeh, A. Carcinoembryonic antigen-related cell adhesion molecules (CEACAMs) in cancer progression and metastasis. Cancer Metastasis Rev. 2013, 32, 643–671. [Google Scholar] [CrossRef]
- Emoto, S.; Ishigami, H.; Yamashita, H.; Yamaguchi, H.; Kaisaki, S.; Kitayama, J. Clinical significance of CA125 and CA72-4 in gastric cancer with peritoneal dissemination. Gastric Cancer 2012, 15, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Gebauer, F.; Wicklein, D.; Horst, J.; Sundermann, P.; Maar, H.; Streichert, T.; Tachezy, M.; Izbicki, J.R.; Bockhorn, M.; Schumacher, U. Carcinoembryonic Antigen-Related Cell Adhesion Molecules (CEACAM) 1, 5 and 6 as Biomarkers in Pancreatic Cancer. PLoS ONE 2014, 9, e113023. [Google Scholar] [CrossRef]
- Meng, Q.; Shi, S.; Liang, C.; Liang, D.; Xu, W.; Ji, S.; Zhang, B.; Ni, Q.; Xu, J.; Yu, X. Diagnostic and prognostic value of carcinoembryonic antigen in pancreatic cancer: A systematic review and meta-analysis. Onco Targets Ther. 2017, 10, 4591–4598. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.-L.; Lan, C.; Pei, H.; Yang, S.-N.; Liu, Y.-F.; Xiao, L.-L. Applicative Value of Serum CA19-9, CEA, CA125 and CA242 in Diagnosis and Prognosis for Patients with Pancreatic Cancer Treated by Concurrent Chemoradiotherapy. Asian Pac. J. Cancer Prev. 2015, 16, 6569–6573. [Google Scholar] [CrossRef]
- Luo, G.; Liu, C.; Guo, M.; Cheng, H.; Lu, Y.; Jin, K.; Liu, L.; Long, J.; Xu, J.; Lu, R.; et al. Potential Biomarkers in Lewis Negative Patients With Pancreatic Cancer. Ann. Surg. 2017, 265, 800–805. [Google Scholar] [CrossRef]
- van Manen, L.; Groen, J.V.; Putter, H.; Vahrmeijer, A.L.; Swijnenburg, R.-J.; Bonsing, B.A.; Mieog, J.S.D. Elevated CEA and CA19-9 serum levels independently predict advanced pancreatic cancer at diagnosis. Biomarkers 2020, 25, 186–193. [Google Scholar] [CrossRef]
- Meng, Q.; Shi, S.; Liang, C.; Xiang, J.; Liang, D.; Zhang, B.; Qin, Y.; Ji, S.; Xu, W.; Xu, J.; et al. Diagnostic Accuracy of a CA125-Based Biomarker Panel in Patients with Pancreatic Cancer: A Systematic Review and Meta-Analysis. J. Cancer 2017, 8, 3615–3622. [Google Scholar] [CrossRef]
- Kaur, S.; Kumar, S.; Momi, N.; Sasson, A.R.; Batra, S.K. Mucins in pancreatic cancer and its microenvironment. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 607–620. [Google Scholar] [CrossRef]
- Nabavinia, M.S.; Gholoobi, A.; Charbgoo, F.; Nabavinia, M.; Ramezani, M.; Abnous, K. Anti-MUC1 aptamer: A potential opportunity for cancer treatment. Med. Res. Rev. 2017, 37, 1518–1539. [Google Scholar] [CrossRef]
- Ganguly, K.; Rauth, S.; Marimuthu, S.; Kumar, S.; Batra, S.K. Unraveling mucin domains in cancer and metastasis: When protectors become predators. Cancer Metastasis Rev. 2020, 39, 647–659. [Google Scholar] [CrossRef]
- Gold, D.V.; Modrak, D.E.; Ying, Z.; Cardillo, T.M.; Sharkey, R.M.; Goldenberg, D.M. New MUC1 serum immunoassay differentiates pancreatic cancer from pancreatitis. J. Clin. Oncol. 2006, 24, 252–258. [Google Scholar] [CrossRef]
- Gold, D.V.; Karanjawala, Z.; Modrak, D.E.; Goldenberg, D.M.; Hruban, R.H. PAM4-Reactive MUC1 Is a Biomarker for Early Pancreatic Adenocarcinoma. Clin. Cancer Res. 2007, 13, 7380–7387. [Google Scholar] [CrossRef] [PubMed]
- Ercan, Ş.; Kaymaz, Ö.; Yücel, N.; Orçun, A. Serum concentrations of CA 125, CA 15-3, CA 19-9 and CEA in normal pregnancy: A longitudinal study. Arch. Gynecol. Obstet. 2012, 285, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Yin, B.W.T.; Dnistrian, A.; Lloyd, K.O. Ovarian cancer antigen CA125 is encoded by the MUC16 mucin gene. Int. J. Cancer 2002, 98, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Lakshmanan, I.; Ponnusamy, M.P.; Das, S.; Chakraborty, S.; Haridas, D.; Mukhopadhyay, P.; Lele, S.M.; Batra, S.K. MUC16 induced rapid G2/M transition via interactions with JAK2 for increased proliferation and anti-apoptosis in breast cancer cells. Oncogene 2012, 31, 805–817. [Google Scholar] [CrossRef]
- Gubbels, J.A.A.; Belisle, J.; Onda, M.; Rancourt, C.; Migneault, M.; Ho, M.; Bera, T.K.; Connor, J.; Sathyanarayana, B.K.; Lee, B.; et al. Mesothelin-MUC16 binding is a high affinity, N-glycan dependent interaction that facilitates peritoneal metastasis of ovarian tumors. Mol. Cancer 2006, 5, 50. [Google Scholar] [CrossRef]
- Gubbels, J.A.A.; Felder, M.; Horibata, S.; Belisle, J.A.; Kapur, A.; Holden, H.; Petrie, S.; Migneault, M.; Rancourt, C.; Connor, J.P.; et al. MUC16 provides immune protection by inhibiting synapse formation between NK and ovarian tumor cells. Mol. Cancer 2010, 9, 11. [Google Scholar] [CrossRef]
- Yang, N.; Zhou, X.; Gong, Y.; Deng, Z. The role of MUC16 in tumor biology and tumor immunology in ovarian cancer. BMC Cancer 2025, 25, 294. [Google Scholar] [CrossRef]
- Chen, S.-H.; Hung, W.-C.; Wang, P.; Paul, C.; Konstantopoulos, K. Mesothelin Binding to CA125/MUC16 Promotes Pancreatic Cancer Cell Motility and Invasion via MMP-7 Activation. Sci. Rep. 2013, 3, 1870. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.; Sagar, S.; Liu, X.; Lee, H.-R.; Grunkemeyer, J.A.; Grandgenett, P.M.; Caffrey, T.; O’Connell, K.A.; Swanson, B.; Marcos-Silva, L.; et al. Isoforms of MUC16 activate oncogenic signaling through EGF receptors to enhance the progression of pancreatic cancer. Mol. Ther. 2021, 29, 1557–1571. [Google Scholar] [CrossRef]
- Das, S.; Rachagani, S.; Torres-Gonzalez, M.P.; Lakshmanan, I.; Majhi, P.D.; Smith, L.M.; Wagner, K.-U.; Batra, S.K. Carboxyl-terminal domain of MUC16 imparts tumorigenic and metastatic functions through nuclear translocation of JAK2 to pancreatic cancer cells. Oncotarget 2015, 6, 5772–5787. [Google Scholar] [CrossRef]
- Song, Y.; Yuan, M.; Wang, G. Update value and clinical application of MUC16 (cancer antigen 125). Expert Opin. Ther. Targets 2023, 27, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Ćwik, G.; Wallner, G.; Skoczylas, T.; Ciechański, A.; Zinkiewicz, K. Cancer Antigens 19-9 and 125 in the Differential Diagnosis of Pancreatic Mass Lesions. Arch. Surg. 2006, 141, 968–973. [Google Scholar] [CrossRef]
- Sakamoto, K.; Haga, Y.; Yoshimura, R.; Egami, H.; Yokoyama, Y.; Akagi, M. Comparative effectiveness of the tumour diagnostics, CA 19-9, CA 125 and carcinoembryonic antigen in patients with diseases of the digestive system. Gut 1987, 28, 323. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhang, Y.; Fu, J.; Zhang, L. Chapter Thirteen-Serum CA125 levels are decreased in rectal cancer but increased in fibrosis-associated diseases and in most types of cancers. In Progress in Molecular Biology and Translational Science; Zhang, L., Ed.; Academic Press: Cambridge, MA, USA, 2019; Volume 162, pp. 241–252. [Google Scholar]
- Funston, G.; Hamilton, W.; Abel, G.; Crosbie, E.J.; Rous, B.; Walter, F.M. The diagnostic performance of CA125 for the detection of ovarian and non-ovarian cancer in primary care: A population-based cohort study. PLoS Med. 2020, 17, e1003295. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, J.; Zhou, Y.; Sheng, S.; Qian, S.Y.; Huo, X. Evaluation of Serum CEA, CA19-9, CA72-4, CA125 and Ferritin as Diagnostic Markers and Factors of Clinical Parameters for Colorectal Cancer. Sci. Rep. 2018, 8, 2732. [Google Scholar] [CrossRef]
- Xu, Z.-L.; Ou, Y.-J.; Dai, H.-S.; Wan, K.; Bie, P.; Chen, Z.-Y.; Zhang, L.-D.; Zhang, C.-C. Elevated preoperative CA125 levels predicts poor prognosis of hilar cholangiocarcinoma receiving radical surgery. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101695. [Google Scholar] [CrossRef]
- Liu, L.; Xu, H.X.; Wang, W.Q.; Wu, C.T.; Xiang, J.F.; Liu, C.; Long, J.; Xu, J.; Fu, D.-L.; Ni, Q.X.; et al. Serum CA125 is a novel predictive marker for pancreatic cancer metastasis and correlates with the metastasis-associated burden. Oncotarget 2016, 7, 5943–5956. [Google Scholar] [CrossRef]
- Luo, G.; Xiao, Z.; Long, J.; Liu, Z.; Liu, L.; Liu, C.; Xu, J.; Ni, Q.; Yu, X. CA125 is Superior to CA19-9 in Predicting the Resectability of Pancreatic Cancer. J. Gastrointest. Surg. 2013, 17, 2092–2098. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Deng, S.; Jin, K.; Gong, Y.; Cheng, H.; Fan, Z.; Qian, Y.; Huang, Q.; Ni, Q.; Luo, G.; et al. Lewis antigen-negative pancreatic cancer: An aggressive subgroup. Int. J. Oncol. 2020, 56, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Skulimowski, A.; Adam, D.; Janusz, S.; and Hogendorf, P. Comparison of clinical usefulness of serum Ca125 and CA19-9 in pancreatic adenocarcinoma diagnosis: Meta-analysis and systematic review of literature. Biomarkers 2021, 26, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Prassas, I.; Dimitromanolakis, A.; Brand, R.E.; Serra, S.; Diamandis, E.P.; Blasutig, I.M. Validation of Biomarkers That Complement CA19.9 in Detecting Early Pancreatic Cancer. Clin. Cancer Res. 2014, 20, 5787–5795. [Google Scholar] [CrossRef]
- Ganguly, K.; Krishn, S.R.; Rachagani, S.; Jahan, R.; Shah, A.; Nallasamy, P.; Rauth, S.; Atri, P.; Cox, J.L.; Pothuraju, R.; et al. Secretory Mucin 5AC Promotes Neoplastic Progression by Augmenting KLF4-Mediated Pancreatic Cancer Cell Stemness. Cancer Res. 2021, 81, 91–102. [Google Scholar] [CrossRef]
- Hoshi, H.; Sawada, T.; Uchida, M.; Iijima, H.; Kimura, K.; Hirakawa, K.; Wanibuchi, H. MUC5AC protects pancreatic cancer cells from TRAIL-induced death pathways. Int. J. Oncol. 2013, 42, 887–893. [Google Scholar] [CrossRef]
- Yamazoe, S.; Tanaka, H.; Sawada, T.; Amano, R.; Yamada, N.; Ohira, M.; Hirakawa, K. RNA interference suppression of mucin 5AC (MUC5AC) reduces the adhesive and invasive capacity of human pancreatic cancer cells. J. Exp. Clin. Cancer Res. 2010, 29, 53. [Google Scholar] [CrossRef]
- Kim, G.E.; Bae, H.I.; Park, H.U.; Kuan, S.F.; Crawley, S.C.; Ho, J.J.; Kim, Y.S. Aberrant expression of MUC5AC and MUC6 gastric mucins and sialyl Tn antigen in intraepithelial neoplasms of the pancreas. Gastroenterology 2002, 123, 1052–1060. [Google Scholar] [CrossRef]
- Manne, A.; Kasi, A.; Esnakula, A.K.; Paluri, R.K. Predictive Value of MUC5AC Signature in Pancreatic Ductal Adenocarcinoma: A Hypothesis Based on Preclinical Evidence. Int. J. Mol. Sci. 2023, 24, 8087. [Google Scholar] [CrossRef]
- Dwertmann Rico, S.; Büscheck, F.; Dum, D.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Hinsch, A.; Höflmayer, D.; Perez, D.; Izbicki, J.R.; et al. Mucin 5AC expression is common but unrelated to tumor progression in pancreatic adenocarcinoma. Int. J. Immunopathol. Pharmacol. 2022, 36, 03946320221106504. [Google Scholar] [CrossRef]
- Luka, J.; Arlen, P.M.; Bristol, A. Development of a Serum Biomarker Assay That Differentiates Tumor-Associated MUC5AC (NPC-1C ANTIGEN) from Normal MUC5AC. BioMed Res. Int. 2011, 2011, 934757. [Google Scholar] [CrossRef]
- Hoshi, H.; Sawada, T.; Uchida, M.; Saito, H.; Iijima, H.; Toda-Agetsuma, M.; Wada, T.; Yamazoe, S.; Tanaka, H.; Kimura, K.; et al. Tumor-associated MUC5AC stimulates in vivo tumorigenicity of human pancreatic cancer. Int. J. Oncol. 2011, 38, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, Y.; Zhao, T.; Li, Y.; Tian, L.; Zhao, J.; Zhang, J. Evaluation of serum MUC5AC in combination with CA19-9 for the diagnosis of pancreatic cancer. World J. Surg. Oncol. 2020, 18, 31. [Google Scholar] [CrossRef]
- Kaur, S.; Smith, L.M.; Patel, A.; Menning, M.; Watley, D.C.; Malik, S.S.; Krishn, S.R.; Mallya, K.; Aithal, A.; Sasson, A.R.; et al. A Combination of MUC5AC and CA19-9 Improves the Diagnosis of Pancreatic Cancer: A Multicenter Study. Am. J. Gastroenterol. 2017, 112, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Manne, A.; Esnakula, A.; Pawlik, T.M.; Manne, U.; Paluri, R.K.; Kasi, A.; Sohal, D.; Khushman, M.; He, K.; Cloyd, J.; et al. 389P Serum MUC5AC predicts recurrence in pancreatic ductal adenocarcinoma patients on neoadjuvant chemotherapy before resection. Ann. Oncol. 2024, 35, S156–S157. [Google Scholar] [CrossRef]
- Yang, K.S.; Ciprani, D.; O’Shea, A.; Liss, A.S.; Yang, R.; Fletcher-Mercaldo, S.; Mino-Kenudson, M.; Fernández-del Castillo, C.; Weissleder, R. Extracellular Vesicle Analysis Allows for Identification of Invasive IPMN. Gastroenterology 2021, 160, 1345–1358.e11. [Google Scholar] [CrossRef] [PubMed]
- Kahles, F.; Findeisen, H.M.; Bruemmer, D. Osteopontin: A novel regulator at the cross roads of inflammation, obesity and diabetes. Mol. Metab. 2014, 3, 384–393. [Google Scholar] [CrossRef]
- Wei, R.; Wong, J.P.C.; Kwok, H.F. Osteopontin—A promising biomarker for cancer therapy. J. Cancer 2017, 8, 2173–2183. [Google Scholar] [CrossRef]
- Koopmann, J.; Fedarko, N.S.; Jain, A.; Maitra, A.; Iacobuzio-Donahue, C.; Rahman, A.; Hruban, R.H.; Yeo, C.J.; Goggins, M. Evaluation of osteopontin as biomarker for pancreatic adenocarcinoma. Cancer Epidemiol. Biomark. Prev. 2004, 13, 487–491. [Google Scholar] [CrossRef]
- Li, J.J.; Li, H.Y.; Gu, F. Diagnostic significance of serum osteopontin level for pancreatic cancer: A meta-analysis. Genet. Test. Mol. Biomark. 2014, 18, 580–586. [Google Scholar] [CrossRef]
- Poruk, K.E.; Firpo, M.A.; Scaife, C.L.; Adler, D.G.; Emerson, L.L.; Boucher, K.M.; Mulvihill, S.J. Serum osteopontin and tissue inhibitor of metalloproteinase 1 as diagnostic and prognostic biomarkers for pancreatic adenocarcinoma. Pancreas 2013, 42, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Sokoll, L.J.; Pasay, J.J.; Rubin, A.L.; Li, H.; Bach, D.M.; Chan, D.W.; Zhang, Z. Identification of Serum Biomarker Panels for the Early Detection of Pancreatic Cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 174–182. [Google Scholar] [CrossRef]
- Rychlíková, J.; Vecka, M.; Jáchymová, M.; Macášek, J.; Hrabák, P.; Zeman, M.; Vávrová, L.; Řoupal, J.; Krechler, T.; Ák, A. Osteopontin as a discriminating marker for pancreatic cancer and chronic pancreatitis. Cancer Biomark. 2016, 17, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, Y.; Shimomura, M.; Saito, K.; Ishii, H.; Doki, Y.; Eguchi, H.; Nakatsura, T.; Itoi, T.; Kuroda, M.; Mori, M.; et al. Circulating cancer-associated extracellular vesicles as early detection and recurrence biomarkers for pancreatic cancer. Cancer Sci. 2022, 113, 3498–3509. [Google Scholar] [CrossRef]
- Takahashi, K.; Ota, Y.; Kogure, T.; Suzuki, Y.; Iwamoto, H.; Yamakita, K.; Kitano, Y.; Fujii, S.; Haneda, M.; Patel, T.; et al. Circulating extracellular vesicle-encapsulated HULC is a potential biomarker for human pancreatic cancer. Cancer Sci. 2020, 111, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Kugeratski, F.G.; Hodge, K.; Lilla, S.; McAndrews, K.M.; Zhou, X.; Hwang, R.F.; Zanivan, S.; Kalluri, R. Quantitative proteomics identifies the core proteome of exosomes with syntenin-1 as the highest abundant protein and a putative universal biomarker. Nat. Cell Biol. 2021, 23, 631–641. [Google Scholar] [CrossRef]
- Balaj, L.; Lessard, R.; Dai, L.; Cho, Y.J.; Pomeroy, S.L.; Breakefield, X.O.; Skog, J. Tumour microvesicles contain retrotransposon elements and amplified oncogene sequences. Nat. Commun. 2011, 2, 180. [Google Scholar] [CrossRef]
- Melo, S.A.; Luecke, L.B.; Kahlert, C.; Fernandez, A.F.; Gammon, S.T.; Kaye, J.; LeBleu, V.S.; Mittendorf, E.A.; Weitz, J.; Rahbari, N.; et al. Glypican-1 identifies cancer exosomes and detects early pancreatic cancer. Nature 2015, 523, 177–182. [Google Scholar] [CrossRef]
- Moutinho-Ribeiro, P.; Adem, B.; Batista, I.; Silva, M.; Silva, S.; Ruivo, C.F.; Morais, R.; Peixoto, A.; Coelho, R.; Costa-Moreira, P.; et al. Exosomal glypican-1 discriminates pancreatic ductal adenocarcinoma from chronic pancreatitis. Dig. Liver Dis. 2022, 54, 871–877. [Google Scholar] [CrossRef]
- Li, J.; Li, Y.; Chen, S.; Duan, W.; Kong, X.; Wang, Y.; Zhou, L.; Li, P.; Zhang, C.; Du, L.; et al. Highly Sensitive Exosome Detection for Early Diagnosis of Pancreatic Cancer Using Immunoassay Based on Hierarchical Surface-Enhanced Raman Scattering Substrate. Small Methods 2022, 6, 2200154. [Google Scholar] [CrossRef]
- Li, B.; Kugeratski, F.G.; Kalluri, R. A novel machine learning algorithm selects proteome signature to specifically identify cancer exosomes. eLife 2024, 12, RP90390. [Google Scholar] [CrossRef]
- Chen, J.; Yao, D.; Chen, W.; Li, Z.; Guo, Y.; Zhu, F.; Hu, X. Serum exosomal miR-451a acts as a candidate marker for pancreatic cancer. Int. J. Biol. Markers 2022, 37, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Rhim, A.D.; Mirek, E.T.; Aiello, N.M.; Maitra, A.; Bailey, J.M.; McAllister, F.; Reichert, M.; Beatty, G.L.; Rustgi, A.K.; Vonderheide, R.H.; et al. EMT and Dissemination Precede Pancreatic Tumor Formation. Cell 2012, 148, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Kim, S.Y.; Chung, S.-H.; Choi, B.; Kim, J.-E.; Yoon, D.; Jang, S.I.; Yeo, A.; Kang, H.G.; Lee, J.; et al. Tumour-associated myeloid cells expressing IL-10R2/IL-22R1 as a potential biomarker for diagnosis and recurrence of pancreatic ductal adenocarcinoma. Br. J. Cancer 2024, 130, 1979–1989. [Google Scholar] [CrossRef] [PubMed]
- Pang, T.C.Y.; Po, J.W.; Becker, T.M.; Goldstein, D.; Pirola, R.C.; Wilson, J.S.; Apte, M.V. Circulating tumour cells in pancreatic cancer: A systematic review and meta-analysis of clinicopathological implications. Pancreatology 2021, 21, 103–114. [Google Scholar] [CrossRef]
- Khoja, L.; Backen, A.; Sloane, R.; Menasce, L.; Ryder, D.; Krebs, M.; Board, R.; Clack, G.; Hughes, A.; Blackhall, F.; et al. A pilot study to explore circulating tumour cells in pancreatic cancer as a novel biomarker. Br. J. Cancer 2012, 106, 508–516. [Google Scholar] [CrossRef]
- Ankeny, J.S.; Court, C.M.; Hou, S.; Li, Q.; Song, M.; Wu, D.; Chen, J.F.; Lee, T.; Lin, M.; Sho, S.; et al. Circulating tumour cells as a biomarker for diagnosis and staging in pancreatic cancer. Br. J. Cancer 2016, 114, 1367–1375. [Google Scholar] [CrossRef]
- Wei, T.; Zhang, X.; Zhang, Q.; Yang, J.; Chen, Q.; Wang, J.; Li, X.; Chen, J.; Ma, T.; Li, G.; et al. Vimentin-positive circulating tumor cells as a biomarker for diagnosis and treatment monitoring in patients with pancreatic cancer. Cancer Lett. 2019, 452, 237–243. [Google Scholar] [CrossRef]
- Stuhr, L.K.; Madsen, K.; Johansen, A.Z.; Chen, I.M.; Hansen, C.P.; Jensen, L.H.; Hansen, T.F.; Kløve-Mogensen, K.; Nielsen, K.R.; Johansen, J.S. Combining sCD163 with CA 19-9 Increases the Predictiveness of Pancreatic Ductal Adenocarcinoma. Cancers 2023, 15, 897. [Google Scholar] [CrossRef]
- Sha, S.; Wang, Y.; Liu, M.; Liu, G.; Fan, N.; Li, Z.; Dong, W. Phaseolus vulgaris Erythroagglutinin (PHA-E)-Positive Ceruloplasmin Acts as a Potential Biomarker in Pancreatic Cancer Diagnosis. Cells 2022, 11, 2453. [Google Scholar] [CrossRef]
- Chung, K.H.; Lee, J.-C.; Lee, J.; Cho, I.-K.; Kim, J.; Jang, W.; Yoo, B.C.; Hwang, J.-H. Serum fibrinogen as a diagnostic and prognostic biomarker for pancreatic ductal adenocarcinoma. Pancreatology 2020, 20, 1465–1471. [Google Scholar] [CrossRef]
- Vreeker, G.C.M.; Hanna-Sawires, R.G.; Mohammed, Y.; Bladergroen, M.R.; Nicolardi, S.; Dotz, V.; Nouta, J.; Bonsing, B.A.; Mesker, W.E.; van der Burgt, Y.E.M.; et al. Serum N-Glycome analysis reveals pancreatic cancer disease signatures. Cancer Med. 2020, 9, 8519–8529. [Google Scholar] [CrossRef]
- Pu, N.; Chen, Q.; Zhang, J.; Yin, H.; Wang, D.; Ji, Y.; Rao, S.; Kuang, T.; Xu, X.; Wu, W.; et al. Circulating cytokines allow for identification of malignant intraductal papillary mucinous neoplasms of the pancreas. Cancer Med. 2023, 12, 3919–3930. [Google Scholar] [CrossRef]
- Jo, J.H.; Kim, S.A.; Lee, J.H.; Park, Y.R.; Kim, C.; Park, S.B.; Jung, D.E.; Lee, H.S.; Chung, M.J.; Song, S.Y. GLRX3, a novel cancer stem cell-related secretory biomarker of pancreatic ductal adenocarcinoma. BMC Cancer 2021, 21, 1241. [Google Scholar] [CrossRef] [PubMed]
- Boyd, L.N.C.; Ali, M.; Comandatore, A.; Garajova, I.; Kam, L.; Puik, J.R.; Fraga Rodrigues, S.M.; Meijer, L.L.; Le Large, T.Y.S.; Besselink, M.G.; et al. Prediction Model for Early-Stage Pancreatic Cancer Using Routinely Measured Blood Biomarkers. JAMA Netw. Open 2023, 6, e2331197. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, G.; Zhang, Y.; Cui, Y.; Liu, J. Protein Induced by Vitamin K Absence II: A Potential Biomarker to Differentiate Pancreatic Ductal Adenocarcinoma from Pancreatic Benign Lesions and Predict Vascular Invasion. J. Clin. Med. 2023, 12, 2769. [Google Scholar] [CrossRef]
- Jiang, S.-H.; Liu, D.; Hu, L.-P.; Zhang, S.; Yu, Y.; Sun, Y.-W.; Ji, J.; Zhang, Z.-G. Modeling of cancer-related body-wide effects identifies LTB4 as a diagnostic biomarker for pancreatic cancer. Ebiomedicine 2022, 80, 104050. [Google Scholar] [CrossRef] [PubMed]
- Digomann, D.; Heiduk, M.; Reiche, C.; Glück, J.; Kahlert, C.; Mirtschink, P.; Klimova, A.; Bösch, F.; Tonn, T.; Gaedcke, J.; et al. Serum immune checkpoint profiling identifies soluble CD40 as a biomarker for pancreatic cancer. NPJ Precis. Oncol. 2023, 7, 104. [Google Scholar] [CrossRef]
- Yablecovitch, D.; Nadler, M.; Ben-Horin, S.; Picard, O.; Yavzori, M.; Fudim, E.; Duchan, M.T.; Sakhnini, E.; Lang, A.; Lahav, M.; et al. Serum matrix metalloproteinase-7, Syndecan-1, and CA 19-9 as a biomarker panel for diagnosis of pancreatic ductal adenocarcinoma. Cancer Med. 2024, 13, e70144. [Google Scholar] [CrossRef]
- Martínez-Bosch, N.; Cristóbal, H.; Iglesias, M.; Gironella, M.; Barranco, L.; Visa, L.; Calafato, D.; Jiménez-Parrado, S.; Earl, J.; Carrato, A.; et al. Soluble AXL is a novel blood marker for early detection of pancreatic ductal adenocarcinoma and differential diagnosis from chronic pancreatitis. EBioMedicine 2022, 75, 103797. [Google Scholar] [CrossRef]
- Boyd, L.N.C.; Ali, M.; Kam, L.; Puik, J.R.; Rodrigues, S.M.F.; Zwart, E.S.; Daams, F.; Zonderhuis, B.M.; Meijer, L.L.; Le Large, T.Y.S.; et al. The Diagnostic Value of the CA19-9 and Bilirubin Ratio in Patients with Pancreatic Cancer, Distal Bile Duct Cancer and Benign Periampullary Diseases, a Novel Approach. Cancers 2022, 14, 344. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.; Hong, S.S.; Jung, K.H.; Kang, S.; Park, M.S.; Kang, S.; Kim, H.S.; Mai, V.H.; Kim, J.; Lee, H.; et al. A Serum Marker for Early Pancreatic Cancer With a Possible Link to Diabetes. J. Natl. Cancer Inst. 2022, 114, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Montoya Mira, J.L.; Quentel, A.; Patel, R.K.; Keith, D.; Sousa, M.; Minnier, J.; Kingston, B.R.; David, L.; Esener, S.C.; Sears, R.C.; et al. Early detection of pancreatic cancer by a high-throughput protease-activated nanosensor assay. Sci. Transl. Med. 2025, 17, eadq3110. [Google Scholar] [CrossRef]
- Sato, S.; Nakagawa, M.; Terashima, T.; Morinaga, S.; Miyagi, Y.; Yoshida, E.; Yoshimura, T.; Seiki, M.; Kaneko, S.; Ueno, M.; et al. EphA2 Proteolytic Fragment as a Sensitive Diagnostic Biomarker for Very Early-stage Pancreatic Ductal Carcinoma. Cancer Res. Commun. 2023, 3, 1862–1874. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Ye, M.; Lin, C.; Hu, M.; Wang, Y.; Lou, Y.; Kong, Q.; Zhang, J.; Li, J.; Zhang, Y.; et al. Mass cytometry-based peripheral blood analysis as a novel tool for early detection of solid tumours: A multicentre study. Gut 2023, 72, 996–1006. [Google Scholar] [CrossRef]
- Odaka, H.; Hiemori, K.; Shimoda, A.; Akiyoshi, K.; Tateno, H. CD63-positive extracellular vesicles are potential diagnostic biomarkers of pancreatic ductal adenocarcinoma. BMC Gastroenterol. 2022, 22, 153. [Google Scholar] [CrossRef]
- Hong, L.; Xu, L.; Jin, L.; Xu, K.; Tang, W.; Zhu, Y.; Qiu, X.; Wang, J. Exosomal circular RNA hsa_circ_0006220, and hsa_circ_0001666 as biomarkers in the diagnosis of pancreatic cancer. J. Clin. Lab. Anal. 2022, 36, e24447. [Google Scholar] [CrossRef]
- Xiao, D.; Dong, Z.; Zhen, L.; Xia, G.; Huang, X.; Wang, T.; Guo, H.; Yang, B.; Xu, C.; Wu, W.; et al. Combined Exosomal GPC1, CD82, and Serum CA19-9 as Multiplex Targets: A Specific, Sensitive, and Reproducible Detection Panel for the Diagnosis of Pancreatic Cancer. Mol. Cancer Res. 2020, 18, 300–310. [Google Scholar] [CrossRef]
- Khan, I.A.; Rashid, S.; Singh, N.; Rashid, S.; Singh, V.; Gunjan, D.; Das, P.; Dash, N.R.; Pandey, R.M.; Chauhan, S.S.; et al. Panel of serum miRNAs as potential non-invasive biomarkers for pancreatic ductal adenocarcinoma. Sci. Rep. 2021, 11, 2824. [Google Scholar] [CrossRef]
- Shi, W.; Wartmann, T.; Accuffi, S.; Al-Madhi, S.; Perrakis, A.; Kahlert, C.; Link, A.; Venerito, M.; Keitel-Anselmino, V.; Bruns, C.; et al. Integrating a microRNA signature as a liquid biopsy-based tool for the early diagnosis and prediction of potential therapeutic targets in pancreatic cancer. Br. J. Cancer 2024, 130, 125–134. [Google Scholar] [CrossRef]
- Dittmar, R.L.; Liu, S.; Tai, M.C.; Rajapakshe, K.; Huang, Y.; Longton, G.; DeCapite, C.; Hurd, M.W.; Paris, P.L.; Kirkwood, K.S.; et al. Plasma miRNA Biomarkers in Limited Volume Samples for Detection of Early-stage Pancreatic Cancer. Cancer Prev. Res. 2021, 14, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Cai, Y.; Chen, X.; Zhu, Y.; Cai, J. Circulating MiR-1290 as a potential diagnostic and disease monitoring biomarker of human gastrointestinal tumors. BMC Cancer 2021, 21, 989. [Google Scholar] [CrossRef]
- Kawai, M.; Fukuda, A.; Otomo, R.; Obata, S.; Minaga, K.; Asada, M.; Umemura, A.; Uenoyama, Y.; Hieda, N.; Morita, T.; et al. Early detection of pancreatic cancer by comprehensive serum miRNA sequencing with automated machine learning. Br. J. Cancer 2024, 131, 1158–1168. [Google Scholar] [CrossRef]
- Jin, F.; Yang, L.; Wang, W.; Yuan, N.; Zhan, S.; Yang, P.; Chen, X.; Ma, T.; Wang, Y. A novel class of tsRNA signatures as biomarkers for diagnosis and prognosis of pancreatic cancer. Mol. Cancer 2021, 20, 95. [Google Scholar] [CrossRef]
- Henriksen, S.D.; Stubbe, B.E.; Madsen, P.H.; Johansen, J.S.; Jensen, B.V.; Hansen, C.P.; Johansen, M.N.; Pedersen, I.S.; Krarup, H.; Thorlacius-Ussing, O. Cell-free DNA promoter hypermethylation as a diagnostic marker for pancreatic ductal adenocarcinoma—An external validation study. Pancreatology 2021, 21, 1081–1091. [Google Scholar] [CrossRef] [PubMed]
- Guler, G.D.; Ning, Y.; Ku, C.-J.; Phillips, T.; McCarthy, E.; Ellison, C.K.; Bergamaschi, A.; Collin, F.; Lloyd, P.; Scott, A.; et al. Detection of early stage pancreatic cancer using 5-hydroxymethylcytosine signatures in circulating cell free DNA. Nat. Commun. 2020, 11, 5270. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Seufert, I.; Al-Shaheri, F.N.; Kurilov, R.; Bauer, A.S.; Manoochehri, M.; Moskalev, E.A.; Brors, B.; Tjaden, C.; Giese, N.A.; et al. DNA-methylation signature accurately differentiates pancreatic cancer from chronic pancreatitis in tissue and plasma. Gut 2023, 72, 2344–2353. [Google Scholar] [CrossRef]
- Haan, D.; Bergamaschi, A.; Friedl, V.; Guler, G.D.; Ning, Y.; Reggiardo, R.; Kesling, M.; Collins, M.; Gibb, B.; Hazen, K.; et al. Epigenomic Blood-Based Early Detection of Pancreatic Cancer Employing Cell-Free DNA. Clin. Gastroenterol. Hepatol. 2023, 21, 1802–1809.e6. [Google Scholar] [CrossRef]
- Abe, T.; Koi, C.; Kohi, S.; Song, K.B.; Tamura, K.; Macgregor-Das, A.; Kitaoka, N.; Chuidian, M.; Ford, M.; Dbouk, M.; et al. Gene Variants That Affect Levels of Circulating Tumor Markers Increase Identification of Patients With Pancreatic Cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 1161–1169.e1165. [Google Scholar] [CrossRef]
- Majumder, S.; Taylor, W.R.; Foote, P.H.; Berger, C.K.; Wu, C.W.; Mahoney, D.W.; Bamlet, W.R.; Burger, K.N.; Postier, N.; de la Fuente, J.; et al. High Detection Rates of Pancreatic Cancer Across Stages by Plasma Assay of Novel Methylated DNA Markers and CA19-9. Clin. Cancer Res. 2021, 27, 2523–2532. [Google Scholar] [CrossRef]
- Wu, H.; Guo, S.; Liu, X.; Li, Y.; Su, Z.; He, Q.; Liu, X.; Zhang, Z.; Yu, L.; Shi, X.; et al. Noninvasive detection of pancreatic ductal adenocarcinoma using the methylation signature of circulating tumour DNA. BMC Med. 2022, 20, 458. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Dbouk, M.; Yoshida, T.; Saba, H.; Abou Diwan, E.; Yoshida, K.; Dbouk, A.; Blackford, A.L.; Lin, M.T.; Lennon, A.M.; et al. Using Tumor Marker Gene Variants to Improve the Diagnostic Accuracy of DUPAN-2 and Carbohydrate Antigen 19-9 for Pancreatic Cancer. J. Clin. Oncol. 2024, 42, 2196–2206. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Ren, S.; Li, C.; Guo, K.; Lu, Z.; Tian, L.; He, J.; Zhang, K.; Cao, Y.; Liu, S.; et al. Biomarkers for pancreatic cancer based on tissue and serum metabolomics analysis in a multicenter study. Cancer Med. 2023, 12, 5158–5171. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, U.M.; Oehrle, B.; Sirtl, S.; Alnatsha, A.; Goni, E.; Regel, I.; Beyer, G.; Vornhülz, M.; Vielhauer, J.; Chromik, A.; et al. Independent Validation and Assay Standardization of Improved Metabolic Biomarker Signature to Differentiate Pancreatic Ductal Adenocarcinoma From Chronic Pancreatitis. Gastroenterology 2022, 163, 1407–1422. [Google Scholar] [CrossRef]
- Zhang, C.; Al-Shaheri, F.N.; Alhamdani, M.S.S.; Bauer, A.S.; Hoheisel, J.D.; Schenk, M.; Hinz, U.; Goedecke, P.; Al-Halabi, K.; Büchler, M.W.; et al. Blood-Based Diagnosis and Risk Stratification of Patients with Pancreatic Intraductal Papillary Mucinous Neoplasm (IPMN). Clin. Cancer Res. 2023, 29, 1535–1545. [Google Scholar] [CrossRef]
- Tanaka, H.; Tamura, K.; Abe, T.; Yoshida, T.; Macgregor-Das, A.; Dbouk, M.; Blackford, A.L.; Borges, M.; Lennon, A.M.; He, J.; et al. Serum Carboxypeptidase Activity and Genotype-Stratified CA19-9 to Detect Early-Stage Pancreatic Cancer. Clin. Gastroenterol. Hepatol. 2022, 20, 2267–2275.e2. [Google Scholar] [CrossRef]
- Yang, Z.; LaRiviere, M.J.; Ko, J.; Till, J.E.; Christensen, T.; Yee, S.S.; Black, T.A.; Tien, K.; Lin, A.; Shen, H.; et al. A Multianalyte Panel Consisting of Extracellular Vesicle miRNAs and mRNAs, cfDNA, and CA19-9 Shows Utility for Diagnosis and Staging of Pancreatic Ductal Adenocarcinoma. Clin. Cancer Res. 2020, 26, 3248–3258. [Google Scholar] [CrossRef]
- Gu, J.; Huang, W.; Wang, X.; Zhang, J.; Tao, T.; Zheng, Y.; Liu, S.; Yang, J.; Chen, Z.-S.; Cai, C.-Y.; et al. Hsa-miR-3178/RhoB/PI3K/Akt, a novel signaling pathway regulates ABC transporters to reverse gemcitabine resistance in pancreatic cancer. Mol. Cancer 2022, 21, 112. [Google Scholar] [CrossRef]
- Liu, M.; Zhang, Y.; Yang, J.; Zhan, H.; Zhou, Z.; Jiang, Y.; Shi, X.; Fan, X.; Zhang, J.; Luo, W.; et al. Zinc-Dependent Regulation of ZEB1 and YAP1 Coactivation Promotes Epithelial-Mesenchymal Transition Plasticity and Metastasis in Pancreatic Cancer. Gastroenterology 2021, 160, 1771–1783.e1. [Google Scholar] [CrossRef]
- Sicard, F.; Gayral, M.; Lulka, H.; Buscail, L.; Cordelier, P. Targeting miR-21 for the Therapy of Pancreatic Cancer. Mol. Ther. 2013, 21, 986–994. [Google Scholar] [CrossRef]
- Peng, C.; Wang, J.; Gao, W.; Huang, L.; Liu, Y.; Li, X.; Li, Z.; Yu, X. Meta-analysis of the Diagnostic Performance of Circulating MicroRNAs for Pancreatic Cancer. Int. J. Med. Sci. 2021, 18, 660–671. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Q.; Zhang, Y.; Xu, Y.; Yang, Y.; Zhang, Z.; Zhou, Y.; Zhang, S.; Zhou, L.; Wan, X.; Yang, X.; et al. tiRNA-Val-CAC-2 interacts with FUBP1 to promote pancreatic cancer metastasis by activating c-MYC transcription. Oncogene 2024, 43, 1274–1287. [Google Scholar] [CrossRef]
- Goodarzi, H.; Liu, X.; Nguyen, H.C.B.; Zhang, S.; Fish, L.; Tavazoie, S.F. Endogenous tRNA-Derived Fragments Suppress Breast Cancer Progression via YBX1 Displacement. Cell 2015, 161, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Shi, X.; Shen, J.; Gao, S.; Wang, H.; Shen, S.; Pan, Y.; Li, B.; Xu, X.; Shao, Z.; et al. Preoperative detection of KRAS G12D mutation in ctDNA is a powerful predictor for early recurrence of resectable PDAC patients. Br. J. Cancer 2020, 122, 857–867. [Google Scholar] [CrossRef]
- Patel, N.; Petrinic, T.; Silva, M.; Soonawalla, Z.; Reddy, S.; Gordon-Weeks, A. The Diagnostic Accuracy of Mutant KRAS Detection from Pancreatic Secretions for the Diagnosis of Pancreatic Cancer: A Meta-Analysis. Cancers 2020, 12, 2353. [Google Scholar] [CrossRef] [PubMed]
- Rozeveld, C.N.; Johnson, K.M.; Zhang, L.; Razidlo, G.L. KRAS Controls Pancreatic Cancer Cell Lipid Metabolism and Invasive Potential through the Lipase HSL. Cancer Res. 2020, 80, 4932–4945. [Google Scholar] [CrossRef]
- Wolrab, D.; Jirásko, R.; Cífková, E.; Höring, M.; Mei, D.; Chocholoušková, M.; Peterka, O.; Idkowiak, J.; Hrnčiarová, T.; Kuchař, L.; et al. Lipidomic profiling of human serum enables detection of pancreatic cancer. Nat. Commun. 2022, 13, 124. [Google Scholar] [CrossRef]
- Guo, M.; Luo, G.; Lu, R.; Shi, W.; Cheng, H.; Lu, Y.; Jin, K.; Yang, C.; Wang, Z.; Long, J.; et al. Distribution of Lewis and Secretor polymorphisms and corresponding CA19-9 antigen expression in a Chinese population. FEBS Open Bio 2017, 7, 1660–1671. [Google Scholar] [CrossRef]
- Wannhoff, A.; Hov, J.R.; Folseraas, T.; Rupp, C.; Friedrich, K.; Anmarkrud, J.A.; Weiss, K.H.; Sauer, P.; Schirmacher, P.; Boberg, K.M.; et al. FUT2 and FUT3 genotype determines CA19-9 cut-off values for detection of cholangiocarcinoma in patients with primary sclerosing cholangitis. J. Hepatol. 2013, 59, 1278–1284. [Google Scholar] [CrossRef]
- Luo, G.; Guo, M.; Jin, K.; Liu, Z.; Liu, C.; Cheng, H.; Lu, Y.; Long, J.; Liu, L.; Xu, J.; et al. Optimize CA19-9 in detecting pancreatic cancer by Lewis and Secretor genotyping. Pancreatology 2016, 16, 1057–1062. [Google Scholar] [CrossRef]
- Dbouk, M.; Abe, T.; Koi, C.; Ando, Y.; Saba, H.; Abou Diwan, E.; MacGregor-Das, A.; Blackford, A.L.; Mocci, E.; Beierl, K.; et al. Diagnostic Performance of a Tumor Marker Gene Test to Personalize Serum CA19-9 Reference Ranges. Clin. Cancer Res. 2023, 29, 4178–4185. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.; Yan, W.; Liu, S.; Ren, W.; Lyu, M.; Wang, S. Trypsin enhances aptamer screening: A novel method for targeting proteins. Anal. Biochem. 2018, 561–562, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Hashemi Tabar, G. DNA Aptamers Selected as Molecular Probes for Diagnosis of cancereous cells. World Appl. Sci. J. 2010, 8, 16–21. [Google Scholar]
- Izabella Abreu de Melo, M.; Rodrigues Correa, C.; da Silva Cunha, P.; Miranda de Góes, A.; Assis Gomes, D.; Silva Ribeiro de Andrade, A. DNA aptamers selection for carcinoembryonic antigen (CEA). Bioorg Med. Chem. Lett. 2020, 30, 127278. [Google Scholar] [CrossRef]
- Wang, Q.-L.; Cui, H.-F.; Du, J.-F.; Lv, Q.-Y.; Song, X. In silico post-SELEX screening and experimental characterizations for acquisition of high affinity DNA aptamers against carcinoembryonic antigen. RSC Adv. 2019, 9, 6328–6334. [Google Scholar] [CrossRef]
- Yarizadeh, K.; Behbahani, M.; Mohabatkar, H.; Noorbakhsh, A. Computational analysis and optimization of carcinoembryonic antigen aptamers and experimental evaluation. J. Biotechnol. 2019, 306, 1–8. [Google Scholar] [CrossRef]
- Yunussova, N.; Sypabekova, M.; Zhumabekova, Z.; Matkarimov, B.; Kanayeva, D. A Novel ssDNA Aptamer Targeting Carcinoembryonic Antigen: Selection and Characterization. Biology 2022, 11, 1540. [Google Scholar] [CrossRef]
- Ferreira, C.S.M.; Matthews, C.S.; Missailidis, S. DNA Aptamers That Bind to MUC1 Tumour Marker: Design and Characterization of MUC1-Binding Single-Stranded DNA Aptamers. Tumor Biol. 2006, 27, 289–301. [Google Scholar] [CrossRef]
- Ferreira, C.S.; Cheung, M.C.; Missailidis, S.; Bisland, S.; Gariépy, J. Phototoxic aptamers selectively enter and kill epithelial cancer cells. Nucleic Acids Res. 2009, 37, 866–876. [Google Scholar] [CrossRef]
- Hu, Y.; Duan, J.; Zhan, Q.; Wang, F.; Lu, X.; Yang, X.-D. Novel MUC1 Aptamer Selectively Delivers Cytotoxic Agent to Cancer Cells In Vitro. PLoS ONE 2012, 7, e31970. [Google Scholar] [CrossRef]
- Scoville, D.J.; Uhm, T.K.B.; Shallcross, J.A.; Whelan, R.J. Selection of DNA Aptamers for Ovarian Cancer Biomarker CA125 Using One-Pot SELEX and High-Throughput Sequencing. J. Nucleic Acids 2017, 2017, 9879135. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, P.; Sachan, M.; Nara, S. Novel ssDNA Ligand Against Ovarian Cancer Biomarker CA125 with Promising Diagnostic Potential. Front. Chem. 2020, 8, 400. [Google Scholar] [CrossRef]
- Gedi, V.; Song, C.K.; Kim, G.B.; Lee, J.O.; Oh, E.; Shin, B.S.; Jung, M.; Shim, J.; Lee, H.; Kim, Y.-P. Sensitive on-chip detection of cancer antigen 125 using a DNA aptamer/carbon nanotube network platform. Sens. Actuators B Chem. 2018, 256, 89–97. [Google Scholar] [CrossRef]
- Lamberti, I.; Scarano, S.; Esposito, C.L.; Antoccia, A.; Antonini, G.; Tanzarella, C.; De Franciscis, V.; Minunni, M. In vitro selection of RNA aptamers against CA125 tumor marker in ovarian cancer and its study by optical biosensing. Methods 2016, 97, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Meirinho, S.G.; Dias, L.s.G.; Peres, A.n.M.; Rodrigues, L.g.R. Electrochemical aptasensor for human osteopontin detection using a DNA aptamer selected by SELEX. Anal. Chim. Acta 2017, 987, 25–37. [Google Scholar] [CrossRef]
- Bhattacharya, S.D.; Mi, Z.; Kim, V.M.; Guo, H.; Talbot, L.J.; Kuo, P.C. Osteopontin regulates epithelial mesenchymal transition-associated growth of hepatocellular cancer in a mouse xenograft model. Ann. Surg. 2012, 255, 319–325. [Google Scholar] [CrossRef]
- Yoo, K.; Cho, H.S.; Kim, J.; Shin, M.; Chu, J.S.; Jang, S.; Bae, H.J.; Jung, H.S.; Kang, H.; Jun, B.H. Aptamer-Conjugated Multi-Quantum Dot-Embedded Silica Nanoparticles for Lateral Flow Immunoassay. Biosensors 2025, 15, 54. [Google Scholar] [CrossRef]
- Xia, J.; Li, Y.; Xin, Y.; Kang, L.; Lu, D. Early detection for carbohydrate antigen-19-9 based on surface enhanced Raman spectroscopy aptamer sensor. Microchem. J. 2024, 207, 111750. [Google Scholar] [CrossRef]
- Lin, F.; Li, X.; Zhang, J.; Zhang, H.; Zhang, Z.; Hou, L.; Shen, B.; Jin, L. Ratiometric electrochemical aptasensor based on functionalized graphene nanocomposites for detection of CA19-9. Anal. Sci. 2025, 1–14. [Google Scholar] [CrossRef]
- Lan, L.; Yao, Y.; Ping, J.; Ying, Y. Recent Progress in Nanomaterial-Based Optical Aptamer Assay for the Detection of Food Chemical Contaminants. ACS Appl. Mater. Interfaces 2017, 9, 23287–23301. [Google Scholar] [CrossRef]
- Nguyen, V.-T.; Kwon, Y.S.; Gu, M.B. Aptamer-based environmental biosensors for small molecule contaminants. Curr. Opin. Biotechnol. 2017, 45, 15–23. [Google Scholar] [CrossRef]
- Luo, C.-P.; Wen, W.; Lin, F.-e.; Zhang, X.; Gu, H.; Wang, S. Simplified aptamer-based colorimetric method using unmodified gold nanoparticles for the detection of carcinoma embryonic antigen. RSC Adv. 2015, 5, 10994–10999. [Google Scholar] [CrossRef]
- Shahbazi, N.; Hosseinkhani, S.; Ranjbar, B. A facile and rapid aptasensor based on split peroxidase DNAzyme for visual detection of carcinoembryonic antigen in saliva. Sens. Actuators B Chem. 2017, 253, 794–803. [Google Scholar] [CrossRef]
- Liu, B.; Zhou, P.; Wang, K.; Gong, S.; Luan, M.; Li, N.; Tang, B. Avoiding False Positive Signals: A Powerful and Reliable Au–Se Dual-Color Probe. ACS Sens. 2021, 6, 1949–1955. [Google Scholar] [CrossRef]
- Liang, K.; Zhai, S.; Zhang, Z.; Fu, X.; Shao, J.; Lin, Z.; Qiu, B.; Chen, G.N. Ultrasensitive colorimetric carcinoembryonic antigen biosensor based on hyperbranched rolling circle amplification. Analyst 2014, 139, 4330–4334. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Cui, M.; Zhang, Y.; Jiang, L.; Liu, H.; Liu, Z. A colorimetric aptasensing assay with adjustable color mutation points for threshold-readout detection of carcinoembryonic antigen. Sens. Actuators B Chem. 2022, 350, 130857. [Google Scholar] [CrossRef]
- Li, P.; Li, W.; Xie, Z.; Zhan, H.; Deng, L.; Huang, J. A label-free and signal-amplifiable assay method for colorimetric detection of carcinoembryonic antigen. Biotechnol. Bioeng. 2022, 119, 504–512. [Google Scholar] [CrossRef]
- Miao, H.; Wang, L.; Zhuo, Y.; Zhou, Z.; Yang, X. Label-free fluorimetric detection of CEA using carbon dots derived from tomato juice. Biosens. Bioelectron. 2016, 86, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhuo, Y.; Zhu, S.; Luo, Y.; Feng, Y.; Xu, Y. Selectively assaying CEA based on a creative strategy of gold nanoparticles enhancing silver nanoclusters’ fluorescence. Biosens. Bioelectron. 2015, 64, 345–351. [Google Scholar] [CrossRef]
- Xu, S.; Feng, X.; Gao, T.; Liu, G.; Mao, Y.; Lin, J.; Yu, X.; Luo, X. Aptamer induced multicoloured Au NCs-MoS2 “switch on” fluorescence resonance energy transfer biosensor for dual color simultaneous detection of multiple tumor markers by single wavelength excitation. Anal. Chim. Acta 2017, 983, 173–180. [Google Scholar] [CrossRef]
- Wu, Z.; Li, H.; Liu, Z. An aptasensor for carcinoembryonic antigen based on upconversion fluorescence resonance energy transfer. Sens. Actuators B Chem. 2015, 206, 531–537. [Google Scholar] [CrossRef]
- Wang, Y.; Wei, Z.; Luo, X.; Wan, Q.; Qiu, R.; Wang, S. An ultrasensitive homogeneous aptasensor for carcinoembryonic antigen based on upconversion fluorescence resonance energy transfer. Talanta 2019, 195, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Shi, L.; Sun, D.-e.; Li, P.; Liu, Z. Fluorescence resonance energy transfer biosensor between upconverting nanoparticles and palladium nanoparticles for ultrasensitive CEA detection. Biosens. Bioelectron. 2016, 86, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.-M.; Feng, Z.; Zhou, J.; Fang, B.-Y.; Qi, X.-X.; Ma, Z.-Y.; Liu, B.; Zhao, Y.-D.; Hu, X.-B. Capillary electrophoresis-chemiluminescence detection for carcino-embryonic antigen based on aptamer/graphene oxide structure. Biosens. Bioelectron. 2015, 64, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.-M.; Feng, Z.; Zhou, J.; Fang, B.-Y.; Ma, Z.-Y.; Liu, B.; Zhao, Y.-D.; Hu, X.-B. Quantum dot-modified aptamer probe for chemiluminescence detection of carcino-embryonic antigen using capillary electrophoresis. Sens. Actuators B Chem. 2015, 210, 158–164. [Google Scholar] [CrossRef]
- Man, J.; Dong, J.; Wang, Y.; He, L.; Yu, S.; Yu, F.; Wang, J.; Tian, Y.; Liu, L.; Han, R.; et al. Simultaneous Detection of VEGF and CEA by Time-Resolved Chemiluminescence Enzyme-Linked Aptamer Assay. Int. J. Nanomed. 2020, 15, 9975–9985. [Google Scholar] [CrossRef]
- Han, R.; Sun, Y.; Dai, Y.; Gao, D.; Wang, X.; Luo, C. A chemiluminescence aptasensor for sensitive detection of carcinoembryonic antigen based on dual aptamer-conjugates biorecognition. Sens. Actuators B Chem. 2021, 326, 128833. [Google Scholar] [CrossRef]
- Shu, Q.; Zhu, Y.; Xiao, Y.; Chen, K.; Mai, X.; Zheng, X.; Yan, X. A novel chemiluminescence biosensor based on dual aptamers bound nanoparticles with multi-site signal amplification for sensitive detection of carcinoembryonic antigen. Microchem. J. 2022, 179, 107482. [Google Scholar] [CrossRef]
- Sun, Y.; Hou, Y.; Cao, T.; Luo, C.; Wei, Q. A Chemiluminescence Sensor for the Detection of α-Fetoprotein and Carcinoembryonic Antigen Based on Dual-Aptamer Functionalized Magnetic Silicon Composite. Anal. Chem. 2023, 95, 7387–7395. [Google Scholar] [CrossRef]
- Wang, D.; Li, Y.; Lin, Z.; Qiu, B.; Guo, L. Surface-Enhanced Electrochemiluminescence of Ru@SiO2 for Ultrasensitive Detection of Carcinoembryonic Antigen. Anal. Chem. 2015, 87, 5966–5972. [Google Scholar] [CrossRef]
- Zhang, X.; Bao, N.; Luo, X.; Ding, S.-N. Patchy gold coated Fe3O4 nanospheres with enhanced catalytic activity applied for paper-based bipolar electrode-electrochemiluminescence aptasensors. Biosens. Bioelectron. 2018, 114, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Tan, L.; Jie, G. Ultrasensitive electrochemiluminescence biosensor for the detection of carcinoembryonic antigen based on multiple amplification and a DNA walker. Sens. Actuators B Chem. 2021, 333, 129586. [Google Scholar] [CrossRef]
- Guo, C.; Su, F.; Song, Y.; Hu, B.; Wang, M.; He, L.; Peng, D.; Zhang, Z. Aptamer-Templated Silver Nanoclusters Embedded in Zirconium Metal-Organic Framework for Bifunctional Electrochemical and SPR Aptasensors toward Carcinoembryonic Antigen. ACS Appl. Mater. Interfaces 2017, 9, 41188–41199. [Google Scholar] [CrossRef]
- Erkal-Aytemur, A.; Şahin, S.; Üstündağ, Z.; Mülazımoğlu, İ.E.; Caglayan, M.O. Determination of carcinoembryonic antigen (CEA) by surface plasmon resonance-enhanced total internal reflection ellipsometry (SPRe-TIRE). Instrum. Sci. Technol. 2024, 52, 203–219. [Google Scholar] [CrossRef]
- Zhang, R.; Liu, L.; Mao, D.; Luo, D.; Cao, F.; Chen, Q.; Chen, J. Construction of electrochemical aptasensor of carcinoembryonic antigen based on toehold-aided DNA recycling signal amplification. Bioelectrochemistry 2020, 133, 107492. [Google Scholar] [CrossRef]
- Niu, C.; Lin, X.; Jiang, X.; Guo, F.; Liu, J.; Liu, X.; Huang, H.; Huang, Y. An electrochemical aptasensor for highly sensitive detection of CEA based on exonuclease III and hybrid chain reaction dual signal amplification. Bioelectrochemistry 2022, 143, 107986. [Google Scholar] [CrossRef]
- Wang, Q.-L.; Cui, H.-F.; Song, X.; Fan, S.-F.; Chen, L.-L.; Li, M.-M.; Li, Z.-Y. A label-free and lectin-based sandwich aptasensor for detection of carcinoembryonic antigen. Sens. Actuators B Chem. 2018, 260, 48–54. [Google Scholar] [CrossRef]
- Yunussova, N.; Tilegen, M.; Pham, T.T.; Kanayeva, D. Rapid detection of carcinoembryonic antigen by means of an electrochemical aptasensor. iScience 2024, 27, 109637. [Google Scholar] [CrossRef]
- Xu, L.; Liu, Z.; Lei, S.; Huang, D.; Zou, L.; Ye, B. A sandwich-type electrochemical aptasensor for the carcinoembryonic antigen via biocatalytic precipitation amplification and by using gold nanoparticle composites. Microchim. Acta 2019, 186, 473. [Google Scholar] [CrossRef]
- Bahri, M.; Fredj, Z.; Qin, P.; Sawan, M. DNA-Coupled AuNPs@ CuMOF for Sensitive Electrochemical Detection of Carcinoembryonic Antigen. ACS Appl. Nano Mater. 2024, 7, 11921–11930. [Google Scholar] [CrossRef]
- Wang, X.; Qin, Z.; Zhang, F.; Li, C.; Yuan, X.; Yang, J.; Yang, H. Label-free electrochemical biosensor based on dual amplification of gold nanoparticles and polycaprolactones for CEA detection. Talanta 2024, 278, 126468. [Google Scholar] [CrossRef] [PubMed]
- Zhai, X.-J.; Wang, Q.-L.; Cui, H.-F.; Song, X.; Lv, Q.-Y.; Guo, Y. A DNAzyme-catalyzed label-free aptasensor based on multifunctional dendrimer-like DNA assembly for sensitive detection of carcinoembryonic antigen. Biosens. Bioelectron. 2021, 194, 113618. [Google Scholar] [CrossRef]
- Zhang, K.; Pei, M.; Cheng, Y.; Zhang, Z.; Niu, C.; Liu, X.; Liu, J.; Guo, F.; Huang, H.; Lin, X. A novel electrochemical aptamer biosensor based on tetrahedral DNA nanostructures and catalytic hairpin assembly for CEA detection. J. Electroanal. Chem. 2021, 898, 115635. [Google Scholar] [CrossRef]
- Li, N.; Zong, S.; Zhang, Y.; Wang, Z.; Wang, Y.; Zhu, K.; Yang, K.; Wang, Z.; Chen, B.; Cui, Y. A SERS-colorimetric dual-mode aptasensor for the detection of cancer biomarker MUC1. Anal. Bioanal. Chem. 2020, 412, 5707–5718. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Wu, X.; Chen, H.; Chen, S.; Zeng, Y.; Zhang, H.; Yu, Y. Colorimetric aptasensor based on magnetic beads and gold nanoparticles for detecting mucin 1. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2024, 315, 124236. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, S.; Huang, H.; Mao, G.; Ji, X.; He, Z. Silicon nanodot-based aptasensor for fluorescence turn-on detection of mucin 1 and targeted cancer cell imaging. Anal. Chim. Acta 2018, 1035, 154–160. [Google Scholar] [CrossRef]
- Wang, W.; Wang, Y.; Pan, H.; Cheddah, S.; Yan, C. Aptamer-based fluorometric determination for mucin 1 using gold nanoparticles and carbon dots. Microchim. Acta 2019, 186, 544. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, Y.; Zhao, Q.; Situ, B.; Zhao, J.; Luo, S.; Li, B.; Yan, X.; Vadgama, P.; Su, L.; et al. Bifunctional aptamer-mediated catalytic hairpin assembly for the sensitive and homogenous detection of rare cancer cells. Anal. Chim. Acta 2018, 1029, 58–64. [Google Scholar] [CrossRef]
- Zhang, J.; Shi, J.; Liu, W.; Zhang, K.; Zhao, H.; Zhang, H.; Zhang, Z. A simple, specific and “on-off” type MUC1 fluorescence aptasensor based on exosomes for detection of breast cancer. Sens. Actuators B Chem. 2018, 276, 552–559. [Google Scholar] [CrossRef]
- Xie, F.-T.; Li, Y.-L.; Guan, Y.; Liu, J.-W.; Yang, T.; Mao, G.-J.; Wu, Y.; Yang, Y.-H.; Hu, R. Ultrasensitive dual-signal electrochemical ratiometric aptasensor based on Co-MOFs with intrinsic self-calibration property for Mucin 1. Anal. Chim. Acta 2022, 1225, 340219. [Google Scholar] [CrossRef]
- Paimard, G.; Shahlaei, M.; Moradipour, P.; Karamali, V.; Arkan, E. Impedimetric aptamer based determination of the tumor marker MUC1 by using electrospun core-shell nanofibers. Microchim. Acta 2019, 187, 5. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, G.; Pakchin, P.S.; Mousivand, M.; Bolhasani, A.J.; Mota, A. A Gold Nanoparticle-based Aptasensor for Specific Detection of CA125: An Aptasensor for CA125. Galen. Med. J. 2024, 13, e3180. [Google Scholar] [CrossRef]
- Tripathi, P.; Kumar, A.; Sachan, M.; Gupta, S.; Nara, S. Aptamer-gold nanozyme based competitive lateral flow assay for rapid detection of CA125 in human serum. Biosens. Bioelectron. 2020, 165, 112368. [Google Scholar] [CrossRef] [PubMed]
- Hamd-Ghadareh, S.; Salimi, A.; Fathi, F.; Bahrami, S. An amplified comparative fluorescence resonance energy transfer immunosensing of CA125 tumor marker and ovarian cancer cells using green and economic carbon dots for bio-applications in labeling, imaging and sensing. Biosens. Bioelectron. 2017, 96, 308–316. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, Y.; Deng, H.; Xiong, X.; Zhang, H.; Liang, T.; Li, C. An aptamer biosensor for CA125 quantification in human serum based on upconversion luminescence resonance energy transfer. Microchem. J. 2021, 161, 105761. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, W.; Yu, Y. Tetrahedral DNA nanostructure enhanced toehold-mediated strand displacement for highly sensitive electrochemiluminescence assay of CA125. Bioelectrochemistry 2024, 155, 108572. [Google Scholar] [CrossRef]
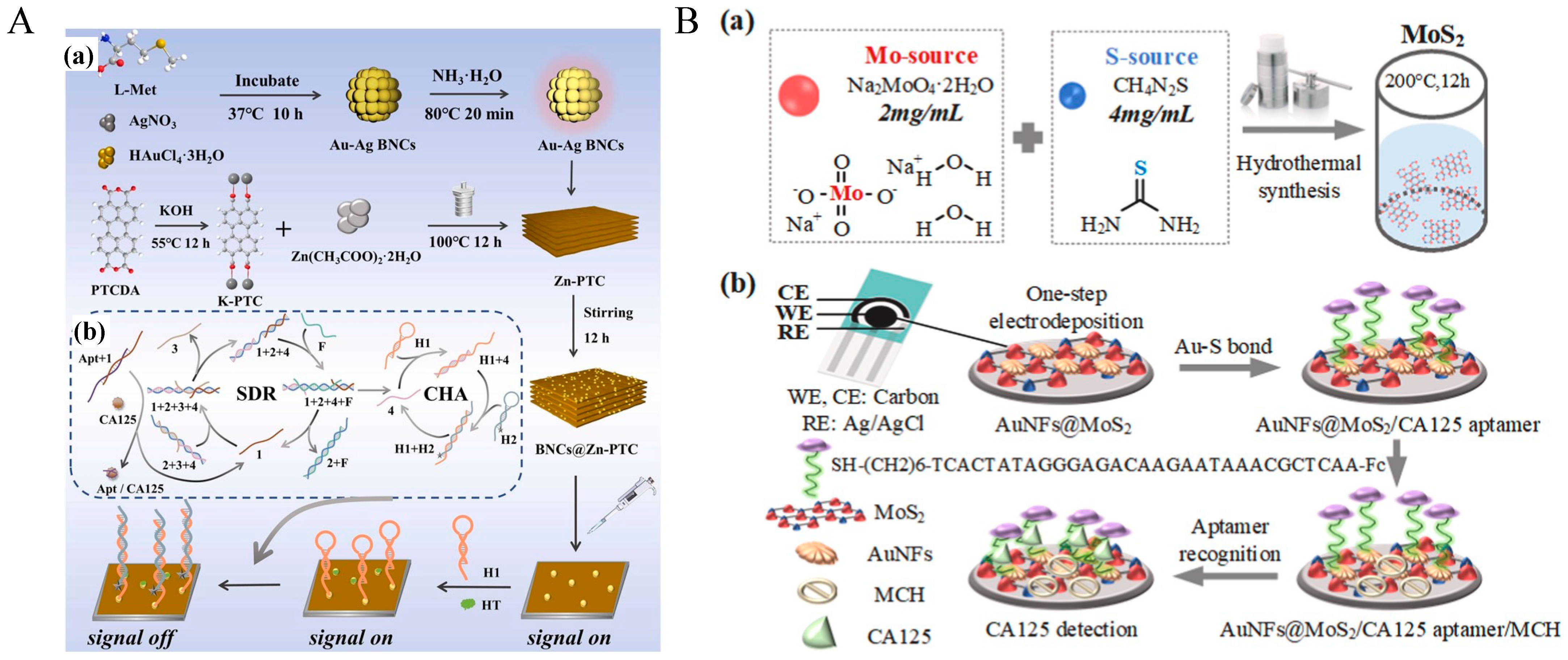
- Chen, Y.; Ye, Z.; Ma, M.; Wu, Y.; Yang, J.; Ma, P.; Zhang, Z.; Song, D. Electrochemiluminescence resonance energy transfer biosensor based on BNCs@Zn-PTC for ultrasensitive and low-potential detection of CA125 in pancreatic cancer diagnostics. Sens. Actuators B Chem. 2025, 427, 137136. [Google Scholar] [CrossRef]
- Shahbazlou, S.V.; Vandghanooni, S.; Dabirmanesh, B.; Eskandani, M.; Hasannia, S. Biotinylated aptamer-based SPR biosensor for detection of CA125 antigen. Microchem. J. 2023, 194, 109276. [Google Scholar] [CrossRef]
- Chen, J.; Hu, W.; Wei, J.; Yu, F.; Wu, L.; Wang, C.; Wang, W.; Zuo, S.; Shang, B.; Chen, Q. An electrochemical aptasensing platform for carbohydrate antigen 125 based on the use of flower-like gold nanostructures and target-triggered strand displacement amplification. Microchim. Acta 2019, 186, 388. [Google Scholar] [CrossRef]
- Zhang, F.; Fan, L.; Liu, Z.; Han, Y.; Guo, Y. A label-free electrochemical aptasensor for the detection of cancer antigen 125 based on nickel hexacyanoferrate nanocubes/polydopamine functionalized graphene. J. Electroanal. Chem. 2022, 918, 116424. [Google Scholar] [CrossRef]
- Hu, C.; Qin, Z.; Fu, J.; Gao, Q.; Chen, C.; Tan, C.S.; Li, S. Aptamer-based carbohydrate antigen 125 sensor with molybdenum disulfide functional hybrid materials. Anal. Biochem. 2023, 675, 115213. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Chen, X.; Wang, J.; Ma, M.; He, A.; Liu, R. Label-free electrochemical biosensor with magnetically induced self-assembly for the detection of cancer antigen 125. Arab. J. Chem. 2023, 16, 105070. [Google Scholar] [CrossRef]
- Wang, W.-S.; Lin, J.-K.; Chiou, T.-J.; Liu, J.-H.; Fan, F.S.; Yen, C.-C.; Lin, T.-C.; Jiang, J.-K.; Yang, S.-H.; Wang, H.-S. CA19-9 as the most significant prognostic indicator of metastatic colorectal cancer. Hepatogastroenterology 2002, 49, 160–164. [Google Scholar]
- Lakemeyer, L.; Sander, S.; Wittau, M.; Henne-Bruns, D.; Kornmann, M.; Lemke, J. Diagnostic and prognostic value of CEA and CA19-9 in colorectal cancer. Diseases 2021, 9, 21. [Google Scholar] [CrossRef]
- Lan, Y.; Ni, W.; Tai, G. Expression of MUC1 in different tumours and its clinical significance. Mol. Clin. Oncol. 2022, 17, 161. [Google Scholar] [CrossRef]
- Otoo, J.A.; Schlappi, T.S. REASSURED multiplex diagnostics: A critical review and forecast. Biosensors 2022, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Shanmugasundaram, K.B.; Li, J.; Sina, A.I.; Wuethrich, A.; Trau, M. Toward precision oncology: SERS microfluidic systems for multiplex biomarker analysis in liquid biopsy. Mater. Adv. 2022, 3, 1459–1471. [Google Scholar] [CrossRef]
- Su, M.; Zhang, Z.; Zhou, L.; Han, C.; Huang, C.; Nice, E.C. Proteomics, personalized medicine and cancer. Cancers 2021, 13, 2512. [Google Scholar] [CrossRef]
- Reese, K.-L.; Pantel, K.; Smit, D.J. Multibiomarker panels in liquid biopsy for early detection of pancreatic cancer–a comprehensive review. J. Exp. Clin. Cancer Res. 2024, 43, 250. [Google Scholar] [CrossRef]
- Ma, C.; Liu, H.; Zhang, L.; Li, H.; Yan, M.; Song, X.; Yu, J. Multiplexed aptasensor for simultaneous detection of carcinoembryonic antigen and mucin-1 based on metal ion electrochemical labels and Ru (NH3)63+ electronic wires. Biosens. Bioelectron. 2018, 99, 8–13. [Google Scholar] [CrossRef]
- Zhao, H.; Liu, Q.; Wang, J.; Huang, A.; Qiu, B.; Lin, Z. Electrochemical aptamer sensor based on metal ion-labeled polyethyleneimine gold nanoparticles for simultaneous detection of multiple disease markers. Electrochim. Acta 2021, 399, 139423. [Google Scholar] [CrossRef]
- Zou, M.; Gong, Y.; Sun, X.; Ding, C. All-in-one magnetic beads: Searching, capturing and simultaneous detection of dual tumor related proteins in real samples. Sens. Actuators B Chem. 2022, 369, 132330. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, S.; Lu, C.; Yang, X. Three kinds of DNA-directed nanoclusters cooperating with graphene oxide for assaying mucin 1, carcinoembryonic antigen and cancer antigen 125. Sens. Actuators B Chem. 2018, 262, 9–16. [Google Scholar] [CrossRef]
- Li, Z.; Gu, Y.; Ge, S.; Mao, Y.; Gu, Y.; Cao, X.; Lu, D. An aptamer-based SERS–LFA biosensor with multiple channels for the ultrasensitive simultaneous detection of serum VEGF and osteopontin in cervical cancer patients. New J. Chem. 2022, 46, 20629–20642. [Google Scholar] [CrossRef]
- Chen, Y.; Ye, Z.; Ma, M.; Yang, J.; Liu, R.; Zhang, Y.; Ma, P.; Song, D. Electrochemiluminescence biosensor for specific detection of pancreatic ductal carcinoma through dual targeting of MUC1 and miRNA-196a. Biosens. Bioelectron. 2024, 254, 116241. [Google Scholar] [CrossRef]
- Kalluri, R.; LeBleu, V.S. The biology, function, and biomedical applications of exosomes. Science 2020, 367, eaau6977. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.S.; Jung, S.B.; Park, S.; Dua, P.; Lee, D.K. Alppl2 Is a Potential Diagnostic Biomarker for Pancreatic Cancer-Derived Extracellular Vesicles. Mol. Ther. Methods Clin. Dev. 2019, 15, 204–210. [Google Scholar] [CrossRef]
- Xu, L.; Chopdat, R.; Li, D.; Al-Jamal, K.T. Development of a simple, sensitive and selective colorimetric aptasensor for the detection of cancer-derived exosomes. Biosens. Bioelectron. 2020, 169, 112576. [Google Scholar] [CrossRef]
- Feng, J.; Jia, L.; Pan, W.; Fan, Y.; Guo, J.; Luo, T.; Liu, C.; Wang, W.; Zheng, L.; Li, B. Rapid and efficient fluorescent aptasensor for PD-L1 positive extracellular vesicles isolation and analysis: EV-ANCHOR. Chem. Eng. J. 2023, 465, 142811. [Google Scholar] [CrossRef]
- Liga, A.; Vliegenthart, A.D.; Oosthuyzen, W.; Dear, J.W.; Kersaudy-Kerhoas, M. Exosome isolation: A microfluidic road-map. Lab. Chip 2015, 15, 2388–2394. [Google Scholar] [CrossRef]
- Zhang, Q.; Ma, R.; Zhang, Y.; Zhao, J.; Wang, Y.; Xu, Z. Dual-Aptamer-Assisted Ratiometric SERS Biosensor for Ultrasensitive and Precise Identification of Breast Cancer Exosomes. ACS Sens. 2023, 8, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Xia, L.; Mei, W.; Zou, Q.; Liu, H.; Wang, H.; Zou, L.; Wang, Q.; Yang, X.; Wang, K. One-step multiplex analysis of breast cancer exosomes using an electrochemical strategy assisted by gold nanoparticles. Anal. Chim. Acta 2023, 1254, 341130. [Google Scholar] [CrossRef] [PubMed]
- Su, W.; Li, J.; Ji, C.; Chen, C.; Wang, Y.; Dai, H.; Li, F.; Liu, P. CRISPR/Cas systems for the detection of nucleic acid and non-nucleic acid targets. Nano Res. 2023, 16, 9940–9953. [Google Scholar] [CrossRef] [PubMed]
- de Voogt, W.S.; Tanenbaum, M.E.; Vader, P. Illuminating RNA trafficking and functional delivery by extracellular vesicles. Adv. Drug Deliv. Rev. 2021, 174, 250–264. [Google Scholar] [CrossRef]
- Laing, S.; Sloan-Dennison, S.; Faulds, K.; Graham, D. Surface Enhanced Raman Scattering for Biomolecular Sensing in Human Healthcare Monitoring. ACS Nano 2025, 19, 8381–8400. [Google Scholar] [CrossRef]

| Biomarker | Aptamer Sequence (5′-3′) | Aptamer Name | Aptamer Type | Kd (nM) | Kd Measurement Method | Immobilization | Ref. |
|---|---|---|---|---|---|---|---|
| CA19-9 | GACTGGCCCAGGCCCCCTCCTCCCGCTGCTGCCCGCCCTC | CA19-9 aptamer | DNA | 20.05 ± 3.02 | Fluorescence assay | Polystyrene plate | [166] |
| CEA | ATACCAGCTTATTCAATT | b1-18 (5′ primer) | DNA | 0.69 | Fluorescence Polarization (FP) | Free in solution | [167] |
| CCGATCCCACCGACCGCGCCCTGCCTCAGCCCCTCCCCGTG | NR * | DNA | 41.49 ± 9.97 | Fluorescence | Polystyrene plate | [166] | |
| GGGGGGTGTATCGTTGACGAGTTGCGCGTGCGTCTCGTG | Apta 3 | DNA | 60.4 ± 5.7 | qPCR | Free in solution | [168] | |
| GGAGCTACGTTTAGCGAGTCCGACGCTCGGTGCCTCTTC | Apta 5 | DNA | 37.8 ± 5.8 | qPCR | Free in solution | [168] | |
| ATACCAGCTTATTCAATTATG | P-ATG | DNA | 4.62 | Biolayer Interferometry (BLI) | Streptavidin-coated biosensor (SSA) | [169] | |
| GACATACCAGCTTATTCAATT | GAC-P | DNA | 3.93 | BLI | Streptavidin-coated biosensor (SSA) | [169] | |
| CCGCTACCCCCCACGCAATCCCG | G3S1.5 | DNA | 2.46 | Isothermal titration calorimetry (ITC) | Free in solution | [170] | |
| GCCAGCGAGTTTTGACCGTTTTTCTCTCTTTTCCGCCTA | Aptamer (6) | DNA | 312.6 | ELONA | CEA-coated plate | [171] | |
| MUC1-APDTRPAPG epitope | GCAGTTGATCCTTTGGATACCCTGG | MUC1 S1.3/S2.2 | DNA | 0.135 | Surface Plasmon Resonance (SPR) | Biotinylated peptide on streptavidin chip | [172] |
| MUC1-5TR-GalNAc (Tn antigen) | GGCTATAGCACATGGGTAAAACGAC | 5TRG2 | DNA | 18.6 | SPR | Nickel-NTA chip | [173] |
| Unglycosylated MUC1-5TR peptide (5 tandem repeats) | GAAGTGAAAATGACAGAACACAACA | 5TR1 | DNA | 21.0 | SPR | Nickel-NTA chip | [173] |
| MUC1-N-acetylgalactosamine (GalNAc) alone | AAGGGATGACAGGATACGCCAAGCT | GalNAc3 | DNA | 47.3 | SPR | 96-well polystyrene plate | [173] |
| MUC1-APDTRPAPG epitope | AACCGCCCAAATCCCTAAGAGTCGGACTGCAACCTATGCTATCGTTGATGTCTGTCCAAGCAACACAGACACACTACACACGCACA | MA3 | DNA | 38.3 | Flow cytometry | Peptide conjugated to magnetic beads | [174] |
| CA125 | AGGCGGGCGGCGTGGCGATGTTACTGCGTGTGTGTTCGTG | CA125-aptamer | DNA | 17.41 ± 2.26 | Fluorescence | Polystyrene plate | [166] |
| ACTAGCTCCGATCTTTCTTATCTAC | CA125 1 | DNA | 207 ± 109 U/mL (FA), 80 ± 38 U/mL (APCE) | Fluorescence Anisotropy (FA), Affinity Probe Capillary Electrophoresis (APCE) | Free in solution | [175] | |
| TGCCTTATTACTCTCTCCTGTTAAC | CA125 12 | DNA | 118 ± 123 U/mL (FA), 131 ± 93 U/mL (APCE) | FA, APCE | Free in solution | [175] | |
| TAGGGAAGAGAAGGACATATGATTTTAGGGAAGAGAAGGACTTTTATGCCGCCTTGACTAGTACATGACCACTTGA | Apt 2.26 | DNA | 166 | Membrane-based assessment of bound ssDNA | Nitrocellulose membrane (0.2 μm pore size) with immobilized CA125 | [176] | |
| ACCACCACCACGACGCACGAGTACCCCGCG | rCAA-8 | DNA | 166 | BLI | Streptavidin-coated optical sensor | [177] | |
| AAAAUGCAUGGAGCGAAGGUGUGGGGGAUACCAACCGCGCCGUG | CA125.1 | RNA | 4.13 | SPR | Covalent immobilization on CM5 biochip | [178] | |
| Osteopontin | TGTGTGCGGCACTCCAGTCTGTTACGCCGC | C10K2 | DNA | 2.5 (30 min), 1.1 (4 h) | Fluorescence assay | Streptavidin-biotin interaction on a gold electrode | [179] |
| CGGCCACAGAAUGAAAAACCUCAUCGAUGUUG | OPN-R3 | RNA | 18.00 | NR * | NR * | [180] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, W.; Cui, J.; Wang, X.-Y.; Siu, R.H.P.; Tanner, J.A. Early-Stage Pancreatic Cancer Diagnosis: Serum Biomarkers and the Potential for Aptamer-Based Biosensors. Molecules 2025, 30, 2012. https://doi.org/10.3390/molecules30092012
He W, Cui J, Wang X-Y, Siu RHP, Tanner JA. Early-Stage Pancreatic Cancer Diagnosis: Serum Biomarkers and the Potential for Aptamer-Based Biosensors. Molecules. 2025; 30(9):2012. https://doi.org/10.3390/molecules30092012
Chicago/Turabian StyleHe, Weisi, Jingyu Cui, Xue-Yan Wang, Ryan H. P. Siu, and Julian A. Tanner. 2025. "Early-Stage Pancreatic Cancer Diagnosis: Serum Biomarkers and the Potential for Aptamer-Based Biosensors" Molecules 30, no. 9: 2012. https://doi.org/10.3390/molecules30092012
APA StyleHe, W., Cui, J., Wang, X.-Y., Siu, R. H. P., & Tanner, J. A. (2025). Early-Stage Pancreatic Cancer Diagnosis: Serum Biomarkers and the Potential for Aptamer-Based Biosensors. Molecules, 30(9), 2012. https://doi.org/10.3390/molecules30092012